Lung cancer remains the most common malignancy and
the leading cause of cancer-related death globally, with non-small
cell lung cancer (NSCLC) accounting for ~85% of all lung cancer
cases and representing the predominant pathological subtype of this
disease (1,2). The management of NSCLC has advanced
into an era of precision medicine, marked by the development of
therapies targeting oncogenic driver genes and immune checkpoint
inhibitors (3,4). However, the emergence of acquired
resistance remains a primary cause of treatment failure (5). This challenge is rooted in one of the
core biological features of NSCLC, namely tumor heterogeneity. It
manifests not only within individual tumors (intratumor
heterogeneity) but also between different metastatic lesions
(intertumor heterogeneity) and markedly evolves over time under the
selective pressure of treatment (clonal evolution) (6,7).
Traditional, static diagnostic and therapeutic models, e.g.,
treatment decisions based solely on initial TNM staging, fixed
chemotherapy regimens for all patients and non-adaptive
radiotherapy planning, typically reliant on single biopsy
specimens, are inadequate for capturing this complex dynamic
landscape, thereby limiting the durability of treatment efficacy.
Recent progress in high-throughput sequencing technologies,
particularly the application of single-cell sequencing, spatial
transcriptomics and liquid biopsy, has enabled the dissection of
the clonal architecture and evolutionary trajectory of NSCLC with
unprecedented resolution (8–10). The
data generated by these technologies necessitate the establishment
of a new conceptual framework capable of integrating spatiotemporal
dynamic information. The present review therefore aimed to propose
and elaborate on such a framework, arguing that the clinical
management strategy for NSCLC must transition from a static,
genotype-based ‘one-time strike’ approach towards a ‘dynamic
management’ strategy founded on continuous monitoring, with the
goal of achieving more prolonged disease control.
Spatial heterogeneity constitutes the geographical
dimension of tumor complexity. Seminal multi-region sequencing
studies determined marked intratumor heterogeneity at the genomic
level within individual NSCLC tumors (6,7,11). For
instance, sequencing different regions of a primary lung lesion may
reveal an uneven distribution of mutant alleles with evolutionary
importance in driver genes (such as EGFR) and even identify
distinct subclonal dominance regions (12). This heterogeneity also extends to
gene expression. Single-cell RNA sequencing has revealed continuous
and diverse cancer cell states within a tumor, including
proliferation, differentiation, epithelial-mesenchymal transition
(EMT) and drug response (13).
Notably, spatial transcriptomics and multiplex immunofluorescence
technologies anchor cellular molecular features to their native
tissue microenvironment (8).
Studies have found that cancer cell subpopulations with stem-like
properties or those in an EMT state are often specifically enriched
at the invasive front of the tumor margin, forming complex spatial
interaction networks with specific immune cells [such as M2-type
macrophages and regulatory T cells (Tregs)] and fibroblasts; these
niches influence tumor progression and therapeutic response by
promoting immunosuppression, remodeling the extracellular matrix,
and secreting pro-survival and pro-invasive factors (14–16).
With regard to intertumor heterogeneity, systematic
genomic comparative analyses of different metastatic lesions
(including the brain, bone and adrenal glands) have revealed a
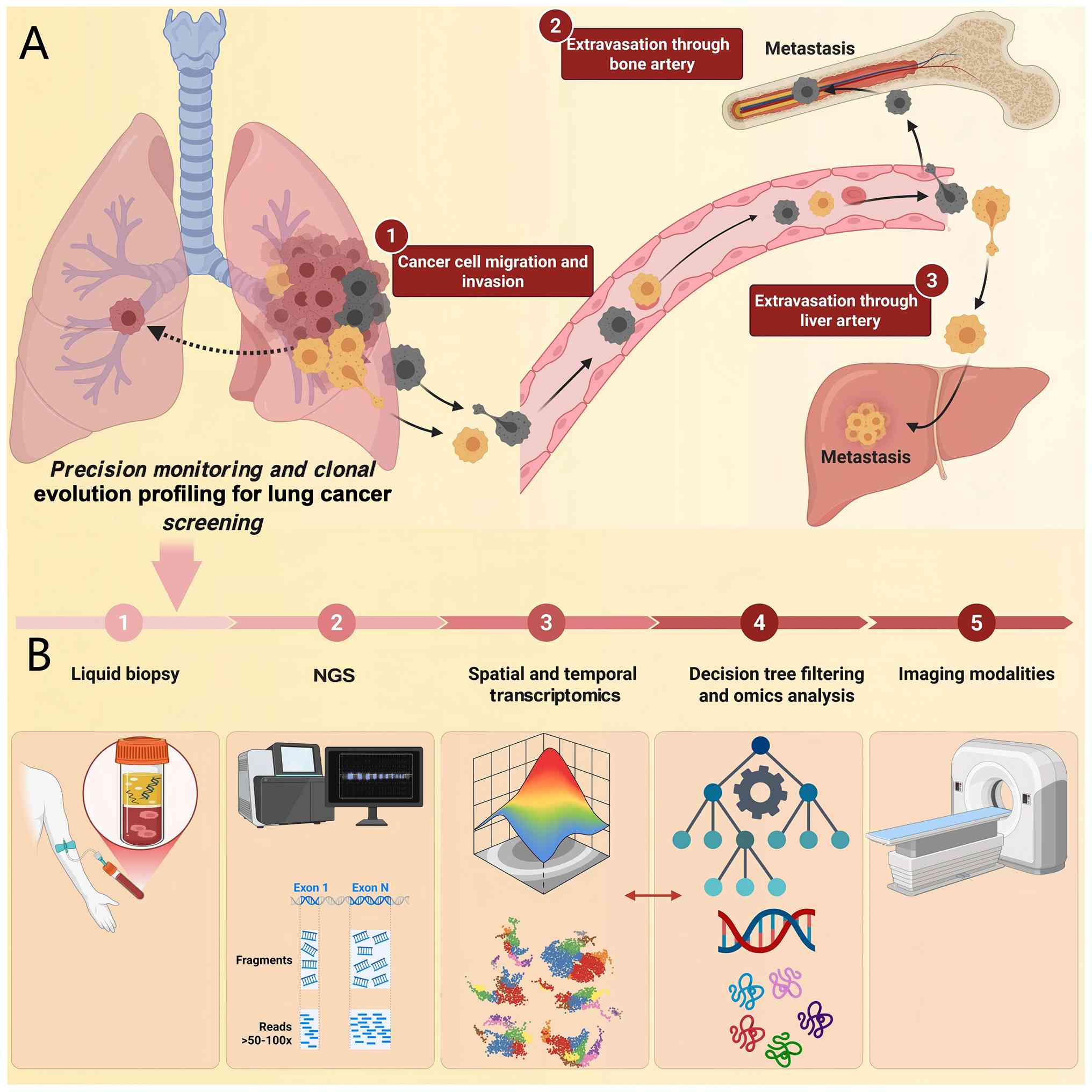
complex clonal dissemination pattern (Fig. 1). Research has indicated that
different metastases may originate from distinct subclonal
populations within the primary tumor, forming independently through
‘parallel evolution’, or arising from a single disseminated
subclone that subsequently undergoes independent genomic and
phenotypic evolution under the selective pressures of different
organ-specific microenvironments (17,18).
