Introduction
Gastric cancer (GC) remains the fifth most common
cancer diagnosis and a leading cause of cancer-related mortality
worldwide (1). Despite advances in
multimodal therapeutic approaches, overall prognosis remains poor
(2). For patients with locally
advanced disease, neoadjuvant chemotherapy (NAC) followed by
radical surgery constitutes a cornerstone of curative management,
with treatment response typically evaluated post-operatively
through conventional imaging and histopathological assessment
(3). Although standard clinical
evaluation serves as an important surrogate of therapeutic efficacy
and is associated with improved survival (4), clinical outcomes remain highly
variable (5,6). Some patients with residual disease
experience prolonged recurrence-free survival (5), whereas relapse may still occur in a
subset of patients showing favorable pathological response
(7). Together, these observations
emphasize the complexity of therapeutic effectiveness and
limitations of traditional evaluation methods in providing a
complete picture, highlighting the need for additional approaches
that can better reflect treatment-associated alterations, thereby
enabling improved post-operative risk stratification in GC.
MiRNAs are small non-coding RNAs of approximately
19–24 nucleotides that regulate gene expression at
post-transcriptional level (8).
These epigenetic regulators modulate multiple cancer-related
processes including proliferation, invasion, metastasis, and
treatment response, functioning either as oncogenic genes or tumor
suppressors (9). Importantly,
miRNAs are detectable in stable cell-free forms in circulation,
making them attractive candidates for non-invasive liquid biopsy
approaches (10). Among candidate
miRNAs, miRNA-30a has been consistently implicated as a
tumor-suppressive regulator across malignancies, with reduced
expression linked to aggressive tumor behavior and treatment
resistance (11,12). However, data regarding its role in
GC, particularly in the neoadjuvant setting, remain limited.
Therefore, the aim of this study was to evaluate the
association between circulating miRNA-30a levels and therapeutic
effect in patients with GC treated with NAC, and to investigate
whether miRNA-30a expression may further help stratify patients
according to treatment-related patterns and clinical outcome.
Materials and methods
Patients and sample collection
A cohort of 67 patients with histologically
confirmed GC was enrolled in the study between March 2022 and
September 2023. Clinical data, including age and sex, were
retrieved from hospital records. The median age of the patients was
67.0 years (IQR, 57.0–73.5 years), with a male-to-female ratio of
6:1. In 42 patients, blood samples were obtained following
completion of NAC and prior to surgical resection. In the remaining
25 patients, samples were collected prior to surgery in the absence
of NAC; these patients served as a treatment-naive (CT-naive)
control group. The study was conducted in accordance with the
Declaration of Helsinki and its subsequent amendments, and was
approved by the Research and Ethics Committee of Aretaieio
Hospital, National and Kapodistrian University of Athens (approval
no. 415/21-02-2022). Written informed consent was obtained from all
participants.
Pre-operative chemotherapy and
clinicopathological characteristics
Neoadjuvant chemotherapy with the FLOT regimen
(5-fluorouracil, oxaliplatin, leucovorin, and docetaxel) was
administered as the predominant treatment approach. Patients
received four cycles of FLOT every two weeks prior to surgery,
followed by gastrectomy within 4–6 weeks after completion.
Pathological evaluation was performed by experienced pathologists.
Tumors were staged according to the American Joint Committee on
Cancer (AJCC) Staging Manual, 8th edition, with yTNM classification
(13), and histological subtype was
determined according to the Lauren classification.
Histopathological tumor regression grade (TRG) of the primary tumor
after therapy was assessed according to Mandards' system.
Patients were categorized into Responders (defined
as TRG 0–2) and Non-responders (defined as TRG 3–5). Pathological
tumor depth was categorized as Tx, T1-T2, or T3-T4, with Tx
indicating absence of residual primary tumor. Nodal burden was
categorized into low (N0) and high (N1-N3). All grouping strategies
were selected to allow meaningful comparisons within the context of
the limited cohort size. Patient and disease characteristics, along
with associations between categorical variables, are summarized in
Table I.
 | Table I.Baseline clinicopathological
characteristics. |
Table I.
Baseline clinicopathological
characteristics.
