Introduction
Gastrointestinal cancers (GICs), including
colorectal cancer (CRC), gastric cancer (GC) and esophageal cancer
(EC), are among the most common malignancies worldwide. CRC is the
third most commonly diagnosed cancer and the second leading cause
of cancer-related death, whereas GC remains one of the leading
causes of cancer-related death (1).
Despite advances in diagnostic and therapeutic strategies, radical
resection remains the cornerstone of treatment for numerous
patients with GIC (2,3). However, postoperative outcomes remain
unsatisfactory, and only ~50% of patients survive >5 years after
surgery (4,5). Therefore, identifying sensitive and
clinically accessible prognostic biomarkers is essential for
improving risk stratification, guiding clinical decision-making,
enabling prompt interventions, and consequently improving the
survival and quality of life of patients with GIC.
Lactate dehydrogenase (LDH) is a widely used and
inexpensive laboratory marker in clinical practice. As a key enzyme
in glycolysis, LDH catalyzes the conversion of pyruvate to lactate
under anaerobic conditions. Its expression is regulated by multiple
factors, including MYC-related oncogenic signaling, hypoxia within
the tumor microenvironment and cellular necrosis (6,7).
Elevated LDH levels may reflect tumor burden, proliferation,
invasiveness and tissue damage. LDH has been identified as a
notable prognostic biomarker in several malignancies, including CRC
and other GICs (8,9).
Serum albumin is another routinely measured clinical
marker that reflects nutritional status and systemic inflammation.
Decreased albumin levels have been associated with a poor prognosis
in patients with EC, GC and CRC (10,11).
Therefore, the LDH-to-albumin ratio (LAR), which integrates
information on tumor metabolism, inflammation and nutritional
status, may provide more comprehensive prognostic information than
either marker alone. However, the prognostic value of LAR in GICs
remains controversial, and to the best of our knowledge, no
previous evidence-based study has systematically evaluated its
clinical significance. Therefore, the present meta-analysis aimed
to synthesize evidence and clarify the prognostic role of
preoperative LAR in patients with GICs. To the best of our
knowledge, the present study is the first meta-analysis to
comprehensively assess the value of LAR in predicting survival
outcomes and postoperative complications in this patient
population.
Materials and methods
Search strategy
On March 20, 2025, a systematic electronic
literature search was performed in PubMed (https://pubmed.ncbi.nlm.nih.gov/), Embase (https://www.embase.com/) and the Cochrane Library
(https://www.cochrane.org/). The search
strategy included relevant terms such as ‘lactate
dehydrogenase-to-albumin ratio’ and ‘lactate dehydrogenase-albumin
ratio’ to identify eligible studies. Only human studies published
in English were considered. The detailed search strategy is
provided in Table SI.
Inclusion and exclusion criteria
Studies were eligible for inclusion if they met the
following criteria: i) Enrolled patients with a confirmed diagnosis
of GIC; ii) evaluated the prognostic significance of baseline or
preoperative LAR; and iii) reported at least one relevant clinical
endpoint, including overall survival (OS), recurrence-free survival
(RFS) or major postoperative complications. The exclusion criteria
were as follows: i) Animal studies, reviews, case reports and
conference abstracts; and ii) Studies that did not provide
extractable hazard ratios (HRs) or odd ratios (ORs) for outcome
assessment in either the main text or supplementary materials.
Data extraction and quality
evaluation
Key information was extracted from each included
study, including the first author, publication year, study period,
country, cancer type, treatment strategy, sample size, patient age
and sex, LAR cut-off value and outcome measures. HRs and ORs
derived from multivariable analyses were preferentially extracted
when available. The methodological quality of the included
observational studies was assessed using the Newcastle-Ottawa Scale
(NOS). Studies with NOS scores of ≥6 were considered to be of high
quality.
Statistical methods
Statistical analyses were performed using Stata
version 18.0 (StataCorp LP), and pooled estimates were presented
using forest plots. Between-study heterogeneity was assessed using
Cochran's Q test and the I2 statistic. For all analyses,
pooled estimates were calculated using a DerSimonian-Laird
random-effects model. Potential publication bias was assessed using
Begg's and Egger's tests (12).
Sensitivity analyses were performed by sequentially omitting each
individual study to evaluate the stability of the pooled results
(13). Subgroup analyses were
conducted according to cancer type, country, Cox model type and LAR
cut-off value. P<0.05 was considered to indicate a statistically
significant difference.
