Introduction
Thymoma is the most common anterior mediastinal
tumor, but it is a rare malignancy overall, with an incidence of
approximately 0.13 cases per 100,000 individuals annually (1). Thymomas are often associated with a
variety of immune abnormalities, particularly autoimmune diseases
such as myasthenia gravis and pure red cell aplasia (PRCA). PRCA is
a rare hematological disorder characterized by significant
normocytic, normochromic anemia, reduced reticulocytes, and
selective marked reduction of erythroid precursors in the bone
marrow.
Cases of thymoma complicated by PRCA are typically
treated by tumor resection plus immunosuppressive therapies such as
cyclosporine, steroids and cyclophosphamide (2,3).
However, the effectiveness of these treatments varies greatly among
individuals, and no standardized treatment guidelines have been
established. Meanwhile, systemic chemotherapy becomes the mainstay
of treatment in cases of metastatic or inoperable advanced thymoma
wherein surgical resection is not an option. In such situations,
using immunosuppressive therapy requires great caution due to the
risk of additive toxicity when combined with cytotoxic agents and
the potential for serious infectious complications. In cases where
immunosuppressive agents cannot be administered, long-term
transfusion support is often required for the management of
PRCA-associated anemia.
This case report describes a patient with metastatic
thymoma complicated by PRCA. The initial treatment was cytotoxic
chemotherapy with the ADOC regimen, which achieved tumor control
and prolonged transfusion intervals. This therapeutic response
enabled the subsequent initiation of immunosuppressive therapy and
thymectomy, ultimately leading to successful withdrawal from
transfusion dependence. This extremely rare clinical course
suggests the potential of cytotoxic chemotherapy (in addition to
immunosuppressive therapy) as a therapeutic option for
thymoma-associated PRCA. This case provides valuable insight that
