Introduction
Lymphomas are malignant lymphoproliferative
disorders that can manifest in lymph nodes or extra-nodal sites.
They are broadly categorized as either Hodgkin's lymphoma, arising
from pre-B-cells, or non-Hodgkin's lymphoma (NHL), arising from the
monoclonal development of malignant B- and T-cells (1,2).
Primary lymphoma of bone (PLB), first described in 1928, is a rare
form of extra-nodal NHL, accounting for just 1% of all malignant
lymphomas and 4–5% of primary malignant bone tumors (2,3).
Approximately 80% of PLB cases are the diffuse large B-cell
lymphoma (DLBCL) subtype, which responds well to immunochemotherapy
regimens such as R-CHOP (rituximab, cyclophosphamide, doxorubicin,
vincristine and prednisone) (4).
While PLB is a curable disease, its diagnosis can be
complex (5). Its histopathological
appearance, characterized by sheets of small round cells, can mimic
other primary bone tumors, including Ewing's sarcoma, small cell
osteosarcoma and neuroblastoma (6).
Immunohistochemistry is therefore an indispensable tool for
differentiating these entities and ensuring an accurate diagnosis.
The present case is unique, as it illustrates PLB's diagnostic
challenges and the management of a significant, long-term
complication following standard therapy. While pathological
fractures are known to occur in PLB, this report details a novel
surgical reconstruction for a non-healing fracture post-treatment,
employing a reverse shoulder megaprosthesis with a cryo-treated
autograft to restore function. This combination is rarely, if ever,
used to treat this specific and complex diagnosis.
Case report
A 42-year-old male with no significant past medical
history presented to the Vietnam National Cancer Hospital (Hanoi,
Vietnam) in November 2022 with a 5-month history of persistent pain
in the proximal left humerus. The patient did not report any B
symptoms, such as fever, night sweats or weight loss. Initial
X-rays revealed an aggressive bone lesion in the proximal humerus
with mixed lytic and sclerotic areas, a moth-eaten pattern and a
wide zone of transition. The lesion exhibited cortical destruction
and extended from the humeral head to the middle third of the
humeral shaft, with suspected soft-tissue involvement. An open
biopsy was performed and pathology results confirmed NHL.
The patient was diagnosed with Stage IV NHL of the
left humerus (Ann Arbor staging system) (7). The patient was treated with 6 cycles
of R-CHOP chemotherapy (Rituximab 375 mg/m2 on day 1,
Cyclophosphamide 750 mg/m2 on day 1, Doxorubicin 50
mg/m2 on day 1, Vincristine 1.4 mg/m2 on day
1, Prednisolone 100 mg on day 1–5) from January to August 2023,
followed by 36 Gy of radiotherapy in September and October 2023.
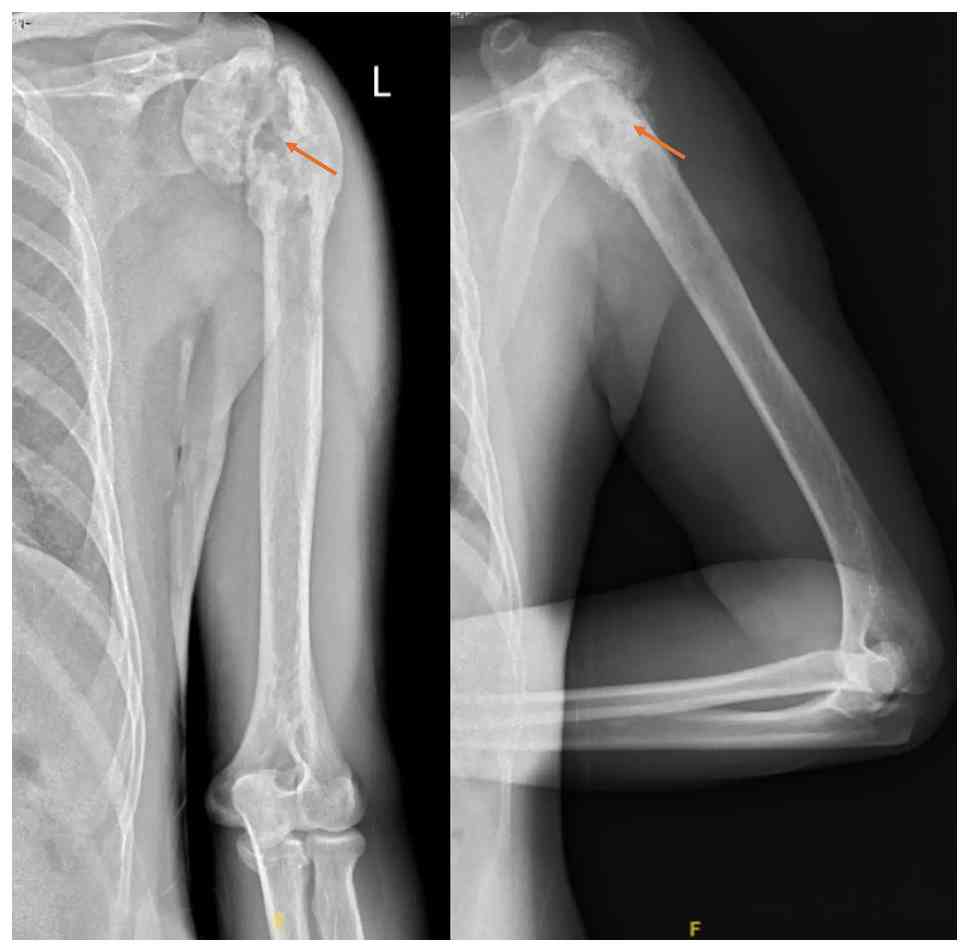
However, follow-up X-rays revealed a pathological fracture at the
anatomical neck of the humerus (Fig.
