Introduction
Salivary duct carcinoma (SDC) is one of the most
aggressive carcinomas of the salivary gland owing to frequent local
recurrence and distant metastases (1). This type of carcinoma typically
resembles mammary ductal carcinoma, with an apocrine phenotype
(1). SDC comprises 5–10% of all
salivary gland malignancies. This aggressive carcinoma commonly
affects middle-aged or elderly individuals, with typical sites
including the major salivary glands, particularly the parotid
glands (1). Histopathologically,
SDC is characterised by the solid, cribriform and/or papillary
proliferation of carcinoma cells with a rich eosinophilic
cytoplasm, large pleomorphic nuclei and prominent nucleoli
(1). Preexisting pleomorphic
adenomas (PAs) may also be present (1). Immunohistochemically, SDC frequently
exhibits positive immunoreactivity for the androgen receptor (AR),
which indicates an apocrine phenotype. HER2 upregulation has also
been noted in an estimated one-third of cases (1).
Heterotopic ossification (HO) is defined as the
formation of mature bone tissue in non-skeletal tissues (2,3).
Intra- or peri-tumoural HO has been reported in a number of benign
and malignant neoplasms (3–8). The prevalent histological type
accompanying HO is papillary thyroid carcinoma and its presence has
also been described in melanocytic naevi (the skin condition
Osteonevus of Nanta), a number of pancreatic neoplasms and
colorectal tumours (3–8). Although markedly rare, HO has been
reported to occur in benign and malignant salivary gland neoplasms
[including mucoepidermoid carcinoma (MEC) (9–11),
carcinoma ex pleomorphic adenoma (CXPA) (12–14)
and PA (15–25)]. However, to the best of our
knowledge, the occurrence of HO in SDC has not yet been reported in
the English literature. Therefore the present report describes the
first reported case of SDC with HO in the parotid gland and reviews
the clinicopathological features of salivary gland neoplasms with
HO.
Case report
A 38-year-old Japanese male initially experienced
left-sided facial pain during mastication in January 2018. The
patient developed a mass in the left parotid region and, 2 months
