Introduction
The emergence of immune checkpoint inhibitors (ICIs)
has been a breakthrough in the treatment of various types of
cancer, including melanoma and non-small cell lung cancer (NSCLC).
Programmed cell death-1/programmed death-ligand 1 (PD-L1)
inhibitors are the most commonly used ICIs and have shown excellent
efficacy in a variety of advanced diseases, including NSCLC
(1,2). Tislelizumab, an immune checkpoint
inhibitor approved for the treatment of NSCLC, has been reported to
be associated with superior progression-free survival (PFS) and
overall survival (OS) compared with chemotherapy in clinical trials
(3,4). While ICIs have achieved a breakthrough
in treatment efficacy, immune-related adverse events (irAEs) due to
ICI administration have also received widespread attention. Among
all types of irAEs that may damage different organs of the body,
checkpoint inhibitor pneumonitis (CIP) is one of the potentially
life-threatening AEs, particularly in patients with NSCLC (5,6). A
large-scale clinical trial reported a 3–5% incidence of CIP in
patients with NSCLC, whereas a higher incidence of 19% was reported
in a real-world study (7,8). Corticosteroids are recommended as the
first-line treatment for the management of a wide variety of irAEs
according to the European Society For Medical Oncology and American
Society of Clinical Oncology guidelines (9,10).
However, biological immunomodulatory agents, such as infliximab and
tocilizumab, are recommended in patients with steroid-refractory or
steroid-resistant irAEs.
Interleukin-6 (IL-6) is a well-known proinflammatory
cytokine with pleiotropic biological functions that is considered
to have a prominent role in the development of irAEs (11,12).
Tocilizumab, a novel recombinant humanized anti-IL-6-receptor
(anti-IL-6R) monoclonal antibody, inhibits the IL-6 signaling
pathway by binding both membrane-bound and soluble forms of the
IL-6R (13). At present,
tocilizumab is mainly used for the treatment of inflammatory
autoimmune diseases, such as rheumatoid arthritis and systemic
onset juvenile idiopathic arthritis (13). In 2017, the U.S. Food and Drug
Administration approved tocilizumab for the treatment of severe or
potentially life-threatening cytokine release syndrome (CRS)
induced by chimeric antigen receptor-T cells in adults and children
≥2 years of age (14).
Additionally, tocilizumab has shown good efficacy in the treatment
of steroid-refractory irAEs. For instance, in a single-center study
involving 34 patients with steroid refractory irAEs receiving
tocilizumab treatment, 79.4% of patients exhibited clinical
improvement (15). However, there
are limited reports on the treatment of CIP with tocilizumab. The
present study reports a clinical experience of using tocilizumab to
treat tislelizumab-related pneumonitis after ineffective
corticosteroid therapy in a patient with stage IV lung cancer.
Case report
A 62-year-old man was admitted to Qingdao Central
Hospital, University of Health and Rehabilitation Sciences
(Qingdao, China) after complaining of lower back pain that had
persisted for 1 month in June 2020. The patient had a 40-pack-year
history of smoking and a 10-year history of refractory type 2
diabetes. A chest computed tomography (CT) scan indicated a
2.1×2.0-cm cavitary mass in the right lower lung alongside
vertebral metastases (Fig. S1).
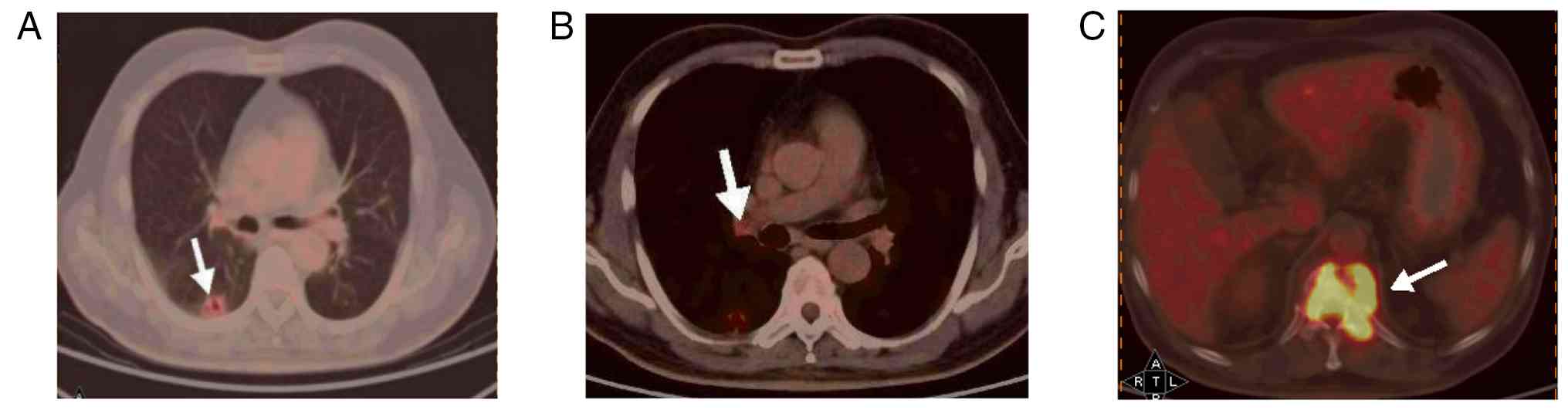
18F-FDG positron emission tomography revealed
right-sided lung cancer with right hilar lymph node metastasis and
vertebral metastases ranging from the 10th thoracic vertebra to the
1st lumbar vertebra (Fig. 1).