1). Despite pain resolution following primary treatment,
radiographic assessment consistently demonstrated absence of callus
formation and no progression toward union over a six-month
observation period, leaving the patient with a significant
functional impairment, unable to move his shoulder.
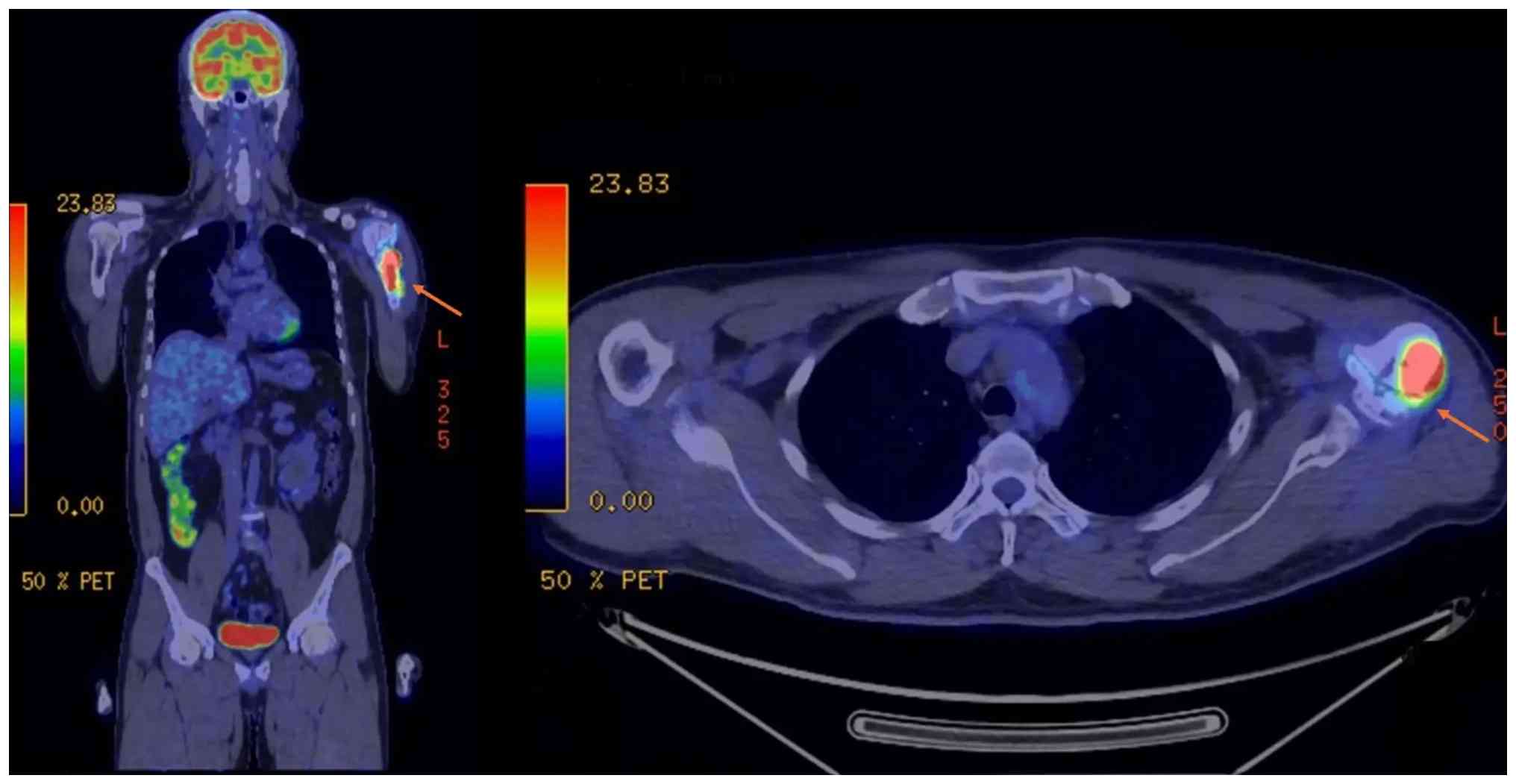
The team conducted a staging workup, including
positron emission tomography (PET)/CT and chest CT. The PET/CT scan
revealed high 18F-fluorodeoxyglucose (FDG) uptake in the
humeral tumor (maximum standardized uptake volume
(SUVmax), 30) (Fig. 2).