later, left-sided facial paralysis and trismus in April 2018. Based
on the results of the physical examination and magnetic resonance
imaging at the medical institution that he first visited, the
patient was suspected of having left parotid gland carcinoma, given
that a tender mass was present in the parotid gland and the patient
developed facial paralysis. The patient was then referred to the
Department of Otolaryngology and Head and Neck Surgery, Osaka
Medical and Pharmaceutical University Hospital (Takatsuki, Japan)
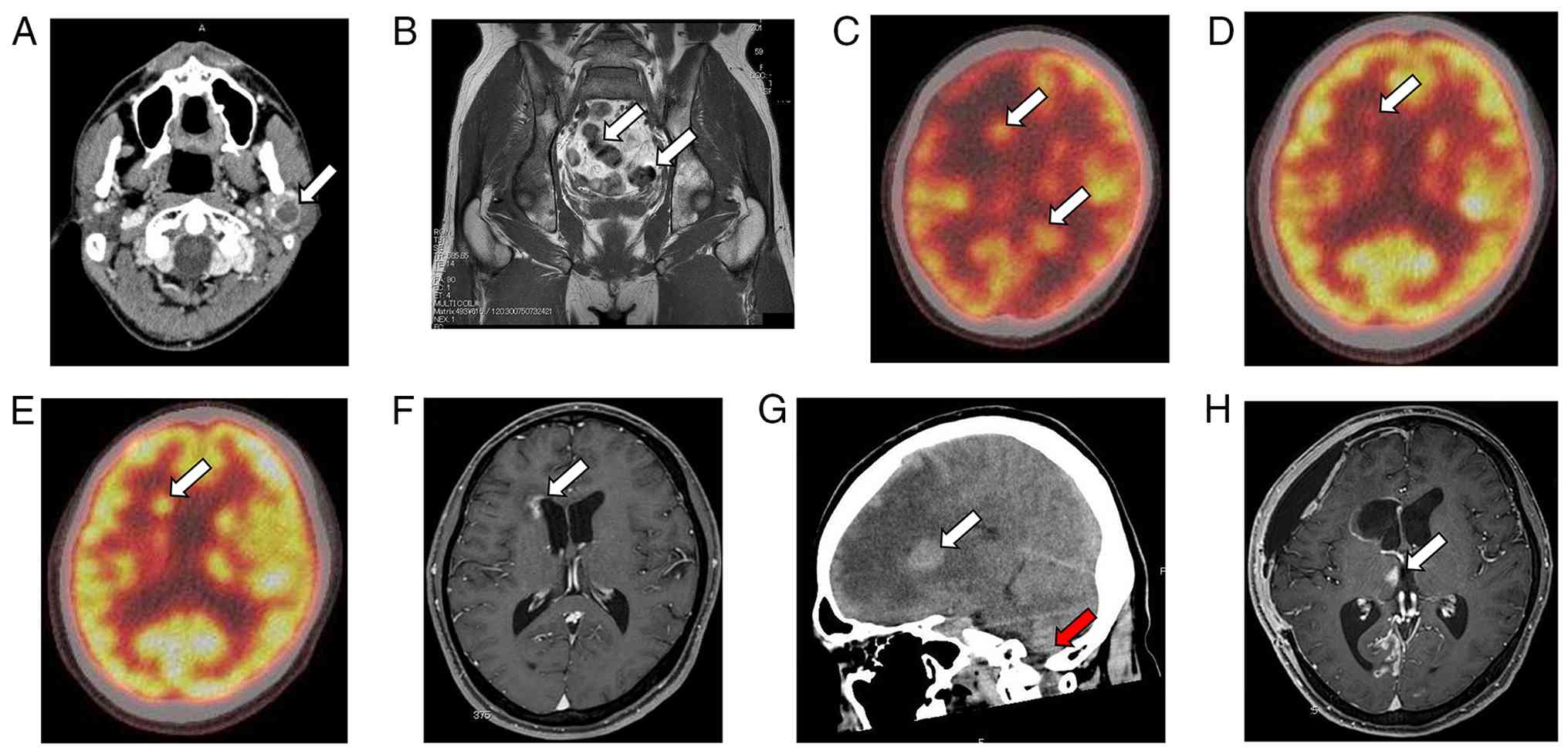
in August 2018. Upon physical examination, a poorly mobile and
tender mass measuring ~2 cm in diameter was palpated in the left
parotid region. A contrast-enhanced CT scan indicated the presence
of a parotid gland carcinoma (Fig.
1A). A total left parotidectomy with left upper neck lymph node
dissection was performed in August 2018. The postoperative course
was uneventful.
In October 2018, post-operative radiation therapy to
the left parotid gland region was performed (66 Gy in 33 fractions)
and no local recurrence was observed. In August 2019, an MRI scan
revealed metastatic lesions in the lumbar spine and pelvis
(Fig. 1B). Needle biopsy of the
iliac bone determined bone metastasis and palliative radiotherapy
(30 Gy in 10 fractions) was initiated. In October 2019, anti-HER2
combination chemotherapy [trastuzumab (4 mg/kg), paclitaxel (80
mg/m2) and carboplatin (270 mg)] was administered. After
the second course, leukopenia developed; thus, combination therapy
was discontinued. From November 2019 to May 2022, trastuzumab
monotherapy (2 mg/kg once a week or once every 2 weeks) was
administered. In May 2021, the patient developed epileptic
seizures, with a PET scan suggesting brain metastasis (Fig. 1C). Therefore, the patient underwent
Gamma Knife radiosurgery (42 Gy in 10 fractions). In January 2022,
reduced fluorodeoxyglucose uptake was noted in the brain metastatic
lesions (Fig. 1D), suggesting
partial response to the Gamma Knife therapy. However,
fluorodeoxyglucose uptake in the brain metastatic lesions was shown
to be increased in January 2023 (Fig.