Magnetic resonance imaging (MRI) of the thoracic and lumbar spine
also showed vertebral metastasis (Fig.
S2). The histological diagnosis was obtained by a CT
scan-guided biopsy of the thoracic vertebral lesions. The specimen
was fixed in 10% neutral buffered formalin at room temperature for
24–48 h, sectioned at 4 µm and stained with hematoxylin and eosin
at room temperature for 5 and 1 min, respectively. The stained
slides were examined under a light microscope (ECLIPSE Ci-plus;
Nikon Corporation), confirming metastatic squamous cell carcinoma
(Figs. S3 and S4). The PD-L1 expression was assessed by
immunohistochemistry using the 22C3 pharmDx assay on the Dako
Autostainer Link 48 platform (cat. no. PRDT_711205; Agilent
Technologies, Inc.). Formalin-fixed, paraffin-embedded tissue
sections (4 µm) were stained according to the manufacturer's
protocol. Tissues were fixed in 10% neutral buffered formalin (room
temperature; 24–48 h). After deparaffinization, antigen retrieval
was performed at 97°C for 20 min, followed by washing with wash
buffer and rehydration through a descending alcohol series
according to the manufacturer's protocol. The stained slides were
examined under a light microscope (ECLIPSE Ci-plus), and the tumor
proportion score (TPS) was evaluated. The result was interpreted as
the TPS defined as the percentage of viable tumor cells exhibiting
partial or complete membrane staining. The PD-L1 (22C3)
immunohistochemistry assay indicated that the TPS was 40% (Fig. S4). Immunohistochemical analysis of
p40, cytokeratin (CK)5/6, CK7 and thyroid transcription factor 1
(TTF1) (Fig. S4) was performed on
formalin-fixed, paraffin-embedded tissue sections from the thoracic
vertebral lesion using the same automated immunostainer and
following the same protocol as described for PD-L1. After antigen
retrieval, sections were blocked with 5% normal goat serum (Vector
Laboratories, Inc.) at room temperature for 30 min. The following
primary antibodies were applied at 4°C overnight: Anti-p40 (1:100;
GT233807; Gene Tech Biotechnology Co., Ltd.), anti-CK5/6 (1:200;
MAB-0744; Fuzhou Maixin Biotechnology Development Co., Ltd.),
anti-CK7 (1:50; GM701807; Gene Tech Biotechnology Co., Ltd.) and
anti-TTF1 (1:100; MAB-0599; Fuzhou Maixin Biotechnology Development
Co., Ltd.). HRP-conjugated secondary antibody was applied using the
ultraView Universal DAB Detection Kit (cat. no. 760–500; Roche
Tissue Diagnostics; Roche Diagnostics, Ltd.) without additional
dilution. After incubation at room temperature for 1 h, staining
was visualized with 3,3′-diaminobenzidine and counterstaining was
performed with hematoxylin at room temperature (25°C) for 2 min.
Positive staining for p40, CK5/6 and CK7, and negative staining for
TTF1 confirmed the diagnosis of metastatic lung squamous cell
carcinoma. Consequently, the patient was diagnosed with stage IV
(cT2N1M1; 8th edition of the American Joint Committee on Cancer
Cancer Staging Manual) lung squamous cell carcinoma with right
hilar lymph node and vertebral metastases (16).
