Introduction
Breast cancer (BC) can originate in the lobules,
ducts or connective tissue; these cancer cells can spread through
blood or lymphatic vessels and if these cancer cells spread to
other tissues, metastasis may occur. A total of 2.3 million cases
of BC were diagnosed in 2022 in women worldwide, and 670,000
mortalities from the disease were recorded (1,2). BC
occurs due to the interaction of factors such as lifestyle
(obesity, physical inactivity), environmental (alcoholism,
smoking), biological (age >50 years, female) and genetic
mutations (in genes such as BRCA1 and BRCA2)
(1,2). Among genetic factors, DNA alterations,
such as chromosomal rearrangements, variants and epigenetic changes
(including promoter methylation), can prevent transcription by
preventing the binding of transcription factors or allowing the
binding of proteins to methyl groups (3).
DNA methylation status has served as an indicator of
BC; Vietri et al (4)
reported that hypermethylation in the promoter region of a tumor
suppressor gene causes inactivation, which can be used to assist
early identification of BC. Radpour et al (5) reported higher methylation in tumor
suppressor genes such as breast cancer susceptibility gene 1
(BRCA1), bone morphogenetic protein 6 (BMP6),
glutathione S-transferase π1 (GSTP1), estrogen receptor 2
(ESR2) and tissue inhibitor of metalloproteinase 3
(TIMP3) in breast tumors and each gene has been associated
with a certain clinical or histopathological characteristic. For
example, BMP6 methylation has been associated with the
presence of lymph node metastasis and has been proposed as a
biomarker of metastasis (6).
BRCA1 methylation causes its inactivation, which is common
in women with triple-negative BC (P=0.043) (7), and this subtype is associated with
increased metastatic risk and a poor prognosis (7). The methylation status of ESR2
allows for the early detection of BC as it is present in cancerous
tissue but not normal tissue (8,9).
GSTP1 methylation is associated with lymph node metastasis
and other aggressive clinical features (P=0.02) (10,11).
Lastly, TIMP3 methylation has been associated with a higher
tumor grade (II–III) (2) and
hormone positivity, reinforcing its role in BC progression
(12).
The aim of the present study was to determine
whether the methylation status of the BMP6, BRCA1, ESR2,
GSTP1 and TIMP3 genes is different in patients with BC
and women without cancer. The present study also aimed to analyze
whether a higher methylation level could be associated with
clinical and histopathological variables that are associated with
the poor prognosis of patients.
Subjects and methods
Subjects
In total, 60 patients with BC and 60 individuals
with benign disease (BD) were included in the present study,
samples were collected between August 2017 and August 2023. All
individuals signed informed consent forms, and blood and breast
tissue samples were obtained at the Mexican Social Security
Institute-Breast Clinic in Guadalajara (Mexico). The present study
was approved by the Bioethics Committee of Western Biomedical
Research Center, Mexican Social Security Institute (approval no.
R-2023-1305-024; Guadalajara, Mexico). The inclusion criteria for
the BC group were as follows: i) Women ≥18 years of age; ii)
patients with a histopathologically confirmed diagnosis, at any
clinical stage according to the TNM classification (2) and with comorbidities; iii) patients
who provided informed consent; while the exclusion criteria in the
BC group were participants whose BC was a secondary tumor. The
inclusion criteria for the BD group were as follows: i) Women ≥18
years of age; ii) individuals with benign breast lesions with
Breast Imaging-Reporting and Data System (BI-RADS) (13) category 4 diagnosis in whom
malignancy was ruled out using histopathological examination; and
iii) individuals who provided informed consent; in the BD group,
the exclusion criterion was a previous history of cancer.
DNA methylation analysis
Tissue DNA was extracted using the
DNeasy® 96 kit (Qiagen GmbH) and 500 ng of tissue DNA
was used for sodium bisulfite conversion using the
EpiTect® Bisulfite kit (Qiagen GmbH). The methylation
status was analyzed using methylation-specific PCR (MS-PCR), the
reaction conditions of which are presented in Table I. Primers for the BMP6, BRCA1,
GSTP, TIMP3 (promoter) and ESR2 (exon 1) genes (Table II) were designed using Methyl
Primer Express™ (version, 1.0; Applied Biosystems; Thermo Fisher
Scientific, Inc.), the software designed the primers in exon 1
specifically for ESR2, as this is where the highest number
of CG sites are located. Negative controls and commercial
methylated/unmethylated DNA (Qiagen GmbH) were included in the
present analysis. Each reaction (12.5 µl) contained 10X PCR buffer,
50 mM MgSO4, 10 mM dNTPs, 10 pM primers, Taq polymerase
(1 U) (Invitrogen; Thermo Fisher Scientific, Inc.) and converted
DNA (50–100 ng/µl), using reagents sourced from Invitrogen (Thermo
Fisher Scientific, Inc.). The products were separated via 2%
agarose gel electrophoresis, stained with SYBR™ Safe DNA Gel Stain
(Thermo Fisher Scientific, Inc.) and visualized using a UV
transilluminator. Sanger sequencing with BigDye Terminator v3.1
Cycle Sequencing Kit (Thermo Fisher Scientific, Inc.) was used as a
confirmatory method in certain samples for the BMP6, BRCA1,
ESR2 and TIMP3 genes, except for the GSTP1 gene
due to a lack of reagents and resources.
 | Table I.PCR conditions for the BMP6,
BRCA1, ESR2, GSTP1 and TIMP3 genes. |
Table I.
PCR conditions for the BMP6,
BRCA1, ESR2, GSTP1 and TIMP3 genes.
| Gene | Stage | Temperature,
°C | Time | Cycles |
|---|
| BMP6 |
Denaturalization | 94.0 | 5 min | 35 |
|
|
| 94.0 | 1 min |
|
|
| Alignment | 58.5 | 30 sec |
|
|
| Extension | 72.0 | 30 sec |
|
|
|
| 72.0 | 3 min |
|
|
|
| 4.0 | 5 min |
|
| BRCA1 |
Denaturalization | 94.0 | 5 min | 30 |
|
|
| 94.0 | 1 min |
|
|
| Alignment | 57.0 | 1 min |
|
|
| Extension | 72.0 | 45 sec |
|
|
|
| 72.0 | 5 min |
|
|
|
| 4.0 | 5 min |
|
| ESR2 |
Denaturalization | 94.0 | 5 min | 30 |
|
|
| 94.0 | 30 sec |
|
|
| Alignment | 58.0 | 1 min |
|
|
| Extension | 72.0 | 30 sec |
|
|
|
| 72.0 | 5 min |
|
|
|
| 4.0 | 5 min |
|
| GSTP1 |
Denaturalization | 94.0 | 10 min | 28 |
|
|
| 94.0 | 30 sec |
|
|
| Alignment | 63.5 | 30 sec |
|
|
| Extension | 72.0 | 30 sec |
|
|
|
| 72.0 | 7 min |
|
|
|
| 4.0 | 5 min |
|
| TIMP3 |
Denaturalization | 94.0 | 10 min | 30 |
|
|
| 94.0 | 30 sec |
|
|
| Alignment | 56.5 | 30 sec |
|
|
| Extension | 72.0 | 30 sec |
|
|
|
| 72.0 | 7 min |
|
|
|
| 4.0 | 5 min |
|
| Table II.Primer sequences used for amplifying
methylated and unmethylated fragments of studied genes. |
Table II.