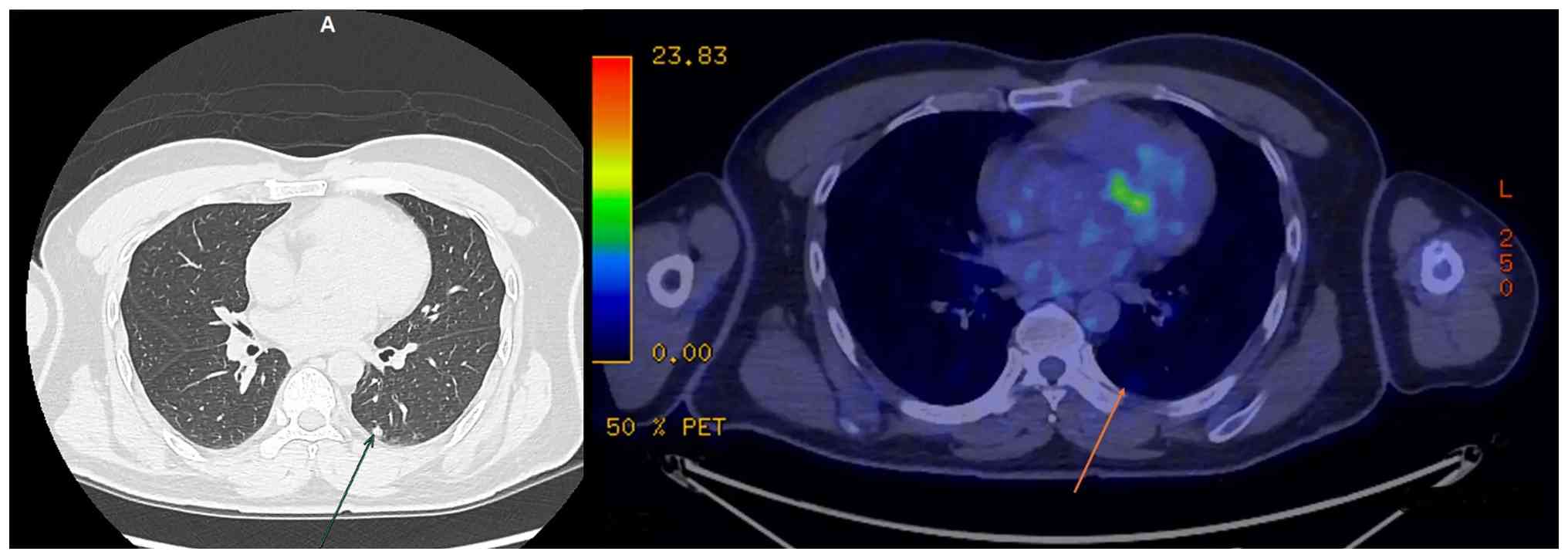
Chest CT showed a new 6.3-mm diameter solid nodule in the left
lower lobe of the lung with mild uptake on PET/CT
(SUVmax 2.2) (Fig. 3).
These results indicated a partial response to chemo-radiotherapy
rather than complete remission. Given its small size, low and
non-specific metabolic activity, and the absence of other
extra-nodal sites of disease, it was most consistent with an
inflammatory or incidental finding rather than a metastatic deposit
or synchronous primary malignancy. The team decided to pursue
active radiologic surveillance rather than immediate biopsy. Serial
chest CT examinations were performed at 3-month intervals over the
1-year follow-up period. The nodule demonstrated no increase in
size or FDG avidity, lending further support to a benign etiology.
No dedicated biopsy was performed, given the nodule's stable
radiologic behavior.
