Introduction
Multiple myeloma (MM), recognized as the second most
prevalent hematological malignancy globally, is responsible for ~1%
of all cancer diagnoses and ~14% of hematological cancers
worldwide, with annual new cases estimated at ~188,000 (1). Even with progress in treatment
modalities, MM is still considered an incurable disease for most
patients, exhibiting a 5-year relative survival rate of ~60% in
developed nations. The global incidence of MM shows geographical
variation, with higher rates observed in North America, Europe and
Australia compared with Asia (1).
The relapsing-remitting nature of MM and the
necessity for ongoing treatment interventions place a substantial
burden on healthcare systems. Although novel agents such as
immunomodulatory drugs and proteasome inhibitors have been
introduced, high-dose therapy (HDT) with melphalan followed by
autologous stem cell transplantation (ASCT) continues to be a
cornerstone treatment for eligible patients, as per established
guidelines (2–4). Notably, regional variations in
treatment protocols exist; for example, recommendations from the
European Myeloma Network (3), the
American Society for Blood and Marrow Transplantation (2) and Chinese (Chinese Hematology
Association, Chinese Society of Hematology and Chinese Myeloma
Committee-Chinese Hematology Association) guidelines (4) differ concerning the use of
consolidation therapy and the specific role of double ASCT,
reflecting differences in clinical practice and resource
allocation.
The landmark study by Attal et al (5) in 1996 first provided a comparative
analysis of response rates, event-free survival (EFS) and overall
survival (OS) between HDT followed by ASCT (HDT/ASCT) and
conventional chemotherapy (CCT). This was followed by several
randomized controlled trials (RCTs) that corroborated the finding
that single HDT/ASCT led to an improved complete response (CR) rate
compared with CCT (6–9). Double HDT/ASCT is defined as the
administration of a second HDT/ASCT procedure within a 6-month
window following the initial transplantation (10). A 2003 report by Attal et al
(11) indicated superior EFS and
7-year survival rates with double HDT/ASCT compared with the single
transplantation approach.
Nonetheless, the clinical benefit of double
transplantation remains a point of contention, as evidenced by the
mixed results from subsequent clinical trials (12–17).
In 2009, Kumar et al (18)
published a meta-analysis assessing the effectiveness and safety
profile of single vs. double HDT/ASCT. However, the retraction of
one study included in the analysis has cast doubt on the robustness
of its conclusions. To address these uncertainties in a
comprehensive manner, the present study performed an updated
systematic review and meta-analysis to re-assess the efficacy and
safety of single vs. double HDT/ASCT. Moreover, a network
meta-analysis was performed to draw comparisons between double
HDT/ASCT and single HDT/ASCT, the latter with or without
consolidation therapy.
Materials and methods
Study registration
The present study was performed and reported in
adherence to the guidelines outlined in the Preferred Reporting
Items for Systematic Reviews and Meta-Analyses statement (19). The protocol for the present
systematic review is registered with the International Prospective
Register of Systematic Reviews (registration no.
CRD42022300207).
Data sources
A systematic search of the literature was performed
across the following electronic databases: PubMed (https://pubmed.ncbi.nlm.nih.gov/), the Cochrane
Library (https://www.cochranelibrary.com/) and Embase
(https://www.embase.com/), covering all entries
from database inception to April 12, 2023. The search strategy
employed a combination of key words and Medical Subject Headings
terms, including: ‘multiple myeloma’, ‘myeloma’, ‘plasma cell
myeloma’, ‘autologous stem cell transplantation’, ‘autologous
transplant’, ‘autograft’, ‘stem cell transplant’, ‘hematopoietic
stem cell transplantation’, ‘tandem transplant’, ‘double
transplant’ and ‘high-dose therapy’. Boolean operators (AND, OR)
were applied to combine search terms appropriately. Restrictions on
publication type were not applied. In addition to examining
published trials, the World Health Organization International
Clinical Trials Registry Platform (www.trialsearch.who.int) was also searched for any
relevant registered trials. To ensure a broad scope, the review
incorporated clinical guidelines from several countries. Moreover,
in an effort to minimize publication bias, grey literature sources,
including conference abstracts and academic dissertations, were
also considered (20).
Study selection
The present study exclusively included RCTs to
minimize selection bias and confounding factors, thereby providing
the highest level of evidence on efficacy. Studies were considered
eligible for inclusion if they met all of the following criteria:
i) RCTs; ii) enrolled patients had a confirmed diagnosis of
symptomatic or progressive, previously untreated MM; iii)
participants were randomized to undergo either a single HDT/ASCT or
a double HDT/ASCT within 6 months after the first ASCT; iv)
reported data on response rates, OS, EFS and/or progression-free
survival (PFS) and treatment-related mortality (TRM) for both
treatment arms; and v) published in the English language. Studies
were excluded if they met any of the following criteria: i)
Non-randomized study designs (such as observational studies, case
series or case reports); ii) studies enrolling patients with
relapsed or refractory MM; iii) studies comparing transplantation
strategies other than single vs. double HDT/ASCT; iv) studies that
did not report at least one of the prespecified outcomes of
interest; v) duplicate publications reporting exactly the same
patient cohort and identical outcomes without providing any new
information (conference abstracts that supply additional subgroup
analyses or long-term follow-up data not available in the
corresponding full-text articles were considered complementary and
were included after confirming no overlap in the extracted patient
data); and vi) reviews, editorials, commentaries or guidelines
without original data.
Data extraction
A total of two independent reviewers assessed each
article against the eligibility criteria. A third reviewer was
consulted to arbitrate any discrepancies that arose. Another pair
of reviewers were responsible for extracting the following data
from the studies that were included: i) General study information
(first author, year of publication, study design and sample size);
ii) baseline patient characteristics (diagnosis, prior treatments,
sex and age); iii) details of the treatment protocols (patient
groups, pre-treatment regimens, treatment plans, duration and
follow-up period); and iv) outcomes measured for each group. The
endpoints of primary interest were OS and PFS. Secondary outcomes
encompassed response rate and TRM. Where available, data on adverse
events were also extracted to evaluate safety.
For conference abstracts that provided additional
subgroup or long-term follow-up data not reported in the
corresponding full-text articles, only those unique estimates were
extracted. It was verified that the same patient cohort was not
counted twice for the same outcome in any meta-analysis.
The potential for bias in the included RCTs was
evaluated using the Cochrane Risk of Bias tool, version 2 (RoB 2)
(21). A summary of this assessment
is presented in Table SI, with
detailed domain-level judgments for each included study. Whilst the
Grading of Recommendations, Assessment, Development and Evaluations
(GRADE) framework is another important system for evaluating
evidence certainty, the principal evaluation of methodological
quality and bias risk was grounded in the Cochrane RoB 2 tool. This
method is specifically tailored and extensively validated for use
with RCTs. Consequently, a formal GRADE assessment was not
performed for this analysis.
Data synthesis
A table was constructed to summarize the
characteristics of the included studies, which helped identify the
data available for synthesis. For comparing categorical outcomes
(such as response rate and TRM) between intervention groups, the
risk ratio (RR) was employed. Estimates of the RR were calculated
using Review Manager 5.3 software (The Cochrane Collaboration).
Pairwise meta-analyses were performed, and the results are
displayed as forest plots. A random-effects model was applied for
all meta-analyses to incorporate potential heterogeneity arising
from variations in study populations, protocols and clinical
settings across the included trials. Heterogeneity was assessed
using the Q test and the I2 statistic for descriptive
purposes.
For time-to-event data (OS, EFS and PFS), hazard
ratio (HR) was used for inter-group comparisons. HR estimates were
derived employing the inverse variance method in Stata 16.0
(StataCorp LP). In cases where HRs and their confidence intervals
(CIs) were not directly reported in the publications, they were
approximated from published Kaplan-Meier curves using established
methodological approaches (22).
A network meta-analysis was performed to assess the
relative effects of different treatment strategies (23), utilizing a mixed-effects model in R
software, version 4.2.1 (https://www.R-project.org/). This methodology enabled
the simultaneous comparison of multiple interventions, even in the
absence of direct head-to-head trials, thus yielding a hierarchical
ranking of treatment efficacy and improving the clinical relevance
of the results. Inconsistency within the network was also assessed
using Cochran's Q statistic and a design-by-treatment interaction
model (24). The effects of each
treatment regimen relative to single HDT/ASCT alone are presented
in a forest plot with 95% CIs.
Reporting bias assessment
Publication bias was assessed using Egger's test for
PFS and OS, and Harbord's test for overall response rate and
treatment-related mortality (25,26).
Additional methods for detecting publication bias have been
described by Jin et al (27). For the network meta-analysis of OS,
a funnel plot was generated.
Results
Study selection
The process of study identification is detailed in
Fig. 1. Initially, 1,101 records
were identified. Following a review of titles and abstracts, 18
records were selected for a full-text assessment based on the
inclusion criteria. A total of 8 studies were considered
potentially relevant. In the final selection, 6 full-text articles
and 2 conference abstracts met the eligibility criteria. The 6
full-text articles (11,12,14,17,28,29)
provided data for the conventional pairwise meta-analysis,
encompassing 2,173 unique patients from the arms directly comparing
double vs. single ASCT. The two conference abstracts (30,31)
did not introduce additional patient cohorts; instead, they
supplied supplementary subgroup analyses and extended follow-up
data derived from the same trial populations already represented in
the included full-text articles. No double counting of patients
occurred in any meta-analysis. Among the 8 studies, 5 categorized
patients into different risk groups according to adverse prognostic
factors, and 3 were incorporated into the subgroup meta-analysis
focusing specifically on high-risk patients.
