Introduction
Pancreatic cancer is an aggressive malignancy with a
poor prognosis (1,2). Approximately 80–85% of newly diagnosed
patients present with either unresectable or metastatic disease,
depriving them of the only potentially curative option-upfront
surgical resection (1–3). Liver metastases are present in nearly
50% of cases and are associated with dismal outcomes, often
measured in weeks to a few months (1). As a result, metastatic pancreatic
cancer is generally considered untreatable.
Palliative chemotherapy provides modest survival
benefit, with overall survival ranging from 8.5 to 10 months
depending on the regimen used (1,2). The
longest survival is observed with the FOLFIRINOX regimen
(fluorouracil, folinic acid, irinotecan, and oxaliplatin) (1,2). In
cases of locally advanced pancreatic cancer, FOLFIRINOX is employed
with the aim of conversion to resectability, which has been
achieved in up to 25.9% of patients (4).
However, in the metastatic setting, particularly
with widespread liver involvement, conversion to surgery is not
considered feasible, and no established treatment pathway exists.
Rare cases demonstrating exceptional response to systemic therapy,
such as the one presented here, remain anecdotal but raise
important questions about tumour biology, treatment sequencing, and
the future of personalized oncology in this disease.
Case report
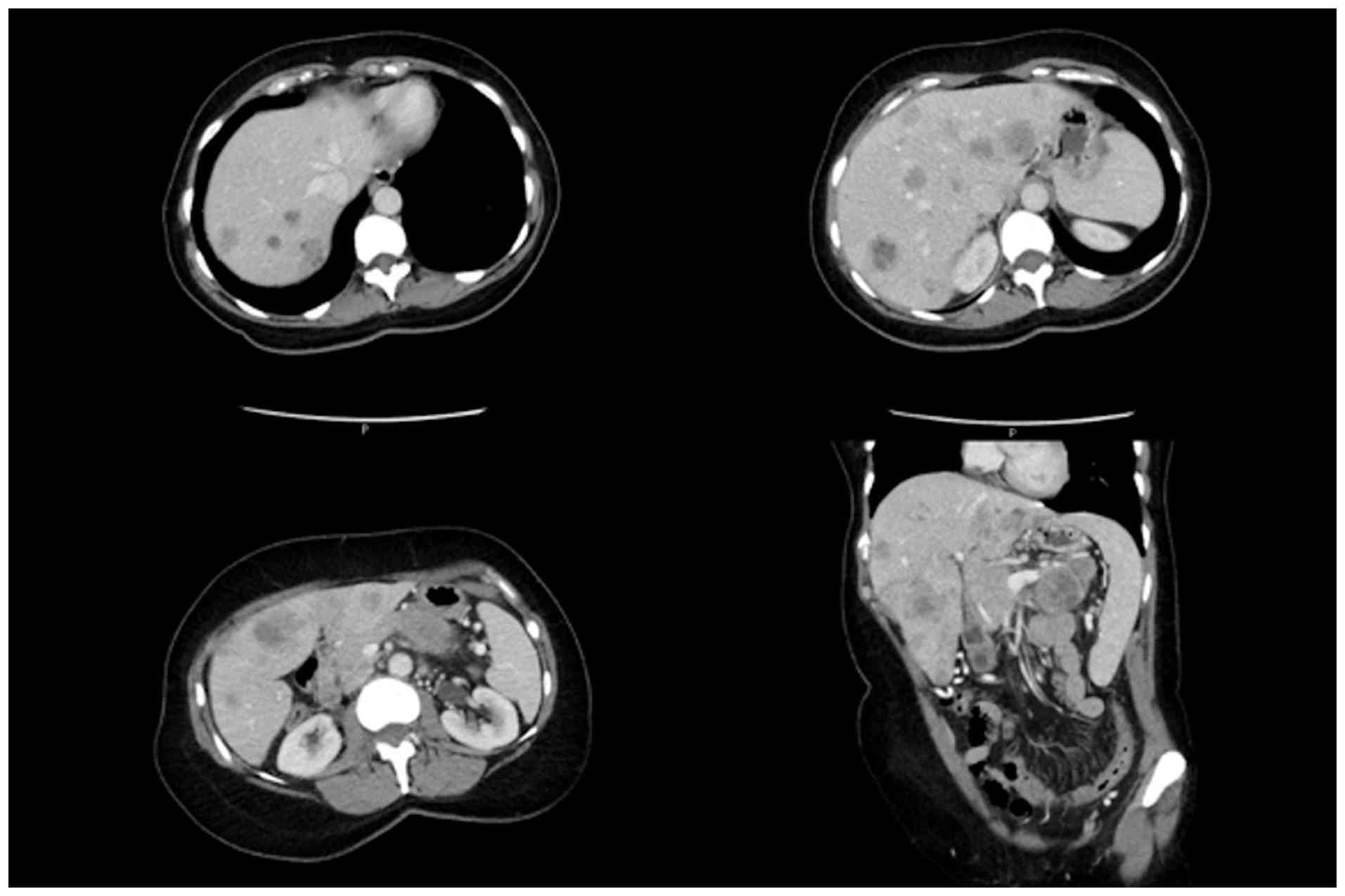
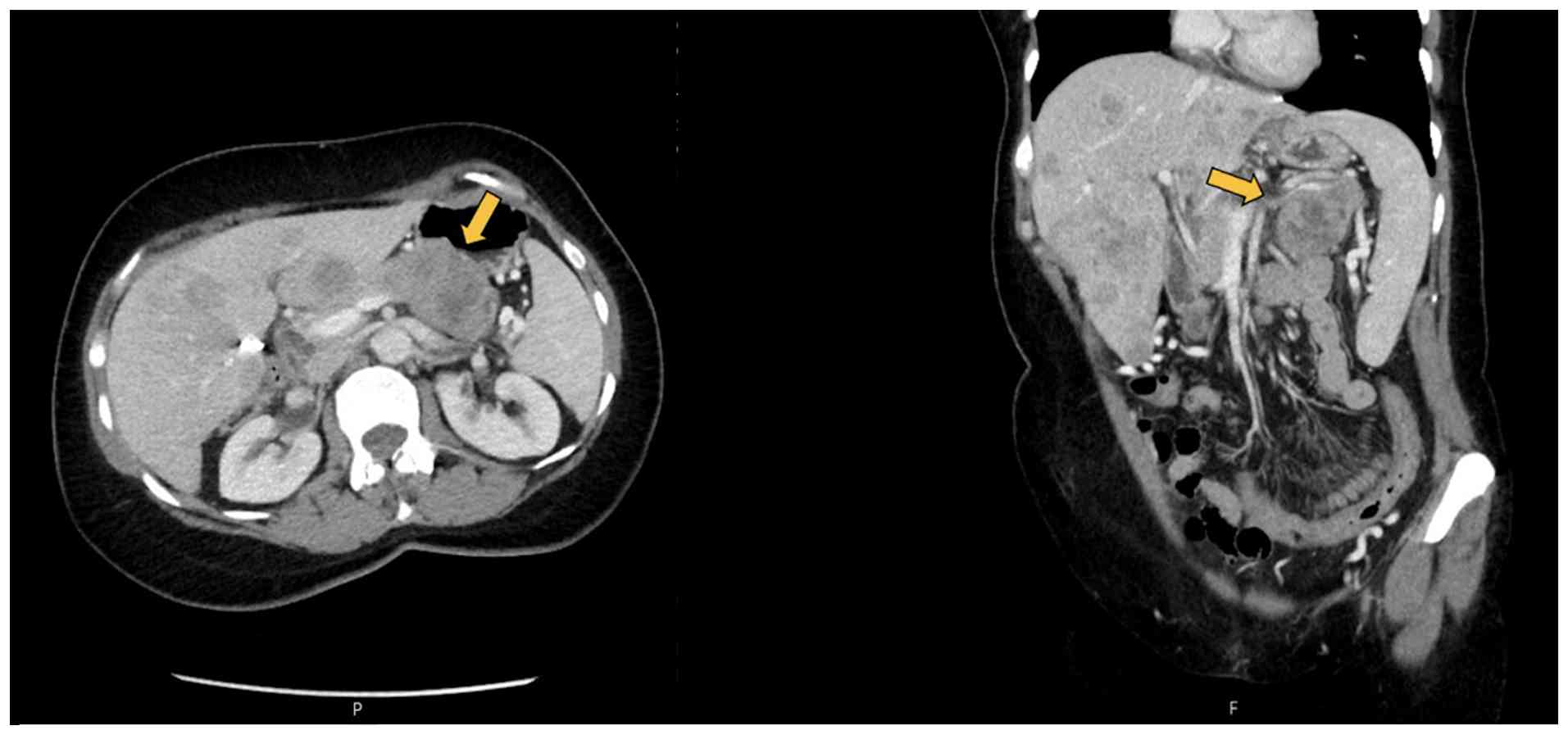
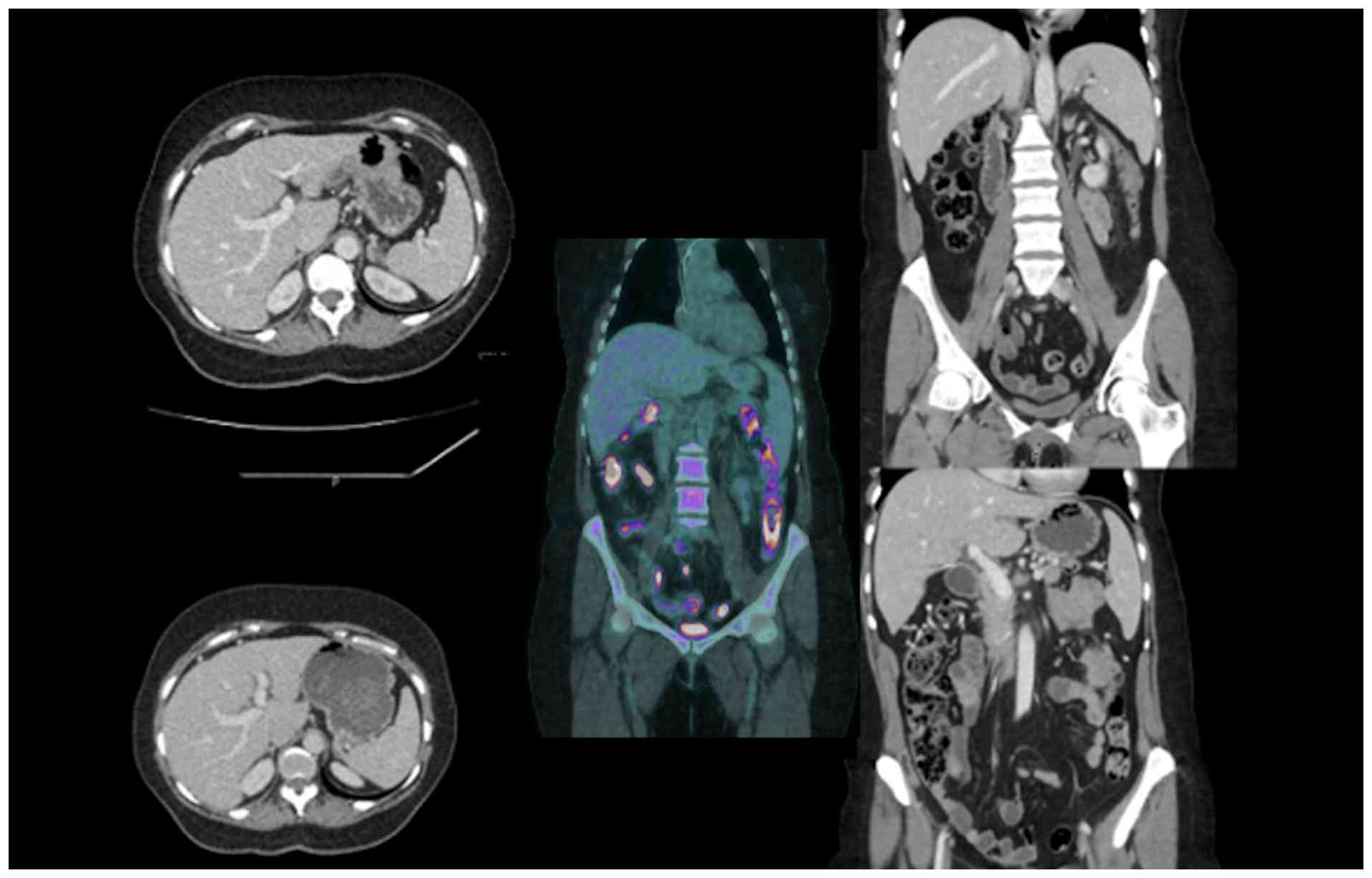
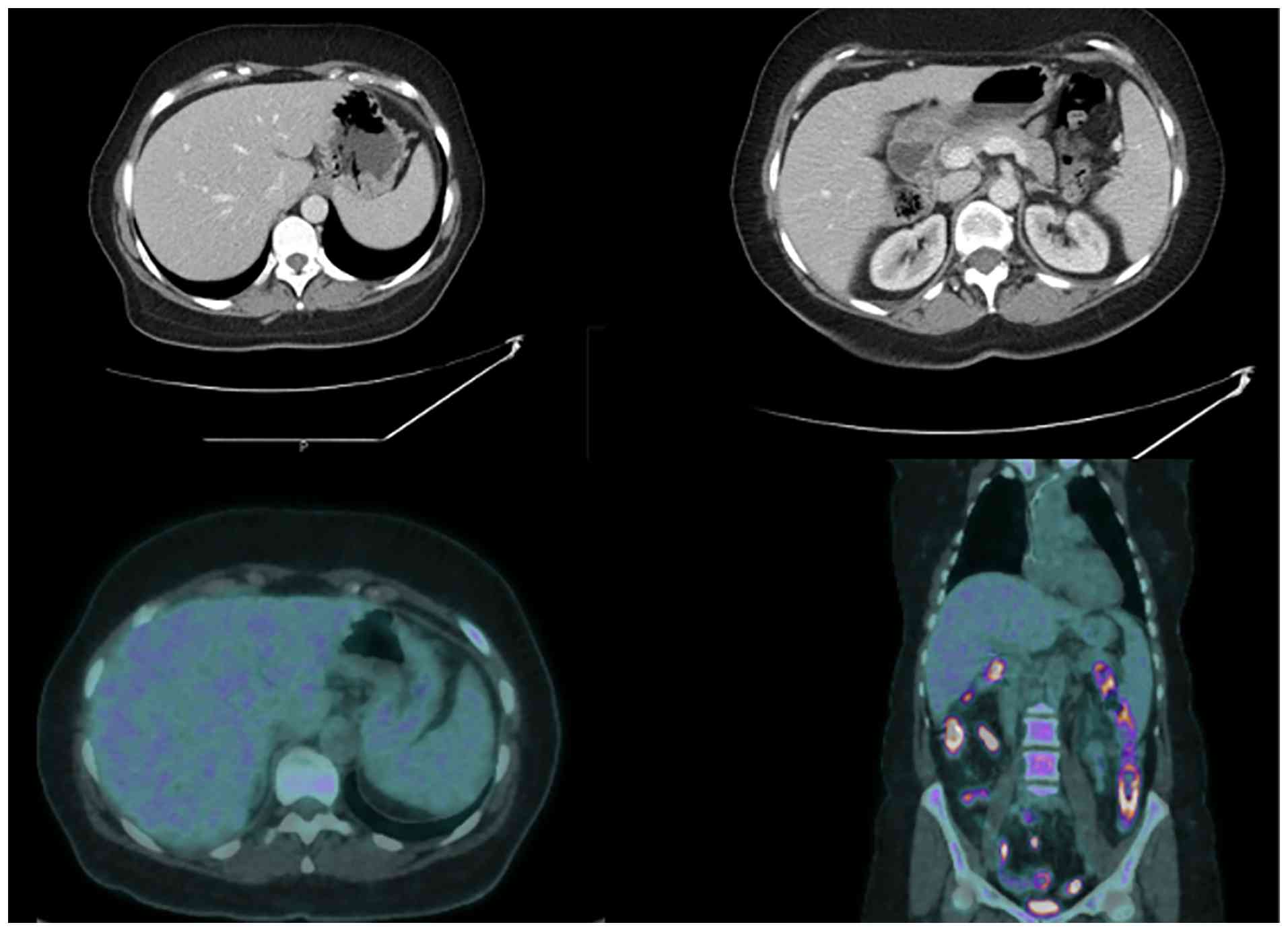
In September 2018, a 60-year-old female was
diagnosed with a poorly differentiated pancreatic body tumour and
multiple liver metastases (Figs. 1
and 2). The patient initially
presented at Derby Teaching Hospitals in United Kingdom and was
referred to King's College Hospital, London, for tertiary
Hepato-Pancreato-Biliary evaluation at a later stage.
The diagnosis was confirmed by endoscopic
ultrasound-guided biopsy of the pancreatic mass. FOLFIRINOX
chemotherapy was initiated in October 2018 with palliative intent.
Given the radiological appearances strongly suggestive of liver
metastases, no histological confirmation of the liver lesions was
pursued, reflecting common clinical practice in the absence of
features suggestive of sepsis or diagnostic doubt.