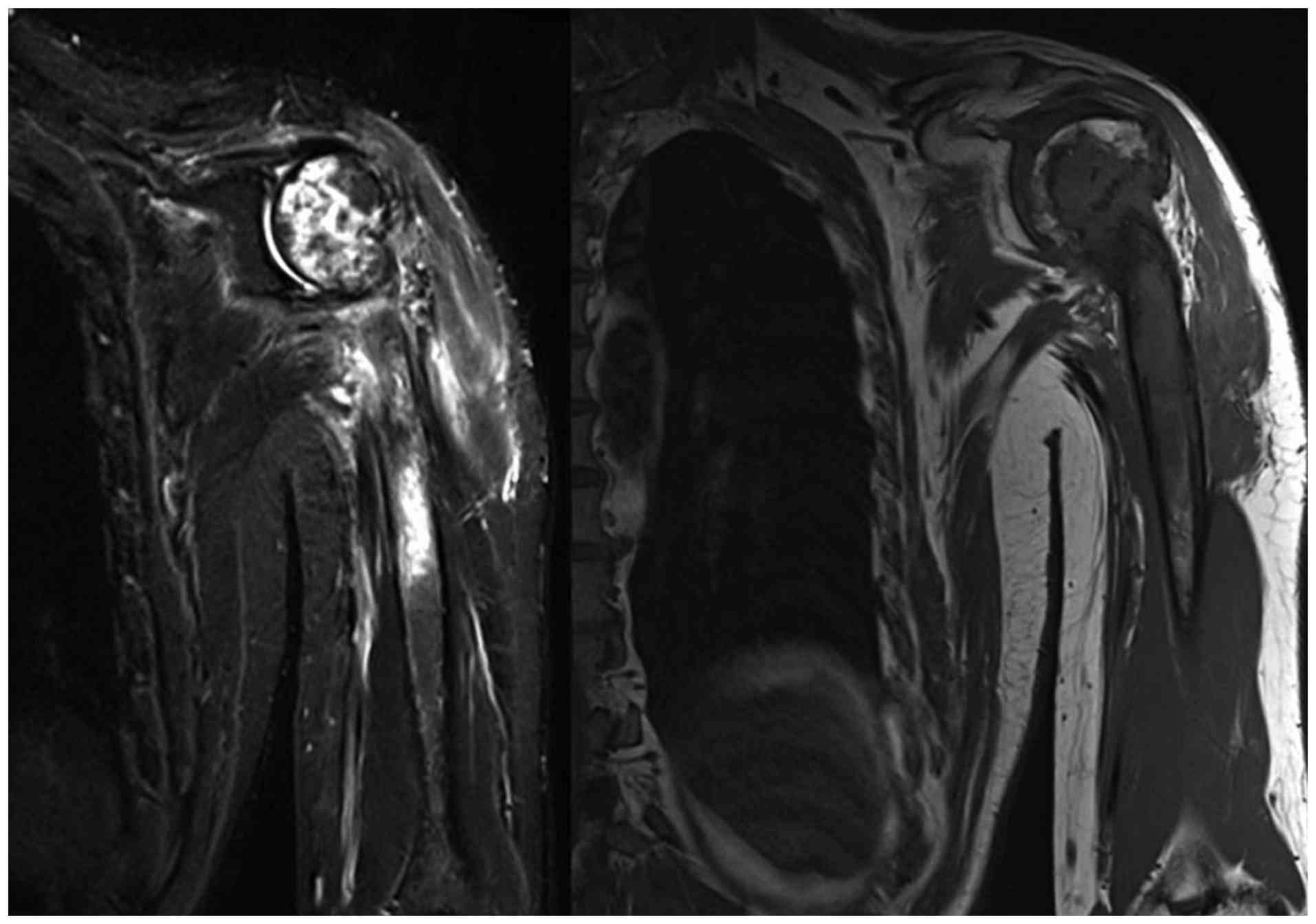
Magnetic resonance imaging (MRI) of the humerus
confirmed an extensively destructive bone lesion ~15 cm in length,
invading surrounding tendons and muscles, but not the neurovascular
bundle (Fig. 4). Taken together,
these findings suggested a case of primary bone lymphoma with a
partial treatment response, which was complicated by a pathological
fracture following radiotherapy. MRI and PET/CT findings were
consistent with residual lymphomatous disease after therapy
completion.