1E). Therefore, additional Gamma Knife radiosurgery was
performed in June 2023 (37 Gy in 10 fractions). An MRI performed in
September 2023 showed a reduction in the size of the brain
metastatic lesions (Fig. 1F). In
June 2024, the patient was once again admitted to the Department of
Neurosurgery, Osaka Medical and Pharmaceutical University Hospital
(Takatsuki, Japan) with worsening cerebral oedema and signs of
brain herniation due to a number of cerebral metastases (Fig. 1G). Surgical resection of the brain
tumour was performed in the right frontal lobe and whole-brain
radiotherapy was performed for disease control (30 Gy in 10
fractions) in July 2024. No obvious residual tumour was noted in
the surgical site; however, a new metastatic lesion was observed
(Fig. 1H). The patient was
transferred to the palliative care unit at another hospital in
January 2025 (6 years and 5 months after the initial surgery) as
his overall health condition deteriorated and he could not
withstand further treatment. No information regarding the status of
the patient was available due to loss of follow-up since the
transfer to another hospital. The aforementioned treatments were
performed according to guidelines from the National Comprehensive
Cancer Network (https://jnccn.org/).
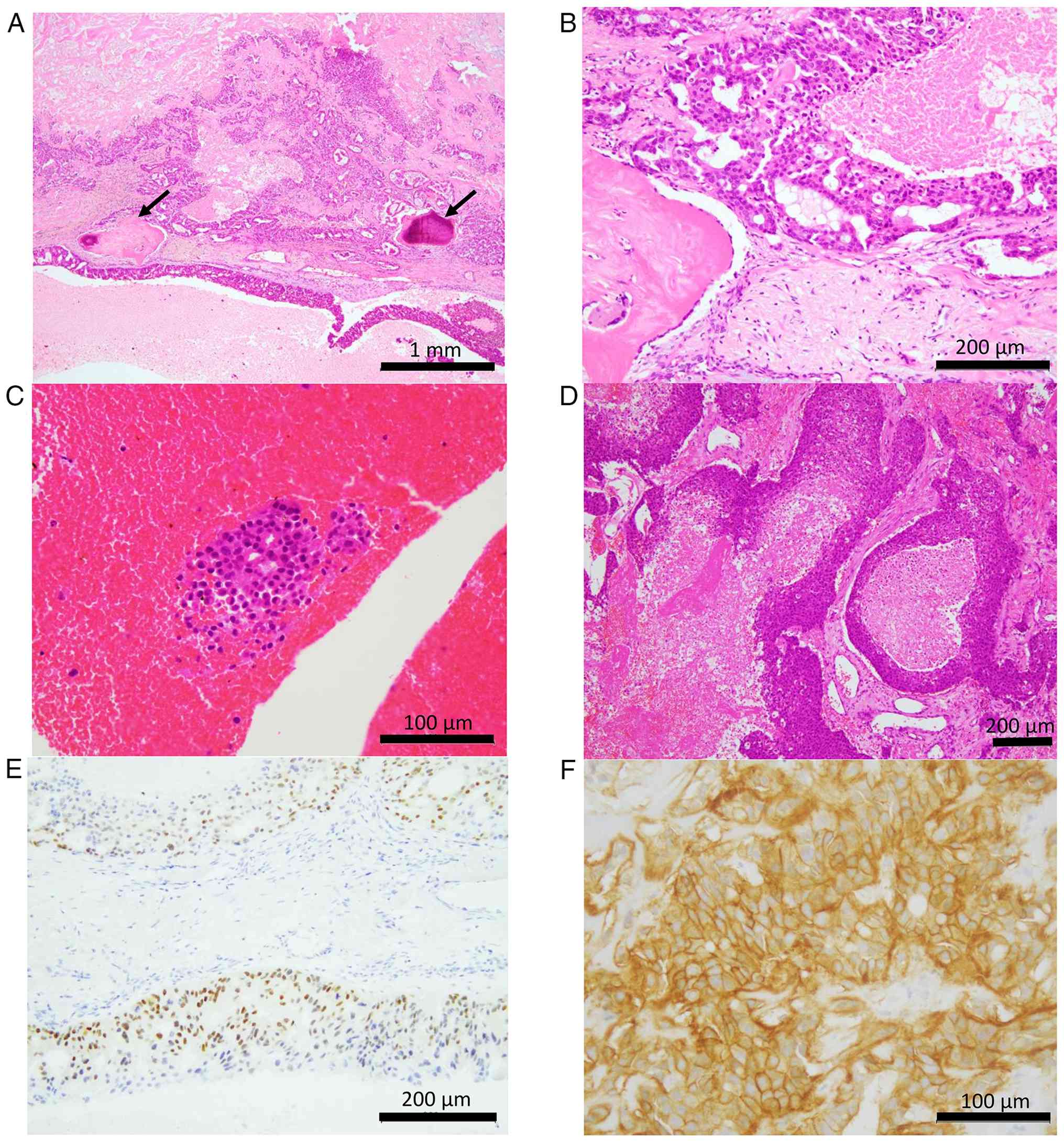
With regard to histopathological characteristics,
surgically resected specimens of the left parotid gland revealed
invasive neoplastic growth into the surrounding nonneoplastic
parotid gland tissue. The tumour exhibited cribriform and papillary
proliferation with comedo-type necrosis (Fig. 2A). These large neoplastic cells were
polygonal in shape and exhibited abundant eosinophilic cytoplasm
and large round to oval nuclei with conspicuous nucleoli (Fig. 2B). Lymphovascular and perineural
invasion was also observed. In addition, one peculiar finding was
the presence of intra- and peri-tumoural bone formation at the
peripheral region of the tumour, with the bone tissues being
surrounded by carcinoma nests (Fig.
2A). Osteoblasts, lacking nuclear atypia, lined the periphery
