Introduction
Endometrial cancer (EC) is one of the most prevalent
malignant tumors of the female reproductive system. Each year, EC
develops in ~142,000 women worldwide, and an estimated 42,000 women
die from this cancer. In recent years, its incidence has been on
the rise globally, particularly in developed countries, and it is
strongly associated with obesity, metabolic syndrome and elevated
estrogen exposure (1). While
patients with early-stage EC can achieve favorable prognoses
through surgical intervention combined with adjuvant radiotherapy
and chemotherapy, the management of advanced, recurrent and
metastatic EC remains a significant challenge. Traditional
therapies are prone to drug resistance and induce considerable
toxicities and side effects, urgently calling for improvement in
patient survival rates (2).
Consequently, the development of novel targeted therapies and
immunotherapeutic strategies has emerged as a critical focus of
contemporary research.
Programmed cell death 1 (PD-1/PDCD1) signaling, as a
fundamental immune checkpoint mechanism, downregulates inflammatory
responses and maintains immune homeostasis (3). The PD-1/programmed cell death ligand 1
(PD-L1) signaling pathway not only serves as an important route for
preventing autoimmune diseases but also exerts a significant impact
on the delicate balance between tumor immune surveillance and
immune tolerance (4). PD-1/PD-L1
inhibitors have emerged as a groundbreaking therapeutic approach,
effectively reversing T-cell exhaustion by blocking negative
regulatory signals (5). The U.S.
Food and Drug Administration has approved anti-PD-1 antibodies as a
second-line therapy for non-microsatellite instability-high and
deficient mismatch repair advanced EC with a PD-L1 Combined
Positive Score ≥1 (6). However, the
response rates of other molecular subtypes to immune checkpoint
inhibitors, particularly p53-mutated EC or special types of
endometrioid carcinoma (e.g., serous papillary carcinoma, clear
cell carcinoma, undifferentiated carcinoma, small cell carcinoma or
mixed cell carcinoma), remain low. Consequently, exploring
combination drug strategies to enhance therapeutic efficacy has
become a key research focus.
Meanwhile, monoclonal antibodies targeting the CD20
antigen on the surface of B cells, (e.g., Rituximab) have been
widely used in the treatment of B-cell lymphomas. Recent studies
have demonstrated that CD20 is abnormally expressed in certain
solid tumors, including breast cancer and ovarian cancer. High CD20
expression has also been detected in EC tissues, and anti-CD20
antibodies exert anti-tumor effects through multiple mechanisms,
including antibody-dependent cellular cytotoxicity (ADCC),
complement-dependent cytotoxicity (CDC) and the induction of tumor
cell apoptosis (7,8). A previous Mendelian randomization
analysis by our group revealed a significant association between
CD20 and EC, suggesting that anti-CD20 antibodies may exert
protective effects against EC and reduce its risk (9). Furthermore, B-cell infiltration and
abnormal activation are observed in the EC microenvironment,
indicating that CD20 may play a role in regulating tumor
progression. However, its expression patterns and biological
functions in EC remain elusive, and its therapeutic potential has
yet to be fully explored.
The occurrence and progression of EC are intricately
associated with uncontrolled cell proliferation, impaired apoptosis
and disrupted cell cycle regulation. Targeting these biological
processes represents a central strategy in anti-tumor therapy
(10). However, the synergistic
mechanisms underlying the combination of anti-CD20 antibodies and
PD-1 antibodies in EC have not been comprehensively investigated.
Specifically, the effects of these agents on tumor cell
proliferation, apoptosis and cell cycle regulation remain to be
fully clarified. In light of this, the present study aims to
investigate the biological impacts of anti-CD20 and PD-1 antibodies
on EC cells. Through in vitro experiments, their effects on
cell proliferation, apoptosis and cell cycle distribution were
explored with the goal of providing a novel theoretical basis for
combined immunotherapy in EC and promoting its translational
research for clinical application.
Materials and methods
Bioinformatics
All raw and processed transcriptomic, genomic and
clinical data for the Uterine Corpus Endometrial Carcinoma (UCEC)
cohort were obtained from The Cancer Genome Atlas (TCGA) 1.0
release. The TCGA overall study accession number in the database of
Genotypes and Phenotypes (https://www.ncbi.nlm.nih.gov/gap) is PHS000178,
TCGA-UCEC dataset official identifier: TCGA-UCEC. Transcriptome
data for patients with EC, initially including 537 tumor samples
and 35 normal endometrial samples, were downloaded from the
TCGA-UCEC database (https://portal.gdc.cancer.gov/projects/TCGA-UCEC).
After exclusion of samples with zero expression values, the final
analytic dataset comprised of 472 tumor samples and 35 normal
endometrial samples.
Cell lines and culture conditions
EC cell lines [Ishikawa (99040201) and HEC-1A
(HTB-112)] were obtained from the EC Cell Bank of the Chinese
Academy of Sciences. Normal endometrial epithelial cells (hEEC)
were purchased from Procell Life Science & Technology Co., Ltd.
Ishikawa cells are estrogen receptor-positive, while HEC-1A cells
show low expression of the estrogen receptor. Cells were cultured
in corresponding media (McCoy's 5A for HEC-1A; Dulbecco's modified
Eagle's medium for Ishikawa; both Gibco; Thermo Fisher Scientific,
Inc.) supplemented with 10% fetal bovine serum (Gibco; Thermo
Fisher Scientific, Inc.) and incubated in a humidified incubator at
37°C with 5% CO2. Cells in the logarithmic growth phase
were selected for use in subsequent experiments.