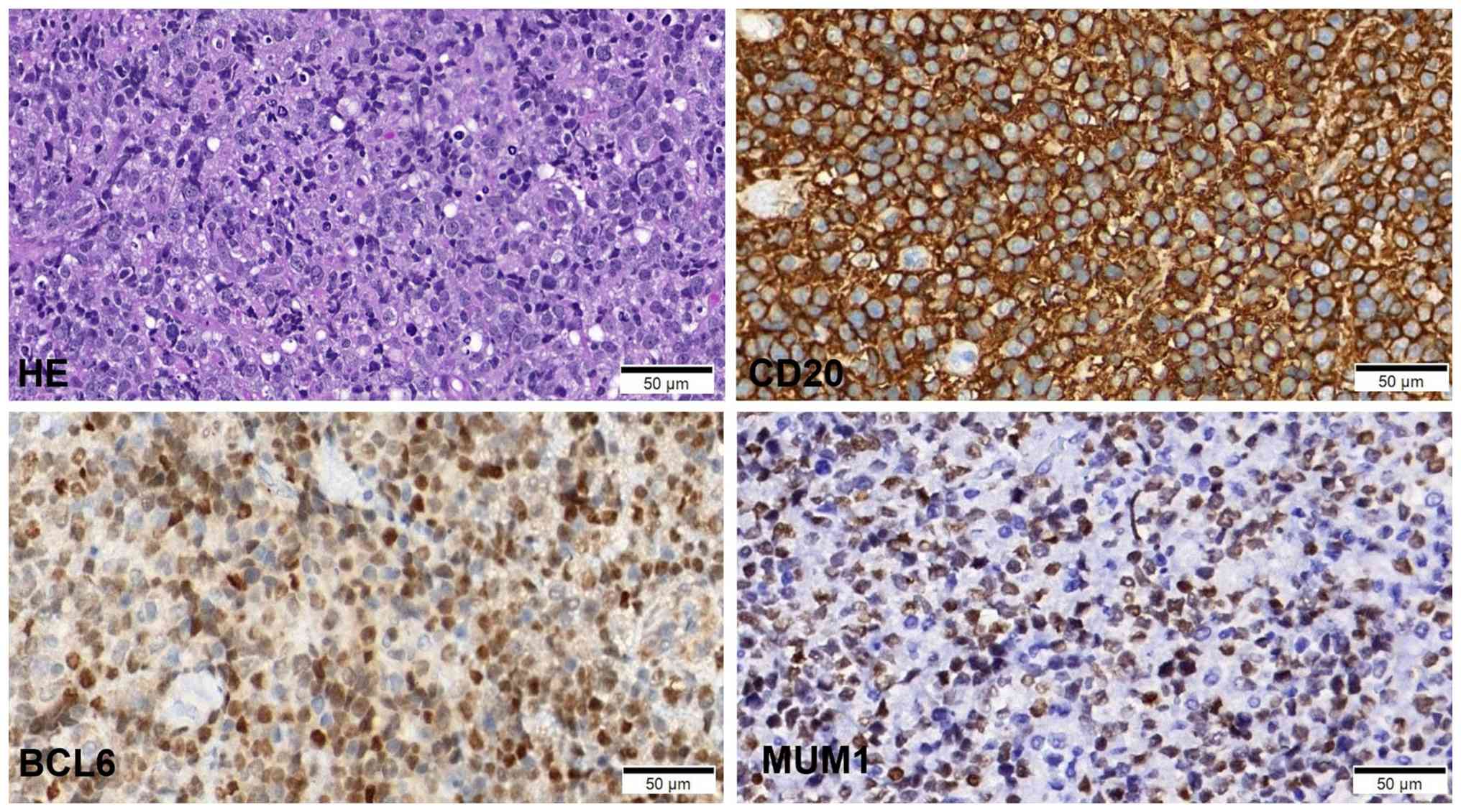
Histopathological examination of the initial biopsy
revealed a diffuse pattern of cells with round nuclei, scant
cytoplasm and frequent mitoses, suggestive of lymphoma. Due to the
rarity of PLB, a differential diagnosis, including Ewing sarcoma
and small cell osteosarcoma, was considered. The diagnosis was
confirmed by immunohistochemical staining, which showed strong CD20
positivity, and positivity for BCL6 (>30%) and multiple myeloma
oncogene 1 (MUM1) (>30%), and a high proliferation index with
Ki67 (>90%). These markers confirmed DLBCL diagnosis,
non-germinal center B-cell type (Fig.
5).