Recent Tracking Cancer Evolution through therapy/Rx (TRACERx)
analyses of 421 patients with NSCLC have determined the
evolutionary patterns of metastases. Frankell et al
(19) found that subclonal
whole-genome doubling (19% of tumors) was associated with shorter
disease-free survival and Al Bakir et al (20) showed that 25% of metastases diverged
before the last clonal sweep in the primary tumor; single-region
sampling would misclassify 83% of late divergence cases as early
dissemination. These findings underscore the need for extensive
spatiotemporal sampling to capture clonal architecture. Such
differentiation in evolutionary paths results in marked disparities
between metastatic sites in the distribution of key driver gene
mutations (including EGFR, anaplastic lymphoma kinase and KRAS),
tumor mutational burden and immune microenvironment features, such
as programmed death-ligand 1 (PD-L1) expression levels and the
composition and density of tumor-infiltrating lymphocytes (21–23).
This biological process may explain a key clinical challenge: When
therapy is targeted against a specific metastasis, failure to
effectively cover the dominant, genotypically and phenotypically
diverse subclonal populations in other lesions may lead to the
rapid progression of these untreated sites in the absence of
competitive suppression (24,25).
This finding underscores the necessity of fully accounting for
intertumor heterogeneity when formulating treatment strategies for
advanced NSCLC. It also highlights the importance of combining
systemic therapy with local interventions.
Temporal heterogeneity, referring to the dynamic
evolutionary process of clonal populations under therapeutic
selection pressure, serves as a primary driver of acquired
resistance (6,26). Circulating tumor DNA (ctDNA)
sequencing, a mainstay in liquid biopsy, provides a pivotal,
non-invasive technical means for the real-time dissection of this
evolutionary process (9), enabling
the capacity to observe the longitudinal evolution of the genomic
landscape in NSCLC.
The core principles of liquid biopsy lie in its
utility as a dynamic monitoring tool for clonal evolution. In
comparison with the static information provided by single-timepoint
tissue biopsies, longitudinal ctDNA analysis enables continuous
tracking of the evolutionary trajectory of tumor genomes (9). Quantitative analysis of the variant
allele frequency of specific gene mutations allows for inferences
regarding dynamic changes in clonal population structure, thereby
facilitating the reconstruction of tumor phylogenetic trees
(6,7). Notable research has indicated that
clonal evolutionary patterns hold marked prognostic importance:
Patients exhibiting highly ‘branched evolutionary’ patterns (such
as concurrent development of numerous subclones) typically
experience worse clinical outcomes compared with patients
exhibiting ‘linear evolutionary’ patterns, attributable to their
higher intratumor heterogeneity and more complex potential
resistance mechanisms (6). The
TRACERx study quantified branching evolution in NSCLC, whereby
Frankell et al (19)
identified subclonal selection for 22 of 40 common cancer genes in
lung adenocarcinoma and copy-number heterogeneity predicted
extrathoracic relapse within 1 year after surgery. These
NSCLC-specific data reinforce the prognostic importance of branched
evolution. Longitudinal ctDNA analyses have also revealed the rise
and fall of dominant clones under the pressure of targeted therapy,
providing direct evidence for the dynamic selection process of
resistant clones (6,9).
Furthermore, ctDNA analysis may serve as an early
warning system for resistance-associated genetic alterations.
Clinical evidence has demonstrated that the emergence or marked
increase in the abundance of resistance-associated gene mutations
can be detected in ctDNA prior to the determination of disease
progression by radiographic assessment (26–28).
Wang et al (29) proposed a
risk-adaptive stratification strategy integrating baseline ctDNA
genotyping with ctDNA-molecular residual disease monitoring to
guide individualized decisions regarding consolidation
immunotherapy after chemoradiotherapy in locally advanced NSCLC.
This study suggested that serine/threonine kinase 11/kelch-like
ECH-associated protein 1 mutations not only predict radiotherapy
resistance but also suggest a potential benefit from
post-radiotherapy immunotherapy, illustrating an adaptive treatment
paradigm guided by genotype-therapy interactions. In EGFR-mutant
NSCLC, serial ctDNA monitoring can preemptively identify resistance
events mediated by EGFR T790M, C797S mutations (including cis/trans
configurations), MET amplification or bypass activation pathways
(26). This ‘lead time’ provides a
key window for clinical intervention, making it possible to adjust
treatment strategies before the onset of clinical symptoms or
radiographic progression, thereby fostering novel clinical
management paradigms such as ‘pre-emptive therapy’ (30). Notably, ctDNA abundance shows a
notable positive association with total tumor burden in the body,
establishing it as a highly sensitive pharmacodynamic biomarker
(31,32). A rapid decrease or clearance of
ctDNA levels following therapeutic intervention has been markedly
associated with objective response rate and longer progression-free
survival, whereas the persistence or early rebound of ctDNA levels
often indicates poor treatment response or primary resistance
(28,32). This dynamic profile provides a
rationale for the real-time assessment of therapeutic efficacy and
for the future exploration of biomarker-guided adaptive therapy
strategies. Beyond ctDNA, other components of liquid biopsies, such
as circulating tumor cells (CTCs) and tumor-derived exosomes, can
provide complementary information (33,34).
CTCs can be utilized for in vitro functional studies, while
exosomes carry molecular information including proteins and RNA,
aiding in the analysis of tumor phenotypic states and intercellular
communication (35,36).
Despite this, given the relative advantages of ctDNA
analysis with regard to technical standardization, detection
sensitivity and specificity and clinical accessibility, it
currently remains the most widely used and evidence-supported
component of liquid biopsy in both research and clinical practice
(37,38). Fig.
1 illustrates how primary tumor subclones disseminate through
the bloodstream to the bone and liver, forming metastatic lesions
with distinct characteristics (spatial heterogeneity). Serial
liquid biopsy tracks ctDNA dynamics, in which changes in allele
frequency reveal clonal evolution and the emergence of early
resistance. This real-time monitoring enables pre-emptive
intervention before radiographic progression, thereby translating
heterogeneity into an actionable clinical strategy.
In response to the challenges posed by
heterogeneity, novel therapeutic strategies are shifting from a
sole focus on ‘maximal cell kill’ towards more strategic
management.
This concept, drawing from evolutionary biology,
aims to actively steer tumor clonal populations towards evolving
into states that are more drug-sensitive or confer a proliferative
disadvantage rather than passively awaiting the emergence of
resistance. Its theoretical basis leverages the fitness cost
experienced by resistant cancer cells relative to their sensitive
counterparts in specific contexts (25,39).
For instance, clones resistant to certain EGFR inhibitors may
regain sensitivity to chemotherapeutic agents or become dependent
on a targetable bypass signaling pathway (40,41).
Clinical applications include alternating therapies with distinct
mechanisms of action or employing low-dose metronomic chemotherapy.