contributes to the accumulation of clinical experience and aids in
the future development of evidence-based treatment guidelines.
Case report
Patient presentation, diagnosis and
treatment course
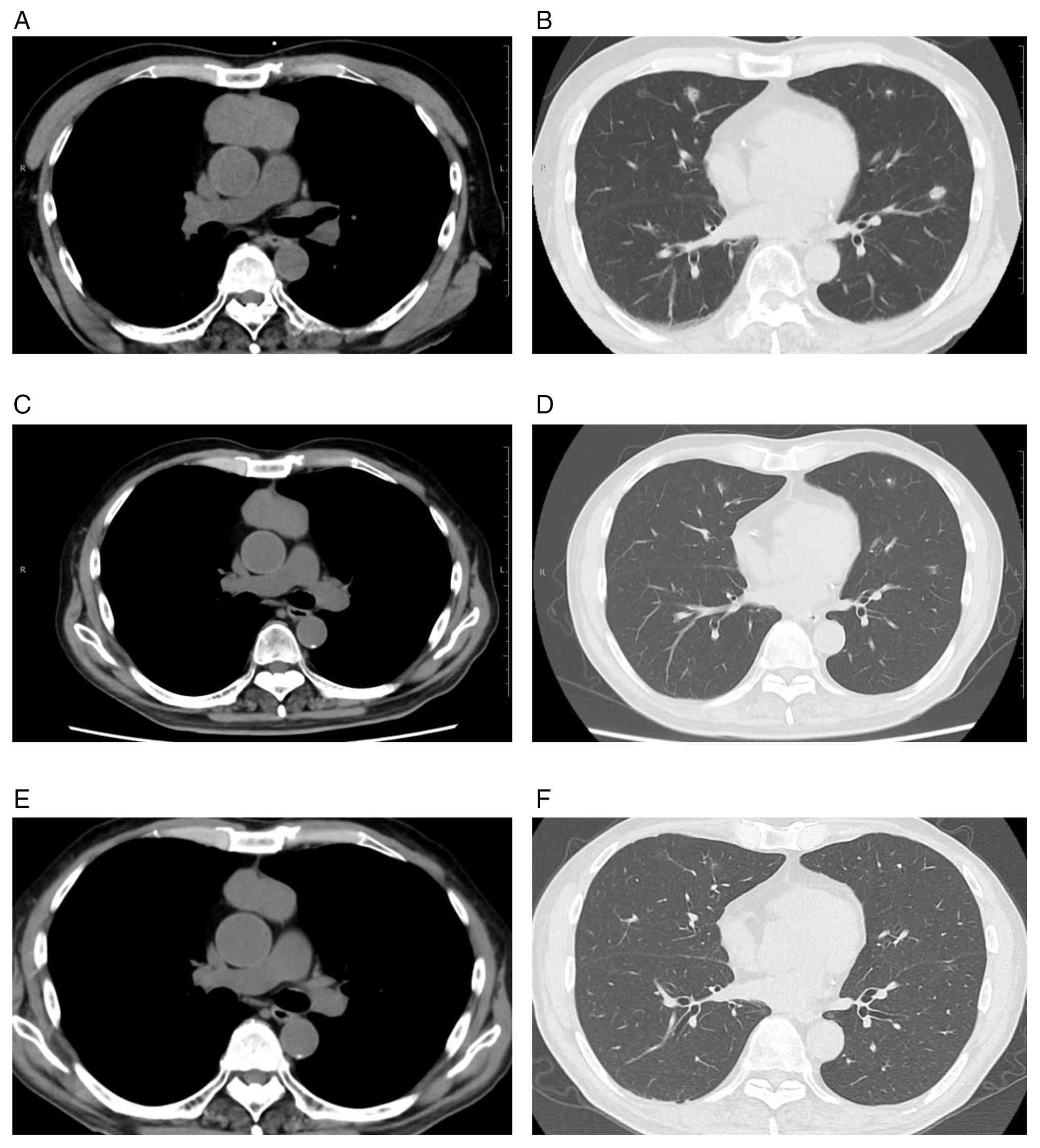
A 69-year-old man presented to a local physician
with a persistent cough since August 2024. Chest computed
tomography (CT) performed in April 2025 revealed a 6-cm mass in the
anterior mediastinum and multiple nodular lesions in both lungs
(Fig. 1A and B). After one month,
the patient was referred to our department of medical oncology for
further evaluation and treatment. Initial laboratory findings
revealed anemia with a hemoglobin level of 6.1 g/dl and a markedly
reduced reticulocyte count of 0.1%. White blood cell and platelet
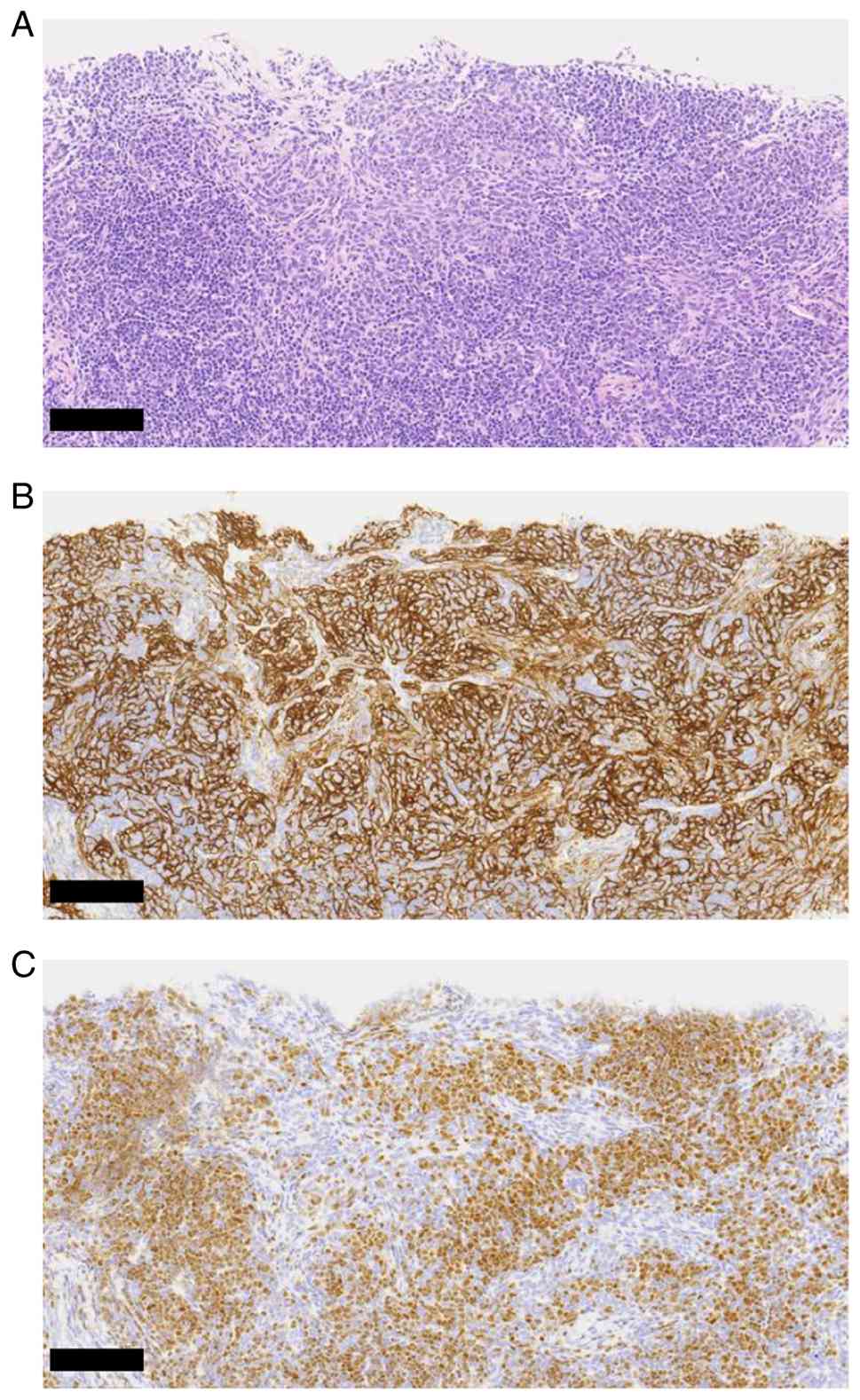
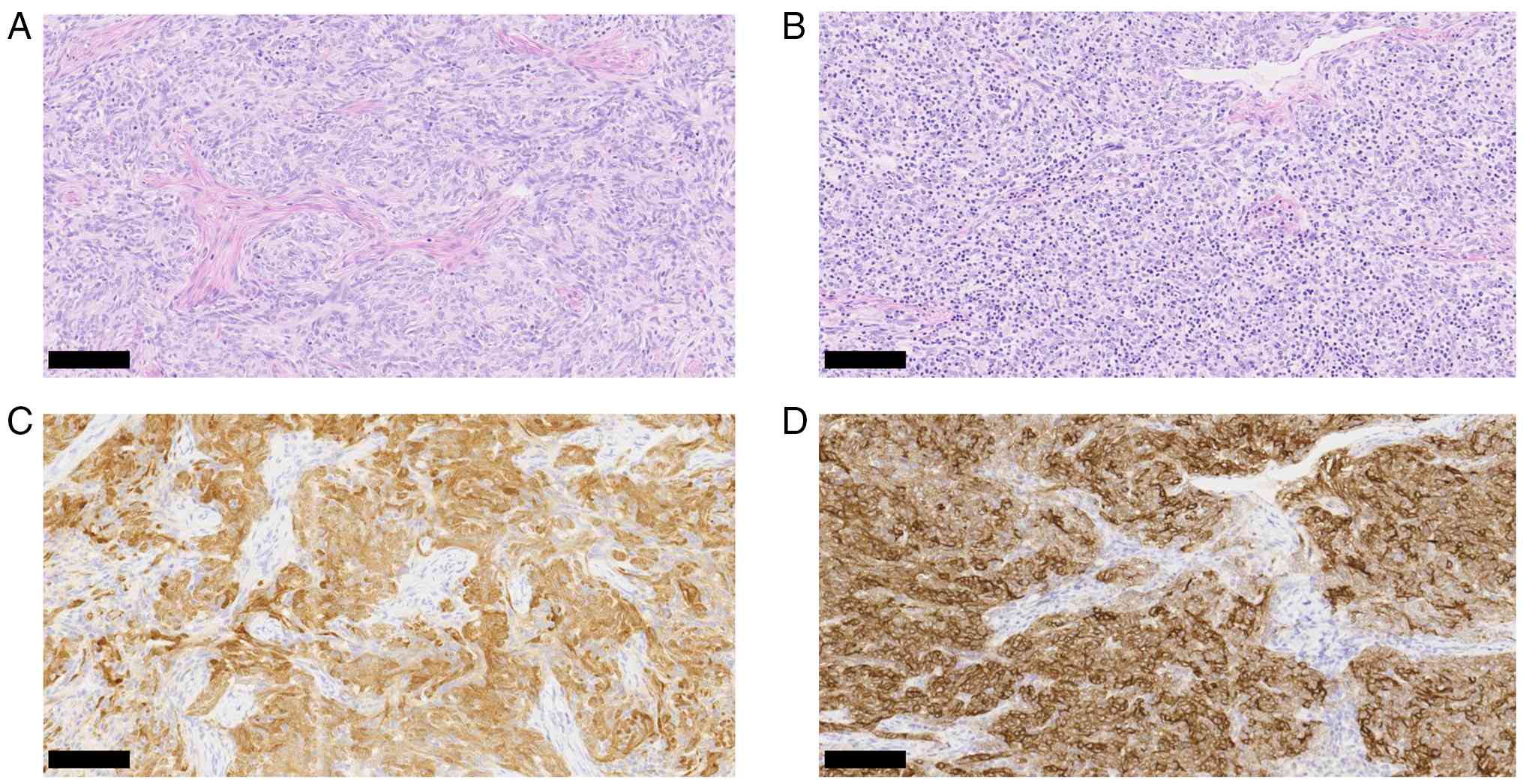
counts were within normal ranges. A CT-guided biopsy of the
anterior mediastinal mass led to a diagnosis of type AB thymoma