The multidisciplinary tumor board of our hospital
recommended surgery, given the non-healing fracture and persistent
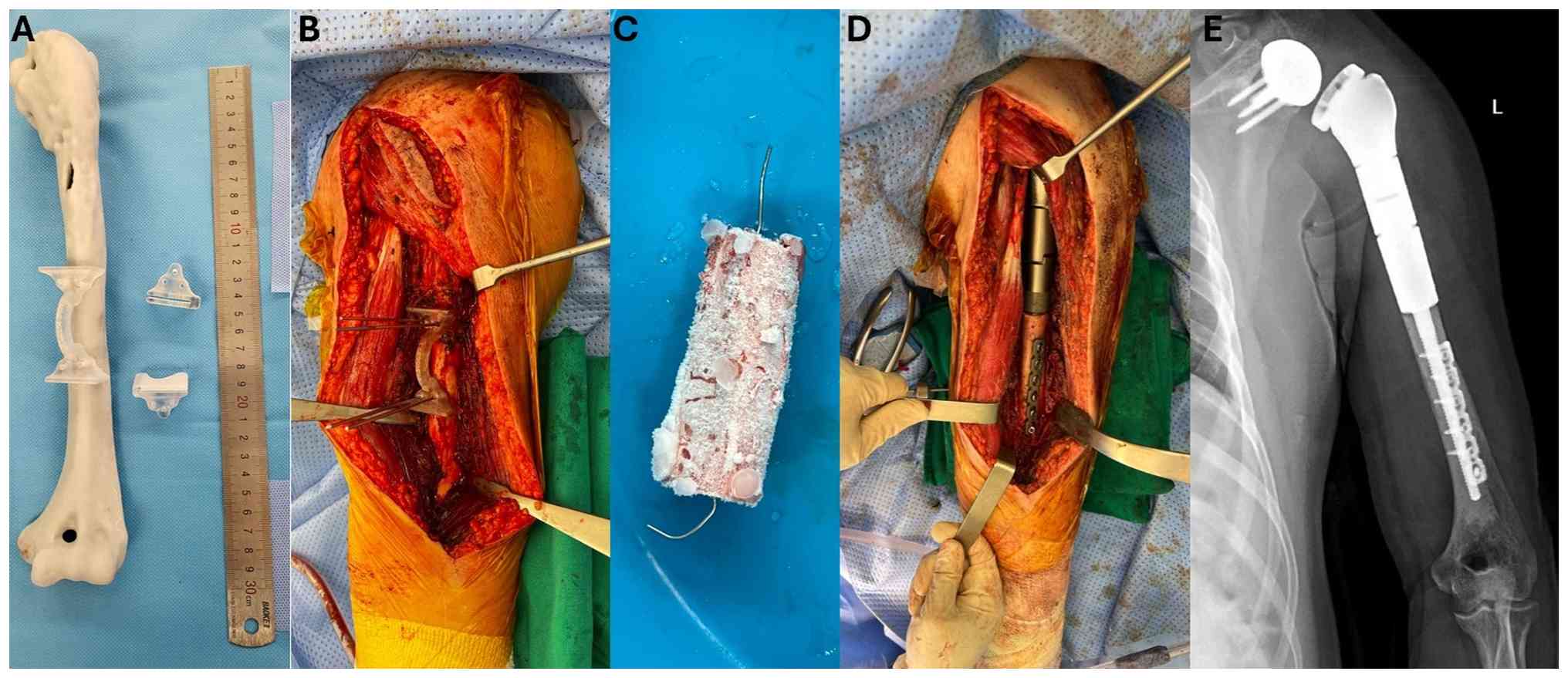
functional deficit post-treatment. Pre-operative planning was
facilitated using a 3-dimensional (3D) printed model of the
patient's proximal humerus, constructed from CT imaging data, to
guide implant selection and simulate the surgical reconstruction
(3D Technology in Medicine Center, College of Health Sciences, Vin
University) (Fig. 6A). The patient
underwent a 20 cm-wide resection of the proximal humerus (Fig. 6B), and a 6-cm segment of the
resected humeral diaphysis was treated with liquid nitrogen to
serve as a devitalized cortical autograft (Fig. 6C). The liquid nitrogen protocol
followed established oncological bone recycling principles: The
bone segment was immersed in liquid nitrogen at −196°C for 20 min,
then allowed to thaw at room temperature for 15 min, followed by
thawing in sterile normal saline for 15 min. This freeze-thaw cycle
ensured complete devitalization of residual tumor cells while
preserving the cortical bone's structural integrity (8).
Reconstruction was performed using a modular reverse
shoulder megaprosthesis (Beijing Chunli Zhengda Medical Instrument
Co., Ltd.) with a 10.5-cm intramedullary stem. The devitalized
autograft was then secured to the prosthetic stem using
polymethylmethacrylate cement and fixed to the remaining humeral
diaphysis using a plate and screws to achieve rotational stability
(Fig. 6D). Soft-tissue
reconstruction was critical to optimize reverse shoulder construct
function. As the rotator cuff tendons had been resected en
bloc with the specimen, the remaining deltoid muscle was
meticulously sutured to pre-designed holes of the humeral
prosthetic component, and the residual musculature was
re-approximated to the autograft using non-absorbable sutures. This
soft-tissue envelope reconstruction was essential for reverse
shoulder megaprosthesis function to provide dynamic stability and
prevent dislocation (9).
Postoperatively, the patient followed a structured
rehabilitation program beginning with passive range-of-motion
exercises at 2 weeks and progressing to active-assisted exercises
at 6 weeks. At the 1-year follow-up, the patient was assessed using
the Musculoskeletal Tumor Society (MSTS) scoring system (10). The preoperative MSTS score was 8/30,
reflecting severe functional impairment, and improved to 22/30 at
the 1-year follow-up. The patient continues to be monitored every 3
months and remains stable with no signs of local recurrence or
distant metastasis on imaging (Fig.
6E).