Primer sequences used for amplifying
methylated and unmethylated fragments of studied genes.
| Gene | Primer sequence
(5′-3′)a | Primer sequence
size, bp | PCR product size,
bp |
|---|
| BMP6 |
|
|
|
|
Methylated | F:
GGTTTAGAGTGATCGCGTC | 19 | 108 |
|
| R:
CGCGCAAATCTCTAAAAAC | 19 |
|
|
Unmethylated | F:
GAGGTTTAGAGTGATTGTGTT | 21 | 108 |
|
| R:
CTCACACAAATCTCTAAAAAC | 21 |
|
| BRCA1 |
|
|
|
|
Methylated | F:
ATAGGTAGCGATTTTGATTTTC | 22 | 154 |
|
| R:
AATCTACCCCCGAATAACG | 19 |
|
|
Unmethylated | F:
ATAATAGGTAGTGATTTTGATTTTT | 25 | 154 |
|
| R:
CCCAATCTACCCCCAAATAACA | 22 |
|
| ESR2 |
|
|
|
|
Methylated | F:
AGTTGTAGGAGGTGCGTTC | 19 | 144 |
|
| R:
CGAAAAAACGCTTACCTTACAA | 22 |
|
|
Unmethylated | F:
TGAGTTGTAGGAGGTGTGTTT | 21 | 144 |
|
| R:
AACAAAAAAACACTTACCTTACAA | 24 |
|
| GSTP1 |
|
|
|
|
Methylated | F:
CGGTTAATATGGTGAAATTTC | 21 | 155 |
|
| R:
TACAATAACGCGATCTCG | 18 |
|
|
Unmethylated | F:
GTTTGGTTAATATGGTGAAATTTT | 24 | 155 |
|
| R:
TACAATAACACAATCTCAACA | 21 |
|
| TIMP3 |
|
|
|
|
Methylated | F:
TTTCGTTTCGTCGGGTATTC | 20 | 123 |
|
| R:
CTCCAAAATTACCGTACGCG | 20 |
|
| Unmethylated | F:
TTATTTTGTTTTGTTGGGTATTT | 23 | 123 |
|
| R:
TCTCCAAAATTACCATACACACC | 23 |
|
Statistical analysis
The clinical and histopathological variables
evaluated in the BC group included age, body mass index (BMI),
clinical stage, histological grade, histology, molecular subtype,
Ki-67 status, lymph node and distant metastasis, progression,
recurrence and survival; in the BD group, age, BMI and BI-RADS were
considered. The gene methylation profile was analyzed using
descriptive statistics. The normality of the quantitative data was
assessed using the Shapiro-Wilk's test and the distribution was
assessed with the Student's t-test, which was unpaired. Methylation
frequencies were compared using the χ2 test. The
methylation frequencies were analyzed according to BC molecular
subtype using χ2 test and Fisher's exact test. The
association between clinical characteristics and methylation status
was evaluated using odds ratio (OR) with 95% confidence intervals
(CIs). Furthermore, binary logistic regression was applied to
analyze the relationship between methylation and the clinical and
histopathological characteristics. P<0.05 was considered to
indicate a statistically significant difference. Statistical
analysis was performed using SPSS statistical software (version,
24.0; IBM Corp.) and Kaplan-Meier curves were plotted with RStudio
(version, 4.3.2; Posit Software).
Results
Clinical and histopathological
characteristics of the BC and BD groups
Table III presents
the clinical and histopathological characteristics of both BC and
BD groups. A statistically significant difference was observed in
the age of the patients in the BC and BD groups, with an average of
55 and 42 years, respectively (P<0.00001). The OR for the ≥50
years subgroup of the BC group compared with BD group was 5.44 (95%
CI, 2.49–11.88; P=0.00002). While no significant difference was
observed for BMI, the average BMI in the BC and BD group was 28.41
and 27.69 kg/m2, respectively (P=0.378), with both
groups being overweight.
| Table III.Clinical and histopathological
characteristics of the BC and BD group. |
Table III.
Clinical and histopathological
characteristics of the BC and BD group.
|
Characteristics | BC (n=60) | BD (n=60) | OR (95% CI) | P-value |
|---|
| Age, years |
|
|
|
|
| Mean ±
SD | 55±11.60 | 42±11.64 | - | 0.00001 |
|
Range | 37-88 | 22-70 | - | - |
| <50
years, n (%) | 18/60 (30) | 42/60 (70) | - | - |
| ≥50
years, n (%) | 42/60 (70) | 18/60 (30) | 5.44
(2.49–11.88) | 0.00002 |
| BMI,
kg/m2 |
|
|
|
|
| Mean ±
SD | 28.41±4.58 | 27.69±5.51 | - | 0.378 |
|
Range | 19.30–37.66 | 18.31–40.79 | - | - |
| Normal,
n (%) | 16/60 (26) | 15/60 (25) | - | 1.0 |
|
Overweight, n (%) | 22/60 (37) | 32/60 (53) | 0.50
(0.24–1.05) | 0.098 |
|
Obesity, n (%) | 22/60 (37) | 13/60 (22) | 2.09
(0.93–4.69) | 0.108 |
| Clinical stage, n
(%) |
|
| - | - |
| In
situ 1/60 (2) | NA |
|
|
|
| I | 7/60 (12) | NA |
|
|
| II | 21/60 (35) | NA |
|
|
|
III | 29/60 (48) | NA |
|
|
| IV | 2/60 (3) | NA |
|
|
| Histological grade,
n (%) |
|
| - | - |
| I | 11/60 (18) | NA |
|
|
| II | 26/60 (44) | NA |
|
|
|
III | 23/60 (38) | NA |
|
|
| Histology, n
(%) |
|
| - | - |
|
Ductal | 56/60 (93) | NA |
|
|
|
Lobular | 4/60 (7) | NA |
|
|
| Molecular subtypes,
n (%) |
|
| - | - |
| Luminal
A | 26/60 (43) | NA |
|
|
| Luminal
B | 15/60 (25) | NA |
|
|
|
HER2 | 10/60 (17) | NA |
|
|
| TN | 9/60 (15) | NA |
|
|
| ER, n (%) |
|
| - | - |
|
Positive | 38/60 (63) | NA |
|
|
|
Negative | 22/60 (37) | NA |
|
|
| PR |
|
| - | - |
|
Positive | 31/60 (52) | NA |
|
|
|
Negative | 29/60 (48) | NA |
|
|
| HER2, n (%) |
|
| - | - |
|
Positive | 19/60 (32) | NA |
|
|
|
Negative | 41/60 (68) | NA |
|
|
| Ki-67, n (%) |
|
| - | - |
|
<20% | 25/60 (42) | NA |
|
|
|
≥20% | 35/60 (58) | NA |
|
|
| Proximal
metastasis, n (%) |
|
| - | - |
|
Positive (≥1) | 40/60 (67) | NA |
|
|
|
Negative (0) | 20/60 (33) | NA |
|
|
| Distant metastasis,
n (%) |
|
| - | - |
|
Yes | 4/60 (7) | NA |
|
|
| No | 56/60 (93) | NA |
|
|
| Progression, n
(%) |
|
| - | - |
|
Yes | 7/60 (12) | NA |
|
|
| No | 53/60 (88) | NA |
|
|
| Recurrence, n
(%) |
|
| - | - |
|
Yes | 10/60 (17) | NA |
|
|
| No | 50/60 (83) | NA |
|
|
| Pathological
response, n (%) |
|
| - | - |
|
Complete | 35/60 (58) | NA |
|
|
| No
response | 25/60 (42) | NA |
|
|
Methylation frequency of the BMP6,
BRCA1, ESR2, GSTP1 and TIMP3 genes in the BC and BD groups
Table IV presents
the methylation results observed for each of the genes analyzed and
the differences between the BC and BD groups. The gene with the
lowest methylation percentage in both groups was BMP6, while
the gene with the highest methylation percentage in both groups was
GSTP1; however, only BRCA1 demonstrated a higher
frequency of methylation in the BC group (32.1%) compared with the
BD group (16.6%)(P=0.040), indicating that methylation of the
BRCA1 gene increased the susceptibility of developing BC in
the examined cohort OR of 2.50 (95% CI, 1.02–6.42; P=0.0001).
Regarding the other genes analyzed in the present study, although
BMP6 demonstrated higher methylation in the BC group (14.3%)
compared with that in the BD group (3.6%), the difference was not
statistically significant (P=0.093). Furthermore, methylation
frequencies were analyzed according to the BC molecular subtype
(including luminal A, luminal B, HER2-enriched and triple-negative
BC), with no statistically significant differences observed among
the molecular subtypes; however, the BMP6 gene was mostly
methylated in the luminal A subtype, BRCA1 in the
triple-negative subtype, ESR2 in the HER2-enriched subtype,
GSTP1 in the triple-negative subtype and TIMP3 in the
HER2-enriched subtype (Table V).
DNA sequencing yielded results consistent with those of MS-PCR for
the BMP6 and TIMP3 genes (Fig. 1).