To alleviate pain and prevent skeletal-related
events, the patient first received hyperfractionated radiotherapy
for the vertebral metastases at doses of 30 and 40 Gy in 10
fractions to the planning target volume and the planning gross
target volume, respectively. After radiotherapy, the patient began
receiving treatment with albumin-bound paclitaxel (300 mg on day
1), nedaplatin (120 mg on day 1) and tislelizumab (200 mg on day 1)
every 3 weeks starting from August 2020. Nedaplatin was removed
from the second cycle due to grade 3 myelosuppression (Common
Terminology Criteria for Adverse Events 5.0) (17). Imaging after two cycles of
chemo-immunotherapy showed stable disease. After receiving the
third cycle, the patient presented with a fever, cough and
shortness of breath. A chest CT scan in late October 2020
demonstrated ground-glass opacities (GGOs), reticular opacities and
consolidations predominantly in the peripheral and lower lung
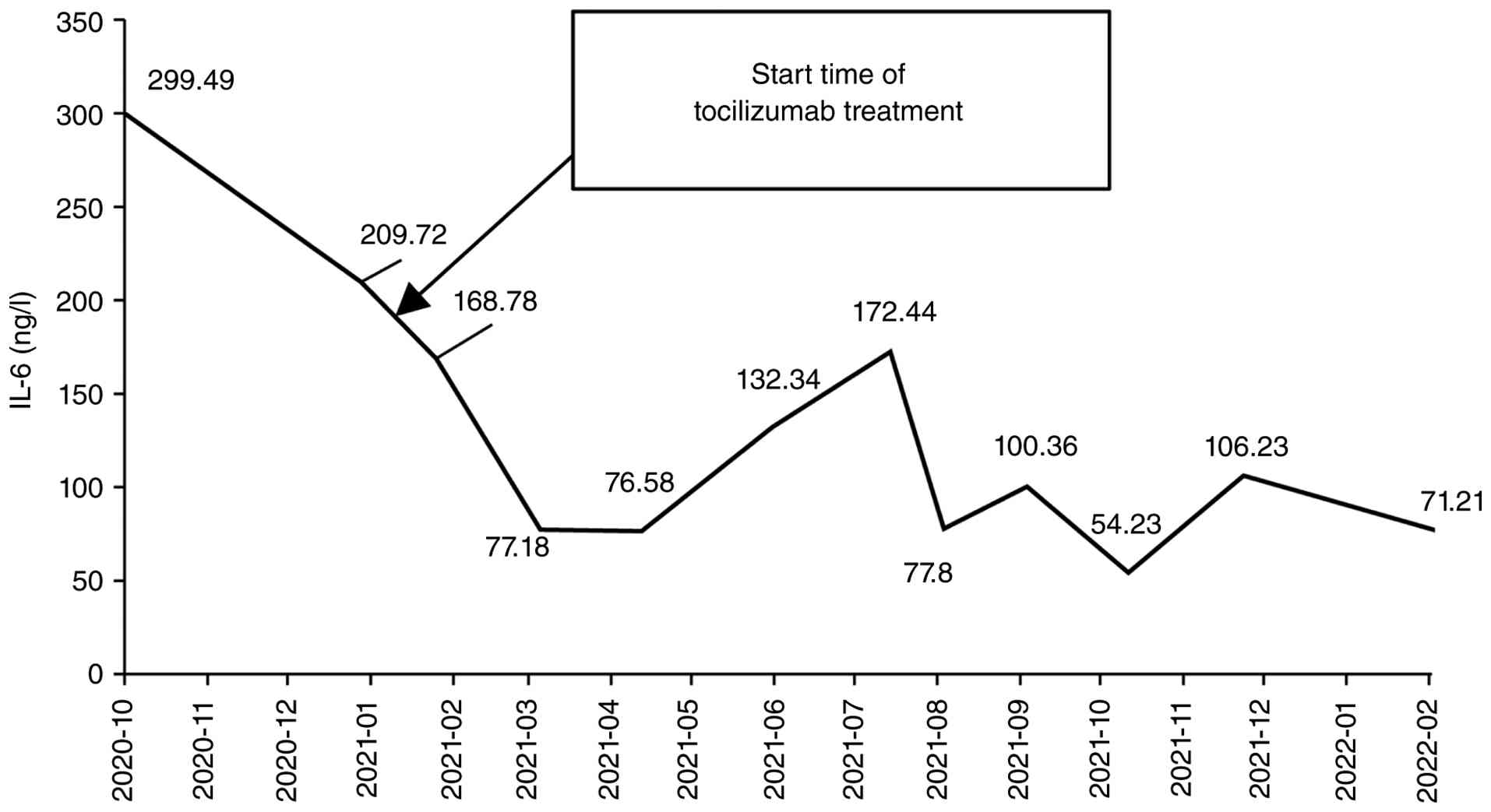
(Fig. 2A and B). The plasma IL-6
levels were markedly elevated and reached 299.45 ng/l (normal
range, 0–5.4 ng/l). CT-guided lung biopsy from the consolidation of
the lower lobe of the right lung, processed in the same manner as
the previous specimens, showed inflammation of the lung tissue and
fibrous tissue hyperplasia (Fig.
S5). Considering the treatment history combined with the
negative results from the pathogenic microbiological tests, the
patient was diagnosed with grade 2 CIP according to the American
Society of Clinical Oncology (ASCO) guideline with a cryptogenic
organizing pneumonia pattern (10).
The chemo-immunotherapy was subsequently suspended. The patient
received an initial intravenous dose of methylprednisolone at 60 mg
per day (~1 mg/kg), which was then gradually tapered off over 12
days until discontinuation, with close monitoring of blood glucose
changes to control hyperglycemia. CT images collected in November
2020 showed notable radiographic improvement after corticosteroid
treatment (Fig. 2C and D). The
patient also experienced marked clinical improvement of the cough
and shortness of breath. After this, the dosage of corticosteroid
was gradually decreased until it was discontinued.