These strategies aim to suppress dominant clones while preserving
populations of sensitive cells that can suppress the expansion of
resistant clones, thereby preventing their rapid proliferation due
to ‘competitive release’ (39,42).
Niche intervention strategies have represented a
shift in therapeutic paradigm. The core premise lies in targeting
the tumor microenvironment (TME), which sustains cancer cell
survival, promotes proliferation and mediates immune escape. This
may prove more effective compared with direct targeting of the
heterogeneous cancer cells themselves. This strategy is based on
the understanding that the TME, acting as the ‘soil’ supporting
tumor growth, promotes disease progression by facilitating immune
evasion, angiogenesis, invasion and metastasis (43,44).
Consequently, systematically remodeling this microenvironment from
a pro-tumor to an anti-tumor state can indirectly and sustainably
control the proliferation, invasion and development of acquired
resistance in diverse cancer cell ‘seeds’ within it. Compared with
directly targeting genotypically diverse and dynamically evolving
tumor cells, niche intervention acts upon relatively stable
host-derived components of the TME, thereby offering broader
therapeutic applicability and the potential for more durable
efficacy.
A primary direction of niche intervention is
reversing the immunosuppressive microenvironment, which is densely
infiltrated by M2-type tumor-associated macrophages (TAMs),
myeloid-derived suppressor cells (MDSCs) and Tregs. These cells
create a physical and functional barrier that impairs effector
immune cells through inhibitory cytokines, immune checkpoint
molecules and metabolic competition (45,46).
Targeting key recruitment and activation pathways of these cells,
for instance, depleting M2 macrophages by antagonizing
colony-stimulating factor 1 receptor or inhibiting MDSC recruitment
by blocking C-C chemokine receptor (CCR)-2/CCR5 signaling, has been
shown in preclinical models to convert immunologically ‘cold’
tumors (T-cell-poor, non-inflamed) into ‘hot’ ones (T-cell-rich,
inflamed), thereby restoring the capacity of the host immune system
to recognize and eliminate diverse cancer cell clones (47–49).
TAMs serve a central role in NSCLC progression. Larionova et
al (50) demonstrated that TAMs
secrete VEGF amongst other pro-angiogenic factors, including
semaphorin, S100A family members and chitinase-like proteins,
limiting the efficacy of anti-angiogenic therapy. In addition,
Huang et al (51)
systematically summarized TAM-mediated resistance mechanisms in
NSCLC and proposed targeting TAMs to overcome resistance.
Meanwhile, cancer-associated fibroblasts (CAFs) participate in
immune regulation by suppressing immune cell function and promoting
immune evasion, primarily through upregulation of COX2/PD-L1 and
secretion of TGF-β/IL-10 (52).
These findings suggest that targeting TAMs and CAFs to remodel the
tumor microenvironment niche represents a promising therapeutic
strategy for NSCLC. In addition, targeting the TGF-β signaling
pathway may not only suppress the activation of cancer-associated
fibroblasts, but also alleviate its potent suppression of T cell
function, demonstrating dual potential in reshaping the immune
microenvironment (53,54).
An additional key strategy involves targeting the
metabolic niche of the tumor. Tumor cells, through reprogramming
their own metabolism and engaging in metabolic coupling with
stromal cells within the TME, promote a local environment that is
acidic, hypoxic and nutrient-depleted. This environment, in turn,
selects for and promotes the expansion of more adaptable clones
(55–57). Drugs targeting key metabolic
pathways shared by tumor cells and immune cells, such as adenosine
pathway antagonists (e.g., A2A/A2B receptor antagonists like
inupadenant and PBF-1129, and CD73 inhibitors like oleclumab and
uliledlimab) and IDO1 inhibitors (e.g., epacadostat), aim to
ameliorate nutrient competition within the TME and relieve
metabolic immunosuppression, thereby indirectly inhibiting cancer
cell growth (58,59).
Furthermore, intervening in the formation of the
pre-metastatic niche represents a long-term application of niche
intervention. The primary tumor systemically remodels the
microenvironment of distant organs via secreted factors (e.g.,
TGF-β, VEGF, LOXL2) and tumor-derived exosomes (carrying integrins,
miRNAs and proteins), making them more conducive for the
colonization of circulating tumor cells, thus forming a
pre-metastatic niche (60–62). Research has suggested that targeting
key molecules involved in this process, such as TGF-β and lysyl
oxidase-like 2, may disrupt the ‘seeding’ process of metastasis in
specific organs, spatially restricting the success rate of clonal
dissemination (63–65).
Radiation therapy is also emerging as a potential
tool for niche intervention. Traditionally viewed primarily as a
local cytotoxic modality (66),
recent studies have indicated that radiotherapy can systemically
reshape the TME by inducing immunogenic cell death, releasing
tumor-associated antigens and inflammatory factors, thereby
activating anti-tumor immune responses and exerting an ‘in
situ vaccine’ effect (67–69).
Among radiotherapy techniques, stereotactic body radiotherapy
(SBRT), known for its high precision and high biologically
effective dose, has garnered notable attention for its ability to
modulate the tumor immune microenvironment (70). Studies have demonstrated synergistic
effects when SBRT is combined with immune checkpoint inhibitors
(70–72). For example, a randomized phase II
trial showed that SBRT combined with nivolumab markedly increased
the response rate of non-irradiated distant lesions (the ‘abscopal
effect’) demonstrating that SBRT can induce a systemic anti-tumor
immune response (72). This finding
highlights the paradigm shift of radiotherapy as a niche
intervention tool, moving from local modulation to systemic immune
activation.
Metabolic niche intervention represents another
emerging frontier. Research has indicated that the composition of
the gut microbiota is a key regulator in the efficacy of programmed
cell death protein 1/PD-L1 inhibitors, with the abundance of
specific beneficial bacterial species being associated with
improved treatment response, thus offering a new target for
improving immunotherapy through microbiota modulation (73). Shan et al (74) reported a novel laser
desorption/ionization time-of-flight mass spectrometry method based
on a gold nanoparticles/cellulose nanocrystals nanocomposite for
direct and highly sensitive detection of intact proteins in NSCLC
serum exosomes. This method identified five characteristic
proteins, namely S100 calcium binding protein A10, urokinase-type
plasminogen activator receptor, C1 inhibitor, FGR proto-oncogene,
Src family tyrosine kinase and mannan-binding lectin serine
protease-2, as effective predictive biomarkers of NSCLC risk,
offering a new technical avenue for liquid biopsy. On the other
hand, in-depth studies of driver mutations such as isocitrate
dehydrogenase 1R132H reveal that they induce profound
metabolic reprogramming in tumor cells by prompting the production
of unique oncometabolites (including 2-hydroxyglutarate) (75–77).
This distinct metabolic dependency itself presents a promising
window for therapeutic intervention.
In summary, the niche intervention strategy, by
systemically modulating the local and systemic environments upon
which tumors depend, offers a novel approach to overcoming the
challenges posed by tumor heterogeneity to direct targeting
strategies. Despite this field facing challenges such as target
specificity, off-target effects and a lack of biomarkers, its
therapeutic philosophy, aimed at altering the fundamental
properties of the tumor ecosystem, represents a key evolutionary
direction in cancer treatment paradigms.