of the lamella bone and the bone marrow was absent. No
cartilaginous tissue was observed. Histopathological evidence of
the presence of PA, such as chondromyxoid stroma and neoplastic
myoepithelial cells without nuclear atypia, was not detected. In
addition, no sarcomatous component was present and no lymph node
metastasis was noted. Accordingly, SDC with HO (pT3N0M0) was
diagnosed at the time of the diagnosis of the parotid gland tumour
(in August 2018).
The needle-biopsy specimen of the iliac bone
demonstrated presence of carcinoma cells having rich eosinophilic
cytoplasm and large nuclei, which was consistent with metastatic
SDC (Fig. 2C). The resected
specimen of the brain metastasis relatively exhibited the same
histopathological features as the parotid gland tumour. Cribriform
or solid proliferation of neoplastic cells with rich eosinophilic
cytoplasm and large nuclei in a background of abundant necrotic
material was observed (Fig. 2D).
Immunohistochemical analyses were performed using a Ventana
BenchMark ULTRA autostainer (Roche Diagnostics). In addition, the
Ventana ultraView Universal DAB Detection Kit (cat. no.
760-500; Roche Diagnostics), including the secondary antibody, was
used. Briefly, resected specimens were fixed in 10% buffered
neutral formalin at room temperature for 24 h, dehydrated in
ethanol and xylene at room temperature and embedded in paraffin.
The 4-µm tissue sections were used for immunostaining with a rabbit
monoclonal antibody against AR (clone: SP107; cat. no. 760-4605;
ready-to-use; Roche Diagnostics) and a rabbit monoclonal antibody
against HER2 (clone: 4B5; cat. no. 790-2991; ready-to-use; Roche
Diagnostics). Tissue sections were incubated with primary
antibodies for 16 min (AR) or 10 min (HER2) at 36°C, with the
secondary antibody (pre-diluted) for 8 min at 36°C and underwent
haematoxylin counterstaining for 4 min at 36°C. A light microscope
(BX51; Olympus Corporation) was used to visualise the
immunohistochemical staining. Immunohistochemical analysis of the
parotid gland tumour showed that AR was expressed in the nuclei of
the carcinoma cells (Fig. 2E).