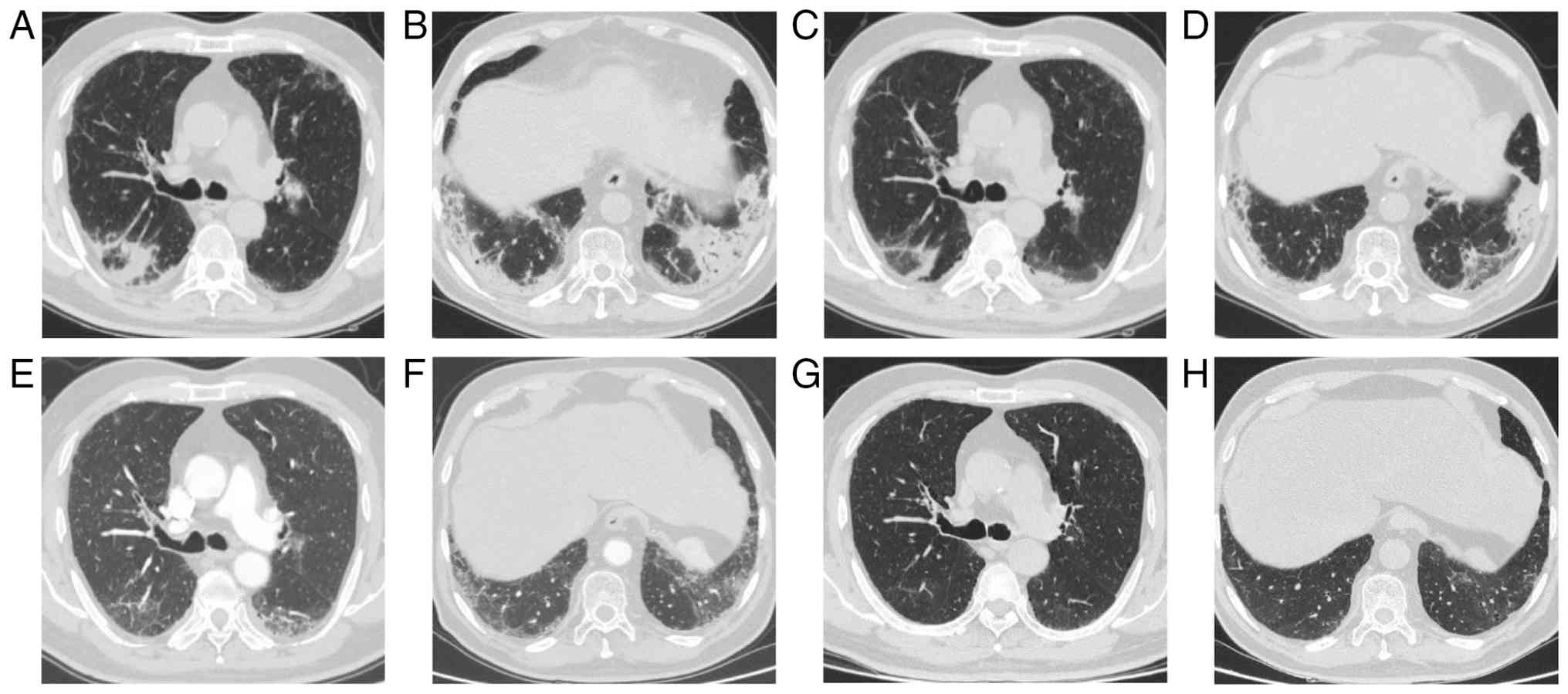
However, 1.5 months after the discontinuation of
corticosteroids and without restarting systemic therapy, the
patient developed dyspnea and a worsening cough again. The chest CT
scan collected in December 2020 demonstrated multifocal areas of
consolidation, reticular opacities and GGOs in the peripheral and
bilateral lower lungs, which were more pronounced than when they
first appeared (Fig. 3A and B).
Additionally, the plasma IL-6 levels were markedly elevated and
reached 209.72 ng/l (Fig. 4). To
block the IL-6R, the patient received four cycles of tocilizumab at
4 mg/kg every 3 weeks from January 2021 to April 2021. After
treatment with tocilizumab, the clinical symptoms and pneumonitis
rapidly and notably improved and then disappeared (Fig. 3C-H). A marked decrease in the plasma
IL-6 levels was also observed (Fig.
4).
