Introduction
Esophageal sarcoma is an extremely rare malignant
tumor, accounting for <1% of all esophageal malignancies
(1–3). In contrast to the predominance of
squamous cell carcinoma (SCC) and adenocarcinoma in esophageal
cancer, primary mesenchymal tumors of the esophagus are uncommon,
and their clinicopathological characteristics and optimal treatment
strategies remain poorly defined (1,2). Due
to this rarity, evidence regarding prognosis and standard
management is limited to small case series and case reports.
Esophageal sarcoma may arise as a pure sarcoma or
coexist with epithelial malignant components, particularly SCC,
which is referred to as carcinosarcoma (1,3).
Histologically, these tumors often demonstrate spindle-cell
proliferation and may exhibit heterogeneous differentiation
patterns, making accurate pathological diagnosis challenging,
especially in small biopsy specimens (2,3).
Clinically, patients commonly present with dysphagia, weight loss,
chest discomfort or bleeding, similar to the symptoms of
conventional esophageal carcinoma (1,2).
Compared with ordinary SCC, esophageal sarcoma tends to form
polypoid or protruding intraluminal masses and may grow rapidly
despite relatively preserved swallowing function during the early
phase (2,3).
Although surgery remains the mainstay of treatment
for resectable disease, no consensus has been established regarding
perioperative chemotherapy or chemoradiotherapy (CRT) due to the
rarity of this tumor (1–3). In unresectable locally advanced cases,
treatment strategies are generally adapted from those for
esophageal SCC. Several reports have suggested that esophageal
sarcoma may respond favorably to CRT, including cases with invasion
into adjacent organs (4,5). However, evidence regarding salvage
surgery after definitive CRT (dCRT) for esophageal sarcoma is
extremely limited.
Robot-assisted minimally invasive esophagectomy has
been increasingly adopted for locally advanced esophageal cancer
due to its superior visualization and precise mediastinal
dissection capabilities, particularly in technically demanding
salvage settings after CRT. Nevertheless, to the best of our
knowledge, no previous report has described salvage robot-assisted
subtotal esophagectomy after dCRT for unresectable esophageal
sarcoma with tracheal invasion.
The present study reports a rare case of
unresectable locally advanced esophageal sarcoma with bulky
mediastinal lymph node metastases invading the trachea, which
achieved a pathological complete response after multidisciplinary
treatment consisting of dCRT followed by salvage robot-assisted
minimally invasive esophagectomy.
Case report
Patient
An 82-year-old man presented to Shitennoji hospital
(Osaka, Japan) in October 2024 with dysphagia for solid food. The
medical history included rectal cancer surgery, a thoracic aortic
aneurysm and aortic valve regurgitation. The patient received a
diagnosis of an esophageal tumor and was referred to National
Hospital Organization Osaka National Hospital (Osaka, Japan). An
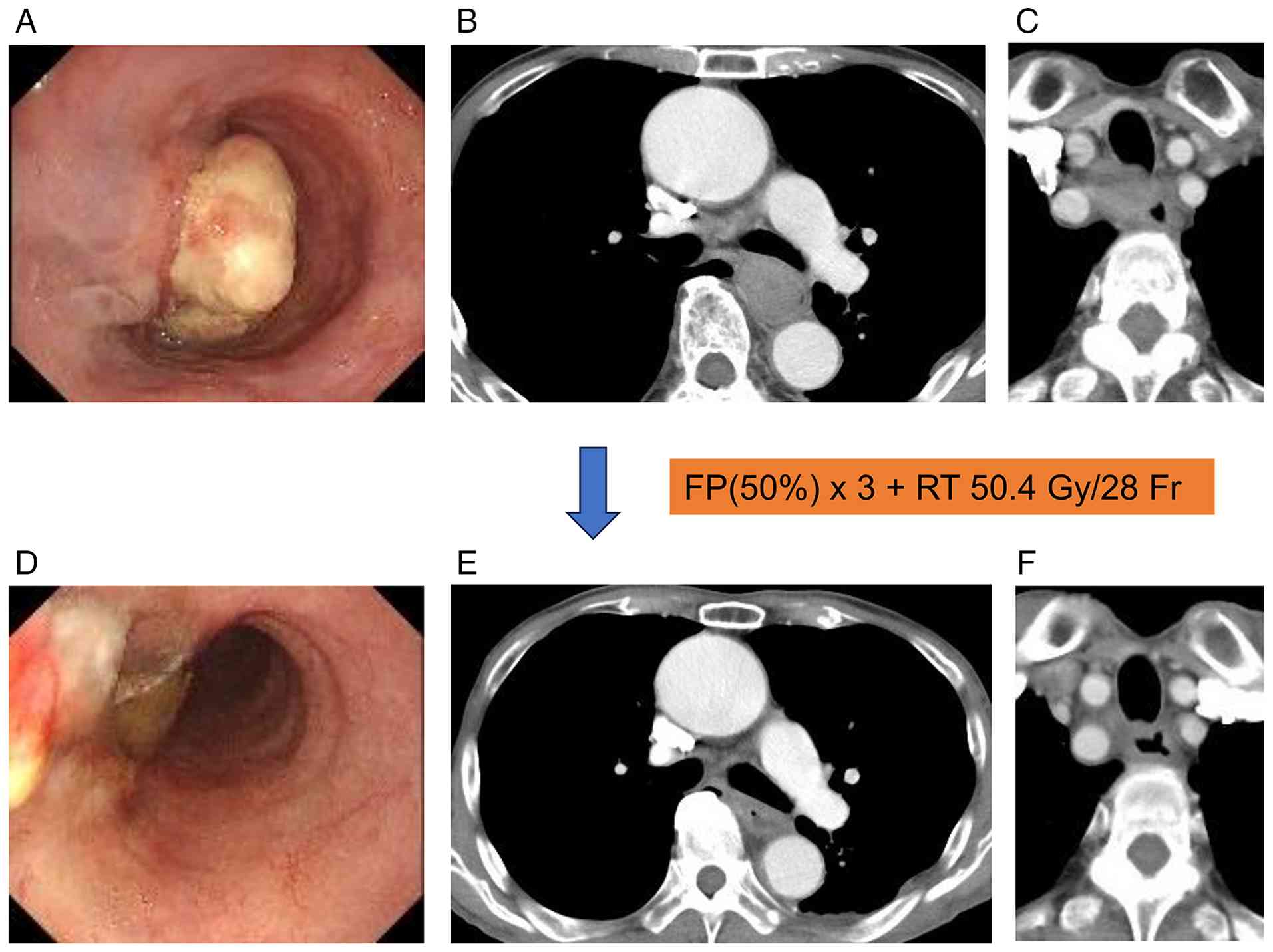
esophagogastroduodenoscopy (EGD) revealed an elevated tumor in the
esophagus at a distance of 30–35 cm from the incisors (Fig. 1A). Endoscopic passage was possible,
and no additional tumors were detected in the stomach or duodenum.