Discussion
This case is notable for two primary reasons: The
diagnostic challenge presented by a rare tumor and, more
significantly, the management of a severe post-treatment
complication with a novel surgical technique. Primary lymphoma of
bone is rare, predominantly affecting males, with a median
diagnostic age in the 7th decade (11), but the patient of the present study
was considerably younger. While local pain is a common presenting
symptom, pathological fractures occur in a substantial number of
cases (25–30%) and are prognostically significant (12).
Diagnosing PLB can be difficult, as its morphology
overlaps with other round cell tumors. As demonstrated in the
present case, small or decalcified biopsy samples can further
complicate diagnosis. The present findings underscore
immunohistochemistry's pivotal role in reaching a definitive
diagnosis. The sample's strong positivity for B-cell markers CD20
and CD45 (13), along with the
specific profile of BCL6, MUM1 and a high Ki-67 index, was crucial
in confirming DLBCL and excluding mimics like Ewing sarcoma.
The primary PLB management is a combination of
chemotherapy and radiotherapy. Surgery is typically reserved for
obtaining a diagnosis or for managing complications like
pathological fractures. The optimal surgical timing and method for
these fractures are not well-established. Scoccianti et al
(14) documented various
approaches, including conservative management, fixation and
resection, with the timing of surgery varying from pre- to
post-chemotherapy.
In the present case, the decision to perform surgery
after the completion of both chemotherapy and radiotherapy was
based on the patient's specific clinical situation: A non-healing
fracture causing significant functional loss, despite the patient
being pain-free. This aligned with the principle of intervening to
enhance function and quality of life. The present surgical
technique addressed substantial bone loss and soft tissue
involvement, consistent with recommendations to consider wide
excision in such scenarios. Furthermore, complete resection was
supported by evidence suggesting improved survival rates compared
to incomplete resection (15). The
uniqueness of the present surgical approach lies in the combination
of a reverse shoulder arthroplasty with the use of a liquid
nitrogen-treated autograft. This technique aimed to provide
stability and improve shoulder function while preserving the
patient's bone stock, representing an innovative evolution in our
surgical practice for humeral cancers (16). Furthermore, Schmitz et al
(15) reported that survival was
significantly higher in patients who underwent complete resection
compared to those who underwent incomplete resection. This supports
our decision to proceed with wide excision followed by
megaprosthesis replacement.
To contextualize the innovation of the proposed
hybrid approach, it is useful to compare it directly to the
principal alternatives: Structural allograft composite arthroplasty
and megaprosthesis reconstruction alone. Osteoarticular or
intercalary allografts offer biological reconstruction and the
potential for tendon reattachment to host tissue. However, they
have high complication rates, including infection, fracture and
non-union, and carry the additional risk of disease transmission
(17). Furthermore, allografts are
not universally available, particularly in resource-limited
healthcare settings such as Vietnam, where the bone banking
infrastructure remains underdeveloped. Additionally, reconstruction
with megaprosthesis alone, while durable and immediately stable,
sacrifices all residual bone stock. In many cases, this option is
not feasible when there is not enough bone left to attach the
implant stem.
The hybrid technique described in this report
addresses these limitations by combining the immediate mechanical
stability of the modular reverse shoulder prosthesis with the
biological advantages of the patient's own devitalized cortical
bone. The recycled autograft serves as a bridging scaffold that
facilitates soft-tissue attachment, augments the bone-prosthesis
interface and preserves the patient's residual cortical stock-all
without the immunological concerns or availability constraints of
an allograft. This approach represents a pragmatic and reproducible
innovation particularly suited to centers where commercial
allografts are unavailable.
In conclusion, this case of primary diffuse large
B-cell lymphoma of the bone highlights the critical importance of
immunohistochemistry for accurate diagnosis when faced with
histopathological mimics. Additionally, the non-healing
pathological fracture of the present patient required a highly
specialized intervention. This case underscores that PLB treatment
goals should extend beyond oncological control to include limb
function preservation and improved quality of life, necessitating a
creative and individualized multidisciplinary approach.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in this study may be requested
from the corresponding author.
Authors' contributions
DTT and VKN conceived the study and wrote original
manuscript. MQD and THL summarized data, operated on the patient
and confirmed the authenticity of the raw data. TQSN operated on
the patient and contributed to writing the manuscript. VAN reviewed
the results of diagnostic imaging. TTHaT and VCT collected,
validated and interpreted the patient's chemotherapy and
radiotherapy treatment data. TTHiT and TDT followed up and
interpreted the patient's outcome. All of the authors have read and
approved the final manuscript.