During the follow-up period until February 2022, the
plasma IL-6 levels fluctuated, with a transient increase to near
pre-tocilizumab levels between May and July 2021 (peak, 172.44
ng/l), followed by a gradual decline to 71.21 ng/l by February
2022. Throughout this period, the CT images showed that the
pneumonitis remained in complete remission (Fig. S6). No AEs related to tocilizumab
were observed. Although the patient refused any anticancer therapy
from the first incidence of CIP, the tumor has remained in a stable
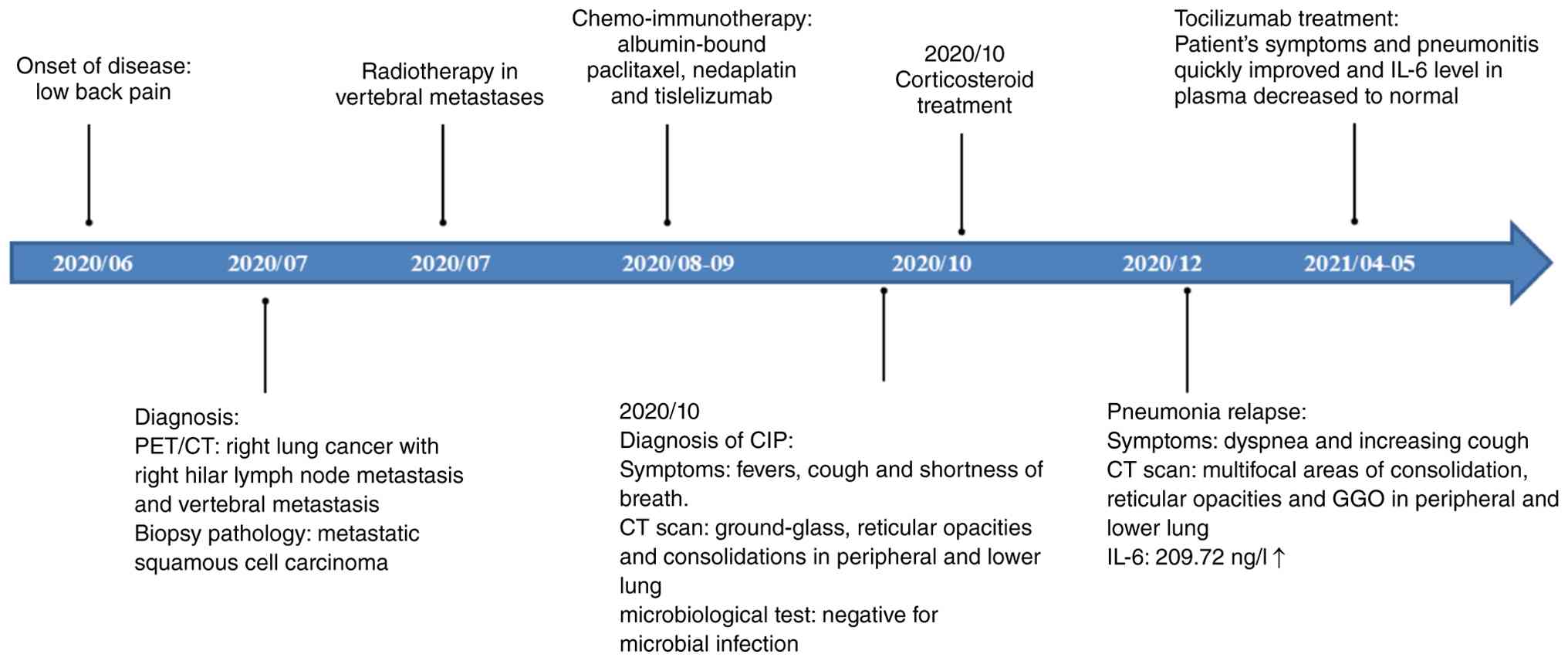
state and there has been no recurrence. As of the submission of the
manuscript, the PFS and OS times of the patient have both exceeded
60 months. The treatment timeline is shown in Fig. 5.
Discussion
Several published guidelines, including the European
Society for Medical Oncology Clinical Practice Guideline and the
ASCO Guideline Update, recommend corticosteroids as a first-line
treatment for the management of irAEs (9,10). For
most steroid-refractory and steroid-resistant irAEs, the guidelines
recommend biological immunomodulatory agents, such as infliximab,
mycophenolate mofetil or intravenous immunoglobulin, as second-line
treatment (18,19). Furthermore, emerging evidence
suggests that different immunopathogenic mechanisms, such as breach
of self-tolerance, cross-antigen reactivity, cytokine production,
off-target effects and microbiome-related factors (including
bacterial, fungal and viral components), result in irAEs (9). Therefore, a personalized treatment
strategy beyond the first-line regimen has been proposed for the
management of irAEs.
A number of inflammatory factors, such as IL-6 and
TNF-α, released during tumor immunotherapy can result in irAEs
(20,21). Among the inflammatory factors, IL-6
serves the most crucial role in the development of irAEs (including
CIP) (22,23). Tocilizumab, a novel recombinant
humanized anti-IL-6R monoclonal antibody, can block the IL-6
signaling pathway and thus disrupt the continuous development of
CIP and restore the damaged alveoli (13). A retrospective multicenter study
evaluated the effectiveness and safety of anti-IL-6R antibodies. A
total of 92 patients with irAEs received therapeutic anti-IL-6R
antibodies (sarilumab or tocilizumab), 73% of whom experienced
resolution or a reduction to grade ≤1 irAEs at a median time of 2.0
months after the initiation of anti-IL-6R therapy (24). This study provided indirect evidence
of IL-6 as one of the essential mediators of irAEs. In the present
study, the patient was diagnosed with CIP (grade 2) after receiving
three cycles of tislelizumab in combination with chemotherapy. The
patient then received a high dose of intravenous corticosteroids in
the first-line treatment of CIP. The patient initially responded to
this treatment but subsequently developed recurrent pneumonitis
(grade 3) after discontinuation of corticosteroids in the absence
of ICI rechallenge. Considering the notably elevated plasma IL-6
levels, the patient received tocilizumab treatment, which resulted
in a subsequent decrease in IL-6, as well as a marked improvement
in the symptoms and radiological findings. For this patient, the
clinical decision to use tocilizumab instead of
guideline-recommended alternatives, such as mycophenolate mofetil
or tacrolimus, was guided by a distinct biomarker profile (25). Specifically, the observation of a
notably elevated serum IL-6 level offered a compelling biological
rationale for selectively inhibiting the IL-6 pathway, rather than
initiating non-specific, broad-spectrum immunosuppression. This
approach exemplifies the shift toward a biomarker-directed,
personalized management strategy for steroid-refractory irAEs,
which aims to target dominant inflammatory pathways over empirical
treatment. Evidence from the present case suggests that blocking
IL-6R can be beneficial for mitigating CIP and that the anti-IL-6R
antibody, tocilizumab, may be an effective approach for the
management of CIP.
