Introduction
Breast cancer (BC) has the second highest
age-standardized incidence rate (46.8 per 100,000) among malignant
tumors worldwide according to recent global cancer burden data
(1). Neoadjuvant therapy (NAT) has
become the acknowledged standard treatment for middle- and
early-stage BC worldwide (2). NAT
offers several clinical advantages, including tumor downstaging,
reduction in tumor size to facilitate breast-conserving surgery,
expansion of surgical options, early assessment of treatment
response, reduction of systemic tumor burden and improvement of
long-term clinical prognosis (3).
Pathological complete response (pCR), defined as the absence of
residual invasive cancer in the breast and axillary lymph nodes
after NAT (4,5), is commonly used as a key endpoint in
clinical studies. Achieving a pCR is associated with markedly
improved long-term survival outcomes, compared with those have
residual tumors (4). Human
epidermal growth factor receptor 2 (HER2)-positive BC represents a
distinct molecular subtype, characterized by high invasiveness,
early metastasis, a poor prognosis and a high risk of recurrence,
as well as reduced sensitivity to conventional chemotherapy
(5,6). In recent years, the development and
clinical application of HER2-targeted therapies and small-molecule
inhibitors have substantially improved treatment outcomes (7). In particular, the combination of
trastuzumab and pertuzumab with chemotherapy drugs has been shown
to be safe and to achieve higher pCR rates (39.38–68%) in multiple
studies (8–10).
Magnetic resonance imaging (MRI), particularly the
combination of dynamic contrast-enhanced MRI (DCE-MRI) and
diffusion weighted imaging (DWI), is currently regarded as a
preferred method for evaluating the efficacy of NAT in BC (11). DCE-MRI combined with DWI enables
morphological assessment for tumor size and post-treatment
contraction patterns in both the primary tumor and axillary lymph
nodes, while also providing functional information on water
molecule diffusion, cellular metabolism and tumor hemodynamics
(12,13). Semi-quantitative parameters, such as
the time intensity curve (TIC), and quantitative measures, such as
the apparent diffusion coefficient (ADC) value, further reflect the
structural and microenvironmental characteristics of tumor tissue
(14).
In addition to imaging data, response to NAT can
also be reflected by various circulating tumor biomarkers (15). Carcinoembryonic antigen (CEA) is a
widely used non-specific tumor marker that is elevated in several
malignancies, including colorectal (16), lung (17) and gastric (18) cancer, as well as BC (19). Carbohydrate antigens (CAs),
including CA125, CA153, CA19-9, CA724, CA242, represent another
group of commonly used markers in clinical practice (19). However, no standardized approach
exists regarding the optimal selection or combination of these
markers for evaluating NAT response in BC. Therefore, integrating
serum tumor markers with imaging data may improve the assessment of
treatment response.
Generally, the early prediction and identification
of patients likely to achieve a pCR during NAT, using readily
available clinical data, can provide valuable guidance for
optimizing surgical timing and strategy, as well as subsequent
treatment planning (20).
Accordingly, the development of predictive models for pathological
response in HER2-positive BC following neoadjuvant targeted therapy
(NTT) has become an important area of research. In the present
study, independent predicators of pCR were identified from
pathological features, DCE-MRI imaging parameters and serum tumor
biomarkers in patients with HER2-positive BC. Based on these
factors, a comprehensive predictive model was developed and
presented as a nomogram to facilitate the preoperative estimation
of treatment response and support individualized clinical
decision-making.
Patients and methods
Study cohorts
The study protocol was reviewed and approved by the
institutional ethics committee of the Third Affiliated Hospital of
Kunming Medical University, Yunnan Cancer Hospital, Yunnan Cancer
Centre, Peking University Cancer Hospital Yunnan Hospital, Kunming,
China (approval no. KYLX2022182). Patients were enrolled after a
diagnosis of early- or mid-stage (less than stage IV) HER2-positive
BC confirmed by preoperative biopsy. Patients were retrospectively
included between January 1, 2018, and December 31, 2021, and
prospectively enrolled between January 1, 2022, and September 30,
2022, at the Breast Cancer Center of the Third Affiliated Hospital
of Kunming Medical University, Yunnan Cancer Hospital (Kunming,
China). Inclusion criteria were as follows: i) Newly diagnosed
early- or mid-stage (less than stage IV) HER2-positive BC; ii)
completion of full-course NAT combining targeted therapy and
chemotherapy; iii) surgery performed after NAT with available
pathological results; and iv) complete MRI and hematological data
at baseline, after the first cycle of NTT, and after completion of
NAT prior to surgery. The exclusion criteria were as follows: i)
Incomplete pathological or hematological data; ii) stage IV BC at
initial diagnosis; iii) failure to complete targeted therapy; iv)
failure to undergo surgery as scheduled; v) contraindications to
MRI (such as claustrophobia or contrast allergy); and vi)
complicated by other primary malignant tumors. The same inclusion
and exclusion criteria were applied uniformly to both the
retrospective and prospective cohorts.
A total of 2,916 patients with HER2-positive
invasive BC were retrospectively screened, 269 of whom met the
eligibility criteria and were included for model development and
internal validation. Subsequently, 24 patients meeting the same
criteria were prospectively enrolled for external validation. The
study flowchart is presented in Fig.
1. All patients included were female, and the median age was 48
years (range, 24–73 years). The retrospective cohort comprised 269
female patients, with a median age of 48 years (range, 24–68
years). The prospective cohort included 24 female patients, with a
median age of 44 years (range, 29–73 years).
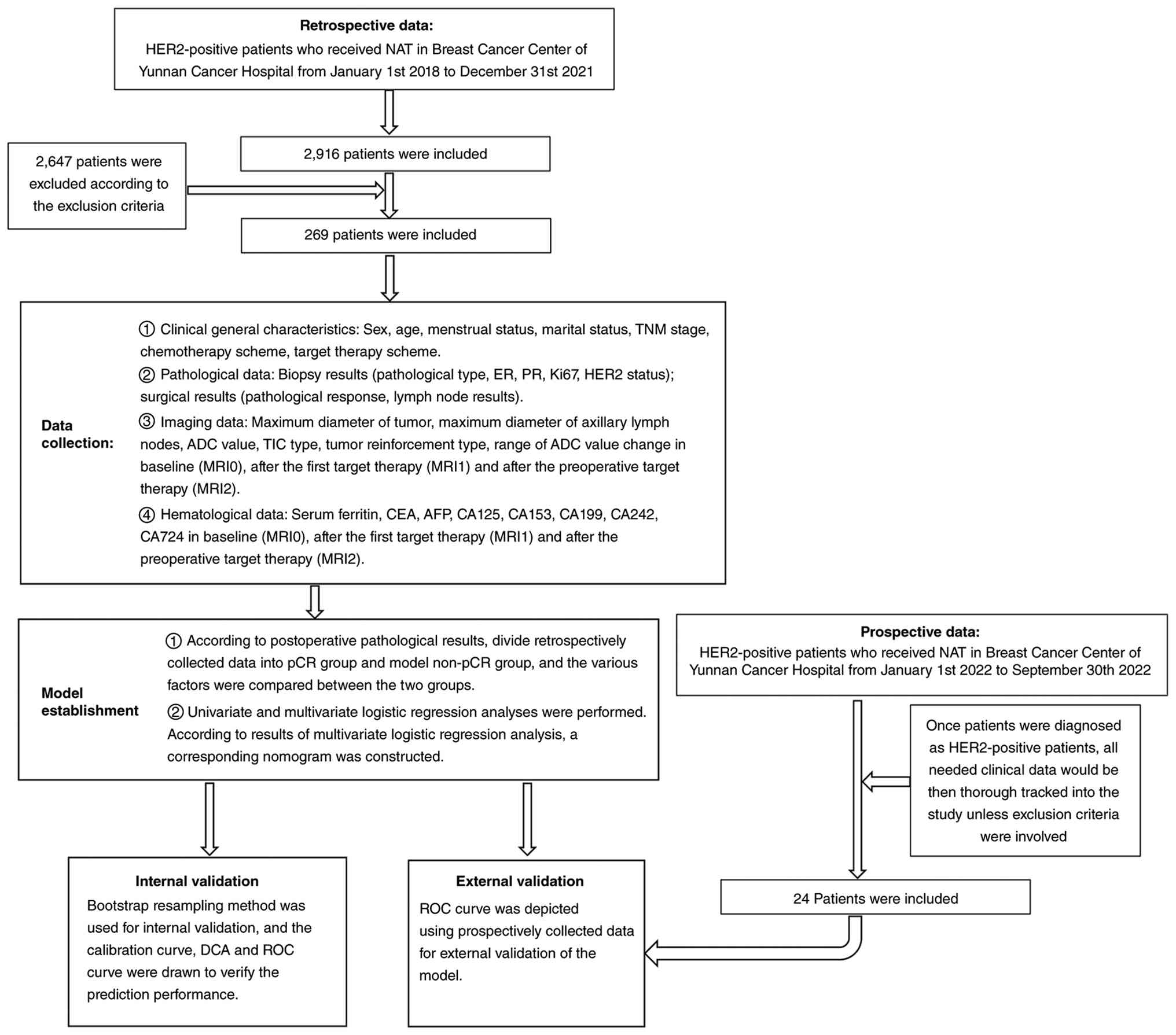 | Figure 1.Flowchart of the whole study. A
simple and clear flowchart of the whole study to demonstrate how
this study was carried out step by step from data collection to
model construction and validation. HER2, human epidermal growth
factor receptor 2; NAT, neoadjuvant therapy; TNM,
Tumor-Node-Metastasis; ER, estrogen receptor; PR, progesterone
receptor; ADC, apparent diffusion coefficient; TIC, time intensity
curve; MRI, magnetic resonance imaging; CEA, carcinoembryonic
antigen; AFP, α-fetoprotein; CA, carbohydrate antigen; pCR,
pathological complete response; DCA, decision curve analysis; ROC,
receiver operating characteristic. |
Clinical data collection
Basic clinical features and NAT regimens
Collected clinically relevant variables included
sex, age, menstrual status, marital status and TNM stage (based on
the 8th edition of the American Joint Committee on Cancer staging
manual (21), as well as
chemotherapy and targeted therapy regimens. Neoadjuvant
chemotherapy regimens in this study primarily included Taxol +
carboplatin (21-day cycle, for six cycles) and anthracyclines +
cyclophosphamide followed by Taxol (21-day cycle, for eight
cycles). Targeted therapy included trastuzumab (Herceptin) alone or
dual-target trastuzumab + pertuzumab (HP), administered every 21
days for a duration of 1 year.
Pathological data
Estrogen receptor (ER), progesterone receptor (PR),
Ki-67 and HER2 status were assessed using immunohistochemistry on
initial biopsy specimens and independently confirmed by two
pathologists, which were directly obtained from the original
diagnostic pathology reports in the patients' medical records, as
assessed by the institutional pathology department. Following
completion of NAT, surgical treatment was performed based on
patient preference, tumor size and relevant clinical status. pCR
was defined as the absence of residual invasive cancer cells in the
breast and negative axillary lymph nodes on postoperative
pathological evaluation.
Imaging data acquisition
MRI examinations were performed using a Siemens
Avanto1.5T system (Siemens AG) with a dedicated four-channel breast
coil. Patients were positioned prone with both breasts placed
within the coil (head advanced, arms raised and bilateral breasts
naturally overhung in the groove of the coil on the surface of the
breast). DCE-MRI was conducting using a three-dimensional dynamic
imaging sequence (repetition time, 4.43 msec; echo time, 1.5 msec;
field of view, 340 mm; slice thickness, 1.7 mm; flip angle, 10°;
average acquisition times, once). After an acquisition of
pre-contrast images, gadodiamide was administered intravenously at
a dose of 0.2 mmol/kg (body weight), and a rate of 2.5 ml/sec
followed by seven sequential dynamic enhancement acquisitions (60
sec per phase).
