Introduction
Compared with female breast cancer, male breast
cancer (MBC) is a rare malignancy, accounting for only 0.6–1% of
all breast cancer cases (1).
Statistics indicate that in 2021, there were only 38,827 new cases
of MBC worldwide, with 13,274 mortalities (2). From 1990 to 2021, the global burden of
MBC increased, exhibiting notable regional disparities.
Specifically, Eastern Sub-Saharan Africa bore the highest burden,
while Oceania had the lowest. Disparities were also observed across
socio-demographic index (SDI) levels: High-middle SDI regions
showed the highest lifetime risk of incidence and low SDI regions
showed the highest mortality risk. Temporal trends differed
markedly by region as well (2).
Risk factors include advanced age, obesity, testicular disease,
intake of medications and exogenous hormones (such as those used in
gender transition therapy) and BRCA2 gene mutations; BRCA2 mutation
carriers face an 80-fold higher cancer risk than the general
population (3). Influenced by
societal perceptions and sex factors, patients with MBC typically
present for medical care at a later stage. At diagnosis, the
disease is often at a more advanced clinical stage and higher
histological grade, resulting in worse overall prognosis and
markedly reduced 5-year survival rates compared with female
patients (4). However, due to the
limited sample size of MBC cases and the lack of large-scale
clinical trial data, clinical treatment often follows female breast
cancer guidelines, leaving the optimal treatment regimen unclear.
Based on current epidemiological and histopathological data,
>90% of patients with MBC are estrogen receptor (ER)-positive
and human epidermal growth factor receptor 2 (HER2)-negative. Their
biological characteristics resemble those of postmenopausal hormone
receptor-positive breast cancer in women. Modified radical
mastectomy is the most common surgical approach, followed by
adjuvant systemic therapy with tamoxifen (5).
The present study reports a case of breast cancer in
a very elderly male patient from China, who presented with advanced
disease involving multiple organ metastases and end-stage renal
disease (ESRD). Unlike prior reports that focused on early-stage or
younger male patients, the present case uniquely combines three
challenging factors: Advanced age (90 years), ESRD [chronic kidney
disease (CKD) stage 3b-5] and a locally advanced ulcerated breast
mass (T4b) (6,7). This combination has rarely been
described and poses distinct therapeutic dilemmas. Following
pathological confirmation of invasive breast cancer, a palliative
mastectomy was performed based on the overall condition of the
patient and comorbidities. Adjuvant endocrine therapy was planned
for subsequent treatment, thereby providing an individualized
diagnostic and therapeutic approach for this special patient
population.
Case report
A 90-year-old male patient was admitted in August
2025 to the Affiliated Hospital of Nanjing University of Chinese
Medicine (Nanjing, China) for a left breast mass with local itching
for >2 months, ulceration with bloody serous discharge and pain
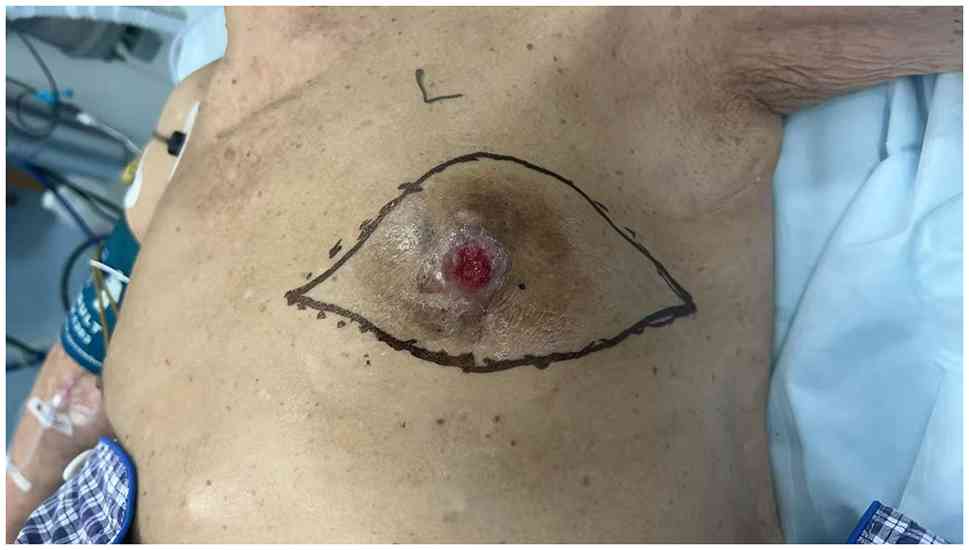
for 1 week. A physical examination revealed destruction of normal
left breast structures. A large ulcerative mass, ~5.0×4.5 cm in
size, was visible in the central region. The ulcer base contained
bloody exudate, with raised, everted and hardened margins
presenting a typical ‘crater-like’ appearance. The mass was firm,
fixed and prone to bleeding upon palpation. The nipple-areolar
complex was absent. The surrounding skin exhibited edema, erythema
and hyperpigmentation. Palpation revealed diffuse glandular
sclerosis with indistinct borders throughout the breast. Enlarged
left axillary lymph nodes were palpable (Fig. 1). The breast ultrasound identified a
suspicious, irregular hypoechoic mass (50.8×45.1×26.1 mm) with
spiculated margins, containing microcalcifications and posterior
acoustic shadowing (breast imaging-reporting and data system 5).