Adaptive therapy represents a paradigm shift,
transitioning the therapeutic objective from ‘maximal cell kill’
towards the long-term control of tumor population dynamics.
Grounded in evolutionary dynamics, this strategy aims to stabilize
tumor burden at a controllable level by modulating therapeutic
selection pressure and leveraging the competitive suppression of
resistant cancer cells by their sensitive counterparts, thereby
delaying the emergence of resistance (39,42).
The core hypothesis of adaptive therapy is that
intrinsic competition exists between drug-sensitive and
drug-resistant cancer cells within the tumor microenvironment
(25,77–79).
Conventional high-dose continuous therapy [e.g., daily
EGFR-tyrosine kinase inhibitor (TKI) or fixed-schedule
chemotherapy], while rapidly reducing tumor volume, simultaneously
eliminates the ecological suppression of resistant cells by
sensitive cells, leading to the rapid expansion of resistant clones
(25,42). By contrast, adaptive therapy employs
dynamically adjusted treatment regimens (including dose reduction
or treatment holidays) intended to maintain a population of
sensitive cells, thereby continuously suppressing the proliferation
advantage of resistant subclones. Mathematical modeling has
demonstrated the potential of this strategy to markedly prolong the
disease control period (39,78).
Its implementation relies on two key elements: i) Reliable
biomarkers for the real-time assessment of tumor burden and clonal
composition; and ii) Pre-defined decision algorithms to guide
treatment adjustments. ctDNA sequencing therefore provides an ideal
tool for this purpose; longitudinal monitoring of specific mutant
allele frequencies allows quantification of the relative
proportions of different clones, establishing a data-driven basis
for therapeutic intervention (9,28,80).
Preclinical models and clinical studies have
demonstrated notable advantages for adaptive therapy (42,81,82).
For instance, in animal models, dynamically adjusting chemotherapy
regimens based on drug sensitivity testing results markedly
extended survival compared with standard fixed-dose regimens
(42). Clinical evidence also
supports the feasibility of ctDNA-guided adaptive therapy in NSCLC.
In a non-randomized controlled trial of 60 patients with advanced
NSCLC who achieved complete remission after targeted therapy and
local consolidative treatment, Dong et al (81) reported a median progression-free
survival of 18.4 months using a ctDNA-guided adaptive de-escalation
TKI strategy. Notably, 23% of patients required no further TKI
treatment and 52% received intermittent TKI retreatment based on
ctDNA or CEA levels before radiographic progression, suggesting
that ctDNA serves as a reliable trigger for treatment re-initiation
(81). Thus, this strategy may be
clinically feasible in a subset of patients with advanced NSCLC.
Real-world data from Noronha et al (82) further demonstrated that
reduced-frequency osimertinib dosing is a viable alternative for
patients unable to tolerate full-dose daily therapy, supporting
individualized dose modulation. Collectively, these studies provide
initial clinical proof-of-concept that biomarker-driven adaptive
therapy can prolong disease control and potentially reduce
treatment burden and toxicity.
The ongoing Canadian Cancer Trials Group BR.36 trial
(trial ID: NCT04767061) is prospectively evaluating ctDNA molecular
response-adaptive immuno-chemotherapy in metastatic NSCLC. Its
first stage validated the feasibility of ctDNA-based response
monitoring, demonstrating that early ctDNA dynamics can guide
treatment adjustment (83). This
trial exemplifies the integration of ctDNA kinetics into adaptive
immunotherapy regimens. The primary challenges facing adaptive
therapy include developing accurate predictive models, determining
optimal thresholds for treatment adjustment and addressing
complexities introduced by tumor clonal plasticity. Furthermore,
this personalized, dynamic treatment model poses new requirements
for traditional clinical trial design and regulatory approval
frameworks. By viewing cancer as a dynamic evolutionary system and
intervening using ecological principles, adaptive therapy offers a
promising new avenue for achieving long-term control in NSCLC. With
advancements in precision monitoring technologies (such as
longitudinal ctDNA and spatial multi-omics) and computational
biology (including AI-driven evolutionary modeling), this strategy
is poised to become an important component in addressing tumor
heterogeneity and drug resistance. Table I summarizes the comparison of
emerging treatment strategies targeting spatiotemporal
heterogeneity in NSCLC.
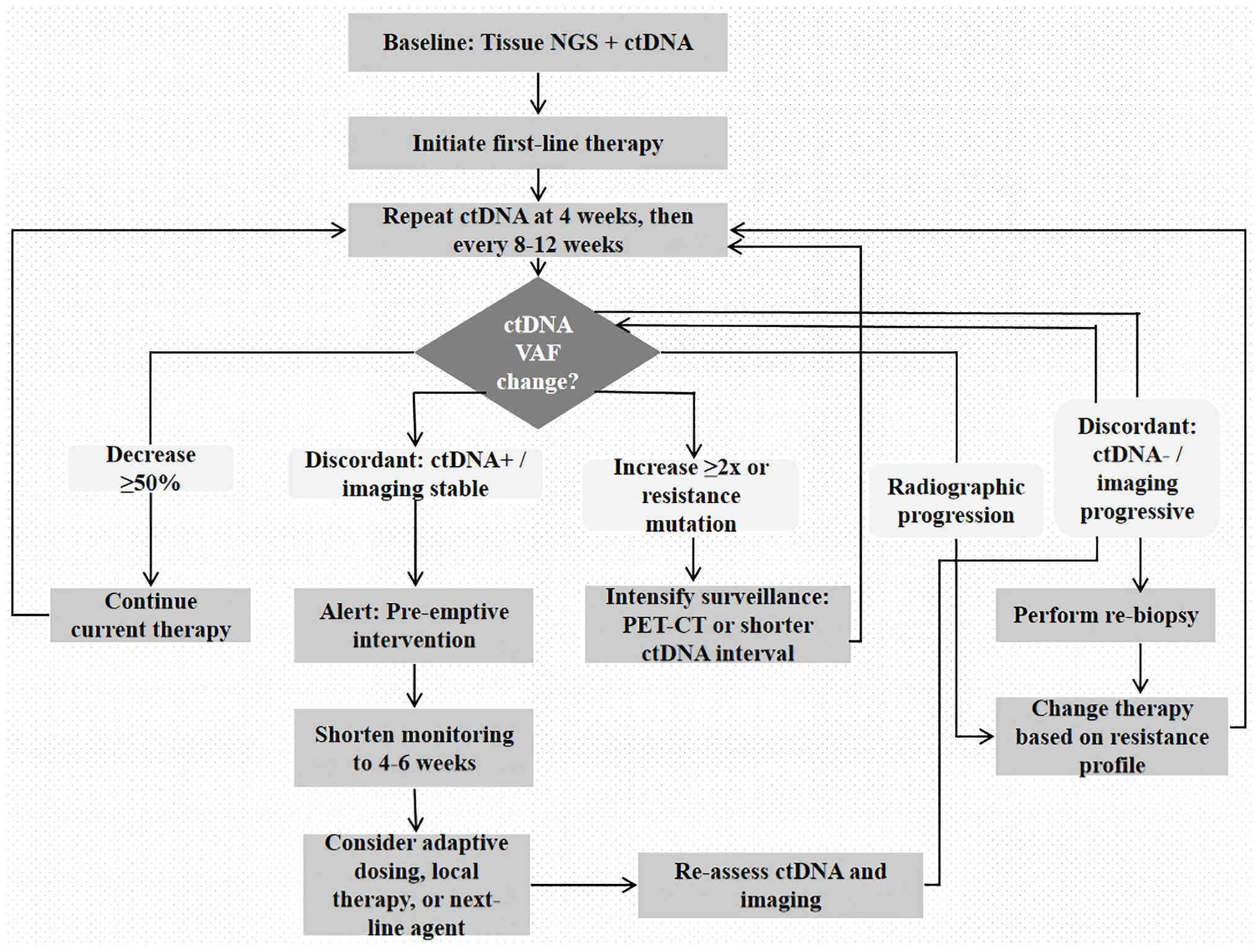
Furthermore, to translate dynamic management into
practice, the present review proposes a ctDNA-based algorithm
(Fig. 2) outlining baseline
assessment, monitoring frequency (week 4, then every 8–12 weeks),
response thresholds (≥50% variant allele frequency decrease),
warning signals (≥2X increase or resistance mutation) and
management of progression or discordant findings.