Contrast-enhanced computed tomography (CT) revealed a tumor in the
mid-thoracic esophagus without evidence of distant metastasis,
accompanied by enlarged lymph nodes (nos. 101R and 106recR)
compressing the trachea (Fig. 1B and
C). CT further showed that the tumor was adherent to
approximately one-third of the tracheal circumference, including
the entire tracheal membranous portion, over a length of 5 cm along
the esophageal axis. On axial imaging, the angle of tracheal
involvement from the tumor center was 70°. Tumor compression
resulted in deformation of the tracheal cartilage rings and the
membranous portion, with the membranous wall clearly protruding
into the tracheal lumen. Based on these findings, tracheal invasion
by the enlarged lymph nodes was suspected. A bronchoscopy was
proposed for further investigation; however, the patient did not
consent. Carcinoembryonic antigen and SCC antigen levels remained
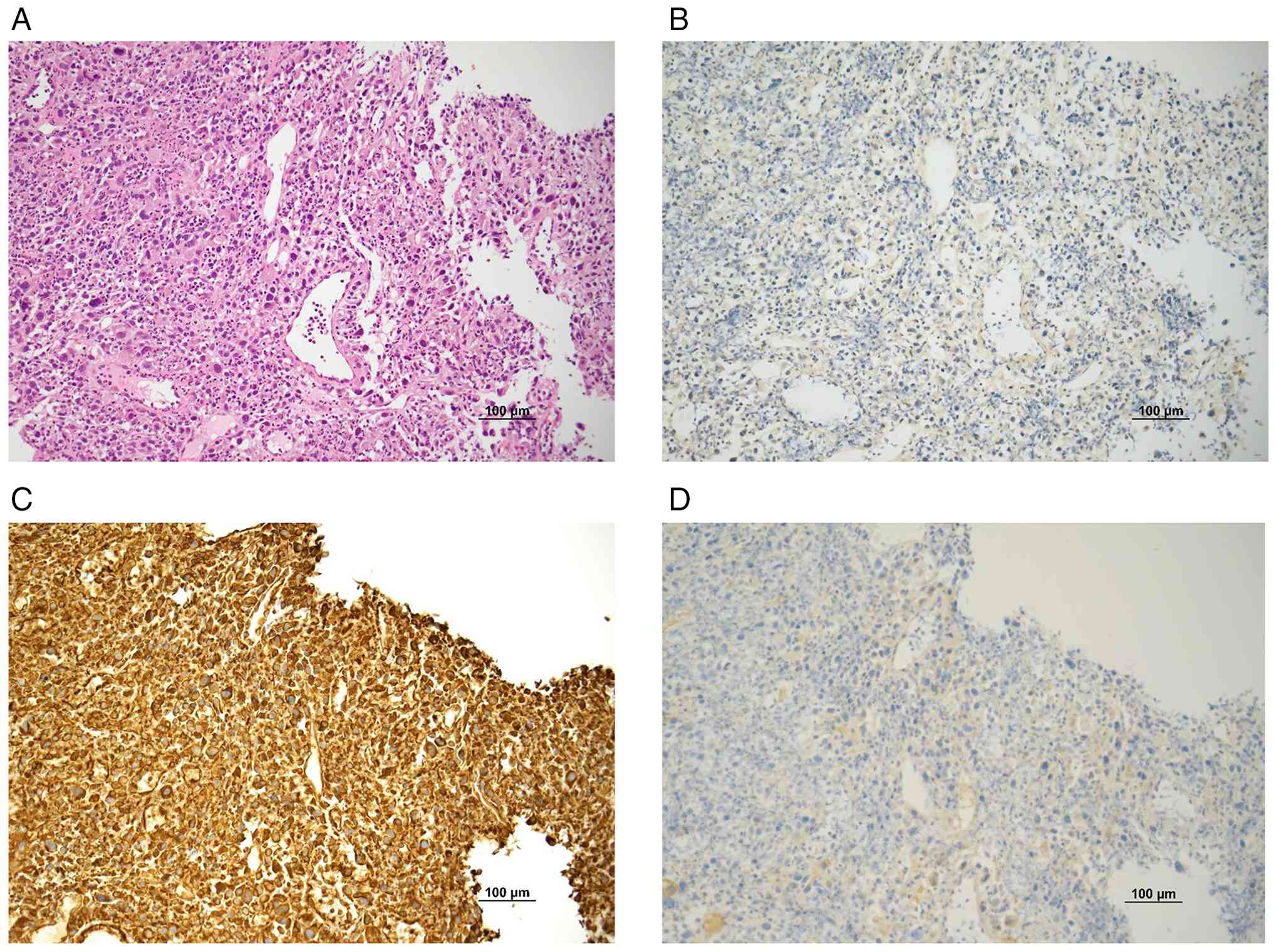
within the normal ranges. Histopathological examination of the
endoscopic biopsy revealed a solid proliferation of atypical
epithelioid cells with enlarged, oval to irregular nuclei on
hematoxylin and eosin staining. During immunohistochemical analysis
(Data S1), AE1/AE3 immunostaining
was negative, while Vimentin immunostaining demonstrated strong
diffuse positivity, indicating the absence of an epithelial
component. Melan-A immunostaining was also negative. Based on these
findings, the endoscopic biopsy was diagnosed as sarcoma (Fig. 2A-D). According to the aforementioned
findings and the 8th edition of the Union for International Cancer
Control Tumor-Node-Metastasis classification, the patient was
diagnosed with locally advanced esophageal sarcoma, cT4
(101R-106recR-trachea) N1M0, cStage IVA, accompanied by enlarged
lymph nodes (nos. 101R and 106recR) infiltrating the trachea
(6,7). After informed consent was obtained
from the patient, definitive CRT was selected as the bulky lymph
nodes (nos. 101R and 106recR) had invaded the trachea and may cause
immediate airway obstruction.