Reverse-transcription quantitative
(RT-q)PCR analysis
Total RNA was isolated from tissue samples, cultured
cells (hEEC, Ishikawa and HEC-1A cells) and exosomes using TRIzol
reagent (Thermo Fisher Scientific, Inc.). The RNA was subsequently
reverse-transcribed into complementary DNA (cDNA) using a reverse
transcription kit (cat. no. RR036A; Takara Bio, Inc.) according to
the manufacturer's instructions. Real-time quantitative PCR was
carried out using SYBR Premix ExTaq™ II (cat. no. RR820A; Takara
Bio, Inc.). According to the manufacturer's instructions, a 20-µl
PCR mixture was used in a Q5 PCR instrument (Thermo Fisher
Scientific, Inc.). The following thermocycling conditions were
applied: Pre-denaturation at 95°C for 30 sec for 40 cycles;
followed by 95°C for 5 sec and 60°C for 34 sec. The gene expression
levels relative to β-actin were determined using the
2-∆∆Cq method. All the steps were carried out in
accordance with the manufacturer's instructions. The primer
sequences used in the analysis are provided in Table I.
 | Table I.Primer sequences (5′-3′). |
Table I.
Primer sequences (5′-3′).
| Gene name | Forward | Reverse |
|---|
| MS4A1 |
TGATGCTGATCTTTGCCTTCTTCC |
TCGTCTCTGTTTCTTCTTCTTCCTC |
| PDCD1 |
GCTGCACTAATTGTCTATTGGG |
CACAGTAATTCGCTTGTAGTCG |
| β-actin |
CACTCTTCCAGCCTTCCTTC |
GTACAGGTCTTTGCGGATGT |
Antibody sources
Anti-CD20 antibodies (e.g., Rituximab; cat. no.
HY-P9913) and immune checkpoint inhibitors (e.g., Pembrolizuma;
cat. no. HY-P9902), with purity exceeding 95%, were procured from
MedChemExpress.
Selection of drug working
concentration and cell proliferation experiments
Ishikawa and HEC-1A cells in the logarithmic growth
phase were seeded into 96-well plates at a density of
5×103 cells per well. After 24 h of cultivation, various
drug concentrations were subsequently added (Rituximab: 0,10, 20,
30, 40, 50 µg/ml; Pembrolizumab: 0,0.001, 0.01, 0.1, 1, 10 nM). At
different time-points post-treatment (24, 48 and 72 h), CCK-8
reagent (Tongren Institute of Chemistry) was added to each well,
followed by a 2-h incubation period. The absorbance values were
measured as the optical density (OD) at a wavelength of 490 nm
using a microplate reader to assess the inhibitory effects of
Rituximab and Pembrolizumab. Based on these results, the optimal
inhibitory concentration was determined. Subsequently, the optimal
inhibitory concentration [half-maximal inhibitory concentration
(IC50)] for the combination treatment group was screened. The cell
proliferation inhibition rate was calculated using the following
formula: Inhibition Rate (%)=(1-OD value of experimental group/OD
value of control group) ×100%. A drug concentration of 0 represents
the negative control group.
Detection of apoptosis by
phycoerythrin/7-amino-actinomycin D (PE/7-AAD) double staining
Ishikawa and HEC-1A cells in the logarithmic growth
phase were seeded into 6-well plates. When the cells reached ~50%
confluence, they were treated with drugs and divided into the
following groups: Rituximab (10, 20, 30 µg/ml); Pembrolizumab
(0.01, 0.1, 1 nM); Combination Groups (0.001, 0.01, 0.1 nM). After
48 h of incubation, the cells were harvested, digested with trypsin
(Gibco; Thermo Fisher Scientific, Inc.), washed with PBS and
resuspended in Binding Buffer. They were then stained with 5 µl PE
and 10 µl 7-AAD (United Division) at 4°C and incubated in the dark
for 15 min. Apoptosis was analyzed using a flow cytometer.
Cell cycle analysis [propidium (PI)
staining]
Cells treated for 48 h were harvested, washed with
prechilled PBS three times and fixed in 70% ethanol at 4°C
overnight. Centrifugation was performed at 300 × g for 5 min at 4°C
to remove the ethanol. The cells were resuspended in a staining
solution containing 50 µg/ml PI and 100 µg/ml RNase A (Thermo
Fisher Scientific, Inc.), and incubated at 37°C in the dark for 30
min. The cell cycle distribution (G0/G1 phase, S phase, G2/M phase)
was analyzed by flow cytometry and the proportions of each phase
were quantified using FlowJo software (v10.10.1; BD
Biosciences).
Statistical analysis
The experimental data are presented as the mean ±
standard deviation. Statistical analysis was performed using
GraphPad Prism 8.0 software (Dotmatics). Intergroup differences
were assessed using one-way ANOVA (Tamhane's T2 test) or unpaired
t-tests, and P<0.05 was considered to indicate statistical
significance. All experiments were independently repeated three
times. In the CCK-8 assay, for the same conditions, 5 parallel
wells were used. After eliminating the two wells with the greatest
difference, a total of 3 parallel wells remained.