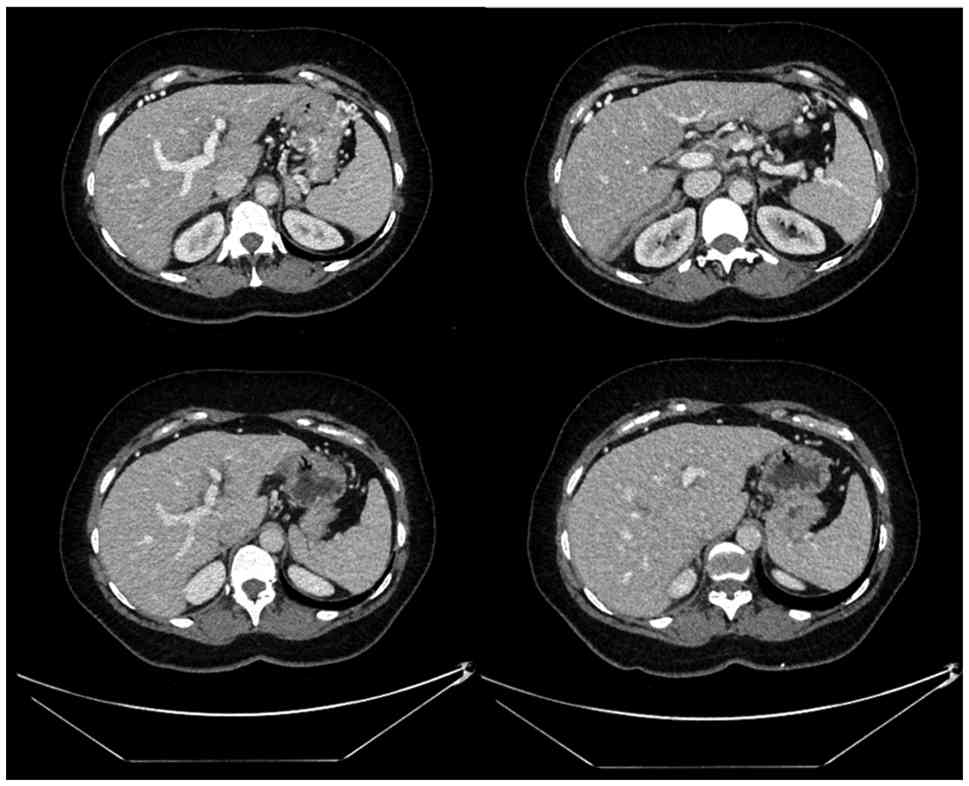
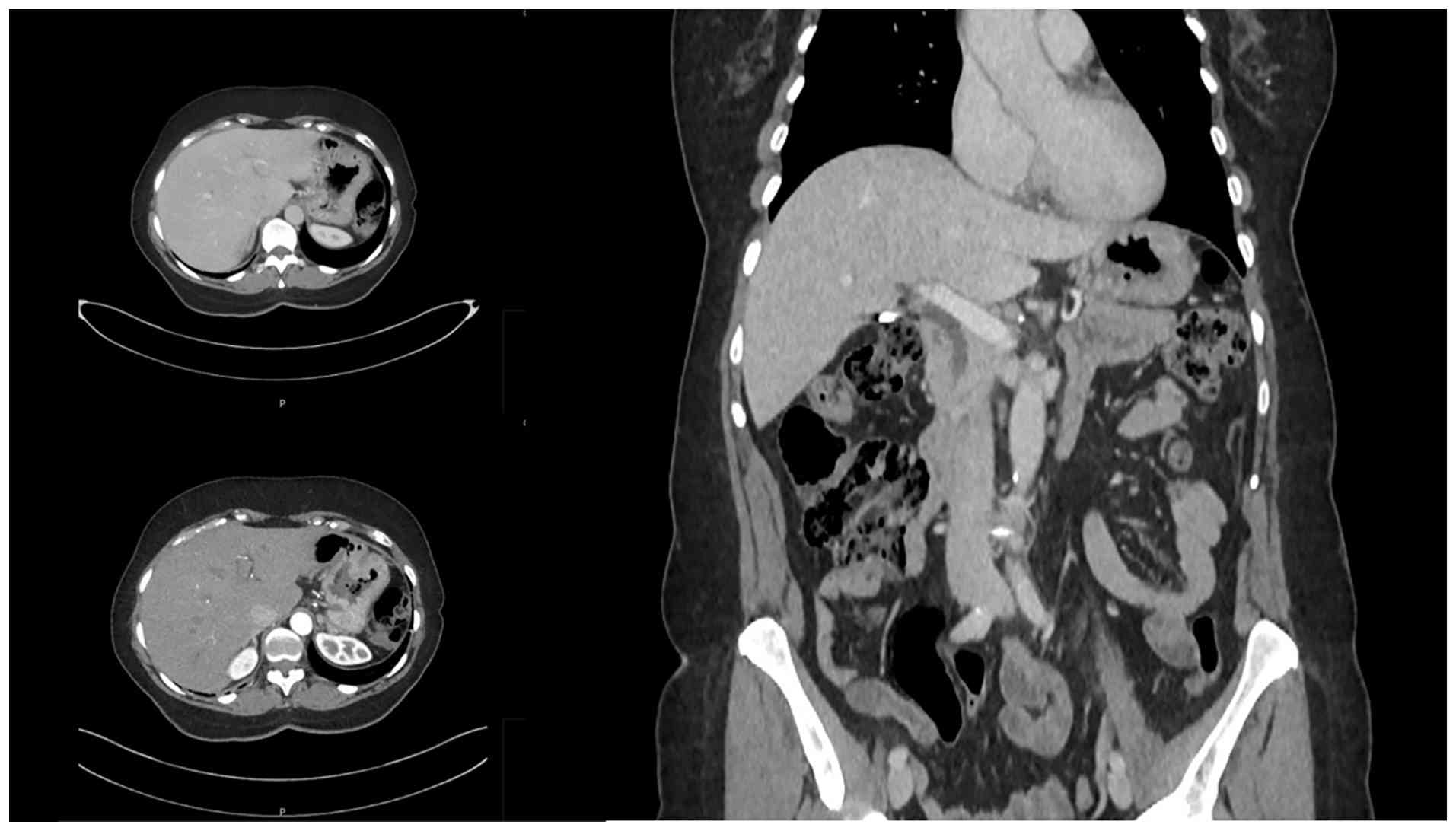
After 6 months of chemotherapy, in April 2019,
imaging revealed significant response at both the primary site and
within the liver, where lesions were now barely detectable
(Fig. 3).