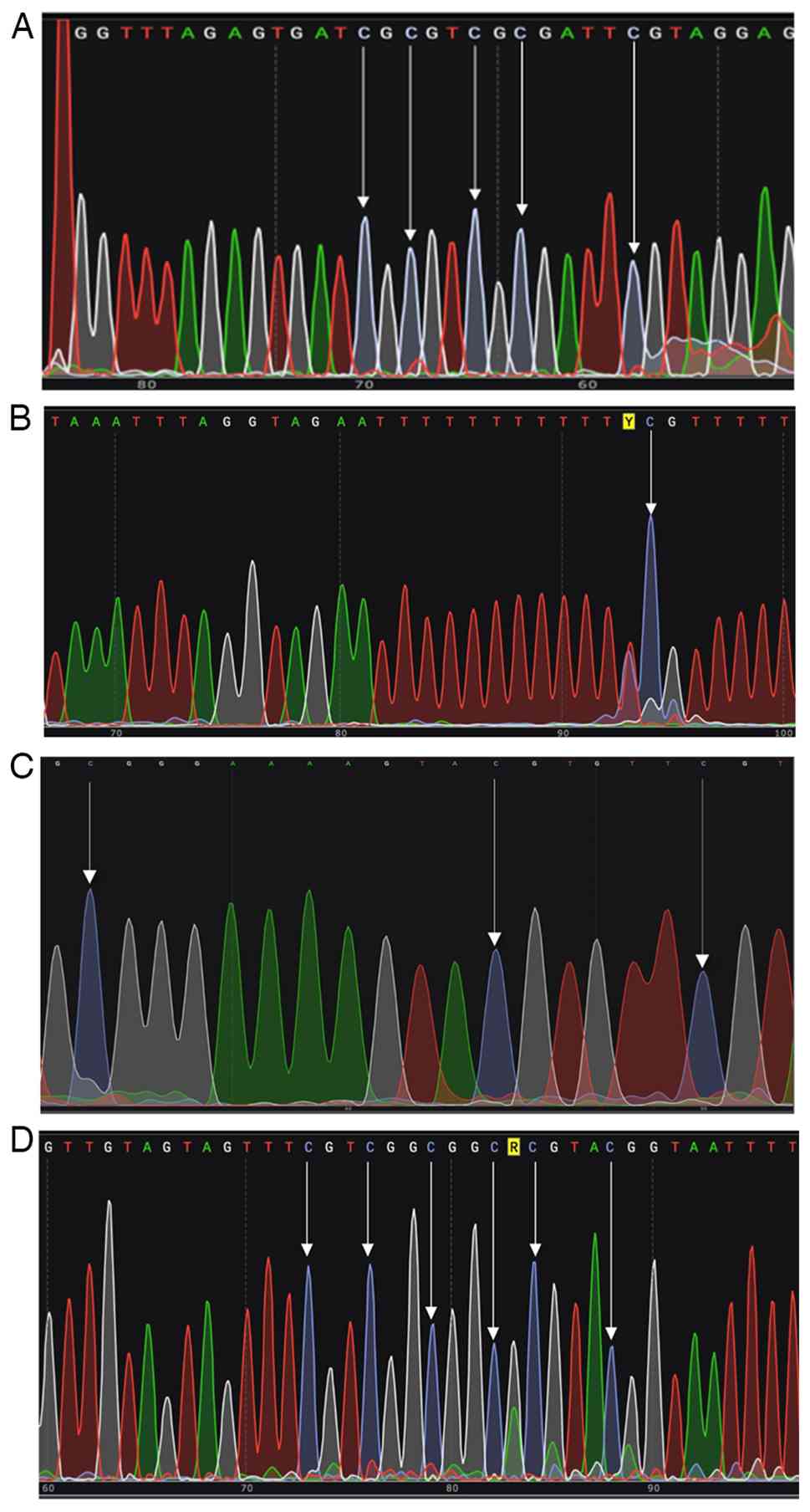 | Figure 1.(A) Partial electropherogram of a DNA
sample positive for methylation in the BMP6 gene. The first
three arrows indicate three CG sites (methylated) detected by the
forward primer 5′-GGTTTAGAGTGATCGCGTC-3′ (bold) using MS-PCR (100%
concordance with DNA sequencing at these 3 sites) and the remaining
two arrows point to other (methylated) CG sites that were
visualized via DNA sequencing. The sequence described in NCBI
Reference Sequence: NC_000006.12 was used as a reference. (B)
Partial electropherogram of a DNA sample positive for methylation
in the BRCA1 gene. The arrow indicates a methylated CG site
not located within the primer sequence; in this case, as the primer
sequence is not visible, it is not possible to determine the
correspondence between the sites observed by MS-PCR and sequencing.
(C) Partial electropherogram of a DNA sample positive for
methylation in the ESR2 gene. The arrows indicate three CG
sites (methylated) not located within the primer sequence; in this
case, as the primer sequence is not presented, it is not possible
to determine the correspondence between the sites observed by
MS-PCR and sequencing. The sequence described in NCBI Reference
Sequence: NG_011535.1 was used as a reference. (D) Partial
electropherogram of a DNA sample positive for methylation in the
TIMP3 gene. The arrows indicate six CG sites (methylated);
the first three indicate sites not located in the primer sequence,
whilst the fourth, fifth and sixth arrows indicate other sites
located in the primer reverse 5′-GGCGCGTACGGTAATTTTGGAG-3′ (bold)
detected by MS-PCR (100% concordance at these 3 sites). MS-PCR,
methylation specific-PCR; BMP6, bone morphogenetic protein
6; BRCA1, breast cancer susceptibility gene 1; TIMP3,
tissue inhibitor of metalloproteinase 3; ESR2, estrogen
receptor 2; NCBI, National Center for Biotechnology
Information. |
| Table IV.Methylation observed for each of the
genes analyzed in patients with BC and BD. |
Table IV.
Methylation observed for each of the
genes analyzed in patients with BC and BD.
| Gene | BC, n (%) | BD, n (%) |
P-valuea | OR | 95% CI |
P-valueb |
|---|
| BMP6 | 8/56 (14.3) | 2/55 (3.6) | 0.093 | 4.36 | 0.81–44.16 | 0.093 |
| BRCA1 | 17/53 (32.1) | 10/60 (16.6) | 0.040c,d | 2.50d | 1.02–6.42 |
<0.001c,d |
| ESR2 | 21/55 (38.2) | 15/53 (28.3) | 0.378 | 0.69 | 0.30–1.56 | 0.378 |
| GSTP1 | 48/51 (94.1) | 55/57 (96.5) | 0.660 | 1.75 | 0.28–10.95 | 0.660 |
| TIMP3 | 9/48 (18.7) | 10/48 (20.0) | 0.830 | 1.11 | 0.40–3.04 | 0.830 |
| Table V.Methylation frequency of the studied
genes across breast cancer molecular subtypes. |
Table V.
Methylation frequency of the studied
genes across breast cancer molecular subtypes.
| Gene | LA, n (%) | LB, n (%) | HER2, n (%) | TN, n (%) | P-valuea |
|---|
| BMP6 | 5/24 (21) | 2/14 (14) | 0/8 (0) | 1/10 (10) | 0.222 |
| BRCA1 | 8/24 (33) | 4/11 (36) | 1/8 (13) | 4/10 (40) | >0.999 |
| ESR2 | 8/24 (33) | 6/14 (43) | 5/9 (56) | 2/9 (22) | >0.999 |
| GSTP1 | 21/24 (88) | 11/12 (92) | 7/8 (88) | 8/8 (100) | >0.999 |
| TIMP3 | 4/24 (17) | 1/10 (10) | 2/8 (25) | 2/10 (20) | >0.999 |
Relationship between BMP6, BRCA1,
ESR2, GSTP1 and TIMP3 gene methylation and clinical and
histopathological variables
Although the TIMP3 gene demonstrated no
significant differences in methylation frequency between the BC
(18.7%) and BD (20%) groups, methylation of the TIMP3 gene
indicated a significant relationship with distant metastasis with
an OR of 8.65 (95% CI, 1.29–57.9; P=0.028); while methylation of
the other genes exhibited no association with clinical
histopathological characteristics (Table VI). However, a trend was observed
between BRCA1 gene methylation and ≥20% Ki-67 protein levels
(P=0.057) as well as lymph node metastasis (P=0.059) (Table VI).
| Table VI.Association between
clinicopathological characteristics and gene methylation status
analyzed using binary logistic regression. |
Table VI.
Association between
clinicopathological characteristics and gene methylation status
analyzed using binary logistic regression.
| Clinicopathological
characteristics | BMP6 | BRCA1 | ESR2 | GSTP1 | TIMP3 |
|---|
| Age (≥50
years) | 0.997 | 0.095 | 0.704 | - | 1.000 |
| BMI | 0.998 | 0.744 | 0.976 | - | 0.998 |
| PR (positive) | 1.000 | 0.920 | 0.650 | - | 0.998 |
| ER (positive) | 0.899 | 0.999 | 0.764 | - | 0.999 |
| HER2
(positive) | 0.974 | 0.999 | 0.562 | - | 0.999 |
| Clinical stage | 0.997 | 0.973 | 0.390 | - | 0.998 |
| Ki-67 (≥20%) | 0.996 | 0.057a (OR, 6.55; 95% CI,
1.01–41.8) | 0.674 | - | 1.000 |
| Lymph node
metastasis | 0.997 | 0.059a (OR, 6.47; 95% CI,
1.01–43.7) | 0.626 | - | 0.998 |
| Distant
metastasis | 0.144 | 0.275 | 1.000 | - | 0.028b (OR, 8.65; 95% CI,
1.29–57.9) |
Relationship between BMP6, BRCA1,
ESR2, GSTP1 and TIMP3 gene methylation and BC prognosis
A progression-free survival (PFS) analysis was
performed using Kaplan-Meier curves (Fig. 2, Fig.