Results
Differential expression of MS4A1 and
PDCD1
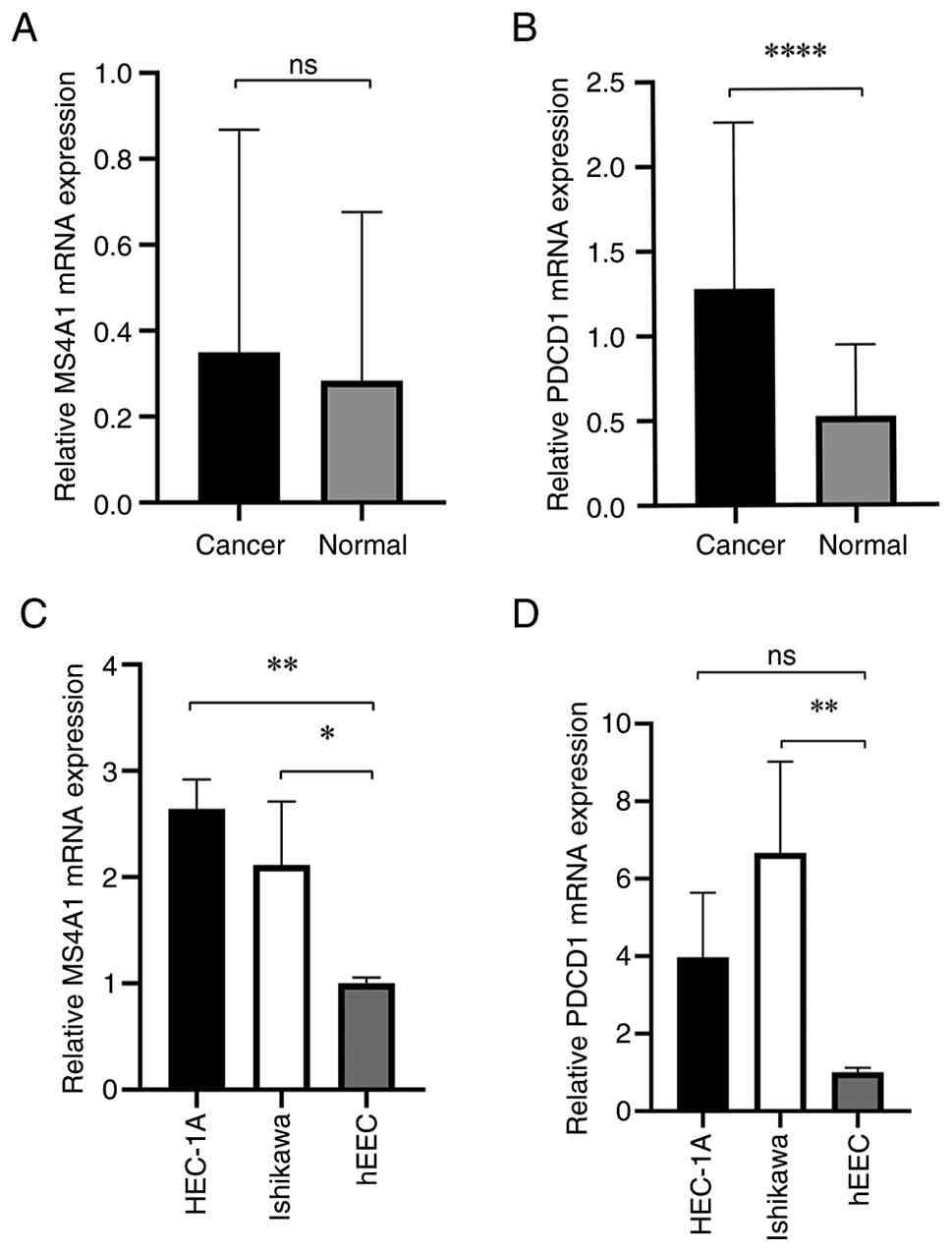
The differential expression analysis of MS4A1 and
PDCD1 was conducted using the EC dataset from the TCGA database.
MS4A1 encodes the CD20 protein, while PDCD1 encodes PD-1. R
programming language was utilized to evaluate the expression levels
of these two genes in EC tissues compared to normal endometrial
tissues. The results showed that MS4A1 exhibited higher expression
in EC tissues; however, this difference was not statistically
significant (Fig. 1A). By contrast,
PDCD1 demonstrated significantly higher expression in EC tissues
compared to normal endometrial tissues (Fig. 1B). Meanwhile, RT-qPCR was used to
assess the differential expression of MS4A1 and PDCD1 in EC cells.
Compared with normal endometrial cells, the expression of MS4A1 and
PDCD1 in EC cells was markedly upregulated (Fig. 1C and D).
Effects of different concentrations of
Rituximab and Pembrolizumab on the proliferation of Ishikawa and
HEC-1A cells
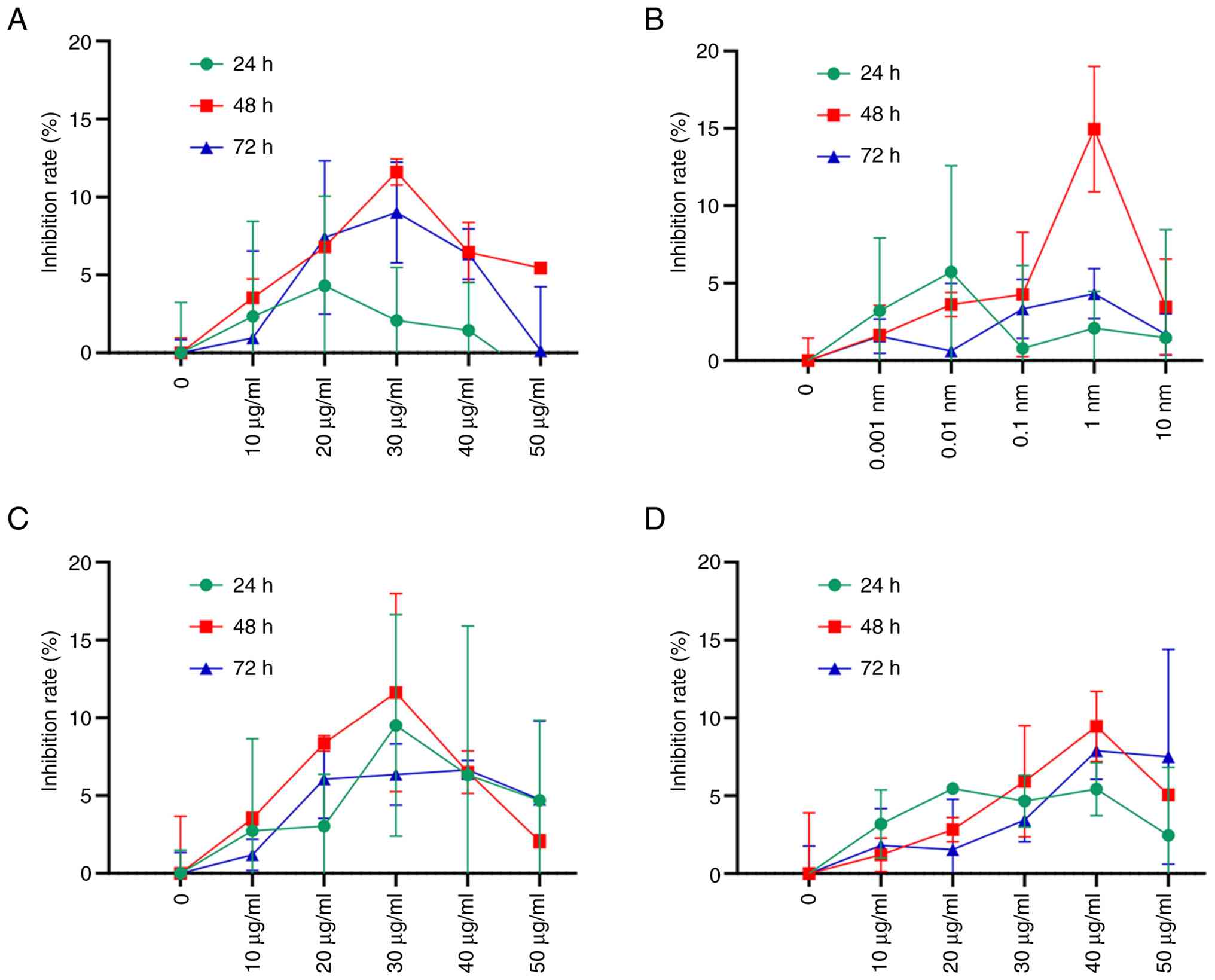
Cell proliferation was assessed via the CCK-8 assay.