Diffuse membrane HER2 upregulation was also observed in these
carcinoma cells (Fig. 2F). These
features were typical for SDC (1).
Discussion
To the best of our knowledge, the present report is
the first case in the literature to describe SDC with HO in the
parotid gland. A total of only 18 patients with salivary gland
neoplasms and HO [3 patients with MEC and CXPA, 11 patients with
PA, and 1 patient with SDC (the present patient)] have been
reported in the English-language literature (Table I) (9–25).
Table I summarises the
clinicopathological features of salivary gland neoplasms with HO.
The predominant histological type of salivary gland neoplasm with
HO was PA, followed by CXPA and MEC (Table I). CXPA is defined as the occurrence
of carcinoma, frequently SDC and myoepithelial carcinoma, arising
from a pre-existing PA. Furthermore, ~80% of salivary gland
neoplasms with HO are PA or associated neoplasms (Table I). Despite 1 case having reported
that three of 19 intraoral PAs harbour osseous components, detailed
clinicopathological information was unavailable (26). Therefore, these 3 PA cases were
excluded from the present review. In addition, minor salivary
glands, including those present in the lip, may show a high
frequency of HO in PA, given that 5 of 11 PA with HO cases were
from the lip or buccal mucosa (Table
I), consistent with the results of the aforementioned report
(26). Despite SDC being one of the
common carcinoma components of CXPA, neither PA nor sarcomatous
component was detected in the present parotid gland tumour.
Therefore, the diagnosis of SDC with HO was made.
 | Table I.Clinicopathological features of
salivary gland neoplasms with heterotopic ossification. |
Table I.
Clinicopathological features of
salivary gland neoplasms with heterotopic ossification.
| First author,
year | Case no. | Age | Sex | Location | Histological
type | Cartilaginous
tissue | (Refs.) |
|---|
| Present case | 1 | 38 | Male | Parotid | Salivary duct
carcinoma | Absent | Present case |
| Yamao et al,
2025 | 2 | 78 | Female | Sublingual | Mucoepidermoid
carcinoma | NA | (9) |
| Wolf et al,
2021 | 3 | 48 | Female | Sublingual | Mucoepidermoid
carcinoma | NA | (10) |
| Maruse et al,
2015 | 4 | 75 | Female | Sublingual | Mucoepidermoid
carcinoma | NA | (11) |
| Rauso et al,
2019 | 5 | 50 | Male | Parotid | CXPA (histology
NA) | NA | (12) |
| Mohan et al,
2015 | 6 | 76 | Male | Parotid | CXPA
(non-invasive) | Present | (13) |
| Spencer et
al, 1991 | 7 | 83 | Female | Parotid | CXPA (poorly
differentiated) | Present | (14) |
| Gubod et al,
2022 | 8 | 32 | Female | Parotid | Pleomorphic
adenoma | Present | (15) |
| Pérez-De-Oliveira
et al, 2020 | 9 | 73 | Female | Lip | Pleomorphic
adenoma | Absent | (16) |
| Mandal et
al, 2008 | 10 | 27 | Male | Buccal mucosa | Pleomorphic
adenoma | Present | (17) |
| Kato et al,
2007 | 11 | 38 | Female | Parotid | Pleomorphic
adenoma | Present | (18) |
| Nakano et
al, 2007 | 12 | 34 | Male | Lip | Pleomorphic
adenoma | NA | (19) |
| Xu et al,
2003 | 13 | 36 | Female | Submandibular | Pleomorphic
adenoma | Present | (20) |
| Shigeishi et
al, 2001 | 14 | 58 | Male | Parotid | Pleomorphic
adenoma | Present | (21) |
| Hamakawa et
al, 1997 | 15 | 53 | Female | Lip | Pleomorphic
adenoma | Present | (22) |
| Takeda and
Yamamoto, 1996 | 16 | 44 | Female | Lip | Pleomorphic
adenoma | Absent | (23) |
| Lee et al,
1992 | 17 | 21 | Male | Maxillary
sinus | Pleomorphic
adenoma | Absent | (24) |
| Yates and Paget,
1952 | 18 | 21 | Male | Submandibular | Pleomorphic
adenoma | Present | (25) |
Although the detailed mechanism of HO development in
salivary gland neoplasms has not been clarified, a number of
hypotheses have been proposed (19). Firstly, neoplastic myoepithelial
cells, one of the main neoplastic components of PA, as well as
ductal cells, serve an important role in the development of HO in
PA (19). Neoplastic myoepithelial