Enlarged axillary and supraclavicular lymph nodes suggested
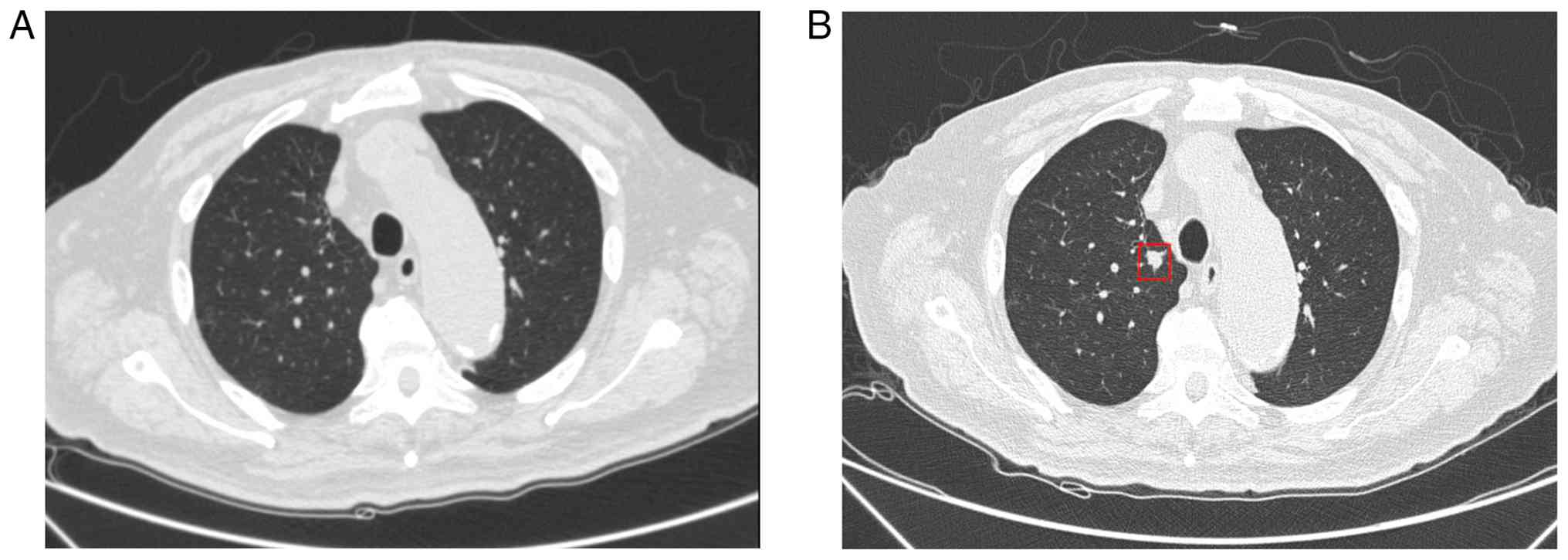
potential metastasis (Fig. 2A-F). A
chest CT confirmed multiple new pulmonary nodules, with a larger
solid nodule located in the apical segment of the right upper lobe
consistent with metastatic characteristics (Fig. 3).
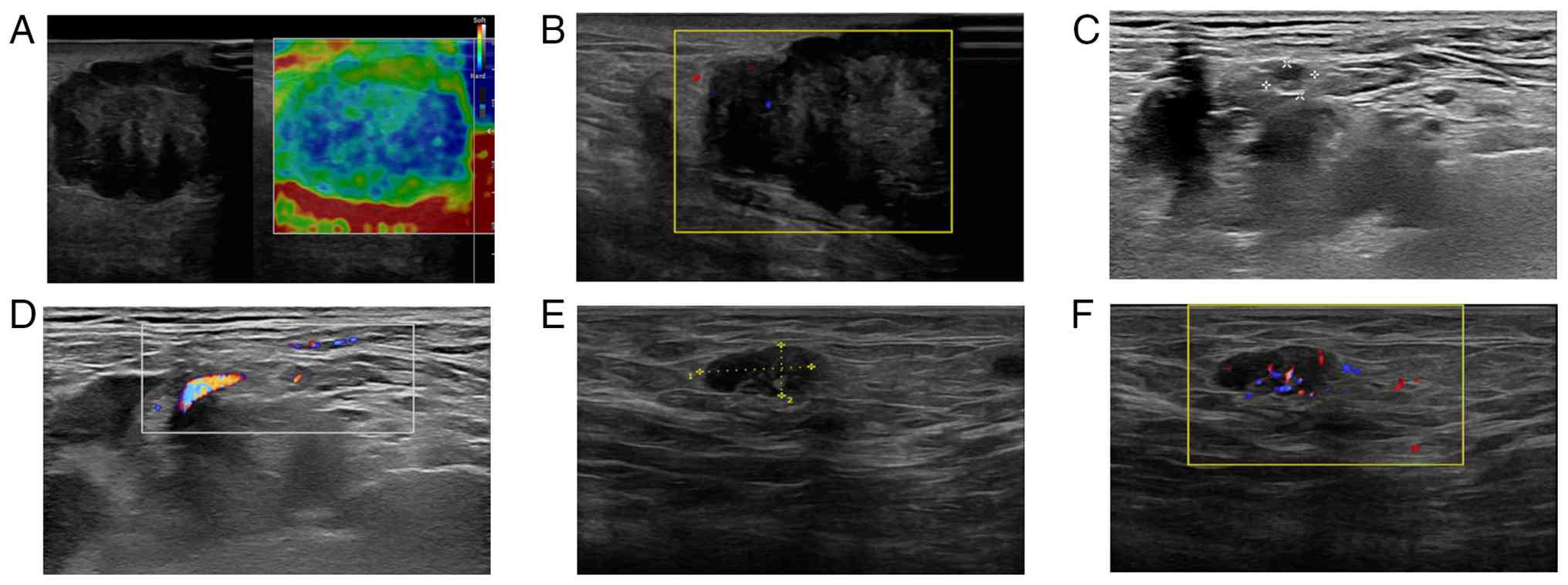 | Figure 2.Ultrasound images of the breast and
lymph nodes. (A) Ultrasound B-mode imaging of the left breast shows
a hypoechoic nodule measuring 50.8×45.1×26.1 mm, with spiked
margins, heterogeneous internal echoes, and posterior acoustic
shadowing. Concomitant elastography demonstrates predominantly blue
color in the central area and green color at the periphery,
corresponding to an elasticity score of 3, indicating increased
tissue stiffness. (B) CDFI reveals intralesional blood flow signals
within the left breast nodule. (C) B-mode ultrasound of the left
supraclavicular fossa demonstrates an oval hypoechoic lesion
measuring 6×4 mm, with clear borders, regular shape, and slightly
heterogeneous cortical echoes. The lymphatic hilum is indistinct.
(D) CDFI shows spot-like and strip-like blood flow signals within
the left supraclavicular hypoechoic lesion. (E) B-mode ultrasound
of the left axilla shows multiple heterogeneous lesions, the
largest of which measures 12.4×8.0 mm, with ill-defined margins,
irregular shape, heterogeneous internal echoes, focal anechoic
areas, and loss of the lymphatic portal structure. (F) CDFI
demonstrates abundant blood flow signals within the enlarged left
axillary lymph node. CDFI, Color Doppler flow imaging. |
The patient had a history of severe ESRD [CKD stage
5; June 2024 serum creatinine, 446.2 µmol/l; estimated glomerular
filtration rate (eGFR), 9.32 ml/min/1.73 m2], which was
managed conservatively. Upon the current admission, renal function
was markedly improved compared with previous assessments, with
serum creatinine at 166.1 µmol/l and eGFR at 32.5 ml/min/1.73
m2 (calculated using the CKD-Epidemiology Collaboration
formula), consistent with CKD stage 3b. Complications of renal
insufficiency included renal anemia (hemoglobin, 101 g/l) and
nephrogenic edema. A suprapubic cystostomy had been performed in