| Variable | Responders TRG 0–2
(n=14) | Non-responders TRG
3–5 (n=28) | P-value |
|---|
| Sex, n (%) |
|
|
|
|
Male | 14 (100.0) | 22 (78.6) | 0.083a |
|
Female | 0 (0.0) | 6 (21.4) |
|
| Tumor location, n
(%) |
|
|
|
|
Stomach | 5 (35.7) | 12 (42.9) | 0.747a |
|
Gastroesophageal junction | 9 (64.3) | 16 (57.1) |
|
| Lauren
classification, n (%) |
|
|
|
|
Intestinal | 2 (14.3) | 10 (35.7) |
<0.001a |
|
Diffuse | 2 (14.3) | 13 (46.4) |
|
|
Mixed | 3 (21.4) | 5 (17.9) |
|
|
Other | 7 (50.0) | 0 (0.0) |
|
| Tumor
differentiation, n (%) |
|
|
|
|
Poor | 3 (21.4) | 20 (71.4) |
<0.001a |
|
Moderate | 4 (28.6) | 7 (25.0) |
|
|
Well | 0 (0.0) | 1 (3.6) |
|
| No
residual tumor | 7 (50.0) | 0 (0.0) |
|
| T stage, n (%) |
|
|
|
| Tx | 7 (50.0) | 1 (3.6) |
<0.001a |
|
T1–T2 | 6 (42.9) | 7 (25.0) |
|
|
T3–T4 | 1 (7.1) | 20 (71.4) |
|
| N stage, n (%) |
|
|
|
| N0 | 10 (71.4%) | 9 (32.1%) | 0.023a |
|
N1-N3 | 4 (28.6%) | 19 (67.9%) |
|
| Age, years |
|
|
|
| Median
(IQR) | 67 (58–74) | 66 (57–73) | 0.811b |
Blood sample preparation and
Quantitative reverse transcription-polymerase chain reaction
(RT-qPCR)
Peripheral venous blood samples were collected using
vacutainer tubes and processed immediately after collection to
minimize the risk of hemolysis. Samples were centrifuged at 1,300 ×
g for 15 min, and then serum was aliquoted and stored at −80°C
until further analysis.
Total RNA extraction from 100 µl of serum samples
was carried out with magnetic bead technology using the
MagMAX™ mirVana™ Total RNA Isolation Kit
(cat. # A27828; Thermo Fisher Scientific, USA) following the
manufacturer's protocol. Synthetic cel-miR-39 was spiked at 10fmol
concentration prior to extraction in each serum sample and served
as an internal spike-in control. Total RNA was eluted in 50 µl
RNase-free water.
Reverse transcription (RT) reaction was prepared
according to the instructions of the TaqMan™ Advanced
miRNA cDNA Synthesis Kit (cat. # A28007; Thermo Fisher Scientific,
USA). Quantitative reverse-transcription polymerase chain reaction
(RT-qPCR) was performed using the TaqMan™ Fast Advanced
Master Mix (cat. # 4444557; Thermo Fisher Scientific, USA) followed
by amplification with TaqMan™ Advanced microRNA assays
(cat. # A25576; Thermo Fisher Scientific, USA) specific for
miRNA-30a and cel-miR-39 (Table
SI) on the StepOnePlus™ Real-Time qPCR System
(Applied Biosystems, USA). The qRT-PCR reaction was performed as
follows: 95°C for 20 sec, then 40 cycles of 95°C for 1 sec, and
60°C for 20 sec.
Each assay was performed with two identical
replicates, and a no-template control was included to assess the
possibility of reaction contamination. Inter-assay variability was
also assessed across independent runs to confirm consistency and
reproducibility. Relative miRNA expression levels of interest were
calculated using the 2−ΔΔCq method (14).
Statistical analysis
Statistical analysis was performed using SPSS
software (version 28.0; SPSS, Chicago, IL, USA) and GraphPad Prism
(version 9.5.1; GraphPad Software, San Diego, CA, USA) was employed
for visualization and generation of all graphical representations.
Numerical variables were expressed as median and range as
appropriate. Categorical variables were expressed as absolute
frequencies and percentages.
Kolmogorov-Smirnov test was used to analyze the
distribution of miRNA expression levels. Differences in miRNA
expression between groups were evaluated using Mann-Whitney U test
for two-group comparisons and Kruskal-Wallis test for comparisons
involving more than two groups, followed by Dunn's post hoc test
for multiple comparisons with Bonferroni correction. Associations
between categorical variables were assessed with Fisher's exact
test and comparisons of continuous variables and miRNA expression
were assessed using Spearman's rank correlation coefficient. MiRNA
discrimination potential was analyzed by computing receiver
operating characteristic (ROC) curves and calculating areas under
the curves (AUC) with corresponding 95% confidence intervals (CI),
as well as the optimal specificity and sensitivity values. Overall
survival (OS) and disease-free survival (DFS) were analyzed using
the Kaplan-Meier method, and differences between groups were
assessed with log-rank (Mantel-Cox) test. Univariate Cox
proportional hazards regression analyses were additionally
performed to estimate hazard ratios (HRs) and 95% confidence
intervals for survival outcomes. Statistical significance was
assumed at P < 0.05 (two-sided) for all analyses.
Results
Patients
A total of 67 patients with GC were included in the
study, comprising NAC-treated patients (n=42, 62.7%) and patients
who did not receive therapy (CT-naive) (n=25, 37.3%), who served as
a treatment-naive reference group. Among NAC-treated patients,
treatment response was assessed based on histopathological tumor
regression grade (TRG), and patients were classified as Responders
(TRG 0–2; n=14, 33.3%) or Non-responders (TRG 3–5; n=28,
66.7%).