Results
Search results and study
characteristics
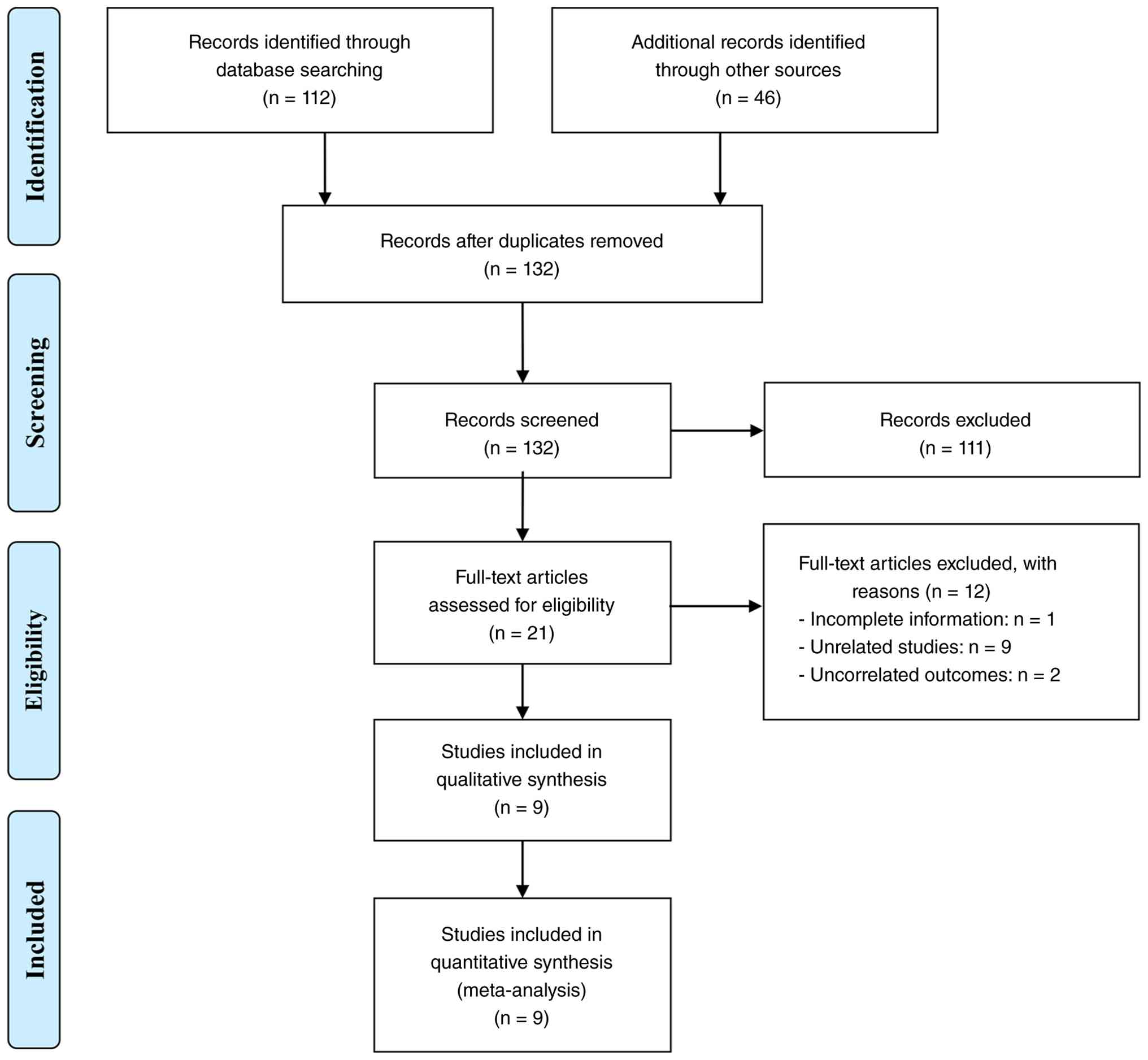
The initial database search, supplemented by manual
screening, identified 158 potentially relevant records. After 26
duplicate records were removed, 111 studies were excluded based on
the screening of titles and abstracts because they did not meet the
inclusion criteria. The full texts of the remaining 21 articles
were assessed, and 12 studies were excluded for not meeting the
predefined eligibility criteria. Finally, nine studies were
included in quantitative analysis (Fig.
1) (14–22).
The main characteristics of the included studies are
summarized in Table I. A total of
6,379 patients were included, with sample sizes ranging from 81 to
3,868. Geographically, five studies were conducted in China, three
in Turkey and one in Japan. All included studies had enrolled
patients who underwent surgery and were retrospective in design.
NOS scores ranged from 6 to 8, indicating generally acceptable
methodological quality (Table
I).
 | Table I.Main characteristics of the studies
included. |
Table I.
Main characteristics of the studies
included.
| Author, year | Sample size | Age, years | Sex, male/female | Cancer type | Treatment | Study period | Country | Cut-point | Cut-off determination
method | NOS | (Refs.) |
|---|
| Shu et al,
2023 | 3,868 | 62.9a | 2,279/1,589 | Colorectal
cancer | Surgery |
01/2011-01/2020 | China | 12.3 | X-tile
software | 8 | (19) |
| Shiratori et
al, 2023 | 236 | 66
(41–83)b | 193/43 | Esophageal
carcinoma | Surgery |
09/2008-03/2020 | Japan | 6.2 | ROC curve
analysis | 8 | (18) |
| Wu et al,
2023 | 382 |
203/179d | 231/151 | Colorectal
cancer | N/A |
10/2015-11/2019 | China | N/A | Continuous
variable; median split | 6 | (21) |
| Çağlar et
al, 2023 | 91 | 63.4±12.1 | 63/28 | Gastric cancer | Surgery | 2016-2020 | Turkey | 5.5 | ROC curve