The treatment regimen consisted of RT (50.4 Gy in 28
fractions, 1.8 Gy/day, 5 days per week) combined with
5-fluorouracil + cisplatin (FP) at doses of 560 mg/m2
intravenous 5-fluorouracil on days 1–4 and 56 mg/m2
intravenous cisplatin on day 1. The doses of 5-fluorouracil and
cisplatin were reduced by 50% compared to the recommended dosage
for esophageal cancer (SCC) due to advanced age and impaired renal
function.
After RT (50.4 Gy) and three cycles of FP therapy,
EGD and CT demonstrated shrinkage of the primary tumor and lymph
nodes. One additional cycle of FP therapy was then performed.
Finally, a partial response (PR) was determined according to the
Response Evaluation Criteria in Solid Tumors, version 1.1 (8), and the tumor was considered resectable
based on findings from EGD and CT after RT (50.4 Gy) with three
cycles of FP therapy (Fig. 1D-F).
The patient declined additional examinations, including positron
emission tomography. During CRT, the patient experienced grade 2
hypokalemia and grade 1 diarrhea according to the Common
Terminology Criteria for Adverse Events, version 5.0 (9).
As the EGD and CT scans suggested the possibility of
residual tumors, a discussion was conducted with the patient with
regard to whether to continue chemotherapy or undergo surgery.
After informed consent was obtained again, robot-assisted minimally
invasive esophagectomy (RAMIE) with two-field lymphadenectomy plus
no. 101R and no. 101L node dissection and gastric tube
reconstruction via a posterior mediastinal route were performed as
salvage surgery following CRT.
Operative technique
The da Vinci Xi Surgical System (version 4)
(Intuitive Surgical Operations, Inc.) was used during the thoracic
phase of the surgery. Under general anesthesia, the patient was
placed in the prone position.
da Vinci ports (8 mm) were inserted as follows: The
1st arm port in the 10th intercostal space (ICS) a long a line
parallel to the anterior axillary line (AL) passing through the
inferior angle of the scapula; the 2nd arm port in the 8th ICS on
the middle AL; the 3rd arm port in the 6th ICS on the middle AL;
and the 4th arm port in the 4th ICS on the anterior AL. Assistant
ports included a 5-mm port in the 9th ICS on the anterior AL and a
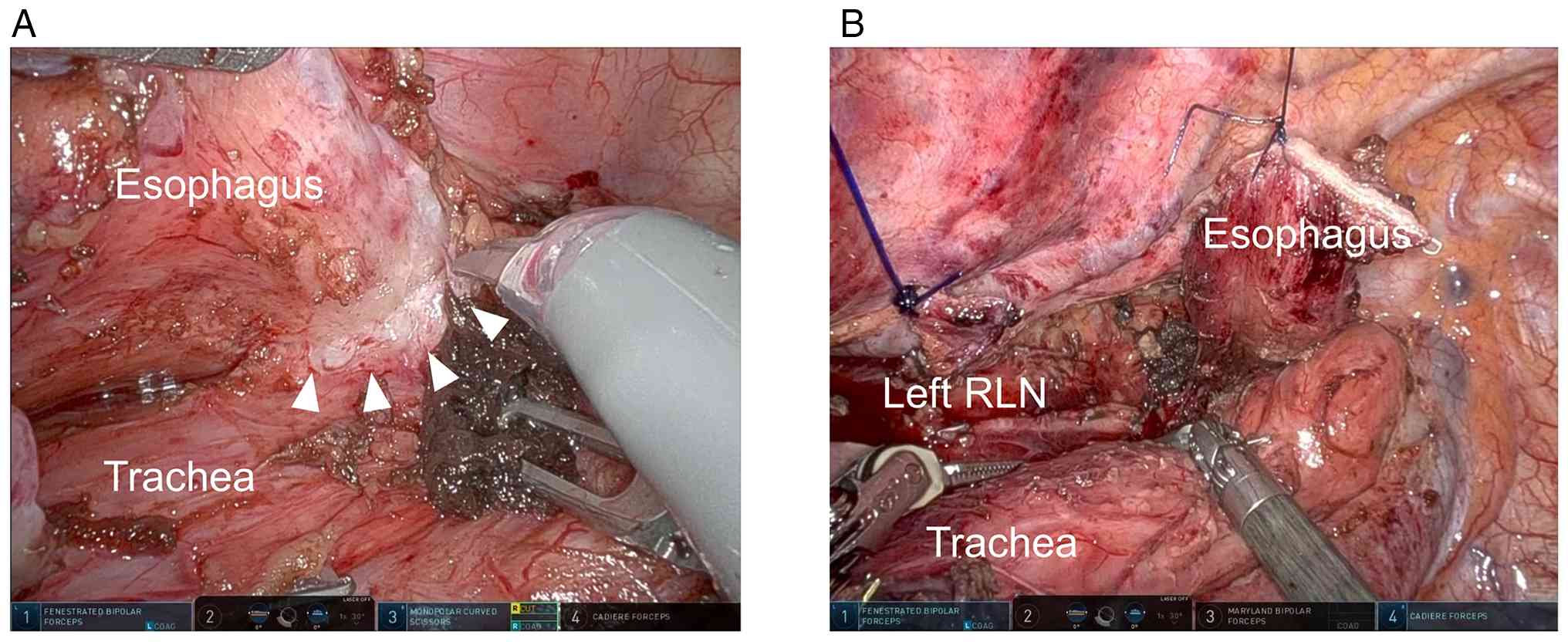
12-mm port in the 7th ICS on the anterior AL. Fibrotic changes
after CRT were observed in the primary esophageal tumor around the
paraesophageal lymph nodes and trachea (Fig. 3A). After completing dissection of
the fibrotic tissue, the thoracic procedure was concluded (Fig. 3B).
After completing the thoracic phase, the patient was
repositioned in a 5 head-up tilt. The abdominal and cervical phases
were performed simultaneously. During the abdominal phase, an upper
abdominal lymphadenectomy and gastric tube construction were
performed laparoscopically. The first port (12 mm) for the camera