Pathological tumor depth was classified as Tx in 8
patients (19.0%), T1-T2 in 13 patients (31.0%), and T3-T4 in 21
patients (50.0%). Low nodal burden was observed in 19 patients
(45.2%), while high nodal burden was present in 23 patients
(54.8%). Median follow-up was 24 months after completion of
treatment.
Association of circulating miRNA-30a
expression with treatment outcome and disease status
Circulating miRNA-30a was assessed following
completion of NAC, reflecting post-treatment expression levels. No
difference was observed between NAC-treated patients and CT-naive
control group (Fig. S1).
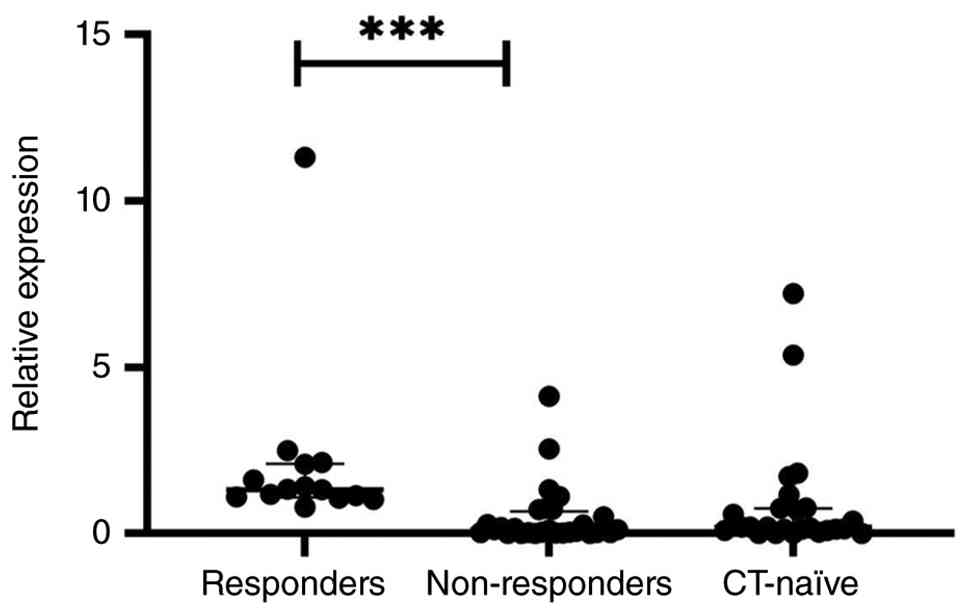
Stratification of NAC-treated patients according to treatment
outcome revealed significant differences in circulating miRNA-30a
levels (P<0.001), with Responders exhibiting higher levels
compared to Non-responders (P<0.001) (Fig. 1). Notably, circulating miRNA-30a
levels in patients without therapeutic effect were similar to those
observed in patients who did not receive therapy, whereas
Responders displayed comparatively higher expression levels,
supporting the differentiation between treatment-responsive and
non-responsive disease states.
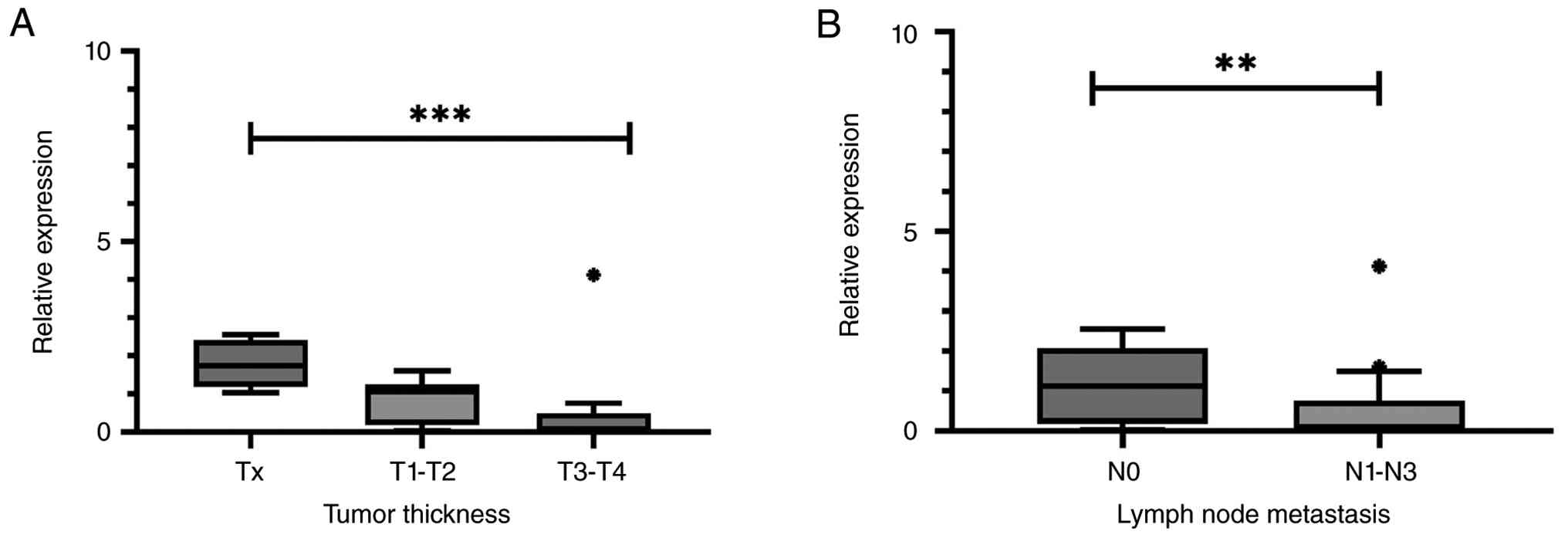
Consistent associations were observed with
pathological tumor burden, as higher miRNA-30a levels were detected
in patients with lower pathological T stage (Tx vs. T1-T2 vs.