The imaging data collected included the maximum
tumor diameter, maximum axillary lymph node diameter, ADC value,
TIC type and tumor enhancement type on MRI at baseline before the
first NTT (MRI0), after the first NTT (MRI1) and after the last NTT
(MRI2). MRI0 data was collected before any invasive procedures such
as biopsy, when the tumor remained completely unaltered by any
intervention, which denotes the most original state of the disease
at the time of initial discovery. The ADC values in MRI0, MRI1 and
MRI2 were recorded as ADC0, ADC1 and ADC2, respectively. Relative
changes in ADC were calculated as ΔADC1 (ADC1 vs. ADC0), ΔADC2
(ADC2 vs. ADC0) and ΔADC3 (ADC2 vs. ADC1). The TIC types in MRI0,
MRI1 and MRI2 were denoted as TIC0, TIC1 and TIC2,
respectively.
Hematological data
Serum ferritin (SF), CEA, α-fetoprotein (AFP),
CA125, CA153, CA199, CA242 and CA724 were measured using a
chemiluminescence immunoassay (Sample source and amount: Fasting
venous blood (5 ml) was collected from each patient before
treatment. Serum was separated by centrifugation at 1,510 × g for
10 min at room temperature. Assay platform and reagents: The serum
levels of SF, CEA, AFP, CA125, CA153, CA199, CA242 and CA724 were
measured using a cobas 8000 e801 electrochemiluminescence
immunoassay analyzer (Roche Diagnostics) with paired reagent kits
(cat. no. 2019062457). All procedures were performed strictly
according to the instrument and reagent instructions). Measurements
were recorded at baseline (−0), after the first cycle of targeted
therapy (−1) and after completion of NAT before surgery (−2).
Construction and validation of
nomogram model
Continuous variables with skewed distributions are
presented as the median (range), whereas normally distributed
variables are expressed as the mean ± standard deviation.
Categorical variables are presented as frequency (percentage).
Patients were categorized into pCR and non-pCR groups based on
postoperative pathological information.
Comparisons between groups were performed using
unpaired independent-samples Student's t-test or Levene's test for
continuous variables, the rank-sum test for ordinal variables, and
Pearson's χ2 test or Fisher's exact test for categorical
variables. For retrospective data, univariate logistic regression
analysis was conducted to identify factors associated with pCR
after NAT, and variables with P<0.10 were subsequently included
in multivariate logistic regression analysis to identify
independent predictors. These predictors were used to construct the
nomogram.
Internal validation was performed using bootstrap
resampling (1,000 iterations). Calibration curves were generated to
assess agreement between predicted and observed outcomes. Decision
curve analysis (DCA) was conducted to evaluate clinical utility
across a range of threshold probabilities. Model discrimination was
assessed using receiver operating characteristic (ROC) curves and
the area under the ROC curve (AUC), with AUC >0.75 indicating
good predictive performance.
External validation was conducted using prospective
data, and ROC curves and AUC values were calculated
accordingly.
Statistical analysis
Statistical analyses were performed using SPSS 22.0
(IBM Corp.), Graphpad Prism version 7.0 (Dotmatics) and R software
(version 4.1.2; http://www.r-project.org/). R packages used included
rms, pROC, rmda and caret. Two-sided P<0.05 was considered to
indicate a statistically significant difference.
Results
Significant differences in the
distribution of four basic clinical characteristics in the
comparison between pCR and non-pCR groups in retrospective
data
A total of 269 patients were included in the
retrospective cohort. All patients were female, married and
diagnosed with invasive ductal carcinoma. Significant differences
were observed in four clinical characteristics between the pCR
group and non-pCR groups. Regarding tumor burden, T stage was
predominantly T2 in both groups; however, the proportion of T2
tumors was significantly higher in the pCR group than in the
non-pCR group (68.32 vs. 50.00%). Similarly, patients in the pCR
group were more frequently classified as early to mid-stage
(2A-3A), whereas those in the non-pCR group were more often in more
advanced stages (2B-3B). In terms of hormone receptor expression,
the proportions of ER-positive (48.15%) and PR-positive (68.52%)
tumors were higher in the non-pCR group than in the pCR group.
Regarding the NAT regimen, anthracycline-based chemotherapy and
dual-target therapy with HP were the main treatment approaches in
both groups (Table I).
 | Table I.Basic clinical characteristic
comparison between the pCR and non-pCR groups in retrospective
data. |
Table I.
Basic clinical characteristic
comparison between the pCR and non-pCR groups in retrospective
data.
|
Characteristics | pCR group | Non-pCR group | t/χ2/Z
value | P-value |
|---|
| Age,
yearsa | 49 (24–68) | 46 (27–65) | 1.242 | 0.216 |
| Sex, n (%) |
|
| 0.000 | 1.000 |
|
Female | 161 (100.00) | 108 (100.00) |
|
|
|
Male | 0 (0.00) | 0 (0.00) |
|
|
| Menstrual status, n
(%) |
|
| 2.226 | 0.136 |
|
Pre-menopausal | 79 (49.07) | 63 (58.33) |
|
|
| After
menopause | 82 (50.93) | 45 (41.67) |
|
|
| Marital status, n
(%) |
|
| 0.000 | 1.000 |
|
Unmarried | 0 (0.00) | 0 (0.00) |
|
|
|
Married | 161 (100.00) | 108 (100.00) |
|
|
| T stage, n (%) |
|
| −3.195 | 0.001b |
| 1 | 6 (3.73) | 4 (3.70) |
|
|
| 2 | 110 (68.32) | 54 (50.00) |
|
|
| 3 | 29 (18.01) | 23 (21.30) |
|
|
| 4 | 16 (9.94) | 27 (25.00) |
|
|
| N stage, n (%) |
|
| −1.204 | 0.229 |
| 0 | 21 (13.04) | 9 (8.33) |
|
|
| 1 | 101 (62.73) | 67 (62.04) |
|
|
| 2 | 31 (19.25) | 29 (26.85) |
|
|
| 3 | 8 (4.97) | 3 (2.78) |
|
|
| TNM stage, n
(%) |
|
| −2.571 | 0.010b |
| 2A | 19 (11.80) | 9 (8.33) |
|
|
| 2B | 78 (48.45) | 40 (37.04) |
|
|
| 3A | 42 (26.09) | 30 (27.78) |
|
|
| 3B | 14 (8.70) | 26 (24.07) |
|
|
| 3C | 8 (4.97) | 3 (2.78) |
|
|
| Pathological type,
n (%) |
|
| 0.000 | 1.000 |
|
Invasive ductal carcinoma | 161 (100.00) | 108 (100.00) |
|
|
| Other
types | 0 (0.00) | 0 (0.00) |
|
|
| ER status, n
(%) |
|
| 5.777 | 0.016b |
|
Positive | 54 (33.54) | 52 (48.15) |
|
|
|
Negative | 107 (66.46) | 56 (51.85) |
|
|
| PR status, n
(%) |
|
| 7.125 | 0.008b |
|
Positive | 84 (52.17) | 74 (68.52) |
|
|
|
Negative | 77 (47.83) | 34 (31.48) |
|
|
| Ki67c | 39.690±17.845 | 37.900±20.500 | 0.758 | 0.449 |
| Target therapy
scheme, n (%) |
|
| 3.503 | 0.061 |
|
Herceptin (trastuzumab) | 37 (22.98) | 36 (33.33) |
|
|
|
Herceptin (trastuzumab) +
pertuzumab | 124 (77.02) | 72 (66.67) |
|
|
| Chemotherapy
scheme, n (%) |
|
| 0.157 | 0.692 |
| Taxol +
carboplatin | 65 (40.37) | 41 (37.96) |
|
|
|
Anthracyclines + | 96 (59.63) | 67 (62.04) |
|
|
|
cyclophosphamide followed by
Taxol |
|
|
|
|
| Number of
postoperative axillary lymph nodesc | 16.660±5.237 | 16.730±5.779 | −0.098 | 0.922 |
In total, 14 basic clinical characteristics were
compared. No significant differences were observed between the pCR
and non-pCR groups in terms of age, sex, menstrual status, marital
status, pathological type, N stage, Ki-67 expression, targeted
therapy regimen, chemotherapy regimen, or number of postoperative
pathological axillary lymph nodes. However, significant differences
were found in T stage, overall TNM stage, ER expression and PR
expression (Table I). Specifically,
lower T stage, earlier TNM comprehensive stage, and negative ER/PR
expression were associated with a higher pCR rate.
Lack of significant differences in the
distribution of basic clinical characteristics in the comparison
between pCR and non-pCR groups in prospective data
A total of 24 patients with HER2-positive BC were
prospectively enrolled as the external validation cohort. The
median age in the prospective data was 48.5 years in the pCR group
and 40.5 years in the non-pCR group. All of these patients were
female, married and had invasive ductal carcinoma. No significant
differences were observed in the distribution of the 14 basic
clinical characteristics between the two groups (Table II). This lack of significance may
be related to the small sample size of the cohort (n=24) limiting
statistical power, and the relatively homogeneous baseline
characteristics of the prospectively enrolled patients.
| Table II.Basic clinical characteristics
comparison between the pCR and non-pCR groups in prospective
data. |
Table II.
Basic clinical characteristics
comparison between the pCR and non-pCR groups in prospective
data.
|
Characteristics | pCR group | Non-pCR group | t/χ2/Z
value | P-value |
|---|
| Age,
yearsa | 48.5 (29–73) | 40.5 (35–52) | 1.565 | 0.132 |
| Sex, n (%) |
|
| 0.000 | 1.000 |
|
Female | 16 (100.00) | 8 (100.00) |
|
|
|
Male | 0 | 0 |
|
|
| Menstrual status, n
(%) |
|
| -b | 0.178 |
|
Pre-menopausal | 8 (50.00) | 7 (87.50) |
|
|
| After
menopause | 8 (50.00) | 1 (12.50) |
|
|
| Marital status, n
(%) |
|
| 0.000 | 1.000 |
|
Unmarried | 0 | 0 |
|
|
|
Married | 16 (100.00) | 8 (10.00) |
|
|
| T stage, n (%) |
|
| −0.283 | 0.777 |
| 1 | 2 (12.50) | 0 |
|
|
| 2 | 9 (56.25) | 6 (75.00) |
|
|
| 3 | 2 (12.50) | 0 |
|
|
| 4 | 3 (18.75) | 2 (25.00) |
|
|
| N stage, n (%) |
|
| −0.245 | 0.806 |
| 0 | 0 | 2 (25.00) |
|
|
| 1 | 8 (50.00) | 6 (75.00) |
|
|
| 2 | 7 (43.75) | 0 |
|
|
| 3 | 1 (6.25) | 0 |
|
|
| TNM stage, n
(%) |
|
| −1.403 | 0.161 |
| 2A | 1 (6.25) | 2 (25.00) |
|
|
| 2B | 5 (31.25) | 4 (50.00) |
|
|
| 3A | 6 (37.50) | 0 |
|
|
| 3B | 3 (18.75) | 2 (25.00) |
|
|
| 3C | 1 (6.25) | 0 |
|
|
| Pathological type,
n (%) |
|
| 0.000 | 1.000 |
|
Invasive ductal carcinoma | 16 (100.00) | 8 (100.00) |
|
|
| Other
types | 0 | 0 |
|
|
| ER status, n
(%) |
|
| -b | 0.099 |
|
Positive | 4 (25.00) | 5 (62.50) |
|
|
|
Negative | 12 (75.00) | 3 (37.50) |
|
|
| PR status, n
(%) |
|
| -b | 0.099 |
|
Positive | 4 (25.00) | 5 (62.50) |
|
|
|
Negative | 12 (75.00) | 3 (37.50) |
|
|
| Ki67c | 30.000±9.832 | 28.125±15.338 | 0.365 | 0.719 |
| Target therapy
scheme, n (%) |
|
| -b | 0.647 |
|
Herceptin (trastuzumab) | 4 (25.00) | 3 (37.50) |
|
|
|
Herceptin (trastuzumab) +
pertuzumab | 12 (75.00) | 5 (62.50) |
|
|
| Chemotherapy
scheme, n (%) |
|
| -b | 0.289 |
| Taxol +
carboplatin | 14 (87.50) | 5 (62.50) |
|
|
|
Anthracyclines +
cyclophosphamide followed by Taxol | 2 (12.50) | 3 (37.50) |
|
|
| Number of
postoperative axillary lymph nodesc | 16.630±6.407 | 14.630±6.301 | −0.725 | 0.476 |
Comparison of MRI findings between the
pCR and non-pCR groups in the retrospective cohort
MRI0 data
Before NTT, the mean maximum tumor diameter was
significantly smaller in the pCR group than that in the non-pCR
group. The mean ADC values were ~0.7 in both groups, with no
significant difference. In >60% of patients in both groups, the
main TIC pattern was the inflow-outflow type (Table III).
| Table III.Comparison of MRI0 data between pCR
group and non-pCR groups. |
Table III.
