Introduction
Diffuse peritoneal mesothelioma (DPM) is a rare and
highly aggressive primary tumor, characterized by its invasive
nature, frequent misdiagnosis and poor prognosis (1–3). DPM
accounts for 7–30% of all mesothelioma cases, with marked
geographic variation in incidence. In the USA, ~15,000 new cases
are reported annually, while in China, the incidence increased from
2.14 to 3.14 per 106 between 2000 and 2013 (4,5). The
etiology of DPM is primarily associated with asbestos exposure;
however, only 33–50% of patients have a clear history of exposure.
Other contributing factors include physicochemical carcinogens,
chronic peritonitis, and genetic susceptibility, such as
BRCA1-associated protein 1 (BAP1) mutations (6,7). As
asbestos has not been completely banned in China, the incidence of
DPM may continue to increase in the future.
Most DPM is asymptomatic or non-specific in the
early stages, with insidious onset, and is diagnosed in the mid- to
late-stage, with a median time from symptom onset to diagnosis of
~4 months (8,9). The diversity of clinical
manifestations depends largely on the extent of tumor spread in the
abdominal cavity. The main clinical manifestations include
abdominal distension (41–86%) and abdominal pain (31–87%), and may
also include weight loss, abdominal masses, and, in some cases,
paraneoplastic syndromes. A definitive diagnosis of DPM requires a
histopathological examination. DPM etiology and pathogenesis remain
to be fully elucidated and current management involves
cytoreductive surgery (CRS) combined with hyperthermic
intraperitoneal chemotherapy (HIPEC) and systemic chemotherapy.
Patients treated with this therapy have improved 5-year overall
survival and progression-free survival (PFS) rates compared with
untreated patients (10–12). The present study reports a case of
DPM misdiagnosed as mesenteric panniculitis, detailing its clinical
course, highlighting the diagnostic challenges, presenting the
management outcomes and discussing the potential association with
occupational asphalt exposure.
Case report
Clinical presentation
A 54-year-old male highway maintenance worker with a
28-year history of occupational exposure to asphalt (1994–2022)
presented with a 2-month history of persistent upper-middle
abdominal pain and weight loss, and was admitted (The First
People's Hospital of Xiaoshan District, Hangzhou, China) in April
2022. The patient was responsible for repairing potholes and paving
road surfaces, and had daily contact with hot-mix (170±5°C)
modified asphalt. The patient did not wear workplace respiratory
protective equipment or protective gloves, resulting in the
inhalation of asphalt fumes via the respiratory tract and skin
contact with hot asphalt. The duration of exposure was long-term,
high-dose and unprotected, lasting for 4–6 h per day and ≥22
days/month. No asbestos testing was conducted in the patient's
workplace. The patient had no history of smoking or alcohol
consumption and no family history of hereditary cancer. The medical
history included a laparoscopic appendectomy in November 2019. The
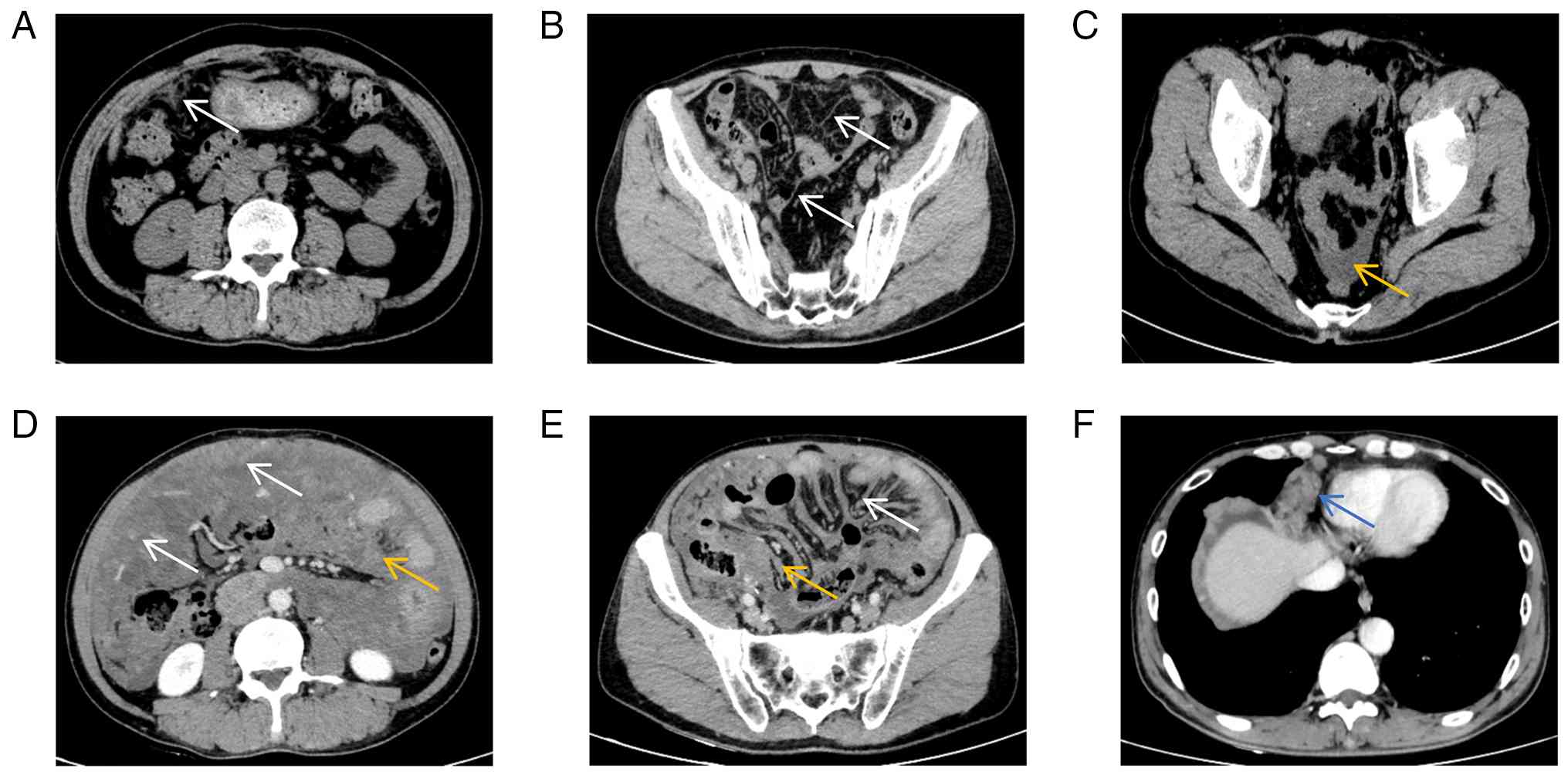
patient sought medical attention multiple times for apparent
mesenteric panniculitis at The First People's Hospital of Xiaoshan
District, The Third People's Hospital of Xiaoshan District, Jinhua
Town Community Health Service Center of Xiaoshan District, as well
as the Second Affiliated Hospital of Zhejiang University School of
Medicine (all Hangzhou, China) between April 2020 and October 2021,
and this condition was diagnosed on the basis of abdominal computed
tomography (CT) scan (Fig.
1A-C).
A physical examination on admission revealed no
jaundice or palpable enlargement of superficial lymph nodes. The
thyroid was normal upon palpation and auscultation of the heart and
lungs showed no abnormalities. The abdomen was soft with no
palpable masses and mild tenderness in the lower middle abdomen,
without rebound tenderness or guarding.