September 2024 due to urinary retention. Vital signs and other
major organ examinations were generally stable.
A multidisciplinary team (MDT) consultation and a
review of relevant treatment guidelines were thoroughly
communicated to the patient and their family. Considering their
advanced age, stage IV breast cancer and concomitant ESRD,
palliative debulking surgery was performed, specifically a simple
left mastectomy, aimed at controlling the local tumor and improving
quality of life. The patient was discharged on the third
postoperative day. During the hospital stay, the surgical wound
healed well without complications such as bleeding, infection or
skin flap necrosis. Quality of life was assessed using the Eastern
Cooperative Oncology Group (ECOG) performance status scale at
admission (ECOG 3), at discharge (ECOG 2), at a 1-month follow-up
(ECOG 1) and at the last follow-up 6 months after surgery (ECOG 1).
The patient reported notable relief from local pain and bleeding,
as well as improved sleep and appetite. As of the last follow-up
(March 2026), the patient remained alive with no evidence of local
recurrence or distant progression. They continued to take tamoxifen
and medications for the renal disease without major adverse events.
At that time, progression-free survival had exceeded 7 months, and
overall survival continued to be followed.
Postoperative pathology
On gross examination, the invasive ductal carcinoma
measured 5.5×3.8×3 cm, with macroscopic involvement of the skin and
nipple-areolar complex accompanied by ulceration. Microscopic
examination confirmed a Nottingham histological grade 3 carcinoma
(histological score 7: Tubule formation 3, nuclear pleomorphism 3,
mitotic count 1), with a high-grade ductal carcinoma in situ
component. Vascular invasion was identified on hematoxylin and
eosin (H&E)-stained sections (+), and perineural invasion was
absent (−). Pathological pTNM staging was classified according to
the 8th edition AJCC staging system, with a stage of pT4bNx
(8). Immunohistochemical staining
was performed on formalin-fixed, paraffin-embedded tumor tissue
following standard pathological protocols at the Affiliated
Hospital of Nanjing University of Chinese Medicine.