Comparison of MRI0 data between pCR
group and non-pCR groups.
| MRI0 | pCR group | Non-pCR group | t/χ2/Z
value | P-value |
|---|
| Maximum diameter of
tumor, cma | 3.776±1.753 | 4.584±2.249 | −3.147 | 0.002b |
| Maximum diameter of
axillary lymph nodes, cma | 1.521±1.180 | 1.293±0.950 | 1.671 | 0.096 |
| ADC0
(×10−3 mm2/sec)a | 0.746±0.151 | 0.716±0.134 | 1.710 | 0.088 |
| MRI0 TIC0 type, n
(%) |
|
| 1.221 | 0.543 |
|
Inflow-inflow | 5 (3.11) | 2 (1.85) |
|
|
|
Inflow-platform | 57 (35.40) | 33 (30.56) |
|
|
|
Inflow-outflow | 99 (61.49) | 73 (67.59) |
|
|
| Reinforcement-type,
n (%) |
|
| 0.260 | 0.878 |
| No
reinforcement | 9 (5.59) | 7 (6.48) |
|
|
|
Reinforcement | 146 (90.68) | 98 (90.74) |
|
|
| Uneven
reinforcement | 6 (3.73) | 3 (2.78) |
|
|
MRI1 data
After the first targeted therapy cycle, significant
differences in MRI parameters were observed between the two groups.
The maximum tumor diameter decreased in both groups and was
significantly smaller in the pCR group than that in the non-pCR
group (2.217±1.307 vs. 3.516±2.179 cm). The reduction in tumor
diameter was greater in the pCR group (41.287%) than in the non-pCR
group (23.298%) (Table IV).
| Table IV.MRI1 data comparison between the pCR
and non-pCR groups. |
Table IV.
MRI1 data comparison between the pCR
and non-pCR groups.
| MRI1 | pCR group | Non-pCR group | t/χ2/Z
value | P-value |
|---|
| Maximum diameter of
tumor, cma | 2.217±1.307 | 3.516±2.179 | −5.560 |
<0.001b |
| Maximum diameter of
axillary lymph nodes, cma | 0.784±0.803 | 0.823±0.691 | −0.409 | 0.683 |
| ADC1
(×10−3 mm2/sec)a | 1.035±0.281 | 0.919±0.228 | 3.721 |
<0.001b |
| MRI1 TIC1 type, n
(%) |
|
| 27.886 |
<0.001b |
|
Inflow-inflow | 41 (25.47) | 12 (11.11) |
|
|
|
Inflow-platform | 83 (51.55) | 38 (35.19) |
|
|
|
Inflow-outflow | 37 (22.98) | 58 (53.70) |
|
|
| Reinforcement type,
n (%) |
|
| 0.254 | 0.881 |
| No
reinforcement | 14 (8.70) | 9 (8.33) |
|
|
|
Reinforcement | 144 (89.44) | 96 (88.89) |
|
|
| Uneven
reinforcement | 3 (1.86) | 3 (2.78) |
|
|
| ΔADC1, % | 28.919±31.935 | 20.384±22.760 | 2.558 | 0.011b |
The mean ADC1 value in the pCR group was
significantly different from that in the non-pCR group. ADC values
increased in both groups compared with baseline. The increase in
ADC1 relative to ADC0 was greater in the pCR group (28.919%) than
in the non-pCR group ΔADC1 (20.384%). In addition, the main TIC
type in the pCR group changed from inflow-outflow to
inflow-platform, whereas the main TIC type in the non-pCR group
remained as inflow-outflow (Table
IV).
MRI2 data
After 4–6 cycles of preoperative NAT, the maximum
tumor diameter was further reduced in both groups, and the tumor
diameter in the pCR group remained significantly smaller than that
in the non-pCR group. In the pCR group, the ADC2 value increased to
1.222±0.256 (×10−3 mm2/sec), which was 18.617
and 47.536% higher than the ADC1 and ADC0 values, respectively. In
the non-pCR group, the average value of ADC2 increased to
0.944±0.264 (×10−3 mm2/sec), which was 2.470
and 22.855% higher than those of the ADC1 and ADC0 values,
respectively. ADC2, ΔADC2 and ΔADC3 were all significantly higher
in the pCR group than those in the non-pCR group. The main TIC type
in the pCR group further changed to the inflow-inflow type (74.5%),
whereas the main TIC type in the non-pCR group changed from the
inflow-outflow at MRI0 and MRI1 to the inflow-platform at MRI2
(Table V).
| Table V.Comparison of MRI2 data between the
pCR and non-pCR groups. |
Table V.
Comparison of MRI2 data between the
pCR and non-pCR groups.
| MRI2 | pCR group | Non-pCR group | t/χ2/Z
value | P-value |
|---|
| Maximum diameter of
tumor, cma | 1.515±1.182 | 2.517±1.860 | −4.965 |
<0.001b |
| Maximum diameter of
axillary lymph nodes, cma | 0.442±0.436 | 0.469±0.501 | −0.472 | 0.637 |
| ADC2
(×10−3 mm2/sec)a | 1.222±0.256 | 0.944±0.264 | 8.613 |
<0.001b |
| MRI2 TIC2 type, n
(%) |
|
|
|
<0.001b |
|
Inflow-inflow | 120 (74.53) | 22 (20.37) | 77.505 |
|
|
Inflow-platform | 29 (18.01) | 51 (47.22) |
|
|
|
Inflow-outflow | 12 (7.45) | 35 (32.41) |
|
|
| Type of
reinforcement, n (%) |
|
| 1.715 | 0.424 |
| No
reinforcement | 17 (10.56) | 11 (10.19) |
|
|
|
Reinforcement | 141 (87.58) | 92 (85.19) |
|
|
| Uneven
reinforcement | 3 (1.86) | 5 (4.63) |
|
|
| ΔADC2, % | 47.536±30.597 | 22.855±25.765 | 7.136 |
<0.001b |
| ΔADC3, % | 18.617±29.274 | 2.470±23.459 | 4.792 |
<0.001b |
Hematological characteristics
comparison between pCR and non-pCR groups in the retrospective
cohort
At baseline, SF0 was significantly higher and CEA0
was significantly lower in the pCR group than those values in the
non-pCR group. After the first targeted therapy cycle, only CEA1
differed significantly between the two groups, and the CEA showed
continuous downward trend from baseline to the last time point in
both groups. After the last preoperative targeted therapy, CEA2,
AFP2 and CA153-2 were significantly lower in the pCR group than in
the non-pCR group. No significant differences were found in CA125,
CA19-9, CA242 and CA724 between the two groups (Table VI).
| Table VI.Tumor marker comparison between the
pCR and non-pCR groups in retrospective data. |
Table VI.
Tumor marker comparison between the
pCR and non-pCR groups in retrospective data.
| Tumor markers | pCR group | Non-pCR group | t/χ2/Z
value | P-value |
|---|
| SF |
|
|
|
|
|
SF0 |
295.994±164.773 |
279.620±328.425 | 2.068 | 0.041a |
|
SF1 |
302.903±248.534 |
277.180±256.492 | 0.765 | 0.445 |
|
SF2 |
268.724±269.541 |
260.738±224.678 | 0.240 | 0.810 |
| CEA |
|
|
|
|
|
CEA0 | 4.110±6.206 | 6.298±8.923 | 2.175 | 0.031a |
|
CEA1 | 2.361±1.487 | 4.070±3.902 | 4.326 |
<0.001a |
|
CEA2 | 2.041±1.213 | 2.693±1.602 | 3.776 |
<0.001a |
| AFP |
|
|
|
|
|
AFP0 | 4.525±2.697 | 3.802±2.300 | 2.129 | 0.034 |
|
AFP1 | 3.526±2.264 | 3.658±2.078 | 0.440 | 0.660 |
|
AFP2 | 3.186±2.173 | 3.821±2.347 | 2.083 | 0.038a |
| CA125 |
|
|
|
|
|
CA125-0 | 19.397±15.353 | 18.621±9.759 | 0.466 | 0.642 |
|
CA125-1 | 15.983±8.139 | 16.790±7.732 | 0.812 | 0.417 |
|
CA125-2 | 13.683±5.758 | 14.923±7.463 | 1.460 | 0.146 |
| CA153 |
|
|
|
|
|
CA153-0 | 16.714±12.249 | 17.442±16.418 | 0.416 | 0.678 |
|
CA153-1 | 19.068±11.397 | 21.599±15.404 | 1.547 | 0.123 |
|
CA153-2 | 17.026±7.557 | 20.117±9.629 | 2.801 | 0.006a |
| CA199 |
|
|
|
|
|
CA199-0 | 14.942±10.995 | 12.799±10.144 | 1.481 | 0.140 |
|
CA199-1 | 14.300±11.163 | 13.946± 8.874 | 0.248 | 0.804 |
|
CA199-2 | 14.538±10.130 | 14.053±10.647 | 0.344 | 0.732 |
| CA242 |
|
|
|
|
|
CA242-0 | 8.507±8.464 | 6.844±5.425 | 1.644 | 0.102 |
|
CA242-1 | 8.217±7.216 | 7.149±5.492 | 1.172 | 0.242 |
|
CA242-2 | 8.822±7.203 | 8.203±7.879 | 0.606 | 0.545 |
| CA724 |
|
|
|
|
|
CA724-0 | 6.913±11.026 | 6.468±9.677 | 0.288 | 0.774 |
|
CA724-1 | 8.025±9.438 | 7.806±20.223 | 0.106 | 0.916 |
|
CA724-2 | 9.257±12.741 | 9.142±17.916 | 0.055 | 0.956 |
Univariate logistic regression
analysis of retrospective data
Univariate logistic regression analysis revealed
that TNM stage 2A (vs. 3B), ER status, PR status, maximum diameter
(in MRI0, MRI1, and MRI2), TIC inflow to inflow type in MRI1 (vs.
inflow to outflow type), TIC inflow to inflow type in MRI2 (vs.
inflow to outflow type and vs. inflow to platform type) ADC1, ADC2,
ΔADC1, ΔADC2, ΔADC3, SF0, CEA-0, CEA1, CEA-2, AFP-0, AFP-2 and
CA153-2 were predictive factors for pCR (Table VII).
| Table VII.Univariate logistics regression
analysis of all factors in retrospective data. |
Table VII.