Laboratory findings included a normal white blood
cell count (9.62×109/l; normal range: 3.5–9.5×109/l) and
an elevated absolute neutrophil count (7.80×109/l;
normal range: 1.8–6.3×109/l), giving a neutrophil percentage of
81.0% (normal range: 40–75%) and a lymphocyte percentage of 13.4%
(normal range: 20–50%). Serum albumin was decreased (30.8 g/l;
normal range: 35.0–55.0 g/l). Tumor markers indicated elevated
carbohydrate antigen 125 (CA125) levels (160.60 U/ml; normal range:
0–35 U/ml) and elevated cytokeratin (CK) 19 fragment (Cyfra 21–1)
levels (16.86 ng/ml; normal range: 0–3.3 ng/ml). Enhanced abdominal
CT imaging showed changes to the omentum, multiple intra-abdominal
masses, ascites, pelvic effusion and a mass at the cardiophrenic
angle (Fig. 1D-F).
Gastro-duodenoscopy showed chronic non-atrophic gastritis, but no
notable abnormalities were seen on colonoscopy.
Treatment and follow-up
The patient was diagnosed with diffuse malignant
peritoneal mesothelioma in April 2022. From May to December 2022,
the patient received six cycles of systemic chemotherapy:
Pemetrexed (800 mg on day 1 plus cisplatin 120 mg (40 mg daily for
3 days, total 75 mg/m2)/cycle. In March 2023, disease
progression was confirmed, and treatment was switched to
intraperitoneal perfusion therapy with cisplatin (30 mg +
bevacizumab 300 mg. In May 2023, one additional cycle of the
original pemetrexed-cisplatin regimen was administered. The patient
died in September 2023 (Table
I).
 | Table I.Treatment timeline. |
Table I.
Treatment timeline.
| Postoperative
time | Date | Event | Efficacy/physical
status assessment |
|---|
| Month 1 | May 2022 | Initiation of the
1st cycle of chemotherapy (pemetrexed + cisplatin) | - |
| Month 3 | July 2022 | 2nd cycle of
chemotherapy | The sum of the
largest diameters of peritoneal masses was reduced by 25% compared
with baseline, achieving a PR; CA125 increased to 556.2 U/ml |
| Month 4 | August 2022 | 3rd cycle of
chemotherapy | No notable adverse
reactions; serum albumin stabilized at 31.2 g/l |
| Month 5 | September 2022 | 4th cycle of
chemotherapy | Peritoneal masses
continued to shrink; ascites remained minimal |
| Month 6 | October 2022 | 5th cycle of
chemotherapy | CA125 decreased to
286.3 U/ml; body weight remained stable |
| Month 8 | December 2022 | Completion of the
6th cycle of chemotherapy | The sum of the
largest diameters of peritoneal masses was reduced by 55% compared
with baseline; CA125 decreased to 156.5 U/ml; PR was
maintained |
| Month 11 | March 2023 | Disease progression
assessed; initiation of intraperitoneal perfusion therapy
(cisplatin + bevacizumab) | Masses increased by
26%; moderate ascites; CA125 increased to 923.3 U/ml; ECOG-PS score
2 |
| Month 13 | May 2023 | Intraperitoneal
perfusion therapy ineffective; additional cycle of chemotherapy
administered | Cachexia worsened;
serum albumin 22.1 g/l; total parenteral nutrition required |
| Month 17 | September 2023 | Patient death | Cachexia was the
main cause of mortality |
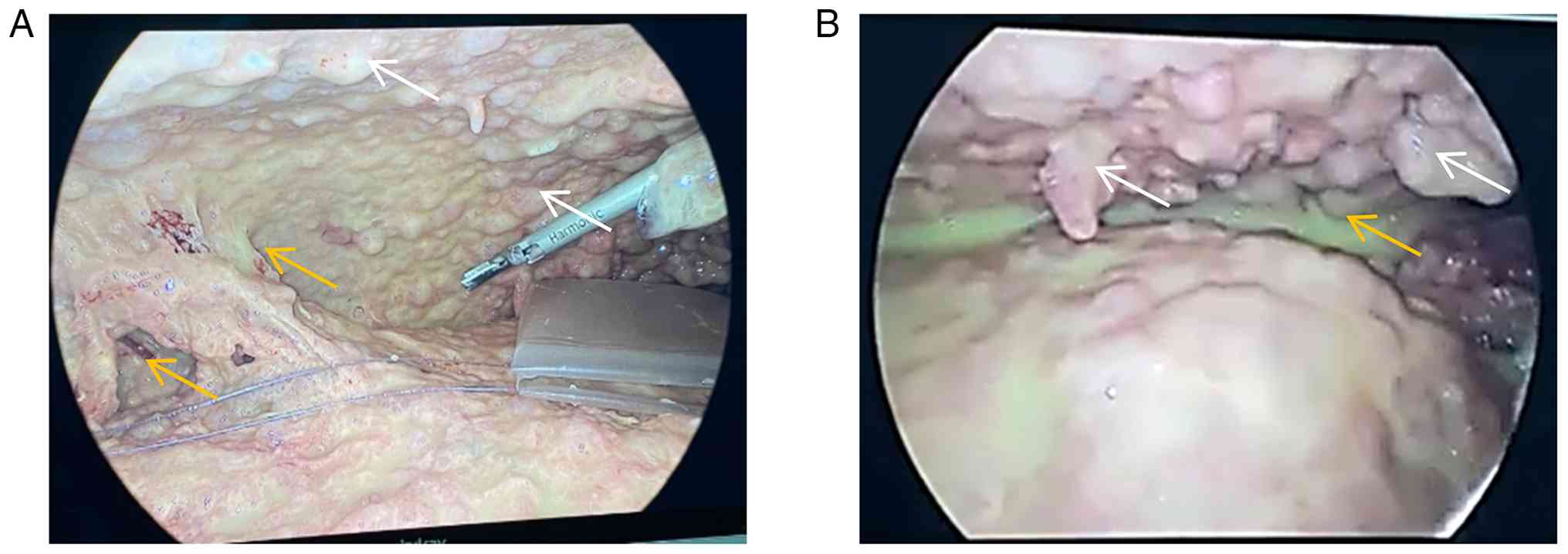
Laparoscopic surgery under general anesthesia with
resection of intra-abdominal lesions, lysis of intestinal
adhesions, omental biopsy and intra-abdominal exploration was
performed in April 2022. A notable quantity of yellow-white
purulent fluid was found in the abdomen, with adhesions in the
right lower abdomen and widespread abdominal wall and omental
nodules, ranging in size from 0.2 to 2 cm, with scattered nodular
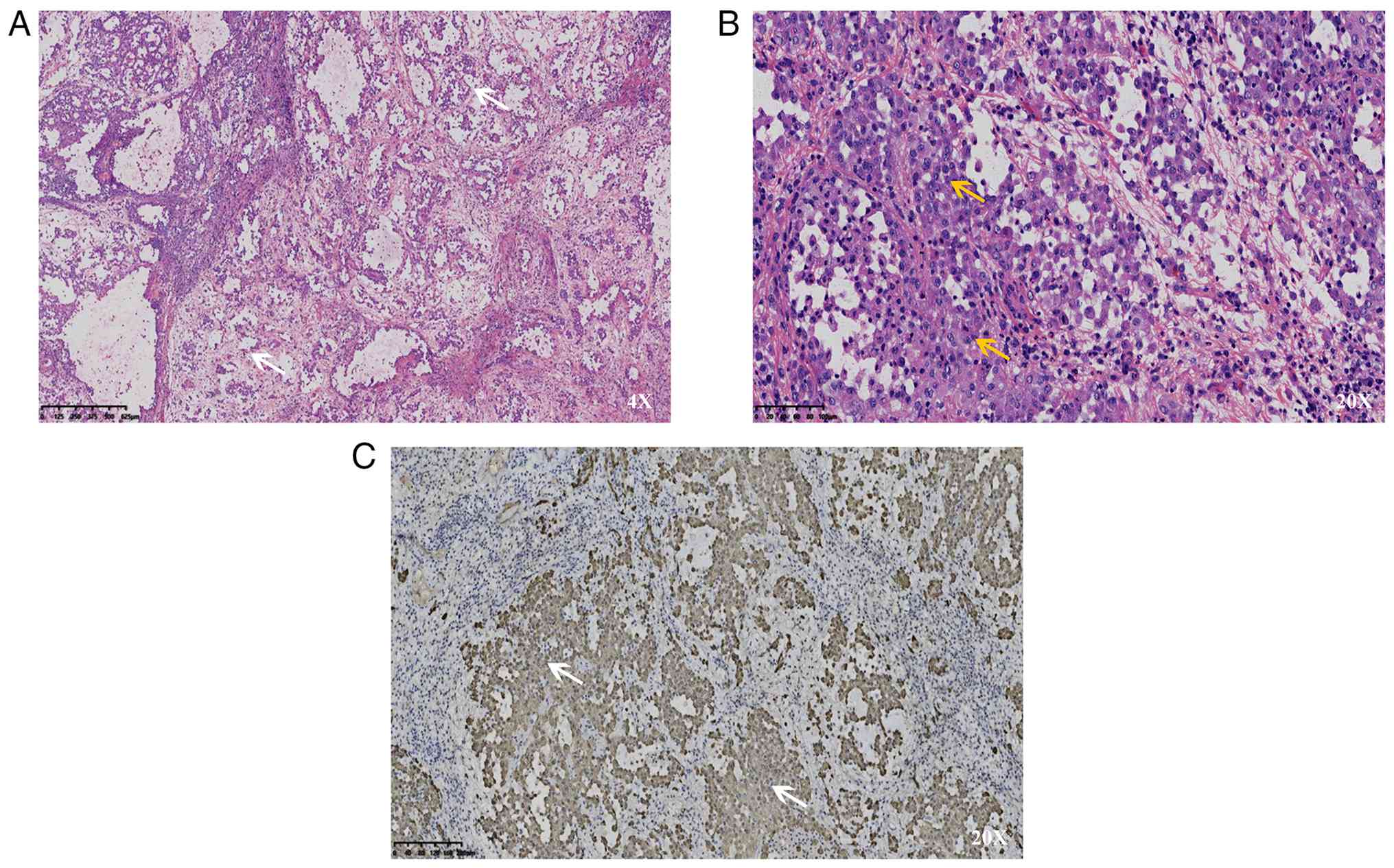
masses on the small intestinal surface (Fig. 2). Histopathological examination of