Despite the marked promise of novel therapeutic
strategies based on spatiotemporal heterogeneity, their clinical
translation faces numerous challenges. Technically, the application
of spatial multi-omics technologies is still limited by high
technical barriers, complex data analysis and a lack of
standardization; the detection sensitivity of liquid biopsy in
patients with early-stage tumors or low tumor burden requires
further improvement. Biologically, the phenotypic plasticity of
tumor cells and non-genetic resistance mechanisms increase the
complexity of predicting clonal evolution. From a clinical
translation perspective, dynamic treatment strategies pose
transformative demands on traditional clinical trial designs,
efficacy evaluation criteria and regulatory approval
frameworks.
Beyond biological and technical complexities,
clinical translation faces multiple practical barriers.
Cost-effectiveness remains a concern, as spatial multi-omics and
liquid biopsy are still expensive with limited reimbursement
coverage. Turnaround time for spatial omics (1–2 weeks) and liquid
biopsy (7–14 days) may exceed the decision window for rapidly
progressive NSCLC. Accessibility differs notably between academic
centers and community hospitals, exacerbating healthcare
disparities (84). Regarding
standardization, data comparability across different platforms
(such as 10× vs. Vizgen) (85) and
ctDNA assays remains poor. International consortia (including
SpaceTx; http://spacetx-starfish.readthedocs.io/) are working
on advancing benchmarking and quality control, yet widespread
clinical harmonization remains a future goal. Overcoming these
barriers is important in translating the dynamic management
paradigm into real-world NSCLC care.
Future research efforts should thus focus on the
following key areas: i) Innovating clinical trial paradigms:
Promoting the adoption of adaptive designs, such as platform and
umbrella trials, as mainstream approaches and establishing endpoint
indicators and statistical models suitable for evaluating dynamic
therapies; ii) deep integration of multi-omics data: Leveraging
artificial intelligence and machine learning algorithms to
integrate multidimensional information from genomics,
transcriptomics and the microenvironment for constructing
high-precision predictive models of clonal evolution; iii)
optimizing dynamic treatment strategies: Exploring the synergistic
effects of different treatment modalities with adaptive dosing and
establishing individualized treatment algorithms based on real-time
biomarker feedback; and iv) promoting technical standardization and
accessibility: Reducing the costs of multi-omics technologies,
establishing standardized data analysis pipelines and facilitating
their widespread clinical adoption.
In summary, overcoming the challenge of
spatiotemporal heterogeneity in NSCLC necessitates surmounting
technical bottlenecks, deepening biological understanding and
innovating clinical practice models. Through multidisciplinary
collaborative innovation, the paradigm shift in NSCLC management,
from reactive response to proactive control, can ultimately be
realized.
Spatiotemporal heterogeneity is an intrinsic
property of NSCLC as a dynamic evolutionary system and constitutes
a key reason for the limitations of current treatment paradigms.
Overcoming this bottleneck necessitates a paradigm shift: froma
static, molecular-subtyping-driven approach towards a dynamic,
evolution-focused strategy that emphasizes continuous monitoring
and adaptive intervention. Advanced technologies have provided us
with the initial capability to map the spatiotemporal atlas of
NSCLC. Emerging strategies, such as evolutionary trap therapy,
niche intervention and adaptive therapy, offer promising directions
for transitioning the treatment goal from ‘eradication’ to
‘intelligent management’. Future success will therefore depend on
the integration of tumor biology, evolutionary ecology,
computational science and clinical medicine, with the ultimate
objective being to transform NSCLC into a chronic disease that can
be controlled long-term.
Not applicable.
Funding: No funding was received.
The data generated in the present study may be
requested from the corresponding author.
LC contributed to the conceptualization, design,
analysis and writing of the original and subsequent drafts. WZ was
responsible for interpretation of the data and reviewed and edited
the manuscript. All authors read and approved the final version of
the manuscript. Data authentication is not applicable.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Bray F, Laversanne M, Sung H, Ferlay J,
Siegel RL, Soerjomataram I and Jemal A: Global cancer statistics
2022: GLOBOCAN estimates of incidence and mortality worldwide for
36 cancers in 185 countries. CA Cancer J Clin. 74:229–263.
2024.PubMed/NCBI
|
|
2
|
Zhou J, Xu Y, Liu J, Feng L, Yu J and Chen
D: Global burden of lung cancer in 2022 and projections to 2050:
Incidence and mortality estimates from GLOBOCAN. Cancer Epidemiol.
93:1026932024. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mok TS, Wu YL, Thongprasert S, Yang CH,
Chu DT, Saijo N, Sunpaweravong P, Han B, Margono B, Ichinose Y, et
al: Gefitinib or carboplatin-paclitaxel in pulmonary
adenocarcinoma. N Engl J Med. 361:947–957. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Garon EB, Rizvi NA, Hui R, Leighl N,
Balmanoukian AS, Eder JP, Patnaik A, Aggarwal C, Gubens M, Horn L,
et al: Pembrolizumab for the treatment of non-small-cell lung
cancer. N Engl J Med. 372:2018–2028. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Pao W, Miller VA, Politi KA, Riely GJ,
Somwar R, Zakowski MF, Kris MG and Varmus H: Acquired resistance of
lung adenocarcinomas to gefitinib or erlotinib is associated with a
second mutation in the EGFR kinase domain. PLoS Med. 2:e732005.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jamal-Hanjani M, Wilson GA, McGranahan N,
Birkbak NJ, Watkins TBK, Veeriah S, Shafi S, Johnson DH, Mitter R,
Rosenthal R, et al: Tracking the evolution of non-small-cell lung
cancer. N Engl J Med. 376:2109–2121. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Gerlinger M, Rowan AJ, Horswell S, Math M,
Larkin J, Endesfelder D, Gronroos E, Martinez P, Matthews N,
Stewart A, et al: Intratumor heterogeneity and branched evolution
revealed by multiregion sequencing. N Engl J Med. 366:883–892.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ståhl PL, Salmén F, Vickovic S, Lundmark
A, Navarro JF, Magnusson J, Giacomello S, Asp M, Westholm JO, Huss
M, et al: Visualization and analysis of gene expression in tissue
sections by spatial transcriptomics. Science. 353:78–82. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Abbosh C, Birkbak NJ, Wilson GA,
Jamal-Hanjani M, Constantin T, Salari R, Le Quesne J, Moore DA,
Veeriah S, Rosenthal R, et al: Phylogenetic ctDNA analysis depicts
early-stage lung cancer evolution. Nature. 545:446–451. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Navin N, Kendall J, Troge J, Andrews P,
Rodgers L, McIndoo J, Cook K, Stepansky A, Levy D, Esposito D, et
al: Tumour evolution inferred by single-cell sequencing. Nature.