cells may serve as a source of bone-forming cells given that they
express osteoblastic marker, such as runt-related transcription
factor 2 (RUNX2) (19). An
additional hypothesis is endochondral ossification given that 70%
(7 of 10) PAs exhibited cartilaginous tissue surrounding the HO
(Table I). The pre-existing PA
component may be associated with the presence of HO in CXPA given
that 2 of 3 CXPAs exhibited cartilaginous tissue surrounding the HO
(13,14). In addition, one CXPA had collagenous
stroma surrounding the HO without cartilaginous tissue; rich stroma
may be associated with the presence of HO given that rich fibrous
stroma is frequently observed in HO in colorectal adenocarcinoma
and mesenchymal cells within rich fibrous stroma could provide a
bone-forming niche (26). MEC is a
common salivary gland carcinoma characterised by the presence of
mucus and intermediate and squamoid carcinoma cells that form
cystic and solid growth patterns (27). As well as SDC, MEC exhibits no
neoplastic myoepithelial cells or cartilaginous components.
Therefore, HO in MEC and SDC is not associated with neoplastic
myoepithelial cells or cartilaginous tissues, as speculated for PA.
Therefore, the mechanisms underlying the development of HO in
patients with PA (including CXPA), MEC and SDC may differ.
Furthermore, it is necessary to determine whether
presence of HO in malignant salivary gland tumours affects the
prognosis, although its presence has not been associated with
prognosis in patients with papillary carcinoma of the thyroid
(8). However, only one SDC and
three MEC have been reported in the English-language literature
(9–11), therefore, the prognostic importance
of HO presence cannot be determined. Accumulation of the
clinicopathological data of malignant salivary gland tumours with
HO is thus required for resolving this issue. In addition, the
patient was young for SDC, however the association between the age
and clinical aggressiveness of the patient or presence of HO
remains unclear due to the rarity of HO in SDC.
Bone morphogenic proteins (BMPs), members of the
TGF-β superfamily, have been recognised as inductive factors for
osteogenesis and BMP2 is a major inducer of HO (28). Higher immunohistochemical expression
of BMP2 has been noted in tumours and/or stromal cells surrounding
HO in colorectal tumours (5). The
BMP2 signalling pathway induces the expression of RUNX2, a master
regulator of osteoblastic differentiation from mesenchymal stem
cells, leading to the differentiation of osteoprogenitor cells into
osteoblasts (5,28,29).
Neoplastic myoepithelial cells surrounding HO in PA exhibit
positive immunoreactivity for RUNX2, indicating their important
role in the development of HO (19). Expression analysis of these
osteogenic molecules in the present specific SDC case with HO was
not performed. Therefore, molecular analyses are required to
further elucidate the molecular mechanisms underlying HO in
salivary gland neoplasms.
In conclusion, to the best of our knowledge, the
present report described the first reported case of SDC with HO in
the salivary gland and reviewed the clinicopathological features of
benign and malignant salivary gland neoplasms with HO. It is
important to recognize that HO can occur in SDC and not to
misunderstand that its presence is almost exclusively found in PA
in diagnostic practice of the salivary gland tumour. The detailed
mechanism of HO in salivary gland neoplasms remains unclear and its
mechanism in SDC may differ from that in PA, although the present
single case does provide sufficient evidence. Further molecular
analyses are thus required to clarify the mechanism of development
of HO in salivary gland neoplasms.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
MI conceived and designed the present study. YF, MI
and AS analysed the histological and immunohistochemical features.