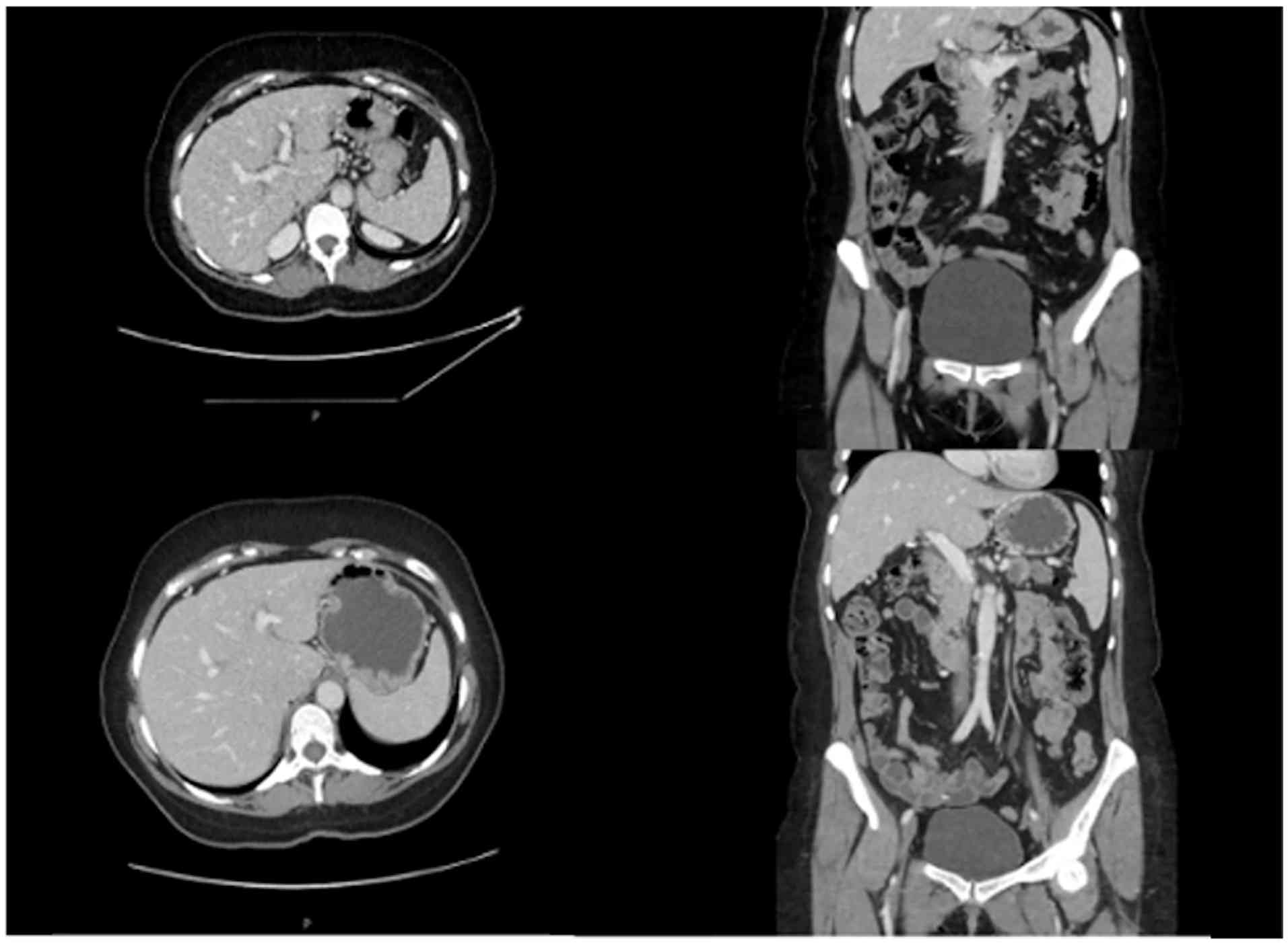
This finding persisted on serial imaging throughout
continued systemic therapy and surveillance for more than two
years. Subsequent FDG-PET imaging demonstrated no abnormal hepatic
metabolic activity (Figs. 4,
5 and 6). At surgical exploration, no macroscopic
liver lesions were identified, and therefore no intraoperative
biopsies were performed.
By August 2019, following a total of 19 cycles of
FOLFIRINOX, repeat imaging demonstrated near-complete resolution of
both the pancreatic mass and hepatic metastases. The patient was
subsequently enrolled in a clinical trial investigating a cancer
vaccine and received two doses, administered four weeks apart. At
her request, chemotherapy was paused.
The case was referred to the
Hepato-Pancreato-Biliary (HPB) multidisciplinary team (MDT) at our
tertiary centre for assessment of surgical resectability. Upon
reviewing the initial and subsequent imaging, the MDT acknowledged
the extraordinary radiological response. However, surgery was
deemed inappropriate at that time due to the initial burden of
hepatic metastatic disease. Surveillance under local oncology
follow-up was recommended.
After a 15-month chemotherapy-free interval,
restaging scans demonstrated sustained disease stability, leading
to resumption of FOLFIRINOX in December 2020. The patient
subsequently completed 12 additional cycles, with the final 4
cycles administered at a reduced dose (60%).
In June 2021, both CT and FDG-PET imaging confirmed
complete radiological and metabolic response at both the primary
and metastatic sites (Fig. 7).
Following MDT discussion and given the sustained disease stability,
the patient was deemed suitable for surgical exploration.
In August 2021, she underwent laparotomy. No
macroscopic evidence of metastatic liver disease was identified
intraoperatively. A left pancreatectomy with splenectomy was
performed.