472:90–94. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
de Bruin EC, McGranahan N, Mitter R, Salm
M, Wedge DC, Yates L, Jamal-Hanjani M, Shafi S, Murugaesu N, Rowan
AJ, et al: Spatial and temporal diversity in genomic instability
processes defines lung cancer evolution. Science. 346:251–256.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zhang J, Fujimoto J, Zhang J, Wedge DC,
Song X, Zhang J, Seth S, Chow CW, Cao Y, Gumbs C, et al: Intratumor
heterogeneity in localized lung adenocarcinomas delineated by
multiregion sequencing. Science. 346:256–259. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tirosh I, Izar B, Prakadan SM, Wadsworth
MH II, Treacy D, Trombetta JJ, Rotem A, Rodman C, Lian C, Murphy G,
et al: Dissecting the multicellular ecosystem of metastatic
melanoma by single-cell RNA-seq. Science. 352:189–196. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wu TD, Madireddi S, de Almeida PE,
Banchereau R, Chen YJ, Chitre AS, Chiang EY, Iftikhar H, O'Gorman
WE, Au-Yeung A, et al: Peripheral T cell expansion predicts tumour
infiltration and clinical response. Nature. 579:274–278. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Rahal Z, El Darzi R, Moghaddam SJ, Cascone
T and Kadara H: Tumour and microenvironment crosstalk in NSCLC
progression and response to therapy. Nat Rev Clin Oncol.
22:463–482. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yang L, Zhang W, Sun J, Yang G, Cai S, Sun
F, Xing L and Sun X: Functional status and spatial interaction of T
cell subsets driven by specific tumor microenvironment correlate
with recurrence of non-small cell lung cancer. Front Immunol.
13:10226382023. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hunter KW, Amin R, Deasy S, Ha NH and
Wakefield L: Genetic insights into the morass of metastatic
heterogeneity. Nat Rev Cancer. 18:211–223. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yates LR, Knappskog S, Wedge D, Farmery
JHR, Gonzalez S, Martincorena I, Alexandrov LB, Van Loo P, Haugland
HK, Lilleng PK, et al: Genomic evolution of breast cancer
metastasis and relapse. Cancer Cell. 32:169–184.e7. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Frankell AM, Dietzen M, Al Bakir M, Lim
EL, Karasaki T, Ward S, Veeriah S, Colliver E, Huebner A, Bunkum A,
et al: The evolution of lung cancer and impact of subclonal
selection in TRACERx. Nature. 616:525–533. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Al Bakir M, Huebner A, Martínez-Ruiz C,
Grigoriadis K, Watkins TBK, Pich O, Moore DA, Veeriah S, Ward S,
Laycock J, et al: The evolution of non-small cell lung cancer
metastases in TRACERx. Nature. 616:534–542. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Wang Z, Duan J, Cai S, Han M, Dong H, Zhao
J, Zhu B, Wang S, Zhuo M, Sun J, et al: Assessment of blood tumor
mutational burden as a potential biomarker for immunotherapy in
patients with non-small cell lung cancer with use of a
next-generation sequencing cancer gene panel. JAMA Oncol.
5:696–702. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Robinson DR, Wu YM, Lonigro RJ, Vats P,
Cobain E, Everett J, Cao X, Rabban E, Kumar-Sinha C, Raymond V, et
al: Integrative clinical genomics of metastatic cancer. Nature.
548:297–303. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Mansfield AS, Aubry MC, Moser JC,
Harrington SM, Dronca RS, Park SS and Dong H: Temporal and spatial
discordance of programmed cell death-ligand 1 expression and
lymphocyte tumor infiltration between paired primary lesions and
brain metastases in lung cancer. Ann Oncol. 27:1953–1958. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
McGranahan N and Swanton C: Clonal
heterogeneity and tumor evolution: Past, present, and the future.
Cell. 168:613–628. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Gatenby RA, Brown J and Vincent T: Lessons
from applied ecology: Cancer control using an evolutionary double
bind. Cancer Res. 69:7499–7502. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Oxnard GR, Hu Y, Mileham KF, Husain H,
Costa DB, Tracy P, Feeney N, Sholl LM, Dahlberg SE, Redig AJ, et
al: Assessment of resistance mechanisms and clinical implications
in patients with EGFR T790M-positive lung cancer and acquired
resistance to osimertinib. JAMA Oncol. 4:1527–1534. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Oxnard GR, Paweletz CP, Kuang Y, Mach SL,
O'Connell A, Messineo MM, Luke JJ, Butaney M, Kirschmeier P,
Jackman DM and Jänne PA: Noninvasive detection of response and
resistance in EGFR-mutant lung cancer using quantitative
next-generation genotyping of cell-free plasma DNA. Clin Cancer
Res. 20:1698–1705. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chaudhuri AA, Chabon JJ, Lovejoy AF,
Newman AM, Stehr H, Azad TD, Khodadoust MS, Esfahani MS, Liu CL,
Zhou L, et al: Early detection of molecular residual disease in
localized lung cancer by circulating tumor DNA profiling. Cancer
Discov. 7:1394–1403. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wang Y, Li C, Zhang T, Wang J, Liu W, Deng
L, Jiang Y, Duan J, Wang L, Ge H and Bi N: Circulating genomic
biomarkers predict chemoradiotherapy resistance and immunotherapy
response in locally advanced non-small-cell lung cancer. VIEW.
6:e202401452025. View Article : Google Scholar
|
|
30
|
Siravegna G, Marsoni S, Siena S and
Bardelli A: Integrating liquid biopsies into the management of
cancer. Nat Rev Clin Oncol. 14:531–548. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Bettegowda C, Sausen M, Leary RJ, Kinde I,
Wang Y, Agrawal N, Bartlett BR, Wang H, Luber B, Alani RM, et al:
Detection of circulating tumor DNA in early- and late-stage human
malignancies. Sci Transl Med. 6:224ra242014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Diehl F, Schmidt K, Choti MA, Romans K,
Goodman S, Li M, Thornton K, Agrawal N, Sokoll L, Szabo SA, et al:
Circulating mutant DNA to assess tumor dynamics. Nat Med.