3, Fig. 4, Fig. 5, Fig.
6) and the log-rank test, which evaluated the probability of
survival rate over 12, 36 and 60 months in patients with BC
according to the baseline methylation status of the target gene
(methylated vs. unmethylated). Baseline promoter methylation status
was determined using the baseline sample from each patient. Median
PFS was estimated from time to progression and event status, that
is, from the time of diagnosis confirmed using histopathology until
5 years of follow-up.
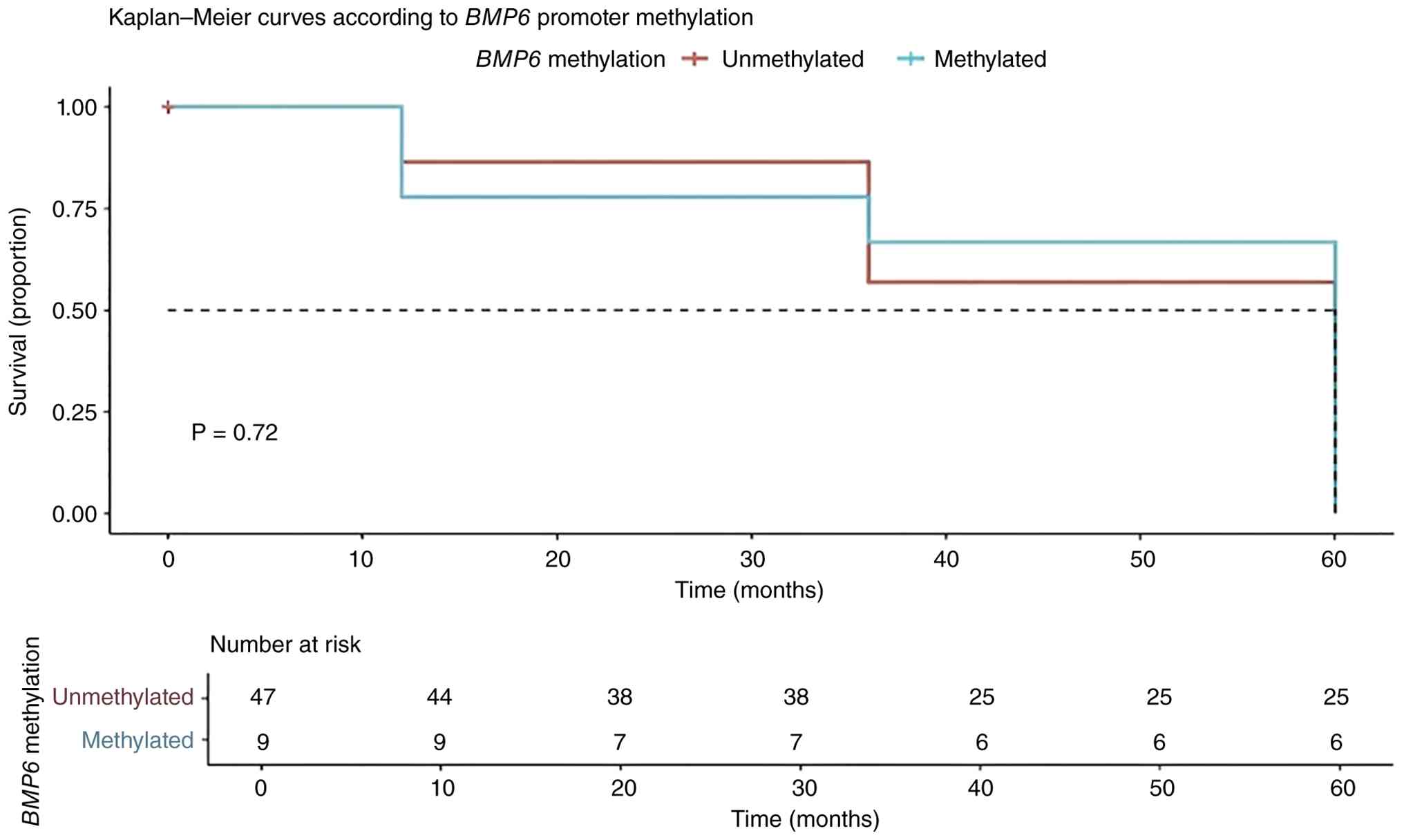
The Kaplan-Meier curve for BMP6 promoter
methylation demonstrated no significant difference (P=0.72) in
survival and progression time. The median PFS was also calculated,
demonstrating a time of 60 months in both the methylated and
unmethylated groups; therefore, there was no statistically
significant difference (P=0.72; Fig.
2).
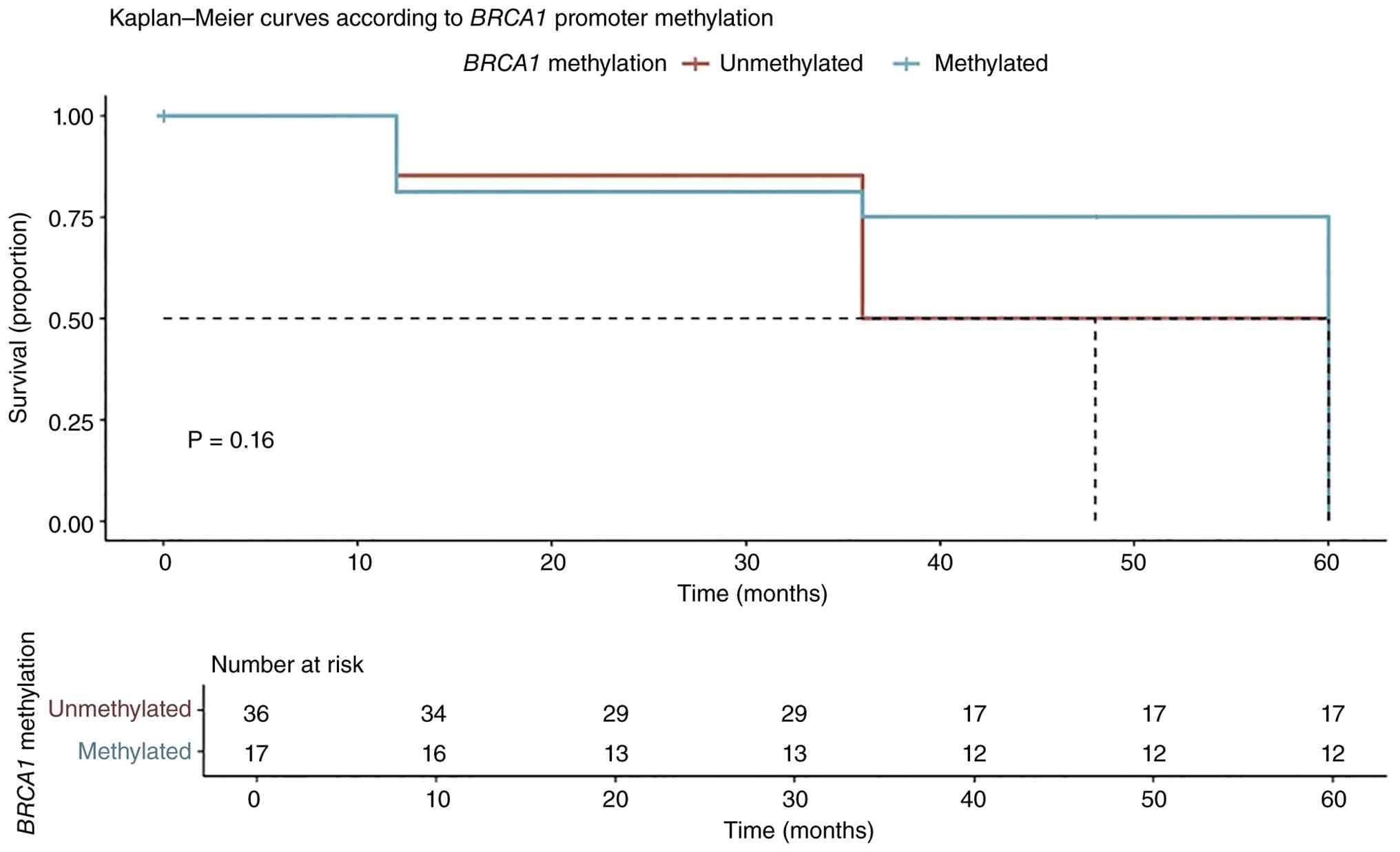
BRCA1 promoter methylation resulted in no
significant difference (P=0.16) in survival and progression time.