was placed at the umbilicus. Four additional ports were placed: A
5-mm port in the right hypochondrium; a 5-mm port in the right
upper abdomen between the right hypochondrial port and the
umbilicus; a 5-mm port in the left hypochondrium; and a 12-mm port
in the left upper abdomen between the left hypochondrial port and
the umbilicus. For the cervical phase, a cervical lymph node
dissection was performed, and complete removal and resection of the
tumor were achieved. The gastric tube was pulled up through a
posterior mediastinal route.
Clinical outcomes
Extubation was performed on postoperative day (POD)
1. However, on POD 3, the patient developed pneumonia and
difficulty expectorating sputum; therefore, intravenous
ampicillin/sulbactam (UNASYN®) at a dose of 3 g three
times daily was initiated and continued for 7 days. Reintubation
was also required. Further examination by the otolaryngology team
did not reveal recurrent laryngeal nerve paralysis. Although
oxygenation stabilized, difficulty with sputum expectoration
persisted, and a tracheostomy was performed on POD 8. The pneumonia
improved by POD 12, and antibiotic administration was discontinued.
Mechanical ventilation was discontinued on POD 17. A tracheostomy
mask was used on POD 31, and a heat and moisture exchanger
(artificial nose) were introduced on POD 45. Subsequently,
rehabilitation focused primarily on swallowing training with
thickened oral intake, and the patient was discharged on POD 93.
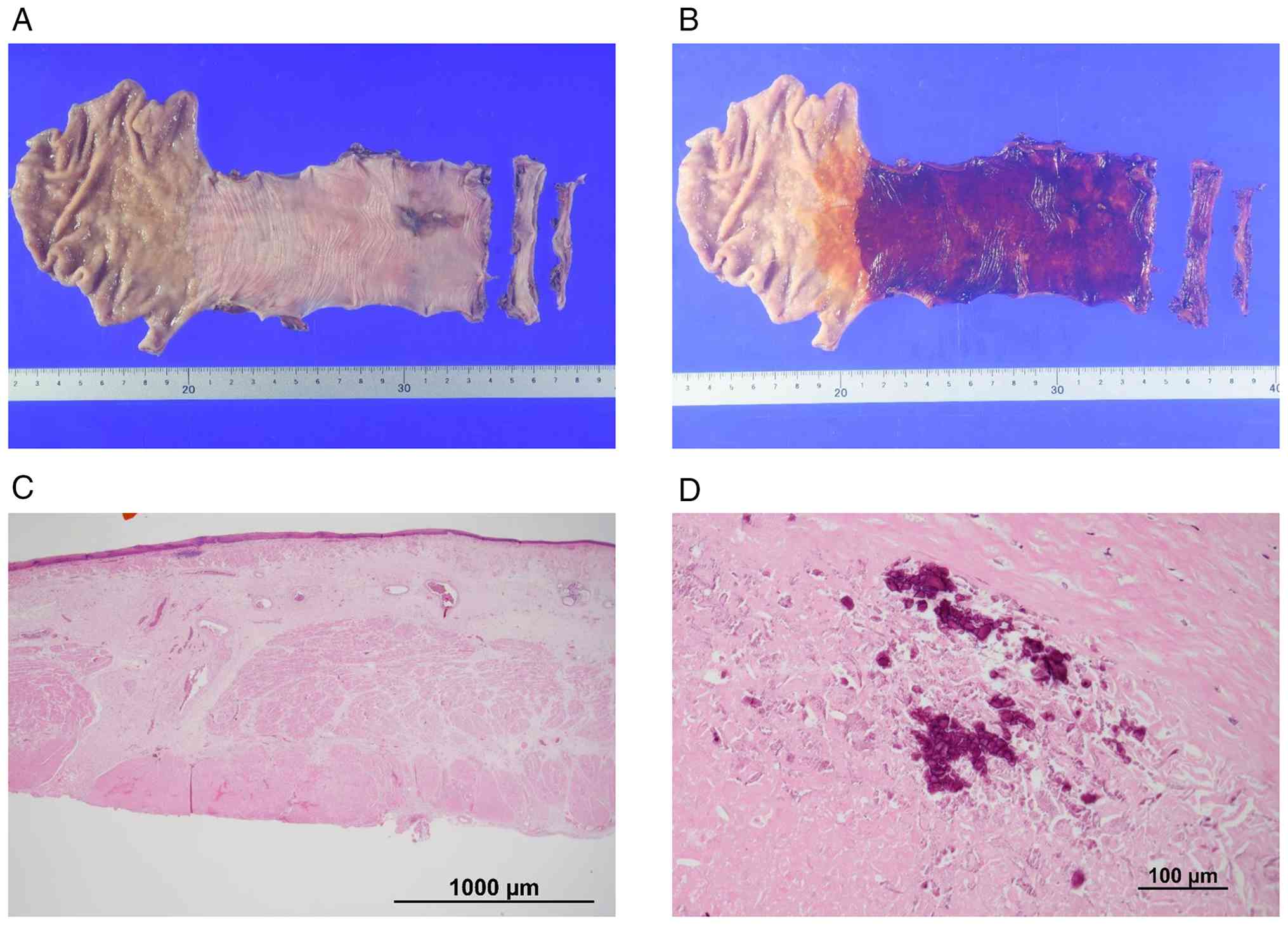
Pathological examination of the resected specimen revealed no
residual tumor, and the therapeutic effect of CRT was evaluated as
grade 3 (no variable cancer cells detected) based on Japanese
Classification of Esophageal Cancer, 12th edition (Fig. 4A-D) (7,10).
After considering the patient's overall condition, no adjuvant
postoperative therapy was administered. A total of 14 months have
passed since the initiation of treatment (10 months since surgery),
with no evidence of recurrence. The patient has been followed up
with tumor marker assessments every 3 months and CT every 6
months.
Discussion
To the best of our knowledge, the current report
presents the first description of a patient with esophageal sarcoma
who achieved a grade 3 pathological response following a subtotal
esophagectomy RAMIE after CRT (7,10).
Esophageal sarcoma represents a rare malignancy and
accounts for 0.5–2.8% of all esophageal cancer cases (1–3). This
condition occurs more frequently in men and typically arises in the
middle thoracic esophagus (1,2). The
macroscopic appearance is often polypoid, and dysphagia due to
impaired food passage has been reported as a common presenting
symptom (1,2). Esophageal sarcoma frequently coexists
with SCC, a presentation referred to as carcinosarcoma (1). When the sarcomatous component