14:985–990. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Cristofanilli M, Budd GT, Ellis MJ,
Stopeck A, Matera J, Miller MC, Reuben JM, Doyle GV, Allard WJ,
Terstappen LW and Hayes DF: Circulating tumor cells, disease
progression, and survival in metastatic breast cancer. N Engl J
Med. 351:781–791. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Sandfeld-Paulsen B, Aggerholm-Pedersen N,
Bæk R, Jakobsen KR, Meldgaard P, Folkersen BH, Rasmussen TR,
Varming K, Jørgensen MM and Sorensen BS: Exosomal proteins as
prognostic biomarkers in non-small cell lung cancer. Mol Oncol.
10:1595–1602. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Yu M, Bardia A, Wittner BS, Stott SL, Smas
ME, Ting DT, Isakoff SJ, Ciciliano JC, Wells MN, Shah AM, et al:
Circulating breast tumor cells exhibit dynamic changes in
epithelial and mesenchymal composition. Science. 339:580–584. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Alix-Panabières C and Pantel K: Clinical
applications of circulating tumor cells and circulating tumor DNA
as liquid biopsy. Cancer Discov. 6:479–491. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Chen C, Douglas MP, Ragavan MV, Phillips
KA and Jansen JP: Clinical validity and utility of circulating
tumor DNA (ctDNA) testing in advanced non-small cell lung cancer
(aNSCLC): A systematic literature review and meta-analysis. Mol
Diagn Ther. 28:525–536. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Ge Q, Zhang ZY, Li SN, Ma JQ and Zhao Z:
Liquid biopsy: Comprehensive overview of circulating tumor DNA
(review). Oncol Lett. 28:5482024. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Gatenby RA, Silva AS, Gillies RJ and
Frieden BR: Adaptive therapy. Cancer Res. 69:4894–903. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Sequist LV, Waltman BA, Dias-Santagata D,
Digumarthy S, Turke AB, Fidias P, Bergethon K, Shaw AT, Gettinger
S, Cosper AK, et al: Genotypic and histological evolution of lung
cancers acquiring resistance to EGFR inhibitors. Sci Transl Med.
3:75ra262011. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Engelman JA, Zejnullahu K, Mitsudomi T,
Song Y, Hyland C, Park JO, Lindeman N, Gale CM, Zhao X, Christensen
J, et al: MET amplification leads to gefitinib resistance in lung
cancer by activating ERBB3 signaling. Science. 316:1039–1043. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Enriquez-Navas PM, Kam Y, Das T, Hassan S,
Silva A, Foroutan P, Ruiz E, Martinez G, Minton S, Gillies RJ and
Gatenby RA: Exploiting evolutionary principles to prolong tumor
control in preclinical models of breast cancer. Sci Transl Med.
8:327ra242016. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Hanahan D and Weinberg RA: Hallmarks of
cancer: The next generation. Cell. 144:646–674. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Özdemir BC, Pentcheva-Hoang T, Carstens
JL, Zheng X, Wu CC, Simpson TR, Laklai H, Sugimoto H, Kahlert C,
Novitskiy SV, et al: Depletion of carcinoma-associated fibroblasts
and fibrosis induces immunosuppression and accelerates pancreas
cancer with reduced survival. Cancer Cell. 25:719–734. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Binnewies M, Roberts EW, Kersten K, Chan
V, Fearon DF, Merad M, Coussens LM, Gabrilovich DI,
Ostrand-Rosenberg S, Hedrick CC, et al: Understanding the tumor
immune microenvironment (TIME) for effective therapy. Nat Med.
24:541–550. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Mantovani A, Marchesi F, Malesci A, Laghi
L and Allavena P: Tumour-associated macrophages as treatment
targets in oncology. Nat Rev Clin Oncol. 14:399–416. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Pyonteck SM, Akkari L, Schuhmacher AJ,
Bowman RL, Sevenich L, Quail DF, Olson OC, Quick ML, Huse JT,
Teijeiro V, et al: CSF-1R inhibition alters macrophage polarization
and blocks glioma progression. Nat Med. 19:1264–1272. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Lim SY, Yuzhalin AE, Gordon-Weeks AN and
Muschel RJ: Targeting the CCL2-CCR2 signaling axis in cancer
metastasis. Oncotarget. 7:28697–28710. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Sanford DE, Belt BA, Panni RZ, Mayer A,
Deshpande AD, Carpenter D, Mitchem JB, Plambeck-Suess SM, Worley
LA, Goetz BD, et al: Inflammatory monocyte mobilization decreases
patient survival in pancreatic cancer: A role for targeting the
CCL2/CCR2 axis. Clin Cancer Res. 19:3404–3415. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Larionova I, Kazakova E, Gerashchenko T
and Kzhyshkowska J: New angiogenic regulators produced by TAMs:
Perspective for targeting tumor angiogenesis. Cancers (Basel).
13:32532021. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Huang Z, Xiao Z, Yu L, Liu J, Yang Y and
Ouyang W: Tumor-associated macrophages in non-small-cell lung
cancer: From treatment resistance mechanisms to therapeutic
targets. Crit Rev Oncol Hematol. 196:1042842024. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Lee H, Hwang M, Jang S and Um SW: Immune
regulatory function of cancer-associated fibroblasts in non-small
cell lung cancer. Tuberc Respir Dis (Seoul). 86:304–318. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Mariathasan S, Turley SJ, Nickles D,
Castiglioni A, Yuen K, Wang Y, Kadel EE III, Koeppen H, Astarita
JL, Cubas R, et al: TGFβ attenuates tumour response to PD-L1
blockade by contributing to exclusion of T cells. Nature.
554:544–548. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Derynck R, Turley SJ and Akhurst RJ: TGFβ
biology in cancer progression and immunotherapy. Nat Rev Clin
Oncol. 18:9–34. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Pavlova NN and Thompson CB: The emerging
hallmarks of cancer metabolism. Cell Metab. 23:27–47. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Fiaschi T, Marini A, Giannoni E, Taddei
ML, Gandellini P, De Donatis A, Lanciotti M, Serni S, Cirri P and
Chiarugi P: Reciprocal metabolic reprogramming through lactate
shuttle coordinately influences tumor-stroma interplay. Cancer Res.