Immunohistochemical staining and mucicarmine staining were
performed to detect the expression of relevant proteins and the
distribution of mucus in tumor tissues, respectively. Mucicarmine
staining revealed positive mucus staining both inside and outside
the tumor cells. Tissue samples were fixed in 4% neutral buffered
formalin at room temperature for 24 h. After rinsing thoroughly,
the specimens were subjected to gradual dehydration with gradient
concentrations of ethanol. The dehydration procedure was performed
sequentially in 70, 80, 90, 95% and absolute ethanol successively
to completely remove internal moisture from tissues. After full
dehydration, the tissues were cleared with xylene and finally
embedded in paraffin wax. Serial sections were cut at a thickness
of 3 µm. Paraffin sections were baked in an incubator at 65°C for
30 min to enhance tissue adherence to glass slides. Subsequently,
the sections were deparaffinized in xylene and rehydrated through a
graded ethanol series. To inhibit endogenous peroxidase activity,
tissue sections were treated with 3% hydrogen peroxide at room
temperature for 20 min. Immunohistochemical staining was performed
using a Benchmark ULTRA automated immunohistochemistry stainer
(Roche Tissue Diagnostics) according to the manufacturer's
instructions with the ultraView Universal DAB Detection Kit (cat.
no. 05269806001; Roche Diagnostics (Shanghai) Co., Ltd.). All
experimental procedures, including blocking, primary antibody
incubation, secondary antibody/linker incubation, HRP polymer
incubation, washing and DAB color development, were automatically
completed by the instrument following preset programs. Known
positive tissue sections were used as positive controls, and PBS
was used instead of the primary antibody as a negative control. All
primary antibodies used in the present study were ready-to-use
commercial reagents without any further manual dilution. The
primary antibodies used were as follows: ER (cat. no. 05278414001;
Clone: SP1; Roche Diagnostics (Shanghai) Co., Ltd.); PR (cat. no.
05278392001; Clone: 1E2; Roche Diagnostics (Shanghai) Co., Ltd.);
AR (cat. no. ZA-0554; Clone: EP120; Beijing Zhongshan Golden Bridge
Biotechnology Co., Ltd.); HER2 (cat. no. 05999570001; Clone: 4B5;
Roche Diagnostics (Shanghai) Co., Ltd.); Ki-67 (cat. no.
05278384001; Clone: 46295; Roche Diagnostics (Shanghai) Co., Ltd.);
Cytokeratin 5/6 (CK5/6; cat. no. 06478441001; Clone: D5/16 B4;
Roche Diagnostics (Shanghai) Co., Ltd.); E-cadherin (cat. no.
04015630983872; Clone: 36; Roche Diagnostics (Shanghai) Co., Ltd.);
p120 (cat. no. 05867088001; Clone: 98; Roche Diagnostics (Shanghai)
Co., Ltd.); EGFR (cat. no. ZA-00505; Clone: EP22; Beijing Zhongshan
Golden Bridge Biotechnology Co., Ltd.); SOX10 (cat. no. ZM-0366;
Clone: MRQ-58; Beijing Zhongshan Golden Bridge Biotechnology Co.,
Ltd.); p40 (cat. no. 07394420001; Clone: BC28; Roche Diagnostics
(Shanghai) Co., Ltd.); TRPS1 (cat. no. ZA-0681; Clone: B22; Beijing
Zhongshan Golden Bridge Biotechnology Co., Ltd.); D2-40 (cat. no.
X0931; Clone: D2-40; Agilent Technologies Co., Ltd.); p63 (cat. no.
05867061001; Clone: 4A4; Roche Diagnostics (Shanghai) Co., Ltd.).
The secondary antibodies and matching linker reagents were
supporting components contained in the ultraView Universal DAB
Detection Kit [cat. no. 05269806001; Roche Diagnostics (Shanghai)
Co., Ltd.]. These reagents were pre-configured ready-to-use
products specifically adapted to the Benchmark ULTRA automatic
staining platform, and all incubation and reaction procedures were
finished automatically by the instrument in accordance with
built-in standard protocols. Stained sections were observed and
images were captured using a Leica DM-2000 light microscope. The
immunohistochemistry results showed ER (~95%, strongly positive),
PR (~10%, moderately to strongly positive), AR (negative), HER2
(1+), Ki-67 (~70% positive), cytokeratin 5/6 (CK5/6; -), E-cadherin
(+++), p120 (cell membrane, +++), EGFR (−), SOX10 (−), p40 (−),
trichorhinophalangeal syndrome 1 (+++), D2-40 (highlighting
vascular channels and p63 (−) (Figs.
4 and S1).