predominates, a polypoid morphology is generally observed, whereas
carcinomatous dominance more commonly results in an ulcerative
lesion (11,12).
Carcinosarcoma is often not difficult to distinguish
clinically based on its macroscopic characteristics. However, it is
a biphasic tumor composed of both sarcomatous and carcinomatous
components. Therefore, depending on the biopsy site, the
pathological diagnosis may reflect only one component, potentially
reducing the accuracy of the preoperative diagnosis. Furthermore,
even when a biopsy specimen is obtained from the sarcomatous
portion of the tumor, the irregular morphology of the cells can
make differentiation between sarcoma and poorly differentiated
carcinoma challenging (13).
Although the origin of the sarcomatous component remains unclear,
the metaplastic theory, which proposes that the sarcomatous
component arises monoclonally from a single ancestral cell, is
widely accepted (14,15). Specifically, the sarcomatous
component may arise from metaplastic changes during the
epithelial-mesenchymal transition of the carcinomatous component.
This concept is supported by observations of transition zones
between the two components and shared gene mutations, including
TP53 mutations and p53 upregulation, in both components (16,17).
Management of esophageal sarcoma generally follows
the therapeutic principles applied to esophageal SCC, as frequent
coexistence with SCC and a high likelihood of lymph node metastasis
have been described (4).
Specifically, in resectable cases, surgical resection or surgical
resection following neoadjuvant chemotherapy is commonly performed.
RT or CRT remains an alternative for patients with unresectable
tumors or for those unable to tolerate surgery. In Japan,
concurrent CRT consisting of 5-fluorouracil and cisplatin with RT
has been widely adopted as a standard treatment for unresectable
locally advanced esophageal cancer, as demonstrated in the Japan
Clinical Oncology Group 9516 study (18). Based on these criteria, CRT was
selected for the present patient due to unresectability at
diagnosis and potential airway obstruction. Following treatment,
the tumor demonstrated a marked reduction in size and was
subsequently deemed resectable.
Table I summarizes
the results of CRT for carcinosarcoma (4,5,12,19–22).
Among the seven cases diagnosed with carcinosarcoma before
treatment, only two cases were diagnosed as SCC alone in the
pathological examination after surgical resection following CRT,
with no sarcomatous component detected. Both cases exhibited a PR,
suggesting that CRT was effective against the sarcomatous component
in 28.6% (2/7) of cases (19,20).
In the remaining five cases, the pathological diagnosis remained
carcinosarcoma both before and after CRT, with three cases showing
PR (60%, 3/5) and two cases (40%, 2/5) being indeterminate
(12,20,21).
