Introduction
Malignant tumors represent one of the leading causes
of mortality worldwide, accounting for 9.7 million deaths in 2022
(1). Acute clinical deterioration
in patients with cancer, often necessitating admission to the
intensive care unit (ICU) for life support and organ replacement
therapy, can be triggered by tumor treatment-associated
complications (such as myelosuppression and infection) or by
disease progression itself (including cachexia, organ metastasis,
malignant pleural effusion or ascites) (2,3). The
in-ICU mortality rate among these patients is markedly higher
compared with that of non-oncological critically ill patients
(58.8% vs. 36.5%) (4), constituting
a particularly challenging clinical problem in the field of
critical care medicine. Consequently, accurately assessing their
mortality risk and identifying key prognostic factors are of
notable importance for guiding clinical decision-making, optimizing
the allocation of medical resources and ultimately improving
patient outcomes.
The lactate-to-albumin ratio (LAR) has gained
attention in critical care research as a novel biomarker that
provides an integrated measure of both tissue hypoxia and
inflammation-nutritional status (5,6). Even
under oxygen-sufficient conditions, tumor cells preferentially
generate energy through high-rate glycolysis, a metabolic process
that produces large amounts of lactate as the end product (7), in advanced or bulky tumors, metabolic
dysregulation within the body is exacerbated, leading to a marked
increase in lactate production. Furthermore, the onset of severe
complications such as sepsis can induce systemic hypoperfusion and
hypoxia, which impairs lactate clearance and further augments its
generation (8,9). In critically ill patients with cancer
admitted to the ICU, this dysregulated lactate metabolism often
signals a poor prognosis (10,11).
The LAR is a prognostic biomarker in conditions including sepsis,
heart failure and acute respiratory failure (12–15).
For instance, in critically ill patients with cirrhosis and sepsis,
LAR has exhibited an L-shaped nonlinear association with mortality
(inflection point at LAR=1.05) and has demonstrated an improved
predictive performance compared with albumin alone (16,17).
In community-acquired pneumonia, LAR has shown comparable efficacy
to traditional scoring systems (such as the pneumonia severity
index or confusion, uremia, respiratory rate, blood pressure, age ≥
65 years score) in predicting the need for ICU admission and
in-hospital mortality (18).
However, it remains unclear whether LAR holds prognostic value
specifically in critically ill patients with malignancy. Therefore,
the present study investigated the association between the LAR
index and prognosis in critically ill patients with cancer.
Materials and methods
Data source and study population
Data from the Medical Information Mart for Intensive
Care IV (MIMIC-IV) database(mimic.mit.edu/) was utilized in the
present study, developed by Beth Israel Deaconess Medical Center
(19). The MIMIC-IV database
contains de-identified clinical data from >400,000 ICU
admissions, encompassing comprehensive records such as patient
demographics, diagnoses, treatments and medications. All data is
rigorously anonymized in compliance with privacy regulations to
ensure patient confidentiality. The present authors completed the
required training course for MIMIC-IV and were granted access to
the database. As the database contains only de-identified
information, the requirement for informed consent was waived for
the present analysis.
Study population
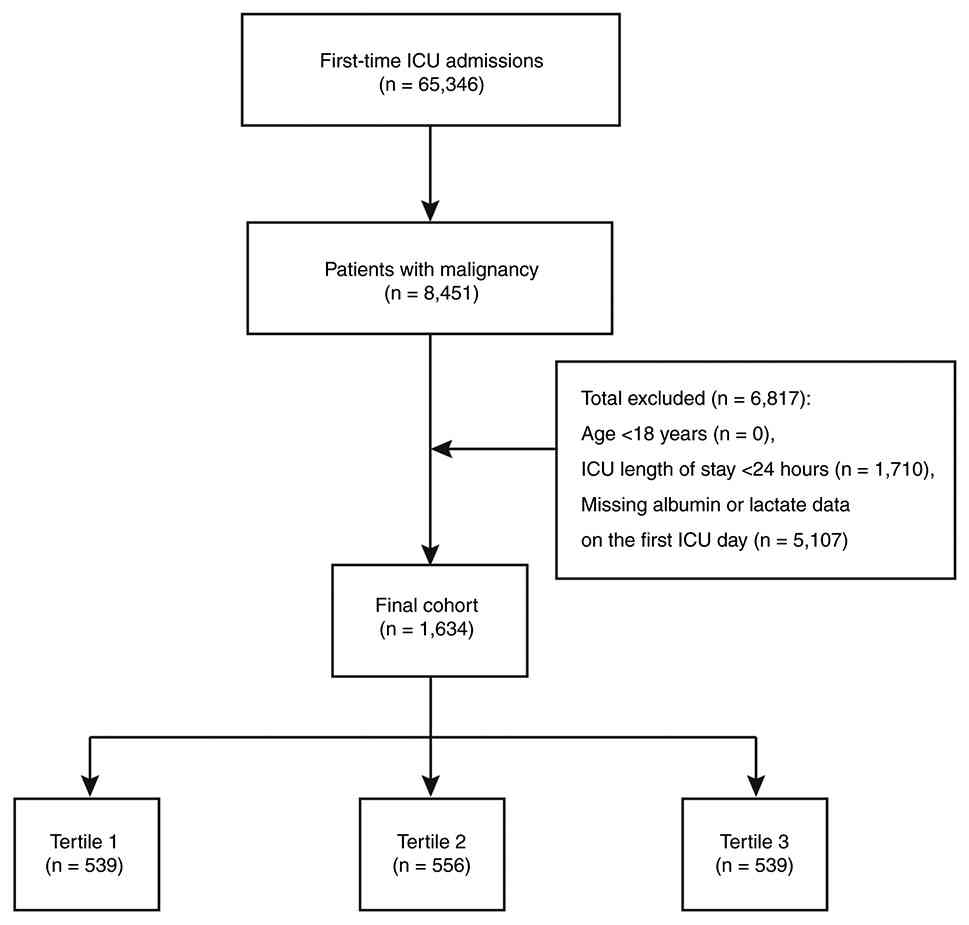
A total of 65,346 patients with their first ICU
admission were initially identified. From this cohort, 8,451
patients with a diagnosis of malignancy were selected based on the
Charlson Comorbidity Index (CCI) (20,21).
The following exclusion criteria were subsequently applied: i)
Patients aged under 18 years (n=0); ii) those with an ICU length of
stay <24 h (n=1,710); and iii) patients lacking lactate or
albumin measurements on the first day of ICU admission (n=5,107).
This resulted in the exclusion of 6,817 patients. Consequently, a
final cohort of 1,634 critically ill patients with malignancy was
included in the analysis. These patients were further stratified
into three groups according to their LAR values: Tertile 1 (T1;
n=539), tertile 2 (T2; n=556) and tertile 3 (T3; n=539; Fig. 1).
Data extraction
All data for the present study were extracted from
the MIMIC-IV database using PostgreSQL software (version 17.4,
postgresql.org/). The extracted data pertained to the first 24 h of
ICU admission and included: i) Baseline demographic information;
ii) vital signs; iii) severity-of-illness scores, including the
Sequential Organ Failure Assessment (SOFA) and Logistic Organ
Dysfunction System (LODS) score; iv) history of chronic
comorbidities (such as coronary artery disease, congestive heart
failure, cerebrovascular disease, chronic lung disease, liver
disease, diabetes or hypertension); v) laboratory parameters
measured within 24 h of ICU admission (including red blood cell
count, white blood cell count, platelet count, sodium, potassium,
calcium, glucose, lactate, albumin, anion gap, blood urea nitrogen
(BUN), creatinine, international normalized ratio (INR),
prothrombin time (PT), activated partial thromboplastin time (APTT)
and urine output); and vi) details regarding medication
administration and treatment regimens (such as epinephrine,
norepinephrine, mechanical ventilation and continuous renal
replacement therapy). Data regarding hospitalization-associated
outcomes were also collected, encompassing hospital and ICU length
of stay, as well as 30-day and 360-day all-cause in-hospital
mortality. Baseline laboratory data were defined as the first
measurements obtained within 24 h of ICU admission (rather than the
highest or lowest values) to reflect the initial physiological
status and minimize the influence of subsequent therapeutic
interventions.
Handling of missing data
In the present study, different strategies were
employed to handle missing data. For variables with a percentage of
missing values <20%, multiple imputation was applied to fill the
gaps. Specifically, the multiple imputation method was used to
generate several imputed datasets, thereby reducing the potential
bias associated with single imputation and ensuring the accuracy
and robustness of the imputed data (22). By contrast, variables with >20%
missing values were excluded from the subsequent analysis to
prevent their influence on the findings.