The median PFS time was also calculated, which was 60 months in the
methylated group and 48 months in the unmethylated group. This
finding indicated that patients with BRCA1 promoter
methylation progressed 1 year later compared with those without
methylation; however, the difference between the two groups was not
statistically significant (P=0.16; Fig.
3).
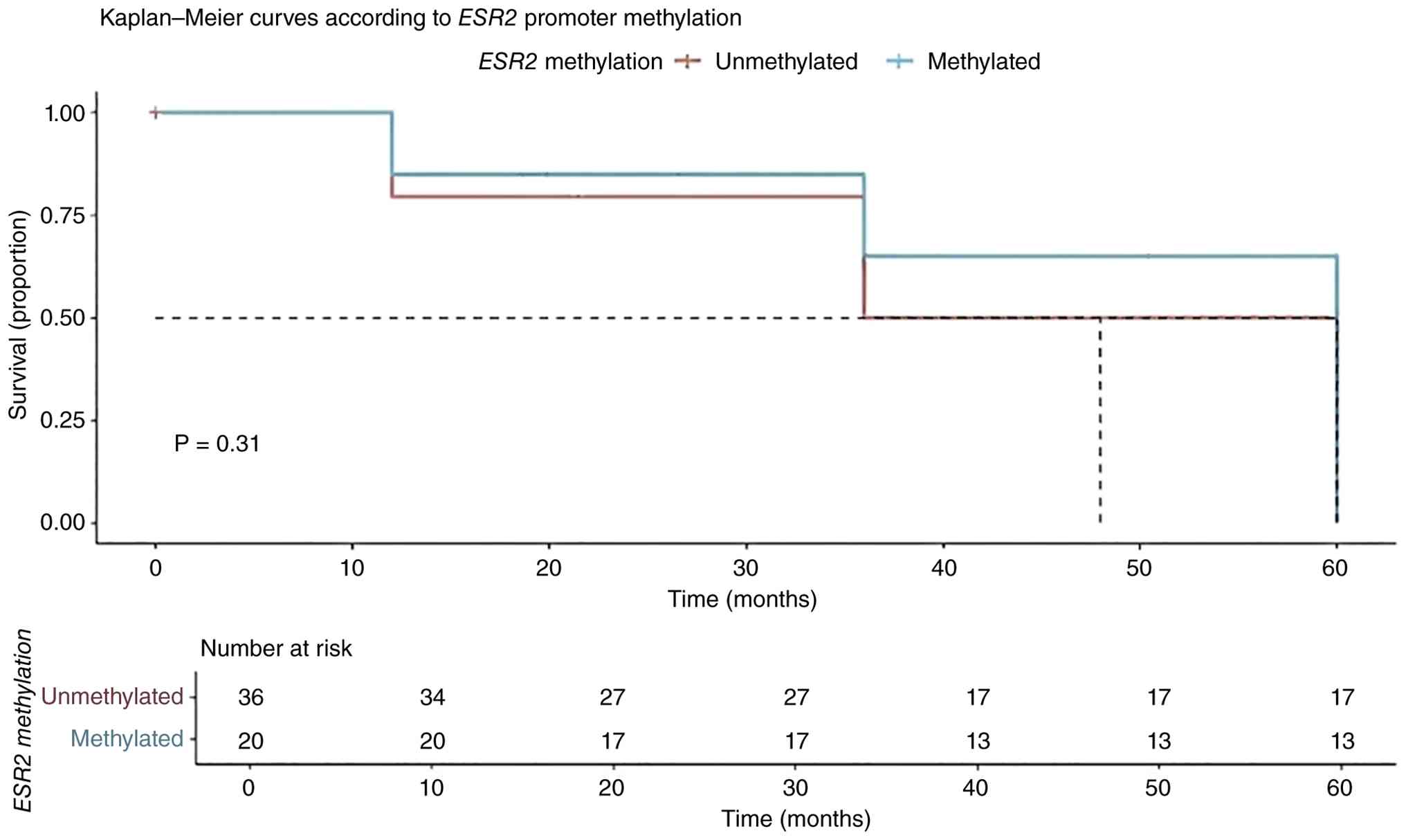
ESR2 promoter methylation resulted in no
significant difference (P=0.31) in survival and progression time.
The median PFS time was also calculated, which was 60 months in the
methylated group and 48 months in the unmethylated group. This
finding demonstrated that patients with ESR2 promoter
methylation progressed 1 year later compared with those without
methylation; however, the difference between the two groups was not
statistically significant (P=0.31; Fig.
4).
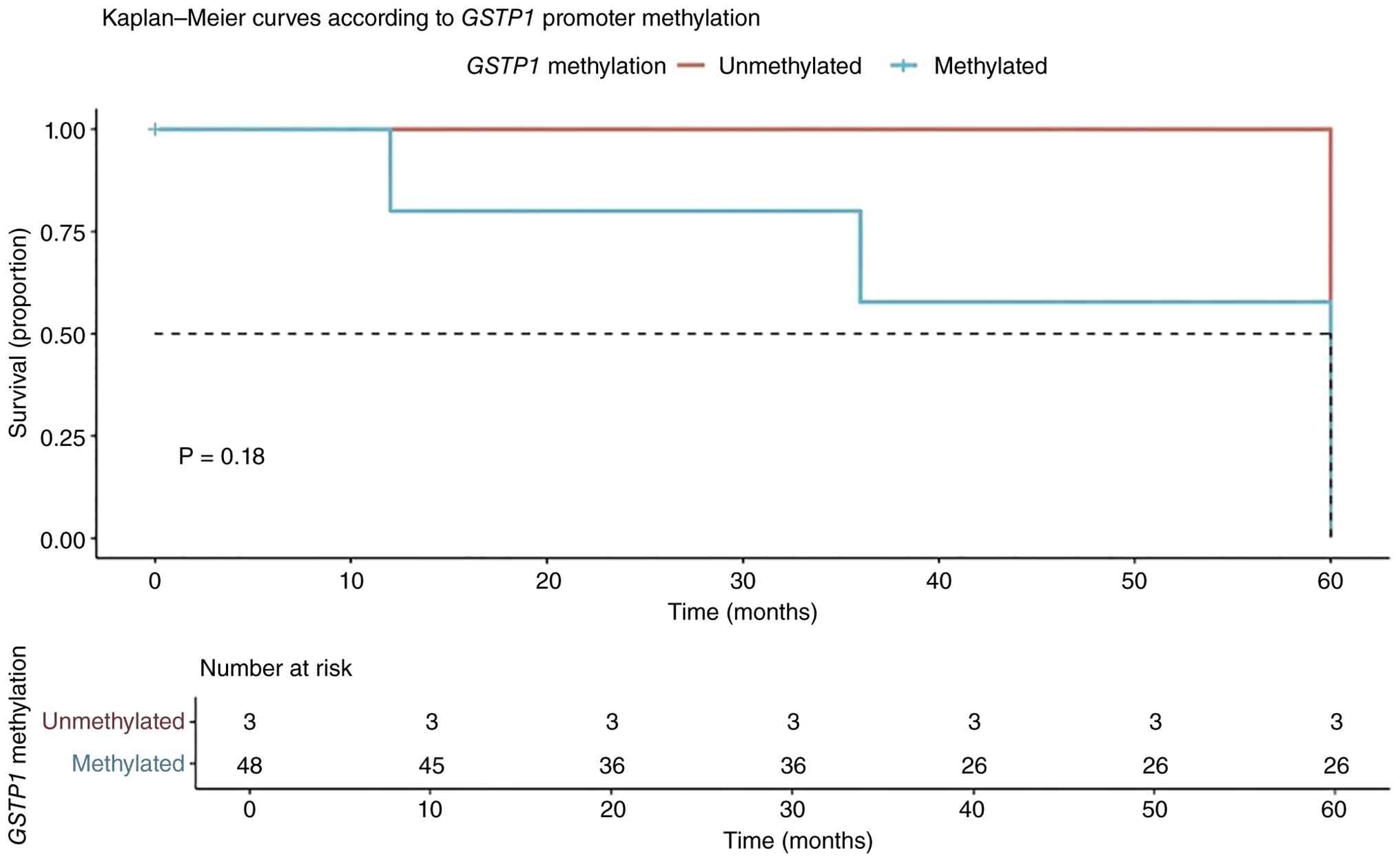
GTSP1 promoter methylation resulted in no
significant difference (P=0.18) in survival and progression time.