T3-T4; P<0.001), showing a stepwise decrease across increasing
tumor stage categories (Fig. 2A),
and in patients without nodal involvement (N0 vs. N1-N3; P=0.004)
(Fig. 2B). No associations were
identified between miRNA-30a expression and other clinical and
pathological variables, including age, sex, tumor location, Lauren
classification, or differentiation status (Table SII).
Association of circulating miRNA-30a
with therapeutic outcome
In univariate logistic regression analysis, higher
miRNA-30a expression was associated with therapeutic outcome, with
increased miRNA-30a corresponding to a reduced probability of
non-response (OR=0.239, 95% CI: 0.084–0.685, P=0.008).
In multivariable models adjusting for T-stage and
N-stage, miRNA-30a remained associated with therapeutic outcome
(adjusted OR=0.174, 95% CI: 0.030–0.995, P=0.049 and OR=0.302, 95%
CI: 0.107–0.849, P=0.023, respectively), whereas pathological
parameters were not significant predictors. (Table SIII).
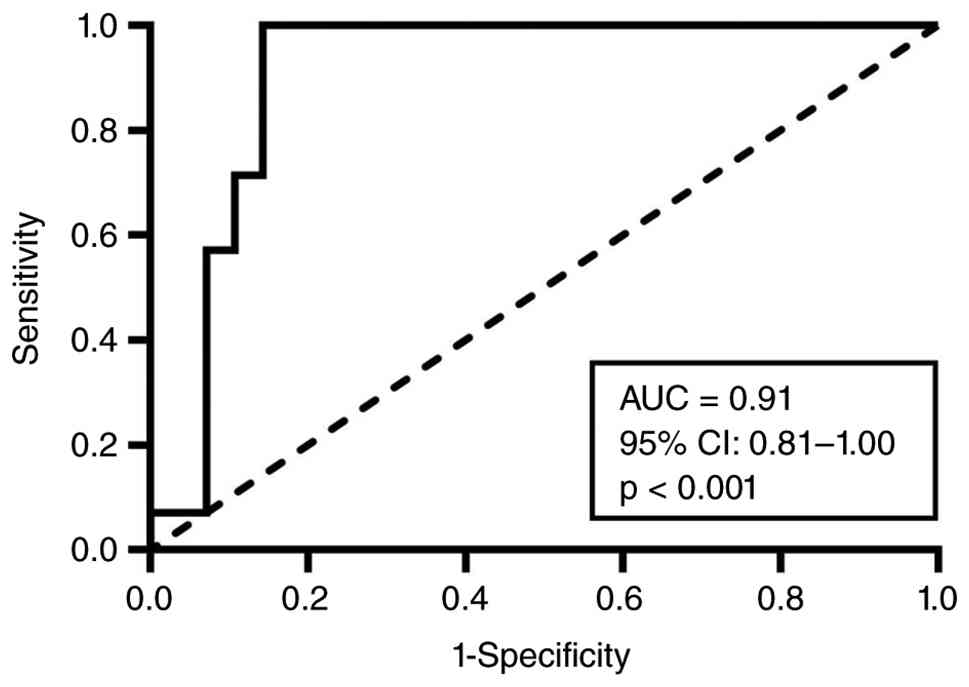
Discriminative performance of
circulating miRNA-30a for therapeutic outcome
ROC curve analysis demonstrated that circulating
miRNA-30a levels were able to distinguish Responders from
Non-responders. The area under the curve (AUC) was 0.91 (95% CI:
0.81–1.00, P<0.001), indicating good discriminatory performance.
The optimal cut-off value was calculated using the Youden index
(0.914) and was used to stratify patients into high and low
expression groups for exploratory survival analysis (Fig. 3).