abdominal wall and omental biopsies showed morphological features
consistent with malignant epithelioid-type mesothelioma (Fig. 3A and B). Immunohistochemical
staining was performed on 4-µm-thick sections obtained from 4%
neutral buffered formalin-fixed (25°C, 24 h), paraffin-embedded
tissue specimens. All specimens were obtained from the same
laparoscopic biopsy of abdominal wall and omental lesions. Antigen
retrieval was performed by heating in EDTA antigen retrieval buffer
(pH 9.0) at 100°C for 20 min. Endogenous peroxidase activity was
blocked with 3% hydrogen peroxide at room temperature for 10 min
and non-specific binding was blocked with 5% BSA (Beijing Solarbio
Science & Technology Co., Ltd.) at room temperature for 30 min.
Sections were incubated with primary antibodies at room temperature
for 40 min:
Cytokeratin (CK), ready-to-use, cat. no. MAB-0093,
Fuzhou Maixin Biotech
Cam5.2, ready-to-use, cat. no. MAB-0209, Fuzhou
Maixin Biotech
Ki-67, 1:200, cat. no. ZM-0166, OriGene
Technologies
CK7, ready-to-use, cat. no. KIT-0021, Fuzhou Maixin
Biotech
CK20, ready-to-use, cat. no. ZA-0574, OriGene
Technologies
Villin, ready-to-use, cat. no. MAB-0540, Fuzhou
Maixin Biotech
CDX2, ready-to-use, cat. no. ZA-0520, OriGene
Technologies
Carcinoembryonic antigen (CEA), ready-to-use, cat.
no. MAB-0010, Fuzhou Maixin Biotech
MUC2, ready-to-use, cat. no. MAB-1101, Fuzhou Maixin
Biotech
MUC4, ready-to-use, cat. no. MAB-1102, Fuzhou Maixin
Biotech
MUC5AC, ready-to-use, cat. no. MAB-1103, Fuzhou
Maixin Biotech
MUC6 (all ready-to-use, cat. no. MAB-1104, Fuzhou
Maixin Biotech
Calretinin (1:100, cat. no. MAB-0064, Fuzhou Maixin
Biotech; Wilms tumor protein (WT-1), ready-to-use, cat. no.
MAB-0037, Fuzhou Maixin Biotech); Hector Battifora mesothelial-1
(HBME-1), ready-to-use, cat. no. MAB-0211, Fuzhou Maixin Biotech);
podoplanin (D2-40), ready-to-use, cat. no. MAB-0049, Fuzhou Maixin
Biotech; Progesterone receptor (PR), ready-to-use, cat. no.
MAB-0158, Fuzhou Maixin Biotech; PAX8, ready-to-use, cat. no.
MAB-0865, Fuzhou Maixin Biotech; p53, ready-to-use, cat. no.
KIT-0010, Fuzhou Maixin Biotech
p16, 1:150, cat. no. CF500036, OriGene Technologies.
HRP-conjugated goat anti-mouse/rabbit IgG polymer (ready-to-use,
cat. no. PV8000D, Beijing Zhongshan Jinqiao Biotechnology Co.,
Ltd.), incubated at room temperature for 15 min. Detection was
performed using a DAB chromogenic kit (cat. no. kit-0014, Fuzhou
Maixin Biotech). Slides were counterstained at 25°C with
hematoxylin for 3 min and eosin for 2 min, dehydrated, cleared, and
mounted, then observed and imaged using a light microscope. For
Ki-67 quantification, the Ki-67 index was determined as the
percentage of positively stained tumor cells in ≥1,000 cells
counted in five randomly selected fields of view using ImageJ
software (v1.53k, National Institutes of Health, Bethesda, MD,
USA).
Immunohistochemical analysis showed that tumor cells
exhibited the following expression results: Cytokeratin (CK)(+),
Cam5.2(+), a Ki-67 index of 50% (indicating high proliferative
activity), CK7(−), CK20(−), villin(−), homeobox protein CDX-2
(CDX-2)(−), carcinoembryonic antigen (CEA)(−) and mucin (MUC)
family (for MUC-2, MUC-4, MUC5A, MUC-6)(−). The results
demonstrated positive expression of calretinin and the
mesothelioma-specific markers Wilms tumor protein (WT-1), Hector
Battifora mesothelial-1 (HBME-1) and podoplanin (D2-40) (Fig. 3C). Representative
immunohistochemical images for all markers are available in
Fig. 4. These findings were
consistent with a diagnosis of peritoneal mesothelioma.