The median PFS was also calculated, with a time of 60 months
observed in both groups; therefore, there was no statistically
significant difference (P=0.18; Fig.
5).
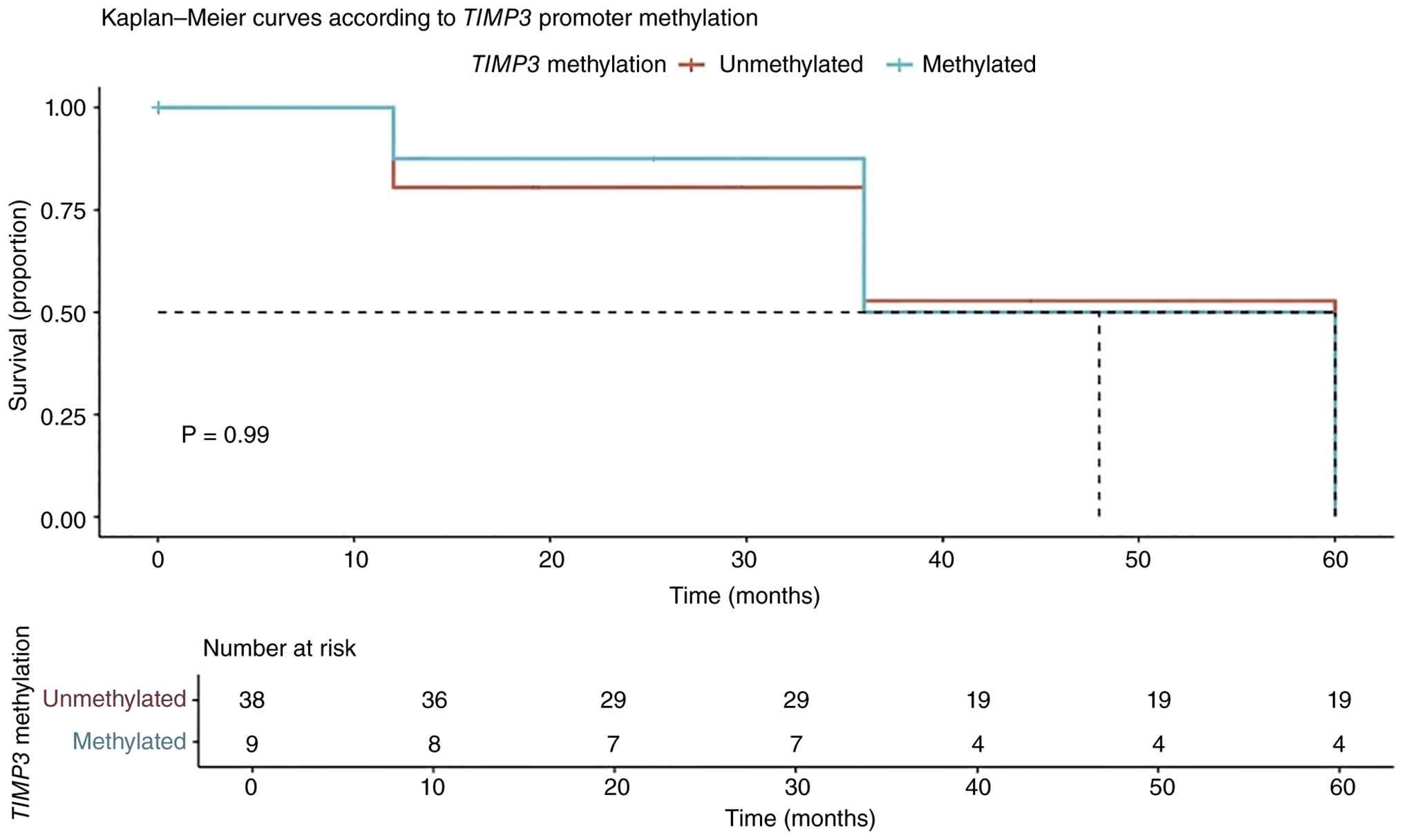
Lastly, TIMP3 promoter methylation resulted
in no significant difference (P=0.99) in survival and progression
time. The median PFS time was also calculated, which was 48 months
in the methylated group and 60 months in the unmethylated group.
This finding indicated that patients with TIMP3 promoter
methylation progressed slightly earlier (48 months) compared with
those without methylation (60 months). Although the methylated
group demonstrated a lower PFS trend, the difference between the
two groups was not statistically significant (P=0.99; Fig. 6).
Discussion
The main objective of the present study was to
analyze the methylation status of the BMP6, BRCA1, ESR2,
GSTP1 and TIMP3 genes in Mexican women with BC or BD and
the association with clinical and histopathological variables
associated with prognosis. The clinical and histopathological
variable results demonstrated that an age of ≥50 years conferred an
increased susceptibility to BC (OR, 5.44; 95% CI, 2.49–11.88;
P=0.00002). The average age was 55 vs. 42 years in the BC and BD
groups, respectively (P<0.00001). These findings were consistent
with those reported by Segovia-Alvarez et al (14) of an average age of 52.29 years for
BC cases and 42.81 years for the control group. In Mexican patients
with BC, age was associated with an OR of 5.75 (14), which is similar to the value
obtained in the present study (OR=5.44). This finding suggested
that women >50 years of age may have a >5-fold increased risk
of developing BC. These results were also consistent with data from
the U.S. National Cancer Institute (15), which reported that the average age
of women diagnosed with BC is ~50 years. The increased risk of
developing BC with advancing age can be explained by the
accumulation of genetic mutations and the decline in DNA repair
mechanisms over time (16).
In the present study, the BMI in the BC and BD
groups were 28.41 and 27.69 kg/m2, respectively, with no
significant difference (P=0.378), indicating an overweight BMI
classification for both groups. According to the Ministry of Health
of Mexico (17), ~70% of adults and
33% of children are overweight or obese, conditions that represent
notable risk factors for the development of chronic
non-communicable diseases, including diabetes mellitus type 2,
hypertension, dyslipidemia and cardiovascular or cerebrovascular
diseases such as ischemic heart disease or strokes. Since the
1980s, the prevalence of obesity in Mexico has demonstrated a
notable increase, currently affecting >30% of the adult
population. It has been estimated that by 2050, obesity rates will
reach 54% in men and 37% in women in Mexico, indicating that the
number of obese individuals will exceed those who are overweight.
This increase has mainly been attributed to a higher consumption of
high calorie foods and the adoption of more sedentary lifestyles.
Obesity is associated with various comorbidities, including
cardiovascular disease, type 2 diabetes mellitus, osteoarthritis,
certain types of cancer (such as breast, colorectal, pancreatic and
liver), obstructive sleep apnea and other health-related conditions
(18). Complications can arise
during BC disease progression when the patient is overweight or
obese. For example, several studies reported that obesity is a
major risk factor in the development and progression of BC
(19–21). Women with a BMI >25
kg/m2 have a higher risk of recurrence and lower
survival rates compared with those of normal weight (19). Furthermore, obesity can decrease the
effectiveness of chemotherapy even when the dose is correctly
adjusted for body weight and is associated with higher surgical
complications and a lower probability of breast reconstruction
(20). Obesity has also been
reported to increase the risk of developing BC after menopause and
is associated with higher mortality (21).
Adipose tissue serves an active role in the
pathophysiology of BC as it functions as an endocrine organ capable
of producing estrogens, adipokines (such as leptin and IL-6) and
proinflammatory factors (22).
Aromatase, an enzyme expressed by adipocytes, converts androgens
into estrogens, which promotes cell proliferation and tumor
progression, particularly in estrogen receptor (ER)+
tumors (22). Furthermore, adipose
tissue-derived stem cells may participate in the formation of
microcalcifications, which are associated with less favorable
prognoses, while insulin resistance and leptin secretion contribute
to tumor growth and metastasis (23). Although no significant differences
in BMI were observed between the groups analyzed in the present
study, these findings provide insight into how the interaction
between metabolism, inflammation and hormonal signaling may
influence the development and progression of BC. Lastly, it is key
to consider not only the specific BMI value, but also the duration
of obesity, to more fully understand its role in the clinical and
biological evolution of BC.
The present study evaluated the promoter methylation
status of the BMP6, BRCA1, ESR2, GSTP1 and TIMP3
genes in Mexican women with BC or BD. The findings highlighted
BRCA1 and TIMP3 as the genes with the most notable
clinical relevance. While BMP6, ESR2 and GSTP1 did
not demonstrate statistically significant associations, these genes
did demonstrate notable trends that may be further explored in
future research.