Definition of exposure and
outcomes
LAR, as the exposure of interest, was calculated
using the following formula: LAR=lactate (mmol/l)/albumin (mg/dl).
The values for both lactate and albumin were obtained from the
first 24 h following ICU admission. The primary outcome of the
present study was 30-day all-cause mortality. The secondary outcome
was 360-day all-cause mortality. Follow-up for all outcomes
commenced from the first day of hospital admission, aiming to
assess both in-hospital and post-discharge long-term mortality
risk.
Statistical analysis
Normality of all continuous variables was assessed
using the Shapiro-Wilk test. Variables conforming to a normal
distribution are presented as the mean ± SD and group comparisons
were performed using an independent sample t-test. Non-normally
distributed variables are summarized as the median with
interquartile range (IQR) and the Mann-Whitney U test was employed
for group comparisons. Categorical variables are expressed as
frequency and percentages (%), and differences were assessed using
the χ2 test, unless any expected cell frequency was less than 5, in
which case Fisher's exact test was used.
Survival rates across groups were visualized and
compared using Kaplan-Meier curves and the log-rank test,
respectively. Kaplan-Meier curves were used to plot survival rates
for different groups, allowing a visual comparison of patient
survival across groups. Differences between groups were assessed
using the log-rank test to determine whether significant
differences existed among the survival curves. To identify risk
factors, univariate Cox proportional hazards regression was
initially performed. In the present study, univariate Cox
regression analysis was first performed to identify potential risk
variables. Variables with a significance level of P<0.05 from
the univariate analysis, along with those considered clinically
relevant, were subsequently incorporated into a multivariate Cox
regression model. This model was used to evaluate the independent
predictive value of the LAR for both 30-day and 360-day all-cause
mortality. Multivariate Cox regression analysis was initially
performed in the crude model without adjusting for any confounding
factors. Subsequently, potential confounders including sex, race,
age and weight were progressively incorporated into the adjusted
models. Further adjustments included clinical variables such as
norepinephrine use, continuous renal replacement therapy, heart
rate, systolic blood pressure, respiratory rate, potassium, anion
gap, BUN, INR and urine output. The covariate selection was guided
by a pre-defined clinical framework, consistent with established
principles of confounder selection in epidemiological research,
rather than a purely data-driven approach (23). CCI was included to account for
baseline comorbidity burden, while the SOFA score was incorporated
to reflect the severity of acute illness at ICU admission. Given
that LAR is derived from lactate and albumin, both of which are
closely associated with shock severity, inflammatory response,
nutritional status and liver function, a multicollinearity
assessment was further performed. All included variables exhibited
Variance Inflation Factor (VIF) values <5, indicating the
absence of significant multicollinearity and supporting the
stability and reliability of the model estimates.
The potential nonlinear association between LAR and
mortality risk was explored using a Restricted Cubic Spline (RCS)
model with four knots. To explore nonlinear associations between
the variables and 30-day and 360-day all-cause mortality, RCS with
three knots were employed. Furthermore, interaction tests were
conducted to assess the heterogeneity of the LAR effect across
different pre-specified subgroups. Interaction tests were also
performed to assess differences in the effect of the variables
across subgroups. Specifically, subgroup analyses were conducted
based on age (<65 years and ≥65 years), sex (female and male),
chronic lung disease (absent and present), liver disease (absent
and present), diabetes (absent and present) and hypertension
(absent and present).
To develop machine learning models, the present
study first split the dataset into a training set and a test set at
a ratio of 7:3. On the training set, the Boruta algorithm (version
8.0.3) was employed in R software (version 4.4.1) for feature
selection to identify the most useful variables for predicting the
risk of mortality. Subsequently, based on the selected variables, a
number of machine learning models were constructed, including Ridge
regression, Elastic Net (ENet), support vector machine (SVM),
K-nearest neighbors (KNN), random forest (RF) and XGBoost. After
model construction, the performance of these models was evaluated
using the test set. The evaluation metrics for model performance
included the receiver operating characteristic (ROC) curve,
precision-recall (PR) curve, calibration curve and decision curve.
These metrics enabled a comprehensive assessment of each model's
performance in predicting 30-day all-cause mortality among patients
with malignancy in the ICU, thereby facilitating the selection of
the optimal predictive model. All statistical analyses were
performed using R software (version 4.5.1; Posit Software, PBC). A
two-tailed P<0.05 was considered to indicate a statistically
significant difference for all tests.
Results
Baseline characteristics
A total of 1,634 patients was included in the final
analysis. The median age of the cohort was 67.77 years (IQR:
60.20–76.46). The overall median LAR was 0.75 (IQR: 0.46–1.26). The
present study population was stratified into tertiles based on LAR
values. Comparison of baseline characteristics across these LAR
tertiles revealed statistically significant differences in key
clinical and physiological parameters, including vital signs (heart