Univariate logistics regression
analysis of all factors in retrospective data.
|
| Univariate
logistics regression analysis |
|---|
|
|
|
|---|
|
Characteristics | β | P-value | OR | 95% CI |
|---|
| Age | 0.017 | 0.215 | 1.017 | 0.990 | 1.045 |
| Menstrual
conditions | 0.374 | 0.136 | 0.688 | 0.421 | 1.125 |
| T stage |
|
|
|
|
|
|
T1-T2 | 0.306 | 0.646 | 1.358 | 0.368 | 5.015 |
|
T1-T3 | 0.174 | 0.805 | 0.841 | 0.212 | 3.336 |
|
T1-T4 | 0.929 | 0.196 | 0.395 | 0.097 | 1.615 |
| N stage |
|
|
|
|
|
|
N0-N1 | 0.437 | 0.308 | 0.646 | 0.279 | 1.496 |
|
N0-N2 | 0.781 | 0.100 | 0.458 | 0.181 | 1.162 |
|
N0-N3 | 0.134 | 0.865 | 1.143 | 0.245 | 5.329 |
| TNM stage |
|
|
|
|
|
|
2A-2B | 0.079 | 0.860 | 0.924 | 0.383 | 2.227 |
|
2A-3A | 0.411 | 0.382 | 0.663 | 0.264 | 1.666 |
|
2A-3B | 1.366 | 0.009a | 0.255 | 0.091 | 0.711 |
|
2A-3C | 0.234 | 0.767 | 1.263 | 0.269 | 5.927 |
| Age | 0.017 | 0.215 | 1.017 | 0.990 | 1.045 |
| ER status | 0.610 | 0.017a | 0.543 | 0.330 | 0.896 |
| PR status | 0.691 | 0.008a | 0.501 | 0.301 | 0.835 |
| Ki67 | 0.005 | 0.448 | 1.005 | 0.992 | 1.018 |
| Target scheme | 0.516 | 0.062 | 1.676 | 0.974 | 2.884 |
| Chemotherapy
scheme | 0.101 | 0.692 | 1.106 | 0.671 | 1.824 |
| Number of
postoperative axillary lymph nodes | 0.002 | 0.921 | 0.998 | 0.954 | 1.043 |
| Maximum diameter of
MRI0 tumor, cm | 0.206 | 0.002a | 0.814 | 0.716 | 0.925 |
| MRI0 maximum
diameter of axillary lymph nodes, cm | 0.197 | 0.098 | 1.218 | 1.218 | 0.964 |
| MRI0 ADC0
(×10−3 mm2/sec) | 1.507 | 0.090 | 4.515 | 0.791 | 25.777 |
| MRI0 TIC0 type |
|
|
|
|
|
| Inflow
to inflow-inflow to platform | 0.370 | 0.669 | 0.691 | 0.127 | 3.763 |
| Inflow
to inflow-inflow to outflow | 0.612 | 0.472 | 0.542 | 0.102 | 2.874 |
| MRI0 reinforcement
type |
|
|
|
|
|
| No
reinforcement-reinforcement | 0.147 | 0.777 | 1.159 | 0.418 | 3.215 |
| No
reinforcement-uneven reinforcement | 0.442 | 0.611 | 1.556 | 0.284 | 8.531 |
| Maximum diameter of
MRI1 tumor, cm | 0.460 |
<0.001a | 0.631 | 0.531 | 0.751 |
| MRI1 maximum
diameter of axillary lymph nodes, cm | 0.067 | 0.682 | 0.935 | 0.679 | 1.288 |
| MRI1 ADC1
(×10−3 mm2/sec) | 1.904 | 0.001a | 6.710 | 2.239 | 20.115 |
| MRI1 TIC1 type |
|
|
|
|
|
| Inflow
to inflow-inflow to platform | 0.447 | 0.242 | 0.639 | 0.302 | 1.352 |
| Inflow
to inflow-inflow to outflow | 1.678 |
<0.001a | 0.187 | 0.087 | 0.401 |
| MRI1 reinforcement
type |
|
|
|
|
|
| No
reinforcement-reinforcement | −0.036 | 0.935 | 0.964 | 0.401 | 2.316 |
| No
reinforcement-uneven reinforcement | −0.442 | 0.632 | 0.643 | 0.106 | 3.913 |
| Maximum diameter of
MRI2 tumor, cm | 0.489 |
<0.001a | 0.613 | 0.499 | 0.754 |
| MRI2 maximum
diameter of axillary lymph nodes, cm | 0.127 | 0.636 | 0.880 | 0.520 | 1.491 |
| MRI2 ADC2
(×10−3 mm2/sec) | 4.516 |
<0.001a | 91.446 | 25.140 | 332.628 |
| MRI2 TIC2 |
|
|
|
|
|
| Inflow
to inflow-inflow to platform | 2.261 |
<0.001a | 0.104 | 0.055 | 0.198 |
| Inflow
to inflow-inflow to outflow | 2.767 |
<0.001a | 0.063 | 0.028 | 0.140 |
| MRI2 reinforcement
type |
|
|
|
|
|
| No
reinforcement-reinforcement | −0.008 | 0.984 | 0.992 | 0.444 | 2.213 |
| No
reinforcement-uneven reinforcement | −0.946 | 0.252 | 0.388 | 0.077 | 1.962 |
|
ΔADC1 | 1.127 | 0.019a | 3.085 | 1.200 | 7.934 |
|
ΔADC2 | 3.347 |
<0.001a | 28.406 | 9.279 | 86.964 |
|
ΔADC3 | 2.339 |
<0.001a | 10.370 | 3.564 | 30.175 |
| SF |
|
|
|
|
|
|
SF0 | 0.001 | 0.025a | 0.999 | 0.998 | 1.000 |
|
SF1 | 0.000 | 0.446 | 1.000 | 0.998 | 1.001 |
|
SF2 | 0.000 | 0.810 | 1.000 | 0.999 | 1.001 |
| CEA |
|
|
|
|
|
|
CEA-0 | 0.004 | 0.039a | 0.957 | 0.918 | 0.998 |
|
CEA-1 | 0.272 |
<0.001a | 0.762 | 0.673 | 0.864 |
|
CEA-2 | 0.336 |
<0.001a | 0.715 | 0.594 | 0.861 |
| AFP |
|
|
|
|
|
|
AFP-0 | 0.117 | 0.036a | 1.124 | 1.007 | 1.253 |
|
AFP-1 | 0.027 | 0.659 | 0.973 | 0.861 | 1.099 |
|
AFP-2 | 0.125 | 0.043a | 0.883 | 0.782 | 0.996 |
| CA125 |
|
|
|
|
|
|
CA125-0 | 0.004 | 0.641 | 1.004 | 0.986 | 1.023 |
|
CA125-1 | 0.013 | 0.417 | 0.987 | 0.958 | 1.018 |
|
CA125-2 | 0.029 | 0.129 | 0.971 | 0.935 | 1.008 |
| CA153 |
|
|
|
|
|
|
CA153-0 | 0.004 | 0.678 | 0.996 | 0.979 | 1.014 |
|
CA153-1 | 0.015 | 0.134 | 0.985 | 0.967 | 1.005 |
|
CA153-2 | 0.043 | 0.005a | 0.958 | 0.930 | 0.987 |
| CA199 |
|
|
|
|
|
|
CA199-0 | 0.020 | 0.143 | 1.020 | 0.993 | 1.048 |
|
CA199-1 | 0.003 | 0.803 | 1.003 | 0.977 | 1.030 |
|
CA199-2 | 0.005 | 0.730 | 1.005 | 0.979 | 1.031 |
| CA242 |
|
|
|
|
|
|
CA242-0 | 0.034 | 0.107 | 1.034 | 0.993 | 1.077 |
|
CA242-1 | 0.025 | 0.243 | 1.026 | 0.983 | 1.070 |
|
CA242-2 | 0.011 | 0.544 | 1.011 | 0.975 | 1.050 |
| CA724 |
|
|
|
|
|
|
CA724-0 | 0.004 | 0.773 | 1.004 | 0.976 | 1.033 |
|
CA724-1 | 0.001 | 0.916 | 1.001 | 0.981 | 1.021 |
|
CA724-2 | 0.001 | 0.956 | 1.001 | 0.982 | 1.019 |
Multivariate logistic regression
analysis of retrospective data
Variables identified as significant in the
univariate logistic regression analysis of retrospective data were
engaged in the multivariate logistic regression analysis. To reduce
the omission of potentially important factors due to interaction,
variables with P<0.10 were identified as predictors. Prior to
multivariate logistic regression, multicollinearity among the
included variables was assessed using variance inflation factors
(VIFs). All VIF values were <5, indicating no significant
collinearity. The results showed that pCR was more likely to occur
in patients with negative PR, higher ADC2 at MRI2, inflow-inflow
type in TIC2, greater ΔADC2, greater ΔADC3, and lower CEA-0, CEA-1
and CA153-2 (Table VIII).
| Table VIII.Multivariate logistic regression
analysis. |
Table VIII.
Multivariate logistic regression
analysis.
|
| Multivariate
logistic regression analysis |
|---|
|
|
|
|---|
|
Characteristics | β | P-value | OR | 95% CI |
|---|
| TNM stage |
|
|
|
|
|
|
2A-2B | 0.257 | 0.714 | 1.293 | 0.328 | 5.099 |
|
2A-3A | 0.124 | 0.880 | 1.132 | 0.229 | 5.597 |
|
2A-3B | 0.008 | 0.993 | 1.008 | 0.147 | 6.924 |
|
2A-3C | 0.240 | 0.858 | 1.272 | 0.091 | 17.698 |
| ER status | 0.390 | 0.464 | 0.677 | 0.238 | 1.924 |
| PR status | 0.962 | 0.095a | 0.382 | 0.124 | 1.183 |
| Maximum diameter of
MRI0 tumor, cm | 0.236 | 0.291 | 1.267 | 0.816 | 1.965 |
| Maximum diameter of
MRI1 tumor, cm | 0.359 | 0.188 | 0.699 | 0.410 | 1.192 |
| MRI1 ADC1
(×10−3 mm2/sec) | 0.753 | 0.685 | 2.124 | 0.056 | 80.899 |
| MRI1 TIC1 type |
|
|
|
|
|
| Inflow
to inflow-inflow to platform | 0.071 | 0.913 | 1.074 | 0.300 | 3.842 |
| Inflow
to inflow-inflow to outflow | 1.134 | 0.856 | 0.857 | 0.207 | 3.698 |
| Maximum diameter of
MRI2 tumor, cm | 0.179 | 0.515 | 1.196 | 0.698 | 2.052 |
| MRI2 ADC2
(×10−3 mm2/sec) | 2.122 | 0.023a | 8.349 | 1.344 | 51.856 |
| MRI2 TIC2 type |
|
|
|
|
|
| Inflow
to inflow-inflow to platform | 2.157 |
<0.001a | 0.116 | 0.038 | 0.351 |
| Inflow
to inflow-inflow to outflow | 3.184 |
<0.001a | 0.041 | 0.009 | 0.190 |
| ΔADC1 (%) | 0.360 | 0.833 | 0.697 | 0.025 | 19.823 |
| ΔADC2 (%) | 3.347 | 0.023a | 28.406 | 9.279 | 86.964 |
| ΔADC3 (%) | 2.339 |
<0.001a | 10.370 | 3.564 | 30.175 |
| SF |
|
|
|
|
|
|
SF-0 | 0.001 | 0.197 | 0.999 | 0.998 | 1.000 |
| CEA |
|
|
|
|
|
|
CEA-0 | 0.004 | 0.078a | 0.957 | 0.918 | 0.998 |
|
CEA-1 | 0.272 | 0.039a | 0.762 | 0.673 | 0.864 |
|
CEA-2 | 0.336 | 0.177 | 0.715 | 0.594 | 0.861 |
| AFP |
|
|
|
|
|
|
AFP-0 | 0.027 | 0.546 | 0.973 | 0.861 | 1.099 |
|
AFP-2 | 0.125 | 0.201 | 0.883 | 0.782 | 0.996 |
| CA153 |
|
|
|
|
|
|
CA153-2 | 0.043 | 0.040a | 0.958 | 0.930 | 0.987 |
Development and evaluation of the
nomogram of the prediction model
Construction of the pCR prediction nomogram
Based on the multivariate logistic regression
analysis of the retrospective data, eight predictive factors were
selected from all included variables. The multivariate prediction
model was visualized, and the nomogram was constructed using R
software (Fig. 2).