Furthermore, among the two cases diagnosed as SCC before treatment,
postoperative pathological examination after CRT revealed
carcinosarcoma in one case and sarcoma alone in the other (5,19,22).
These findings suggest that preoperative endoscopic biopsies may
have sampled only the SCC component, indicating that an accurate
diagnosis of carcinosarcoma may be difficult depending on the site
of the preoperative endoscopic biopsy. Furthermore, considering
sensitivity to CRT, the SCC component appears to be more responsive
than the sarcomatous component, which may explain why only the
sarcomatous component remained after CRT in some cases (19,21,22).
Regarding RT alone for carcinosarcoma, there are reports of a PR in
patients with unresectable carcinosarcoma who received RT alone,
although differences in radiosensitivity between the sarcomatous
and carcinomatous components remain unclear (19,23,24).
While long-term prognosis remains uncertain, temporary local
control may be achieved with RT. Chemotherapy alone for
carcinosarcoma appears to demonstrate greater efficacy against the
carcinomatous component than against the sarcomatous component,
whereas the therapeutic effect on the sarcomatous component appears
limited (19,21,22).
 | Table I.Cases of esophageal carcinosarcoma
treated with preoperative chemoradiotherapy followed by
esophagectomy. |
Table I.
Cases of esophageal carcinosarcoma
treated with preoperative chemoradiotherapy followed by
esophagectomy.
| First author,
year | Age, years | Sex | Biopsy pathological
diagnosis | Location | TNM before
treatment | Chemotherapy | Radiation, Gy | Clinical
response | TNM after
surgery | Histological
responsea | Pathological
diagnosis | OS time,
months | Dead/alive | (Refs.) |
|---|
| Okuda et al,
2005 | 57 | M | SCC | Mt | T3N2M1 | FP | 30 | SD | T4N2M1 | N/A | Carcinosarcoma | 4 | Dead | (5) |
| Zuiki et al,
2009 | 50 | M | Carcinosarcoma | UtCe | T3N1M0 | FP | 40 | PR | T1bN2M0 | N/A | SCC | 35 | Alive | (19) |
|
| 66 | M | SCC | Lt | N/A | FP | 40.8 | PR | T1bN0M0 | N/A | Sarcoma | 19 | Alive |
|
| Kuo (4) et al, 2010 | 68 | M | Carcinosarcoma | Ut | T3N1M0 | N/A | N/A | N/A | N/A | N/A | N/A | 27 | Alive | (4) |
|
| 45 | M | Carcinosarcoma | Lt | T4N1M0 | N/A | N/A | N/A | N/A | N/A | N/A | 6 | Alive |
|
| Kobayashi et
al, 2010 | 68 | M | Carcinosarcoma | CeUt | T3N1M0 | S1 + CDDP | 40 | PR | TisN0M0 | Grade 2 | SCC | 60 | Alive | (20) |
|
| 64 | M | Carcinosarcoma | Ce | T2N1M0 | FP | 38 | PR | T1aN0M0 | Grade 2 | Carcinosarcoma | 7 | Dead |
|
| Katsuya et
al, 2017 | 67 | F | Carcinosarcoma | Mt | T1bN1M0 | FP | 50.4 | PR | T1bN0M0 | Grade 1 | Carcinosarcoma | 10.9 | Dead | (21) |
|
| 73 | F | Carcinosarcoma | Lt | T2N1M0 | FP | 41.4 | PR | T1bN0M0 | Grade 2 | Carcinosarcoma | 47 | Alive |
|
| Yamauchi et
al, 2022 | 65 | M | SCC | N/A | T3N1M0 | FP | 60 | N/A | T2N0M1 | N/A | Carcinosarcoma | 12 | Dead | (22) |
| Yang et al,
2022 | 70 | M | Carcinosarcoma | N/A | T3N1M0 | S1 | 44.94 | PR | T2N0M0 | Grade 1 | Carcinosarcoma | 37.4 | Alive | (12) |
|
| 62 | M | Carcinosarcoma | N/A | T1N1M0 | EP | 47.08 | PR | T3N0M0 | N/A | Carcinosarcoma | 22.7 | Alive |
|
| Present case | 81 | M | Sarcoma | MtLt | T4N1M0 | FP | 50.4 | PR | T0N0M0 | Grade 3 | Sarcoma | 14 | Alive |
|
Regarding surgery, surgical procedures following the
pattern of esophageal SCC, such as transthoracic subtotal
esophagectomy with lymph node dissection, are frequently performed
(3). Recent years have shown
widespread adoption of a minimally invasive esophagectomy, with
thoracoscopic esophageal procedures being actively utilized.
Moreover, the use of RAMIE has expanded rapidly in clinical
practice (25,26). In the present case, RAMIE was
performed as salvage treatment for a patient with esophageal
sarcoma. Robotic surgery provides multiple advantages for
esophagectomy compared with thoracoscopic or open approaches
(25–27). RAMIE enables highly precise surgical
procedures through three-dimensional magnified visualization,
tremor elimination and multiple articulations of the endo-wrist.
This technique appears particularly beneficial for post-CRT
patients with esophageal sarcoma undergoing salvage surgery, where
these technical advantages can be fully utilized.
In the present case, the pre-treatment diagnosis
was, strictly speaking, sarcoma. As the resected specimen showed no
residual tumor, a definitive conclusion could not be drawn.
Therefore, this remains a limitation of the present report.
However, considering the reported frequency of esophageal sarcoma,
we infer that the pre-treatment biopsy likely sampled the
sarcomatous component of a carcinosarcoma (3). Several reports have reported the use
of CRT for patients with esophageal carcinosarcoma (Table I) (4,5,12,19–22).