YF and MI confirm the authenticity of all the raw data. YF, MI, AS,
TJ, TT, SIH and YH contributed to data collection and analysis. YF
and MI wrote the manuscript and prepared figures and tables. All
authors read and approved the final version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written consent for the publication of patient data
and associated images was obtained from the patient.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
AR
|
androgen receptor
|
|
BMP
|
bone morphogenetic protein
|
|
CXPA
|
carcinoma ex pleomorphic adenoma
|
|
HO
|
heterotopic ossification
|
|
MEC
|
mucoepidermoid carcinoma
|
|
PA
|
pleomorphic adenoma
|
|
RUNX2
|
runt-related transcription factor
2
|
|
SDC
|
salivary duct carcinoma
|
References
|
1
|
Chiosea S, Agaimy A, Hellquist H, Nagao T,
Simpson RHW and van Herpen CML: Salivary duct carcinoma. WHO
Classification of Tumours, Skin Tumours. 5th edition. IARC; Lyon:
pp. 225–227. 2024
|
|
2
|
Meyers C, Lisiecki J, Miller S, Levin A,
Fayad L, Ding C, Sono T, McCarthy E, Levi B and James AW:
Heterotopic ossification: A comprehensive review. JBMR Plus.
3:e101722019. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Liu K, Tripp S and Layfield LJ:
Heterotopic ossification: Review of histologic findings and tissue
distribution in a 10-year experience. Pathol Res Pract.
203:633–640. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Fukuma Y, Ishida M, Yasuda E, Nakanishi K,
Kushiyama S, Tomioka A, Asakuma M and Hirose Y: Ossification in
pancreatic neoplasms: A report of three cases of neuroendocrine
tumor, mucinous cystic neoplasm, and intraductal papillary mucinous
neoplasm with review of the literature. Biomed Rep. 24:102025.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Vos AM, Pijnenborg L, van Vliet S, Kodach
LL, Ciompi F, van der Post RS, Simmer F and Nagtegaal ID:
Biological background of colorectal polyps and carcinomas with
heterotopic ossification: A national study and literature review.
Hum Pathol. 145:34–41. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bezić J, Karaman I, Zekić Tomaš S,
Živković PM and Božić J: Osteonevus of Nanta revisited:
Clinicopathological features of 33 cases. Am J Dermatopathol.
38:859–861. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ishida M, Iwai M, Kagotani A, Iwamoto N
and Okabe H: Epidermal cyst of the skin with ossification: Report
of two cases. Int J Clin Exp Pathol. 7:1823–1825. 2014.PubMed/NCBI
|
|
8
|
Bai Y, Zhou G, Nakamura M, Ozaki T, Mori
I, Taniguchi E, Miyauchi A, Ito Y and Kakudo K: Survival impact of
psammoma body, stromal calcification, and bone formation in
papillary thyroid carcinoma. Mod Pathol. 22:887–894. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yamao N, Shimamoto H, Munshi MZ, Nishimura
DA, Takagawa N, Assapattarapun V, Hirose K, Oya K, Uchihashi T,
Kreiborg S, et al: Imaging diagnosis of mucoepidermoid carcinoma
with intratumoral bone formation: A case report. Oral Radiol.
42:460–466. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wolf B, Roth S, Fantasia J and Nannini V:
‘Ossifying’ mucoepidermoid carcinoma: A deceptive clinical
presentation. Oral Surg Oral Med Oral Pathol Oral Radiol.
131:217–220. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Maruse Y, Kawano S, Kiyoshima T, Goto Y,
Matsubara R, Chikui T, Yoshiga D and Nakamura S: Case of
mucoepidermoid carcinoma of the sublingual gland accompanied with
extensive dystrophic calcification and intratumoral bone formation.
Head Neck. 37:E161–E164. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Rauso R, Colella G, Franco R, Ronchi A and
Chirico F: Ossified carcinoma ex pleomorphic adenoma in accessory
lobe of parotid gland: Complexity in clinical, imaging and
histologic diagnosis and minimally invasive surgery. Oral Oncol.