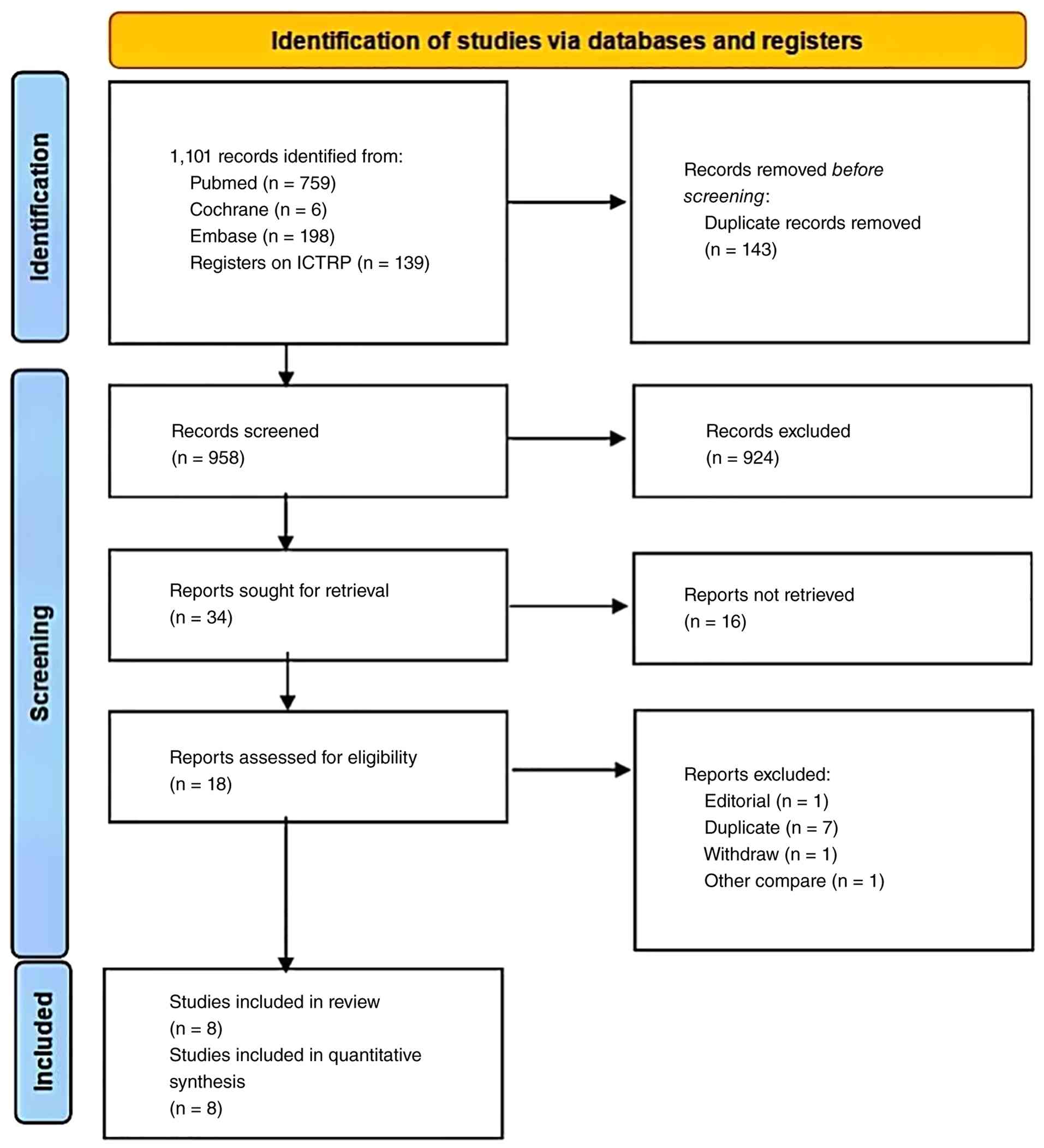 | Figure 1.Preferred Reporting Items for
Systematic reviews and Meta-Analyses flow diagram of the study
selection process outlining the systematic process for identifying,
screening and including studies in the systematic review and
meta-analysis comparing double vs. single ASCT in patients with
multiple myeloma. A total of 1,101 records were identified through
systematic searches of electronic databases (PubMed, n=759;
Cochrane Library, n=6; and Embase, n=198) and the World Health
Organization ICTRP (n=139). After removing 143 duplicate records,
958 unique records underwent title and abstract screening. Of
these, 924 records were excluded as irrelevant. The full text of 34
reports was sought for retrieval; 16 reports could not be
retrieved. The remaining 18 reports were assessed for eligibility
based on the predefined inclusion criteria. A total of 10 reports
were excluded for the following reasons: Editorial material (n=1),
duplicate publication (n=7), withdrawn study (n=1) and comparison
of other interventions (n=1). Ultimately, 8 studies (comprising 6
full-text articles and 2 conference abstracts) met all eligibility
criteria and were included in the qualitative synthesis (systematic
review). All 8 studies also provided sufficient data for
quantitative synthesis (meta-analysis). ACT, autologous stem cell
transplantation; ICTRP, International Clinical Trials Registry
Platform. |
Characteristics of the included
studies
The key features of the included studies are
summarized in Table I. The median
duration of follow-up across these studies varied from 38–134
months. The patient population in each treatment arm ranged between
76–501 individuals. All studies provided a direct comparison of
single vs. double ASCT in patients with MM.
 | Table I.Baseline characteristics of the
randomized controlled trials included in the systematic review and
meta-analysis. |
Table I.
Baseline characteristics of the
randomized controlled trials included in the systematic review and
meta-analysis.
|
|
|
|
|
|
|
| More effective
procedure according to outcomea |
|
|---|
|
|
|
|
|
|
|
|
|
|
|---|
| First author/s,
year | Publication
type | Total patients,
n | Intervention,
n | Induction
(dose) | Consolidation | Median follow-up,
months (range) | OS | PFS | Response rate | TRM | (Refs.) |
|---|
| Attal et al,
2003 | Full text | 399 | ASCT, 200; S-ASCT,
199 | Melphalan (140
mg/m2) | Neither | 75 (36–93) | Neither | D-ASCT | Neither | Neither | (11) |
| Cavo et al,
2007 | Full text | 321 | D-ASCT, 158;
S-ASCT, 163 | Melphalan (200
mg/m2) | Neither | 70 (32–112) | D-ASCT | D-ASCT | D-ASCT | Neither | (12) |
| Cavo et al,
2013 | Abstract | 606 | D-ASCT, 352;
S-ASCT, 254 | Not reported | Neither | Not reported | D-ASCT | D-ASCT | Not reported | Not reported | (30) |
| Mai et al,
2016 | Full text | 358 | D-ASCT, 181;
S-ASCT, 177 | Melphalan (200
mg/m2) | Neither | 134 | Neither | Neither | Neither | Not reported | (14) |
| Rocchi et
al, 2019 | Abstract | 909 | D-ASCT, 408;
S-ASCT, 501 | Not reported | Neither | 117 (91–126) | D-ASCT | D-ASCT | Not reported | Not reported | (31) |
| Stadtmauer et
al, 2019 | Full text | 758 | D-ASCT, 247;
S-ASCT, 257; | Melphalan | RVD | 38 | Neither | Neither | Neither | Neither | (17) |
|
|
|
| S-ASCT + C,
254 | (200
mg/m2) |
|
|
|
|
|
|
|
| Cavo et al,
2020 | Full text | 419 | D-ASCT, 210;
S-ASCT, 209 | Melphalan (200
mg/m2) | Neither | 60 (52–68) | D-ASCT | D-ASCT | Not reported | Not reported | (28) |
| Straka et
al, 2021 | Full text | 340 | D-ASCT, 96; S-ASCT,
76; S-ASCT + C, 76; D-ASCT + C, 92 | Melphalan (140 or
200 mg/m2) | V | 51 | Neither | D-ASCT | Not reported | Not reported | (29) |
The study by Attal et al (11) involved previously untreated patients
classified with Durie-Salmon stage I, II or III myeloma. All
participants received 3–4 cycles of vincristine, doxorubicin,
dexamethasone (VAD) induction chemotherapy prior to
transplantation. The conditioning regimen for the single ASCT arm
consisted of melphalan (140 mg/m2) combined with
total-body irradiation. For the double transplant group, the first
procedure used melphalan (140 mg/m2) alone, and the
second procedure employed the same regimen as the single-transplant
group. Maintenance therapy with interferon-α (IFN-α) was
administered to all patients. Cavo et al (12) (the Bologna 96 trial) enrolled
previously untreated patients with symptomatic MM. All participants
received VAD induction therapy. The conditioning regimen for the
initial transplant was melphalan (200 mg/m2). Patients
assigned to the double transplantation group underwent a second
transplant 3–6 months later, which utilized melphalan (120
mg/m2) combined with busulfan (12 mg/kg). IFN-α served
as the maintenance therapy. This study also performed an analysis
of outcomes specifically for patients who failed to achieve at
least a near-CR after a single transplant. Both Mai et al
(14) (the GMMG-HD2 trial) and
Stadtmauer et al (17) (the
BMT CTN 0702 trial) used high-dose melphalan (200 mg/m2)
as the conditioning regimen. However, these trials did not include
subgroup analyses focused on high-risk patients. Cavo et al
(28) (the EMN02/HO95 MM trial)
also reported outcomes for participants with high-risk cytogenetic
profiles. Straka et al (29)
analyzed pooled data from two clinical trials (NCT00416273 and
NCT00416208), proposing that double ASCT may extend EFS in newly
diagnosed MM. Finally, two conference abstracts (30,31)
also provided data on EFS and OS for the overall patient population
and for subsets with adverse prognostic factors.
Risk of bias in the studies
The results of the risk of bias assessment are
presented in Table SI, with
detailed domain-level judgments for each included study. Whilst all
studies described their randomization procedures, a high
risk-of-bias related to deviations from the intended interventions
was identified. This was primarily due to the inherent difficulty,
if not impossibility, of blinding both participants and healthcare
providers to the transplantation assignment. In certain instances,
participants did not adhere to the study protocol, partly due to
their awareness of the assigned intervention and partly due to
disease progression. All studies reported performing
intention-to-treat analyses. The two conference abstracts (30,31)
lacked detailed information on random sequence generation and the
handling of missing data. Overall, the risk-of-bias for all
included studies was judged to entail ‘some concerns’. A detailed
account of the methodological quality assessment is provided in
Table SI.