based on the World Health Organization (WHO) classification
(Fig. 2). The clinical stage was
cT1bN0M1b, stage IVB, based on the American Joint Committee on
Cancer 9th edition staging system. Serum levels of iron, copper,
zinc, and relevant vitamins were unremarkable, and parvovirus B19
IgM (EIA) was negative.
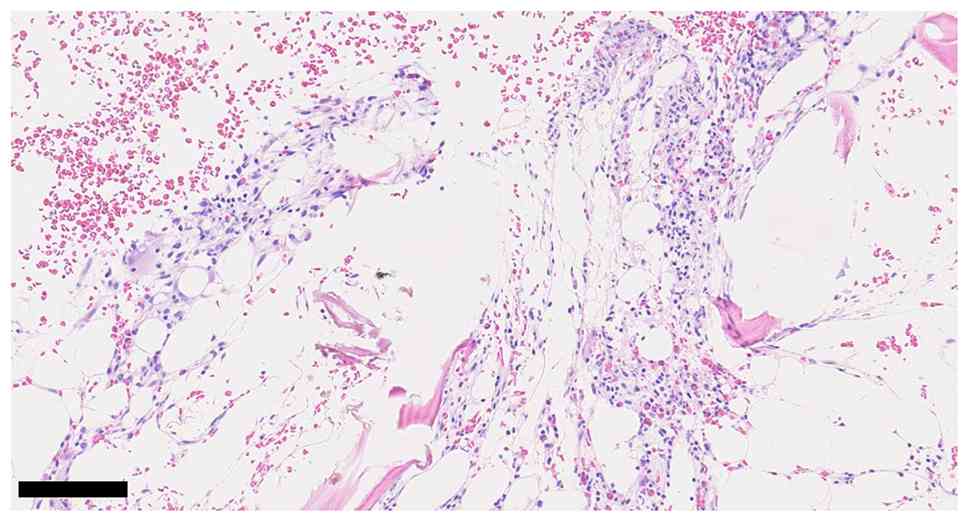
Since PRCA was suspected, a bone marrow biopsy was
performed by the hematology department. Histological examination
revealed a predominance of fatty marrow, with poorly visualized
erythroid islands and megakaryocytes, and no evidence of normal
hematopoietic cell clusters (Fig.
3). G-banding analysis of the bone marrow revealed no apparent
chromosomal abnormalities. Magnetic resonance imaging of the
thoracolumbar spine also demonstrated findings consistent with
fatty marrow replacement. Although aplastic anemia was initially
considered, the preserved white blood cell and platelet counts
supported a diagnosis of thymoma-associated PRCA.