analysis | 7 | (16) |
| Xie et al,
2022 | 126 | 66 (19–89)c | 66/60 | Colorectal | Surgery cancer |
06/2012-12/2015 | China | 4.9 | ROC curve
analysis | 7 | (20) |
| Aday et al,
2020 (gastric cancer cohort) | 81 | 60.2±13.8 | 55/26 | Gastric cancer | Surgery |
06/2013-06/2019 | Turkey | 5.5 | Time-dependent ROC
analysis | 6 | (15) |
| Aday et al,
2020 (colorectal cancer cohort) | 295 | 55.8±14.1 | 178/117 | Colorectal
cancer | Surgery |
01/2013-06/2019 | Turkey | 5.3 | Time-dependent ROC
analysis | 7 | (14) |
| Feng et al,
2019 | 346 |
147/199d | 270/76 | Esophageal
carcinoma | Surgery |
01/2007-12/2010 | China | 5.5 | X-tile
software | 8 | (17) |
| Hu et al,
2022 | 954 | 58.5±11.9 | 557/397 | Colorectal
cancer | Surgery |
07/2013-09/2017 | China | 4.5 | RCS analysis with
Cox models | 7 | (22) |
Association between preoperative LAR
and OS
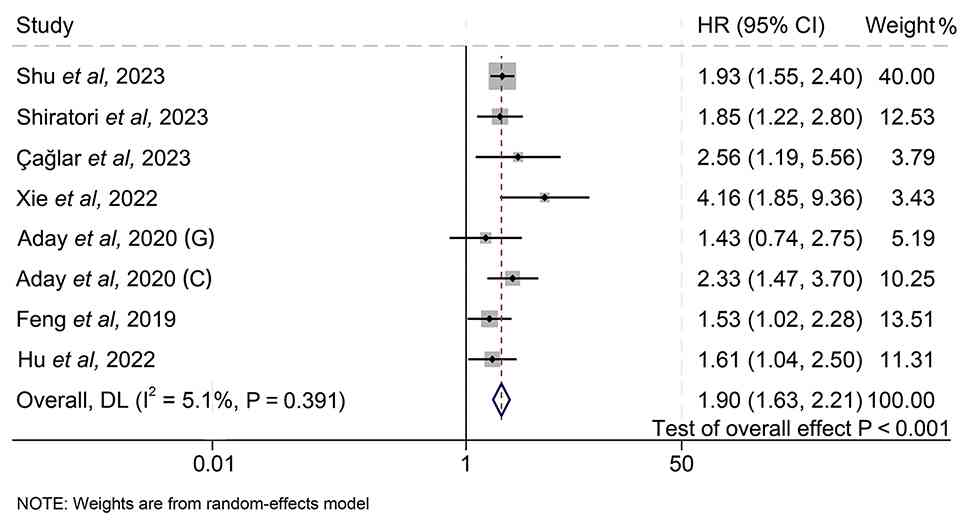
A total of nine independent studies involving 6,379
patients were analyzed to evaluate the association between LAR and
OS in patients with GIC. Among these studies, eight stratified
patients into high- and low-LAR groups. The pooled results
indicated that a higher LAR was significantly associated with worse
OS (HR=1.90; 95% CI, 1.63–2.21; P<0.001; Fig. 2). Similarly, Wu et al
(21) analyzed LAR as a continuous
variable and reported that a higher LAR was associated with worse
OS (HR=1.13; 95% CI, 1.02–1.45; P=0.030).
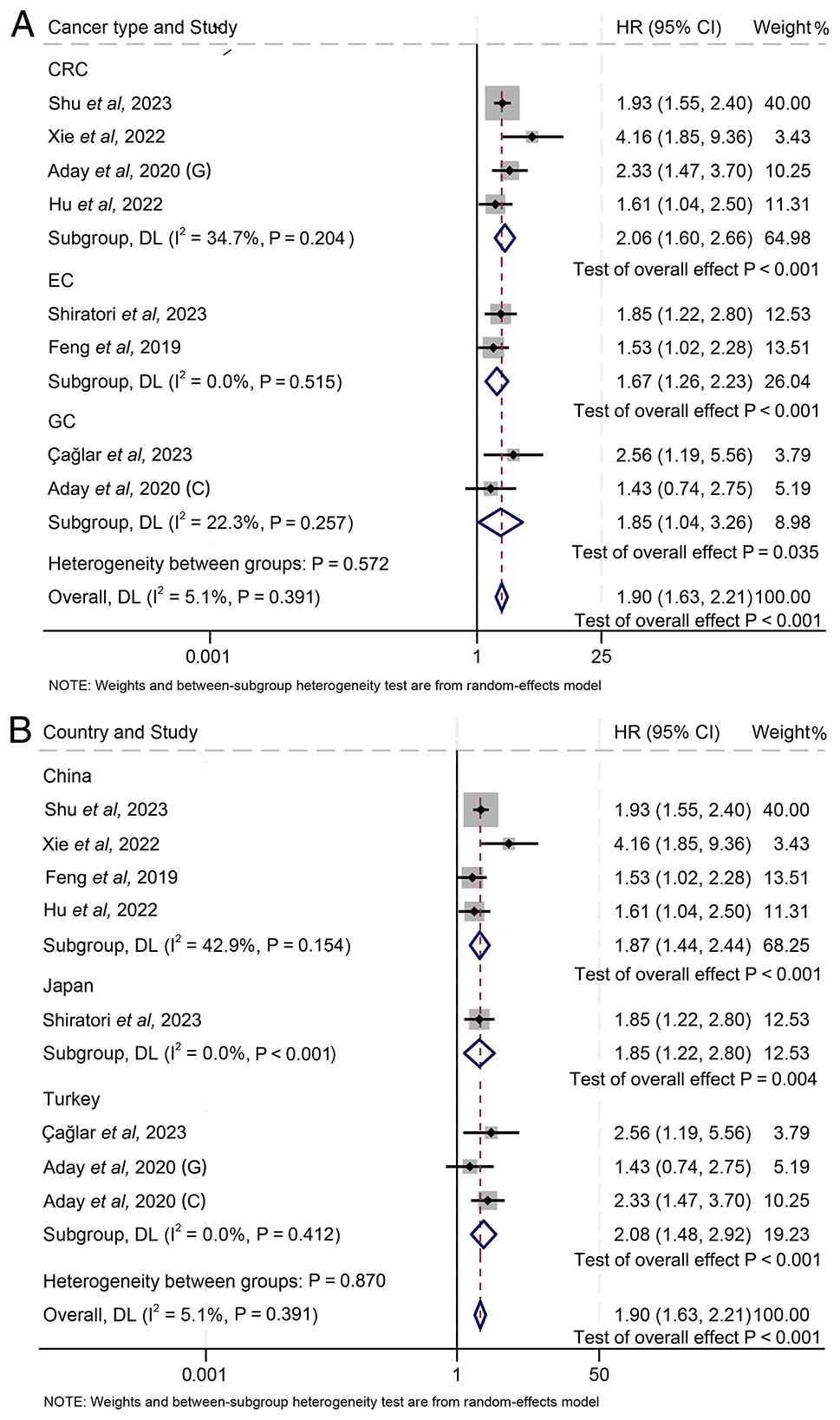
Subgroup analysis revealed that elevated LAR was
consistently associated with unfavorable OS across different cancer
types. Specifically, a higher LAR was associated with worse OS in
patients with CRC (HR=2.06; 95% CI, 1.60–2.66; P<0.001), EC
(HR=1.67; 95% CI, 1.26–2.23; P<0.001) and GC (HR=1.85; 95% CI,
1.04–3.26; P=0.035) (Fig. 3A).