Meta-analyses
Fig. 2 shows
response rates and TRM and Fig. 3
presents survival outcomes for high-risk patients.
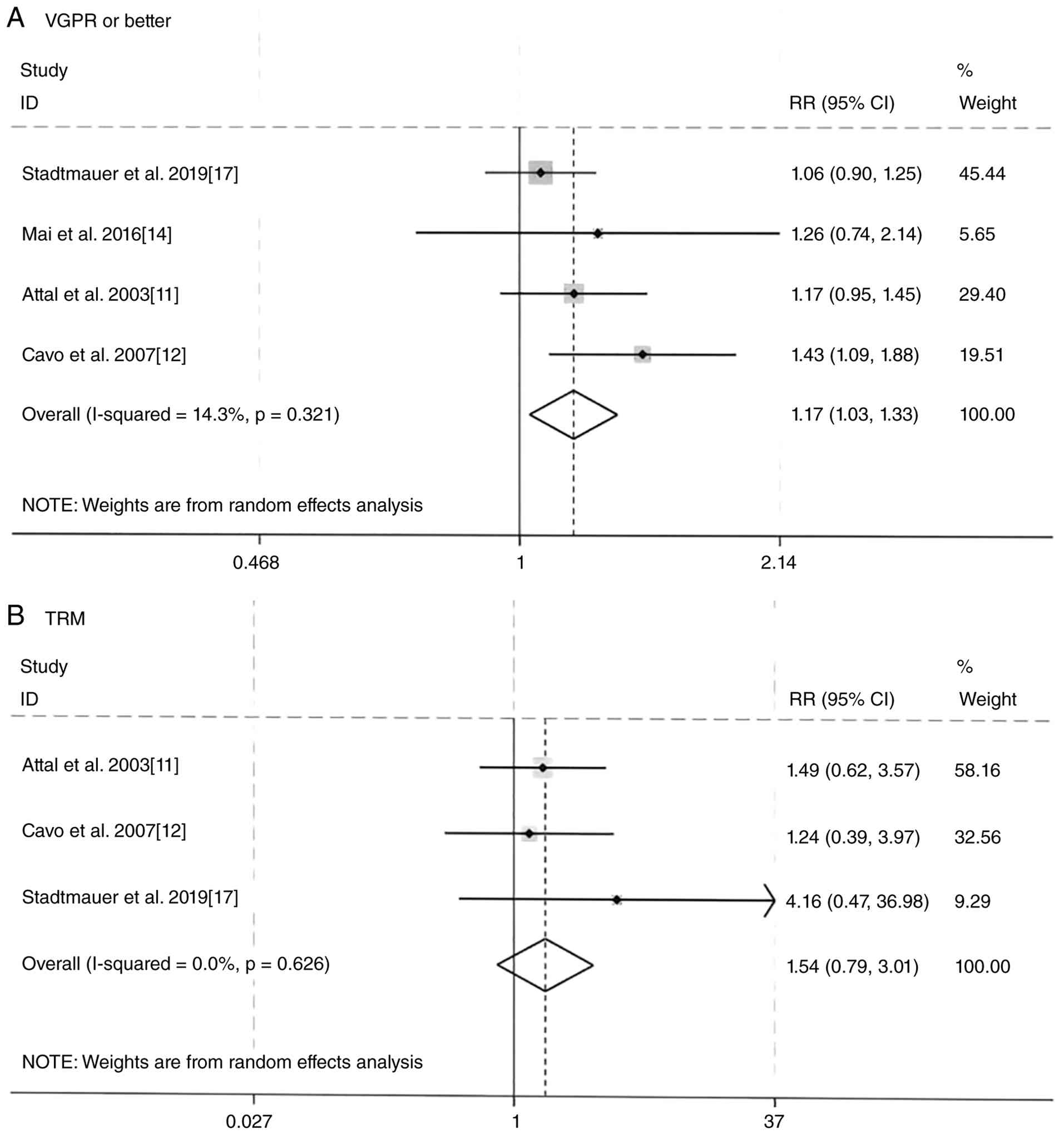 | Figure 2.Forest plots for meta-analysis of
response rates and TRM. (A) Forest plot comparing the achievement
of at least a VGPR between double and single HDT/ASCT. The combined
RR demonstrates a statistically significant benefit in favor of
double HDT/ASCT (RR, 1.17; 95% CI, 1.03–1.33; P=0.02).
Heterogeneity was low (I2=14.3%; P=0.321). (B) Forest
plot comparing TRM between double and single HDT/ASCT. The combined
RR shows no statistically significant difference between the two
strategies (RR, 1.54; 95% CI, 0.79–3.01; P=0.17). No heterogeneity
was observed (I2=0%; P=0.626). A random-effects model
was used for both meta-analyses. TRM, treatment-related mortality;
RR, risk ratio; VGPR, very good partial response; HDT, high-dose
therapy; ASCT, autologous stem cell transplantation; CI, confidence
interval. |
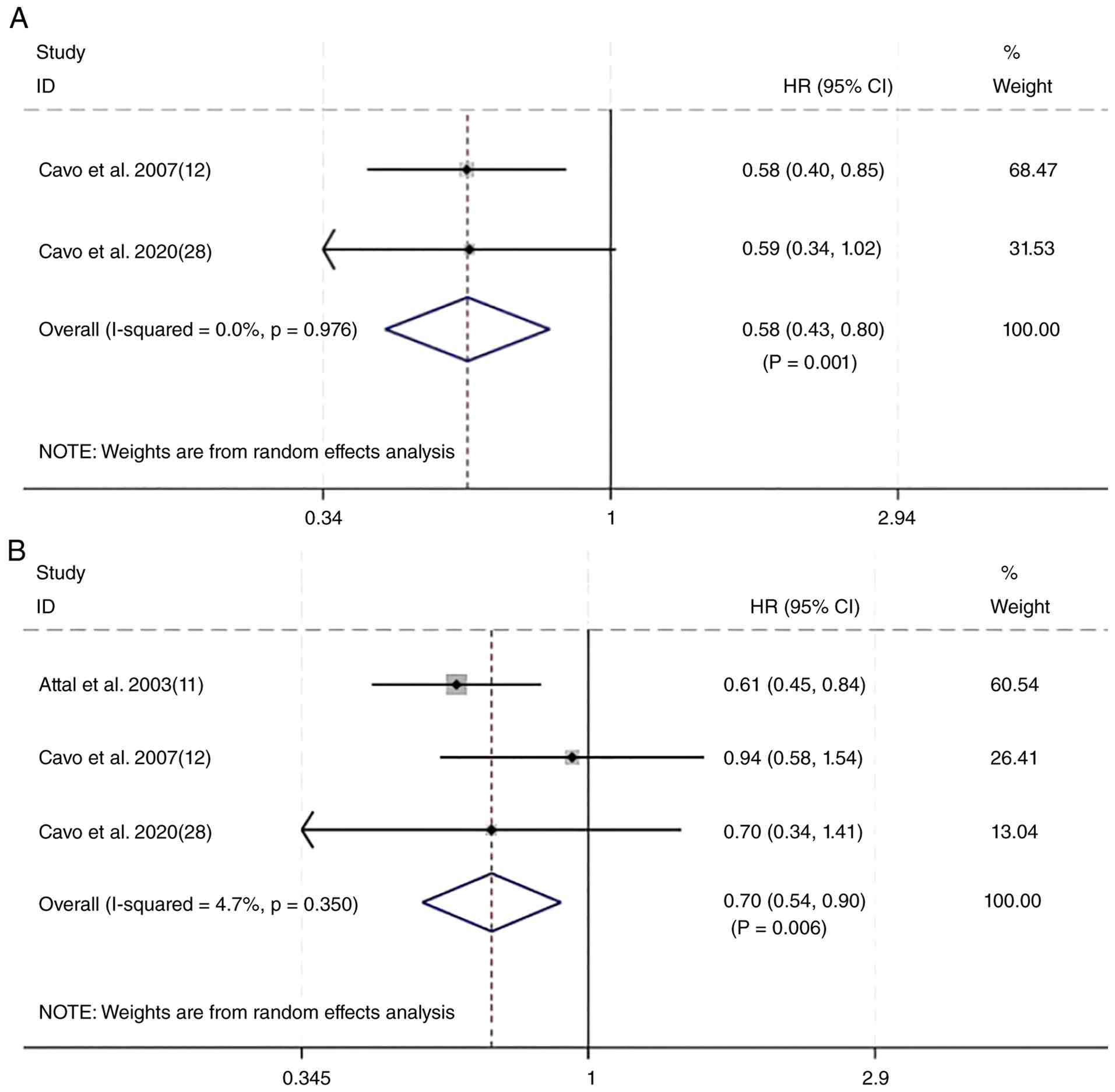 | Figure 3.Forest plots of PFS and OS for
high-risk patients. (A) Forest plot comparing PFS between double
and single HDT/ASCT in patients with at least one adverse
prognostic factor. The combined HR demonstrates a statistically
significant PFS benefit in favor of double HDT/ASCT (HR, 0.58; 95%
CI, 0.43–0.80; P=0.001). (B) Forest plot comparing OS between
double and single HDT/ASCT in the same high-risk patient
population. The combined HR shows a statistically significant OS
benefit for double HDT/ASCT (HR, 0.70; 95% CI, 0.54–0.90; P=0.006).
For the purpose of this analysis, high-risk was defined by the
presence of at least one of the following: Failure to achieve at
least a very good partial response after induction or first
transplant, high-risk cytogenetics or International Staging System
stage II/III disease. A random-effects model was used for both
meta-analyses. PFS, progression-free survival; OS, overall
survival; HDT, high-dose therapy; ASCT, autologous stem cell
transplantation; HR, hazard ratio; CI, confidence interval. |
Meta-analysis of response rates
Data on response rates were available from 5 studies
(11,12,14,17,28).