Ethics approval and consent to
participate
This study's procedures adhered to the tenets of the
Declaration of Helsinki. Case reports are approved by the Joint
Consultation for Approval of Surgery of Vinmec Times City
International Hospital, Vinmec Healthcare System, 458 Minh Khai,
Vinh Tuy, Hanoi and are exempt from requiring ethical approval at
the Vinmec Healthcare System.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of this case report, including clinical
information and accompanying images.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
PLB
|
primary lymphoma of bone
|
|
DLBCL
|
diffuse large B-cell lymphoma
|
|
MRI
|
magnetic resonance imaging
|
|
CT
|
computed tomography
|
References
|
1
|
Jiang M, Bennani NN and Feldman AL:
Lymphoma classification update: T-cell lymphomas, Hodgkin
lymphomas, and histiocytic/dendritic cell neoplasms. Expert Rev
Hematol. 10:239–249. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Shanbhag S and Ambinder RF: Hodgkin
lymphoma: A review and update on recent progress. CA Cancer J Clin.
68:116–132. 2018.PubMed/NCBI
|
|
3
|
Choi JY, Hahn JS, Suh CO and Yang WI:
Primary lymphoma of bone-Survival and prognosis. Korean J Intern
Med. 17:191–197. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yohannan B and Rios A: Primary diffuse
large B-cell lymphoma of the bone. J Hematol. 12:75–81. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Rezazadeh A, Szabo A, Khurana A, Inwards
DJ, Lunning MA, Bartlett NL, Caimi PF, Rodgers TD, Barr PM,
Chowdhury SM, et al: Outcomes of limited stage primary bone diffuse
large B-cell lymphoma in the rituximab era: A multicenter,
retrospective study. Haematologica. 109:1439–1444. 2024.PubMed/NCBI
|
|
6
|
Kanavos T, Birbas E, Papoudou-Bai A,
Hatzimichael E, Kitsouli A, Karpathiou G and Kanavaros P: Primary
bone lymphoma: A review of the literature with emphasis on
histopathology and histogenesis. Diseases. 11:422023. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Edge SB and Compton CC: The American Joint
Committee on Cancer: the 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Dang QM, Nguyen Tran Quang SQ, Duc TT,
Dung TT, Tran Van C, Le HT, Tran HTT and Van Nguyen K: 128P.
Innovative limb salvage: Liquid nitrogen approach in reconstruction
after bone tumor resection. ESMO Open. (Suppl 2):9:1025172024.
View Article : Google Scholar
|
|
9
|
Cianni L, Capece G, Fiore L, De Fazio A,
Martellini S, Maccauro G and Saccomanno MF: Glenohumeral
instability and clinical outcomes following proximal humerus
resection and megaprosthesis implantation: A systematic review. J
Clin Med. 14:78502025. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Rizzo A, Paderno M, Saccomanno MF, Milano
F and Milano G: The Musculoskeletal Tumor Society Scoring system is
a valid subjective and objective tool to evaluate outcomes of
surgical treatment of patients affected by upper and lower
extremity tumors. Musculoskelet Surg. 108:201–214. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Benkhadra R, Auster M, Nayfeh T, Abbas AS,
Alsibai R, Benkhadra K, Datta P and Kaur S: Systematic review
determining the characteristics of primary bone lymphoma. J Clin
Oncol. 41 (Suppl 16):e195432023. View Article : Google Scholar
|
|
12
|
Cai L, Stauder MC, Zhang YJ, Poortmans P,
Li YX, Constantinou N, Thariat J, Kadish SP, Nguyen TD, Kirova YM,
et al: Early-stage primary bone lymphoma: A retrospective,
multicenter Rare cancer network (RCN) study. Int J Radiat Oncol
Biol Phys. 83:284–291. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chisholm KM, Ohgami RS, Tan B, Hasserjian
RP and Weinberg OK: Primary lymphoma of bone in the pediatric and
young adult population. Hum Pathol. 60:1–10. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Scoccianti G, Rigacci L, Puccini B,
Campanacci DA, Simontacchi G, Bosi A and Capanna R: Primary
lymphoma of bone: Outcome and role of surgery. Int Orthop.
37:2437–2442. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Schmitz C, Rekowski J, Müller SP,
Farsijani N, Hertenstein B, Franzius C, von Verschuer U, La Rosée
P, Freesmeyer M, Wilop S, et al: Impact of complete surgical
resection on outcome in aggressive non-Hodgkin lymphoma treated
with immunochemotherapy. Cancer Med. 9:8386–8396. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tran DT, Tran TD, Nguyen SB, Nguyen SQT,
Dang QM and Tran CV: Combination of reverse shoulder prosthesis,
elbow prosthesis, and polyetheretherketone: A modified total
humeral replacement for osteosarcoma humerus treatment. Case Rep
Oncol. 15:12–20. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wisanuyotin T, Paholpak P, Sirichativapee
W and Kosuwon W: Allograft versus autograft for reconstruction
after resection of primary bone tumors: A comparative study of
long-term clinical outcomes and risk factors for failure of
reconstruction. Sci Rep. 12:143462022. View Article : Google Scholar : PubMed/NCBI
|