rate, systolic and diastolic blood pressure, and respiratory rate),
severity-of-illness scores (LODS and VIF), and the prevalence of
chronic comorbidities such as congestive heart failure,
cerebrovascular disease, chronic pulmonary disease and liver
disease (Table I; all
P<0.05).
 | Table I.Baseline characteristics of the total
study population (n=1634) and LAR tertiles. |
Table I.
Baseline characteristics of the total
study population (n=1634) and LAR tertiles.
| Characteristic | Overall
(n=1634) | T1 (n=539) | T2 (n=556) | T3 (n=539) | P-value |
|---|
| Median age, years
(IQR) | 67.77
(60.20–76.46) | 69.38
(61.05–78.03) | 67.72
(60.07–76.22) | 66.80
(59.65–75.55) | 0.050 |
| Sex (%) |
|
|
|
| 0.014 |
|
Female | 640 (39) | 238 (44) | 202 (36) | 200 (37) |
|
|
Male | 994 (61) | 301 (56) | 354 (64) | 339 (63) |
|
| Ethnicity, n
(%) |
|
|
|
| 0.070 |
|
Other | 489 (30) | 155 (29) | 153 (28) | 181 (34) |
|
|
White | 1145 (70) | 384 (71) | 403 (72) | 358 (66) |
|
| Weight, kg | 78.00
(65.00–93.00) | 77.00
(64.00–93.00) | 78.05
(65.05–93.35) | 78.00
(65.90–91.80) | 0.459 |
| Heart rate,
bmp | 91.38
(79.62–102.64) | 86.64
(76.84–97.58) | 91.24
(79.85–102.35) | 95.60
(85.00–107.31) | <0.001 |
| SBP, mmHg | 110.61 | 115.42 | 110.43 | 107.50 | <0.001 |
|
|
(102.39–122.80) |
(105.48–127.58) |
(102.41–123.02) | (99.73–117.45) |
|
| DBP, mmHg | 61.08
(55.05–68.00) | 61.58
(55.21–69.23) | 61.67
(55.03–68.57) | 60.05
(54.98–66.26) | 0.013 |
| RR, bmp | 19.56
(16.94–23.07) | 19.23
(16.85–21.88) | 19.49
(16.67–22.98) | 20.21
(17.35–24.12) | <0.001 |
| Temperature,
°C | 36.82
(36.59–37.13) | 36.84
(36.62–37.15) | 36.87
(36.62–37.13) | 36.76
(36.50–37.09) | <0.001 |
| SpO2, % | 96.96
(95.36–98.31) | 96.96
(95.24–98.16) | 96.80
(95.22–98.20) | 97.12
(95.56–98.53) | 0.049 |
| LODS | 6.00
(4.00–8.00) | 5.00
(3.00–7.00) | 6.00
(4.00–8.00) | 7.00
(5.00–10.00) | <0.001 |
| VIF | 2.00
(1.00–4.00) | 1.00
(0.00–3.00) | 2.00
(1.00–4.00) | 3.00
(1.00–6.00) | <0.001 |
| CCI | 8.00
(6.00–10.00) | 8.00
(6.00–10.00) | 8.00
(6.00–10.00) | 8.00
(6.00–10.00) | 0.554 |
| Myocardial infarct
(%) | 187 (11) | 69 (13) | 62 (11) | 56 (10) | 0.445 |
| Congestive heart
failure, n (%) | 355 (22) | 146 (27) | 120 (22) | 89 (17) | <0.001 |
| Cerebrovascular
disease, n (%) | 142 (9) | 63 (12) | 46 (8) | 33 (6) | 0.005 |
| Chronic pulmonary
disease, n (%) | 389 (24) | 154 (29) | 126 (23) | 109 (20) | 0.004 |
| Liver disease, n
(%) | 412 (25) | 46 (9) | 160 (29) | 206 (38) | <0.001 |
| Diabetes, n
(%) | 437 (27) | 148 (27) | 146 (26) | 143 (27) | 0.896 |
| Hypertension, n
(%) | 986 (60) | 336 (62) | 344 (62) | 306 (57) | 0.116 |
| RBC,
109/l | 3.23
(2.77–3.73) | 3.21
(2.76–3.79) | 3.23
(2.80–3.75) | 3.22
(2.74–3.66) | 0.469 |
| WBC,
109/l | 11.46
(7.23–16.82) | 10.55
(6.80–15.40) | 11.58
(7.93–16.70) | 12.61
(7.15–18.97) | <0.001 |
| Platelet,
109/l | 160.00 | 194.50 | 152.58 | 133.00 | <0.001 |
|
| (89.22–259.00) |
(126.00–283.00) | (89.00–255.42) | (78.00–222.50) |
|
| Sodium, mmol/l | 137.67 | 138.00 | 137.33 | 137.67 | 0.059 |
|
|
(134.50–140.33) |
(134.67–140.33) |
(134.13–139.67) |
(134.60–140.75) |
|
| Potassium,
mmol/l | 4.20
(3.86–4.65) | 4.10
(3.80–4.55) | 4.15
(3.81–4.55) | 4.37
(3.95–4.84) | <0.001 |
| Calcium, mg/dl | 8.15
(7.67–8.67) | 8.37
(7.85–8.80) | 8.10
(7.65–8.60) | 8.00
(7.58–8.56) | <0.001 |
| Glucose, mg/dl | 138.71 | 130.67 | 142.37 | 149.67 | <0.001 |
|
|
(112.00–179.50) |
(106.67–156.00) |
(115.00–188.75) |
(115.00–196.00) |
|
| Lactate,
mmol/l | 2.06
(1.37–3.40) | 1.20
(1.00–1.40) | 2.10
(1.80–2.53) | 4.18
(3.28–6.18) | <0.001 |
| Albumin, mg/dl | 2.88
(2.40–3.30) | 3.13
(2.80–3.60) | 2.80
(2.48–3.25) | 2.55
(2.10–2.93) | <0.001 |
| LAR | 0.75
(0.46–1.26) | 0.39
(0.32–0.46) | 0.75
(0.64–0.89) | 1.64
(1.27–2.47) | <0.001 |
| Anion gap | 14.20
(12.00–17.00) | 13.33
(11.50–15.50) | 13.69
(12.00–16.20) | 16.20
(13.40–19.67) | <0.001 |
| BUN, mg/dl | 23.00
(15.00–38.75) | 21.33
(14.00–36.17) | 22.63
(15.00–37.00) | 26.00
(16.50–42.50) | <0.001 |
| Creatinine,
mg/dl | 1.10
(0.77–1.73) | 1.00
(0.70–1.63) | 1.04
(0.75–1.49) | 1.33
(0.90–1.87) | <0.001 |
| INR | 1.40
(1.20–1.70) | 1.30
(1.15–1.50) | 1.40
(1.22–1.65) | 1.60
(1.35–1.90) | <0.001 |
| PT, sec | 15.44
(13.55–18.30) | 14.15
(12.65–15.93) | 15.46
(13.72–18.06) | 17.31
(14.90–20.77) | <0.001 |
| PTT, sec | 32.77
(28.30–42.10) | 30.65
(27.40–36.75) | 32.41 (27.70,
39.50) | 36.28
(30.20–47.90) | <0.001 |
| Urine output,
ml | 1,245.00 | 1,474.00 | 1,268.50 | 1,005.00 | <0.001 |
|
|
(705.00–2025.00) |
(861.00–2370.00) |
(772.50–2031.50) |
(496.00–1642.00) |
|
| Epinephrine, n
(%) | 59 (4) | 3 (1) | 15 (3) | 41 (8) | <0.001 |
| Norepinephrine, n
(%) | 562 (34) | 130 (24) | 180 (32) | 252 (47) | <0.001 |
| MV, n (%) | 1,399 (86) | 458 (85) | 480 (86) | 461 (86) | 0.812 |
| CRRT, n (%) | 131 (8) | 23 (4) | 31 (6) | 77 (14) | <0.001 |
| Los hospital,
days | 11.76
(7.03–20.26) | 11.08
(6.85–18.69) | 11.34
(7.10–19.74) | 13.05
(7.04–23.50) | 0.106 |
| Los ICU, days | 2.92
(1.84–5.33) | 2.80
(1.77–5.12) | 2.86
(1.93–5.01) | 3.24
(1.82–6.64) | 0.045 |
| 30-day hospital
mortality, % | 527 (32) | 124 (23) | 170 (31) | 233 (43) | <0.001 |
| 360-day hospital
mortality, % | 950 (58) | 273 (51) | 314 (56) | 363 (67) | <0.001 |
Association between LAR and
in-hospital mortality in critically ill patients with cancer
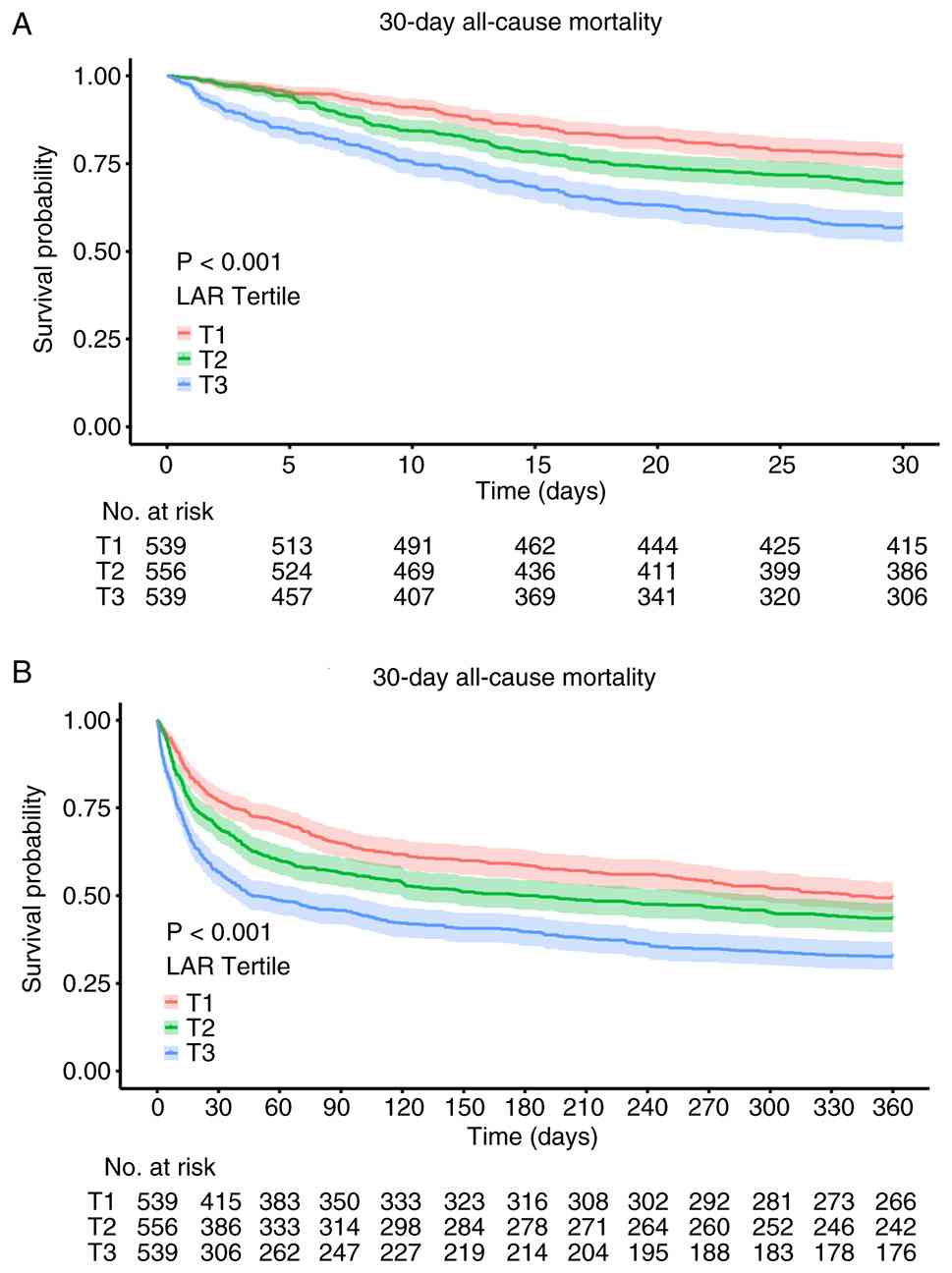
Kaplan-Meier survival curves were plotted for
patients stratified by LAR tertiles and compared using the log-rank
test. The results demonstrated statistically significant
differences in mortality among the LAR tertiles at both 30-day and
360-day follow-ups (Fig. 2;
P<0.05). Patients in T1 exhibited the most favorable prognosis,
whereas those in T3 demonstrated the worst prognosis. These
findings indicated that elevated LAR levels were associated with
poorer short-term and long-term outcomes in critically ill patients
with malignancy.