The results showed that various concentrations of Rituximab and
Pembrolizumab markedly inhibited the viability of Ishikawa and
HEC-1A cells, with the inhibitory effect increasing as the drug
concentration increased. Notably, Rituximab at a concentration of
30 µg/ml and Pembrolizumab at a concentration of 1 nM exhibited the
most pronounced inhibitory effects after 48 h (P<0.05). Thus, 48
h was selected for subsequent experiments (Fig. 2 and Table II). The relatively weaker
inhibitory effect of rituximab on HEC-1A cells at 48 h may be due
to a plateau effect or mild compensatory cell proliferation after
prolonged treatment. Additionally, the optimal concentration of
Rituximab (30 µg/ml) and the concentration gradient of
Pembrolizumab in the combination group were investigated (Table III). The concentration of
Rituximab (30 µg/ml) was determined based on preliminary
dose-response experiments in EC cells. This concentration produced
a moderate but significant inhibitory effect on cell proliferation
without excessive cytotoxicity, which was suitable for evaluating
the synergistic effect in combination with pembrolizumab. The
findings revealed that the optimal concentration of Pembrolizumab
in the combination group was 0.1 nM, which was subsequently
utilized for further experiments (Table IV).
| Table II.Effects of Rituximab on endometrial
cancer cell proliferation. |
Table II.
Effects of Rituximab on endometrial
cancer cell proliferation.
|
| Ishikawa | HEC-1A |
|---|
|
|
|
|
|---|
| Concentration,
µg/ml | Mean±SD | P-value | Mean±SD | P-value |
|---|
| 0 | 0±1.58 |
| 0±0.56 |
|
| 10 | 2.44±0.79 | 0.14 | 1.93±1.98 | 0.37 |
| 20 | 2.93±0.15 | 0.08 | 4.88±3.91 | 0.04 |
| 30 | 9.20±1.67 | <0.001 | 9.09±1.90 | <0.001 |
| 40 | 5.99±1.51 | 0.00 | 4.88±0.32 | 0.04 |
| 50 | 3.82±2.47 | 0.03 | 4.35±1.55 | 0.06 |
| Table III.Effects of Pembrolizumab on
endometrial cancer cell proliferation. |
Table III.
Effects of Pembrolizumab on
endometrial cancer cell proliferation.
|
| Ishikawa | HEC-1A |
|---|
|
|
|
|
|---|
| Concentration,
nm | Mean±SD | P-value | Mean±SD | P-value |
|---|
| 0 | 0±3.47 |
| 0±0.75 |
|
| 0.001 | 4.15±0.68 | 0.18 | 2.35±1.30 | 0.05 |
| 0.01 | 6.20±0.40 | 0.09 | 5.17±0.83 | <0.001 |
| 0.1 | 6.50±0.71 | 0.06 | 7.05±1.26 | <0.001 |
| 1 | 13.75±1.09 | <0.001 | 9.72±1.50 | <0.001 |
| 10 | 7.98±0.29 | 0.01 | 4.63±0.21 | <0.001 |
| Table IV.Effects of combination treatment on
endometrial cancer cell proliferation. |
Table IV.
Effects of combination treatment on
endometrial cancer cell proliferation.