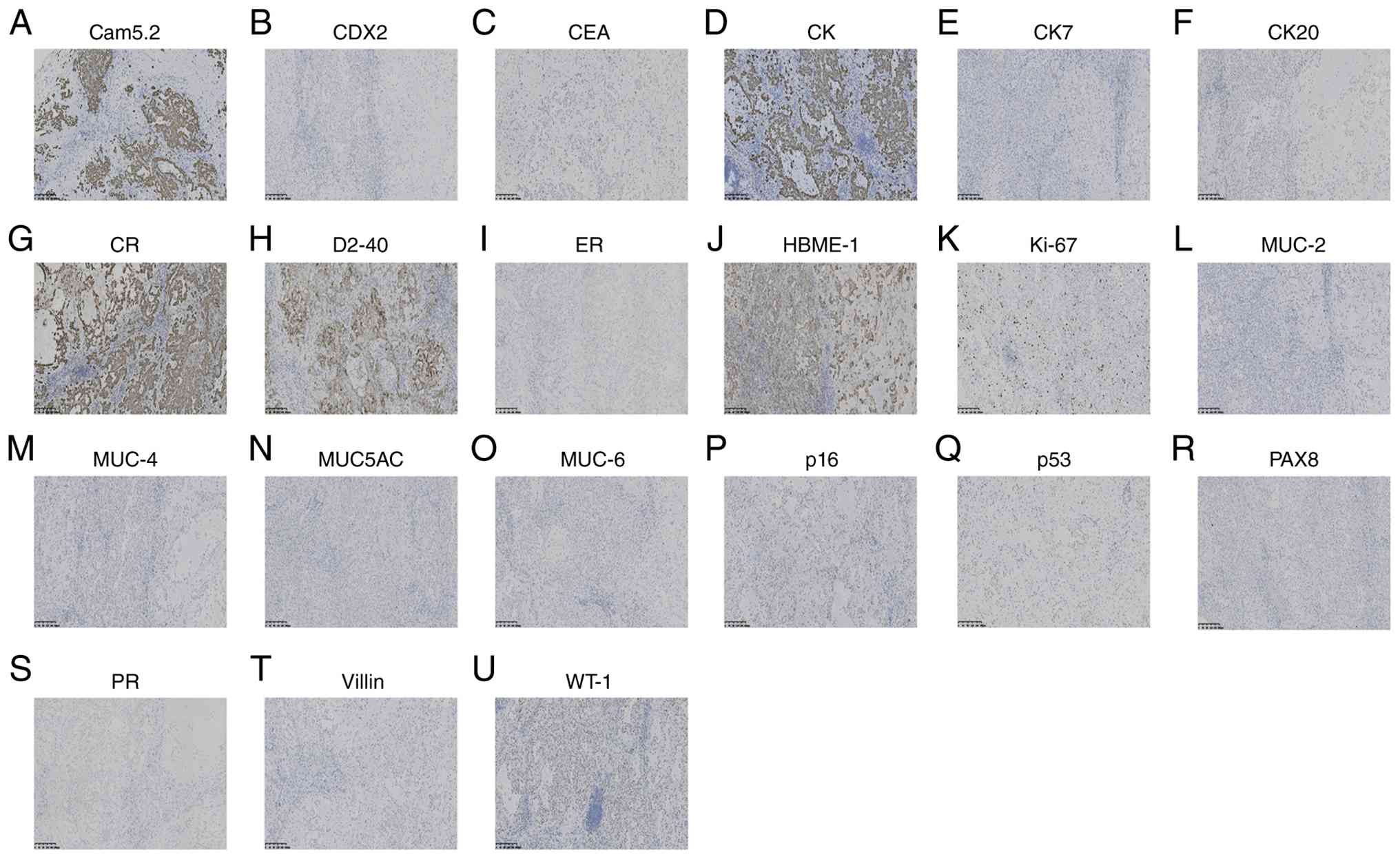 | Figure 4.Immunohistochemical results. Images
of staining for (A) Cam5.2, (B) CDX2, (C) CEA, (D) CK, (E) CK7, (F)
CK20, (G) CR, (H) D2-40, (I) ER, (J) HBME-1, (K) Ki-67, (L) MUC-2,
(M) MUC-4, (N) MUC5AC, (O) MUC-6, (P) p16, (Q) p53, (R) PAX8, (S)
PR, (T) villin and (U) WT-1. CDX2, homeobox protein CDX2; CEA,
carcinoembryonic antigen; CK, cytokeratin; CR, calretinin; D2-40,
podoplanin; ER, estrogen receptor; HBME-1, Hector Battifora
mesothelial-1; MUC, mucin; PAX8, paired box gene 8; PR,
progesterone receptor; WT-1, Wilms tumor protein; CK, cytokeratin.
Scale: 200 µm. |
The Eastern Cooperative Oncology Group-Performance
Status (ECOG-PS) was 1 (13), with
serum albumin at 30.8 g/l (mild hypoalbuminemia) at diagnosis in
April 2022. During chemotherapy (May-December 2022), grade II
nausea and vomiting occurred according to the National Cancer
Institute Common Terminology Criteria for Adverse Events version
5.0 (14), resolving after
symptomatic treatment. Albumin levels remained stable at 29.5–32.1
g/l and body weight was stable (no marked decline). Following
disease progression (March 2023), the ECOG-PS was 2, the albumin
level dropped to 26.3 g/l and mild cachexia developed (8% weight
loss over 6 months). In August 2023, the ECOG-PS was 4, the albumin
level was 22.1 g/l and the severe cachexia required total
parenteral nutritional support.
The patient underwent targeted sequencing using a
120-gene pan-cancer panel (Shanghai Yijian Intelligent
Manufacturing Life Technology Co., Ltd.). Genomic DNA was extracted
from formalin-fixed paraffin-embedded clinical specimens and
circulating cell-free DNA. Sample quality and integrity were
validated using Invitrogen Qubit 4 Fluorometer (Thermo Fisher
Scientific, Inc.) and the Agilent 2100 Bioanalyzer (Agilent
Technologies) for library fragment distribution assessment,
according to the manufacturer's protocols. Library preparation was
performed with the Human FFPE DNA 120 Gene Mutation Detection or
the Human Circulating Free DNA 120 Gene Mutation Detection Kit
(both Shanghai Yijian Intelligent Manufacturing Life Technology
Co., Ltd.). Sequencing was performed on the YJSeq 300 Dx Genetic
Sequencer (Shanghai Yijian Intelligent Manufacturing Life
Technology Co., Ltd.) using the Sequencing Reaction Universal Kit
(Shanghai Yijian Intelligent Manufacturing Life Technology Co.,
Ltd.), in paired-end 2X150 cycles mode (300 cycles total read
length). The final library concentration was measured using the
Invitrogen Qubit 4 Fluorometer, and the average library fragment
size (bp) was determined using the Agilent 2100 Bioanalyzer;
libraries were loaded at a final concentration of 1–20 pM. Raw
sequencing data were processed and analyzed using YJ-Tumor Tumor
Gene Mutation Detection Analysis Software v1.0.0 (Shanghai Yijian
Intelligent Manufacturing Life Technology Co., Ltd.), which
performs data preprocessing, sequence alignment, quality control,
variant calling, microsatellite instability (MSI) analysis, and
variant annotation. The panel covers genes associated with
therapeutic targets for mesothelioma and common solid tumors,
including EGFR, anaplastic lymphoma kinase, ROS proto-oncogene 1,
receptor tyrosine kinase, RAF, neurotrophic tropomyosin receptor
kinase 1/2/3, programmed death ligand 1, CDK inhibitor 2A, TP53,
neurofibromatosis type 1 (NF1), BRCA-1 associated protein 1 and
NF2. Following bioinformatics annotation and filtering, no
pathogenic single nucleotide variants, insertions/deletions, copy
number variations or gene fusions were detected, and no clear
targets for targeted therapy were identified. Accordingly, neither
immunotherapy nor targeted therapy could be recommended for this
patient.