Variables for the multivariate Cox regression models
were selected based on both univariate Cox regression analysis
(P<0.10) and established clinical evidence regarding mortality
predictors in critically ill patients with cancer. Covariates with
recognized clinical relevance and biological associations with
mortality, including organ dysfunction assessed by the Sequential
Organ Failure Assessment (SOFA) score and major comorbidities, were
prioritized for adjustment (24,25).
In addition, the variable selection strategy followed the principle
of integrating statistical significance with clinical relevance,
which is widely recommended in prognostic modeling studies to
improve model interpretability and clinical applicability (26). The multivariate Cox regression
models were then used to assess the associations of continuous LAR
values and LAR tertiles with 30-day and 360-day all-cause mortality
(Table II). For 30-day mortality,
the continuous LAR remained a significant predictor of mortality
risk in the fully adjusted model (model 3), with a HR of 1.13 (95%
CI: 1.04–1.22; P=0.004). Analysis using LAR tertiles revealed that
patients in the highest tertile (T3) continued to exhibit a
significantly increased risk compared with the reference group
(T1), with an HR of 1.29 (95% CI: 1.01–1.64; P=0.040). With regard
to 360-day mortality, the continuous LAR was also a significant
independent predictor in model 3 (HR=1.15; 95% CI: 1.07–1.23;
P<0.001). Similarly, the tertile analysis determined that the T3
group was associated with a significantly elevated mortality risk
(HR=1.26; 95% CI: 1.06–1.49; P=0.010).
| Table II.Cox proportional hazards regression
analysis of LAR and mortality in critically ill patients with
cancer. |
Table II.
Cox proportional hazards regression
analysis of LAR and mortality in critically ill patients with
cancer.
|
| Model 1 | Model 2 | Model 3 |
|---|
|
|
|
|
|
|---|
| Variable | HR (95% CI) | P-value | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| 30-day all-cause
mortality |
|
|
|
|
|
|
|
LAR | 1.39
(1.31~1.48) | <0.001 | 1.38
(1.31~1.47) | <0.001 | 1.13
(1.04~1.22) | 0.004 |
| LAR tertile |
|
|
|
|
|
|
| T1 | 1.00
(reference) |
| 1.00
(reference) |
| 1.00
(reference) |
|
| T2 | 1.41
(1.12~1.78) | 0.004 | 1.44
(1.14~1.81) | 0.002 | 1.17
(0.92~1.48) | 0.204 |
| T3 | 2.23
(1.80~2.78) | <0.001 | 2.31
(1.85~2.87) | <0.001 | 1.29
(1.01~1.64) | 0.040 |
| 360-day all-cause
mortality |
|
|
|
|
|
|
|
LAR | 1.32
(1.25~1.39) | <0.001 | 1.32
(1.26~1.39) | <0.001 | 1.15
(1.07~1.23) | <0.001 |
| LAR tertile |
|
|
|
|
|
|
| T1 | 1.00
(reference) |
| 1.00
(reference) |
| 1.00
(reference) |
|
| T2 | 1.23
(1.05~1.45) | 0.013 | 1.27
(1.08~1.50) | 0.004 | 1.12
(0.95~1.32) | 0.188 |
| T3 | 1.73
(1.48~2.03) | <0.001 | 1.83
(1.56~2.14) | <0.001 | 1.26
(1.06~1.49) | 0.010 |
To evaluate the incremental clinical value of LAR, a
comparative analysis with the SOFA score was then performed. The
results showed that the SOFA score alone had limited discriminative
ability for predicting 30-day mortality [area under the curve
(AUC)=0.540], whereas incorporation of LAR significantly improved
the model performance, increasing the AUC to 0.622 (DeLong's test,
P<0.001; Fig. S1A). LAR
remained an independent predictor after adjustment for the SOFA
score, indicating its prognostic robustness across different acute
clinical settings. ROC curve analysis was also performed,
identifying the optimal cut-off value of the LAR for predicting
30-day mortality as 0.760, with a sensitivity of 62.2% and a
specificity of 56.2% (Fig. S1B).
In clinical practice, this cut-off may serve as an additional tool
for identifying patients with cancer who are at increased risk
despite relatively stable conventional organ dysfunction scores,
such as the SOFA score. Elevated lactate levels are associated with
occult tissue hypoperfusion and metabolic stress (27), whereas hypoalbuminemia reflects
systemic inflammation and impaired nutritional reserve (25). By integrating these
pathophysiological dimensions, the LAR may provide complementary
prognostic information beyond conventional organ dysfunction
assessment and improve clinical risk stratification (28). Consequently, patients with elevated
LAR values may warrant closer monitoring and more comprehensive
clinical evaluation in critical care settings.
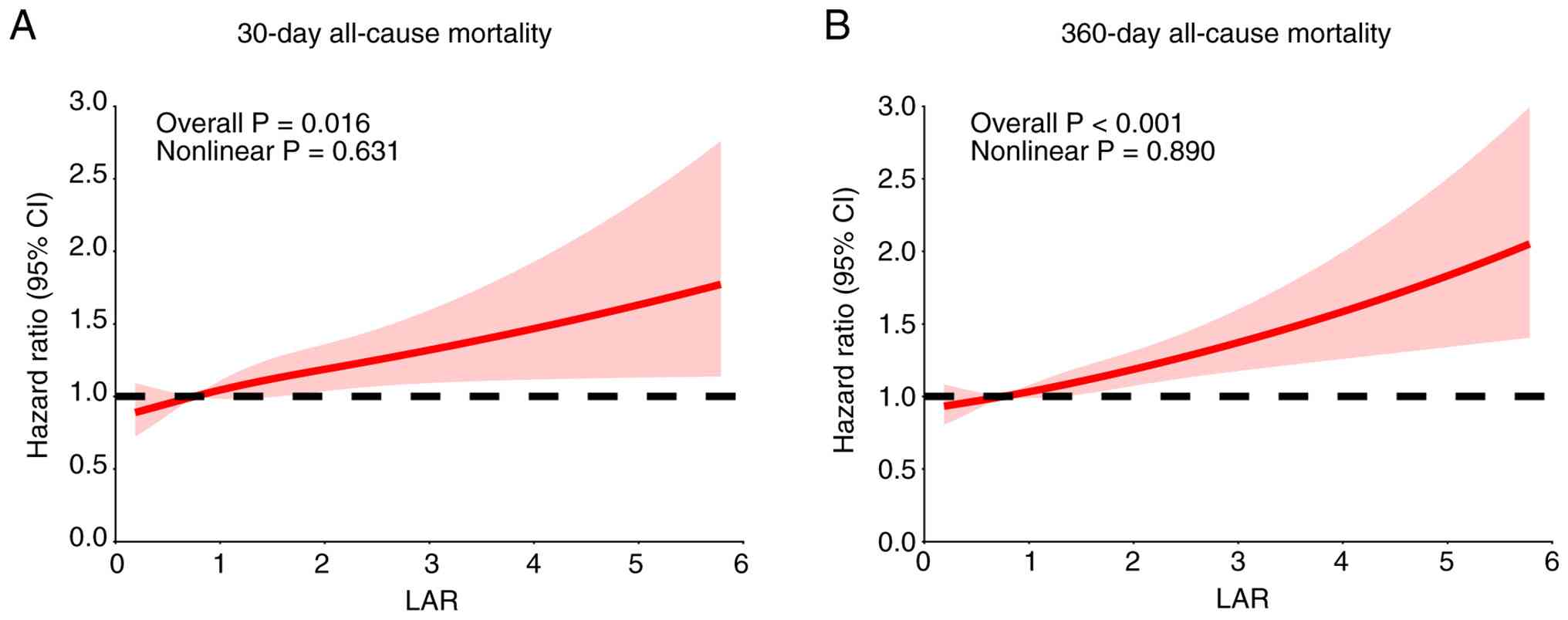
LAR exhibits a linear association with
all-cause mortality risk, consistent across subgroups
RCS was employed to assess the potential non-linear
association between LAR and both 30-day and 360-day all-cause
mortality. The results indicated no significant deviation from
linearity for the association between LAR and mortality at either
time point (nonlinearity P>0.05; Fig. 3). However, a significant overall
positive association was observed, demonstrating a linear increase
in mortality risk with rising LAR levels. Furthermore, subgroup
analyses revealed no significant interaction effects, demonstrating
the consistent association between elevated LAR and increased
mortality risk across all predefined patient subgroups. While liver
disease can influence both lactate metabolism and albumin
synthesis, the present interaction analysis indicated that LAR
remained a robust predictor of mortality irrespective of hepatic
comorbidity, reinforcing its utility as a simple, integrated risk
marker in the present heterogeneous population.