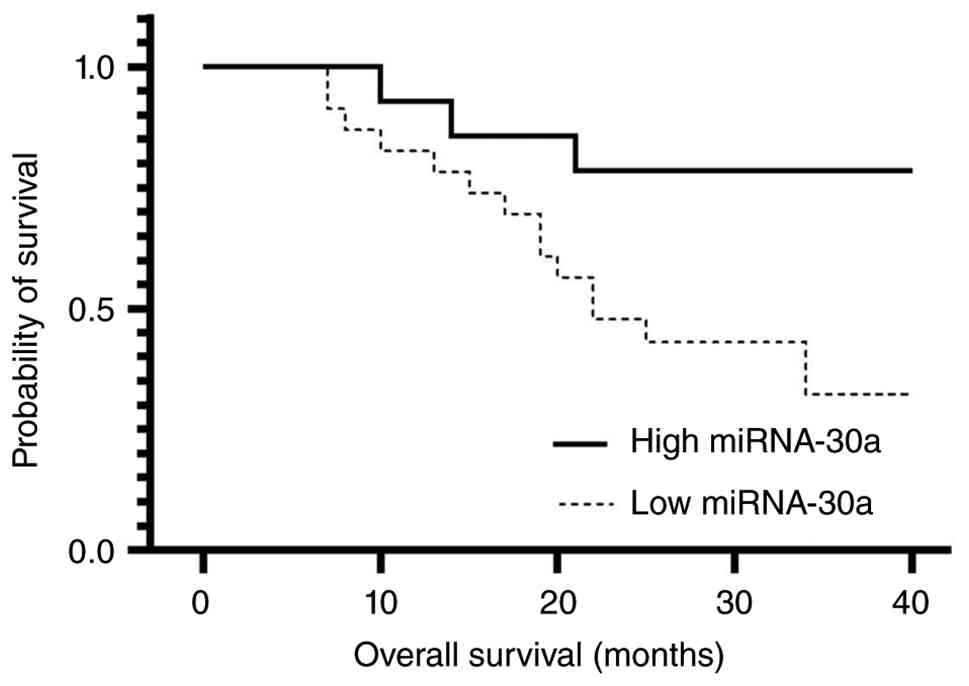
Association of circulating miRNA-30a
expression with overall and disease-free survival
Kaplan-Meier analysis using the ROC-derived cut-off
showed that patients with higher circulating miRNA-30a expression
had longer overall survival compared to those with lower expression
(P=0.033) (Fig. 4). No difference
in disease-free survival was observed between the two groups
(P=0.200) (Fig. S2). Cox
regression analysis revealed similar findings, with higher
miRNA-30a levels associated with a reduced risk of death (HR=0.283,
95% CI: 0.081–0.985, P=0.047).
Discussion
In the NAC setting, variability in therapeutic
outcome remains a major clinical challenge in GC, highlighting the
need for improved post-operative patient stratification. While
response to therapy provides important information, it may not
fully reflect disease behavior after treatment. Accordingly,
therapeutic effect is a multifactorial process that extends beyond
tumor-intrinsic characteristics, including systemic factors such as
circulating mediators and inflammatory and signaling pathways that
may influence both tumor progression and response to therapy
(15). Emerging evidence further
suggests that tumors actively interact with and modulate systemic
homeostasis through neuroendocrine and immune signaling networks,
thereby influencing host physiology in ways that may support tumor
adaptation and progression (16).
MiRNAs have been implicated in the regulation of
these processes and may contribute to the dynamic interplay between
tumor biology and systemic circulation. In this setting, expression
patterns of circulating miRNAs are closely linked to therapeutic
intervention. Patterns observed in untreated disease primarily
reflect intrinsic tumor biology, whereas profiles evaluated
following therapeutic exposure may provide insight into disease
characteristics that persist or emerge after treatment. Such
expression signatures may capture therapy-associated differences
that are not fully represented by imaging or pathological
assessment alone (17–19), thereby offering additional
information relevant to post-treatment stratification and patient
management. In this framework, differences in circulating miRNA-30a
expression between responders and non-responders observed in the
present study, indicate an association with therapeutic outcome
reflecting post-treatment, response-associated expression patterns
rather than predictive capacity.
Across malignancies, miRNA-30a is generally
described as a tumor-suppressive regulator, although its molecular
mechanisms are not yet fully understood. Studies indicate that
reduced miRNA-30a expression is associated with enhanced
proliferation (20–22), invasion (23–28),
and epithelial-mesenchymal transition (EMT) (29–31),
while restoration of expression suppresses oncogenic signaling
pathways and limits tumor progression. In GC, miRNA-30a has been
shown to inhibit proliferation and cell-cycle progression through
targets such as MAD2L1 (32) and
FAPα (33), supporting its role in
maintaining a less aggressive tumor phenotype.
