Introduction
Malignant melanoma arises from melanocytes derived
from multipotent neural crest cells (1). These cells are located in the skin,
mucosal membranes, eyes, and neural crest migration sites such as
the gastrointestinal tract and brain (1). The metastatic potential of melanoma is
wide, with abdominal involvement reported in ~60% of cases
(2,3). The biliary tract is rarely involved,
with metastasis reported in 15% of gallbladder cases and ~6% of the
remaining biliary tree (3,4). Within the biliary tract, the cystic
duct and gallbladder are rare metastatic sites, while primary CBD
involvement is even less frequent and only sparsely documented
(4–6). Primary CBD melanoma is exceptionally
rare, and its histopathological definition remains debated, with
only 13 cases previously reported (6–9).
Prognosis is poor: primary biliary melanoma of the gallbladder has
a median survival of 21 months, whereas metastatic melanoma of the
gallbladder has a median survival of 8.4 months (6).
Case report
In late October 2024, a 44-year-old male with no
significant past medical history and an Eastern Cooperative
Oncology Group (ECOG) performance status of 0 presented to King's
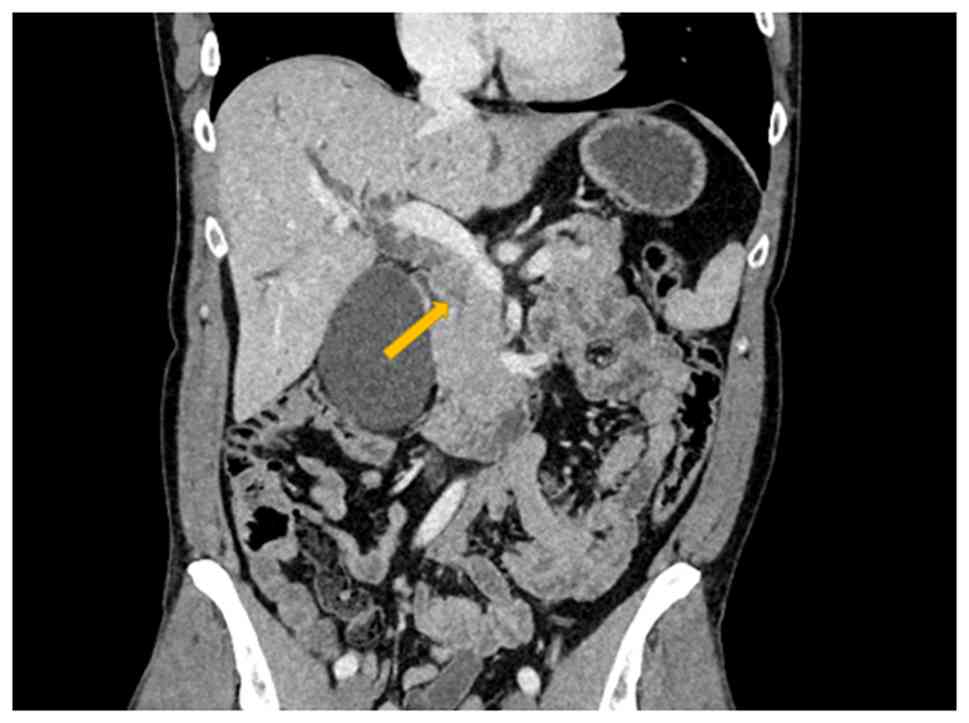
College Hospital with obstructive jaundice. Computed tomography
(CT) revealed a 3.5-cm soft tissue mass within the mid common bile
duct (CBD), causing upstream biliary dilatation (Figs. 1 and 2). Liver function tests demonstrated
cholestatic derangement, with total bilirubin 153 µmol/l, alanine
transferase 638 IU/l, alkaline phosphatase (ALP) 721 IU/l, and
gamma-glutamyl transferase (GGT) 832 IU/l. Endoscopic retrograde
cholangiopancreatography (ERCP) demonstrated an intraductal mass
extending 2 cm into the lower common hepatic duct and involving the
cystic duct orifice. A sphincterotomy with plastic biliary stent
placement relieved obstruction, resulting in bilirubin
normalization to 20 µmol/l within one week. Brush cytology obtained
during ERCP was non-diagnostic.
Staging investigations did not reveal any evidence
of metastatic disease, thus the patient was counselled for
pancreaticoduodenectomy, with intraoperative frozen section of the
upper bile duct margin planned to determine the need for additional
hepatic resection if positive for malignancy.