Tocilizumab has a marked effect in the management of
irAEs, but the optimal dose and frequency of tocilizumab for their
treatment remains unknown. The recommended dose of 8 mg/kg
tocilizumab has been approved for systemic juvenile idiopathic
arthritis (14). The current
evidence regarding the dosing of tocilizumab for irAEs is primarily
derived from retrospective case reports (15,26),
with no standardized guidelines established. The most commonly
reported regimen involves a single intravenous dose of 4 mg/kg,
which may be repeated at intervals of 2–4 weeks depending on the
clinical and radiological responses of the patients. Most patients
exhibit a response within 1 to 2 cycles of treatment. The total
number of treatment cycles is tailored to individual patient
response and clinical judgment, allowing for multiple cycles when
deemed necessary. In the present case, the patient was treated with
four cycles of 4 mg/kg tocilizumab. However, further study is still
needed to evaluate the optimal dose and frequency of tocilizumab
for the treatment of CIP. The safety of tocilizumab in the
treatment of irAEs is also a main concern. However, there is a lot
of available evidence supporting the safety of tocilizumab. The
most common AEs observed in tocilizumab studies are headaches,
upper respiratory tract infections and gastrointestinal events, but
most of them can be well tolerated (27). In a single-dose tocilizumab (10 or
20 mg/kg) study involving healthy subjects, neutropenia was the
only main dose-related toxicity (28). A retrospective analysis also
established the safety of 8 mg/kg tocilizumab for the treatment of
patients with T cell-induced CRS (14). A large retrospective study also
highlighted the efficacy and safety of tocilizumab in the treatment
of irAEs without hindering the ICI-induced tumor response (4). In the current patient with NSCLC,
short-term treatment with four cycles of tocilizumab was
demonstrated to be safe, with no treatment-related AEs observed. To
determine the optimal dosing regimen and timing of administration,
future studies should focus on prospective dose-finding trials
designed to evaluate the safety and efficacy of different dosing
strategies, such as comparing 4 vs. 8 mg/kg, and to establish the
most effective and safe treatment protocol.
Although irAEs are potentially life-threatening,
effective management of irAEs has been shown to be associated with
improved long-term survival in patients with NSCLC (29). A multicenter retrospective study
showed that patients with NSCLC whose CIP was successfully managed
achieved a significantly longer PFS time than those who did not
develop CIP (30). A meta-analysis
of 54 studies demonstrated that patients whose irAEs were
successfully managed achieved a significantly higher objective
response rate (odds ratio, 3.44), longer PFS time (HR, 0.51) and
longer OS time (HR, 0.58) than those without irAEs (31). In the present study, the observed
long-term PFS and OS are fundamentally attributed to the successful
management of CIP. This supports a key principle that effective
control of severe irAEs is a crucial foundation for ensuring
patient safety and the potential survival benefits of
immunotherapy. The present case demonstrates that tocilizumab may
serve as an effective salvage therapy for a specific subset of
steroid-refractory CIP characterized by significant activation of
the IL-6 pathway. Compared with long-term, high-dose corticosteroid
use, its targeted mechanism of action offers a potentially more
favorable risk-benefit profile. In contrast to other biological
agents or broad-spectrum immunosuppressants in this specific
context, tocilizumab exerts a more selective effect, which may
better align with the underlying disease pathophysiology. This
highlights the importance of individualized treatment approach
rather than a uniform strategy in the management of irAEs.
In conclusion, the present case suggests that IL-6
may be involved in the pathogenesis of irAEs and that tocilizumab
may be an effective treatment option for the personalized
management of CIP. As a single-case report, the findings may lack
generalizability. The response to tocilizumab observed in this
patient may not be representative of the entire population of
patients with NSCLC and CIP, and therefore, validation in larger
patient cohorts is necessary to confirm its efficacy, establish the
optimal dosing regimen and comprehensively evaluate its safety
profile. Furthermore, factors such as the patient's age, underlying
medical conditions, tumor characteristics and prior corticosteroid
use, as well as the timing and dosage of tocilizumab
administration, may have influenced the treatment outcomes.