The meta-analysis of response rates [achievement of at least very
good partial response (VGPR)] included 4 studies that provided
sufficient data for pooling, with results shown in Fig. 2A. Cavo et al (12) reported a significant increase in the
CR/near-CR rate from ~33% with single ASCT to ~47% with double ASCT
(P=0.008). Mai et al (14)
also reported a significant rise in CR rates from the first to the
second HDT/ASCT procedure (P=0.04). By contrast, Attal et al
(11) reported no statistically
significant difference in the CR/VGPR rates between the single and
double transplant groups (42 vs. 50%; P=0.10). Similarly,
Stadtmauer et al (17)
reported no significant advantage for achieving a response of at
least a VGPR with double vs. single HDT/ASCT (P=0.37). The pooled
RR for the ORR (defined as at least partial response) showed no
significant difference between the treatment groups (RR, 1.03;
P=0.42; data not shown). However, using a random-effects model, the
combined RR for achieving a response of at least a VGPR was 1.17
(95% CI, 1.03–1.33; P=0.02), demonstrating a statistically
significant advantage for the double HDT/ASCT approach (Fig. 2A). The analysis indicated no
significant heterogeneity among the studies (I2=14.3%;
P=0.321).
Meta-analysis of TRM
A total of 3 studies provided data on TRM (11,12,17).
The corresponding forest plot is presented in Fig. 2B. No heterogeneity was detected
among these studies (I2=0%; P=0.626). Furthermore, the
results indicated no statistically significant difference in the
risk of TRM between the double and single HDT/ASCT groups (RR,
1.54; 95% CI, 0.79–3.01).
Meta-analysis of double vs. single
transplantation only in patients with adverse prognostic
factors
For this specific analysis, patients were classified
into a high-risk category if they possessed at least one of the
following adverse prognostic factors: i) Failure to achieve at
least a near CR or VGPR following induction therapy or the first
transplant; ii) high-risk cytogenetic abnormalities, as defined by
the original studies [such as the presence of t(4;14), t(14;16) or
del(17p)]; and iii) International Staging System (ISS) stage II or
III disease (32).
A total of 4 studies reported on PFS in patients
characterized by the aforementioned adverse factors (12,28,30,31).
However, only 2 studies (28,30)
provided extractable HR estimates with CIs suitable for
quantitative pooling. Cavo et al (12) reported subgroup findings without
providing usable HRs and Rocchi et al (31) presented median PFS values without
HRs. To avoid potential double-counting of patients from
overlapping cohorts in the conference abstracts, the most complete
and non-duplicative data were prioritized. Therefore, data from
Cavo et al (28) and Cavo
et al (30) were pooled in
the meta-analysis (Fig. 3A). Cavo
et al (30) reported that
double HDT/ASCT was associated with a significantly longer PFS for
patients possessing one or two adverse factors (HR, 0.70; P=0.006).
Rocchi et al (31) reported
a significant PFS benefit from double ASCT in patients with
high-risk cytogenetics (median PFS, 36 months for double ASCT vs.
20 months for single ASCT; P=0.032). The other 2 studies reported
findings consistent with these results. The pooled HR was 0.58 (95%
CI, 0.43–0.80; P=0.001; Fig. 3A),
indicating that double HDT/ASCT significantly extended PFS in
patients presenting with at least one adverse prognostic
factor.
OS data for patients with adverse factors were
available from 4 studies (12,28,30,31).
Cavo et al (30) reported
that patients with two adverse factors who received double HDT/ASCT
had a significantly longer OS compared with those planned for
single HDT/ASCT (HR, 0.32; P=0.001). The OS advantage was
particularly notable for patients who failed to achieve a CR after
induction and who also had high-risk cytogenetics (HR, 0.22;
P=0.001) or ISS stage III MM (HR, 0.42; P=0.033). Rocchi et
al (31) reported an OS benefit
with double HDT/ASCT in the subgroup with high-risk cytogenetics
(10-year OS rates, 51% for double ASCT vs. 34% for single ASCT;
P=0.004). A subgroup meta-analysis for OS was performed using the 3
studies that provided extractable HRs with CIs for patients with
adverse prognostic factors (12,28,30).
Rocchi et al (31) reported
10-year OS rates but did not provide an HR suitable for pooling and
was therefore excluded from the quantitative synthesis. The pooled
analysis demonstrated no significant heterogeneity
(I2=4.7%; P=0.350). Moreover, the combined HR revealed a
statistically significant OS benefit favoring double ASCT for
patients with at least one adverse prognostic factor (HR, 0.70; 95%
CI, 0.54–0.90; P=0.006; Fig.
3B).
Reporting biases
For the pairwise meta-analyses, each outcome
included <10 studies; therefore, funnel plots were not
generated. Instead, quantitative tests were used to assess
publication bias. Egger's test detected no significant bias for PFS
(P=0.437) or OS (P=0.725). Harbord's test showed no significant
bias for overall response rate (P=0.947) or treatment-related
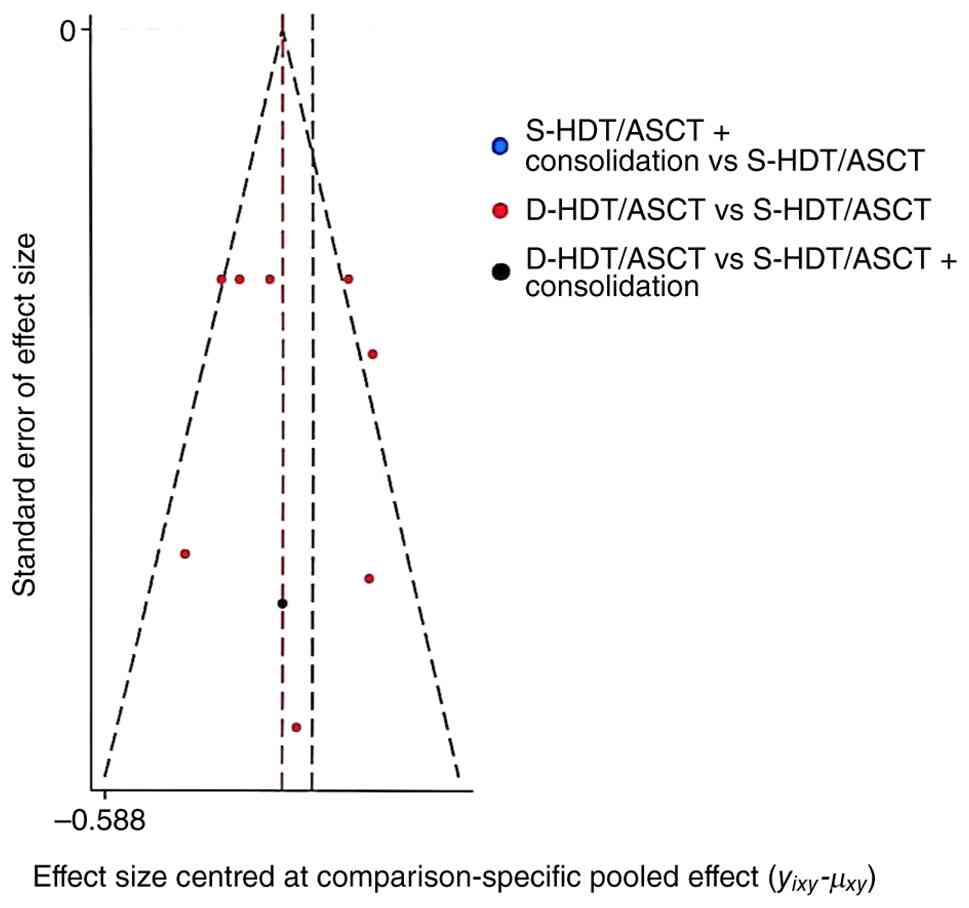
mortality (P=0.470). For the network meta-analysis of overall
survival, a funnel plot is presented in Fig. 4; the symmetrical distribution of
points suggests a low risk of publication bias across the
network.
Network meta-analysis
A network meta-analysis incorporating 6 studies
evaluated PFS across three strategies: Double HDT/ASCT, single
HDT/ASCT augmented with consolidation therapy and single HDT/ASCT
alone (11,12,14,17,28,29).