At laparotomy, frozen section analysis of the upper
CBD margin was negative for malignancy. As the lower CBD was
involved by tumour, a pylorus-preserving pancreaticoduodenectomy
was performed. The pancreas was soft with a non-dilated duct, and a
modified invagination technique was used for the
pancreatico-jejunostomy. The patient's initial recovery was
uneventful, and he was discharged on postoperative day 8 with no
evidence of pancreatic fistula. One week later, however, he was
readmitted with abdominal bleeding secondary to a gastroduodenal
artery pseudoaneurysm. This was successfully managed with
embolization and hepatic artery stent placement under angiographic
guidance, after which he made a full recovery.
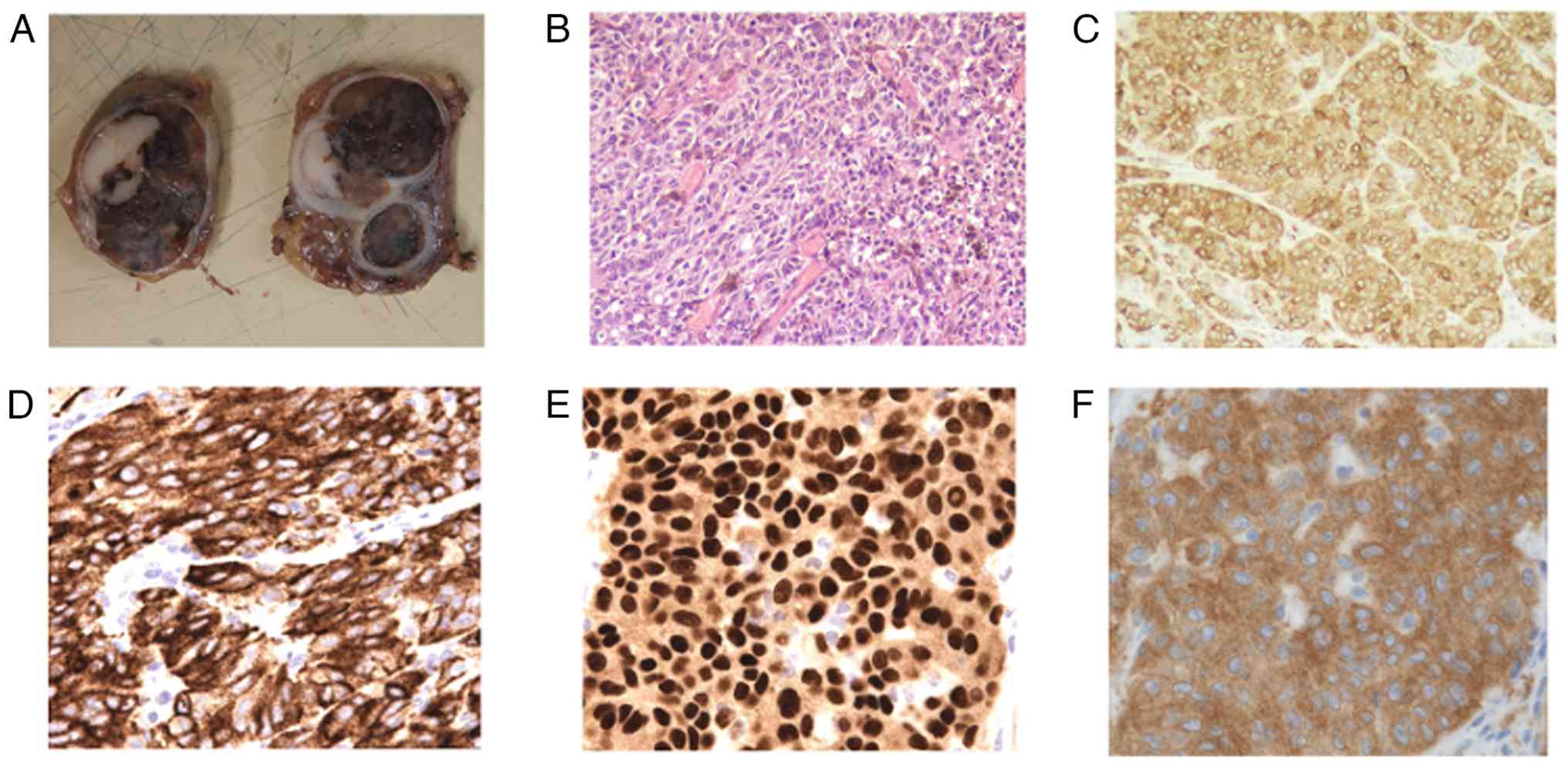
Histopathological examination revealed the CBD
lesion to be malignant melanoma. Gross examination of the specimen
demonstrated an intraductal polypoid tumour almost completely
obliterating the mid CBD and cystic duct, with a dark brown to
black solid cut surface containing whitish areas (Fig. 3A). Microscopically, the tumour was
composed of epithelioid malignant cells arranged in solid nests and
trabeculae, with moderately pleomorphic nuclei and lightly
pigmented cytoplasm. Mitotic figures were scattered, and melanin
pigment was observed within neoplastic cells and infiltrating
macrophages. The stroma was moderately infiltrated by lymphocytes
(Fig. 3B). Immunohistochemistry
demonstrated diffuse positivity for melanocytic markers (HMB-45,
Melan-A, SOX10) and BRAF V600E, while epithelial markers (AE1/AE3,
MNF116, CK7) were negative (Fig.