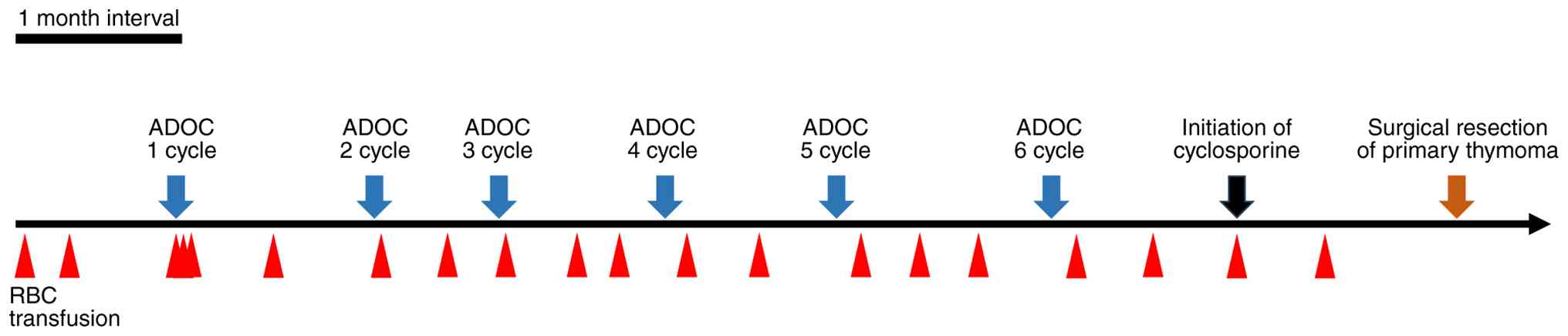
Upon the initial visit, the patient required regular
red blood cell transfusions (approximately 2 units per week) to
manage the anemia. Complete surgical resection of the anterior
mediastinal tumor was deemed unfeasible due to the multiple
pulmonary metastases, and thus systemic chemotherapy was initiated
in June 2025 to achieve disease control. Upon starting
chemotherapy, daily transfusions of 2 units of red blood cells were
required to maintain a hemoglobin level of 7 g/dl (Fig. 4). The patient was treated with the
ADOC regimen, consisting of doxorubicin (40 mg/m2),
cisplatin (25 mg/m2), vincristine (0.6 mg/m2)
and cyclophosphamide (700 mg/m2). A 50% reduced dose of
cisplatin (from 50 to 25 mg/m2) was used due to
preexisting renal dysfunction.
Remarkably, after the first cycle of chemotherapy,
transfusion dependence improved, with the interval between
transfusions extending to once every 7–17 days. However, on day 11
after the initial treatment, the patient developed febrile
neutropenia. During the second cycle, the doses of doxorubicin and
cyclophosphamide were reduced by 20%, and pegfilgrastim was
administered to support neutrophil recovery. After completing four
cycles, contrast-enhanced CT performed in September 2025
demonstrated shrinkage of the anterior mediastinal mass, as well as
reduction and partial obscuration of the pulmonary masses and
nodular lesions in both lungs (Fig. 1C
and D). The overall response was assessed as stable disease as
per Response Evaluation Criteria in Solid Tumors (RECIST) version
1.1. After six cycles, contrast-enhanced CT in November 2025
revealed further reduction of the anterior mediastinal mass, and
the pulmonary nodular lesions remained decreased in size,
indicating sustained disease control (Fig. 1E and F). The overall response
continued to meet the criteria for stable disease as per RECIST
version 1.1. Chemotherapy was completed after six cycles. Following
multidisciplinary discussion, a strategy of local tumor control was
adopted.
Anticipating further improvement in transfusion
dependence, cyclosporine was initiated in December 2025.
Cyclosporine was started at a dose of 150 mg/day, considering renal
function, and the trough level was 60.6 ng/ml eight days later. The
same dose was continued, and the desired effect was achieved. In
January 2026, robot-assisted resection of the anterior mediastinal
tumor was performed. Histopathological examination confirmed type
AB thymoma as per the WHO classification (Fig. 5), which is consistent with the
initial diagnosis established via CT-guided biopsy. Regarding the
need for transfusion, the final transfusion (2 units) was
administered 2 weeks after initiating cyclosporine. Thereafter, the
patient achieved transfusion independence, accompanied by
improvement in hemoglobin levels and reticulocyte counts.
Immunohistochemistry methods
Immunohistochemical staining was performed as
follows. CK AE1/AE3 staining employed an Agilent antibody (GA053,
clone AE1/AE3) and was performed on the DAKO Omnis system (EnVision
FLEX kit) with antigen retrieval at pH 9, 97°C for 30 min. TdT
staining was conducted using a Leica antibody (NCL-L-TdT-339, clone
SEN28) at a 1:50 dilution. Antigen retrieval was performed at 100°C
for 20 min, and staining was carried out on the Leica BOND-III
system using Protocol F. CD20 staining was performed using a Roche
antibody (760-2531, clone L26) on the BenchMark ULTRA PLUS system
(OptiView kit). PSMB11 (β5t) staining used a Proteintech antibody
(55143-1-AP, polyclonal) at a 1:300 dilution on the Leica BOND III
system (Protocol F), with antigen retrieval at pH 9, 100°C for 20
min. All immunostainings were interpreted according to standard
histopathological criteria.