The compiled cases highlight several important observations
regarding esophageal sarcoma and carcinosarcoma treated with
esophagectomy following CRT. First, a clear discrepancy has emerged
between pre-treatment biopsy diagnosis and the final pathological
diagnosis. In multiple cases, biopsies suggested SCC or
carcinosarcoma, although post-surgical histopathology revealed
either sarcomatous or carcinomatous components alone. This finding
emphasizes the diagnostic challenge in accurately identifying
esophageal sarcoma preoperatively, likely due to tumor
heterogeneity and the limited sampling inherent to endoscopic
biopsy. Second, the clinical response to CRT was generally
favorable in most cases, with a PR observed even in tumors
initially classified as T3 or T4. This suggests that esophageal
sarcoma, traditionally considered less responsive to CRT, may
exhibit substantial sensitivity under certain conditions,
supporting the potential role of CRT as a neoadjuvant strategy.
Notably, in the current case, the patient achieved grade 3 tumor
regression after CRT, which represents the highest response
observed in this series (7,10). The present case demonstrates that
curative outcomes can be achieved with CRT even when the tumor is
deemed unresectable at initial diagnosis, suggesting that CRT alone
may represent a highly effective treatment option. Finally, these
findings collectively highlight the need for treatment strategies
aligned with esophageal SCC protocols when sarcoma is suspected or
diagnosed via limited biopsy, due to both diagnostic uncertainty
and the potential for a notable response to CRT. In other words,
even if a patient presents with a carcinosarcoma or sarcoma, they
may be candidates for multimodality treatment.
In conclusion, the present study reports a case in
which CRT was performed followed by robotic-assisted subtotal
esophagectomy for unresectable esophageal sarcoma with infiltration
into other organs. The patient achieved a pathological complete
response after multimodality treatment and remains disease-free at
14 months after treatment initiation (10 months after surgery).
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
All authors contributed to the preparation and
revision of this manuscript. MY, AT, and MH participated in the
surgery. MY, AT, and MH managed the patient. MY, AT, MH, ST, YM,
RT, KK, YT, KS, NH, TK, and KT designed the study and advised on
patient treatment or analyzed patient data. MY wrote the
manuscript. KM and YH performed the pathological diagnosis. All
authors have read and approved the final manuscript. AT and MH
confirm the authenticity of all the raw data.
Ethics approval and consent to
participate
This case report was conducted under a protocol
approved by the Institutional Ethics Committee of National Hospital
Organization Osaka National Hospital (Osaka, Japan) (approval no.
21106), according to institutional policy. The study was conducted
in accordance with the principles of the Declaration of Helsinki
(revised in 2013).
Patient consent for publication
Written informed consent for publication was
obtained from the patient.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
EGD
|
esophagogastroduodenoscopy
|
|
CT
|
computed tomography
|
|
SCC
|
squamous cell carcinoma
|
|
CRT
|
chemoradiotherapy
|
|
dCRT
|
definitive chemoradiotherapy
|
|
FP
|
5-fluorouracil + cisplatin
|
|
RAMIE
|
robot-assisted minimally invasive
esophagectomy
|
|
ICS
|
intercostal space
|
|
AL
|
axillary line
|
|
POD
|
postoperative day
|
References
|
1
|
Hatch GF III, Wertheimer-Hatch L, Hatch
KF, Davis GB, Blanchard DK, Foster RS Jr and Skandalakis JE: Tumors
of the esophagus. World J Surg. 24:401–411. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Iyomasa S, Kato H, Tachimori Y, Watanabe
H, Yamaguchi H and Itabashi M: Carcinosarcoma of the esophagus: A
twenty-case study. Jpn J Clin Oncol. 20:99–106. 1990.PubMed/NCBI
|
|
3
|
Mege D, Depypere L, Piessen G, Slaman AE,
Wijnhoven BPL, Hölscher A, Nilsson M, van Berge Henegouwen MI, van
Lanschot JJB, Schroeder W, et al: Surgical management of esophageal
sarcoma: A multicenter European experience. Dis Esophagus. Feb
9–2018.(Epub ahead of print). View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kuo CJ, Lin TN, Lin CJ, Wu RC, Chang HK,
Chu YY, Lien JM, Su MY and Chiu CT: Clinical manifestation of
esophageal carcinosarcoma: A Taiwan experience. Dis Esophagus.
23:122–127. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Okuda K, Sano M, Narita H, Shibata T, Kato
K and Usami S: A Case of Double Esophageal Carcinoma Along with
So-called Carcinosarcoma and Squamous Cell Carcinoma. Jpn J
Gastroenterol Surg. 38:1296–300. 2005.(In Japanese). View Article : Google Scholar
|
|
6
|
Brierley JD, Gospodarowicz MK and
Wittekind C: TNM classification of malignant tumors. International
Union Against Cancer. 8th edition. Wiley; Oxford: 2017
|
|
7
|
Doki Y, Tanaka K, Kawachi H, Shirakawa Y,
Kitagawa Y, Toh Y, Yasuda T, Watanabe M, Kamei T, Oyama T, et al:
Japanese classification of esophageal cancer, 12th edition: Part
II. Esophagus. 12:216–269. 2024. View Article : Google Scholar
|
|
8
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Common Terminology Criteria for Adverse
Events (CTCAE), . Version 5.0. Available from. https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docsNovember
29–2024
|
|
10
|
Mine S, Tanaka K, Kawachi H, Shirakawa Y,
Kitagawa Y, Toh Y, Yasuda T, Watanabe M, Kamei T, Oyama T, et al:
Japanese classification of esophageal cancer, 12th edition: Part I.