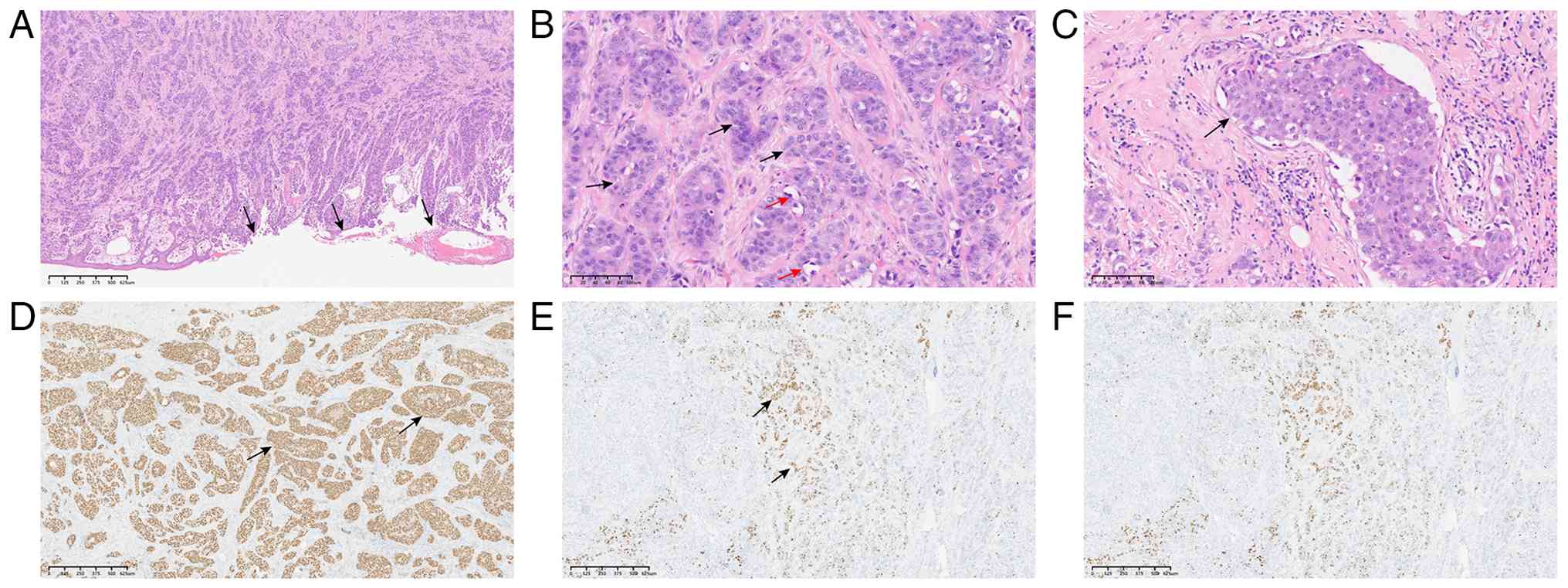 | Figure 4.Postoperative pathological images of
invasive breast carcinoma in the patient (August 2025). (A) H&E
staining shows invasive breast carcinoma invading the epidermis
with ulceration. Arrows indicate the edge of epidermal ulceration
(original magnification, ×40; scale bar, 625 µm). (B) H&E
staining reveals that tumor cells are arranged in nests or tubular
structures with glandular lumina, separated by collagen fibers.
Tumor cells are large and pleomorphic with slightly eosinophilic or
vacuolated cytoplasm, marked nuclear atypia, prominent nucleoli and
readily visible mitotic figures. Black arrows indicate tumor
nests/tubular structures separated by collagen fibers, and red
arrows point to pleomorphic tumor cells with prominent nucleoli and
mitotic figures (original magnification, ×200; scale bar, 100 µm).
(C) H&E staining demonstrates intravascular tumor thrombi;
arrows indicate tumor cell clusters (vascular tumor emboli) within
the vascular lumen (original magnification, ×200; scale bar, 100
µm). Immunohistochemical results, (D) Tumor cells show strong
nuclear positivity for estrogen receptor (ER). Arrows indicate
nuclear positivity in tumor cells (original magnification, ×40;
scale bar, 625 µm). (E) Tumor cells exhibit moderate-to-strong
nuclear positivity for progesterone receptor (PR). Arrows indicate
nuclear positivity in tumor cells (original magnification, ×40;
scale bar, 625 µm). (F) Tumor cells show low expression of human
epidermal growth factor receptor 2 (HER2), with weak and incomplete
membranous staining in a portion of tumor cells and no
circumferential membranous staining (IHC 1+; original
magnification, ×200; scale bar, 100 µm). |
Immunohistochemistry results demonstrated strong
hormone receptor positivity (ER, 95%; PR, 10%), indicating that the
patient was suitable for adjuvant endocrine therapy. After a
comprehensive assessment of the risks and benefits associated with
their advanced age, poor general condition and ESRD, tamoxifen was
selected as the first-line agent. The patient is currently taking
daily tamoxifen and renal protective medication. During treatment,
renal function has been closely monitored and remained stable, with
no evidence of deterioration related to tamoxifen administration.
Close monitoring for drug-related adverse reactions will be
continued, with particular emphasis on changes in renal function.
This individualized treatment plan aims to maximize therapeutic
benefit while minimizing the risk of further renal impairment.
Discussion
The present report describes the management of an
extremely rare case of metastatic breast cancer in a very elderly
(90-year-old) male patient, whose condition was notably complicated
by concomitant ESRD. The present case highlights the immense
challenges in developing individualized treatment strategies when
very advanced age, multiple comorbidities (particularly ESRD) and
advanced cancer coexist. Most published MBC cases involve patients
without severe renal impairment or with early-stage disease. The
present patient's triad of very advanced age (90 years), ESRD
requiring cystostomy and T4b ulcerated tumor represents a rare
clinical scenario that demands individualized palliative
management. The core dilemma lies in balancing limited oncological
benefit against substantial risks of treatment-related
toxicity.