Discussion
PRCA reportedly occurs in approximately 5% of
patients with thymoma (4,5). The standard management includes
surgical resection of the thymoma plus immunosuppressive therapy,
among which cyclosporine is the most frequently reported effective
agent (2,3).
In the present case, multiple bilateral pulmonary
metastases were identified at the initial visit, and therefore
systemic chemotherapy was prioritized over local treatment. The
ADOC regimen was chosen due to its previously demonstrated efficacy
in invasive thymoma (6). Initially,
the patient required weekly transfusions of 2 units of red blood
cells, and this progressively intensified until daily transfusions
of 2 units were needed to maintain a hemoglobin level of 7 g/dl at
the initiation of chemotherapy. Remarkably, after only a single
cycle of ADOC, the transfusion requirement decreased to 2 units
every 7–17 days.
In patients with metastatic thymoma complicated by
PRCA, immunosuppressive therapy (e.g., cyclosporine) may delay the
initiation of systemic chemotherapy. The concomitant administration
of immunosuppressive agents and cytotoxic chemotherapy may also
increase treatment-related toxicity. Meanwhile, the present case
demonstrates that transfusion dependence due to PRCA can be
ameliorated with cytotoxic chemotherapy alone. Such reports are
exceedingly rare, and only isolated cases have been previously
documented (7). This case provides
valuable insight into a potential therapeutic strategy in similarly
complex clinical scenarios. The decreased transfusion dependence
seen after the ADOC regimen could be because the hematological
improvement occurred concurrently with radiographic tumor
shrinkage. In other words, the antitumor effect of chemotherapy may
have helped ameliorate PRCA as a paraneoplastic syndrome. The
reduced tumor burden could have attenuated the immune dysregulation
caused by the thymoma, thereby partially restoring erythropoiesis.
Although components of the ADOC regimen, particularly
cyclophosphamide and the corticosteroids administered as part of
antiemetic prophylaxis, may have contributed to the hematological
improvement through their immunosuppressive effects, the regimen
was primarily administered for its antitumor activity. Reports
describing improvement of PRCA in this context remain extremely
limited; therefore, this case may provide clinically meaningful
insight into situations in which determining the optimal sequencing
of chemotherapy and immunosuppressive therapy is challenging.
Nevertheless, due to the inherent limitations of being a single
case report, definitive conclusions regarding the underlying
mechanism cannot be drawn. Although the transfusion-dependent
anemia improved alongside the antitumor response in this patient,
previous reports have suggested that antitumor effects do not
necessarily correlate with the therapeutic effect on PRCA as a
paraneoplastic syndrome (8). Thus,
treatment strategies should be individualized according to the
clinical course in each case, and further accumulation of similar
cases is warranted.
After six cycles of ADOC, the primary thymic tumor
was markedly reduced, and the pulmonary metastases also
demonstrated significant shrinkage with partial obscuration. No new
metastatic lesions were detected at that time. Although transfusion
dependence had improved compared with the pre-chemotherapy status,
the patient still required red blood cell transfusions every 7–17
days. Based on these findings, a multidisciplinary discussion was
conducted, and surgical resection of the primary thymic tumor was
planned. In this context, it is important to note that the
pulmonary metastatic lesions had already shown marked shrinkage
following systemic chemotherapy. Furthermore, a previous
meta-analysis has suggested a potential survival benefit of
debulking surgery in patients with unresectable thymoma (9). Taking these factors into account, a
multidisciplinary team-including thoracic surgeons, oncologists,
and hematologists-concluded that surgical resection at a time when
the primary tumor had sufficiently regressed would be a reasonable
strategy. After completing six cycles of chemotherapy in
preparation for surgery, it became feasible to initiate
immunosuppressive therapy. Cyclosporine was started in December
2025, and surgical resection of the primary thymoma was performed
in January 2026. Two weeks after initiating cyclosporine, the
patient received two units of red blood cells, which was the final
transfusion required. Thereafter, the patient achieved transfusion
independence and has remained free from further transfusion
support. For future management, cyclosporine will be continued, and
the patient will undergo regular imaging follow-up. If pulmonary
lesions become clinically apparent, local treatment with
radiofrequency ablation will be considered.