Response evaluation criteria in solid tumors 1.1
(15) for tumor response assessment
were applied throughout the present study. Following the initial
pemetrexed-cisplatin chemotherapy regimen, follow-up
contrast-enhanced CT revealed a 25% reduction in the sum of the
largest diameters of peritoneal masses compared with baseline
(decreasing from 6.0 to 4.5 cm), along with a marked decrease in
ascites (from ‘massive ascites’ prior to treatment to ‘minimal
ascites’). This met the criteria for a partial response (PR) but
tumor markers remained elevated (CA125 increased from 160.60 to
556.2 U/ml). During the second to sixth chemotherapy cycles,
follow-up contrast-enhanced CT showed continued reduction in the
sum of the largest diameters of peritoneal masses, decreasing by
55% from baseline (from 6.0 to 2.7 cm). The minimal ascites
remained stable and tumor markers continued to decline (CA125
decreased from 556.20 to 156.5 U/ml), meeting the criteria for a
PR. Disease progression parameters at 11 months (using the value
before peritoneal perfusion therapy as the new baseline) showed
that the sum of the largest diameters of peritoneal masses
increased by 26% compared with the PR assessment (from 2.7 to 3.4
cm), ascites volume increased again (moderate amount), CA125 rose
to 923.3 U/ml, and the patient experienced worsening abdominal pain
and distension along with further weight loss (5 kg over 2 months).
This met the criteria for disease progression.
During a laparoscopy, the surgical team in
collaboration with the Department of Radiology assessed the
patient's peritoneal cancer index (PCI) (16) with a total score of points. A PCI
score >15 indicates a high tumor burden with a low probability
(<30%) of achieving complete cytoreductive surgery, according to
Peritoneal Surface Oncology Group International (PSOGI) (17) guidelines. The patient refused
surgery and a ‘non-surgical treatment’ approach was selected. The
patient received six cycles of chemotherapy (21-day) between May
and December 2022 with 500 mg/m2 (actual dose, 800 mg)
pemetrexed on day 1 and 75 mg/m2 cisplatin administered
on days 1, 2, and 3 (40 mg daily).. The body surface area of the
patient was calculated as 1.68 m2 using the Mosteller
formula (18) (height, 170 cm;
weight, 60 kg). According to RECIST 1.1 (15), pemetrexed-cisplatin chemotherapy
achieved a PR after six cycles, with a 55% decrease in the sum of
the largest diameters of peritoneal masses (from 6.0 to 2.7 cm),
but was accompanied by severe adverse events, mainly grade III
myelosuppression and grade II gastrointestinal reactions. Treatment
was adjusted to intraperitoneal perfusion with 30 mg cisplatin plus
300 mg bevacizumab administered on day 1 every 3 weeks in the 11th
post-operative month, a compassionate-use protocol which was
submitted to the hospital's Ethics Committee for special review and
was approved (approval no. 2024–07-01). The patient and his family
were informed of the lack of clear evidence-based support,
potential risks and benefits, and then provided written informed
consent. This process complies with the relevant provisions
regarding compassionate use in the Declaration of Helsinki and
China's Drug Administration Law. Disease progression was recorded
and one additional cycle of pemetrexed and cisplatin was given in
the 13th post-operative month. The patient died in September 2023
with cachexia noted as a contributing condition.
Discussion
To the best of our knowledge, the present case is
the first reported instance worldwide of a road maintenance worker
with long-term exposure to asphalt who developed DPM and was
misdiagnosed with mesenteric panniculitis. A previous study
reported the misdiagnosis of DPM as ovarian cancer or abdominal
tuberculosis (3). To the best of
our knowledge, the present case is the first to define the
characteristic imaging evolution over 18 months during which
diffuse peritoneal mesothelioma was initially misdiagnosed as
mesenteric panniculitis (presenting as mild omental thickening and
minimal effusion) and demonstrated typical features of DPM
including diffuse omental thickening, intra-abdominal masses, and
cardiophrenic angle lymph node metastasis. This progression gives
imaging indications for the early clinical differentiation between
the two conditions. A rare calretinin-negative immunophenotype of
epithelioid DPM was identified, which accounts for 8.7% of
epithelioid DPM cases (12). A
triple-marker panel of WT-1, HBME-1 and D2-40 was used to avoid
misconceptions based on calretinin-only testing and to refine the
DPM immunohistochemical diagnostic system. Clinical evidence for
the non-surgical treatment of patients with DPM with a high PCI
score (27 points) who refuse surgery is provided in the study.
Pemetrexed + cisplatin chemotherapy achieved a 55% decrease in the
sum of the longest diameters of peritoneal masses (from 6.0 to 2.7
cm), as calculated per RECIST 1.1 criteria (15), representing tumor regression
although standard doses were associated with grade III
myelosuppression. A dose adjustment regimen of 600–700
mg/m2 was proposed, filling the clinical gap of a lack
of standardized treatment protocols for patients with diffuse
peritoneal mesothelioma, PCI >15), and who refuse cytoreductive
surgery.
A potential association between asphalt exposure and
DPM was identified. An epidemiological meta-analysis by Partanen
and Boffetta (19) reported a
2.3-fold increased risk of developing malignant tumors in the
abdominal cavity among individuals exposed to asphalt and showed a
dose-response relationship. The present patient had a 28-year
history of unprotected exposure to asphalt, constituting high-risk
exposure. Asphalt contains carcinogens, such as polycyclic aromatic
hydrocarbons (PAHs) and benzo(a)pyrene, which cause DNA damage in
peritoneal mesothelial cells by generating reactive oxygen species,
a similar mechanism to that of asbestos (20). A global population study by Jin
et al (21) showed that DPM
incidence did not decrease markedly following the ban or
restriction of asbestos, suggesting a potential role for
non-asbestos carcinogens. The present case gives the first clinical
evidence to support this conclusion.
Asbestos exposure is associated with DPM, although
with a weaker association than for the more common pleural
mesothelioma (17,21). The length of asbestos fibers, which
may exceed the capacity for phagocytosis, causing release of
reactive oxygen species (ROS) and an inflammatory and mutagenic
environment, seems a likely explanation for mesothelioma occurrence
at both the pleural and peritoneal sites (20,22).
Less is known about the impact of genetic susceptibility at the two
sites, although some predisposing polymorphisms in genes including
BAP1, TP53, GSTT1 and XRCC1 have been linked to the pleural form of
the disease (23). DPM is
characterized by extensive proliferation along peritoneal surfaces,
often adhering to organs. Typical radiological findings include
diffuse peritoneal and omental thickening, abdominal masses,
ascites and lymph node metastases (24).