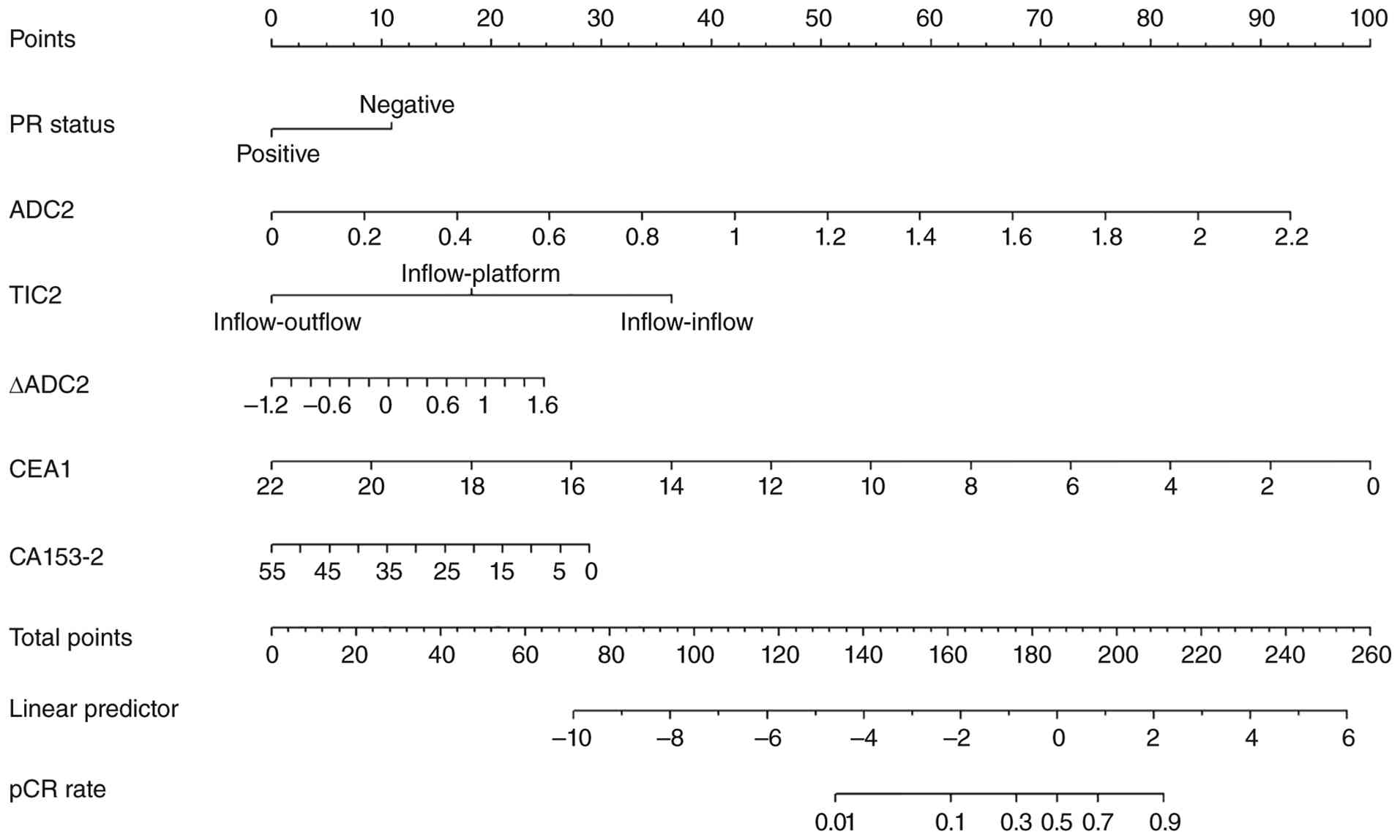 | Figure 2.Nomogram to predict the probability
of pCR in human epidermal growth factor receptor 2-positive breast
cancer after neoadjuvant targeted therapy A predictive model based
on the multivariate analysis of the present study from the
retrospectively collected data. According to the nomogram, each
screened predictor was projected to the scale above the nomogram to
calculate the individual score of each factor, and the total score
was calculated after adding the individual scores. The
corresponding prediction probability was then obtained according to
the relationship between the total score and pCR in the nomogram.
pCR, pathological complete response; PR, progesterone receptor;
ADC, apparent diffusion coefficient; TIC, time intensity curve;
CEA, carcinoembryonic antigen; CA, carbohydrate antigen; ADC2, ADC
after completion of neoadjuvant therapy before surgery; TIC2, TIC
type after completion of neoadjuvant therapy before surgery; ΔADC2,
calculated change in ADC value (ADC2 vs. ADC0); CEA1, CEA after the
first cycle of targeted therapy; CA153-2, CA153 after completion of
NAT before surgery. |
Internal validation of the pCR
prediction model
The nomogram was internally validated using the
bootstrap method. The Hosmer-Lemeshow test indicated good fit of
the prediction model (P=0.453). A calibration curve was then
constructed according to the relationship between the predicted
results and the actual outcomes, showing close agreement between
the model performance curve and the diagonal reference line. This
indicated good consistency between the predicted and observed pCR
outcomes (Fig. 3).
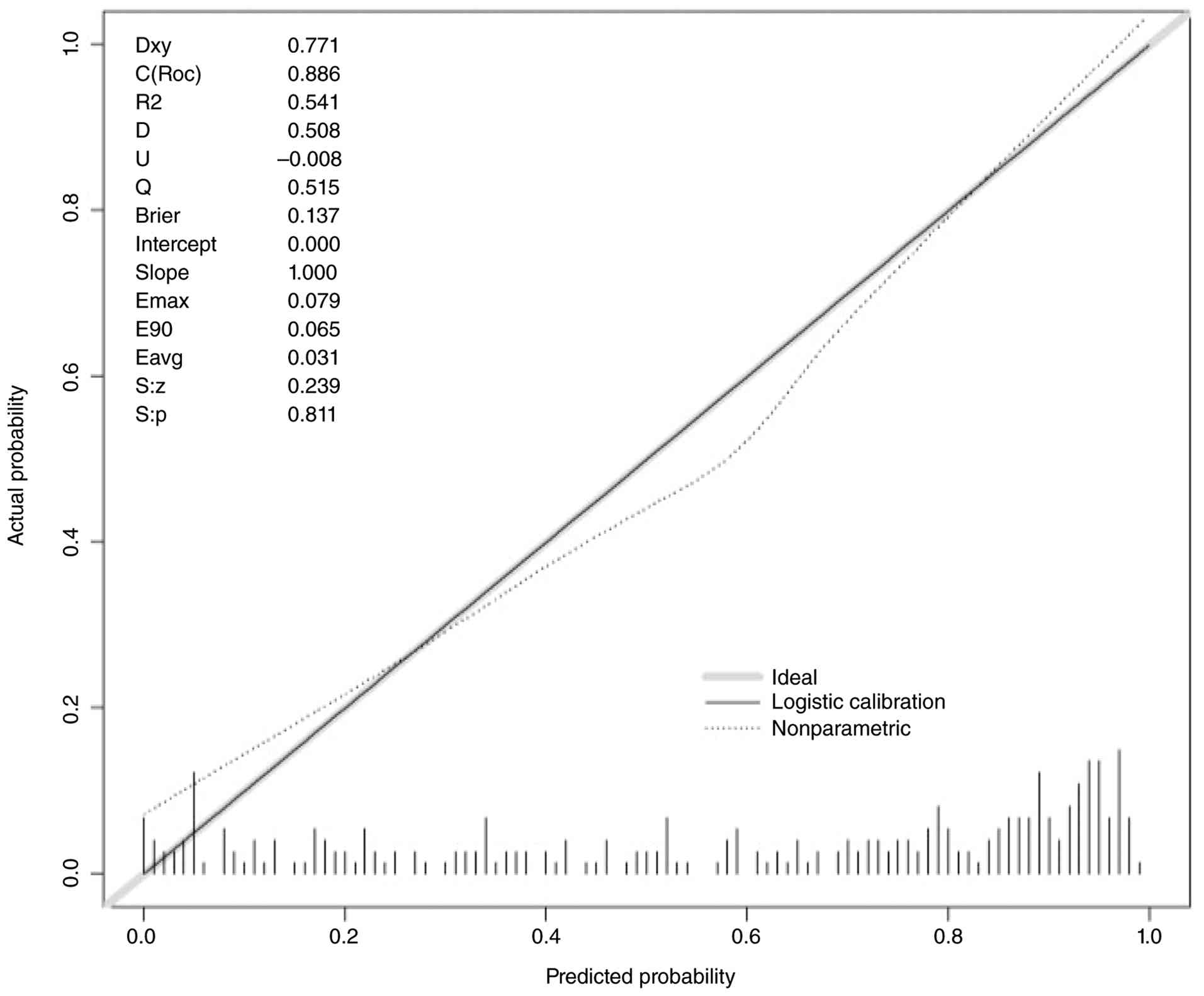 | Figure 3.Calibration curve of the constructed
predictive model from internal validation data. As part of the
internal validation, the calibration curve was drawn according to
the relationship between the prediction results and the actual
situation. The calibration curve showed that the dotted line and
diagonal line of the model were coincident, indicating that the
nomogram had good consistency between the prediction of pCR and the
actual occurrence of pCR, and the prediction ability was good. The
following internal validation metrics were obtained: Somer's Dxy
rank correlation was 0.771; concordance index (C-index) was 0.886
(indicating good discrimination); R2 was 0.541 (indicating moderate
explanatory power); Brier score was 0.137 (<0.25, indicating
acceptable overall prediction accuracy); calibration intercept was
0.000 (ideal value was 0, indicating no systematic over- or
under-estimation); calibration slope was 1.000 (ideal value was 1,
indicating perfect calibration slope); maximum calibration error
(Emax) was 0.079; 90th percentile calibration error (E90) was
0.065; mean absolute calibration error (Eavg) was 0.031 (all
indicating small prediction errors). The Spiegelhalter's Z-test