Several case reports have described tumor shrinkage
of thymoma accompanied by improvement of PRCA after cyclosporine
therapy (8,10). Despite the limited evidence, the
potential antitumor effect of cyclosporine cannot be excluded.
Nevertheless, in patients with metastatic thymoma complicated by
PRCA, further investigation is required to clarify whether systemic
chemotherapy should be prioritized or if early introduction of
cyclosporine is preferable. The significance of this case lies in
the fact that the ADOC regimen achieved both an antitumor effect
and partial improvement of PRCA in metastatic thymoma, which
subsequently enabled surgical resection and the initiation of
cyclosporine therapy, ultimately leading to transfusion
independence. The present evidence suggests that treatment
decisions should be individualized alongside careful evaluation of
both oncological and hematological responses. Further accumulation
of clinical evidence regarding this rare and therapeutically
challenging condition is essential to develop optimal therapeutic
strategies.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
NH conceptualized the manuscript. Data acquisition
and interpretation were performed by NH, RS, YK, YY, MO, SOk, SOc,
RM, MH, SA, MaiT, AY and MasT. The original draft was written by
NH, while the final manuscript was written, reviewed and edited by
NH and MasT. NH and MasT confirm the authenticity of all the raw
data. All authors read and approved the final manuscript, and agree
to be accountable for all aspects of the research in ensuring that
the accuracy or integrity of any part of the work are appropriately
investigated and resolved.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of this case report and the accompanying
images. The patient was informed that all identifying information
would be removed to ensure anonymity.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
PRCA
|
pure red cell aplasia
|
|
CT
|
computed tomography
|
|
WHO
|
World Health Organization
|
|
ADOC
|
doxorubicin, cisplatin, vincristine
and cyclophosphamide
|
|
RECIST
|
Response Evaluation Criteria in Solid
Tumors
|
References
|
1
|
Engels EA: Epidemiology of thymoma and
associated malignancies. J Thorac Oncol. 5 (10 Suppl 4):S260–S265.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hirokawa M, Sawada K, Fujishima N, Nakao
S, Urabe A, Dan K, Fujisawa S, Yonemura Y, Kawano F, Omine M, et
al: Long-term response and outcome following immunosuppressive
therapy in thymoma-associated pure red cell aplasia: A nationwide
cohort study in Japan by the PRCA Collaborative Study Group.
Haematologica. 93:27–33. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Xavier RD, Devaraj S, Sadasivam V,
Prakasam O, Menon N, Hariharan A and Sundaramoorthi T: Thymoma
associated with pure red cell aplasia: A case report and literature
review. Indian J Thorac Cardiovasc Surg. 36:404–408. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yen CC, Huang WL, Li SS, Chen YP, Tseng
YL, Yen YT, Chu CY, Hsu YT and Chen TY: Pure red cell aplasia and
other haematological diseases associated with thymoma: A case
series and systematic review. Front Med (Lausanne). 8:7599142021.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Moriyama S, Yano M, Haneda H, Okuda K,
Kawano O, Sakane T, Oda R, Watanabe T and Nakanishi R: Pure red
cell aplasia associated with thymoma: A report of a single-center
experience. J Thorac Dis. 10:5066–5072. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fornasiero A, Daniele O, Ghiotto C, Piazza
M, Fiore-Donati L, Calabró F, Rea F and Fiorentino MV: Chemotherapy
for invasive thymoma: A 13-year experience. Cancer. 68:30–33. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lesire B, Durieux V, Grigoriu B, Girard N
and Berghmans T: Management of thymoma associated autoimmune pure
red cell aplasia: Case report and systematic review of the
literature. Lung Cancer. 157:131–146. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Muratori L, Delcuratolo MD, Sperone P and
Scagliotti GV: Discrepancy between tumor response and hematologic
response in a patient with thymoma and aplastic anemia treated with
ciclosporin. Mediastinum. 4:82020. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hamaji M, Kojima F, Omasa M, Sozu T, Sato
T, Chen F, Sonobe M and Date H: A meta-analysis of debulking
surgery versus surgical biopsy for unresectable thymoma. Eur J
Cardiothorac Surg. 47:602–607. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Isshiki Y, Tanaka H, Suzuki Y and Yoshida
Y: Cyclosporine is a potential curative treatment option for
advanced thymoma. Exp Hematol Oncol. 6:132017. View Article : Google Scholar : PubMed/NCBI
|