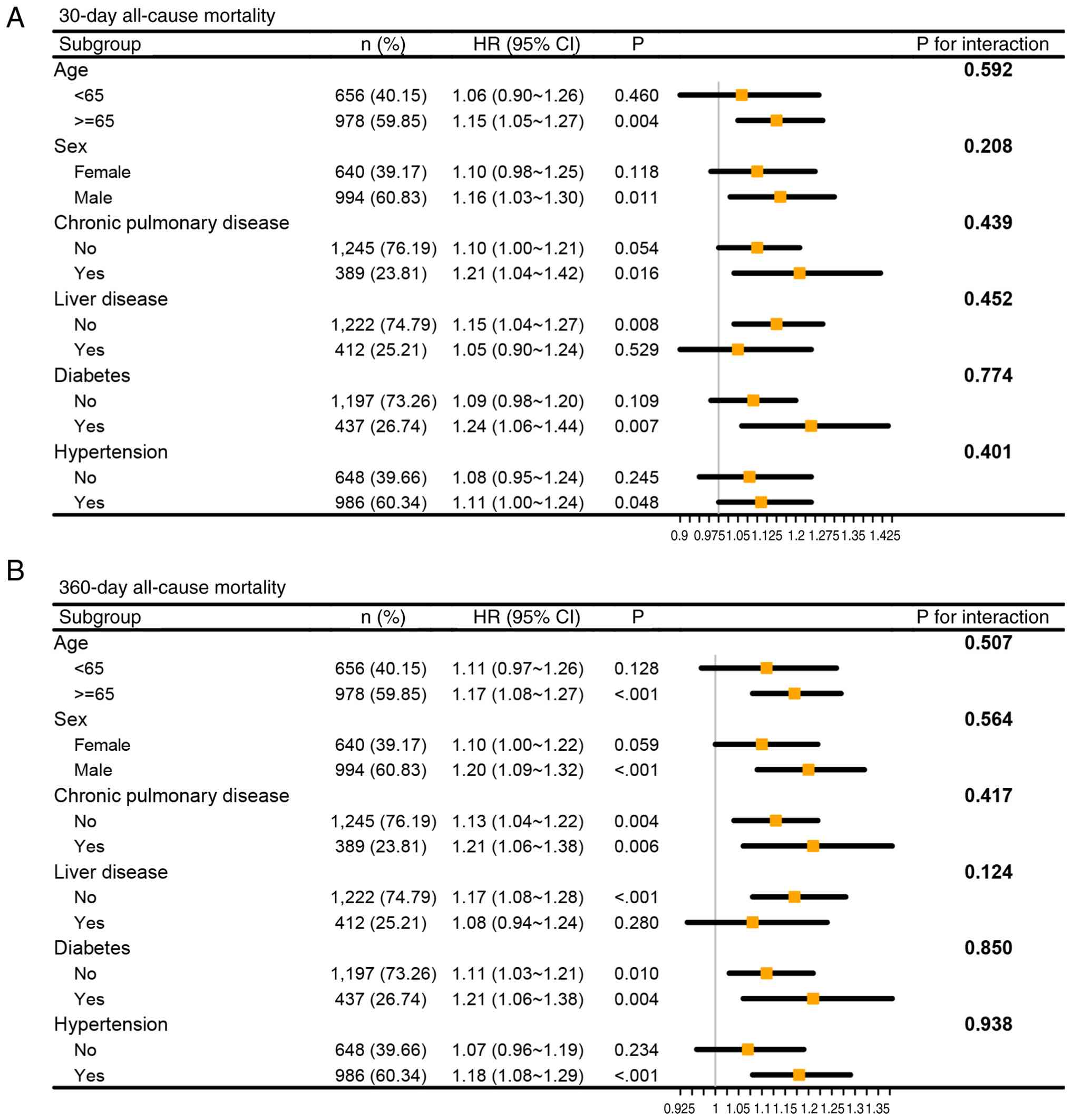
Subgroup analysis revealed no significant
interaction effects between LAR and any pre-specified subgroups for
both 30-day and 360-day all-cause mortality (all interaction
P>0.05; Fig. 4). This indicated
that the positive association between elevated LAR and increased
mortality risk was consistent and independent of the subgroup
factors examined. Specifically, stratified and interaction analyses
were performed according to liver disease status, which exhibited a
non-significant interaction effect (interaction P=0.375; Table III), supporting the consistency of
LAR across different hepatic conditions.
| Table III.Stratified and interaction analyses
by liver disease status. |
Table III.
Stratified and interaction analyses
by liver disease status.
| Liver disease | Patients | Events (n) | HR (95% CI) | P value | P for
interaction |
|---|
| Yes | 412 | 85 | 1.28
(1.11–1.48) | 0.001 | 0.375 |
| No | 1,222 | 206 | 1.25
(1.18–1.32) | <0.001 |
|
Model development and performance
comparison
Based on the selected variables, machine learning
models were developed on the training set, including Ridge
regression, ENet, SVM, KNN, RF and XGBoost. During model
development, grid search was employed for hyperparameter tuning.
Grid search is a systematic approach that considers all parameter
combinations within a specified subset of the hyperparameter space
to identify the configuration that maximizes model performance,
thereby mitigating the risk of overfitting during the tuning
process (29).