Therefore, caution should be exercised when generalizing these
findings to other patients. Future rigorously designed prospective
studies are warranted to validate the association between
biomarkers such as IL-6 and treatment response to tocilizumab in a
broader patient population. Additionally, the management of irAEs
will become an important challenge for clinicians. Further
exploration of effective biomarkers for adverse reactions and
therapeutic targets is also needed to improve patient
prognosis.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
LY was the attending physician for the patient and
drafted the manuscript. QMG was responsible for testing and
analyzing the patient's plasma IL-6 levels and modified the
manuscript. YW and LL performed the treatment and follow-up of the
patient. FC collected the clinical data and obtained the CT and MRI
images. XTZ guided the treatment of the patient and conceptualized
the work. QMG and XTZ confirm the authenticity of all the raw data.
All authors have read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of Qingdao Central Hospital, University of Health and
Rehabilitation Sciences (approval no. KY202600401).
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of this case report and any
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Nishino M, Hatabu H and Hodi FS: Imaging
of cancer immunotherapy: Current approaches and future directions.
Radiology. 290:9–22. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Park H, Sholl LM, Hatabu H, Awad MM and
Nishino M: Imaging of precision therapy for lung cancer: Current
state of the art. Radiology. 293:15–29. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wang J, Lu S, Yu X, Hu Y, Zhao J, Sun M,
Yu Y, Hu C, Yang K, Song Y, et al: Tislelizumab plus chemotherapy
versus chemotherapy alone as first-line treatment for advanced
squamous non-small-cell lung cancer: Final analysis of the
randomized, phase III RATIONALE-307 trial. ESMO Open. 9:1037272024.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yue D, Wang W, Liu H, Chen Q, Chen C, Liu
L, Zhang P, Zhao G, Yang F, Han G, et al: Perioperative
tislelizumab plus neoadjuvant chemotherapy for patients with
resectable non-small-cell lung cancer (RATIONALE-315): An interim
analysis of a randomised clinical trial. Lancet Respir Med.
13:119–129. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sears CR, Peikert T, Possick JD, Naidoo J,
Nishino M, Patel SP, Camus P, Gaga M, Garon EB, Gould MK, et al:
Knowledge gaps and research priorities in immune checkpoint
Inhibitor-related pneumonitis. An Official American Thoracic
Society Research Statement. Am J Respir Crit Care Med. 200:e31–e43.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhang Q, Tang L, Zhou Y, He W and Li W:
Immune checkpoint Inhibitor-associated pneumonitis in Non-Small
cell lung cancer: Current understanding in characteristics,
diagnosis, and management. Front Immunol. 12:6639862021. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Khunger M, Jain P, Rakshit S, Pasupuleti
V, Hernandez AV, Stevenson J, Pennell NA and Velcheti V: Incidence
of pneumonitis with use of PD-1 and PD-L1 inhibitors in non-small
cell lung cancer: A systematic review and meta-analysis of trials.
Clin Lung Cancer. 19:e335–e348. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rizvi NA, Mazières J, Planchard D,
Stinchcombe TE, Dy GK, Antonia SJ, Horn L, Lena H, Minenza E,
Mennecier B, et al: Activity and safety of nivolumab, an anti-PD-1
immune checkpoint inhibitor, for patients with advanced, refractory
squamous non-small-cell lung cancer (CheckMate 063): A phase 2,
single-arm trial. Lancet Oncol. 16:257–265. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Haanen J, Obeid M, Spain L, Carbonnel F,
Wang Y, Robert C, Lyon AR, Wick W, Kostine M, Peters S, et al:
Management of toxicities from immunotherapy: ESMO Clinical Practice
Guideline for diagnosis, treatment and follow-up. Ann Oncol.
33:1217–1238. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Schneider BJ, Naidoo J, Santomasso BD,
Lacchetti C, Adkins S, Anadkat M, Atkins MB, Brassil KJ, Caterino
JM, Chau I, et al: Management of Immune-related adverse events in
patients treated with immune checkpoint inhibitor therapy: ASCO
guideline update. J Clin Oncol. 39:4073–4126. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hunter CA and Jones SA: IL-6 as a keystone
cytokine in health and disease. Nat Immunol. 16:448–457. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Naqash AR, Yang LV, Sanderlin EJ, Atwell
DC and Walker PR: Interleukin-6 as one of the potential mediators
of immune-related adverse events in non-small cell lung cancer
patients treated with immune checkpoint blockade: Evidence from a
case report. Acta Oncol. 57:705–708. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sebba A: Tocilizumab: The first
interleukin-6-receptor inhibitor. Am J Health Syst Pharm.
65:1413–1418. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Le RQ, Li L, Yuan W, Shord SS, Nie L,
Habtemariam BA, Przepiorka D, Farrell AT and Pazdur R: FDA approval
summary: Tocilizumab for treatment of chimeric antigen Receptor T
Cell-Induced severe or Life-Threatening cytokine release syndrome.