3C-F). The tumour was predominantly intraductal with only focal
invasion of the superficial duct wall. A definitive junctional
component at the mucosal-submucosal interface was not identified.
S-100 immunohistochemistry was not performed, as the diagnosis was
supported by diffuse positivity for specific melanocytic markers
including HMB-45, Melan-A, and SOX10. All resection margins and
regional lymph nodes were free of tumour.
The patient reported a history of nevus excision six
years prior, histologically confirmed as a dysplastic nevus without
features of melanoma; this lesion was re-examined and again
confirmed to be benign. A family history revealed melanoma in a
second-degree relative (a cousin), with no additional family
history of melanoma or other malignancies. Comprehensive
dermatological assessment and full-body skin mapping did not
identify any suspicious cutaneous, mucosal, or ocular lesions.
Following multidisciplinary discussion, the patient
commenced adjuvant immunotherapy with nivolumab at a standard dose
of 480 mg administered intravenously every 4 weeks, for a planned
duration of 12 months. This approach was considered appropriate in
the context of a BRAF V600E-mutant melanoma, with scheduled
interval imaging for surveillance. At the time of last follow-up,
the patient remains disease-free 12 months after surgery.
Discussion
Painless obstructive jaundice is the most common
presentation of pancreatobiliary malignancy. Cholangiocarcinoma
typically affects patients in the sixth decade of life, and cases
occurring under the age of 50 remain understudied (10). Distal cholangiocarcinoma accounts
for 20–30% of all cases (11).
Malignant melanoma has the potential to metastasize
to virtually any organ (12).
Abdominal involvement is reported in up to 60% of cases with
metastatic melanoma (1). The
biliary tract is affected in 4–20% of cases, most frequently at the
level of the gallbladder (9,13).
Cetiner et al (12) reported
fewer than 20 cases of metastatic melanoma involving the common
bile duct (CBD), and to date, no systematic review has been
performed.
The clinical spectrum of metastatic disease varies
from widespread dissemination with poor prognosis and no curative
options (13) to isolated lesions
amenable to surgical resection, such as gallbladder metastasis,
where cholecystectomy may provide limited disease-free survival
(13). Historically, the prognosis
of metastatic melanoma was dismal, with 2-year survival rates
<2% reported three decades ago (14). However, more recent series
demonstrate that resection of isolated intra-abdominal metastatic
deposits can yield 5-year survival rates of 12–25% in selected
cases (14–16). Complete resection appears to be
critical for long-term survival. Wood et al (17) reported a 24% 5-year survival among
patients undergoing resection of solid organ metastases
(adrenalectomy, splenectomy, hepatectomy, pancreatectomy), whereas
no long-term survivors were observed following incomplete
resection.
Primary melanoma of the CBD is exceedingly rare, and
its pathological diagnosis remains controversial due to the absence
of specific immunohistochemical features (13). Ricci et al (18) proposed diagnostic criteria for
primary gallbladder melanoma, which have also been applied to CBD
melanoma: absence of prior melanoma, exclusion of other primary
sites, solitary polypoid lesion, and presence of a junctional
component. Wagner et al (19) subsequently emphasized the
histological finding of junctional melanocytes at the
mucosal-submucosal interface, confirmed by S-100 immunoreactivity,
as the strongest criterion for primary CBD melanoma. However, this
feature has not been consistently reported by other authors
(6–8).
In the present case, the diagnostic criteria
proposed by Ricci et al (18) are largely fulfilled, including the
absence of a prior melanoma, exclusion of alternative primary sites
after comprehensive dermatological and systemic assessment, and the
presence of a solitary intraductal polypoid lesion. Although a
definitive junctional component, as emphasised by Wagner et
al (19), was not identified,
this feature has not been consistently demonstrated in previously
reported cases of primary CBD melanoma. Given the predominantly
intraductal growth pattern with only focal superficial invasion and
the absence of metastatic disease, a primary biliary origin remains
the most plausible diagnosis.