The present patient had no history of asbestos
exposure but had long been engaged in highway maintenance work. The
base asphalt + modifier products commonly used in highway
maintenance do not contain natural asbestos but, when heated to
160–180°C, they release PAHs, benzo(a)pyrene and volatile organic
compounds. The asphalt aggregate contains additional heavy metal
impurities, such as chromium and nickel, which are classified as
Group 1 or Group 2A carcinogens by the International Agency for
Research on Cancer (25). Asphalt
carcinogens induce malignant transformation of peritoneal
mesothelial cells through two pathways (20,26).
First, PAHs are metabolized by cytochrome P450 to produce ROS,
causing point mutations in tumor suppressor genes, such as p53 and
CDKN2A, which disrupt cell cycle regulation. Second, long-term
accumulation of asphalt microparticles and heavy metals in the
peritoneal cavity may trigger chronic aseptic inflammation,
activate the NF-κB pathway and create a tumor-promoting
microenvironment, leading to abnormal proliferation and invasion of
mesothelial cells. Occupational exposure to potential carcinogens,
such as asphalt, may have occurred in the present case (19,21,27)
and contributed to the disease. However, causal evidence is lacking
and further epidemiological and mechanistic studies are needed to
validate the association. Mesothelioma may involve the pleura,
peritoneum and pericardium with pleural mesothelioma being the most
common (accounting for 80–85%), followed by peritoneal mesothelioma
(15%) and pericardial mesothelioma being rare (<1%) (21,28).
The present case involved peritoneal involvement without
manifestations of pleural or pericardial involvement (chest CT
showed no pleural thickening or pericardial effusion), consistent
with the typical site characteristics of DPM.
An accurate diagnosis of DPM relies on
histopathological examination, including morphological observation
of biopsy specimens and immunohistochemical verification. Tumor
cell morphological features, such as a tubular arrangement of
epithelioid cells and spindle-shaped morphology of sarcomatoid
cells, must be examined microscopically and combined with
positivity for at least two mesothelioma-specific markers (such as
WT-1, D2-40 and HBME-1) and two negative markers (such as CEA and
thyroid transcription factor 1) while excluding metastatic
carcinoma or other peritoneal tumors (29,30).
The following tests for markers associated with metastatic cancer
of gastrointestinal and female reproductive tract origin were
performed for the present case with the following results: CK7(−),
CK20(−), CDX2(−), p16(−), paired box gene 8 (PAX8)(−), p53
(wild-type, positivity rate <10%), estrogen receptor (ER)(−) and
progesterone receptor (PR)(−). Combined with the previous negative
results for CEA and MUC family, common malignant tumors with
peritoneal metastasis, such as gastrointestinal adenocarcinoma, may
be excluded, meeting the core requirement of ‘exclusion of
metastatic cancer’ in the 2023 IMIG Mesothelioma Diagnostic
Guidelines (29). The annual
age-adjusted incidence of secondary peritoneal metastases is
99.00/1,000,000 persons, compared with only 4.36 per 1,000,000
persons for primary peritoneal malignancies including mesothelioma
(31). The combination of the
aforementioned markers is key to the differential diagnosis, since
tumors of gastrointestinal origin are often CK7/CK20/CDX2-positive
and tumors of female reproductive tract origin are frequently
associated with abnormal expression of PAX8, ER/PR or p16 (30). All of these were negative for the
present patient, and the mesothelioma-specific phenotype of WT-1,
HBME-1 and D2-40 confirmed the accuracy of the DPM diagnosis.
Tumor, lymph node involvement and metastasis staging must factor in
the PCI, which evaluates the size and distribution of peritoneal
tumors (32). The American Cancer
Society has reported that patients have markedly improved prognosis
in the earlier stages, with 5-year survival rates being 87% at
stage I, 53% at stage II and 29% at stage III (33,34).
Laparoscopic biopsy allowed a definitive diagnosis for the present
case. A nodular lesion was identified at the site of the
laparoscopic port in the right lower quadrant of the abdominal wall
at 1 month post-surgery, indicating the occurrence of implantation
metastasis. This observation indicates the aggressive nature of
this type of tumor and may suggest a particularly poor prognosis
for the patient (35).
Standardized treatment protocols have yet to be
established for DPM. CRS + HIPEC is recommended by the PSOGI, with
the aim of removing visible tumors and separate adhesions to
improve HIPEC efficiency (21).
This therapeutic strategy carries a notable rate of grade 3–4
complications; however, the 5-year survival rate has been extended
to 42% from the baseline of <15% for patients treated with
non-CRS + HIPEC regimens (36).
Systemic chemotherapy protocols for DPM have their basis in those
established for pleural mesothelioma, and pemetrexed in combination
with cisplatin, carboplatin or gemcitabine is generally preferred,
especially for patients who are not candidates for CRS + HIPEC.
Intraperitoneal chemotherapy increases local drug concentrations,
giving more efficacious treatment of peritoneal surface
malignancies and reducing systemic side effects (37). Promising results were reported for
the treatment of 26 patients with unresectable DPM treated with
pressurized intraperitoneal aerosol chemotherapy. The treatment
achieved clinical symptom improvement in 32% of patients and
ascites control in 46%; 54% of patients underwent successful CRS +
HIPEC, with a median progression-free survival of 33.5 months in
resected patients vs. 7.4 months in unresected patients (38). Although the present patient
initially achieved a PR with pemetrexed at a close to standard
dose, grade III myelosuppression developed. Therefore, patients
with DPM who have a high PCI score and refuse surgery are
recommended a dose-adjusted regimen (such as pemetrexed 600–700
mg/m2) to balance efficacy and safety.
No targets suitable for immunotherapy were
identified in the present case by genetic testing, rendering
immunotherapy inappropriate. The patient received six cycles of
chemotherapy with pemetrexed (800 mg on day 1) combined with
cisplatin (40 mg on days 1–3). Although a PR was achieved (35%
reduction in peritoneal mass; CA125 decreased from 160.6 to 156.5
U/ml), Grade III bone marrow suppression (lowest neutrophil count
0.8×109/l) and grade II gastrointestinal reactions
developed. This indicates that while the regimen is effective for
low-grade epithelioid DPM, enhanced toxicity management is required
(for example, prophylactic use of granulocyte colony-stimulating
factor and 5-HT3 receptor antagonists). The reasons for the
ineffectiveness of intraperitoneal perfusion therapy could be due
to the regimen being adjusted to intraperitoneal cisplatin (30 mg)
+ bevacizumab (300 mg) at 11 months while disease progression
occurred within 1 month. This treatment regimen constitutes
off-label compassionate use. The treatment decision was based on
two factors. First, the patient's disease progressed after six
cycles of pemetrexed plus cisplatin chemotherapy and no standard
second-line regimen was available. Second, the anti-angiogenic
mechanism of bevacizumab may have a synergistic effect on malignant
peritoneal tumors and a small number of studies (39,40) on
intraperitoneal administration for ovarian cancer and colorectal
cancer with peritoneal metastases have demonstrated a potential for
local tumor control (38). The
tumor may have extensively invaded extraperitoneal tissues (such as
peritoneal wall puncture site metastasis), rendering local drug
concentrations insufficient to effectively cover the lesions, and
there exists a lack of medical evidence for bevacizumab in the
intraperitoneal treatment of DPM (38). This suggests that careful evaluation
of the extent of tumor invasion should be made when selecting
intraperitoneal perfusion regimens. The present case suggests that
patients with DPM with high PCI scores (>15) who refuse surgery
should have initial chemotherapy that prioritizes ‘dose-adjusted
regimens with manageable toxicity’ (for example, reducing
pemetrexed to 600–700 mg/m2) while monitoring tumor
markers (CA125 and Cyfra 21–1) and imaging changes to identify
disease progression early and adjust treatment strategies.