Similar trends were observed in country-based subgroup analysis. A
higher LAR was significantly associated with worse OS in studies
from China (HR=1.87; 95% CI, 1.44–2.44; P<0.001) and Turkey
(HR=2.08; 95% CI, 1.48–2.92; P<0.001) (Fig. 3B). The Japanese subgroup included
only one study and showed that a high LAR was associated with worse
OS (HR=1.85; 95% CI, 1.22–2.80; P=0.004). However, because this
subgroup was based on a single study, the result should be
interpreted with caution.
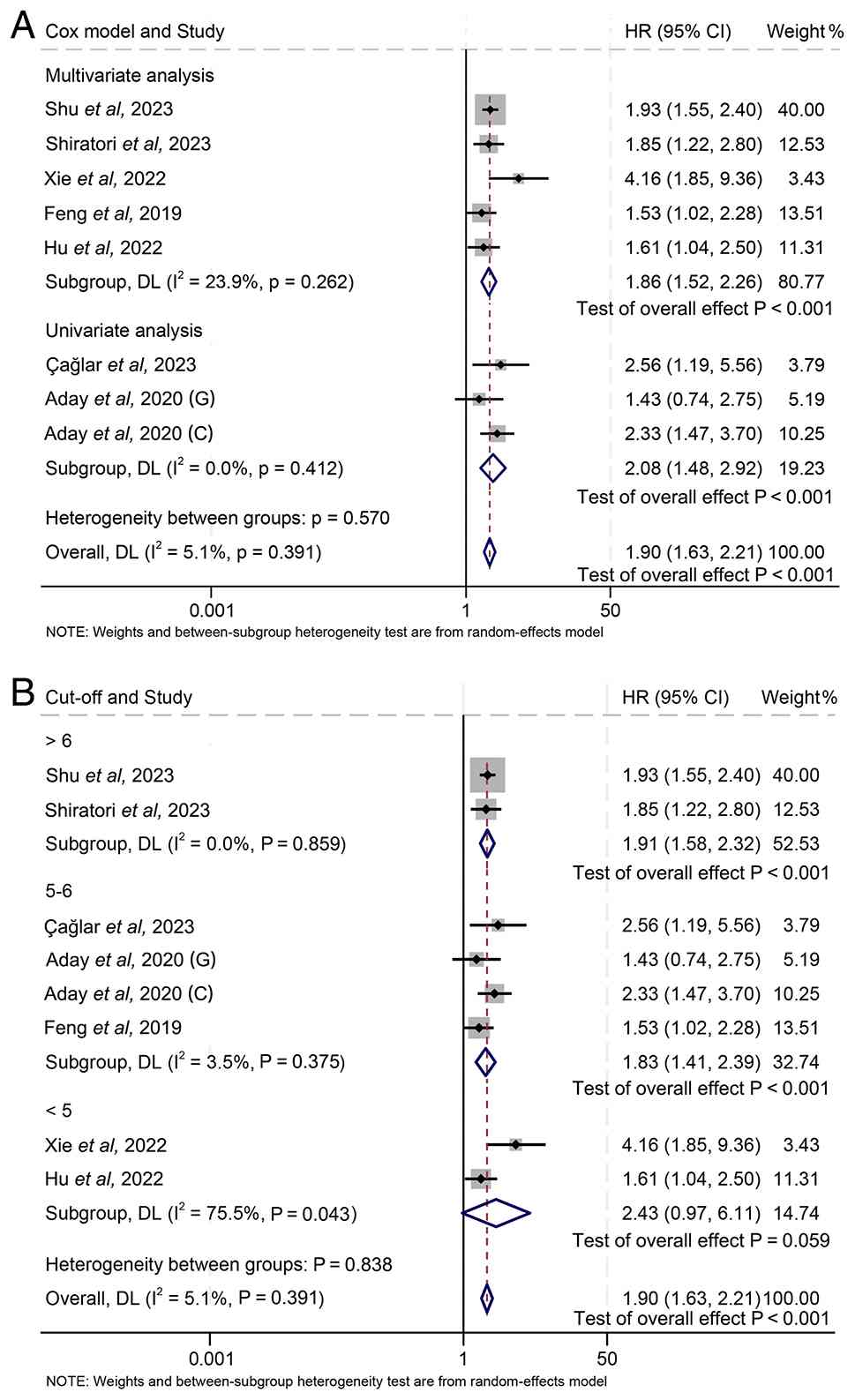
Subgroup analysis based on Cox model type further
supported the stability of the association between LAR and OS
(Fig. 4A). In the multivariate Cox
model subgroup, high LAR was significantly associated with poor OS
(HR=1.86; 95% CI, 1.52–2.26; P<0.001), with low heterogeneity
among studies (I2=23.9%; P=0.262). Similarly, in the
univariate Cox model subgroup, the pooled HR remained significant
(HR=2.08; 95% CI, 1.48–2.92; P<0.001), with no observed
heterogeneity (I2=0.0%; P=0.412). No significant
heterogeneity was observed between the multivariate and univariate
subgroups (P=0.570).