Consistent with this background, our findings
indicate that higher circulating miRNA-30a levels are linked to
improved therapeutic outcome. Patients with increased miRNA-30a
were more likely to derive clinical benefit from treatment and
exhibited reduced disease burden, including lower pathological T
stage and absence of nodal involvement. In parallel, higher
miRNA-30a levels were also observed among patients with longer
overall survival following NAC, suggesting an improved outcome. A
notable difference in expression patterns was detected between
responders and non-responders, with patients who benefited from
therapy exhibiting a distinct profile, whereas those who did not,
showed expression levels comparable to CT-naive patients,
suggesting that, in the absence of therapeutic effect,
post-treatment expression patterns may resemble those observed in
untreated disease. These observations are consistent with previous
reports linking miRNA-30a downregulation to tumor progression and
metastatic potential (34), as well
as with studies in other malignancies where reduced miRNA-30a
expression has been associated with poorer pathological response
and less favorable outcomes, including triple-negative breast
cancer treated with neoadjuvant anthracycline- and taxane-based
regimens (35–37). Evidence also suggests that
restoration of miRNA-30a enhances sensitivity to platinum-based
agents through suppression of epithelial-mesenchymal transition
(EMT) and modulation of autophagy-related pathways, both implicated
in chemoresistance (38,39). In addition, preclinical studies
demonstrating reduced proliferation and invasive capacity following
miRNA-30a upregulation further support the association between
elevated levels and less aggressive disease features observed in
our cohort (25,34).
Recent epidemiological evidence indicates that
survival outcomes in GC have improved over time, particularly in
patients with earlier-stage disease, largely reflecting advances in
multimodal treatment approaches, including NAC. Population-based
data indicate marked stage-dependent differences in survival, with
reported 5-year relative survival rates of 77.7% for localized
disease, 37.4% for regional disease, and 10.2% for distant-stage
GC. Nevertheless, variability in clinical outcomes persists,
especially among patients with more advanced disease stages,
highlighting the significant variability in disease behavior even
within stage-defined groups (40–42).
In this context, circulating miRNA-30a, considered alongside
survival outcomes and treatment efficacy, may provide additional
insight into post-treatment disease behavior and support a more
comprehensive assessment beyond conventional methods. Rather than
directly reflecting population-level survival trends, it may
capture inter-individual differences in treatment-associated
disease dynamics that are not fully accounted for by standard
clinicopathological parameters.
An important limitation of this observational study
is that no causal or mechanistic conclusions can be drawn, and the
observed associations should be interpreted in the context of
complex tumor-host systemic interactions that require further
functional investigation (16). In
addition, the relatively small cohort size may restrict the
detection of more subtle expression differences, and some of the
observed findings may be influenced by the imbalance in subgroup
sizes. Therefore, the findings of multivariable and survival
analyses should be considered exploratory and interpreted with
caution, particularly given the limited number of events and
subgroup sizes. Larger prospective studies including all treatment
phases and extended follow-up are needed to clarify expression
changes of miRNA-30a and determine whether monitoring may improve
clinical evaluation and relapse prediction. The clinical relevance
of such approaches is underscored by ongoing efforts such as the
ENLIGHT trial (NCT07243015), which aims to develop and validate
miRNA-based liquid biopsy signatures for minimal residual disease
detection in GC (43).
Overall, several key findings with biological
relevance and clinical potential were identified. Circulating
miRNA-30a expression is linked to therapeutic outcome and appears
to reflect treatment benefit in patients with GC treated with NAC.
Its application alongside conventional assessment strategies may
contribute to improved post-treatment disease monitoring and
patient stratification, subject to further validation in larger
prospective studies.
Supplementary Material
Supporting Data
Supporting Data
Acknowledgements
Not applicable.
Funding
This work was supported by ERAPerMed-Joint Transnational Call
for Proposals (2019) for ‘Personalised Medicine: Multidisciplinary
Research Towards Implementation’ [grant no. ERAPerMed 2019-275
(GRAMMY)].
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
VKD and MMK were involved in the conception and
design of the study. VKD, AM and AT provided administrative
support, were responsible for sample and data collection, and
performed experiments. VKD, MMK and PTA were involved in the
provision of study materials and patient enrollment. VKD, AV and
PTA performed data analysis and interpretation. All authors
contributed to manuscript writing. All authors critically revised
the manuscript, commented on previous versions, and read and
approved the final manuscript. VKD, MMK and PTA confirm the
authenticity of all the raw data.
Ethics approval and consent to
participate
The study was approved by the Research and Ethics
Committee of Aretaieio Hospital, National and Kapodistrian
University of Athens (approval no. 415/21-02-2022). Written
informed consent was obtained from all participants prior to
inclusion in the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
GC
|
gastric cancer
|
|
NAC
|
neoadjuvant chemotherapy
|
|
RT-qPCR
|
reverse transcription-quantitative
polymerase chain reaction
|
|
CT-naive
|
chemotherapy-naive
|
References
|
1
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 71:209–249.
2021.PubMed/NCBI
|
|
2
|
Lü Y, Wu J, Yang T, Lian L, Yu H, Sun J
and Hu J: Global, regional, and national burdens of early onset
gastric cancer aged 15–49 years from 1990 to 2021 with projections
to 2035: A population-based study. BMC Cancer. 25:15332025.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hsu JT, Lin YN, Chen YF, Kou HW, Wang SY,
Chou WC, Wu TR and Yeh TS: A comprehensive overview of gastric
cancer management from a surgical point of view. Biomed J.