Moreover, although S-100 immunoreactivity and a
junctional component have been proposed as diagnostic criteria,
these features are not consistently reported in published cases of
primary CBD melanoma, and their absence does not preclude the
diagnosis when supported by morphology, specific melanocytic
markers, and exclusion of alternative primary sites.
To date, only 13 cases of primary CBD melanoma have
been described (6–9), with most diagnoses based on exclusion
after extensive negative systemic work-up. In both primary and
metastatic cases, upfront surgical resection remains the mainstay
of treatment (6,17).
Applying the criteria from previous reports, the
present case represents the 14th description of primary malignant
melanoma of the CBD. While histological confirmation remains
debated, the absence of cutaneous, mucosal, or ocular melanoma and
the solitary intraductal lesion strongly support this
diagnosis.
The identification of a BRAF V600E mutation in the
present case is clinically significant and has important
therapeutic implications. BRAF mutations are present in
approximately 40–50% of cutaneous melanomas and have been
associated with responsiveness to targeted therapy using BRAF
inhibitors (20,21). Although data on molecular profiling
in primary biliary melanoma are extremely limited, the presence of
a BRAF V600E mutation provides a rationale for considering targeted
therapy in the event of disease recurrence or metastatic
progression. This molecular finding further distinguishes the
present case from many previously reported cases and highlights the
importance of comprehensive immunohistochemical and molecular
assessment in rare melanocytic tumours of the biliary tract
(20,21).
Although the prognosis of both primary and
metastatic biliary melanoma has historically been poor, the present
case may represent a more favourable biological and clinical
scenario. Young age at presentation, complete (R0) surgical
resection, and access to contemporary adjuvant immunotherapy are
factors that have been associated with improved outcomes in
melanoma more broadly. Nevertheless, given the rarity of primary
CBD melanoma and the relatively short duration of follow-up in this
case, which represents a limitation of this report, any prognostic
inference must be made with caution, and longer-term surveillance
remains essential to better define oncological outcomes.
This case underscores the importance of careful
evaluation of patient demographics and history, particularly in
younger individuals presenting with obstructive jaundice. Although
preoperative differentiation from cholangiocarcinoma is difficult,
clinicians must be aware of this rare entity. A diagnosis of
melanoma after curative-intent pancreaticoduodenectomy represents a
major shift in prognosis and postoperative management, with
implications for patients, families, and the multidisciplinary
team.
In conclusion, metastatic involvement of the biliary
tree occurs in 4–20% of cases of metastatic melanoma. Primary CBD
melanoma is exceedingly rare, with only 13 cases previously
described. Both entities are associated with poor prognosis, with
5-year survival not exceeding 25% even in resected cases.
Nevertheless, complete resection remains the standard of care,
offering the best chance for long-term survival.
A comprehensive evaluation of patient history, prior
skin lesions, and family history is essential when assessing
younger patients with obstructive jaundice. While rare, the
possibility of primary or metastatic melanoma should be considered,
as unexpected histological findings following major
hepatopancreatobiliary surgery can profoundly alter the oncological
pathway.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
EF conceived and designed the study, collected
clinical data, performed analysis, and drafted the manuscript. HA
contributed to data collection and clinical management. YZ
performed histopathological analysis and interpretation. PS and AP
contributed substantially to surgical decision-making and operative
management, provided critical clinical input during case review,
and contributed to data interpretation. All authors contributed to
drafting and revising the manuscript. EF, YZ and PS confirmed the
authenticity of all raw data. All authors agree to be accountable
for all aspects of the work. All authors have read and approved the
final version of the manuscript.
Ethics approval and consent to
participate
This case report was conducted in accordance with
institutional requirements. The requirement for ethical approval
was waived, as this is a single case report not requiring formal
review.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of this report and accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Castro-Pérez E, Singh M, Sadangi S,
Mela-Sánchez C and Setaluri V: Connecting the dots: Melanoma cell
of origin, tumour cell plasticity, trans-differentiation, and drug
resistance. Pigment Cell Melanoma Res. 36:330–347. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Dasgupta T and Brasfield R: Metastatic
melanoma: A clinicopathological study. Cancer. 17:1323–1339. 1964.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Verbanck JJ, Rutgeerts LJ, van Aelst FJ,
Tytgat JH, Decoster JM, Noyez DN, Theunynck PJ and Geboes KJ:
Primary malignant melanoma of the gallbladder, metastatic to the
common bile duct. Gastroenterology. 91:214–218. 1986. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Garas G, Bramston B and Edmunds SE:
Malignant melanoma metastatic to the common bile duct. J
Gastroenterol Hepatol. 15:1348–1351. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Dasgupta TK and Brasfield RD: Metastatic
melanoma of the gastrointestinal tract. Arch Surg. 88:969–973.