|
| Ishikawa | HEC-1A |
|---|
|
|
|
|
|---|
| Pembrolizumab
concentration, nm | Mean±SD | P-value | Mean±SD | P-value |
|---|
| 0 | 0±3.76 |
| 0±2.46 |
|
| 0.001 | 7.01±3.03 | 0.01 | 7.61±4.50 | 0.01 |
| 0.01 | 9.89±1.37 | <0.001 | 6.31±1.77 | 0.04 |
| 0.1 | 15.45±1.04 | <0.001 | 14.60±1.38 | <0.001 |
| 1 | 11.44±1.81 | <0.001 | 3.70±2.50 | 0.19 |
| 10 | 7.61±0.71 | 0.01 | 5.02±2.31 | 0.09 |
Effects of Rituximab and Pembrolizumab
on EC cell apoptosis
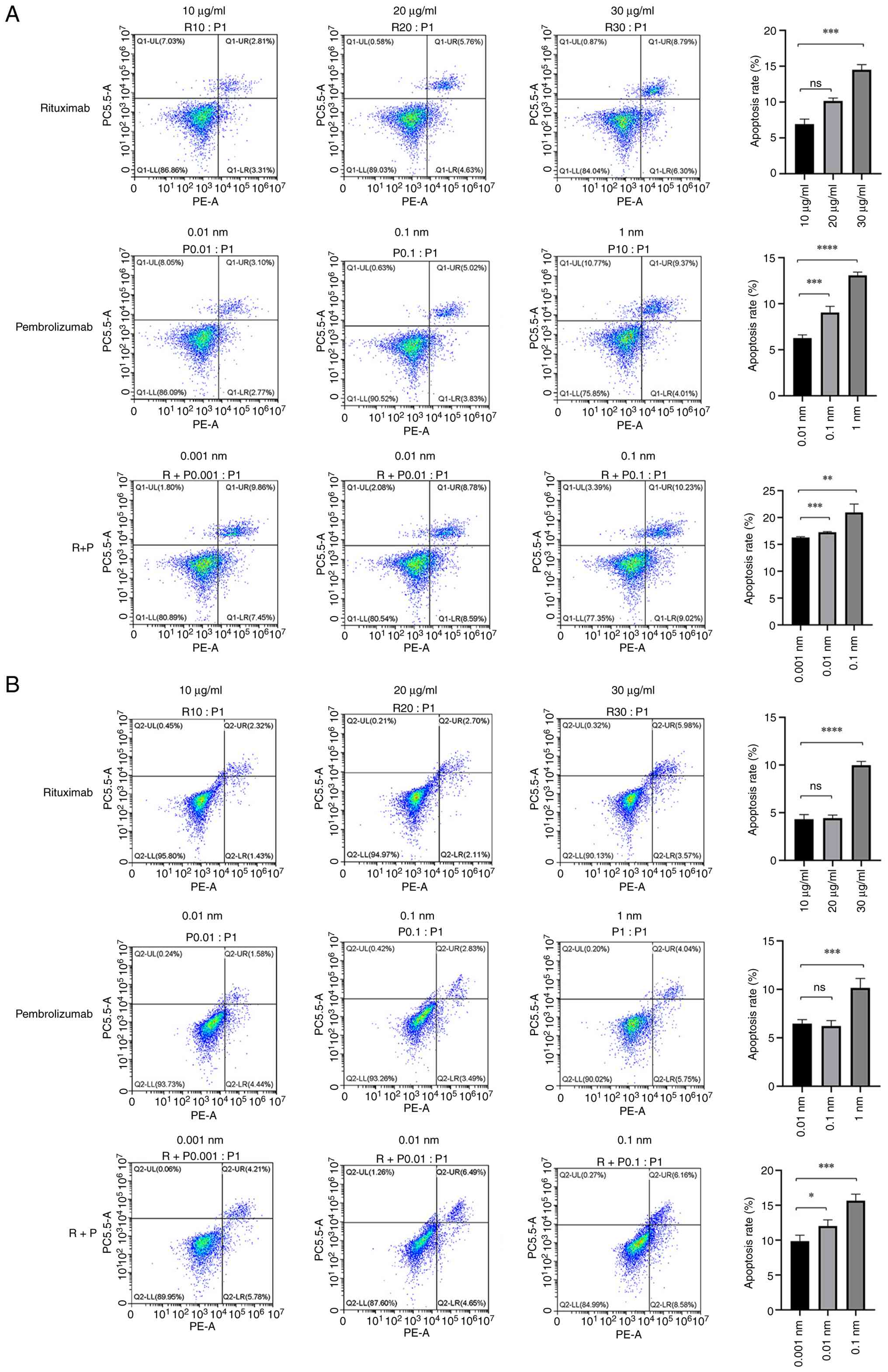
To explore the dose-dependent effect of the drugs
and revalidate their optimal concentrations, apoptosis was assessed
using PE/7-AAD double staining. The results demonstrated that
varying concentrations of Rituximab and Pembrolizumab significantly
suppressed the viability of Ishikawa and HEC-1A cells, with the
inhibitory effect increasing as the drug concentration rose.
Further analysis revealed that the proportion of apoptotic cells in
the combination treatment group was significantly higher than in
the single-drug groups, suggesting a synergistic effect of the two
antibodies in inducing apoptosis (Fig.
3).
Effects of Rituximab and Pembrolizumab
on EC cell cycle
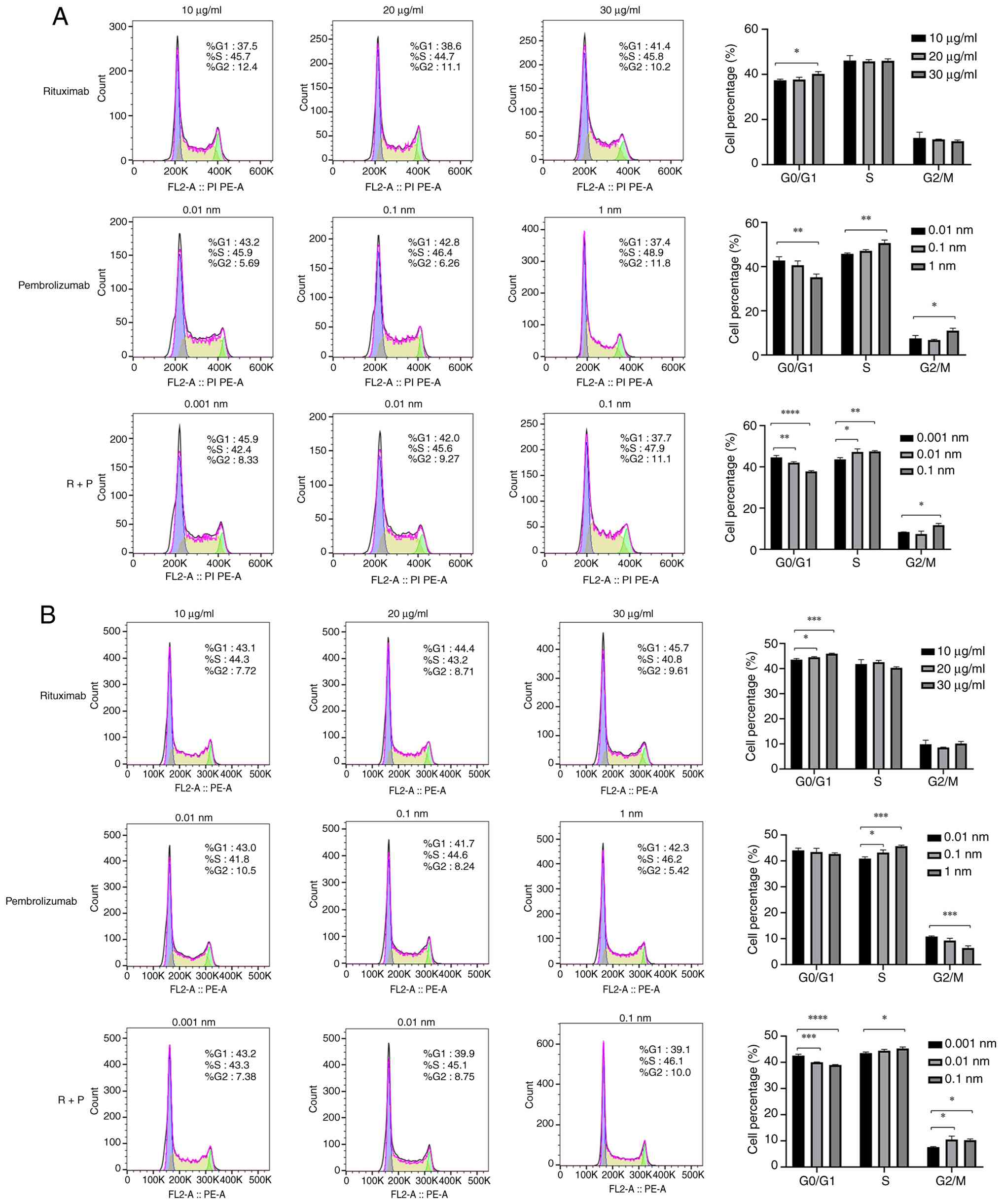
The cell cycle distribution was analyzed using PI
staining. The results demonstrated that gradients of Rituximab at
different concentrations elevated the proportion of Ishikawa and
HEC-1A cells in the G0/G1 phase, indicating that Rituximab inhibits
cell proliferation by inducing G0/G1 phase arrest. Conversely,
different concentrations of Pembrolizumab raised the proportion of
Ishikawa and HEC-1A cells in the S phase, suggesting that
Pembrolizumab suppresses cell proliferation by inducing S-phase
arrest. The combination of the two antibodies further elevated the
cell ratio in the S and G2/M phases, indicating that the two
antibodies inhibit cell proliferation by inducing S- and G2/M phase
arrest, with Pembrolizumab playing a predominant role (Fig. 4).
Discussion
In recent years, immunotherapy has achieved
remarkable breakthroughs in the treatment of malignant tumors,
particularly with the widespread clinical application of immune
checkpoint inhibitors and monoclonal antibodies. To date, the roles
of anti-CD20 antibodies and immune checkpoint inhibitors (e.g.,
PD-1 antibodies) in EC have been confirmed. However, systematic
explorations of the synergistic effects of these two therapeutic
modalities remain relatively scarce. This study was the first, to
the best of our knowledge, to comprehensively evaluate the
individual and combined effects of the anti-CD20 antibody Rituximab
and the PD-1 antibody Pembrolizumab on EC cells, thus offering
novel insights into the clinical management of this prevalent
gynecological malignancy.
Anti-CD20 antibodies can effectively inhibit tumor
progression through diverse antitumor mechanisms. CD20 is a
transmembrane cellular protein that has been validated as a
therapeutic target for B-cell malignancies (11). Rituximab, the first CD20 monoclonal