statistic (S:z) was 0.239 (P=0.811, S:p), indicating no significant
deviation from perfect calibration. Collectively, these metrics
demonstrate that the nomogram has good calibration and predictive
performance. pCR, pathological complete response. |
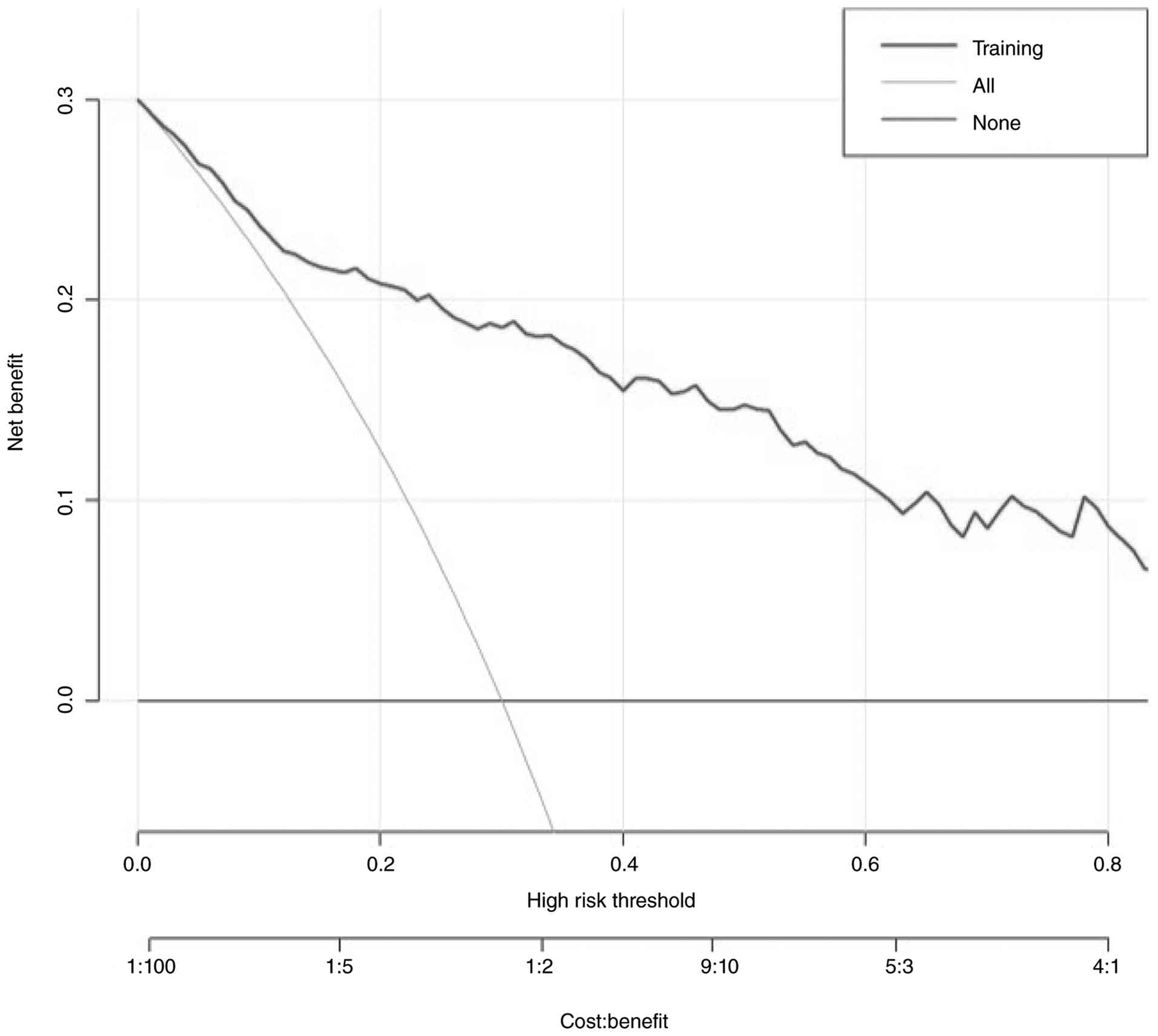
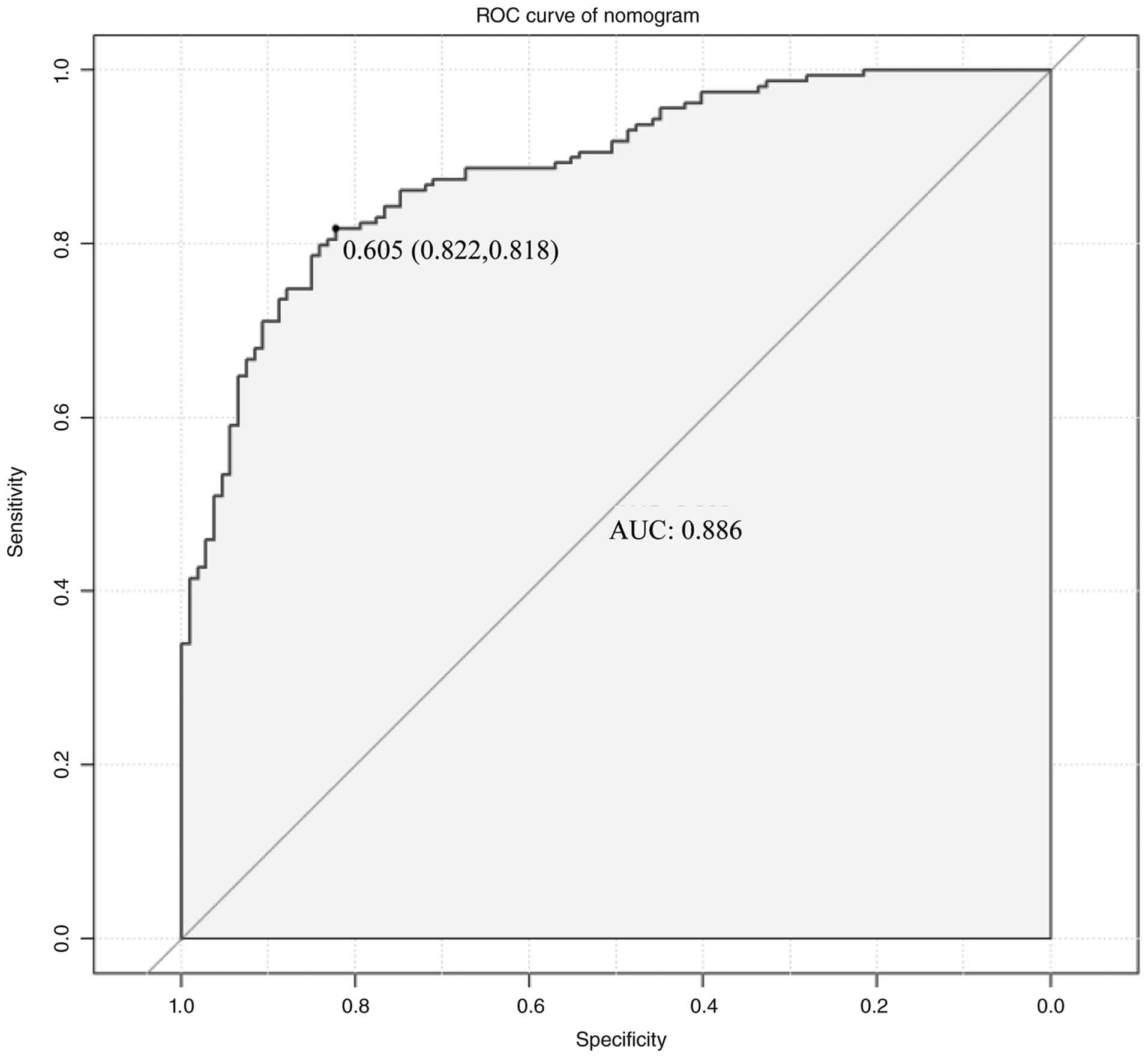
The DCA curve further showed that the prediction
model provided net benefit across a threshold probability range of
0–80% (Fig. 4). ROC analysis
yielded an AUC of 0.886, with an optimal cut-off value of 0.605,
sensitivity of 0.822 and specificity of 0.818, indicating good
predictive performance and accuracy (Fig. 5).
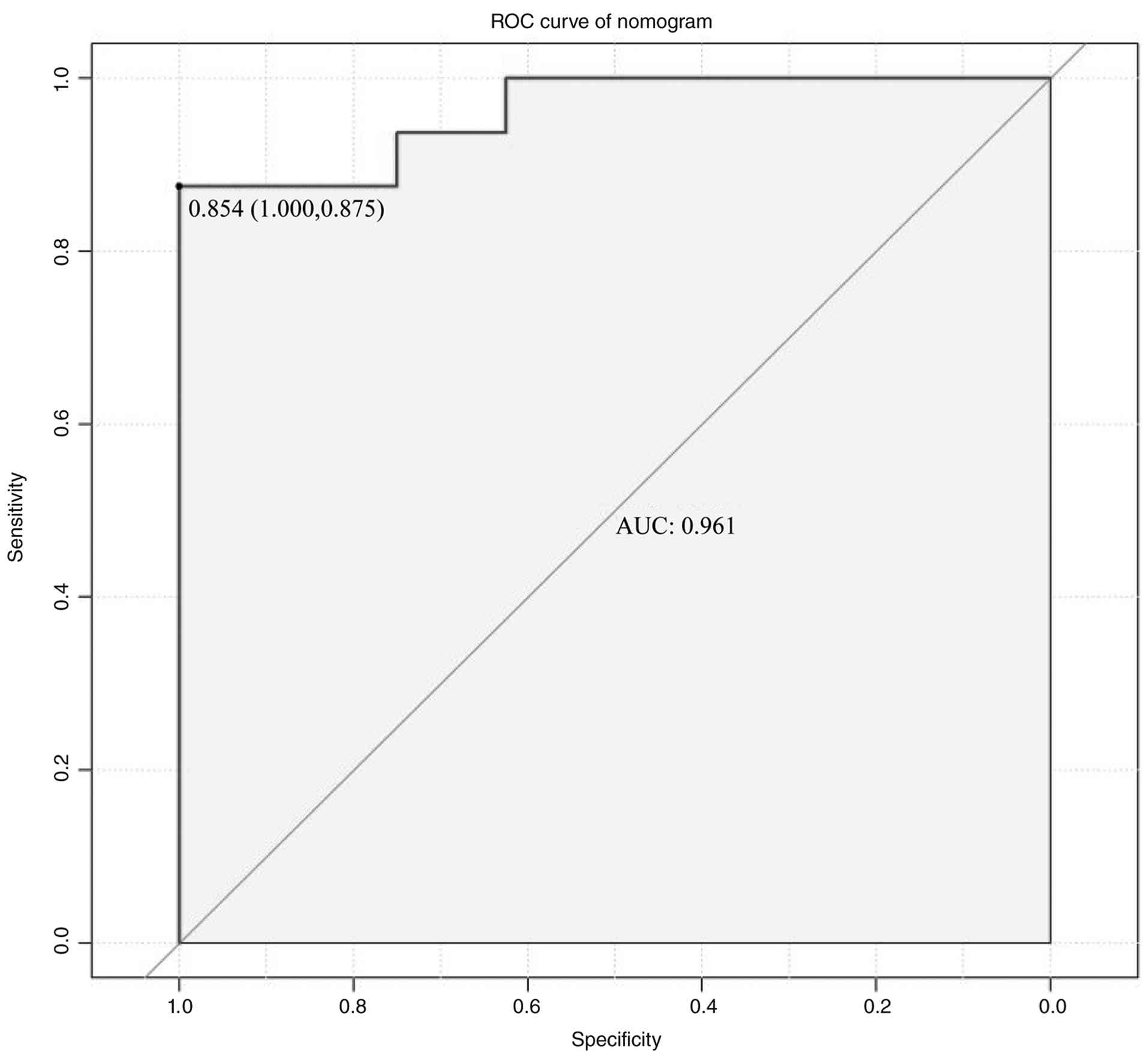
External validation of the pCR
prediction model
A total of 24 patients with HER2-positive BC were
prospectively included as the external validation cohort, and an
ROC curve was generated for external validation. The AUC value was
0.961 (P=0.001), with an optimal cut-off value of 0.854,
sensitivity of 1.000 and specificity of 0.875, indicating good
predictive performance and high accuracy in the external validation
cohort (Fig. 6).
Discussion
pCR is an important endpoint in the management of
HER2-positive BC, and pCR rates after first-line NAT scheme are
relatively high in patients with this subtype (22,23).
Previous studies, including the NeoSphere trial, demonstrated that
patients achieving a pCR had improved 5-year progression-free
survival rates compared with those without a pCR (85 vs. 76%; HR,
0.54; 95% CI, 0.29–1.00) (9).
Similar findings were reported in the PEONY trial, in which the pCR
group showed a higher 5-year disease-free survival rate than the
non-pCR group (91.5 vs. 82.1%) (24). These findings have led some
investigators to propose pCR as a surrogate endpoint for prognosis
in patients with HER2-positive BC (25–27).
However, improving outcomes in HER2-positive BC requires not only
advances in targeted therapies but also accurate monitoring of
treatment response. Therefore, there is an increasing need to
develop reliable predictive tools, such as nomograms, based on
clinically available auxiliary examination indicators to estimate
pCR.
In the present study, a nomogram for pCR
incorporating MRI features and tumor markers was developed to
predict pCR. The model indicated that pCR was more likely to occur
when PR was negative, ADC2 was higher, TIC2 was of inflow-inflow
type, ΔADC2 and ΔADC3 were larger, and CEA-0, CEA-1 and CA153-2
were lower. The further internal and external validation confirmed
that the nomogram had good predictive performance for pCR patients
with HER2-positive BC.
HR status plays an important part in the prognosis,
diagnosis and treatment of BC (28). HR status determines the molecular
subtype and guides the use of endocrine therapy, and is also
associated with response to NAT (29–30).