1964. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Smith NE, Taube JM, Warczynski TM, Collier
KD and Pawlik TM: Primary biliary tract melanoma: Report of a case
and review of the literature. Int J Surg Case Rep. 3:441–444. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wang X, Deng X, Shu Z and Wu J: Diagnosis
of primary biliary melanoma with distinct imaging features: A case
report and literature review. J Int Med Res.
51:30006052311640052023. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Addepally NS, Klair JS, Lai K, Aduli F and
Girotra M: Primary bile duct melanoma causing obstructive jaundice.
ACG Case Rep J. 3:e1282016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cameselle-García S, Pérez JLF, Areses MC,
de Castro JDF, Mosquera-Reboredo J and García-Mata J: Primary
malignant melanoma of the biliary tract: A case report and
literature review. World J Clin Cases. 7:2302–2308. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Reddy S, Goksu SY, Sanford NN, Kainthla R,
Hsiehchen D, Sanjeevaiah A, Jones AL, Karagkounis G, Al Mutar S,
Ahn C, et al: Characteristics and clinical outcomes in young-onset
cholangiocarcinoma. Cancer Med. 12:14094–14103. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Banales JM, Marin JJG, Lamarca A,
Rodrigues PM, Khan SA, Roberts LR, Cardinale V, Carpino G, Andersen
JB, Braconi C, et al: Cholangiocarcinoma 2020: The next horizon in
mechanisms and management. Nat Rev Gastroenterol Hepatol.
17:557–588. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Cetiner OF, Dundar HE, Kantarcioglu-Coskun
S, Torun S and Tokmak S: Metastatic melanoma of the common bile
duct presented with dyspepsia. Korean J Gastroenterol. 83:163–166.
2024. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Giannini I, Cutrignelli DA, Resta L,
Gentile A and Vincenti L: Metastatic melanoma of the gallbladder:
Report of two cases and a review of the literature. Clin Exp Med.
16:295–300. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Morton DL, Essner R and Balch C: Surgical
excision of distant metastases. Cutaneous melanoma. 4th edition.
Balch C, Houghton A, Sober A, et al: Quality Medical Publishing;
St. Louis, MO, USA: pp. 547–572. 2003
|
|
15
|
Tung CC, Chang MC and Chang YT: An unusual
case of obstructive jaundice. Diagnosis: Metastatic melanoma.
Gastroenterology. 141:e12–e13. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wakasugi M, Tori M, Akamatsu H, Yoshidome
K, Ueshima S, Omori T, Tei M, Masuzawa T, Iwamoto T and Nishida T:
Pancreatoduodenectomy for melanoma with metastasis to the common
bile duct. Surg Today. 42:1119–1124. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wood TF, DiFronzo LA, Rose DM, Haigh PI,
Stern SL, Wanek L, Essner R and Morton DL: Does complete resection
of melanoma metastatic to solid intra-abdominal organs improve
survival? Ann Surg Oncol. 8:658–662. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ricci R, Maggiano N, Martini M, Mulé AM,
Pierconti F, Capelli A and Larocca LM: Primary malignant melanoma
of the gallbladder in dysplastic naevus syndrome. Virchows Arch.
438:159–165. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wagner MS, Shoup M, Pickleman J and Yong
S: Primary malignant melanoma of the common bile duct: A case
report and review of the literature. Arch Pathol Lab Med.
124:419–422. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Chapman PB, Hauschild A, Robert C, Haanen
JB, Ascierto P, Larkin J, Dummer R, Garbe C, Testori A, Maio M, et
al: Improved survival with vemurafenib in melanoma with BRAF V600E
mutation. N Engl J Med. 364:2507–2516. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Robert C, Karaszewska B, Schachter J,
Rutkowski P, Mackiewicz A, Stroiakovski D, Lichinitser M, Dummer R,
Grange F, Mortier L, et al: Improved overall survival in melanoma
with combined dabrafenib and trametinib. N Engl J Med. 372:30–39.
2015. View Article : Google Scholar : PubMed/NCBI
|