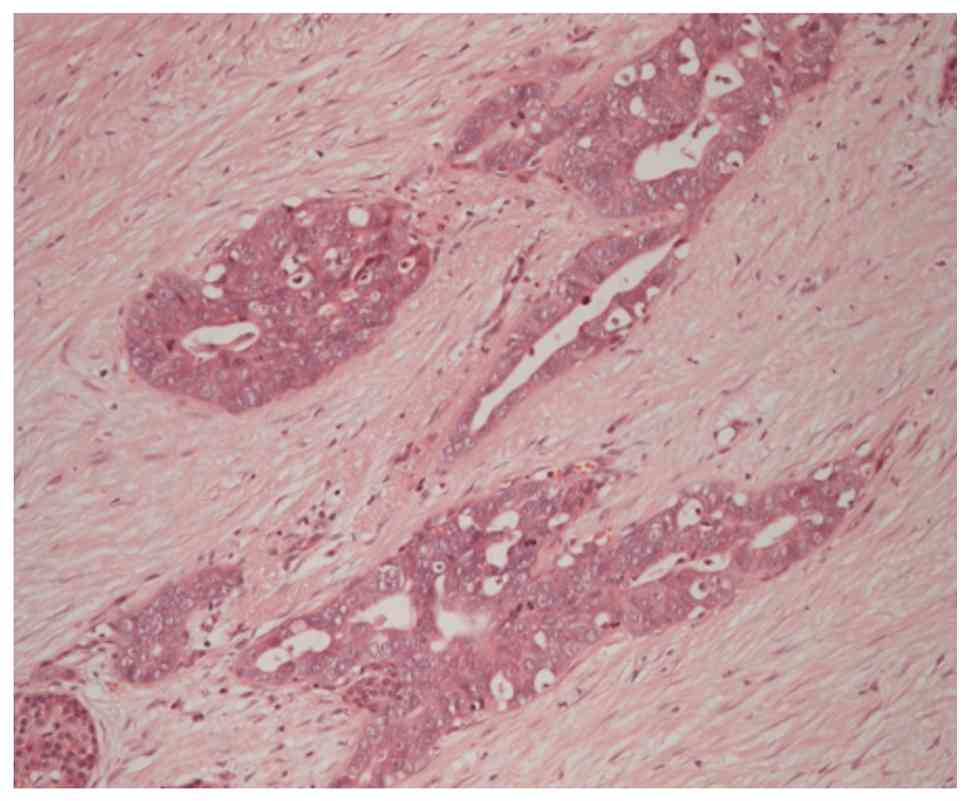
Final histopathology revealed a 20 mm pancreatic
ductal adenocarcinoma arising in a 50 mm high-grade intraductal
papillary mucinous neoplasm (IPMN) of pancreatobiliary subtype.
There was infiltration of the splenic vein, and 1 of 9 resected
peripancreatic lymph nodes contained metastatic disease. The
pancreatic duct showed low-grade dysplasia at the margin, but there
was no high-grade dysplasia or invasive cancer. Resection margins
were negative. Final staging was ypT2 pN1 (1/9) LV1 PN0 R0.
Representative haematoxylin and eosin-stained sections are shown in
Fig. 8, demonstrating viable
residual pancreatic ductal adenocarcinoma following systemic
chemotherapy.
The postoperative course was uneventful.
The patient was monitored with 6-monthly interval CT
scans. She did not receive further adjuvant chemotherapy. As of the
most recent follow-up, she remains alive and disease-free 84 months
(7 years) after her initial diagnosis and 4 years post-resection
(Fig. 9). A timeline summarising
the disease course is presented in Table I.
 | Table I.Timeline of disease course. |
Table I.
Timeline of disease course.
| Date | Clinical event |
|---|
| September 2018 | Diagnosis of poorly
differentiated pancreatic adenocarcinoma with liver metastases at
Derby |
| Teaching | Hospitals NHS
Foundation Trust. |
| October 2018 | Initiation of
palliative FOLFIRINOX chemotherapy. |
| April 2019 | Following 6 cycles,
CT demonstrated significant regression of liver metastases. |
| August 2019 | Completion of 19
cycles of FOLFIRINOX. Enrolment in the ACIT-1 vaccine trial and
administration of two doses four weeks apart. |
| September 2019 | CT imaging
demonstrated sustained response at the primary site; liver
metastases no longer visible. |
| February 2020 | Referral to King's
College Hospital Hepato-Pancreato-Biliary multidisciplinary team;
decision for ongoing surveillance. Patient requested a chemotherapy
break. |
| September
2019-December 2020 | Chemotherapy-free
interval of 15 months. |
| November 2020 | Radiological
progression at the primary site; FOLFIRINOX treatment resumed with
dose reduction to 60% for the final four cycles (total 12
cycles). |
| June 2021 | CT and FDG PET show
complete radiological and metabolic response. Reviewed by the
Hepato-Pancreato-Biliary multidisciplinary team; resection of the
primary tumor offered to patient. |
| August 2021 | Patient underwent
left pancreatectomy and splenectomy. Histology confirmed invasive
adenocarcinoma with high-grade intraductal papillary mucinous
neoplasm (with final staging of ypT2N1PN0 LV1R0). |
| July 2025 | Patient remains free
of disease. |
Discussion
Pancreatic cancer was the fourth leading cause of
cancer-related deaths in the USA and Europe based on 2018 data and
is projected to become the leading cause by 2030 (4). Metastatic pancreatic cancer (mPC)
accounts for approximately 50% of cases at diagnosis, with a
reported 5-year survival rate of just 3% in this group (4).
Invasive pancreatic cancer arising from intraductal
papillary mucinous neoplasm (IPMN) has been shown to confer
improved overall survival in resected patients, with 5- and 10-year
survival rates of 72 and 62%, respectively (5). However, survival data specific to
metastatic IPMN-associated pancreatic cancer remain unavailable, as
these cases are typically grouped under the broader mPC category
(5).
Long-term survivors with mPC are exceedingly rare
and have been sparsely reported in the literature (6,7).