There were several limitations to the present study.
Current international guidelines recommend CRS + HIPEC as the
first-line treatment for resectable DPM with patients receiving
this regimen achieving a 5-year survival rate of 42% (36). By contrast, the present case
received only systemic chemotherapy (pemetrexed + cisplatin) and
intraperitoneal perfusion therapy (cisplatin + bevacizumab),
falling within the second-line treatment category for
‘unresectable/ surgery refusal’. The treatment efficacy (13-month
survival) reflects outcomes only for this patient population and
cannot be extrapolated to patients with DPM eligible for CRS +
HIPEC. In addition, due to the absence of efficacy data from a CRS
+ HIPEC treatment group (such as tumor burden reduction and PFS),
the outcome in this case of PR to pemetrexed-cisplatin chemotherapy
followed by progression does not validate the superiority of
‘non-surgical treatment vs. surgery combined with HIPEC’ and acts
as a reference only for patients similarly unable to undergo CRS +
HIPEC. There are also ethical review limitations: The
intraperitoneal bevacizumab combined with cisplatin regimen has not
undergone institutional review board approval. Informed consent was
obtained from the patient and their family but strict adherence to
ethical review procedures is still required in subsequent clinical
practice to ensure the compliance of the treatment regimen. The
purulent fluid found in the peritoneal cavity during laparoscopy
was not subjected to cytological examination or microbiological
culture and the possibility of a concurrent infection cannot be
ruled out. The diagnosis of malignancy could not be supported by
the cytological analysis of peritoneal fluid, which may have
impacted clinical decision-making. The present PCI score of 27
points was determined from combined assessment by laparoscopic
examination and radiologists (32).
However, laparoscopic PCI assessment has limitations due to
incomplete visualization of the abdominal cavity, particularly
regarding tumor involvement in hidden areas such as subphrenic and
retrohepatic regions, and may lead to underestimation of the true
tumor burden (34). By contrast,
open surgery allows for complete abdominal exploration and yields a
more accurate PCI score (41).
Furthermore, there is a lack of high-level (randomized controlled
trials, systematic reviews, or meta-analyses) evidence supporting
intraperitoneal bevacizumab therapy for DPM, and the lack of
response observed in the present case underscores the uncertainty
of this treatment regimen (37).
The use off-label intraperitoneal cisplatin + bevacizumab was made
to inform potential treatment options for patients with advanced
disease and may serve as a reference for future studies.
In conclusion, the present study presents a case of
DPM initially misdiagnosed as mesenteric panniculitis, illustrating
the difficulties of the early diagnosis and treatment of DPM. More
effective therapeutic interventions are needed which may be
diversified by future developments in immunotherapy and genotyping
techniques to inform future treatment strategies for DPM.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be found
in Figshare under accession number 10.6084/m9.figshare.32287683 at
the following URL: https://doi.org/10.6084/m9.figshare.32287683.
Authors' contributions
YC conceived and designed the study, collected,
analyzed and interpreted data, participated in clinical management
and perioperative care, constructed the figures and tables and
wrote the original manuscript. QF performed the histopathological
and immunohistochemical examination. JX collected the clinical and
follow-up data, supervised the clinical management, and edited the
manuscript for important intellectual content. RW performed and
interpreted all computed tomography images, provided formal
radiological analysis, and contributed to the imaging methodology.
YM collected and analyzed data. YL designed the study, supervised
the entire research process, and administered the project. YC and
YL confirm the authenticity of all the raw data. All authors have
read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of The First People's Hospital of Xiaoshan District
(Hangzhou, China) in accordance with the Declaration of Helsinki
(approval no. 2024-07). Written informed consent was obtained from
the patient's family.
Patient consent for publication
The patient provided written informed consent for
the publication of the case report and associated images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Malpica A: Peritoneal mesothelioma-an
update. Adv Anat Pathol. 30:262–274. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chun CP, Song LX, Zhang HP, Guo DD, Xu GX,
Li Y, Xin X, Cao J and Li F: Malignant peritoneal mesothelioma. Am
J Med Sci. 365:99–103. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Houssaini ZI, Agouri HE, Amalik S,
Khouchoua S, Jerguigue H, Latib R, Khannoussi BE and Omor Y:
Diffuse malignant peritoneal mesothelioma mimicking ovarian cancer.
Radiol Case Rep. 17:779–783. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bianchi C and Bianchi T: Global
mesothelioma epidemic: Trend and features. Indian J Occup Environ
Med. 18:82–88. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zhao J, Zuo T, Zheng R, Zhang S, Zeng H,
Xia C, Yang Z and Chen W: Epidemiology and trend analysis on
malignant mesothelioma in China. Chin J Cancer Res. 29:361–368.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bridda A, Padoan I, Mencarelli R and Frego
M: Peritoneal mesothelioma: A review. MedGenMed.
9:322007.PubMed/NCBI
|
|
7
|
Gazdar AF and Carbone M: Molecular
pathogenesis of malignant mesothelioma and its relationship to
simian virus 40. Clin Lung Cancer. 5:177–181. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sun L, Li C and Gao S: Diffuse malignant
peritoneal mesothelioma: A review. Front Surg. 9:10158842023.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kusamura S, Baratti D, De Simone M,
Pasqual EM, Ansaloni L, Marrelli D, Robella M, Accarpio F, Valle M,
Scaringi S, et al: Diagnostic and therapeutic pathway in diffuse
malignant peritoneal mesothelioma. Cancers (Basel). 15:6622023.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Chatterjee A, Kusamura S, Baratti D,
Guaglio M, Battaglia L and Deraco M: Impact of perioperative
systemic chemotherapy on survival for patients who have diffuse
malignant peritoneal mesothelioma treated with CRS-HIPEC. Ann Surg
Oncol. 31:556–566. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Su YD, Yang ZR, Li XB, Yu Y, Du XM and Li
Y: Key factors for successful cytoreductive surgery plus
hyperthermic intraperitoneal chemotherapy to treat diffuse
malignant peritoneal mesothelioma: Results from specialized
peritoneal cancer center in China. Int J Hyperthermia. 39:706–712.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Nava FL, Kusamura S, Shimonovitz-Moore M,
Cavalleri T, Baratti D, Guaglio M, Cabras AD, Colletti G, Deraco M
and Milione M: Optimizing the pathological diagnosis of diffuse
malignant peritoneal mesothelioma. Eur J Surg Oncol. 51:1103772025.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the eastern cooperative oncology group. Am J Clin
Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
National Cancer Institute, . Common
Terminology Criteria for Adverse Events (CTCAE). Version 5.0. U.S.