In the present study, PR status was associated with neoadjuvant
pCR, with a higher probability of achieving a pCR observed in
patients with PR-negative tumors (OR, 0.543; 95% CI, 0.330–0.896;
P=0.017). Previous studies have similarly reported that patients
with the HR-negative subtype are more likely to achieve a pCR than
their HR-positive counterparts (P=0.011) (31), particularly in younger patients with
HER2-positive BC and lower tumor burden who receive standardized
HER2-targeted therapy (32).
Potential mechanisms include the role of PR in regulating growth
factor-related signaling pathways and interactions between HR and
HER2 signaling during dual-target therapy (33), as well as HR-mediated promotion of
tumor cell proliferation and potential induction of trastuzumab
resistance (34).
In recent years, the role of imaging data in
predicting the response to NAT has also been increasingly
recognized, and MRI is considered one of the most accurate imaging
modalities for the evaluation of breast lesions (35). In the present study, both
morphological and functional imaging parameters, including the
maximum tumor diameter, maximum axillary lymph node diameter, TIC
type and ADC value, were assessed at three time points. Before NAT,
the maximum tumor diameter was associated with prognosis, with
larger tumors diameter showing a lower probability of achieving a
pCR. This finding is consistent with those of a previous study
(36) and further supports the
importance of tumor size in predicting NAT efficacy and informing
surgical planning (37).
The TIC reflects changes in contrast enhancement on
DCE-MRI. Malignant lesions typically show higher vascular density,
greater vascular permeability and a larger extravascular space,
resulting in a more rapid contrast agent flow rate. According to
the Kulh criteria (38), malignant
tumors usually present with a type III curve, namely an
inflow-outflow pattern. In the present study, the predominant TIC
pattern at baseline was inflow-outflow in both the pCR and the
non-pCR groups. However, after NTT, as the tumor gradually
regressed or disappeared, the vascular characteristics of the tumor
also changed, accompanied by conversion of TIC type. The pCR group
showed earlier and more marked downgrading of TIC types than the
non-pCR group. After one cycle of NTT, the predominant TIC type in
the pCR group changed to the inflow-plateau type (51.6%), and after
the final cycle, it further changed to the inflow-inflow type
(74.53%). By contrast, in the non-pCR group, the predominant TIC
type changed only after the last cycle of NTT, shifting from
inflow-outflow at the first two time points to inflow-plateau at
the final assessment. Previous studies have similarly shown that,
after NAT, TIC patterns in patients with a histologically
significant response tend to show downgrading, whereas little or no
such change is observed in non-responders (39,40),
which is consistent with the present findings.
Malignant tumors generally have high cellular
density, which restricts the movement of water molecules within the
tissue (41). As NAT progresses,
tumor cellularity decreases and water diffusion increases, which
can be quantitatively reflected by the ADC value derived from DWI
(42). Since ADC values differ
significantly between benign and malignant lesions, changes in ADC
value may also serve as an indirect indicator of treatment response
(13). In the present study, ADC
values were higher in the pCR group than those in the non-pCR group
at all three MRI time points, and this difference was already
evident after the initiation of NTT. In addition, changes in ADC
from baseline were greater in the pCR group, and larger ΔADC2 and
ΔADC3 values were associated with a higher probability of achieving
a pCR after surgery. Previous studies have similarly shown that
increases in ADC during NAT have predictive value for pCR (43,44).
However, Park et al (13) reported that patients with low ADC
values before NAT had a better response to chemotherapy, which
differs from the present findings. This discrepancy may be related
to the differences in the included study populations. Previous
studies of other tumors types have suggested that poor perfusion of
antitumor drugs within necrotic tissue may reduce the efficacy of
NAT (45). After treatment, reduced
cellular density in necrotic tissue may lessen restriction of water
molecule movement, thereby leading to higher ADC values (12,45).
Accordingly, Park et al (13) suggested that low ADC values may
reflect breast masses with less necrotic tissue and higher cellular
density in patients who respond better to NAT. By contrast, it is
possible that the tumor cell density in the present cohort was
lower than that in the non-pCR group before NAT, resulting in less
restricted water diffusion and therefore higher baseline ADC
values. However, this possibility was not examined by pathological
or cytomolecular analyses in the present study, and further basic
investigations are needed to clarify this issue.
In addition to imaging data, hematological markers
are often used to evaluate cancer occurrence, progression,
treatment efficacy and prognosis (46). However, due to their high
sensitivity but limited specificity, single markers are rarely used
alone as predictors and are more commonly interpreted in
combination with other clinical indicators (28,47,48).
In the present study, CEA-0, CEA-1 and CA153-2 were identified as
predictive factors for NAT response in HER2-positive BC. CEA is a
commonly used broad-spectrum tumor marker in clinical practice
(15), whereas CA153 is a
traditional marker for BC, with a reported positive rate of
22.5–49.2% in these patients (49).
Serum CEA and CA153 levels are higher in malignant than in benign
tumors (50), and their
concentrations are positively associated with the degree of
malignancy (19). Liu et al
(51) compared CEA and CA153 levels
before and after NAT in patients with HER2-positive BC treated with
or without trastuzumab. The study found that CEA and CA153 levels
were significantly lower in the trastuzumab group than in the
non-trastuzumab group, whereas treatment efficacy and prognosis
were better in the trastuzumab group (52). Therefore, CEA and CA153 levels may
reflect tumor burden in patients with BC, and reductions in tumor
burden after treatment may be indirectly reflected by changes in
these markers. The present findings were generally consistent with
this pattern, as CEA levels in both groups showed a continuous
decreasing trend from baseline to after the first targeted therapy
and then to the last targeted therapy.
A major strength of the present study is the
comprehensive integration of multiple types of clinical data. In
addition, rather than relying on cross-sectional data from a single
time point, this study was based on dynamic longitudinal
observation, allowing more comprehensive use of clinical
examination results throughout treatment. The model may help
predict whether patients with HER2-positive BC are likely to
achieve pCR before surgery during the NAT course. It may also
provide a reference for clinicians in treatment planning, including
adjustment of NAT duration, selection of surgical timing and
approach, and formulation of postoperative adjuvant
chemoradiotherapy strategies.
Nevertheless, several limitations should be
acknowledged. First, the present study was based on a single-center
cohort, and the nomogram was not validated in a larger multicenter
external cohort. Second, the largest solid component of the tumor
was selected as the study variable, which may not fully represent
the entire lesion, as the whole tumor was not measured. Further
multi-center studies with larger patient cohorts are needed to
validate the predictive performance of this nomogram. In addition,
whole-tumor volumetric segmentation or multi-region sampling should
be adopted to capture the full heterogeneity of the lesion and to
improve the accuracy of pCR prediction based on tumor imaging.
In conclusion, the nomogram developed in the present
study, based on PR, ADC2, TIC2, ΔADC2, ΔADC3, CEA-0, CEA-1 and
CA153-2, may help predict pCR in patients with HER2-positive BC and
may also support individualized treatment decision-making to some
extent. By integrating pathological data, imaging parameters and
hematological markers obtained during NAT, this combined model may
predict postoperative pathological response and provide useful
information for prognostic evaluation and subsequent individualized
treatment planning in clinical practice. However, this study has
several limitations, including the single-center design and the
relatively small sample size. Therefore, further validation in
large-scale multicenter cohorts is warranted to optimize the model,
and independent cohort studies with rigorous validation are
required before clinical application can be considered.
Acknowledgements
Not applicable.
Funding
The present study was financially supported by the First-Class
Discipline Team of Kunming Medical University (Kunming Medical
University Breast Cancer Precision and Translational Medicine
Research Team) (grant no. CXTD202211) and the National Natural
Scientific Foundation of China (grant no. 82160532).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
KZ, ZL, JW and SH conceived and designed the study.
KZ, ZL, CW, JW and SZ acquired the data, and KZ, RG and JL
performed the statistical analysis and interpreted the data. DC,
YT, YD and JN contributed to data interpretation and provided
critical intellectual input during manuscript revision. CW, JW and
SZ also provided essential study materials and patient data. KZ and
SH drafted the manuscript, and all authors (including DC, YT, YD,
JN, RG, JL, CW, JW, SZ, ZL and WJ) critically revised it for
important intellectual content. WJ, NJ and SH supervised the entire
study, obtained funding and were responsible for the overall
integrity of the work. KZ, WJ, SH and NJ confirm the authenticity
of all the raw data. All authors have read and approved the final
manuscript and agree to be accountable for all aspects of the
work.
Ethics approval and consent to
participate
This study involving human participants was reviewed
and approved by the Independent Ethics Committee of Yunnan Cancer
Hospital, The Third Affiliated Hospital of Kunming Medical
University (Kunming, China; approval no. KYLX2022182). The patients
provided written informed consent to participate in this study.
Patient consent for publication
Written informed consent was obtained from the
individual(s) for the publication of any potentially identifiable
images or data included in this article.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
AC
|
anthracyclines + cyclophosphamide
|
|
ADC
|
apparent diffusion coefficient
|
|
AFP
|
α-fetoprotein
|
|
AJCC
|
American Joint Committee on Cancer
|
|
AUC
|
area under the ROC curve
|
|
BC
|
breast cancer
|
|
CA
|
carbohydrate antigen
|
|
CEA
|
carcinoembryonic antigen
|
|
DCA
|
decision curve analysis
|
|
DCE-MRI
|
dynamic contrast-enhanced magnetic
resonance imaging
|
|
DWI
|
diffusion-weighted imaging
|
|
ER
|
estrogen receptor
|
|
HER2
|
human epidermal growth factor receptor
2
|
|
HP
|
Herceptin (trastuzumab) +
pertuzumab
|
|
NAT
|
neoadjuvant therapy
|
|
NTT
|
neoadjuvant targeted therapy
|
|
pCR
|
pathological complete response
|
|
PR
|
progesterone receptor
|
|
ROC
|
receiver operating characteristic
|
|
SF
|
serum ferritin
|
|
TIC
|
time intensity curve
|
|
VIF
|
variance inflation factor
|
References
|
1
|
Bray F, Laversanne M, Sung H, Ferlay J,
Siegel RL, Soerjomataram I and Jemal A: Global cancer statistics
2022: GLOBOCAN estimates of incidence and mortality worldwide for
36 cancers in 185 countries. CA Cancer J Clin. 74:229–263.
2024.PubMed/NCBI
|
|
2
|
Harbeck N and Gnant M: Breast cancer.
Lancet. 389:1134–1150. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Traub L, Thill M and Nitschmann S: The
20-year results of 5-year hormone therapy in breast cancer: Early
Breast Cancer Trialists' Collaborative Group (EBCTCG). Internist
(Berl). 56:410–412. 2018.(In German). View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Spring LM, Fell G, Arfe A, Sharma C,
Greenup R, Reynolds KL, Smith BL, Alexander B, Moy B, Isakoff SJ,
et al: Complete response after neoadjuvant chemotherapy and impact
on breast cancer recurrence and survival: A comprehensive
Meta-analysis. Clin Cancer Res. 26:2838–2848. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Haque W, Verma V, Hatch S, Suzanne
Klimberg V, Brian Butler E and Teh BS: Response rates and
pathologic complete response by breast cancer molecular subtype
following neoadjuvant chemotherapy. Breast Cancer Res Treat.
170:559–567. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Blanco SA, Yébenes L, Berjón A and
Hardisson D: Evaluation of pathological response to neoadjuvant
chemotherapy in breast cancer: Correlation with molecular
phenotype. Rev Esp Patol. 54:8–16. 2021.(In Spanish). PubMed/NCBI
|
|
7
|
Harbeck N: Neoadjuvant and adjuvant
treatment of patients with HER2-positive early breast cancer.