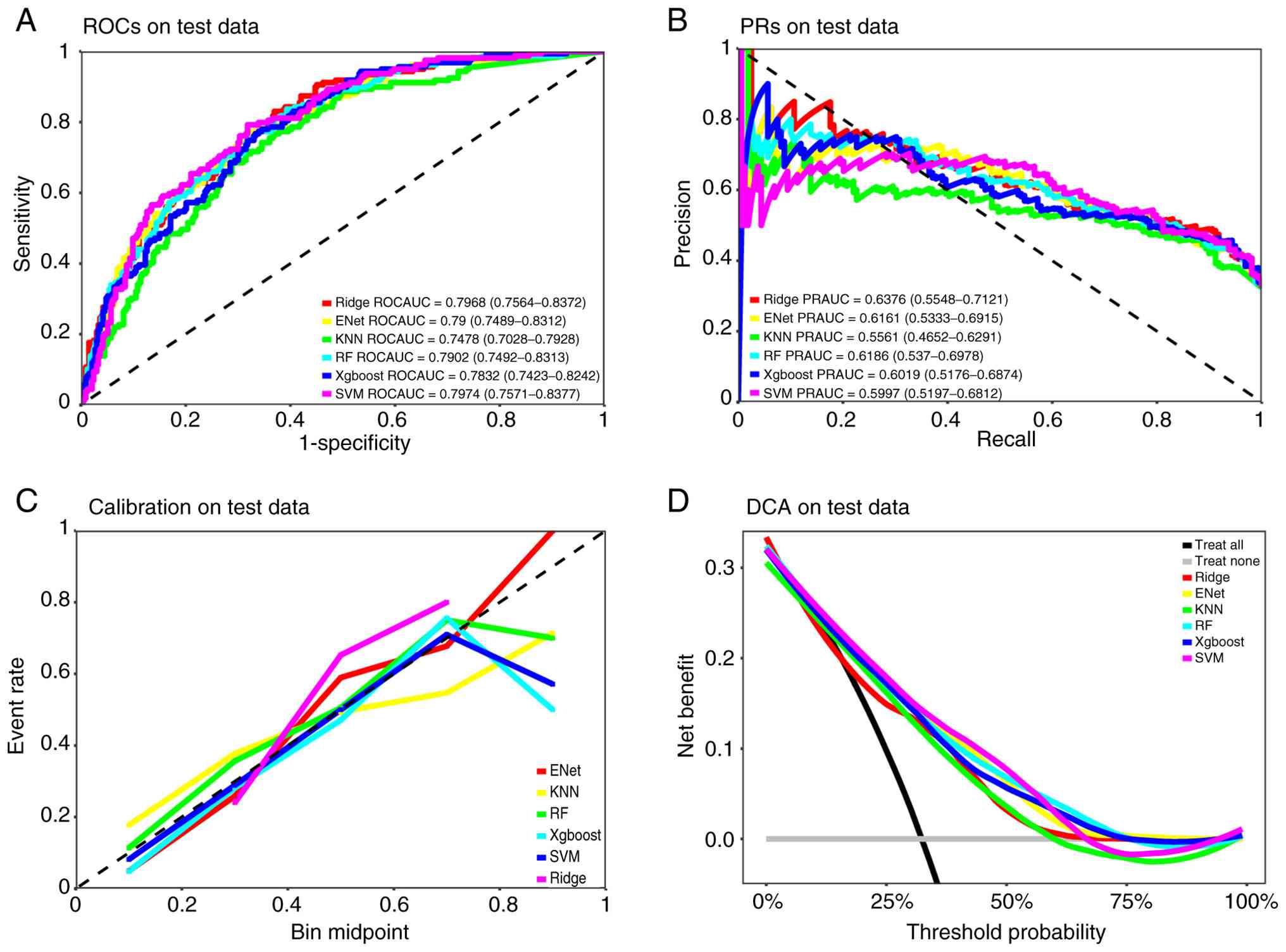
On the test set, the area under the ROC curve
(ROCAUC) results for each model were as follows (Fig. 5A): Ridge regression was 0.7968 (95%
CI: 0.7564–0.8372), ENet was 0.7900 (95% CI: 0.7489–0.8312), KNN
was 0.7478 (95% CI: 0.7028–0.7928), RF was 0.7902 (95% CI:
0.7492–0.8313), XGBoost was 0.7832 (95% CI: 0.7423–0.8242) and SVM
was 0.7974 (95% CI: 0.7571–0.8377).
On the test set, the area under the precision-recall
curve (PRAUC) results for each model were as follows (Fig. 5B): Ridge regression was 0.6376 (95%
CI: 0.5548–0.7121), ENet was 0.6161 (95% CI: 0.5333–0.6915), KNN
was 0.5561 (95% CI: 0.4652–0.6291), RF was 0.6186 (95% CI:
0.537–0.6978), XGBoost was 0.6019 (95% CI: 0.5176–0.6874) and SVM
was 0.5997 (95% CI: 0.5197–0.6812). These results indicated that
the Ridge regression model achieved the best PRAUC performance on
the test set, with the highest PRAUC value (0.6376), whereas the
KNN model exhibited a relatively poorer PRAUC performance.
Following comparisons of calibration curves and decision curves on
the test set, the SVM was ultimately identified as the optimal
model, demonstrating favorable predictive value (Fig. 5C and D).
Discussion
Critically ill patients with malignancy frequently
require ICU management due to both disease progression and
treatment-associated complications. The high mortality rate in this
population poses a challenge in the field of critical care
medicine. Therefore, the accurate identification of prognostic risk
factors and the optimization of risk assessment strategies is
important in improving patient outcomes. Based on the MIMIC-IV
database, to the best of our knowledge, the present study is the
first to systemically investigate the prognostic value of the LAR
in critically ill patients with cancer. The present results
determined that an elevated LAR was significantly associated with
increased 30-day and 360-day all-cause mortality and serves as an
independent risk factor. These findings thus present a novel
potential biomarker for prognostic assessment in this vulnerable
patient population.
The prognostic value of the LAR stems from its role
as an integrated marker reflecting multiple underlying
pathophysiological states (17,30).
The unique glycolytic metabolism of tumor cells continuously
generates large amounts of lactate. In advanced-stage tumors or
under notable tumor burden, metabolic dysregulation is exacerbated,
leading to lactate accumulation (31,32).
Furthermore, complications frequently encountered in critically ill
patients with cancer, including infections and sepsis, can induce
inadequate tissue perfusion and hypoxia, thereby further promoting
lactate generation while simultaneously inhibiting its clearance
(33). On the other hand, tumor
burden, systemic inflammation and inadequate nutritional intake
lead to reduced albumin synthesis. As a key protein in maintaining
vascular osmotic pressure, binding toxins and modulating
inflammatory responses, decreased albumin levels exacerbate the
pathological damage to the patient (34). The LAR provides a comprehensive
assessment of patient disease severity and prognosis by integrating
the dynamics of both lactate and albumin, thereby reflecting the
extent of tumor metabolic aberration, tissue hypoxia, as well as
the inflammatory status and nutritional reserves of the body
(30,35,36).
In the present study, the T3 group, which exhibited a higher LAR,
also exhibited significantly higher LODS and SOFA scores, along
with a greater rate of norepinephrine use, demonstrating the
association between LAR and disease severity.
LAR holds prognostic value in critically ill
patients beyond the oncology setting (37–40).
Studies have shown that in patients with sepsis, the LAR
outperforms either lactate or albumin alone in predicting mortality
(41,42) and among septic patients with
co-existing heart failure, an LAR >0.98 has been associated with
an elevated mortality risk (43).
The present findings demonstrated a linear association between LAR
and mortality in critically ill patients with cancer that is
unaffected by age, sex or underlying diseases. This linear
association diverges from the nonlinear dynamics observed in
studies of cirrhotic patients with sepsis (16,44), a
difference that may stem from the distinct metabolic and
pathophysiological state of patients with tumors. Critically, LAR
was found to be an independent prognostic factor, retaining
significance after correcting for confounders including SOFA score
and organ-support interventions. Addressing the potential issue of
over-adjustment, it should be acknowledged that adjustment for
variables located along the mediational pathway between LAR and
clinical outcomes, such as organ support-associated variables, may
partially attenuate the effect estimates. Despite this, such
adjustments were considered necessary to demonstrate that the
prognostic value of LAR is not just a reflection of acute
physiological derangement in the present study. This implies that
LAR could deliver supplemental prognostic insight beyond
conventional scoring systems, thereby potentially augmenting risk
stratification in severely ill cohorts where cancer-associated
metabolic dysregulation is prominent.
The prognostic evaluation of critically ill patients
with cancer necessitates dual consideration of the specific traits
of the neoplasm and the attendant pathophysiological changes of
critical illness. Whereas conventional scoring systems [such as
SOFA and Acute Physiology and Chronic Health Evaluation (APACHE)]
are capable of indicating organ function impairment (41), they fall short in specifically
addressing cancer-associated metabolic aberrations. The LAR is
readily obtainable through routine laboratory tests within 24 h of
ICU admission, offering a cost-effective and convenient tool for
rapid risk stratification. This facilitates the development of
individualized treatment strategies: Patients with a high LAR
warrant intensified lactate monitoring, optimized tissue perfusion
and aggressive management of nutrition and inflammation, with early
organ support if indicated, whereas a more conservative approach
can be adopted for those with a low LAR to avoid overtreatment and
optimize resource allocation. Furthermore, the linear association
of LAR with risk provides an intuitive metric for clinicians to
track clinical deterioration and enhances objective doctor-patient
communication (45).
The present study exhibits a number of limitations.
Firstly, its retrospective design and reliance on a single database
may have introduced selection bias and detailed information
regarding specific tumor pathology and treatment regimens was
lacking. Although the SOFA score was used to reflect the overall
acute physiological derangement and the degree of organ dysfunction
at ICU admission, residual confounding associated with the reason
for ICU admission cannot be completely excluded. Owing to MIMIC-IV
limitations, TNM stage and detailed treatment data were
unavailable. The present study adjusted for CCI, tumor type and
metastatic status (all VIF<5). Residual confounding may persist,
yet LAR remained independently prognostic, indicating added
metabolic risk beyond conventional oncological variables. Secondly,
the analysis utilized only the LAR from the first ICU day, failing
to capture its dynamic trends and their potential impact on
prognosis. Finally, the absence of a direct comparison with
established scoring systems such as APACHE II or SOFA precludes a
definitive assessment of the incremental predictive value of LAR.