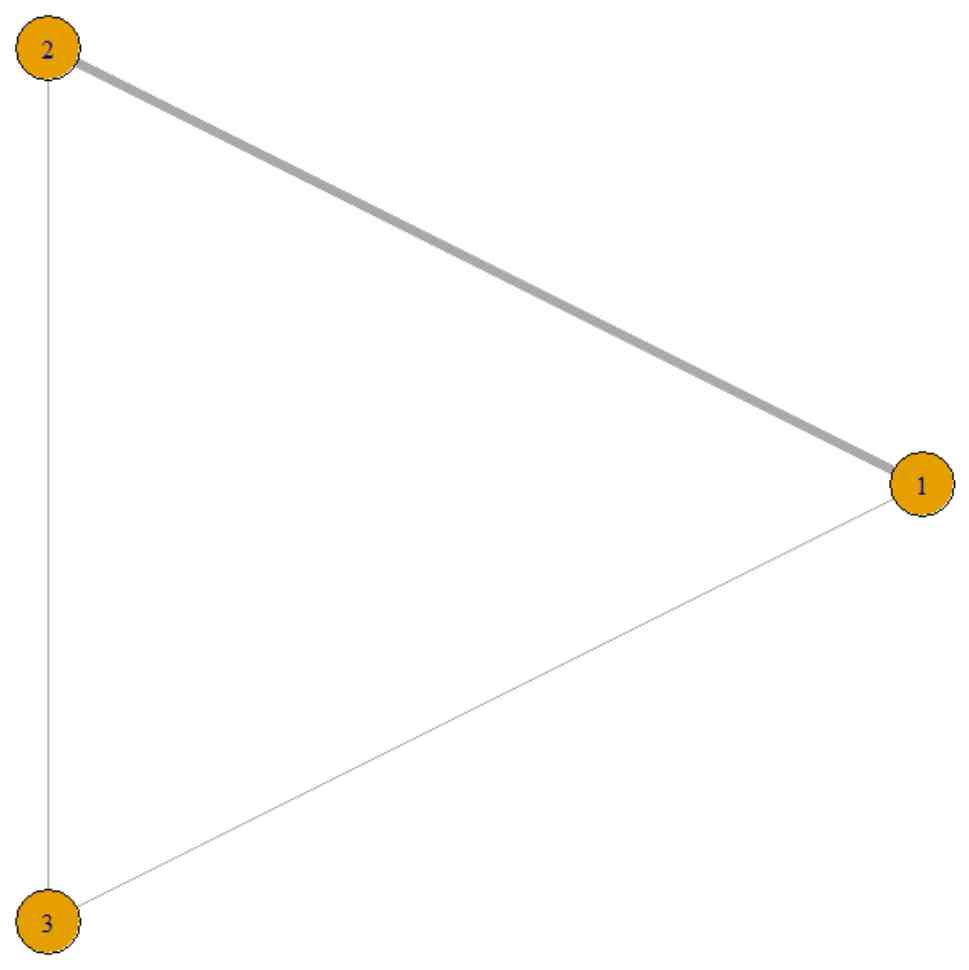
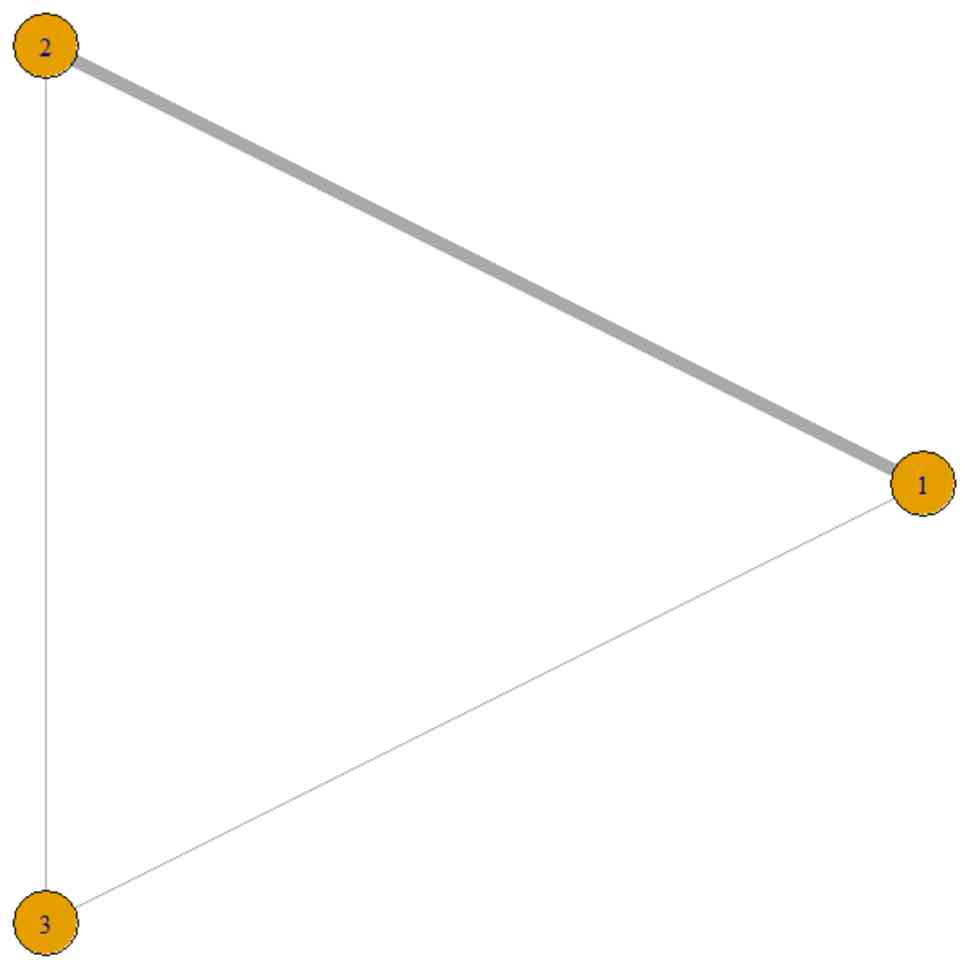
The network structure for these comparisons is illustrated in
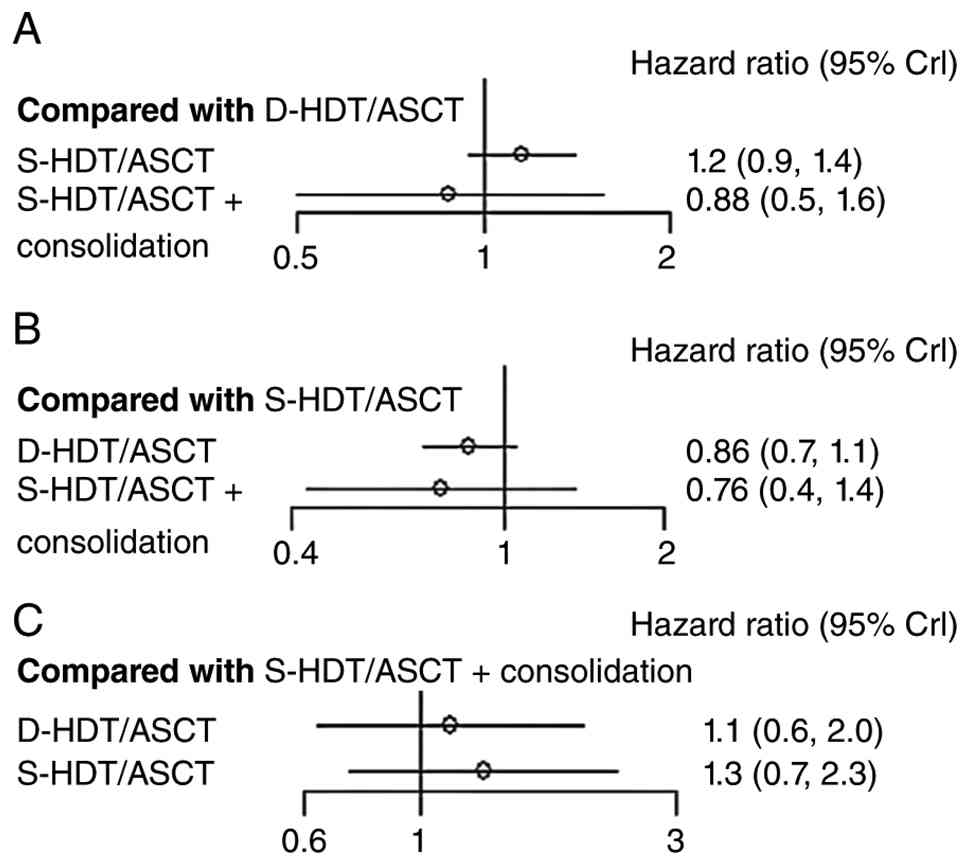
Fig. 5 (PFS network) and Fig. 6 (OS network). Fig. S1, Fig.
S2, Fig. S3 provide network
meta-analysis forest plots for PFS with different references. When
double HDT/ASCT was used as the reference (Fig. S1), single HDT/ASCT alone (HR, 1.2;
95% CI, 1.1–1.4) and single HDT/ASCT with consolidation therapy
(HR, 1.0; 95% CI, 0.8–1.4) did not show a PFS benefit. With single
HDT/ASCT alone as the reference (Fig.
S2), double HDT/ASCT demonstrated a significant PFS benefit
(HR, 0.83; 95% CI, 0.72–0.94), whereas single HDT/ASCT with
consolidation therapy did not (HR, 0.84; 95% CI, 0.6–1.1). When
single HDT/ASCT with consolidation therapy was used as the
reference (Fig. S3), no
significant difference was observed for double HDT/ASCT (HR, 0.99;
95% CI, 0.7–1.3) or single HDT/ASCT alone (HR, 1.2; 95% CI,
0.9–1.6).
Another network meta-analysis, which included all
studies, evaluated OS among the same set of treatment strategies
(11,12,14,17,28–31).