FOLFIRINOX was the chemotherapeutic regimen used in most reported
cases, although modifications, particularly reducing or omitting
oxaliplatin, were often necessary due to adverse effects (7,8). One
such survivor was BRCA1-positive with a history of multiple
malignancies (7). In a striking
case reported by Balta et al (6), multimodal treatment including
chemotherapy, radiotherapy, transhepatic arterial chemoembolization
(TACE), radiofrequency ablation (RFA) for a renal deposit,
pancreaticoduodenectomy, liver wedge resection, Cyber-Knife
radiosurgery, and repeated genomic analysis enabled nearly 5 years
of survival. This underscores how a tailored combination of
treatments can achieve prolonged survival and quality of life in a
disease typically considered rapidly fatal.
While palliative chemotherapy does not
conventionally aim for conversion, neoadjuvant therapy in
borderline resectable or locally advanced pancreatic cancer seeks
tumour downstaging to enable surgical resection. In this context,
the role of pathologic complete response (pCR) remains
controversial. pCR has been reported in approximately 4.8–10% of
resected pancreatic adenocarcinoma cases following neoadjuvant
chemotherapy (9–12), though its association with improved
disease-free survival is inconsistent (11,12).
In the present case, pCR was not achieved; however,
long-term disease-free survival was. This challenges the assumption
that pCR is either necessary or predictive of prolonged survival.
One report documented mPC with pCR and an additional six months of
survival post-resection, in a patient treated with adjuvant
monotherapy using the PARP inhibitor Olaparib (13). Similarly, mPC treated with
FOLFIRINOX achieving both pCR and 5-year survival has also been
described (8,14). Collectively, these cases suggest
that pCR is not essential to survival outcomes and that achieving
it should not be viewed as the primary goal.
The interpretation of an apparent complete hepatic
response in mPC warrants careful consideration. In the case
described here, while serial multiphasic contrast-enhanced CT and
FDG-PET imaging demonstrated sustained absence of radiologically
and metabolically detectable liver lesions in this case, current
imaging modalities have recognised limitations in reliably
excluding residual subcentimeter or microscopic disease,
particularly following prolonged systemic chemotherapy.
Treatment-related changes may render previously metastatic deposits
radiologically occult or metabolically inactive, leading to
underestimation of residual tumour burden. FDG-PET, although
valuable for functional assessment, lacks sufficient sensitivity to
definitively exclude microscopic viable disease, especially in the
post-treatment setting.
Intraoperative assessment in this case was limited
to systematic macroscopic inspection of the liver, and no
intraoperative ultrasound or targeted biopsies were performed, as
no suspicious lesions were identified on repeated imaging or at
surgical exploration. Consequently, histological confirmation of
complete metastatic clearance was not obtained, and the presence of
occult residual disease cannot be entirely excluded. This
represents an inherent limitation of the present study and reflects
broader challenges in defining true complete response in metastatic
pancreatic cancer.
In this context, the terms ‘vanishing liver
metastases’ and ‘complete radiological regression’ are used
descriptively to denote the durable absence of detectable hepatic
disease on serial cross-sectional and metabolic imaging, rather
than to imply histologically confirmed eradication. The prolonged
stability of this response over several years of follow-up,
together with favourable clinical outcome, underscores the
exceptional nature of this case while acknowledging the limitations
of current diagnostic techniques.
The present case represents a particularly
remarkable and, to our knowledge, previously undescribed clinical
phenomenon within mPC. While rare long-term survivors of mPC have
been reported, this case is distinguished by the early and complete
radiological disappearance of liver metastases after approximately
six months of systemic chemotherapy, followed by sustained absence
of detectable hepatic disease on serial cross-sectional and
metabolic imaging over a prolonged period. Notably, this durable
hepatic response persisted despite treatment interruptions and over
several years of follow-up, an observation that challenges
conventional expectations of metastatic pancreatic cancer biology.
Whether immune-mediated mechanisms, potentially augmented by
subsequent vaccine exposure, contributed to the long-term
maintenance of this response remains speculative but biologically
plausible.
The ACIT-1 trial is an early-phase clinical study
investigating the safety and immunogenicity of a novel allogeneic
cell-based cancer vaccine (ACIT-1) (15–17).
Designed to stimulate host immunity against tumour-associated
antigens, the trial included patients with late-stage solid
tumours, including pancreatic cancer, using a dose-escalation
strategy to balance immunologic response and toxicity (15–17).
While its clinical efficacy remains under
investigation, our patient received two doses during a
chemotherapy-free interval. Whether ACIT-1 contributed to disease
control or to the favourable response observed during subsequent
FOLFIRINOX administration is unclear. Importantly, the liver
metastases had already shown significant response early in the
first course of FOLFIRINOX. Robust conclusions on ACIT-1′s role
await further data, and, to date, no peer-reviewed clinical outcome
results have been published from this trial (NCT03096093) (16).
To our knowledge, this is the first reported case of
mPC with initially extensive liver metastases demonstrating
complete and sustained regression over the long term. This case is
not only remarkable due to the radiological disappearance of liver
disease but also because of the durable systemic response, raising
the possibility of true cure, an outcome almost unheard of in the
context of metastatic pancreatic cancer.
The convergence of favourable tumour biology,
multimodal treatment strategies, and evolving molecular profiling
to guide targeted therapies (e.g., immunotherapy, vaccines) may
hold the key to improved outcomes in select cases. A deeper
understanding of these components is critical to redefining the
therapeutic landscape of this formidable malignancy.
In conclusion, this case illustrates a unique
clinical course in which a patient with initially metastatic
pancreatic cancer achieved sustained remission and underwent
curative-intent resection following systemic chemotherapy. It
challenges the long-held belief that metastatic pancreatic cancer
is invariably terminal and highlights the importance of
individualized, biology-driven treatment pathways. Rare though they
may be, such cases underscore the need for continued exploration of
predictive biomarkers and tailored therapeutic strategies that may
convert inoperable disease into surgical candidates, ultimately
improving survival and quality of life.