Due to the retrospective nature of the MIMIC database, the present
study was unable to obtain accurate records of albumin infusion and
nutritional support for all patients and could not analyze the
impact of these dynamic interventions on prognosis. Future
prospective studies should therefore consider collecting such
information to more comprehensively evaluate the predictive value
of the LAR. Furthermore, tumor heterogeneity is a key factor
influencing prognosis, encompassing intrinsic heterogeneity at the
molecular level (genetic, epigenetic and transcriptomic
differences) and observable heterogeneity at the clinical level
(tumor type, stage, metastatic burden and differences in treatment
response). Due to the original data sources and data structure of
the MIMIC-IV database, there are inherent limitations in the
systematic availability of staging information. The CCI score is
one of the most widely used comorbidity assessment tools in cancer
prognosis research (46–48). Validation studies in specific cancer
types such as lung cancer, breast cancer and gastric cancer have
shown that the CCI score has varying degrees of prognostic
predictive value across different cancer types (46,48,49).
In a cohort of patients with non-small cell lung cancer, the CCI
score was systematically compared with other comorbidity scores to
optimize the prediction of 4-month survival (50). The present study adopted the CCI
score primarily because it includes the highly weighted category of
‘metastatic disease’, which allows for some incorporation of the
impact of metastasis on prognosis. However, it must be acknowledged
that the aggregated total CCI score cannot disentangle the
independent prognostic contributions of different sources,
tumor-related factors (metastatic burden), treatment-related
factors and comorbidities unrelated to treatment, implying that the
predictive performance of the present model may be diluted by
heterogeneity. Future multi-center prospective studies are
therefore needed to validate the applicability of LAR across
different tumor types, investigate the importance of its dynamic
monitoring and develop integrated prediction models that
incorporate LAR to enhance prognostic accuracy in critically ill
patients with cancer.
In conclusion, based on the present analytical
findings, the LAR demonstrates guiding value for predicting ICU
outcomes in patients with cancer, exhibiting a linear association
with mortality risk. As an inexpensive and readily accessible
clinical biomarker, the LAR effectively integrates information on
both metabolic and nutritional status in this patient population,
thereby providing a reliable reference for prognosis. This
indicator holds promise as an effective tool for risk
stratification in clinical practice, offering valuable insights for
optimizing clinical decision-making and healthcare resource
allocation. However, its application in clinical prognostic
assessment still requires further validation through large-scale,
multicenter studies.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
The present study was funded by the Science & Technology
Development Fund of Tianjin Education Commission for Higher
Education (grant no. 2022KJ230), the Tianjin Health Research
Project (grant no. TJWJ2023QN014) and the Tianjin Science and
Technology Plan Project (grant nos. 21JCYBJC01450 and
24JCYBJC00750).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
JB conceived and designed the study, analyzed data
and drafted the manuscript. YX analyzed data and manuscript
revision. JB and YX confirm the authenticity of all the raw data.
KW interpreted data and revised the manuscript. XF designed and
supervised the study, and performed a final review of the
manuscript. All authors have read and approved the final version of
the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
LAR
|
lactate-to-albumin ratio
|
|
RCS
|
restricted cubic spline
|
|
MIMIC-IV
|
Medical Information Mart for Intensive
Care IV
|
|
SOFA
|
Sequential Organ Failure
Assessment
|
|
LODS
|
Logistic Organ Dysfunction System
|
|
IQR
|
interquartile range
|
|
CCI
|
Charlson Comorbidity Index
|
|
INR
|
international normalized ratio
|
References
|
1
|
Bray F, Laversanne M, Sung H, Ferlay J,
Siegel RL, Soerjomataram I and Jemal A: Global cancer statistics
2022: GLOBOCAN estimates of incidence and mortality worldwide for
36 cancers in 185 countries. CA Cancer J Clin. 74:229–263.
2024.PubMed/NCBI
|
|
2
|
Dong Q, Xia R, Xing XZ, Wang CS, Ma G,
Wang HZ, Zhu B, Zhao JH, Zhou DM, Zhang L, et al: Intensive care
unit outcomes and prognostic factors of colorectal cancer. World J
Gastrointest Oncol. 17:1085392025. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Theodoulidis V, Kissoudi K,
Chatzistamatiou K, Tzitzis P, Zouzoulas D, Theodoulidis I,
Anthoulakis C, Sifaki F, Moysiadis T, Koraki E, et al: Predictors
of extended intensive care unit utilization after ovarian cancer
surgery. Cancers (Basel). 17:32032025. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Al Khamis M, Aljishi M, Busbaih A, Al
Dandan R, Salam A and Al Yousef H: Evaluating prognosis and
prognostic factors in critically Ill patients with and without
cancer: An observational comparative study. Cureus.
17:e964932025.PubMed/NCBI
|
|
5
|
Wang HX, Huang XH, Ma LQ, Yang ZJ, Wang
HL, Xu B and Luo MQ: Association between Lactate-to-Albumin ratio
and Short-Time mortality in patients with acute respiratory
distress syndrome. J Clin Anesth. 99:1116322024. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yang X, Ying S, Yuan X, Ying J, Yang J and
Lv L: Lactate-to-albumin ratio as an independent predictor of
mortality in critically ill patients with gastrointestinal
bleeding: A retrospective cohort study. BMC Gastroenterol.
25:6532025. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Aydin H: The Cancer-Induced lactate load
and oncologic remodeling hypothesis: Lactate as a driver of
biosynthesis and epigenetics in cancer. Front Oncol.
15:16381082025. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Huang K, Han Y, Chen Y, Shen H, Zeng S and
Cai C: Tumor metabolic regulators: Key drivers of metabolic
reprogramming and the promising targets in cancer therapy. Mol
Cancer. 24:72025. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Altea-Manzano P, Decker-Farrell A,
Janowitz T and Erez A: Metabolic interplays between the tumour and
the host shape the tumour macroenvironment. Nat Rev Cancer.
25:274–292. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bozgul SMK, Kurtulmus IA, Gunes A, Koymen
G, Bozkurt D, Karaman ZT, Islamoglu K, Ozkilic B, Barutcuoglu B,
Cilli FF and Soyer NA: Lactate level is an independent predictor of
mortality in patients with hematologic malignancy receiving urgent
chemotherapy in intensive care unit. Curr Res Transl Med.
72:1034512024.PubMed/NCBI
|
|
11
|
Erdur A, Guven R, Can D, Gurkan TT, Ak E
and Avci A: Prognostic importance of lactate and blood gas
parameters in predicting mortality in patients with critical
malignancies. Ethiop J Health Sci. 33:255–262. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Liu Q, Zheng HL, Wu MM, Wang QZ, Yan SJ,
Wang M, Yu JJ and Li DP: Association between lactate-to-albumin
ratio and 28-days all-cause mortality in patients with acute
pancreatitis: A retrospective analysis of the MIMIC-IV database.
Front Immunol. 13:10761212022. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Shin J, Hwang SY, Jo IJ, Kim WY, Ryoo SM,
Kang GH, Kim K, Jo YH, Chung SP, Joo YS, et al: Prognostic value of
the Lactate/Albumin ratio for predicting 28-Day mortality in
critically ILL sepsis patients. Shock. 50:545–550. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kong T, Chung SP, Lee HS, Kim S, Lee J,
Hwang SO, Shin SD, Song KJ, Cha KC and You JS; Korean Cardiac
Arrest Research Consortium (KoCARC) Investigators, : The Prognostic
usefulness of the lactate/Albumin ratio for predicting clinical
outcomes in Out-of-hospital cardiac arrest: A prospective,
multicenter observational study (koCARC) study. Shock. 53:442–451.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ren J, Kang Q, Wang F and Yu W:
Association of lactate/albumin ratio with in-hospital mortality in
ICU patients with acute respiratory failure: A retrospective
analysis based on MIMIC-IV database. Medicine (Baltimore).