Subgroup analysis according to the LAR cut-off value
also showed broadly consistent results (Fig. 4B). In studies using a cut-off value
>6, high LAR was significantly associated with worse OS
(HR=1.91; 95% CI, 1.58–2.32; P<0.001), with no heterogeneity
(I2=0.0%; P=0.859). In studies using a cut-off value of
5–6, the association remained significant (HR=1.83; 95% CI,
1.41–2.39; P<0.001), with low heterogeneity (I2=3.5%;
P=0.375). In the subgroup with a cut-off value <5, the pooled HR
was 2.43 (95% CI, 0.97–6.11; P=0.059), but substantial
heterogeneity was observed (I2=75.5%; P=0.043), and the
result should therefore be interpreted cautiously.
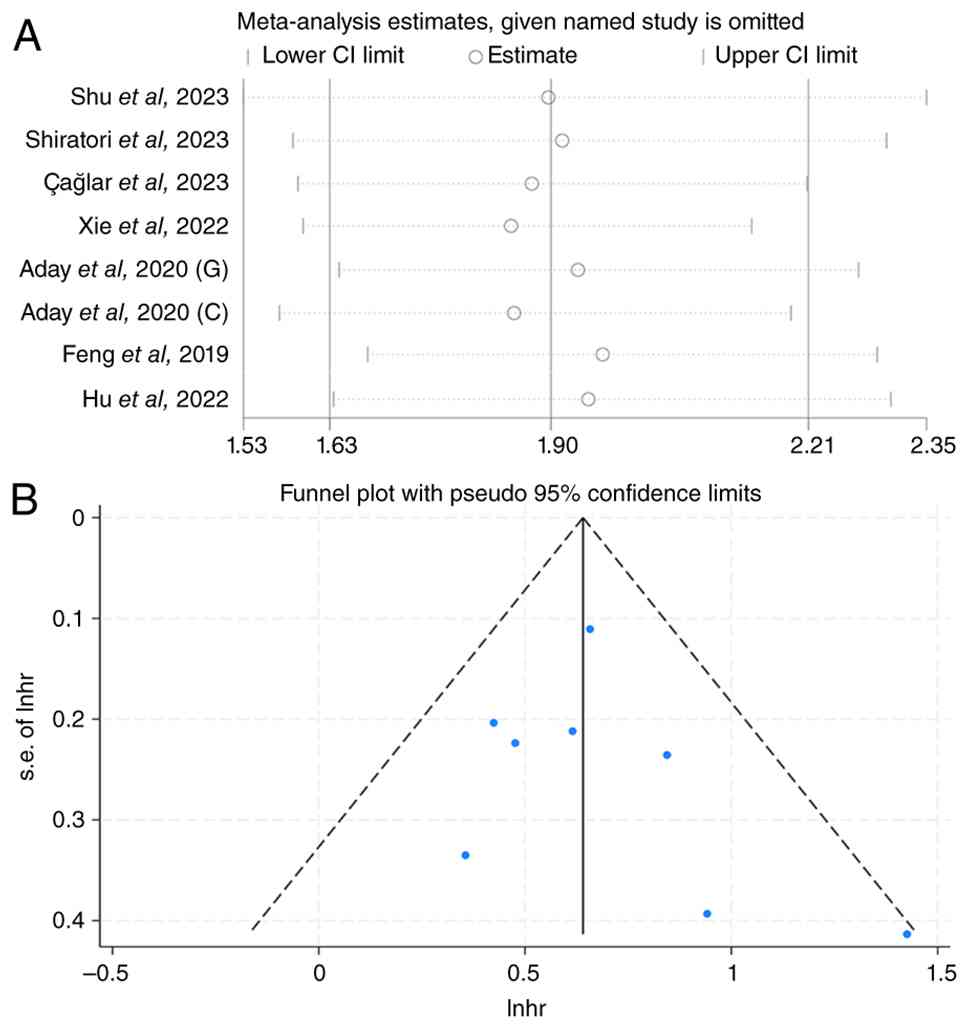
Sensitivity analysis was conducted using a
leave-one-out method to evaluate the robustness of the pooled HR
for OS (Fig. 5A). Specifically,
each included study was sequentially excluded, and the pooled HR
was recalculated after each omission. The overall pooled estimate
was 1.90 (95% CI, 1.63–2.21). After sequential exclusion of
individual studies, the recalculated pooled HRs remained stable,
ranging from 1.85 to 1.96. The lowest pooled estimate was observed
after excluding Xie et al (20) (HR=1.85, 95% CI, 1.60–2.14), whereas
the highest pooled estimate was observed after excluding Feng et
al (17) (HR=1.96; 95% CI,
1.68–2.29). Notably, all recalculated 95% CIs remained above the
null value of 1.0, and the direction and statistical significance
of the association were unchanged (Fig.
5A). These findings indicate that no single study had a
disproportionate influence on the overall result, supporting the
robustness and stability of the pooled estimate. The funnel plot
appeared symmetrical (Fig. 5B), and
Begg's (P=0.266) and Egger's (P=0.482) tests did not suggest
significant publication bias.