72:5130–5140. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Estrella V, Chen T, Lloyd M, Wojtkowiak J,
Cornnell HH, Ibrahim-Hashim A, Bailey K, Balagurunathan Y, Rothberg
JM, Sloane BF, et al: Acidity generated by the tumor
microenvironment drives local invasion. Cancer Res. 73:1524–1535.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Allard B, Longhi MS, Robson SC and Stagg
J: The ectonucleotidases CD39 and CD73: Novel checkpoint inhibitor
targets. Immunol Rev. 276:121–144. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Wang R, Liu Z, Wang T, Zhang J, Liu J and
Zhou Q: Landscape of adenosine pathway and immune checkpoint dual
blockade in NSCLC: Progress in basic research and clinical
application. Front Immunol. 15:13202442024. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Peinado H, Zhang H, Matei IR, Costa-Silva
B, Hoshino A, Rodrigues G, Psaila B, Kaplan RN, Bromberg JF, Kang
Y, et al: Pre-metastatic niches: Organ-specific homes for
metastases. Nat Rev Cancer. 17:302–317. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Hoshino A, Costa-Silva B, Shen TL,
Rodrigues G, Hashimoto A, Tesic Mark M, Molina H, Kohsaka S, Di
Giannatale A, Ceder S, et al: Tumour exosome integrins determine
organotropic metastasis. Nature. 527:329–335. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Liu Y and Cao X: Characteristics and
significance of the pre-metastatic niche. Cancer Cell. 30:668–681.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Padua D and Massagué J: Roles of TGFbeta
in metastasis. Cell Res. 19:89–102. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Padua D, Zhang XH, Wang Q, Nadal C, Gerald
WL, Gomis RR and Massagué J: TGFbeta primes breast tumors for lung
metastasis seeding through angiopoietin-like 4. Cell. 133:66–77.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Pan W, Gao X, Zhang X, Li Y, Zhao Q, Wang
D, Zhao M, Wu Z and Zhang Y: Exosomes promote pre-metastatic niche
formation in lung cancer. Cancer Cell Int. 25:3792025. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Cheng SH, Tu KY and Lee HH: The dynamic
duo: A narrative review on the synergy between stereotactic body
radiotherapy and immunotherapy in lung cancer treatment (review).
Oncol Rep. 52:962024. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Wang Y, Li Y, Yang Y, Swift M, Zhang Z, Wu
S, Sun Y and Yang K: In situ vaccination caused by diverse
irradiation-driven cell death programs. Theranostics. 14:1147–1167.
2024. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Chen X, Yang M, Huang Y, Tu J, Cai Y and
Yuan X: Molecular mechanisms underlying the abscopal effect induced
by radiotherapy and its synergistic translational potential with
immunotherapy. Ther Adv Med Oncol. 17:175883592513875342025.
View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Formenti SC and Demaria S: Combining
radiotherapy and cancer immunotherapy: A paradigm shift. J Natl
Cancer Inst. 105:256–265. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Theelen WSME, Peulen HMU, Lalezari F, van
der Noort V, de Vries JF, Aerts JGJV, Dumoulin DW, Bahce I,
Niemeijer AN, de Langen AJ, et al: Effect of pembrolizumab after
stereotactic body radiotherapy vs pembrolizumab alone on tumor
response in patients with advanced non-small cell lung cancer:
Results of the PEMBRO-RT phase 2 randomized clinical trial. JAMA
Oncol. 5:1276–1282. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Huang J, Theelen WSME, Belcaid Z, Najjar
M, van der Geest D, Singh D, Cherry C, Balan A, White JR, Wehr J,
et al: Combination of pembrolizumab and radiotherapy induces
systemic antitumor immune responses in immunologically cold
non-small cell lung cancer. Nat Cancer. 6:1676–1692. 2025.
View Article : Google Scholar : PubMed/NCBI
|
|
72
|
McBride S, Sherman E, Tsai CJ, Baxi S,
Aghalar J, Eng J, Zhi WI, McFarland D, Michel LS, Young R, et al:
Randomized phase II trial of nivolumab with stereotactic body
radiotherapy versus nivolumab alone in metastatic head and neck
squamous cell carcinoma. J Clin Oncol. 39:30–37. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
He Y, Fu L, Li Y, Wang W, Gong M, Zhang J,
Dong X, Huang J, Wang Q, Mackay CR, et al: Gut microbial
metabolites facilitate anticancer therapy efficacy by modulating
cytotoxic CD8+ T cell immunity. Cell Metab.
33:988–1000.e7. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Shan L, Qiao Y, Ma L, Zhang X, Chen C, Xu
X, Li D, Qiu S, Xue X, Yu Y, et al: AuNPs/CNC nanocomposite with A
‘dual dispersion’ effect for LDI-TOF MS analysis of intact proteins
in NSCLC serum exosomes. Adv Sci (Weinh). 11:e23073602024.
View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Yan B, Hu Y, Ma T and Wang Y: IDH1
mutation promotes lung cancer cell proliferation through
methylation of Fibulin-5. Open Biol. 8:1800862018. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Rodriguez EF, De Marchi F, Lokhandwala PM,
Belchis D, Xian R, Gocke CD, Eshleman JR, Illei P and Li MT: IDH1
and IDH2 mutations in lung adenocarcinomas: Evidences of subclonal
evolution. Cancer Med. 9:4386–4394. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Dang L, White DW, Gross S, Bennett BD,
Bittinger MA, Driggers EM, Fantin VR, Jang HG, Jin S, Keenan MC, et
al: Cancer-associated IDH1 mutations produce 2-hydroxyglutarate.
Nature. 462:739–744. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Zhang J, Cunningham JJ, Brown JS and
Gatenby RA: Integrating evolutionary dynamics into treatment of
metastatic castrate-resistant prostate cancer. Nat Commun.
8:18162017. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Aktipis CA, Kwan VS, Johnson KA, Neuberg
SL and Maley CC: Overlooking evolution: A systematic analysis of
cancer relapse and therapeutic resistance research. PLoS One.
6:e261002011. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Wan JCM, Massie C, Garcia-Corbacho J,
Mouliere F, Brenton JD, Caldas C, Pacey S, Baird R and Rosenfeld N:
Liquid biopsies come of age: Towards implementation of circulating
tumour DNA. Nat Rev Cancer. 17:223–238. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Dong S, Wang Z, Zhang JT, Yan B, Zhang C,
Gao X, Sun H, Li YS, Yan HH, Tu HY, et al: Circulating tumor
DNA-guided de-escalation targeted therapy for advanced non-small
cell lung cancer: A nonrandomized controlled trial. JAMA Oncol.
10:932–940. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Noronha V, Sahu H, Kapoor A, Patil V,
Menon N, Shah M, Davis D, Roy R, Vivek S, Janu A, et al: Reduced
frequency dosing of osimertinib in EGFR-mutant non-small cell lung
carcinoma: real world data. Ecancermedicalscience. 18:17212024.
View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Anagnostou V, Ho C, Nicholas G, Juergens
RA, Sacher A, Fung AS, Wheatley-Price P, Laurie SA, Levy B, Brahmer
JR, et al: ctDNA response after pembrolizumab in non-small cell
lung cancer: Phase 2 adaptive trial results. Nat Med. 29:2559–2569.
2023. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Ramalingam S, Dinan MA and Crawford J:
Survival comparison in patients with stage IV lung cancer in
academic versus community centers in the United States. J Thorac
Oncol. 13:1842–1850. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Wang H, Huang R, Nelson J, Gao C, Tran M,
Yeaton A, Krishna S, Felt K, Pfaff KL, Bowman T, et al: Systematic
benchmarking of imaging spatial transcriptomics platforms in FFPE
tissues. Nat Commun. 16:102152025. View Article : Google Scholar : PubMed/NCBI
|