Esophagus. 12:179–215. 2024. View Article : Google Scholar
|
|
11
|
Chino O, Kijima H, Shimada H, Nishi T,
Tanaka H, Oshiba G, Kise Y, Kenmochi T, Himeno H, Tsuchida T, et
al: Clinicopathological studies of esophageal carcinosarcoma:
analyses of its morphological characteristics using endoscopic,
histological, and immunohistochemical procedures. Endoscopy.
32:706–711. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yang S, Wang W, Bi N, Zhou Z, Feng Q, Xiao
Z, Chen D, Liang J, Lu J, Wang J, et al: Intensity modulated
radiotherapy might be effective for locally advanced esophageal
carcinosarcoma: A single center's experience and review of
literature. Medicine (Baltimore). 101:e312152022. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ohkura Y: Clinicopathological features of
esophageal ‘carcinosarcoma’: histopathological problems of
subclassification. Pathol Clin Med. 20:489–495. 2002.(In
Japanese).
|
|
14
|
Sung CO, Park CK and Kim SH:
Classification of epithelial-mesenchymal transition phenotypes in
esophageal squamous cell carcinoma is strongly associated with
patient prognosis. Mod Pathol. 24:1060–1068. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sung CO, Choi H, Lee KW and Kim SH:
Sarcomatoid carcinoma represents a complete phenotype with various
pathways of epithelial mesenchymal transition. J Clin Pathol.
66:601–606. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cha RR, Jung WT, Oh HW, Kim HJ, Ha CY, Kim
HJ, Kim TH and Ko GH: A case of metachronous development of
esophageal squamous cell carcinoma in the patient with esophageal
carcinosarcoma. Korean J Gastroenterol. 64:364–369. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ishida H, Fujishima F, Onodera Y,
Konno-Kumagai T, Maruyama S, Okamoto H, Sato C, Heishi T, Sakurai
T, Taniyama Y, et al: Esophageal carcinosarcoma with basaloid
squamous cell carcinoma: A case report and review of the
literature. Tohoku J Exp Med. 249:255–263. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ishida K, Ando N, Yamamoto S, Ide H and
Shinoda M: Phase II study of cisplatin and 5-fluorouracil with
concurrent radiotherapy in advanced squamous cell carcinoma of the
esophagus: A Japan Esophageal Oncology Group (JEOG)/Japan Clinical
Oncology Group trial (JCOG9516). Jpn J Clin Oncol. 34:615–619.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Zuiki T, Hosoya Y, Ui T, Haruta H,
Kurashina K, Saito S, Lefor A, Niki T, Nakazawa M and Yasuda Y:
Therapeutic effectiveness of chemoradiotherapy for carcinosarcoma
of the esophagus: Two case reports and a review of the literature.
Esophagus. 6:189–195. 2009. View Article : Google Scholar
|
|
20
|
Kobayashi D, Koike M, Kodera Y, Fujiwara
M, Nakayama G and Nakao A: Carcinosarcoma of the esophagus treated
with chemoradiotherapy: Report of four cases. Esophagus. 7:119–125.
2010. View Article : Google Scholar
|
|
21
|
Katsuya Y, Honma Y, Taniguchi H, Kato K,
Okita N, Takashima A, Iwasa S, Hamaguchi T, Boku N, Umezawa R, et
al: Clinicopathological features and pathological evaluation of
preoperative treatment of patients with resectable esophageal
carcinosarcoma. Esophagus. 14:317–323. 2017. View Article : Google Scholar
|
|
22
|
Yamauchi T, Taniyama Y, Fujishima F,
Sasano H, Unno M and Kamei T: Rapidly growing carcinosarcoma of the
esophagus following definitive chemoradiotherapy: A case report and
the literature review. Int J Surg Case Rep. 94:1071162022.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Katsuragi M, Nobe T, Okumura Y, Kuwasaki
S, Noge S, Hata K, Furusawa M and Hayashi I: Two cases of so-called
carcinosarcoma of the esophagus. Rinsho Hoshasen. 32:735–378.
1987.(In Japanese). PubMed/NCBI
|
|
24
|
Hanada N, Tanaka M, Nishitani D, Hasegawa
H, Shinagawa H, Kawatsu S and Fukuda S: A case of esophageal
carcinosarcoma successfully treated by radiotherapy. J Aomori
Rosai. 17:20–23. 2007.(In Japanese).
|
|
25
|
van der Sluis PC, van der Horst S, May AM,
Schippers C, Brosens LAA, Joore HCA, Kroese CC, Haj Mohammad N,
Mook S, Vleggaar FP, et al: Robot-assisted minimally invasive
thoracolaparoscopic esophagectomy versus open transthoracic
esophagectomy for resectable esophageal cancer: A randomized
controlled trial. Ann Surg. 269:621–630. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Yun JK, Lee IS, Gong CS, Kim BS, Kim HR,
Kim DK, Park SI and Kim YH: Clinical utility of robot-assisted
transthoracic esophagectomy in advanced esophageal cancer after
neoadjuvant chemoradiation therapy. J Thorac Dis. 11:2913–2923.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Espinoza-Mercado F, Imai TA, Borgella JD,
Sarkissian A, Serna-Gallegos D, Alban RF and Soukiasian HJ: Does
the approach matter? Comparing survival in robotic, minimally
invasive, and open esophagectomies. Ann Thorac Surg. 107:378–385.
2019. View Article : Google Scholar : PubMed/NCBI
|