48:1008172025. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kang YK, Yook JH, Park YK, Lee JS, Kim YW,
Kim JY, Ryu MH, Rha SY, Chung IJ, Kim IH, et al: PRODIGY: A phase
III study of neoadjuvant docetaxel, oxaliplatin, and S-1 plus
surgery and adjuvant S-1 versus surgery and adjuvant S-1 for
resectable advanced gastric cancer. J Clin Oncol. 39:2903–2913.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zhong Q, Weng CM, Jiang MC, Sun YQ, Li BL,
Zhao W, Zhang HX, Zhang ZQ, Ma YB, Wu SC, et al: Patterns of
survival and recurrence in poor responders to neoadjuvant therapy
for gastric cancer: A real-world multicenter study. Ann Surg Oncol.
32:6794–6804. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Anderson E, LeVee A, Kim S, Atkins K, Guan
M, Placencio-Hickok V, Moshayedi N, Hendifar A, Osipov A, Gangi A,
et al: A comparison of clinicopathologic outcomes across
neoadjuvant and adjuvant treatment modalities in resectable gastric
cancer. JAMA Netw Open. 4:e21384322021. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Leijonmarck W, Mattsson F and Lagergren J:
Neoadjuvant chemotherapy in relation to long-term mortality in
individuals cured of gastric adenocarcinoma. Gastric Cancer.
28:96–101. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Jorge AL, Pereira ER, Oliveira CS,
Ferreira EDS, Menon ETN, Diniz SN and Pezuk JA: MicroRNAs:
Understanding their role in gene expression and cancer. Einstein
(Sao Paulo). 19:eRW59962021. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Behl T, Kumar C, Makkar R, Gupta A and
Sachdeva M: Intercalating the role of microRNAs in cancer: As enemy
or protector. Asian Pac J Cancer Prev. 21:593–598. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Turchinovich A, Samatov TR, Tonevitsky A
and Burwinkel B: Circulating miRNAs: Cell-cell communication
function? Front Genet. 4:1192013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Jiang LH, Zhang HD and Tang JH: MiR-30a: A
novel biomarker and potential therapeutic target for cancer. J
Oncol. 2018:51678292018. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yang X, Chen Y and Chen L: The versatile
role of microRNA-30a in human cancer. Cell Physiol Biochem.
41:1616–1632. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Amin MB, Edge SB, Greene FL, Byrd DR,
Brookland RK, Washington MK, Gershenwald JE, Compton CC, Hess KR,
Sullivan DC, et al: AJCC cancer staging manual. 8th edition.
Springer; New York: 2017
|
|
14
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(−Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chakraborty C, Sharma AR, Sharma G and Lee
SS: The interplay among miRNAs, major cytokines, and cancer-related
inflammation. Mol Ther Nucleic Acids. 20:606–620. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Slominski RM, Raman C, Chen JY and
Slominski A: How cancer hijacks the body's homeostasis through the
neuroendocrine system. Trends Neurosci. 46:263–275. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Passaro A, Al Bakir M, Hamilton EG, Diehn
M, André F, Roy-Chowdhuri S, Mountzios G, Wistuba II, Swanton C and
Peters S: Cancer biomarkers: Emerging trends and clinical
implications for personalized treatment. Cell. 187:1617–1635. 2024.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wang Z, Wang H, Zhou S, Mao J, Zhan Z and
Duan S: miRNA interplay: Mechanisms and therapeutic interventions
in cancer. MedComm Oncol. 3:e932024. View
Article : Google Scholar
|
|
19
|
Baskaran N, Ranjan J, Baskaran B and
Soundararajan S: MicroRNAs as cancer biomarkers: Unveiling
diagnostic and prognostic potential. J Med Inform. 1:25–34.
2025.
|
|
20
|
Chen X, Li J, Zhang S, Xu W, Shi D, Zhuo
M, Liang S, Lei W and Xie C: MicroRNA-30a regulates cell
proliferation, migration, invasion and apoptosis in human
nasopharyngeal carcinoma via targeted regulation of ZEB2. Mol Med
Rep. 20:1672–1682. 2019.PubMed/NCBI
|
|
21
|
Xie M, Qin H, Luo Q, Huang Q, He X, Yang
Z, Lan P and Lian L: MicroRNA-30a regulates cell proliferation and
tumor growth of colorectal cancer by targeting CD73. BMC Cancer.
17:3052017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zhu Q, Li H, Li Y and Jiang L:
MicroRNA-30a functions as tumor suppressor and inhibits the
proliferation and invasion of prostate cancer cells by
down-regulation of SIX1. Hum Cell. 30:290–299. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chen Q, Gao Y, Yu Q, Tang F, Zhao P, Luo
S, Lin JS and Mei H: miR-30a-3p inhibits the proliferation of liver
cancer cells by targeting DNMT3a through the PI3K/AKT signaling
pathway. Oncol Lett. 19:606–614. 2020.PubMed/NCBI
|
|
24
|
Cheng CC, Yang BL, Chen WC, Ho AS, Sie ZL,
Lin HC and Chang CC: STAT3 mediated miR-30a-5p inhibition enhances
proliferation and inhibits apoptosis in colorectal cancer cells.