Breast cancer is a rare disease in men, accounting
for ~1% of all breast cancer cases. Its occurrence is associated
with increased age, familial inheritance, obesity, testicular
disease and elevated serum estrogen levels due to radiation
exposure (9). Previous studies have
confirmed that high-risk BRCA1/2 gene mutations not only increase
men's risk of developing breast cancer but are also linked to an
elevated risk of prostate cancer (10–12). A
real-world study examining the characteristics of MBC in China
(13) conducted a retrospective
analysis of 1,119 Chinese patients with MBC. The average age at
diagnosis was 60.9 years, with most patients clinically staged at
stage II and hormone receptor-positive subtypes predominating.
Therapeutically, the vast majority underwent mastectomy followed by
adjuvant chemotherapy, with hormone receptor-positive cases
additionally receiving endocrine therapy. Due to insufficient
breast cancer health education and screening coverage, Chinese
patients are more likely than their American counterparts to
present with locally advanced disease (14).
Currently, due to the lack of clinical research data
specifically targeting MBC, its diagnosis and treatment strategies
generally follow guidelines for female breast cancer, primarily
including surgery, chemotherapy, radiotherapy and adjuvant
endocrine and targeted therapies (15). However, existing literature lacks
systematic reports on treatment strategies for very elderly male
patients with advanced breast cancer, particularly regarding
individualized treatment options in cases involving multiple
comorbidities (such as ESRD) and metastatic disease. This gap
underscores the urgency and importance of individualized treatment
decisions based on chronological age, functional status,
comorbidity burden and patient preferences. For this special
population, treatment goals should prioritize quality of life
improvement and local symptom control, while more real-world
studies and consensus guidelines are needed to inform clinical
practice.
The present case presents an extremely rare instance
of breast cancer in a very elderly male patient concurrent with
ESRD. The presence of ESRD notably limits treatment options and
increases treatment risks. When kidney disease progresses to its
final stage, it is termed ESRD, representing kidney failure where
renal function is completely lost, necessitating renal replacement
therapy such as hemodialysis or kidney transplantation (16). ESRD impacts all aspects of cancer
treatment. Studies indicate dialysis patients face a 42% higher
risk of developing breast cancer compared with the general
population (17,18). This increased risk may be attributed
to chronic inflammation, immune dysfunction, prolonged uremic toxin
exposure or impaired DNA repair mechanisms in patients with
end-stage renal disease (19).
Furthermore, the persistent oxidative stress and chronic
inflammatory state associated with ESRD may exacerbate mitotic
activity and tumor cell proliferation, contributing to increased
breast cancer aggressiveness (20).
ESRD alters drug pharmacokinetics, compromises renal clearance,
elevates blood drug concentrations and increases toxicity risks
(18). Patients with ESRD exhibit
compromised immunity, heightened infection susceptibility and
greater vulnerability to adverse reactions such as bone marrow
suppression and neurotoxicity. Drugs such as platinum-based agents,
capecitabine, methotrexate and cyclophosphamide, which are renally
excreted, require discontinuation or notable dose adjustments in
these patients. This severely limits treatment options, reduces
tolerance to antitumor therapy, and consequently impacts overall
survival and quality of life (21–23).
The present patient underwent palliative surgery
followed by endocrine therapy. Due to the advanced age of the
patient and potential for systemic metastasis, the goal was to
reduce tumor burden through palliative surgery while balancing
survival outcomes with quality-of-life benefits.
Immunohistochemistry demonstrated strong hormone receptor
positivity, leading to subsequent oral endocrine therapy. Tamoxifen
is primarily metabolized by the liver, posing minimal renal risk to
the patient; however, careful monitoring of hepatic and renal
function remains essential.
Metastatic breast cancer is incurable, necessitating
palliative treatment strategies focused on systemic therapy guided
by breast cancer subtype. Palliative care is a patient-centered
approach emphasizing optimal symptom management and providing
psychosocial and spiritual support based on the needs of the
patient, values, beliefs and culture. Palliative care can improve
quality of life and symptoms while reducing mortality rates
(24,25). Palliative surgery controls local
breakdown, bleeding and infection symptoms, aiming to reduce tumor
burden and improve quality of life. Multiple retrospective studies
indicate that palliative surgery in patients with metastatic breast
cancer may also yield certain survival benefits (26–28).
In the present case, due to the age of the patient, ESRD and
metastatic status, the decision to perform palliative surgical
resection while forgoing radiotherapy and chemotherapy, and to
continue subsequent endocrine therapy, represented an inevitable
outcome of risk-benefit balancing. This also highlights the central
role of MDT collaboration in decision-making for such complex
cases.
The present study has limitations. First, as a
single case report, it cannot yield generalizable conclusions.
Second, the follow-up period was relatively short, precluding
assessment of long-term oncological outcomes. Finally, the
treatment decision in the present case was highly individualized.
Due to the advanced age of the patient and multiple comorbidities,
the personalized approach combining palliative surgery with
endocrine therapy may not apply to all patients with advanced
metastatic breast cancer.