Department of Health and Human Services; 2017
|
|
15
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Jacquet P and Sugarbaker PH: Clinical
research methodologies in diagnosis and staging of patients with
peritoneal carcinomatosis. Cancer Treat Res. 82:359–374. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kepenekian V, Sgarbura O, Marchal F,
Villeneuve L, Kusamura S and Deraco M: 2022 PSOGI consensus on
HIPEC regimens for peritoneal malignancies: Diffuse malignant
peritoneal mesothelioma. Ann Surg Oncol. 30:7803–7813. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Mosteller RD: Simplified calculation of
body-surface area. N Engl J Med. 317:10981987. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Partanen T and Boffetta P: Cancer risk in
asphalt workers and roofers: Review and meta-analysis of
epidemiologic studies. Am J Ind Med. 26:721–740. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Carbone M and Yang H: Molecular pathways:
Targeting mechanisms of asbestos and erionite carcinogenesis in
mesothelioma. Clin Cancer Res. 18:598–604. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Jin W, Ding Z, Zhang M, Shen L, Wang H,
Huang J, Xuzhang W, Huang Y, Dong C, Li C, et al: The global burden
of mesothelioma and its association with asbestos bans, 1990–2021:
A population-based study. Lung Cancer. 203:1085342025. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zwijsen K, Heirwegh E, Schillebeeckx E,
Marcq E, Covaci A, de Beeck KO, van Meerbeeck JP, Raskin J,
Janssens A, Snoeckx A and Lamote K: Multi-omic screening for
pleural mesothelioma in asbestos-exposed populations: A literature
review and recommendations. Lung Cancer. 212:1088932026. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Carbone M, Amelio I, Affar EB, Brugarolas
J, Cannon-Albright LA, Cantley LC, Cavenee WK, Chen Z, Croce CM,
Andrea AD, et al: Consensus report of the 8 and 9th weinman
symposia on gene × environment Interaction in carcinogenesis: Novel
opportunities for precision medicine. Cell Death Differ.
25:1885–1904. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gupta S, Chandola S, Goel D, Khandelwal Y,
Haria P, Ray MD and Das CJ: Imaging of peritoneal surface
malignancies: Diagnosis and clinical implications. Abdom Radiol
(NY). 51:1085–1104. 2026. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
de Conti A, Madia F, Schubauer-Berigan MK
and Benbrahim-Tallaa L: Carcinogenicity of some metals evaluated by
the IARC Monographs: A synopsis of the evaluations of arsenic,
cadmium, cobalt, and antimony. Toxicol Appl Pharmacol.
504:1175062025. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Møller P and Jacobsen NR: Weight of
evidence analysis for assessing the genotoxic potential of carbon
nanotubes. Crit Rev Toxicol. 47:867–884. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Boffetta P, Burstyn I, Partanen T,
Kromhout H, Svane O, Langård S, Järvholm B, Frentzel-Beyme R,
Kauppinen T, Stücker I, et al: Cancer mortality among European
asphalt workers: An international epidemiological study. I. Results
of the analysis based on job titles. Am J Ind Med. 43:18–27. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Mikou P, Pergaris A, Engels M and Chandra
A: Review of the impact of the international system for serous
fluid cytopathology. Cytopathology. 35:16–22. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Husain AN, Chapel DB, Attanoos R, Beasley
MB, Brcic L, Butnor K, Chirieac LR, Churg A, Dacic S,
Galateau-Salle F, et al: Guidelines for pathologic diagnosis of
mesothelioma: 2023 update of the consensus statement from the
international mesothelioma interest group. Arch Pathol Lab Med.
148:1251–1271. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Parra-Medina R, Castañeda-González JP,
Chaves-Cabezas V, Alzate JP and Chaves JJ: Diagnostic performance
of immunohistochemistry markers for malignant pleural mesothelioma
diagnosis and subtypes. A systematic review and meta-analysis.
Pathol Res Pract. 257:1552762024. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Cortés-Guiral D, Hübner M, Alyami M, Bhatt
A, Ceelen W, Glehen O, Lordick F, Ramsay R, Sgarbura O, Van Der
Speeten K, et al: Primary and metastatic peritoneal surface
malignancies. Nat Rev Dis Primers. 7:912021. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Salo SAS, Lantto E, Robinson E,
Myllärniemi M, Laaksonen S, Salo JA, Rantanen T and Ilonen I:
Prognostic role of radiological peritoneal cancer index in
malignant peritoneal mesothelioma: National cohort study. Sci Rep.
10:132572020. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Sauter JL, Dacic S, Galateau-Salle F,
Attanoos RL, Butnor KJ, Churg A, Husain AN, Kadota K, Khoor A,
Nicholson AG, et al: The 2021 WHO classification of tumors of the
pleura: Advances since the 2015 classification. J Thorac Oncol.
17:608–622. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Yan TD, Deraco M, Elias D, Glehen O,
Levine EA, Moran BJ, Morris DL, Chua TC, Piso P, Sugarbaker PH, et
al: A novel tumor-node-metastasis (TNM) staging system of diffuse
malignant peritoneal mesothelioma using outcome analysis of a
multi-institutional database*. Cancer. 117:1855–1863. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Nunez MF, Sardi A, Jimenez W, Nieroda C,
Sittig M, MacDonald R, Aydin N, Milovanov V and Gushchin V:
Port-site metastases is an independent prognostic factor in
patients with peritoneal carcinomatosis. Ann Surg Oncol.
22:1267–1273. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Acs M, Gerken M, Gajic I, Mayr M, Zustin J
and Piso P: Ten-year single-center experience with treatment of
primary diffuse malignant peritoneal mesothelioma (DMPM) by
cytoreductive surgery (CRS) and hyperthermic intraperitoneal
chemotherapy (HIPEC). Langenbecks Arch Surg. 407:3057–3067. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Sugarbaker PH and Chang D: Long-term
regional chemotherapy for patients with epithelial malignant
peritoneal mesothelioma results in improved survival. Eur J Surg
Oncol. 43:1228–1235. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Kepenekian V, Péron J, You B, Bonnefoy I,
Villeneuve L, Alyami M, Bakrin N, Rousset P, Benzerdjeb N and
Glehen O: Non-resectable malignant peritoneal mesothelioma treated
with pressurized intraperitoneal aerosol chemotherapy (PIPAC) plus
systemic chemotherapy could lead to secondary complete
cytoreductive surgery: A cohort study. Ann Surg Oncol.
29:2104–2113. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Classe JM, Meeus P, Hudry D, Wernert R,
Quenet F, Marchal F, Houvenaeghel G, Bats AS, Lecuru F, Ferron G,
et al: Hyperthermic intraperitoneal chemotherapy for recurrent
ovarian cancer (CHIPOR): A randomised, open-label, phase 3 trial.
Lancet Oncol. 25:1551–1562. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Rietveld PCS, Guchelaar NAD, van Eerden
RAG, de Boer NL, de Bruijn P, Sassen SDT, Madsen EVE, Koch BCP,
Verhoef C, Burger JWA, et al: Intraperitoneal pharmacokinetics of
systemic oxaliplatin, 5-fluorouracil and bevacizumab in patients
with colorectal peritoneal metastases. Biomed Pharmacother.
176:1168202024. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Yurttas C, Überrück L, Nadiradze G,
Königsrainer A and Horvath P: Limitations of laparoscopy to assess
the peritoneal cancer index and eligibility for cytoreductive
surgery with HIPEC in peritoneal metastasis. Langenbecks Arch Surg.
407:1667–1675. 2022. View Article : Google Scholar : PubMed/NCBI
|