102:e354102023. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wang J, Chen X, Qin C, Shi R, Huang Y,
Gong J, Zeng X and Wang D: Lactate-to-Albumin ratio as a potential
prognostic predictor in patients with cirrhosis and sepsis: A
retrospective cohort study. BMC Infect Dis. 25:2232025. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Gou J, Liu C, Lang M and Yao F: Prognostic
value of the lactate-to-albumin ratio in critically ill chronic
heart failure patients with sepsis: Insights from a retrospective
cohort study. Front Med (Lausanne). 12:15935242025. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hanci P, Temel E, Bilir F and Kaya BS:
Lactate to albumin ratio as a determinant of intensive care unit
admission and mortality in hospitalized patients with
Community-Acquired pneumonia. BMC Pulm Med. 25:2242025. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Johnson AEW, Bulgarelli L, Shen L, Gayles
A, Shammout A, Horng S, Pollard TJ, Hao S, Moody B, Gow B, et al:
Author Correction: MIMIC-IV, a freely accessible electronic health
record dataset. Sci Data. 10:2192023. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Charlson ME, Pompei P, Ales KL and
MacKenzie CR: A new method of classifying prognostic comorbidity in
longitudinal studies: Development and validation. J Chronic Dis.
40:373–383. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Quan H, Sundararajan V, Halfon P, Fong A,
Burnand B, Luthi JC, Saunders LD, Beck CA, Feasby TE and Ghali WA:
Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10
administrative data. Med Care. 43:1130–1119. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Heymans MW and Twisk JWR: Handling missing
data in clinical research. J Clin Epidemiol. 151:185–188. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
VanderWeele TJ: Principles of confounder
selection. Eur J Epidemiol. 34:211–219. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Vincent JL, Moreno R, Takala J, Willatts
S, De Mendonca A, Bruining H, Reinhart CK, Suter PM and Thijs LG:
The SOFA (Sepsis-related Organ Failure Assessment) score to
describe organ dysfunction/failure. On behalf of the Working Group
on Sepsis-Related Problems of the European Society of Intensive
Care Medicine. Intensive Care Med. 22:707–710. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
den Boer S, de Keizer NF and de Jonge E:
Performance of prognostic models in critically ill cancer
patients-a review. Crit Care. 9:R458–R463. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Steyerberg EW, Vickers AJ, Cook NR, Gerds
T, Gonen M, Obuchowski N, Pencina MJ and Kattan MW: Assessing the
performance of prediction models: A framework for traditional and
novel measures. Epidemiology. 21:128–138. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Bakker J and Jansen TC: Don't take vitals,
take a lactate. Intensive Care Med. 33:1863–1865. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Lichtenauer M, Wernly B, Ohnewein B, Franz
M, Kabisch B, Muessig J, Masyuk M, Lauten A, Schulze PC, Hoppe UC,
et al: The Lactate/Albumin ratio: A valuable tool for risk
stratification in septic patients admitted to ICU. Int J Mol Sci.
18:18932017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Hastie T, Tibshirani R, Friedman J and
Franklin J: The elements of statistical learning: Data mining,
inference, and prediction. Math Intell. 27:83–85. 2004.
|
|
30
|
Gharipour A, Razavi R, Gharipour M and
Mukasa D: Lactate/Albumin Ratio: An early prognostic marker in
critically Ill patients. Am J Emerg Med. 38:2088–2095. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Vayakkattil AB, Pazhanchery AS, Andrews S
and Vayakkattil U: The warburg effect redefined: A kinetic and
regulatory perspective. Cureus. 17:e933312025.PubMed/NCBI
|
|
32
|
Hou X, Hong Z, Zen H, Zhang C, Zhang P, Ma
D and Han Z: Lactylation in cancer biology: Unlocking new avenues
for research and therapy. Cancer Commun (Lond). 45:1367–1406. 2025.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Nuyttens L, Heyerick M, Heremans G, Moens
E, Roes M, Van Dender C, De Bus L, Decruyenaere J, Dewaele J,
Vandewalle J and Libert C: Unraveling mitochondrial pyruvate
dysfunction to mitigate hyperlactatemia and lethality in sepsis.
Cell Rep. 44:1160322025. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Kring SK, Beck AM, Wessel I, Ustrup KS,
Dieperink KB, Zwisler AD and Kristensen MB: Nutrition screening and
assessment tools for adult patients with cancer and survivors of
cancer: A systematic review. Nutr Cancer. 78:7–29. 2026. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Zhao K, Zhou L, Ni Y, Tao J, Yu Z, Li X
and Wang L: Association between lactate-to-Albumin ratio and 28-day
all-cause mortality in critical care patients with COPD: Can both
arterial and peripheral venous lactate serve as predictors? Int J
Chron Obstruct Pulmon Dis. 20:1419–1434. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Dong Y, Shi X, Wang C, Hu Y, Li J, Luo H,
Zhu M, Hu F and Chu Q: The impact of the lactate-to-albumin ratio
on long-term mortality risk in patients with severe heart failure
and type 2 diabetes. BMC Cardiovasc Disord. 25:2342025. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Zhang R, Yao J, Li H, Liu D and Lin D:
Lactate to albumin ratio as a novel predictor of short-term
prognosis for liver cirrhosis in ICU. Sci Rep. 15:357542025.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Acharya CP, Yadav A, Pokhrel S, Bastola S
and Jha S: Prognostic significance of lactate/albumin ratio in
respiratory failure and sepsis. Ann Med. 57:24820242025. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Song Z, Miao H, Xin X, Guo D, Deng Y, Wang
H and Wang F: Elevated lactate-to-albumin ratio predicts short- and
long-term mortality in trauma and surgical intensive care patients:
A retrospective MIMIC-IV cohort study. Sci Rep. 15:451212025.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Wu Y, Wang L and Wen Q: Association of
lactate to albumin ratio with short-term and long-term mortality in
critically ill patients with heart failure complicated by sepsis: A
retrospective study using the MIMIC-IV database. Front Cardiovasc
Med. 12:16363752025. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Ranzani OT, Singer M, Salluh JIF,
Shankar-Hari M, Pilcher D, Berger-Estilita J, Coopersmith CM,
Juffermans NP, Laffey J, Reinikainen M, et al: Development and
validation of the sequential organ failure assessment (SOFA)-2
Score. JAMA. 334:2090–2103. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Bugarin-Arellano AL, Ramirez-Gonzalez LR,
Suarez-Carreon LO, Lopez-Bernal NE, Leon-Flores PG, Gonzalez-Ojeda
A and Fuentes-Orozco C: Lactate/albumin index as mortality
predictor in abdominal sepsis. Cir Cir. 93:361–366. 2025.PubMed/NCBI
|
|
43
|
Liu Y: Association between lactate/albumin
ratio and 28-day mortality in ICU critical patients with coronary
heart disease: A retrospective analysis of the MIMIC-IV database.
Front Cardiovasc Med. 11:14866972024. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Ma Y, Du L, Bai L and Tang H: Association
between lactate-to-albumin ratio and all-cause mortality in
critically ill cirrhotic patients with sepsis: A retrospective
analysis of the MIMIC-IV database. BMC Gastroenterol. 25:1122025.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Han D, Sun S, Liu A, Hao C and Sun J:
Lactate dehydrogenase-to-albumin ratio predicts 30-day and 90-day
mortality in glucocorticoid-treated ICU patients with pneumonia: A
secondary analysis of a multicenter cohort. Front Med (Lausanne).
13:18329432026. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Salas M, Henderson M, Sundararajan M, Tu
N, Islam Z, Ebeid M and Horne L: Use of comorbidity indices in
patients with any cancer, breast cancer, and human epidermal growth
factor Receptor-2-positive breast cancer: A systematic review. PLoS
One. 16:e02529252021. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Kubo Y, Tanaka K, Yamasaki M, Yamashita K,
Makino T, Saito T, Yamamoto K, Takahashi T, Kurokawa Y, Motoori M,
et al: Influences of the charlson comorbidity index and nutrition
status on prognosis after esophageal cancer surgery. Ann Surg
Oncol. 28:7173–7182. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Cao W, Liu S, Wang S, Wang S, Song Y and
He Y: Effect of charlson comorbidity index and treatment strategy
on survival of elderly patients after endoscopic submucosal
dissection for gastric adenocarcinoma: A multicenter retrospective
study. Front Public Health. 9:8031132022. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Lin JX, Huang YQ, Xie JW, Wang JB, Lu J,
Chen QY, Cao LL, Lin M, Tu RH, Huang ZN, et al: Age-adjusted
charlson comorbidity index (ACCI) is a significant factor for
predicting survival after radical gastrectomy in patients with
gastric cancer. BMC Surg. 19:532019. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Pluchart H, Bailly S, Chanoine S,
Moro-Sibilot D, Bedouch P and Toffart AC: Comparison of seven
comorbidity scores on Four-month survival of lung cancer patients.
BMC Med Res Methodol. 23:2562023. View Article : Google Scholar : PubMed/NCBI
|