antibody approved for use in cancer patients, is a human/mouse
chimeric anti-CD20 monoclonal antibody. Additionally, it exhibits
an excellent safety profile in patients with various CD20+ lymphoid
malignancies (12). Studies have
shown that anti-CD20 antibodies exhibit effective therapeutic
outcomes in patients with multiple sclerosis (13). Schlaak et al (14) demonstrated that although melanoma
has low CD20 expression, anti-CD20 antibody treatment remains
efficient. The anti-tumor mechanisms of anti-CD20 antibodies
include: i) High-density CD20+ B cells may possess anti-tumor
immunity potential; ii) certain tumor cell lines express CD20, and
anti-CD20 antibodies can directly kill tumor cells through ADCC and
CDC; iii) anti-CD20 antibodies may indirectly enhance T
cell-mediated anti-tumor immune responses by depleting
immunosuppressive B-cell subsets, such as regulatory B cells
(15). Tertiary lymphoid structures
(TLS) are ectopic lymphoid aggregates that occur in inflamed,
infected or neoplastic tissues. These structures share features
analogous to lymph node architecture, including the presence of
large clusters of CD20-positive B lymphocytes, which are critical
for mediating adaptive immune responses (16). Previous studies have demonstrated an
association between TLS and favorable prognosis as well as enhanced
immunotherapy responsiveness in patients with endometrial cancer
(EC) (17,18). A high level of CD20+ B-cell
infiltration has been observed in EC, with significant CD20
expression detected in EC tissues (19,20),
corroborating the findings from a bioinformatics analysis performed
as part of the present study regarding the elevated expression of
MS4A1. However, the difference was not statistically significant,
potentially attributable to the limited sample size. CD20 is highly
expressed in EC tissues but it remains unknown whether CD20 is
highly expressed on the tumor cells themselves or on the
infiltrating B cells within the tumor microenvironment. Mendelian
randomization analyses have revealed a strong correlation between
CD20 and EC, suggesting that anti-CD20 antibodies may exert
protective effects and reduce EC risk (9). Consistent with this hypothesis, the
current study found that Rituximab inhibits EC-cell proliferation
and promotes apoptosis by inducing G0/G1-phase arrest, with the
inhibitory effect increasing in a concentration-dependent manner,
thereby validating the protective role of anti-CD20 antibodies in
EC cells.
PD-1 antibodies can effectively inhibit tumor
progression through diverse anti-tumor mechanisms. PD-1 receptor
and its ligand, PD-L1, constitute a critical immune checkpoint
pathway responsible for regulating T-cell activation (21). PD-1 is primarily expressed on T
cells and PD-L1 on tumor, immune and stromal cells. PD-L1 is
upregulated on various cancer cells, facilitating tumor immune
escape. Over the past decade, therapeutic antibodies targeting the
PD-1/PD-L1 axis have been developed to alleviate the
immunosuppression caused by these two proteins (22,23).