Int J Mol Sci. 21:73152020. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Min J, Han TS, Sohn Y, Shimizu T, Choi B,
Bae SW, Hur K, Kong SH, Suh YS, Lee HJ, et al: microRNA-30a
arbitrates intestinal-type early gastric carcinogenesis by directly
targeting ITGA2. Gastric Cancer. 23:600–613. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Zhong M, Bian Z and Wu Z: miR-30a
suppresses cell migration and invasion through downregulation of
PIK3CD in colorectal carcinoma. Cell Physiol Biochem. 31:209–218.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Xiao B, Shi X and Bai J: miR-30a regulates
the proliferation and invasion of breast cancer cells by targeting
Snail. Oncol Lett. 17:406–413. 2018.PubMed/NCBI
|
|
28
|
Wang D, Ge Y and Zhao Y: MicroRNA-30a-3p
inhibits the progression of lung cancer via the PI3K/AKT by
targeting DNA methyltransferase 3a. Onco Targets Ther.
12:7015–7024. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kumarswamy R, Mudduluru G, Ceppi P,
Muppala S, Kozlowski M, Niklinski J, Papotti M and Allgayer H:
MicroRNA-30a inhibits epithelial-to-mesenchymal transition by
targeting Snai1 and is downregulated in non-small cell lung cancer.
Int J Cancer. 130:2044–2053. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Wang HY, Li YY, Fu S, Wang XP, Huang MY,
Zhang X, Shao Q, Deng L, Zeng MS, Zeng YX and Shao JY: MicroRNA-30a
promotes invasiveness and metastasis in vitro and in vivo through
epithelial-mesenchymal transition and results in poor survival of
nasopharyngeal carcinoma patients. Exp Biol Med (Maywood).
239:891–898. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Wei W, Yang Y, Cai J, Cui K, Li RX, Wang
H, Shang X and Wei D: MiR-30a-5p suppresses tumor metastasis of
human colorectal cancer by targeting ITGB3. Cell Physiol Biochem.
39:1165–1176. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Wang Y, Wang F, He J, Du J, Zhang H, Shi
H, Chen Y, Wei Y, Xue W, Yan J, et al: miR-30a-3p targets MAD2L1
and regulates proliferation of gastric cancer cells. Onco Targets
Ther. 12:11313–11324. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Yu T, Gong L, Li W, Zuo Q, Cai D, Mao H,
Wang L, Lin J and Xiao B: MiR-30a suppresses metastasis of gastric
adenocarcinoma via targeting FAPα. Cancer Biomark. 27:471–484.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Soliman SE, Elabd NS, El-Kousy SM and Awad
MF: Down regulation of miR-30a-5p and miR-182-5p in gastric cancer:
Clinical impact and survival analysis. Biochem Biophys Rep.
27:1010792021.PubMed/NCBI
|
|
35
|
Wang LL, Zhang XH, Zhang X and Chen JK:
MiR-30a increases cisplatin sensitivity of gastric cancer cells
through suppressing epithelial-to-mesenchymal transition (EMT). Eur
Rev Med Pharmacol Sci. 20:1733–1739. 2016.PubMed/NCBI
|
|
36
|
Wang X, Qiu H, Tang R, Song H, Pan H, Feng
Z and Chen L: miR-30a inhibits epithelial-mesenchymal transition
and metastasis in triple-negative breast cancer by targeting ROR1.
Oncol Rep. 39:2635–2643. 2018.PubMed/NCBI
|
|
37
|
Dharshini LCP and Mandal AKA:
Network-based insights into miR-30a-5p-mediated regulation and EGCG
targeting in triple-negative breast cancer. Front Bioinform.
5:17351062025. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Du X, Liu B, Luan X, Cui Q and Li L:
miR-30 decreases multidrug resistance in human gastric cancer cells
by modulating cell autophagy. Exp Ther Med. 15:599–605.
2018.PubMed/NCBI
|
|
39
|
Li C, Zou J, Zheng G and Chu J: MiR-30a
decreases multidrug resistance (MDR) of gastric cancer cells. Med
Sci Monit. 22:4509–4515. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Zhang H, Yang W, Tan X, He W, Zhao L, Liu
H and Li G: Long-term relative survival of patients with gastric
cancer from a large-scale cohort: A period-analysis. BMC Cancer.
24:14202024. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Li Y, Feng A, Zheng S, Chen C and Lyu J:
Recent estimates and predictions of 5-year survival in patients
with gastric cancer: A model-based period analysis. Cancer Control.
29:107327482210992272022. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Mamun TI, Younus S and Rahman MH: Gastric
cancer-Epidemiology, modifiable and non-modifiable risk factors,
challenges and opportunities: An updated review. Cancer Treat Res
Commun. 41:1008452024.PubMed/NCBI
|
|
43
|
Detection of minimal residual disease
using exosomal miRNA distant metastasis markers. TrialX New York:
2026
|