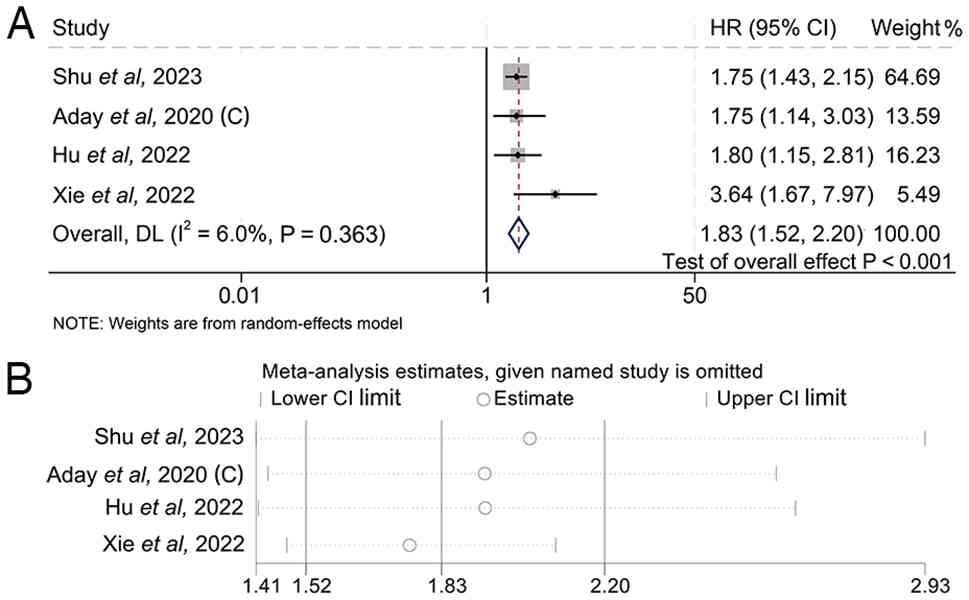
Association between preoperative LAR
and RFS
A total of four studies involving 5,243 patients
evaluated the prognostic significance of LAR for RFS in patients
with GIC. The pooled results indicated that a higher LAR was
significantly associated with worse RFS (HR=1.83; 95% CI,
1.52–2.20; P<0.001; Fig.
6A).
Sensitivity analysis was conducted using a
leave-one-out approach to evaluate the robustness of the pooled HR
for RFS. The overall pooled HR was 1.83 (95% CI, 1.52–2.20). After
sequentially excluding each included study, the recalculated pooled
HRs remained statistically significant and ranged from 1.76 to
2.03, with corresponding 95% CIs ranging from 1.41 to 2.93. The
lowest estimate was obtained after excluding Xie et al
(20) (HR=1.76; 95% CI, 1.48–2.09),
and the highest estimate was obtained after excluding Shu et
al (19) (HR=2.03; 95% CI,
1.41–2.93). Since all recalculated 95% CIs were >1.0 and the
direction of the association remained unchanged, the pooled result
was not driven by any single study and was considered robust
(Fig. 6B).
Begg's (P=0.308) and Egger's (P=0.290) tests did not
indicate significant publication bias; however, these findings
should be interpreted cautiously because only a limited number of
studies were included.
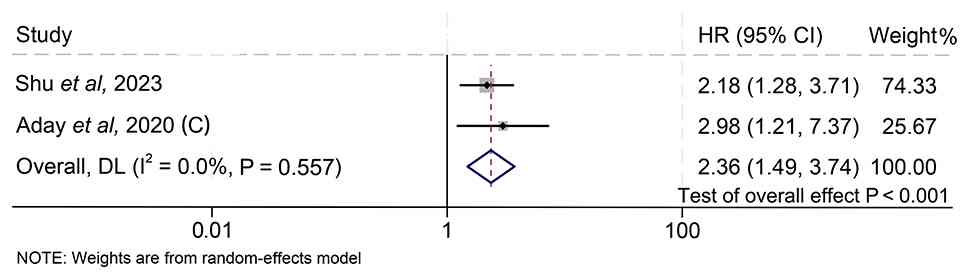
Association between preoperative LAR
and major postoperative complications
A total of two studies involving 4,163 patients were
included to assess the association between LAR and major
postoperative complications. The pooled results indicated that
patients with a higher LAR had a significantly higher risk of major
postoperative complications than those with a lower LAR (OR=2.36;
95% CI, 1.49–3.74; P<0.001; Fig.
7).
Discussion
The present meta-analysis indicated that elevated
preoperative LAR was significantly associated with worse OS, worse
RFS and a higher risk of major postoperative complications in
patients with GIC. These findings suggest that LAR, a low-cost and
readily available biomarker derived from routine preoperative blood
tests, shows clinical value for prognostic assessment and
perioperative risk stratification. Subgroup analyses further
revealed that the association between LAR and prognosis remained
consistent across different cancer types, Cox model types,
countries and LAR cut-off values.
Metabolic reprogramming is a hallmark of tumor
progression (23), and LDH is a key
enzyme involved in glucose metabolism and promotes the conversion
of pyruvate to lactate. Even under normoxic conditions, tumor cells
often heavily rely on glycolysis, leading to increased lactate
production. Lactate accumulation contributes to acidification of
the tumor microenvironment (24),
which may promote tumor invasion, metastasis (25), immune evasion (26) and angiogenesis (27). Therefore, elevated LDH may reflect
aggressive tumor biology and a higher tumor burden. LDH is widely
distributed in multiple tissues, and cellular injury can lead to
its release into the bloodstream. In addition, elevated serum LDH
levels may occur as a result of tumor-associated tissue
destruction, rapid tumor growth, hypoxia or metastasis. Previous
studies have reported that elevated LDH is associated with poor
prognosis in various malignancies, such as renal cell carcinoma and
nasopharyngeal carcinoma (28,29).
Importantly, this association has also been reported in GICs. For
example, elevated pretreatment serum LDH has been associated with
unfavorable survival outcomes in patients with colorectal cancer
and gastric cancer. These findings suggest that LDH is not only a
general marker of tumor burden and aggressive tumor biology, but
may also have prognostic relevance in GICs (30,31).
Serum albumin reflects nutritional status and
systemic inflammation, both of which are closely related to cancer
outcomes. Malnutrition and systemic inflammation can suppress
hepatic albumin synthesis, leading to decreased serum albumin
levels. Albumin-based prognostic markers have been shown to predict
outcomes in multiple cancers. For example, Matsunaga et al
(32) reported that systemic
inflammatory response, together with sarcopenia, was associated
with poor prognosis in patients with esophageal cancer, which is a
type of GIC. Yue et al (33)
also demonstrated that the pretreatment albumin-to-globulin ratio
was a significant prognostic marker in patients with diffuse large
B-cell lymphoma. These findings indicate that albumin-related
markers may reflect both nutritional and inflammatory status.