Breast. 62 (Suppl 1):S12–S16. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Gianni L, Eiermann W, Semiglazov V, Lluch
A, Tjulandin S, Zambetti M, Moliterni A, Vazquez F, Byakhov MJ,
Lichinitser M, et al: Neoadjuvant and adjuvant trastuzumab in
patients with HER2-positive locally advanced breast cancer (NOAH):
Follow-up of a randomised controlled superiority trial with a
parallel HER2-negative cohort. Lancet Oncol. 15:640–647. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gianni L, Pienkowski T, Im YH, Tseng LM,
Liu MC, Lluch A, Starosławska E, de la Haba-Rodriguez J, Im SA,
Pedrini JL, et al: 5-year analysis of neoadjuvant pertuzumab and
trastuzumab in patients with locally advanced, inflammatory, or
early-stage HER2-positive breast cancer (NeoSphere): A multicentre,
open-label, phase 2 randomised trial. Lancet Oncol. 17:791–800.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gianni L, Pienkowski T, Im YH, Roman L,
Tseng LM, Liu MC, Lluch A, Staroslawska E, de la Haba-Rodriguez J,
Im SA, et al: Efficacy and safety of neoadjuvant pertuzumab and
trastuzumab in women with locally advanced, inflammatory, or early
HER2-positive breast cancer (NeoSphere): A randomised multicentre,
open-label, phase 2 trial. Lancet Oncol. 13:25–32. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Baltzer A, Dietzel M, Kaiser CG and
Baltzer PA: Combined reading of contrast enhanced and diffusion
weighted magnetic resonance imaging by using a simple sum score.
Eur Radiol. 26:884–891. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
van Ramshorst MS, Loo CE, Groen EJ,
Winter-Warnars GH, Wesseling J, van Duijnhoven F, Peeters MTV and
Sonke GS: MRI predicts pathologic complete response in
HER2-positive breast cancer after neoadjuvant chemotherapy. Breast
Cancer Res Treat. 164:99–106. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Park SH, Moon WK, Cho N, Song IC, Chang
JM, Park IA, Han W and Noh DY: Diffusion-weighted MR imaging:
Pretreatment prediction of response to neoadjuvant chemotherapy in
patients with breast cancer. Radiology. 257:56–63. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kim Y, Kim SH, Song BJ, Kang BJ, Yim KI,
Lee A and Nam Y: Early prediction of response to neoadjuvant
chemotherapy using dynamic Contrast-enhanced MRI and ultrasound in
breast cancer. Korean J Radiol. 19:682–691. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Duffy MJ, Walsh S, McDermott EW and Crown
J: Biomarkers in breast cancer: Where are we and where are we
going? Adv Clin Chem. 71:1–23. 2015.PubMed/NCBI
|
|
16
|
Nicholson BD, Shinkins B, Pathiraja I,
Roberts NW, James TJ, Mallett S, Perera R, Primrose JN and Mant D:
Blood CEA levels for detecting recurrent colorectal cancer.
Cochrane Database Syst Rev. 2015:CD0111342015.PubMed/NCBI
|
|
17
|
Grunnet M and Sorensen JB:
Carcinoembryonic antigen (CEA) as tumor marker in lung cancer. Lung
Cancer. 76:138–143. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Shibata C, Nakano T, Yasumoto A, Mitamura
A, Sawada K, Ogawa H, Miura T, Ise I, Takami K, Yamamoto K and
Katayose Y: Comparison of CEA and CA19-9 as a predictive factor for
recurrence after curative gastrectomy in gastric cancer. BMC Surg.
22:2132022. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wang BT and Wang XF: Application value of
serum tumor markers combined with dynamic detection in the
diagnosis and monitoring of breast cancer. Med Innov China.
3:66–11. 2021.(In Chinese).
|
|
20
|
Dowling GP, Keelan S, Toomey S, Daly GR,
Hennessy BT and Hill ADK: Review of the status of neoadjuvant
therapy in HER2-positive breast cancer. Front Oncol.
13:10660072023. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Amin MB, Edge SB, Greene GL, Byrd DR,
Brookland RK, Washington MK, Gershenwald JE, Compton CC, Vega LRM
and Gress DM: AJCC cancer staging manual. 8th edition. New York,
NY: Springer; 2017
|
|
22
|
Loibl S and Gianni L: HER2-positive breast
cancer. Lancet. 389:2415–2429. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Cortazar P, Zhang L, Untch M, Mehta K,
Costantino JP, Wolmark N, Bonnefoi H, Cameron D, Gianni L,
Valagussa P, et al: Pathological complete response and long-term
clinical benefit in breast cancer: The CTNeoBC pooled analysis.
Lancet. 384:164–172. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Huang L, Pang D, Yang H, Li W, Wang S, Cui
S, Liao N, Wang Y, Wang C, Chang YC, et al: Neoadjuvant-adjuvant
pertuzumab in HER2-positive early breast cancer: Final analysis of
the randomized phase III PEONY trial. Nat Commun. 15:21532024.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kong X, Moran MS, Zhang N, Haffty B and
Yang Q: Meta-analysis confirms achieving pathological complete
response after neoadjuvant chemotherapy predicts favourable
prognosis for breast cancer patients. Eur J Cancer. 47:2084–2090.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Earl H, Provenzano E, Abraham J, Dunn J,
Vallier AL, Gounaris I and Hiller L: Neoadjuvant trials in early
breast cancer: Pathological response at surgery and correlation to
longer term outcomes-what does it all mean? BMC Med. 13:2342015.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Provenzano E, Bossuyt V, Viale G, Cameron
D, Badve S, Denkert C, MacGrogan G, Penault-Llorca F, Boughey J,
Curigliano G, et al: Standardization of pathologic evaluation and
reporting of postneoadjuvant specimens in clinical trials of breast
cancer: Recommendations from an international working group. Mod
Pathol. 28:1185–201. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Duffy MJ, Harbeck N, Nap M, Molina R,
Nicolini A, Senkus E and Cardoso F: Clinical use of biomarkers in
breast cancer: Updated guidelines from the European Group on Tumor
Markers (EGTM). Eur J Cancer. 75:284–298. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Houssami N, Macaskill P, von Minckwitz G,
Marinovich ML and Mamounas E: Meta-analysis of the association of
breast cancer subtype and pathologic complete response to
neoadjuvant chemotherapy. Eur J Cancer. 48:3342–3354. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Park C, Park K, Kim J, Sin Y, Park I, Cho
H, Yang K, Bae BN, Kim KW, Ahn S, et al: Prognostic values of
negative estrogen or progesterone receptor expression in patients
with luminal B HER2-negative breast cancer. World J Surg Oncol.
14:2442016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Yang QZ, Lv YL, Mu WM and Li Y: Effect of
hormone receptor status on Her-2 positive breast cancer. Chin J Med
Sci. 4:15–19. 2022.(In Chinese).
|
|
32
|
Li JL and Zhu DM: The Value of TAP Content
in Peripheral Blood in Predicting the Efficacy of Neoadjuvant
Chemotherapy for Her-2 Positive Breast Cancer. J Jinzhou Med Univ.
6:51–55. 2022.(In Chinese).
|
|
33
|
McDermott MSJ, Canonici A, Ivers L, Browne
BC, Madden SF, O'Brien NA, Crown J and O'Donovan N: Dual inhibition
of IGF1R and ER enhances response to trastuzumab in HER2 positive
breast cancer cells. Int J Oncol. 50:2221–2228. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Luo Y and Huang J: New Mechanism of ER-α36
Mediating Trastuzumab Resistance in Breast Cancer. Med
Recapitulate. 27:1722–1727. 2021.(In Chinese).
|
|
35
|
Bitencourt AGV, Gibbs P, Rossi Saccarelli
C, Daimiel I, Lo Gullo R, Fox MJ, Thakur S, Pinker K, Morris EA,
Morrow M and Jochelson MS: MRI-based machine learning radiomics can
predict HER2 expression level and pathologic response after
neoadjuvant therapy in HER2 overexpressing breast cancer.
EBioMedicine. 61:1030422020. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Mermut O, Inanc B, Gursu RU, Arslan E,
Trabulus DC, Havare SB and Ulusan MB: Factors affecting
pathological complete response after neoadjuvant chemotherapy in
breast cancer: A single-center experience. Rev Assoc Med Bras
(1992). 67:845–850. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Wahl RL, Jacene H, Kasamon Y and Lodge MA:
From RECIST to PERCIST: Evolving Considerations for PET response
criteria in solid tumors. J Nucl Med. 50 (Suppl 1):122S–150S. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Kuhl CK, Mielcareck P, Klaschik S, Leutner
C, Wardelmann E, Gieseke J and Schild HH: Dynamic breast MR
imaging: Are signal intensity time course data useful for
differential diagnosis of enhancing lesions? Radiology.
211:101–110. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Xu HD and Zhang YQ: Evaluation of the
efficacy of neoadjuvant chemotherapy for breast cancer using
diffusion-weighted imaging and dynamic contrast-enhanced magnetic
resonance imaging. Neoplasma. 64:430–436. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Nie Y, He Y, Wang J, Zhang H and Su J: MRI
Images-Based evaluation of efficacy of neoadjuvant chemotherapy for
breast cancer and its effect on depression and immune function of
patients. Contrast Media Mol Imaging. 2022:86856802022. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Iima M, Honda M, Sigmund EE, Ohno
Kishimoto A, Kataoka M and Togashi K: Diffusion MRI of the breast:
Current status and future directions. J Magn Reson Imaging.
52:70–90. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Gao W, Guo N and Dong T:
Diffusion-weighted imaging in monitoring the pathological response
to neoadjuvant chemotherapy in patients with breast cancer: A
meta-analysis. World J Surg Oncol. 16:1452018. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Li XR, Cheng LQ, Liu M, Zhang YJ, Wang JD,
Zhang AL, Song X, Li J, Zheng YQ and Liu L: DW-MRI ADC values can
predict treatment response in patients with locally advanced breast
cancer undergoing neoadjuvant chemotherapy. Med Oncol. 29:425–431.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Hottat NA, Badr DA, Lecomte S,
Besse-Hammer T, Jani JC and Cannie MM: Value of diffusion-weighted
MRI in predicting early response to neoadjuvant chemotherapy of
breast cancer: Comparison between ROI-ADC and whole-lesion-ADC
measurements. Eur Radiol. 32:4067–4078. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Humphries PD, Sebire NJ, Siegel MJ and
Olsen ØE: Tumors in pediatric patients at diffusion-weighted MR
imaging: Apparent diffusion coefficient and tumor cellularity.
Radiology. 245:848–854. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Yilihamu Y, Wang L, Ma T, Zhao T, Wang Y
and Sun G: The effects of preoperative serum carcinoembryonic
antigen, cancer antigen 15-3 and cancer antigen 125 on the
prognosis of breast cancer patients with different molecular
subtypes. J Clin Med Res. 16:491–502. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Crosby D, Bhatia S, Brindle KM, Coussens
LM, Dive C, Emberton M, Esener S, Fitzgerald RC, Gambhir SS, Kuhn
P, et al: Early detection of cancer. Science. 375:eaay90402022.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Chen S, Zeng J, Gong K, Liu Y, Long S, Han
L and Luo D: A novel four-serum marker model for early detection
and therapeutic monitoring of breast cancer. Sci Rep. 16:6142025.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Xu SX, Huo QY, Zhang MY, Wei YH, Yang Y,
Ji JH, Zhang CF and Zhao BY: Clinical value of combined serum
CAl53, CEA, SF, CT and Hcy in the diagnosis of breast cancer. J Mol
Diagn Ther. 12:190–194. 2020.(In Chinese).
|
|
50
|
Wu B, Zhu H, Sha DH and Guo YT: Study on
diagnostic value of DWI combined with serum carbohydrate antigen
153, 125 and carcinoembryonic antigen in breast cancer. J Med
Imaging. 31:1326–1329. 13462021.(In Chinese).
|
|
51
|
Liu RJ: The Effect of Trastuzumab in the
Treatment of HER-2 Positive Advanced Breast Cancer and its Effect
on Serum CEA and CA153 Levels. J Med Inform. 34:125–127. 2021.(In
Chinese).
|
|
52
|
Tarighati E, Keivan H and Mahani H: A
review of prognostic and predictive biomarkers in breast cancer.
Clin Exp Med. 23:1–16. 2023.PubMed/NCBI
|