Despite extensive research, the prognostic significance of PD-1
remains controversial and its functional role within the tumor
microenvironment awaits further elucidation (24). Regarding the anti-tumor mechanism,
the PD-1 antibody specifically binds to PD-1 on the surface of
tumor cells or immune cells, thereby blocking its interaction with
PD-L1. This action releases T cells from their inhibitory state,
restoring their cytotoxic capabilities against tumors. Upon
blockade of the PD-L1/PD-1 signaling pathway, T cells regain their
capacity for proliferation, cytokine secretion (e.g., IFN-γ, TNF-α)
and direct tumor cell killing. Additionally, the PD-1 antibody may
indirectly activate dendritic cells and natural killer cells,
enhancing antigen presentation and the overall anti-tumor immune
response (25). In gastric cancer
treatment, the use of PD-1 antibodies effectively prolongs
progression-free survival (PFS) and overall survival (OS), while
minimizing adverse reactions and improving clinical outcomes
(26). PD-1 antibody therapy,
either as monotherapy or in combination with chemotherapy, has
shown significant improvements in OS and PFS in patients with lung
cancer and high PD-1 expression (27). As adjuvant therapy for high-risk
stage III melanoma, PD-1 antibodies have significantly prolonged
recurrence-free survival when compared to placebo (28). In advanced or recurrent EC, the
addition of Pembrolizumab to standard chemotherapy resulted in
significantly longer PFS compared to chemotherapy alone (29). The bioinformatics analysis of the
present study revealed that PDCD1 expression was significantly
upregulated in EC tissues relative to normal endometrial tissues.
Furthermore, cellular experiments indicated that Pembrolizumab
could inhibit EC-cell proliferation by inducing S-phase arrest and
promoting apoptosis, thereby clarifying the underlying mechanism of
PD-1 antibody action on EC cells.
Combined anti-CD20 and PD-1 antibodies can
effectively inhibit tumor progression through diverse anti-tumor
mechanisms. Two Phase II studies demonstrated that the combination
of Pembrolizumab and Rituximab effectively blocked PD-1 signaling
in patients with relapsed or refractory follicular lymphoma,
achieving an objective response rate of 67%. This finding suggests
that the combination of anti-CD20 antibodies and PD-1 antibodies
exhibits synergistic anticancer effects (30). Additionally, certain studies have
indicated that incorporating PD-1 antibodies into anti-CD20
antibody regimens may counteract the poor prognosis associated with
aberrant activation of the PD-1/PD-L1 pathway (31). Furthermore, the present study
revealed that the proportion of apoptotic cells in the combination
group was significantly higher than that in the single-agent group,
accompanied by an increased proportion of cells in the S and G2/M
phases, indicating a synergistic apoptosis-inducing effect of the
two antibodies. However, the underlying mechanism of interaction
remains elusive. It may be hypothesized that the anti-CD20 antibody
improves the tumor immune microenvironment by regulating B cells,
thereby enhancing the T-cell activating effect of the PD-1
antibody; further investigation is therefore warranted.
Regarding advantages and limitations, the present
study reports the mRNA expression levels of MS4A1 and PDCD1;
however, the protein expression levels have not yet been verified.
The effects of anti-CD20 and PD-1 antibodies on the proliferation,
apoptosis and cell cycle of EC cells were only demonstrated in
vitro, but no in vivo experiments and no clinical
experiments were performed. Meanwhile, the absence of immune cells
in cell culture limits the interpretation of ADCC/CDC mechanisms;
such mechanisms cannot be inferred without immune cells.
In conclusion, the present in vitro results
demonstrate that combined treatment with anti-CD20 and PD-1
antibodies effectively suppresses EC-cell proliferation and
markedly promotes apoptosis, providing preliminary experimental
evidence supporting further mechanistic and in vivo
validation.
Acknowledgements
Not applicable.
Funding
This project was supported by the National Natural Science
Foundation of China (grant no. 82160443), the Guangxi Natural
Science Foundation (grant no. 2020GXNSFAA159023), the independent
research project of the Regional Key Laboratory of Early Prevention
and Treatment of High-incidence Tumors in 2021 (grant no. GKE-ZZ
202147), the 18th batch of Guangxi ‘New Century Ten Hundred
Thousand Talents Project’ second-level candidate special fund
(grant no. 2015226) and the Guangxi Medical High-level Backbone
Talent Training ‘139’ Plan special fund (grant no. G201903032).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
JS and HW designed the research. YY and JD collected
and analyzed the data. MF, QH and BL collected and analyzed the
data and supervised the study. JS drafted the article and HW edited
it. JS and HW confirm the authenticity of all the raw data. All
authors read and approved the final version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Sorosky JI: Endometrial cancer. Obstet
Gynecol. 120:383–397. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Makker V, MacKay H, Ray-Coquard I, Levine
DA, Westin SN, Aoki D and Oaknin A: Endometrial cancer. Nat Rev Dis
Primers. 7:882021. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Francisco LM, Sage PT and Sharpe AH: The
PD-1 pathway in tolerance and autoimmunity. Immunol Rev.
236:219–242. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
He X and Xu C: Immune checkpoint signaling
and cancer immunotherapy. Cell Res. 30:660–669. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kurachi M: CD8+ T cell exhaustion. Semin
Immunopathol. 41:327–337. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mittica G, Ghisoni E, Giannone G, Aglietta
M, Genta S and Valabrega G: Checkpoint inhibitors in endometrial
cancer: Preclinical rationale and clinical activity. Oncotarget.
8:90532–90544. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Casadesús AV, Cruz BM, Díaz W, González
MÁ, Gómez T, Fernández B, González A, Ledón N, Sosa K, Castro K, et
al: Potent immunomodulatory and antitumor effect of
anti-CD20-IL2no-alpha tri-functional immunocytokine for cancer
therapy. Front Immunol. 13:10218282022. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hamed MM, Gouida MS, Abd El-Aziz SR and
El-Sokkary AMA: Evaluation PD-L1, CD8 and CD20 as early predictor
and tracking markers for breast cancer (BC) in Egypt. Heliyon.