While the individual components of the present case
(MBC, advanced age and ESRD) are not rare, their combination in a
single patient, especially the triad of 90 years, ESRD with CKD
stage 3b-5 and a T4b ulcerated tumor, has been scarcely documented.
Moreover, the successful use of palliative mastectomy followed by
tamoxifen alone, without radiotherapy or chemotherapy, in a patient
who could not tolerate standard systemic therapy due to renal
failure, provides a real-world example of risk-benefit
decision-making. The present report does not claim a novel
molecular discovery but offers practical guidance for clinicians
facing similar therapeutic dilemmas in frail, multi-morbid elderly
patients.
Reports on metastatic breast cancer in very elderly
males remain scarce in both domestic and international literature.
The present case underscores several key principles in geriatric
oncology treatment and care. First, comprehensive and systematic
assessments must be conducted based on disease management
guidelines, considering the functional status of the patient and
the burden of comorbidities. This enables the development of
individualized treatment plans aimed at improving quality of life
without compromising survival outcomes. Second, for patients with
advanced tumors and severe comorbidities, palliative care becomes
essential for symptom control, tumor burden reduction, quality of
life enhancement and humanistic care. In this context, palliative
surgery serves as an effective tool for managing local tumor
symptoms and may extend survival to some extent. Third, managing
complex cases such as elderly patients with cancer requires MDT
collaboration. Integrating expertise from breast surgery, oncology,
anesthesiology, nephrology and palliative care enables the
provision of optimal treatment plans and clinical care. In summary,
while the long-term outcome of the present case remains to be
observed, it presents a valuable example for developing
individualized treatment plans for elderly patients with cancer
with severe comorbidities. Enhancing male awareness of breast
cancer can facilitate early detection and treatment, reduce stigma,
encourage proactive management and ultimately improve patient
prognosis.
In conclusion, the present case demonstrates the
successful management of a very elderly male patient with
metastatic breast cancer complicated by ESRD. Through
multidisciplinary evaluation, individualized palliative local
surgery and planned endocrine therapy were implemented. The present
case illustrates that even for patients with extremely complex
conditions, meaningful clinical interventions remain achievable
through patient-centered, quality-of-life-oriented individualized
strategies.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
The present work was supported by the Natural Science Foundation
of Jiangsu Province (grant no. BK20221424) and the National Natural
Science Foundation of China Young Scientist Fund (grant no.
82505693).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
MFC and CY conceived the overall concept and
designed the framework of this study. MFC and MF collected the
clinical case data and drafted the manuscript. XYL and HHW sorted
and analyzed the ultrasound and CT imaging data derived from
medical records, interpreted the radiological findings, and
participated in the writing and discussion of imaging
characteristics in the manuscript. KH participated in revising the
manuscript for important intellectual content, critically reviewed
the pathological and imaging data, and took part in the analysis
and interpretation of the research results. MFC and CY confirm the
authenticity of all the raw data. All authors meet the ICMJE
criteria for authorship, and have read and approved the final
version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of the present case report.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Miao H, Verkooijen HM, Chia KS, Bouchardy
C, Pukkala E, Larønningen S, Mellemkjær L, Czene K and Hartman M:
Incidence and outcome of male breast cancer: An International
population-based study. J Clin Oncol. 29:4381–4386. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Li Y, Huang Y, Huang H, Wei T, Zhang A,
Xing L, Yin X, Li H, Ren G and Li F: Global, Regional, and National
Burden of male breast cancer in 204 countries and territories: A
systematic analysis from the Global Burden of disease study,
1990–2021. EClinicalMedicine. 80:1030272025. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Fox S, Speirs V and Shaaban AM: Male
breast cancer: An update. Virchows Arch. 480:85–93. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wang F, Shu X, Meszoely I, Pal T, Mayer
IA, Yu Z, Zheng W, Bailey CE and Shu XO: Overall mortality after
diagnosis of breast cancer in men vs women. JAMA Oncol.
5:1589–1596. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Korde LA, Zujewski JA, Kamin L, Giordano
S, Domchek S, Anderson WF, Bartlett JM, Gelmon K, Nahleh Z, Bergh
J, et al: Multidisciplinary meeting on male breast cancer: Summary
and research recommendations. J Clin Oncol. 28:2114–2122. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wang Y, Chen K, Yang Y, Tan L, Chen L, Zhu
L, Su F, Liu X and Li S: Incidence and survival outcomes of early
male breast cancer: A population-based comparison with early female
breast cancer. Ann Transl Med. 7:5362019. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Li N, Wang X, Zhang H and Wang H: Young
male breast cancer, a small crowd, the survival, and prognosis?: A
population-based study. Medicine (Baltimore). 97:e126862018.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Amin MB, Greene FL, Edge SB, Compton CC,
Gershenwald JE, Brookland RK, Meyer L, Gress DM, Byrd DR and
Winchester DP: The Eighth Edition AJCC Cancer Staging Manual:
Continuing to build a bridge from a population-based to a more
‘personalized’ approach to cancer staging. CA Cancer J Clin.