Importantly, because esophageal cancer is included within GICs, the
relationship between albumin-related prognostic factors and
outcomes has been previously reported in at least one type of
GIC.
Because LDH and albumin may each be affected by
various non-cancer-related conditions, their combined assessment as
LAR may provide a more comprehensive indicator of tumor metabolism,
systemic inflammation and nutritional status. The present findings
support the potential use of LAR as part of routine preoperative
evaluation to improve risk stratification and guide individualized
management.
Several limitations of the present meta-analysis
should be acknowledged. First, all included studies were
retrospective cohort studies, which may have introduced selection
bias and residual confounding. Although a majority of the studies
adjusted for clinicopathological factors, the possibility of
unmeasured confounders cannot be completely excluded. Therefore,
the findings of the present study should be interpreted as
associations rather than evidence of causality. Second, the
geographic distribution of the included studies was relatively
limited. A majority of the studies were conducted in China and
Turkey, and only one study was from Japan. Therefore, the
generalizability of the present findings to other ethnic groups,
healthcare systems and geographic regions remains uncertain.
Further validation in large, multicenter cohorts from different
countries is needed. Third, the LAR cut-off values varied across
the included studies. The original studies used different methods
to determine the optimal LAR threshold, including time-dependent
receiver operating characteristic (ROC) analysis, conventional ROC
analysis, X-tile software, restricted cubic spline analysis and
median-based grouping. This methodological heterogeneity may limit
the direct clinical application of LAR. To address this issue,
subgroup analysis was performed based on LAR cut-off values, and
the association between elevated LAR and poor prognosis remained
stable. However, a standardized and clinically applicable LAR
cut-off value remains to be established. In addition, although
several included studies reported clinicopathological variables,
such as tumor stage and tumor markers (such as carcinoembryonic
antigen), these data were not consistently available and were
reported using heterogeneous definitions and statistical methods.
Therefore, the association between LAR and tumor stage or tumor
markers could not quantitatively assessed. Future studies should
further investigate whether elevated LAR is associated with
advanced tumor stage, increased tumor marker levels and other
aggressive clinicopathological features.
In conclusion, the present meta-analysis indicated
that elevated preoperative LAR is significantly associated with
worse survival outcomes and an increased risk of major
postoperative complications in patients with GICs. As an
inexpensive and easily accessible biomarker, LAR may help
clinicians improve preoperative risk assessment, perioperative
decision-making and postoperative management. Further prospective
multicenter studies are warranted to validate these findings and
establish standardized LAR cut-off values for clinical use.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
YY, LY, KL and TH conceptualized and designed the
study. YY, LY, KL and TH were responsible for data collection,
assembly, analysis and interpretation. Additionally, YY, LY, KL and
TH contributed to manuscript drafting and were actively involved in
its revision. YY and TH confirm the authenticity of all the raw
data. All authors read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Filho AM, Laversanne M, Ferlay J, Colombet
M, Piñeros M, Znaor A, Parkin DM, Soerjomataram I and Bray F: The
GLOBOCAN 2022 cancer estimates: Data sources, methods, and a
snapshot of the cancer burden worldwide. Int J Cancer.
156:1336–1346. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Nordlinger B, Sorbye H, Glimelius B,
Poston GJ, Schlag PM, Rougier P, Bechstein WO, Primrose JN, Walpole
ET, Finch-Jones M, et al: Perioperative FOLFOX4 chemotherapy and
surgery versus surgery alone for resectable liver metastases from
colorectal cancer (EORTC 40983): Long-term results of a randomised,
controlled, phase 3 trial. Lancet Oncol. 14:1208–1215. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zhang L, Zhao K, Kuang T, Wang K, Chai D,
Qiu Z, Liu R, Deng W and Wang W: The prognostic value of the
advanced lung cancer inflammation index in patients with
gastrointestinal malignancy. BMC Cancer. 23:1012023. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tarantino I, Warschkow R, Worni M, Cerny
T, Ulrich A, Schmied BM and Güller U: Prognostic relevance of
palliative primary tumor removal in 37,793 metastatic colorectal
cancer patients: A population-based, propensity score-adjusted
trend analysis. Ann Surg. 262:112–120. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zhang L, Feng J, Kuang T, Chai D, Qiu Z,
Deng W, Dong K, Zhao K and Wang W: Blood biomarkers predict
outcomes in patients with hepatocellular carcinoma treated with
immune checkpoint Inhibitors: A pooled analysis of 44 retrospective
sudies. Int Immunopharmacol. 118:1100192023. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zha X, Wang F, Wang Y, He S, Jing Y, Wu X
and Zhang H: Lactate dehydrogenase B is critical for hyperactive
mTOR-mediated tumorigenesis. Cancer Res. 71:13–18. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Le A, Cooper CR, Gouw AM, Dinavahi R,
Maitra A, Deck LM, Royer RE, Vander Jagt DL, Semenza GL and Dang
CV: Inhibition of lactate dehydrogenase A induces oxidative stress
and inhibits tumor progression. Proc Natl Acad Sci USA.
107:2037–2042. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yu SL, Xu LT, Qi Q, Geng YW, Chen H, Meng
ZQ, Wang P and Chen Z: Serum lactate dehydrogenase predicts
prognosis and correlates with systemic inflammatory response in
patients with advanced pancreatic cancer after gemcitabine-based
chemotherapy. Sci Rep. 7:451942017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wei Y, Xu H, Dai J, Peng J, Wang W, Xia L
and Zhou F: Prognostic significance of serum lactic acid, lactate
dehydrogenase, and albumin levels in patients with metastatic
colorectal cancer. Biomed Res Int. 2018:18040862018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Guo HW, Yuan TZ, Chen JX and Zheng Y:
Prognostic value of pretreatment albumin/globulin ratio in
digestive system cancers: A meta-analysis. PLoS One.