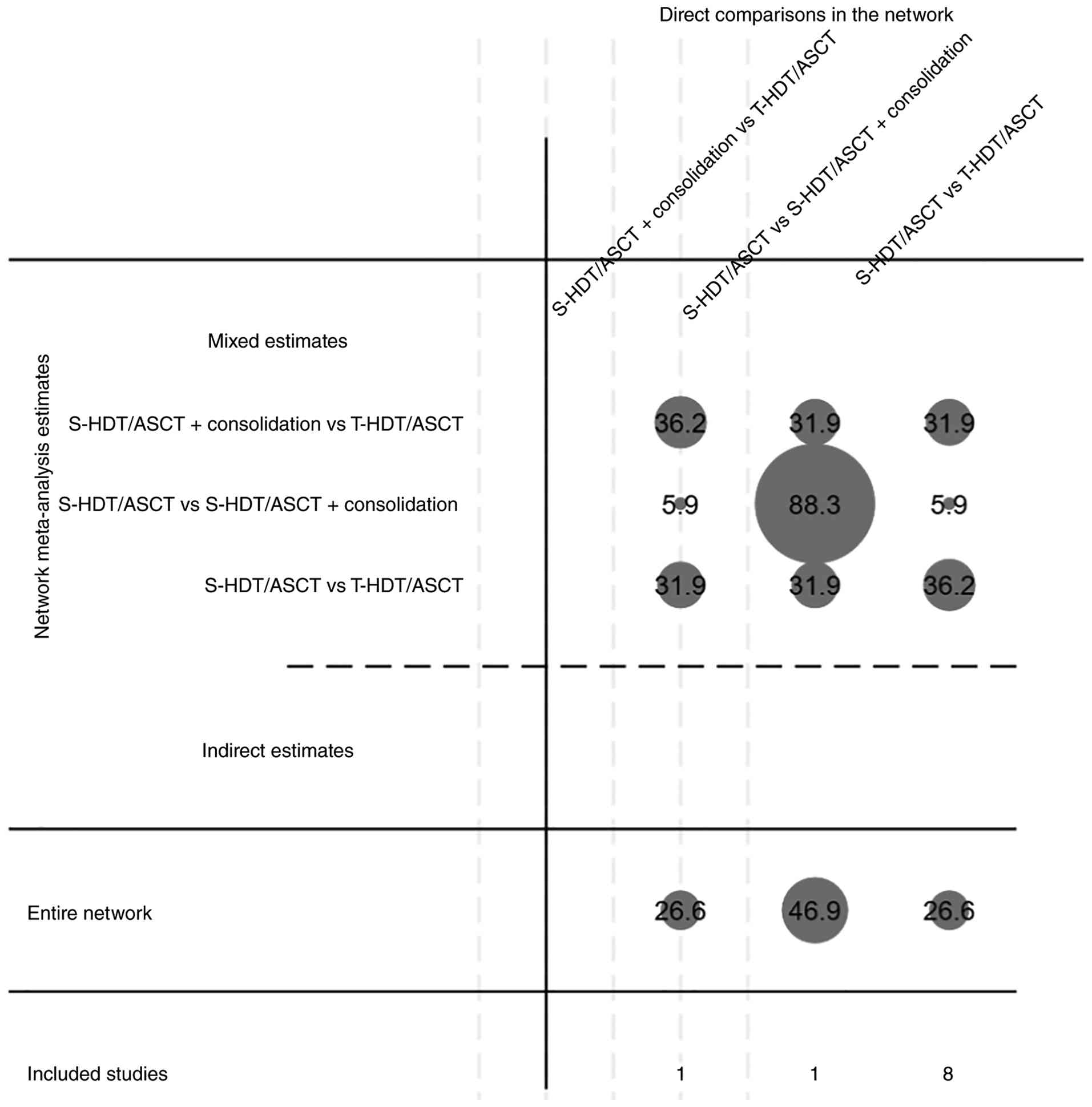
The contribution of direct and indirect evidence to the OS network
estimates is illustrated in Fig. 7,
and the forest plots for all pairwise OS comparisons are
consolidated in Fig. 8. Assessment
for potential publication bias within the OS network is presented
in Fig. 4, and loop-specific
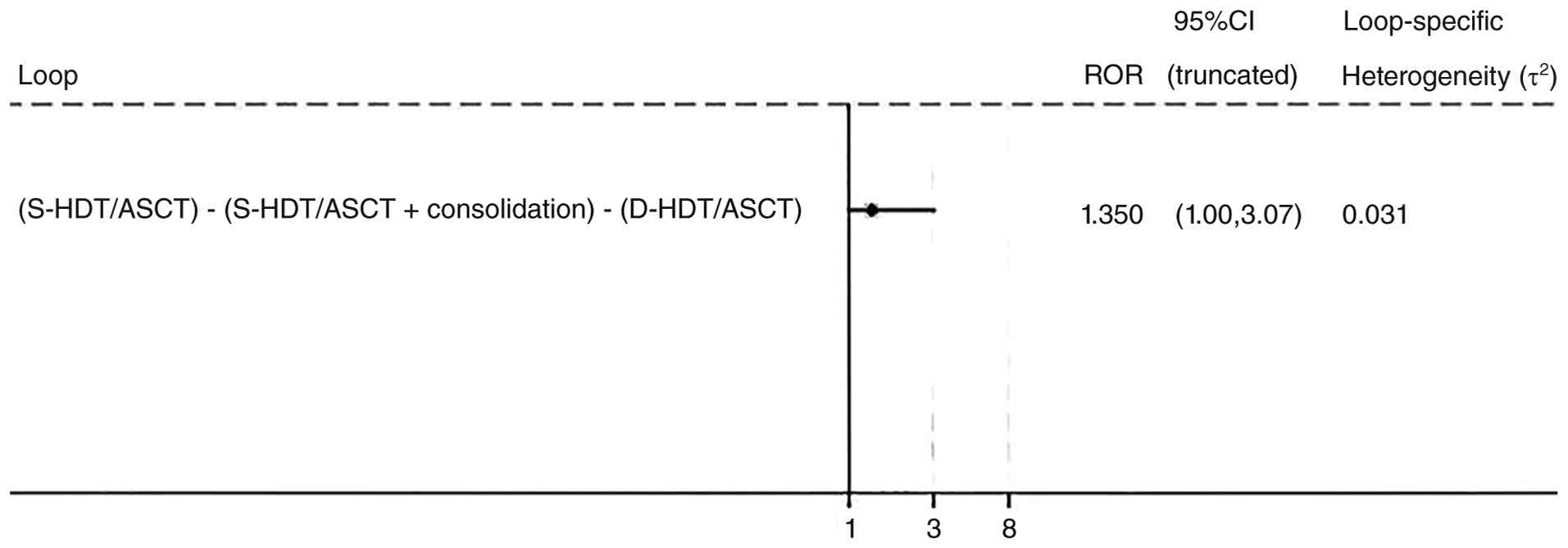
inconsistency is shown in Fig. 9.
Neither double HDT/ASCT (HR, 0.86; 95% CI, 0.71–1.10) nor single
HDT/ASCT with consolidation therapy (HR, 0.76; 95% CI, 0.40–1.40)
showed a statistically significant OS benefit compared with single
HDT/ASCT alone (Fig. 8B).
Furthermore, no significant difference in OS was demonstrated
between double HDT/ASCT and single HDT/ASCT supplemented with
consolidation therapy (HR, 1.10; 95% CI, 0.60–2.00; Fig. 8C). The funnel plot (Fig. 4) demonstrates symmetry around the
vertical line, with points evenly distributed, suggesting a low
risk of publication bias across the studies included in the network
meta-analysis. The 95% CI of the odds ratios (1.00–3.07) from
Fig. 9 included 1, indicating no
statistically significant inconsistency between the direct and
indirect evidence within the network. This supports the consistency
and validity of the network meta-analysis results.
Discussion
The present meta-analysis offers a current and
comprehensive assessment of the efficacy and safety of double vs.
single HDT/ASCT, placing particular emphasis on patients with
high-risk disease characteristics. The key findings revealed that,
for patients harboring at least one adverse prognostic factor,
double HDT/ASCT provided statistically significant and clinically
meaningful enhancements in both PFS (HR, 0.58; P<0.001) and OS
(HR, 0.70; P=0.006), without a concomitant increase in TRM.
Additionally, although the ORR was similar between the two
strategies, the double transplantation approach resulted in a
significantly greater proportion of patients achieving a response
level of at least a VGPR.
The therapeutic role of double HDT/ASCT in the
management of MM has been a long-debated topic. The findings of the
present study may help to resolve this controversy by demonstrating
that the observable benefits of double transplantation are
predominantly concentrated within a specific patient subgroup,
namely those with high-risk disease. This crucial differentiation
may account for the conflicting conclusions reported in earlier
publications. For instance, the influential 2009 meta-analysis by
Kumar et al (18), which
included both randomized and non-randomized studies, concluded that
double ASCT did not offer a marked OS advantage over single ASCT
(relative risk, 1.01; 95% CI, 0.92–1.10). Similarly, a Cochrane
systematic review by Naumann-Winter et al (6) reported no significant differences in
OS or EFS between the two strategies. It is critical to recognize
that these earlier analyses primarily evaluated the effects within
the general MM population and were not sufficiently powered to
performed detailed subgroup analyses based on risk stratification.
By specifically aggregating data from high-risk subgroups across
multiple RCTs, the present study provides evidence that the
apparent absence of an OS benefit in an unselected population
conceals a notable survival advantage for the high-risk cohort.
The biological basis for the aforementioned
observation is sound. High-risk MM, often defined by aggressive
disease biology and rapid clonal evolution (3,28,32),
may not be adequately controlled by a single intensive therapy. A
second, sequential high-dose treatment could potentially achieve a
more notable level of tumor cell reduction (cytoreduction) and
eliminate more therapy-resistant subclones, thereby postponing
disease relapse and improving survival outcomes in this vulnerable
group. This concept is reinforced by the finding of a superior VGPR
rate in the double transplantation arm observed in the present
study, suggesting that deeper therapeutic responses may be both
achievable and clinically impactful.
Moreover, the conclusions of the present study are
in agreement with post-hoc analyses from several major trials. For
example, the EMN02/HO95 study (28)
reported that double ASCT notably improved PFS compared with single
ASCT, with the most pronounced benefit observed in high-risk
patients, including those with high-risk cytogenetics or a
suboptimal response to induction therapy. The integrated analysis
of phase III European studies by Cavo et al (30) also strongly supported the use of
double ASCT for patients with two adverse prognostic factors. In
recent years, numerous meta-analyses and real-world investigations
have further assessed the role of transplant strategies in MM,
providing a wider context for the results of the present study. The
finding of PFS and OS benefits with double ASCT in high-risk
patients is corroborated by several of these contemporary studies.
For example, the recent systematic review and meta-analysis by Chen
et al (33) reported that
double ASCT improved PFS and OS in high-risk individuals.
Similarly, a retrospective propensity score-matching study by Wu
et al (34) and a systematic
review with meta-analysis by Li et al (35) both reported superior survival
outcomes with double ASCT in selected patient subgroups, which
aligns with the primary findings of the present study. Further
bolstering the external validity of the results of the present
study, real-world studies from diverse geographical regions,
including the study by Dou et al (36) in China and Grieb et al
(37) in Germany, reported that the
survival benefit of double ASCT is especially notably in high-risk
cases. However, the clinical context is continuously evolving.
Venner et al (38) proposed
that in the current era of effective maintenance therapy, the
benefit of double ASCT for high-risk patients might be reduced.
This nuance is consistent with the network meta-analysis finding of
the present study, which revealed no significant difference between
double ASCT and single ASCT combined with consolidation therapy.