67:93–99. 2017.PubMed/NCBI
|
|
9
|
Gucalp A, Traina TA, Eisner JR, Parker JS,
Selitsky SR, Park BH, Elias AD, Baskin-Bey ES and Cardoso F: Male
breast cancer: A disease distinct from female breast cancer. Breast
Cancer Res Treat. 173:37–48. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Nyberg T, Frost D, Barrowdale D, Evans DG,
Bancroft E, Adlard J, Ahmed M, Barwell J, Brady AF, Brewer C, et
al: Prostate cancer risks for male BRCA1 and BRCA2 mutation
carriers: A prospective cohort study. Eur Urol. 77:24–35. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cheng HH, Shevach JW, Castro E, Couch FJ,
Domchek SM, Eeles RA, Giri VN, Hall MJ, King MC, Lin DW, et al:
BRCA1, BRCA2, and associated cancer risks and management for male
patients: A review. JAMA Oncol. 10:1272–1281. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Li S, Silvestri V, Leslie G, Rebbeck TR,
Neuhausen SL, Hopper JL, Nielsen HR, Lee A, Yang X, McGuffog L, et
al: Cancer risks associated with BRCA1 and BRCA2 pathogenic
variants. J Clin Oncol. 40:1529–1541. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Gao Y, Zhang M, Sun G, Ma L, Nie J, Yuan
Z, Liu Z, Cao Y, Li J, Liu Q, et al: The features of male breast
cancer in China: A real-world study. Breast. 76:1037622024.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Gao Y, Zhang M, Nie J, Ye G, Sun G, Ma L,
Wang H, Jiang Z and Lin Y: Comparison of male breast cancer in
China and the US: A real-world cohort study. Transl Breast Cancer
Res. 7:32026. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Faridi A, Gerber B and Hartmann S:
Diseases of the male breast: Gynecomastia and breast cancer. Dtsch
Arztebl Int. 122:406–411. 2025.PubMed/NCBI
|
|
16
|
Tufenkjy E and Lahdo R: Hemodialysis and
minerals in end stage renal disease. Clin Chim Acta.
577:1204852025. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Butler AM, Olshan AF, Kshirsagar AV,
Edwards JK, Nielsen ME, Wheeler SB and Brookhart MA: Cancer
incidence among US Medicare ESRD patients receiving hemodialysis,
1996–2009. Am J Kidney Dis. 65:763–772. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Khan S, Araji G, Yetiskul E, Keesari PR,
Haddadin F, Khamis Z, Chowdhry V, Niazi M, Afif S, Dhar M and
El-Sayegh S: Systemic oncological therapy in breast cancer patients
on dialysis. World J Clin Oncol. 15:730–744. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hu M, Wang Q, Liu B, Ma Q, Zhang T, Huang
T, Lv Z and Wang R: Chronic kidney disease and cancer:
Inter-relationships and mechanisms. Front Cell Dev Biol.
10:8687152022. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Iff S, Craig JC, Turner R, Chapman JR,
Wang JJ, Mitchell P and Wong G: Reduced estimated GFR and cancer
mortality. Am J Kidney Dis. 63:23–30. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Pedrazzoli P, Silvestris N, Santoro A,
Secondino S, Brunetti O, Longo V, Mancini E, Mariucci S, Rampino T,
Delfanti S, et al: Management of patients with end-stage renal
disease undergoing chemotherapy: Recommendations of the
associazione Italiana di Oncologia Medica (AIOM) and the Societa
Italiana di Nefrologia (SIN). ESMO Open. 2:e0001672017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Egorin MJ, Van Echo DA, Tipping SJ, Olman
EA, Whitacre MY, Thompson BW and Aisner J: Pharmacokinetics and
dosage reduction of
cis-diammine(1,1-cyclobutanedicarboxylato)platinum in patients with
impaired renal function. Cancer Res. 44:5432–5438. 1984.PubMed/NCBI
|
|
23
|
Tian H and Cronstein BN: Understanding the
mechanisms of action of methotrexate: Implications for the
treatment of rheumatoid arthritis. Bull NYU Hosp Jt Dis.
65:168–173. 2007.PubMed/NCBI
|
|
24
|
Temel JS, Greer JA, Muzikansky A,
Gallagher ER, Admane S, Jackson VA, Dahlin CM, Blinderman CD,
Jacobsen J, Pirl WF, et al: Early palliative care for patients with
metastatic non-small-cell lung cancer. N Engl J Med. 363:733–742.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Greer JA, Jackson VA, Meier DE and Temel
JS: Early integration of palliative care services with standard
oncology care for patients with advanced cancer. CA Cancer J Clin.
63:349–363. 2013.PubMed/NCBI
|
|
26
|
Yip CH: Palliation and breast cancer. J
Surg Oncol. 115:538–543. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Headon H, Wazir U, Kasem A and Mokbel K:
Surgical treatment of the primary tumour improves the overall
survival in patients with metastatic breast cancer: A systematic
review and meta-analysis. Mol Clin Oncol. 4:863–867. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Somsekhar SP, Geeta K, Jain R, Nayyer R,
Halder S, Malik VK, Parikh P, Aggarwal S and Koul R: Practical
consensus recommendations regarding role of mastectomy in
metastatic breast cancer. South Asian J Cancer. 7:79–82. 2018.
View Article : Google Scholar : PubMed/NCBI
|