13:e01898392018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Fujii T, Sutoh T, Morita H, Katoh T,
Yajima R, Tsutsumi S, Asao T and Kuwano H: Serum albumin is
superior to prealbumin for predicting short-term recurrence in
patients with operable colorectal cancer. Nutr Cancer.
64:1169–1173. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zhang L, Li X, Wang K, Wu M, Liu W and
Wang W: Prognostic impact of body composition in hepatocellular
carcinoma patients with immunotherapy. Ann Med. 56:23950622024.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhang L, Wang K, Liu R, Kuang T, Chen C,
Yao F and Wang W: Body composition as a prognostic factor in
cholangiocarcinoma: A meta-analysis. Nutr J. 23:1452024. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Aday U, Böyük A and Akkoç H: The
prognostic significance of serum lactate dehydrogenase-to-albumin
ratio in colorectal cancer. Ann Surg Treat Res. 99:161–170. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Aday U, Tatlı F, Akpulat FV, İnan M,
Kafadar MT, Bilge H, Başol Ö and Oğuz A: Prognostic significance of
pretreatment serum lactate dehydrogenase-to-albumin ratio in
gastric cancer. Contemp Oncol (Pozn). 24:145–149. 2020.PubMed/NCBI
|
|
16
|
Çağlar R: The relationship of different
preoperative inflammatory markers with the prognosis of gastric
carcinoma. Asian J Surg. 46:360–365. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Feng JF, Wang L, Yang X and Jiang YH:
Prognostic value of lactate dehydrogenase to albumin ratio (LAR) in
patients with resectable esophageal squamous cell carcinoma. Cancer
Manag Res. 11:7243–7251. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Shiratori F, Suzuki T, Yajima S, Oshima Y,
Nanami T, Funahashi K and Shimada H: Is high score of preoperative
lactate dehydrogenase to albumin ratio predicting poor survivals in
esophageal carcinoma patients? Ann Thorac Cardiovasc Surg.
29:215–222. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Shu XP, Xiang YC, Liu F, Cheng Y, Zhang W
and Peng D: Effect of serum lactate dehydrogenase-to-albumin ratio
(LAR) on the short-term outcomes and long-term prognosis of
colorectal cancer after radical surgery. BMC Cancer. 23:9152023.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Xie Z, Zhou H, Wang L and Wu Y: The
significance of the preoperative lactate dehydrogenase/albumin
ratio in the prognosis of colon cancer: A retrospective study.
PeerJ. 10:e130912022. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Wu J, Wu A, Wang S, Zeng C, Wang R, Zhou J
and Wang D: The value of lactate dehydrogenase to albumin ratio and
immune inflammation biomarkers in colorectal cancer. Front Surg.
10:11184032023. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hu Y, Zhou Y, Cao Y, Wang H, Yang Y, Jiang
R, Gong Q and Zhou Q: Nomograms based on lactate dehydrogenase to
albumin ratio for predicting survival in colorectal cancer. Int J
Med Sci. 19:1003–1012. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Bergers G and Fendt SM: The metabolism of
cancer cells during metastasis. Nat Rev Cancer. 21:162–180. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
de la Cruz-López KG, Castro-Muñoz LJ,
Reyes-Hernández DO, García-Carrancá A and Manzo-Merino J: Lactate
in the regulation of tumor microenvironment and therapeutic
approaches. Front Oncol. 9:11432019. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sun K, Tang S, Hou Y, Xi L, Chen Y, Yin J,
Peng M, Zhao M, Cui X and Liu M: Oxidized ATM-mediated glycolysis
enhancement in breast cancer-associated fibroblasts contributes to
tumor invasion through lactate as metabolic coupling. EBioMedicine.
41:370–383. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Brown TP and Ganapathy V: Lactate/GPR81
signaling and proton motive force in cancer: Role in angiogenesis,
immune escape, nutrition, and Warburg phenomenon. Pharmacol Ther.
206:1074512020. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ding J, Karp JE and Emadi A: Elevated
lactate dehydrogenase (LDH) can be a marker of immune suppression
in cancer: Interplay between hematologic and solid neoplastic
clones and their microenvironments. Cancer Biomark. 19:353–363.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Shen J, Chen Z, Zhuang Q, Fan M, Ding T,
Lu H and He X: Prognostic value of serum lactate dehydrogenase in
renal cell carcinoma: A systematic review and meta-analysis. PLoS
One. 11:e01664822016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wei Z, Zeng X, Xu J, Duan X and Xie Y:
Prognostic value of pretreatment serum levels of lactate
dehydrogenase in nonmetastatic nasopharyngeal carcinoma:
Single-site analysis of 601 patients in a highly endemic area. Onco
Targets Ther. 7:739–749. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Chen J and Zou X: Prognostic significance
of lactate dehydrogenase and its impact on the outcomes of gastric
cancer: A systematic review and meta-analysis. Front Oncol.
13:12474442023. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Li G, Wang Z, Xu J, Wu H, Cai S and He Y:
The prognostic value of lactate dehydrogenase levels in colorectal
cancer: A meta-analysis. BMC Cancer. 16:2492016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Matsunaga T, Miyata H, Sugimura K, Motoori
M, Asukai K, Yanagimoto Y, Takahashi Y, Tomokuni A, Yamamoto K,
Akita H, et al: Prognostic significance of sarcopenia and systemic
inflammatory response in patients with esophageal cancer.
Anticancer Res. 39:449–458. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Yue W, Liu B, Gao L, He M, Wang J, Zhang
W, Chen L, Hu X, Xu L and Yang J: The pretreatment albumin to
globulin ratio as a significant predictor in patients with diffuse
large B cell lymphoma. Clin Chim Acta. 485:316–322. 2018.
View Article : Google Scholar : PubMed/NCBI
|