Other reviews have addressed related but distinct questions, such
as the role of allogeneic transplantation (39–41) or
sequential autologous-allogeneic strategies (42,43) or
have provided historical overviews of ASCT (44,45).
Whilst these studies do not directly contradict the findings of the
present study, they underscore the complexity of the treatment
landscape in which the analysis is positioned. The collective
evidence from these publications (33–45)
confirms the ongoing relevance of the present work and its
consistency with an expanding body of literature that advocates for
a risk-adjusted approach to treatment intensification.
Notably, the network meta-analysis performed in the
present study introduces a refined perspective to clinical
decision-making. It was demonstrated that there was no
statistically significant difference in the extension of PFS or OS
between double HDT/ASCT and single HDT/ASCT followed by
consolidation therapy. This implies that the strategy for
intensifying treatment in high-risk patients may not be exclusively
confined to a second transplant; potent, drug-based consolidation
could represent an alternative method to improve clinical outcomes.
This aligns with the evolving treatment paradigm wherein novel
agents are being incorporated into all phases of MM therapy
(3,4,28).
However, it is imperative to acknowledge a marked limitation of the
present analysis: The majority of the included trials were
performed during a period when the use of contemporary induction
regimens and maintenance therapy was limited. The BMT CTN 0702
trial (17), which integrated both
consolidation and maintenance therapy into its design, did not
demonstrate superior outcomes for double ASCT over single ASCT with
consolidation, suggesting the potential for modern drug-based
strategies to reduce the necessity for a second transplant.
Consequently, a pivotal and still unresolved question is whether
double ASCT remains superior to single ASCT followed by effective
consolidation and maintenance therapy in high-risk patients who
have been treated with modern triplet or quadruplet induction
regimens. Therefore, there is a pressing need for future clinical
trials that directly compare these two intensification strategies
within the context of contemporary therapeutic protocols.
Beyond the evidence from randomized trials, several
large real-world studies have also investigated the role of double
ASCT. Although these analyses are susceptible to potential
selection biases, they offer valuable insights into the
effectiveness of this strategy in broader, more heterogeneous
clinical practice settings. For example, a large registry analysis
by Côté et al (46) reported
superior survival outcomes with double ASCT compared with single
ASCT in high-risk patients, particularly those with high-risk
cytogenetic profiles. This finding aligns with the results of the
present study and strengthens the generalizability of the
conclusion that high-risk patients derive the most benefit from
transplant intensification, defined as the administration of a
second, sequential high-dose therapy followed by autologous stem
cell transplantation (double ASCT) within 6 months of the first
procedure (10). The convergence of
evidence from both rigorous RCTs and extensive real-world data
reinforces the potential value of double ASCT as a strategic option
for this challenging patient population.
However, several limitations inherent in the present
study should be considered. First, the number of studies available
for the high-risk subgroup meta-analysis was relatively small,
which prevented more detailed analyses, such as those based on the
number of risk factors or specific types of high-risk features
[such as del(17p) vs. t(4;14)]. Second, the definition of
‘high-risk’ was not uniform across the included trials,
incorporating clinical, biochemical and cytogenetic factors, which
introduced a degree of heterogeneity into the analysis. Third, the
applicability of the findings to patients receiving current
standard-of-care induction and maintenance therapy remains
uncertain.
Notwithstanding the aforementioned limitations, the
present study provides robust evidence to support the use of double
ASCT for patients with MM with high-risk characteristics. Moreover,
it helps to reconcile previously contradictory literature by
emphasizing risk status as a pivotal factor determining which
patients are most likely to benefit.
In conclusion, the results of the present study
indicate that double HDT/ASCT exhibits a safety profile comparable
with that of single HDT/ASCT. Patients with high-risk MM may obtain
significant survival benefits from undergoing double HDT/ASCT,
which should be considered a valuable therapeutic alternative for
this specific population.
Supplementary Material
Supporting Data
Supporting Data
Acknowledgements
Not applicable.
Funding
This research was funded by the Sanming Project of Medicine in
Shenzhen (grant no. SZSM202301035).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
WC and HC conceived the study and developed its
design. SQ performed literature search and screening, data
extraction from eligible studies, and prepared the initial draft of
the manuscript. LZ conducted data extraction, quality assessment
using the RoB 2 tool, and contributed to the preparation of summary
tables. YL performed the formal meta-analysis and network
meta-analysis, including all statistical analyses. QZ, PZ, FD, JC,
XX and DL participated in data curation, verification of extracted
data and critical review of the manuscript. SQ, YL and LZ confirm
the authenticity of all the raw data. All authors read and approved
the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
ASCT
|
autologous stem cell
transplantation
|
|
CCT
|
conventional chemotherapy
|
|
CI
|
confidence interval
|
|
CR
|
complete response
|
|
EFS
|
event-free survival
|
|
HDT
|
high-dose therapy
|
|
HR
|
hazard ratio
|
|
IFN-α
|
interferon-α
|
|
ISS
|
international staging system
|
|
MM
|
multiple myeloma
|
|
ORR
|
overall response rate
|
|
OS
|
overall survival
|
|
PFS
|
progression-free survival
|
|
RCTs
|
randomized controlled trials
|
|
RoB 2
|
risk of bias tool version 2
|
|
RR
|
risk ratio
|
|
TRM
|
treatment-related mortality
|
|
VAD
|
vincristine, doxorubicin,
dexamethasone
|
|
VGPR
|
very good partial response
|
References
|
1
|
Mafra A, Laversanne M, Marcos-Gragera R,
Chaves HVS, McShane C, Bray F and Znaor A: The global multiple
myeloma incidence and mortality burden in 2022 and predictions for
2045. J Natl Cancer Inst. 117:907–914. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Shah N, Callander N, Ganguly S, Gul Z,
Hamadani M, Costa L, Sengsayadeth S, Abidi M, Hari P, Mohty M, et
al: Hematopoietic stem cell transplantation for multiple myeloma:
Guidelines from the American society for blood and marrow
transplantation. Biol Blood Marrow Transplant. 2:1155–1166. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Engelhardt M, Terpos E, Kleber M, Gay F,
Wäsch R, Morgan G, Cavo M, van de Donk N, Beilhack A, Bruno B, et
al: European myeloma network recommendations on the evaluation and
treatment of newly diagnosed patients with multiple myeloma.
Haematologica. 99:232–242. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Chinese Hematology Association; Chinese
Society of Hematology; Chinese Myeloma Committee-Chinese Hematology
Association, : The guidelines for the diagnosis and management of
multiple myeloma in China (2020 revision). Zhonghua Nei Ke Za Zhi.
59:341–346. 2020.(In Chinese).
|
|
5
|
Attal M, Harousseau JL, Stoppa AM, Sotto
JJ, Fuzibet JG, Rossi JF, Casassus P, Maisonneuve H, Facon T, Ifrah
N, et al: A prospective, randomized trial of autologous bone marrow
transplantation and chemotherapy in multiple myeloma. Intergroupe
Français du Myélome. N Engl J Med. 335:91–97. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Naumann-Winter F, Greb A, Borchmann P,
Bohlius J, Engert A and Schnell R: First-line tandem high-dose
chemotherapy and autologous stem cell transplantation versus single
high-dose chemotherapy and autologous stem cell transplantation in
multiple myeloma, a systematic review of controlled studies.
Cochrane Database Syst Rev. 10:CD0046262012.PubMed/NCBI
|
|
7
|
Child JA, Morgan GJ, Davies FE, Owen RG,
Bell SE, Hawkins K, Brown J, Drayson MT and Selby PJ; Medical
Research Council Adult Leukaemia Working Party, : High-dose
chemotherapy with hematopoietic stem-cell rescue for multiple
myeloma. N Engl J Med. 348:1875–1883. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bladé J, Rosiñol L, Sureda A, Ribera JM,
Díaz-Mediavilla J, García-Laraña J, Mateos MV, Palomera L,
Fernández-Calvo J, Martí JM, et al: High-dose therapy
intensification compared with continued standard chemotherapy in
multiple myeloma patients responding to the initial chemotherapy:
Long-term results from a prospective randomized trial from the
Spanish cooperative group PETHEMA. Blood. 106:3755–3759. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fermand JP, Katsahian S, Divine M, Leblond
V, Dreyfus F, Macro M, Arnulf B, Royer B, Mariette X, Pertuiset E,
et al: High-dose therapy and autologous blood stem-cell
transplantation compared with conventional treatment in myeloma
patients aged 55 to 65 years: Long-term results of a randomized
control trial from the Group MyelomeAutogreffe. J Clin Oncol.
23:9227–9233. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ntanasis-Stathopoulos I, Gavriatopoulou M,
Kastritis E, Terpos E and Dimopoulos MA: Multiple myeloma: Role of
autologous transplantation. Cancer Treat Rev. 82:1019292020.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Attal M, Harousseau JL, Facon T, Guilhot
F, Doyen C, Fuzibet JG, Monconduit M, Hulin C, Caillot D,
Bouabdallah R, et al: Single versus double autologous stem-cell
transplantation for multiple myeloma. N Engl J Med. 349:2495–2502.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Cavo M, Tosi P, Zamagni E, Cellini C,
Tacchetti P, Patriarca F, Di Raimondo F, Volpe E, Ronconi S,
Cangini D, et al: Prospective, randomized study of single compared
with double autologous stem-cell transplantation for multiple
myeloma: Bologna 96 clinical study. J Clin Oncol. 25:2434–2441.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sonneveld P, van der Holt B, Segeren CM,
Vellenga E, Croockewit AJ, Verhoe GE, Cornelissen JJ, Schaafsma MR,
van Oers MH, Wijermans PW, et al: Intermediate-dose melphalan
compared with myeloablative treatment in multiple myeloma:
Long-term follow-up of the Dutch Cooperative Group HOVON 24 trial.
Haematologica. 92:928–935. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Mai EK, Benner A, Bertsch U, Brossart P,
Hänel A, Kunzmann V, Naumann R, Neben K, Egerer G, Ho AD, et al:
Single versus tandem high-dose melphalan followed by autologous
blood stem cell transplantation in multiple myeloma: Long-term
results from the phase III GMMG-HD2 trial. Br J Haematol.