In the present study, the BRCA1 gene (a
caretaker tumor suppressor gene) exhibited a higher frequency of
methylation in the BC group (32.1%) compared with the BD group
(16.6%), a statistically significant difference (P=0.040). Several
studies have indicated that methylation in the promoter of the
BRCA1 gene decreases its expression (24,25).
Within the BRCA1 gene CpG sites region analyzed in the
present study (from −315 to +97) there is a CCAAT box
(position-173) (24); thus,
methylation occurring near these sites could interfere with gene
expression by interfering with the binding of transcription factors
[transcription factor II (TFII)D, TFIIB, TFIIF, TFIIE and TFIIH] to
the CCAAT box (25). In the present
study, this epigenetic event was associated with increased
susceptibility to BC (OR, 2.50; 95% CI, 1.02–6.42; P=0.0001).
Similar to previous studies that identified BRCA1
methylation was associated with risk, proliferation (Ki-67),
metastasis and aggressive phenotypes (7,26–32),
the present study identified a potential association with Ki-67
protein (P=0.057) and lymph node metastasis (P=0.059). The
frequency of BRCA1 methylation is reported to be between 2.7
and 65.2% in BC, although this percentage may vary depending on the
selection criteria of the group and the techniques used (26–32).
Lobanova et al (27)
reported that methylation of the BRCA1 gene promoter is
significantly associated with late-stage metastatic cancer (OR,
4.04; 95% CI, 1.19–13.65; P=0.038). Furthermore, high levels of
proliferation, as indicated by elevated Ki-67 protein, are reported
to associate with greater tumor aggressiveness and a worse
prognosis for patients with BRCA1 methylated compared with
unmethylated (32). Khan et
al (7) reported that lymphatic
vascular invasion, ductal carcinoma in situ and lymph node
metastasis (≥3) are observed at a higher rate in tumors with
BRCA1 methylation compared with healthy tissue. This finding
is particularly relevant, as BRCA1 inactivation by
methylation could have therapeutic implications in the selection of
patients who are candidates for poly-ADP ribose polymerase
inhibitors (33).
In the present study, the TIMP3 gene
(classified as a gatekeeper gene) demonstrated no significant
differences in methylation frequency between the BC (18.7%) and BD
(20%) groups. However, an association was observed between
TIMP3 gene methylation and the development of distant
metastasis (OR, 8.65; P=0.028), suggesting that epigenetic loss of
TIMP3 may promote metastasis through matrix dysregulation.
This may be due to methylation inhibiting gene function and
suppressing the regulation of angiogenesis and metastasis, which is
generally associated with greater tumor aggressiveness compared
with normal tissue (9). Although
the frequency of TIMP3 methylation was similar between the
BC and BD groups, the relationship with distant metastasis
suggested that this epigenetic event could be more relevant in
advanced stages of the disease.
Regarding the other genes analyzed in the present
study, although BMP6 demonstrated higher methylation in the
BC group (14.3%) compared with that in the BD group (3.6%), the
difference was not statistically significant (P=0.093), nor were
there any significant differences regarding BMP6 methylation
and the clinical and histopathological characteristics. In another
study conducted by our research group, BMP6 promoter
methylation was analyzed in women with BC (n=97) and BD (n=25) and
the study demonstrated that the percentage of methylation was
higher in the BC group (9.3%) compared with the BD group (4%)
(34). However, these differences
were not statistically significant either (P=0.365). The results of
the present study and that of García (34) are similar since no statistically
significant differences were reported in both studies examining
this same population of Mexican women; however, they differ from
European studies where notable methylation was reported in tumor
tissue (5,6).
Various environmental, dietary and lifestyle factors
can modify DNA methylation patterns and contribute to the
development of BC. Factors such as diet, alcohol and tobacco
consumption, exposure to pollutants, endocrine disruptors and
medication use can alter the activity of DNA methyltransferases,
the availability of methyl group donors and cellular redox balance
(35,36). Furthermore, ethnicity influences
methylation profiles, which may explain the differences in cancer
incidence and mortality among different population groups (35,37–39).
According to GLOBOCAN 2022 estimates, breast cancer was the most
commonly diagnosed cancer among women worldwide, with approximately
2.3 million new cases and 666,000 mortalities. The distribution of
the disease burden showed significant differences across
continents. Asia accounted for the highest number of new cases,
985,817 and mortalities, 315,309, followed by Europe, with 557,532
new cases and 144,439 mortalities. North America recorded 306,307
new cases and 49,744 mortalities, while Latin America and the
Caribbean reported 220,124 cases and 59,700 mortalities. Africa,
meanwhile, reported 198,553 new cases and 91,252 mortalities,
standing out for having the highest mortality-to-incidence ratio
among the regions evaluated, suggesting significant challenges in
accessing timely diagnosis and treatment. Finally, Oceania recorded
28,507 cases and 5,483 mortalities (35,37–40).
Diet serves a key role as nutrients such as folate,
vitamin B12, methionine and omega-3 fatty acids promote
methylation, while polyphenols and vitamin D can inhibit
methylation (36). Additionally,
comorbidities such as diabetes mellitus type 2 alter DNA
methylation by generating insulin resistance, chronic inflammation
and metabolic dysregulation, favoring the activation of oncogenes
and the inactivation of tumor suppressor genes (36).
The differences between the results of the present
study and those of García (34)
compared with those previously reported by Radpour et al
(5) and Barekati et al
(6) may be explained by
methodological factors. For example, Radpour et al (5) used matrix-assisted laser
desorption/ionization-time of flight mass spectrometry, Barekati
et al (6) used the
T-cleavage assay and mass spectrometry and García (34) used Sanger sequencing. Furthermore,
in the present study, BC tissue samples were compared with those
from women with BD, whereas Radpour and Barekati et al
(6) analyzed adjacent tissue. The
present study considered that adjacent tissue is not an adequate
control since, according to the tumor microenvironment theory,
there may be cancer cells involved in the development, invasion and
metastasis in this type of tissue (41).
In the present study, the ESR2 gene exhibited
frequent methylation (38.2% in the BC group vs. 28.3% in the BD
group) without reaching statistical significance (P=0.378) or
statistical significance with clinical and histopathological
characteristics. Silencing of ESR2 by methylation resulted
in decreased expression, not only in the early stages of BC
(42), but also in premalignant
stages, suggesting that ESR2 promoter methylation is a focal
event rather than a phenomenon that generally occurs in the breast
due to aging processes (43).
Although no statistically significant differences were observed
between the BC and BD groups in the present study, the high
frequency of ESR2 methylation suggested that this epigenetic
event occurs early during the transformation of the mammary
epithelium. The gatekeeper nature of ESR2 implies that it
could facilitate the proliferative imbalance that precedes invasive
cancer.
Lastly, in the present study, GSTP1 was the
gene with the highest overall methylation frequency (>90% in
both groups, BC and BD), with no statistically significant
differences (P=0.83). Although certain studies have proposed
GSTP1 methylation as a prognostic biomarker (44,45),
its clinical value was limited in the present study cohort. In the
present study, no relationship was observed between GSTP1
gene methylation and prognostic variables such as age, BMI,
progesterone receptor (PR), ER, clinical stage, Ki-67 protein
proliferation index or metastasis and progression.
Overall, the results of the present study
highlighted that BRCA1 and TIMP3 methylation had a
more evident clinical impact since BRCA1 was associated with
tumor susceptibility and aggressiveness, while TIMP3 to
metastatic risk. In the present cohort BMP6, ESR2 and
GSTP1 appear to be involved in specific stages or contexts
of tumor progression; however, without clear diagnostic or
prognostic value. These findings underscored the importance of
validating epigenetic biomarkers in specific populations and
suggested that the integration of BRCA1 and TIMP3
into predictive models could improve risk stratification and
therapy selection in BC.
A limitation of the present study is that
methylation status was assessed qualitatively using
methylation-specific PCR, based on the presence or absence of bands
on agarose gels, and the lack of confirmatory tests on all samples,
such as DNA sequencing or bisulfite pyrosequencing. Gel
interpretation was not conducted under blinded conditions, which
may introduce potential observer bias. However, this approach is
extensively used for the detection of methylation patterns,
although it does not provide quantitative information on
methylation levels.
Another limitation of the present study is the lack
of availability of relevant gynecological and obstetric variables
in the present study cohort, including reproductive history, parity
and use of hormonal therapy. These factors may act as confounders
and could influence DNA methylation patterns as well as clinical
outcomes. The absence of these variables may have affected the
assessment of the association between methylation status and the
analyzed outcomes. Despite this, key clinical variables such as
age, BMI, molecular subtype, ER and PR status, clinical stage,
Ki-67 proliferation index and the presence of distant and lymph
node metastasis were included as covariates in the binary logistic
regression models to partially control for confounding.