8:e094742022. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Su J, Li Z, Wang J, Liu N, Bao L, Du J, Li
Y, Yu Y and Wang H: The causal relationship between anti-CD20
antibodies and endometrial cancer: A Mendelian randomization study.
Discov Oncol. 15:6132024. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Markowska A, Pawałowska M, Lubin J and
Markowska J: Signalling pathways in endometrial cancer. Contemp
Oncol (Pozn). 18:143–148. 2014.PubMed/NCBI
|
|
11
|
Cragg MS, Walshe CA, Ivanov AO and Glennie
MJ: The biology of CD20 and its potential as a target for mAb
therapy. Curr Dir Autoimmun. 8:140–174. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kumar A, Planchais C, Fronzes R, Mouquet H
and Reyes N: Binding mechanisms of therapeutic antibodies to human
CD20. Science. 369:793–799. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Moreno Torres I and García-Merino A:
Anti-CD20 monoclonal antibodies in multiple sclerosis. Expert Rev
Neurother. 17:359–371. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Schlaak M, Schmidt P and Bangard C,
Schlaak M, Schmidt P and Bangard C: Regression of metastatic
melanoma in a patient by antibody targeting of cancer stem cells.
Oncotarget. 3:22–30. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Smith MR: Rituximab (monoclonal anti-CD20
antibody): Mechanisms of action and resistance. Oncogene.
22:7359–7368. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Dieu-Nosjean MC, Goc J, Giraldo NA,
Sautès-Fridman C and Fridman WH: Tertiary lymphoid structures in
cancer and beyond. Trends Immunol. 35:571–580. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Qin M, Hamanishi J, Ukita M, Yamanoi K,
Takamatsu S, Abiko K, Murakami R, Miyamoto T, Suzuki H, Ueda A, et
al: Tertiary lymphoid structures are associated with favorable
survival outcomes in patients with endometrial cancer. Cancer
Immunol Immunother. 71:1431–1442. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Shimizu Y, Suzuki S, Ukai M, Hattori S,
Yoshikawa N and Kajiyama H: The prognostic significance of
peritumoral lymphocytes' Band-like structure in Type II endometrial
cancer. Anticancer Res. 41:249–258. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Jia HQ, Zhang SP, Chen Y, Qiao YH, Yao YF,
Zhang XY, Wu SY, Song YL and Xing XM: Characteristics and
significance of tertiary lymphoid structures based on molecular
subtypes in endometrial cancer. Int J Gynecol Pathol. 43:595–604.
2024. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Guo YE, Liu Y, Zhang W, Luo H, Shu P, Chen
G and Li Y: The clinicopathological characteristics, prognosis and
immune microenvironment mapping in MSI-H/MMR-D endometrial
carcinomas. Discov Oncol. 13:122022. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Rozali EN, Hato SV, Robinson BW, Lake RA
and Lesterhuis WJ: Programmed death ligand 2 in cancer-induced
immune suppression. Clin Dev Immunol. 2012:6563402012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Chen J, Jiang CC, Jin L and Zhang XD:
Regulation of PD-L1: A novel role of pro-survival signalling in
cancer. Ann Oncol. 27:409–416. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Liu CQ, Xu J, Zhou ZG, Jin LL, Yu XJ, Xiao
G, Lin J, Zhuang SM, Zhang YJ and Zheng L: Expression patterns of
programmed death ligand 1 correlate with different
microenvironments and patient prognosis in hepatocellular
carcinoma. Br J Cancer. 119:80–88. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Drakes ML, Mehrotra S, Aldulescu M, Potkul
RK, Liu Y, Grisoli A, Joyce C, O'Brien TE, Stack MS and Stiff PJ:
Stratification of ovarian tumor pathology by expression of
programmed cell death-1 (PD-1) and PD-ligand-1 (PD-L1) in ovarian
cancer. J Ovarian Res. 11:432018. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lin X, Kang K, Chen P, Zeng Z, Li G, Xiong
W, Yi M and Xiang B: Regulatory mechanisms of PD-1/PD-L1 in
cancers. Mol Cancer. 23:1082024. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Janjigian YY, Shitara K, Moehler M,
Garrido M, Salman P, Shen L, Wyrwicz L, Yamaguchi K, Skoczylas T,
Campos Bragagnoli A, et al: First-line nivolumab plus chemotherapy
versus chemotherapy alone for advanced gastric, gastro-oesophageal
junction, and oesophageal adenocarcinoma (CheckMate 649): A
randomised, open-label, phase 3 trial. Lancet. 398:27–40. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Gandhi L, Rodríguez-Abreu D, Gadgeel S,
Esteban E, Felip E, De Angelis F, Domine M, Clingan P, Hochmair MJ,
Powell SF, et al: Pembrolizumab plus chemotherapy in metastatic
Non-Small-cell lung cancer. N Engl J Med. 378:2078–2092. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Eggermont AMM, Blank CU, Mandala M, Long
GV, Atkinson V, Dalle S, Haydon A, Lichinitser M, Khattak A,
Carlino MS, et al: Adjuvant pembrolizumab versus placebo in
resected stage III melanoma. N Engl J Med. 378:1789–1801. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Eskander RN, Sill MW, Beffa L, Moore RG,
Hope JM, Musa FB, Mannel R, Shahin MS, Cantuaria GH, Girda E, et
al: Pembrolizumab plus chemotherapy in advanced endometrial cancer.
N Engl J Med. 388:2159–2170. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Zeng Z, Yang A, Yang J, Zhang S, Xing Z,
Wang X, Mei W, Jiang C, Lin J, Wu X, et al: Sintilimab (anti-PD-1
antibody) combined with high-dose methotrexate, temozolomide, and
rituximab (anti-CD20 antibody) in primary central nervous system
lymphoma: A phase 2 study. Signal Transduct Target Ther. 9:2292024.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Cho H, Kim SH, Kim SJ, Chang JH, Yang WI,
Suh CO, Kim YR, Jang JE, Cheong JW, Min YH and Kim JS: Programmed
cell death 1 expression is associated with inferior survival in
patients with primary central nervous system lymphoma. Oncotarget.
8:87317–87328. 2017. View Article : Google Scholar : PubMed/NCBI
|