92:95–98. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Mohan S, Puram SV, Yarlagadda B, Nosé V
and Deschler DG: Ossifying parotid carcinoma ex pleomorphic
adenoma. Case Rep Otolaryngol. 2015:3953582015.PubMed/NCBI
|
|
14
|
Spencer J, Mason A and Denton K: Ossifying
parotid carcinoma ex pleomorphic adenoma: CT findings. J Comput
Assist Tomogr. 15:516–518. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gubod ER, Ramanathan A, Chong Mei Yee S
and Tilakaratne WM: Bone formation in pleomorphic adenoma: A case
report. Cureus. 14:e228682022.PubMed/NCBI
|
|
16
|
Pérez-De-Oliveira ME, Leite AA, de Lima
Morais TM, Lopes MA, de Almeida OP and Vargas PA: Intraoral
pleomorphic adenoma with extensive bone formation. Int J Surg
Pathol. 28:410–411. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Mandal S, Dhingra K, Roy S and Khurana N:
Extensive bone with marrow formation in pleomorphic adenoma. Report
of a case. ANZ J Surg. 78:323–324. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kato H, Kanematsu M, Ando K, Mizuta K, Ito
Y, Hirose Y and Hoshi H: Ossifying pleomorphic adenoma of the
parotid gland: A case report and review. Australas Radiol. 51
(Suppl 1):B173–B175. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Nakano K, Watanabe T, Shimizu T and
Kawakami T: Immunohistochemical characteristics of bone forming
cells in pleomorphic adenoma. Int J Med Sci. 4:264–266. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Xu H, Shimizu Y, Niki T, Nagasaka H,
Kawamura H and Ooya K: Pleomorphic adenoma of the submandibular
salivary glands with marked ossification. J Oral Pathol Med.
32:499–501. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Shigeishi H, Hayashi K, Takata T, Kuniyasu
H, Ishikawa T and Yasui W: Pleomorphic adenoma of the parotid gland
with extensive bone formation. Pathol Int. 51:883–886. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hamakawa H, Takarada M, Ito C and Tanioka
H: Bone-forming pleomorphic adenoma of the upper lip: Report of a
case. J Oral Maxillofac Surg. 55:1471–1475. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Takeda Y and Yamamoto H: Stromal bone
formation in pleomorphic adenoma of minor salivary gland origin. J
Nihon Univ Sch Dent. 38:102–104. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lee KC, Chan JK and Chong YW: Ossifying
pleomorphic adenoma of the maxillary antrum. J Laryngol Otol.
106:50–52. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Yates PO and Paget GE: A mixed tumour of
salivary gland showing bone formation with a histochemical study of
the tumour mucoids. J Pathol Bacteriol. 64:881–888. 1952.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Pérez-de-Oliveira ME, Leonel ACLDS, de
Castro JFL, Carvalho EJA, Vargas PA and Perez DEDC:
Histopathological findings of intraoral pleomorphic adenomas: A
retrospective study of a case series. Int J Surg Pathol.
27:729–735. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Leivo I, Bishop JA, Cipriani NA,
Costes-Martineau V, Inagaki H and Vielh P: Mucoepidermoid
carcinoma. WHO Classification of Tumours, Skin Tumours. 5th
edition. IARC; Lyon: pp. 200–203. 2024
|
|
28
|
Akiyama T, Raftery LA and Wharton KA: Bone
morphogenetic protein signaling: The pathway and its regulation.
Genetics. 226:iyad2002024. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Njie R, Xu S, Wu T, Pi J, Lin S, Zhang P,
Wang J, Dai Q, Shen H, Zhang N and Chen G: Hedgehog signalling in
osteogenesis and bone metabolism: Molecular mechanisms, regulatory
networks and implications for skeletal disease. J Cell Mol Med.
29:e708132025. View Article : Google Scholar : PubMed/NCBI
|