Acknowledgements
The authors would like to thank Professor Yoh Zen
(Pathology Department, Institute of Liver Studies, King's College
Hospital, London, UK) for his expert histopathological input and
assistance with interpretation of the histological images included
in this report.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
EF conceived and designed the study, collected and
curated the clinical data, performed data analysis and
interpretation, and drafted the manuscript. PR contributed to data
interpretation and provided critical intellectual input during
manuscript revision, particularly with respect to oncological
management and systemic therapy. PS contributed to acquisition and
interpretation of surgical data and provided critical revision of
the manuscript for important intellectual content. AP contributed
to study conception, interpretation of surgical and
histopathological findings, and critical revision of the manuscript
for important intellectual content. All authors read and approved
the final manuscript and agree to be accountable for all aspects of
the work. EF and AP confirm the authenticity of all raw data.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of this report and accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Mizrahi JD, Surana R, Valle JW and Shroff
RT: Pancreatic cancer. Lancet. 395:2008–2020. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Frigerio I, Malleo G, de Pastena M, Deiro
G, Surci N, Scopelliti F, Esposito A, Regi P, Giardino A, Allegrini
V, et al: Prognostic factors after pancreatectomy for pancreatic
cancer initially metastatic to the liver. Ann Surg Oncol.
29:8503–8510. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Chan KKW, Guo H, Cheng S, Beca JM,
Redmond-Misner R, Isaranuwatchai W, Qiao L, Earle C, Berry SR,
Biagi JJ, et al: Real-world outcomes of FOLFIRINOX vs gemcitabine
and nab-paclitaxel in advanced pancreatic cancer: A
population-based propensity score-weighted analysis. Cancer Med.
9:160–169. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lee M, Kang JS, Kim H, Kwon W, Lee SH, Ryu
JK, Kim YT, Oh DY, Chie EK and Jang JY: Impact of conversion
surgery on survival in locally advanced pancreatic cancer patients
treated with FOLFIRINOX chemotherapy. J Hepatobiliary Pancreat Sci.
30:111–121. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Addeo P, Canali G, Paul C, de Mathelin P,
Averous G and Bachellier P: Long-term survival after resection of
invasive pancreatic intraductal papillary mucinous neoplasm.
Langenbecks Arch Surg. 409:3612024. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Balta KY, Welch S, Vincent M and Breadner
D: Near 5-year survival in metastatic pancreatic cancer patient
with ROS1 rearrangement, HER2 amplification, and KRAS G12C
mutation-a case report. J Gastrointest Oncol. 14:2273–2278. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Campoverde LE, Batalini F, Bulushi Y and
Bullock A: Response in BRCA1 mutation carrier with
metastatic pancreatic adenocarcinoma treated with FOLFIRINOX. BMJ
Case Rep. 15:e2493702022. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Shelemey PT, Amaro CP, Ng D, Falck V and
Tam VC: Metastatic pancreatic cancer with complete response to
FOLFIRINOX treatment. BMJ Case Rep. 14:e2383952021. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Laura A, Anna C, Cinquepalmi M, Giovanni
M, Sole MM, Nava AK, Niccolò P, Giuseppe N, Stefano V, Paolo A, et
al: Is complete pathologic response in pancreatic cancer
overestimated? A systematic review of prospective studies. J
Gastrointest Surg. 24:2336–2348. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Blair AB, Yin LD, Pu N, Yu J, Groot VP,
Rozich NS, Javed AA, Zheng L, Cameron JL, Burkhart RA, et al:
Recurrence in patients achieving pathological complete response
after neoadjuvant treatment for advanced pancreatic cancer. Ann
Surg. 274:162–169. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
He J, Blair AB, Groot VP, Javed AA,
Burkhart RA, Gemenetzis G, Hruban RH, Waters KM, Poling J, Zheng L,
et al: Is a pathological complete response following neoadjuvant
chemoradiation associated with prolonged survival in patients with
pancreatic cancer? Ann Surg. 268:1–8. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zhou Y, Liao S, You J and Wu H: Conversion
surgery for initially unresectable pancreatic ductal adenocarcinoma
following induction therapy: A systematic review of the published
literature. Updates Surg. 74:43–53. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Okada K, Uemura K, Okamoto W, Sumiyoshi T,
Shintakuya R, Otsuka H, Serikawa M, Ishii Y, Arihiro K and
Takahashi S: Pathologic complete response following FOLFIRINOX and
olaparib treatment for hepatic metastasized pancreatic ductal
adenocarcinoma with a germline BRCA mutation. Clin J Gastroenterol.
16:283–288. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Luu AM, Hoehn P, Vogel SR,
Reinacher-Schick A, Munding J, Uhl W and Braumann C: pathologic
complete response of pancreatic cancer following neoadjuvant
FOLFIRINOX treatment in hepatic metastasized pancreatic cancer.
Visc Med. 35:387–391. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Health Research Authority, . Investigation
of a therapeutic vaccine (ACIT-1) in late-stage cancer. Health
Research Authority (UK). https://www.hra.nhs.uk/planning-and-improving-research/application-summaries/research-summaries/investigation-of-a-therapeutic-vaccine-acit-1-in-late-stage-cancer/May
16–2025
|
|
16
|
ClinicalTrials.gov, . A Phase I Clinical
Study to Determine the Optimal Dose for the Safe Immune Restoration
and Immune Response of Allogeneic Cell Immunotherapy (ACIT-1) in
Adult Cancer Patients. ClinicalTrials.gov identifier: NCT03096093.
National Library of Medicine; Bethesda, MD: 2017, https://clinicaltrials.gov/study/NCT03096093July
11–2025
|
|
17
|
Gomari MM, Ghantabpour T, Pourgholam N,
Rostami N, Hatfield SM, Namazifar F, Abkhiz S, Eslami SS,
Ramezanpour M, Darestanifarahani M, et al: Breaking barriers: Smart
vaccine platforms for cancer immunomodulation. Cancer Commun
(Lond). 45:529–571. 2025. View Article : Google Scholar : PubMed/NCBI
|