Oncologist. 23:943–947. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Stroud CR, Hegde A, Cherry C, Naqash AR,
Sharma N, Addepalli S, Cherukuri S, Parent T, Hardin J and Walker
P: Tocilizumab for the management of immune mediated adverse events
secondary to PD-1 blockade. J Oncol Pharm Pract. 25:551–557. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Amin MB, Edge SB, Greene FL, Byrd DR,
Brookland RK, Washington MK, Gershenwald JE, Compton CC, Hess KR,
Sullivan DC, et al: AJCC Cancer Staging Manual. (8th edition).
Springer International Publishing; 2017
|
|
17
|
Freites-Martinez A, Santana N,
Arias-Santiago S and Viera A: Using the common terminology criteria
for adverse events (CTCAE-Version 5.0) to evaluate the severity of
adverse events of anticancer therapies. Actas Dermosifiliogr (Engl
Ed). 112:90–92. 2021.(In English, Spanish). View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Reuss JE, Suresh K and Naidoo J:
Checkpoint inhibitor pneumonitis: Mechanisms, characteristics,
management strategies, and beyond. Curr Oncol Rep. 22:562020.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Esfahani K, Elkrief A, Calabrese C,
Lapointe R, Hudson M, Routy B, Miller WH and Calabrese L: Moving
towards personalized treatments of immune-related adverse events.
Nat Rev Clin Oncol. 17:504–515. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Xu Y, Fu Y, Zhu B, Wang J and Zhang B:
Predictive biomarkers of immune checkpoint Inhibitors-related
toxicities. Front Immunol. 11:20232020. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Wang M, Zhai X, Li J, Guan J, Xu S, Li Y
and Zhu H: The role of cytokines in predicting the response and
adverse events related to immune checkpoint inhibitors. Front
Immunol. 12:6703912021. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lin X, Deng H, Yang Y, Wu J, Qiu G, Li S,
Xie X, Liu M, Xie Z, Qin Y, et al: Peripheral blood biomarkers for
early diagnosis, severity, and prognosis of checkpoint
Inhibitor-related pneumonitis in patients with lung cancer. Front
Oncol. 11:6988322021. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kowalski B, Valaperti A, Bezel P, Steiner
UC, Scholtze D, Wieser S, Vonow-Eisenring M, Widmer A, Kohleret M
and Franzen D: Analysis of cytokines in serum and bronchoalveolar
lavage fluid in patients with immune-checkpoint
inhibitor-associated pneumonitis: A cross-sectional case-control
study. J Cancer Res Clin Oncol. 148:1711–1720. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Fa'ak F, Buni M, Falohun A, Lu H, Song J,
Johnson DH, Zobniw CM, Trinh VA, Awiwi MO, Tahon NH, et al:
Selective immune suppression using interleukin-6 receptor
inhibitors for management of immune-related adverse events. J
Immunother Cancer. 11:e0068142023. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Campochiaro C, Farina N, Tomelleri A,
Ferrara R, Lazzari C, De Luca G, Bulotta A, Signorelli D, Palmisano
A, Vignale D, et al: Tocilizumab for the treatment of
immune-related adverse events: A systematic literature review and a
multicentre case series. Eur J Intern Med. 93:87–94. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ke W, Zhang L and Dai Y: The role of IL-6
in immunotherapy of non-small cell lung cancer (NSCLC) with
immune-related adverse events (irAEs). Thorac Cancer. 11:835–839.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Smolen JS, Beaulieu A, Rubbert-Roth A,
Ramos-Remus C, Rovensky J, Alecock E, Woodworth T and Alten R:
Effect of interleukin-6 receptor inhibition with tocilizumab in
patients with rheumatoid arthritis (OPTION study): A double-blind,
placebo-controlled, randomised trial. Lancet. 371:987–997. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Grange S, Schmitt C, Banken L, Kuhn B and
Zhang X: Thorough QT/QTc study of tocilizumab after single-dose
administration at therapeutic and supratherapeutic doses in healthy
subjects. Int J Clin Pharmacol Ther. 49:648–655. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Maillet D, Corbaux P, Stelmes JJ, Dalle S,
Locatelli-Sanchez M, Perier-Muzet M, Duruisseaux M,
Kiakouama-Maleka L, Freyer G, Boespflug A, et al: Association
between immune-related adverse events and long-term survival
outcomes in patients treated with immune checkpoint inhibitors. Eur
J Cancer. 132:61–70. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Fujimoto D, Yoshioka H, Kataoka Y,
Morimoto T, Kim YH, Tomii K, Ishida T, Hirabayashi M, Hara S,
Ishitokoet M, et al: Efficacy and safety of nivolumab in previously
treated patients with non-small cell lung cancer: A multicenter
retrospective cohort study. Lung Cancer. 119:14–20. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lin L, Liu Y, Chen C, Wei A and Li W:
Association between immune-related adverse events and immunotherapy
efficacy in non-small-cell lung cancer: A meta-analysis. Front
Pharmacol. 14:11900012023. View Article : Google Scholar : PubMed/NCBI
|