173:731–741. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Cavo M, Gay FM, Patriarca F, Zamagni E,
Montefusco V, Dozza L, Galli M, Bringhen S, Testoni N, Grasso M, et
al: Double autologous stem cell transplantation significantly
prolongs progression-free survival and overall survival in
comparison with single autotransplantation in newly diagnosed
multiple myeloma: An analysis of phase 3 EMN02/H095 study. Blood.
130 (Suppl 1):S4012017.
|
|
16
|
Cavo M, Goldschmidt H, Rosinol L, Pantanil
Zweegman S, Salwender HJ, Lahuerta JJ, Lokhorst HM, Petrucci MT,
Igor B, et al: Double vs. single autologous stem cell
transplantation for newly diagnosed multiple myeloma: Long-term
follow-up (10-years) analysis of randomized phase 3 studies. Blood.
132 (Suppl 1):S1242018. View Article : Google Scholar
|
|
17
|
Stadtmauer EA, Pasquini MC, Blackwell B,
Hari P, Bashey A, Devine S, Efebera Y, Ganguly S, Gasparetto C,
Geller N, et al: Autologous transplantation, consolidation, and
maintenance therapy in multiple myeloma: Results of the BMT CTN
0702 trial. J Clin Oncol. 37:589–597. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kumar A, Kharfan-Dabaja MA, Glasmacher A
and Djulbegovic B: Tandem versus single autologous hematopoietic
cell transplantation for the treatment of multiple myeloma: A
systematic review and meta-analysis. J Natl Cancer Inst.
101:100–106. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Page MJ, McKenzie JE, Bossuyt PM, Boutron
I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan
SE, et al: The PRISMA 2020 statement: An updated guideline for
reporting systematic reviews. BMJ. 372:n712021. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Higgins J and Green S: Cochrane handbook
for systematic reviews of interventions version 5.0.0. Cochrane
Collaboration. John Wiley & Sons Ltd.; West Sussex: 2008,
Available from:. www.cochrane-handbook.org
|
|
21
|
Sterne JAC, Savović J, Page MJ, Elbers RG,
Blencowe NS, Boutron I, Cates CJ, Cheng HY, Corbett MS, Eldridge
SM, et al: Rob 2: A revised tool for assessing risk of bias in
randomised trials. BMJ. 366:l48982019. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tierney JF, Stewart LA, Ghersi D, Burdett
S and Sydes MR: Practical methods for incorporating summary
time-to-event data into meta-analysis. Trials. 8:162007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Rücker G, Schwarzer G and Krahn U:
Netmeta: Network metaanalysis using frequentist methods. Version
0.8–0. 2016.Available from:. https://cran.r-project.org/web/packages/netmeta/index.html
|
|
24
|
Higgins JPT, Jackson D, Barrett JK, Lu G,
Ades AE and White IR: Consistency and inconsistency in network
meta-analysis: Concepts and models for multi-arm studies. Res Synth
Methods. 3:98–110. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sterne JAC, Sutton AJ, Ioannidis JPA,
Terrin N, Jones DR, Lau J, Carpenter J, Rücker G, Harbord RM,
Schmid CH, et al: Recommendations for examining and interpreting
funnel plot asymmetry in meta-analyses of randomised controlled
trials. BMJ. 343:d40022011. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Rücker G, Schwarzer G and Carpenter J:
Arcsine test for publication bias in meta-analyses with binary
outcomes. Stat Med. 27:746–763. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Jin ZC, Zhou XH and He J: Statistical
methods for dealing with publication bias in meta-analysis. Stat
Med. 34:343–360. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Cavo M, Gay F, Beksac M, Pantani L,
Petrucci MT, Dimopoulos MA, Dozza L, van der Holt B, Zweegman S,
Oliva S, et al: Autologous haematopoietic stem-cell transplantation
versus bortezomib-melphalan-prednisone, with or without
bortezomib-lenalidomide-dexamethasone consolidation therapy, and
lenalidomide maintenance for newly diagnosed multiple myeloma
(EMN02/HO95): A multicentre, randomised, open-label, phase 3 study.
Lancet Haematol. 7:e456–e468. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Straka C, Salwender H, Knop S, Vogel M,
Müller J, Metzner B, Langer C, Sayer H, Jung W, Dürk HA, et al:
Full or intensity-reduced high-dose melphalan and single or double
autologous stem cell transplant with or without bortezomib
consolidation in patients with newly diagnosed multiple myeloma.
Eur J Haematol. 107:529–542. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Cavo M, Salwender H, Rosiñol L, Moreau P,
Petrucci MT, Blau IW, Bladé J, Attal M, Patriarca F, Weisel K, et
al: Double vs single autologous stem cell transplantation after
bortezomib-based induction regimens for multiple myeloma: An
integrated analysis of patient-level data from phase European III
studies. Blood. 122:7672013. View Article : Google Scholar
|
|
31
|
Cavo M, Goldschmidt H, Rosinol L, Pantani
L, Zweegman S, Salwender HJ, Lahuerta JJ, Lokhorst HM, Petrucci MT,
Blau I, et al: Double vs single autologous stem cell
transplantation for newly diagnosed multiple myeloma: Long-term
follow-up (10-years) analysis of randomized phase 3 studies. Blood.
132 (Supplement 1):1242018. View Article : Google Scholar
|
|
32
|
Greipp PR, San Miguel J, Durie BGM,
Crowley JJ, Barlogie B, Bladé J, Boccadoro M, Child JA,
Avet-Loiseau H, Kyle RA, et al: International staging system for
multiple myeloma. J Clin Oncol. 23:3412–3420. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Chen YH, Fogel L, Sun AY, Yang C, Patel R,
Chang WC, Chen PH, Jhou HJ, Chen YC, Dai MS and Lee CH: The
efficacy and safety of tandem transplant versus single stem cell
transplant for multiple myeloma patients: A systematic review and
meta-analysis. Diagnostics (Basel). 14:10302024. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Wu SQ, Li XF, Qiu ZJ, Zhu ZJ, Chen XL,
Chen P, Yuan XH, Zhan R and Li NN: Comparison of tandem and single
autologous stem cell transplantation in multiple myeloma: A
retrospective propensity score-matching study. Blood Sci.
7:e002352025. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Li H, Zheng Y, Gao K and Tian C: Tandem
autologous hematopoietic stem cell transplantation for patients
with multiple myeloma: A systematic review and meta-analysis.
Hematology. 29:23431642024. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Dou X, Ren J, Li J, Liu X, Bao L, Chen Y,
Zhao P, Zhong Y, Peng N, Wen L, et al: Tandem versus single
autologous stem cell transplantation for high-risk multiple myeloma
in the era of novel agents: A real-world study of China. Cancer
Med. 14:e705732025. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Grieb N, Oeser A, Ferle M, Hanke F,
Flossdorf S, Sauer S, Goldschmidt H, Müller-Tidow C, Salwender HJ,
Fenk R, et al: Single versus tandem autologous stem cell
transplantation in newly diagnosed multiple myeloma. Bone Marrow
Transplant. 60:335–345. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Venner CP, Duggan P, Song K, Reece D,
Sharma S, Su J, Jimenez-Zepeda VH, McCurdy A, Louzada M, Mian H, et
al: Tandem autologous stem cell transplantation does not benefit
high-risk myeloma patients in the maintenance era: real-world
results from the Canadian myeloma research group database.
Transplant Cell Ther. 30:889–901. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Khorochkov A, Prieto J, Singh KB, Nnadozie
MC, Shrestha N, Dominic JL, Abdal M, Abe RAM, Masroor A and
Mohammed L: The role of allogeneic stem cell transplantation in
multiple myeloma: A systematic review of the literature. Cureus.
13:e183342021.PubMed/NCBI
|
|
40
|
Liberatore C, Fioritoni F and Di Ianni M:
Allogeneic stem cell transplantation in multiple myeloma: Is there
still a place? Front Oncol. 14:14021062024. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Aslam MF, Cheema AY, Shahid D, Maryam B,
Mukhopadhyay D, Munir M, Najam A, Ali HM, Bashir Q and Anwer F:
Historical perspective of allogeneic hematopoietic stem cell
transplantation for multiple myeloma. Acta Haematol. 148:315–329.
2025. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Wei M, Xie C, Huang J, Liu Q and Lai Y:
Autologous followed by allogeneic versus tandem-autologous
transplantation in high-risk, newly diagnosed multiple myeloma: A
systematic review and meta-analysis. Hematology. 28:22695092023.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Kröger N, Wulf G, Hegenbart U, Burchert A,
Stelljes M, Gagelmann N, Brecht A, Kaufmann M, Müller L, Ganser A,
et al: Autologous-allogeneic versus autologous tandem stem cell
transplantation and maintenance therapy with thalidomide for
multiple myeloma patients under 60 years of age: A prospective,
phase II study. Haematologica. 109:1469–1479. 2024.PubMed/NCBI
|
|
44
|
Cohen I, Vaxman I and Gertz MA: Historical
perspective of high-dose therapy followed by autologous stem cell
transplantation in multiple myeloma. Acta Haematol. 148:289–299.
2025.PubMed/NCBI
|
|
45
|
Lin CM, Chang LC, Shau WY, Chen CL, Yao CY
and Tien FM: Treatment benefit of upfront autologous stem cell
transplantation for newly diagnosed multiple myeloma: A systematic
review and meta-analysis. BMC Cancer. 23:4462023. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Côté J, LeBlanc R, Mian H, Chu MP, McCurdy
A, Masih-Khan E, Su J, Jimenez-Zepeda VH, Song K, Louzada M, et al:
Real-world results of autologous stem cell transplantation in newly
diagnosed multiple myeloma: A report from the Canadian Myeloma
Research Group database. Blood Cancer J. 13:1372023. View Article : Google Scholar : PubMed/NCBI
|