In conclusion, the methylation status of the
BMP6, BRCA1, ESR2, GSTP1 and TIMP3 genes was
evaluated in women with BC or BD in the present study to determine
the association with poor prognosis. Only the BRCA1 gene
exhibited a significantly higher frequency of methylation in women
with BC (32.1%) compared with BD (16.6%) (P=0.040), particularly in
the triple-negative subtype and methylation demonstrated a
potential association with cell proliferation Ki-67 (P=0.057) and
lymph node metastasis (P=0.059). Methylation of the TIMP3
gene was associated with up to an eight-fold increased risk of
distant metastasis, indicating that both the BRCA1 and
TIMP3 genes could be prognostic biomarkers. Methylation of
the BMP6, ESR2 and GSTP1 genes did not exhibit
statistically significant differences between the BC and BD groups,
nor with the examined clinical and pathological characteristics,
which may be due to interindividual variability, cell selection,
technique sensitivity or confounding factors such as reproductive
history. These results highlighted the potential utility of
BRCA1 and TIMP3 methylation as prognostic biomarkers
and the need for further research into DNA methylation as a
diagnostic and therapeutic tool in BC.
Acknowledgements
Not applicable.
Funding
Financial support for the present study was received from the
Mexican Social Security Institute in accordance with the Mexican
Social Security Institute call for proposals for the 2023 fiscal
year on Priority health issues, vulnerable populations and emerging
issues (grant no. R-2023-1305-024). Samantha Rebeca de la
Torre-Guzmán and Carolina Vázquez Gastélum received scholarships
from the Consejo Nacional de Ciencia y Tecnología (CONACYT),
Mexico.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
SRDLTG contributed to conception and design, data
acquisition, data analysis and interpretation, manuscript drafting
and reviewing of key intellectual content. AMGM contributed to
sampling, clinical data collection and analysis. BPC contributed to
sampling and clinical data collection. CVG contributed to data
analysis, manuscript drafting and interpretation. MPGA contributed
to data interpretation and statistical analysis. ESR contributed to
data analysis and interpretation. SOMC contributed to analysis and
interpretation of clinical and experimental data and sample
collection. JYSL contributed to conception and design and reviewing
of key intellectual content. SRDLTG and JYSL confirm the
authenticity of all the raw data. All authors contributed to
editorial changes in the manuscript. All authors have participated
sufficiently in the work and agreed to be accountable for all
aspects of the work. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The present study was conducted in accordance with
the Declaration of Helsinki and was approved by the Institutional
Review Board (Ethics Committee 1305) of Western Biomedical Research
Center (approval no. R-2023-1305-024; Guadalajara, Mexico) for
studies involving humans. All participants were invited to take
part in the study and signed informed consent forms at the Breast
Clinic of the Mexican Social Security Institute in Guadalajara
(Mexico).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
World Health Organization (WHO), . Breast
cancer. WHO; Geneva: 2025 October 28–2025https://www.who.int/news-room/fact-sheets/detail/breast-cancer
|
|
2
|
American Cancer Society, . Breast Cancer.
American Cancer Society; Hagerstown, MD: 2025 October
28–2025https://www.cancer.org/cancer/types/breast-cancer.html
|
|
3
|
Provenzano E, Ulaner GA and Chin SF:
Molecular classification of breast cancer. PET Clin. 13:325–338.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Vietri MT, D'Elia G, Benincasa G, Ferraro
G, Caliendo G, Nicoletti GF and Napoli C: DNA methylation and
breast cancer: A way forward. Int J Oncol. 59:982021. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Radpour R, Kohler C, Haghighi MM, Fan AX,
Holzgreve W and Zhong XY: Methylation profiles of 22 candidate
genes in breast cancer using high-throughput MALDI-TOF mass array.
Oncogene. 28:2969–2978. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Barekati Z, Radpour R, Lu Q, Bitzer J,
Zheng H, Toniolo P, Lenner P and Zhong XY: Methylation signature of
lymph node metastases in breast cancer patients. BMC Cancer.
12:2442012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Khan F, Agarwal P, Gupta S, Maurya MK,
Singh P, Agarwal A, Singh K, Sonkar AA and Goel MM: BRCA1 promoter
methylation and its immunohistochemical correlation in sporadic
breast cancer. Indian J Med Res. 158:47–54. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kent WJ, Sugnet CW, Furey TS, Roskin KM,
Pringle TH, Zahler AM and Haussler D: The human genome browser at
UCSC. Genome Res. 12:996–1006. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Radpour R, Barekati Z, Kohler C, Lv Q,
Burki N, Diesch C, Bitzer J, Zheng H, Schmid S and Zhong XY:
Hypermethylation of tumor suppressor genes involved in critical
regulatory pathways for developing a blood-based test in breast
cancer. PLoS One. 6:e160802011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cui J, Li G, Yin J, Li L, Tan Y, Wei H,
Liu B, Deng L, Tang J, Chen Y and Yi L: GSTP1 and cancer:
Expression, methylation, polymorphisms and signaling (Review). Int
J Oncol. 56:867–878. 2020.PubMed/NCBI
|
|
11
|
Pongtheerat T, Pakdeethai S, Purisa W,
Chariyalertsak S and Petmitr S: Promoter methylation and genetic
polymorphism of glutathione S-transferase P1 gene (GSTP1) in Thai
breast cancer patients. Asian Pac J Cancer Prev. 12:2731–2734.
2011.PubMed/NCBI
|
|
12
|
Lui EL, Loo WT, Zhu L, Cheung MN and Chow
LW: DNA hypermethylation of TIMP3 gene in invasive breast ductal
carcinoma. Biomed Pharmacother. 59 (Suppl 2):S363–S365. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Breastcancer.orgThe Breast Imaging Reporting and Data
System (BI-RADS). Available from:. https://www.breastcancer.org/screening-testing/mammograms/bi-rads-resultsJune
19–2026
|
|
14
|
Segovia-Alvarez G, Bonfil-Rodriguez MI,
Valdivieso-Contreras L and Flores-Villegas J: Risk factors
associated in breast cancer patients Mexico 2023. Br J Psychol Res.
11:59–70. 2023. View Article : Google Scholar
|
|
15
|
National Cancer Institute (NCI), . Large
study verifies cancer risk for women carrying BRCA1 or BRCA2
mutations. NCI; Maryland: 2025 October 28–2025https://www.cancer.gov/news-events/cancer-currents-blog/2017/brca-mutation-cancer-risk
|
|
16
|
Blokzijl F, de Ligt J, Jager M, Sasselli
V, Roerink S, Sasaki N, Huch M, Boymans S, Kuijk E, Prins P, et al:
Tissue-specific mutation accumulation in human adult stem cells
during life. Nature. 538:260–264. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Shamah-Levy T, Lazcano-Ponce EC,
Cuevas-Nasu L, Romero-Martínez M, Gaona-Pineda EB, Gómez-Acosta LM,
Mendoza-Alvarado LR and Méndez-Gómez-Humarán I: Encuesta Nacional
de Salud y Nutrición Continua 2023. Resultados Nacionales.
Instituto Nacional de Salud Pública; Cuernavaca, México: 2024,
https://insp.mx/resources/images/stories/2025/docs/250108_Ensanut_23.pdfJune
19–2026(In Spanish).
|
|
18
|
Pati S, Irfan W, Jameel A, Ahmed S and
Shahid RK: Obesity and cancer: A current overview of epidemiology,
pathogenesis, outcomes, and management. Cancers (Basel).
15:4852023. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Nguyen HL, Geukens T, Maetens M, Aparicio
S, Bassez A, Borg A, Brock J, Broeks A, Caldas C, Cardoso F, et al:
Obesity-associated changes in molecular biology of primary breast
cancer. Nat Commun. 14:44182023. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lee K, Kruper L, Dieli-Conwright CM and
Mortimer JE: The impact of obesity on breast cancer diagnosis and
treatment. Curr Oncol Rep. 21:412019. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Bhardwaj P, Au CM, Benito-Martin A,
Ladumor H, Oshchepkova S, Moges R and Brown KA: Estrogens and
breast cancer: Mechanisms involved in obesity-related development,
growth and progression. J Steroid Biochem Mol Biol. 189:161–170.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Rybinska I, Agresti R, Trapani A,
Tagliabue E and Triulzi T: Adipocytes in breast cancer, the thick
and the thin. Cells. 9:5602020. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Aguilera-Eguia RA, Roco Videla A,
Lopez-Soto OP, Herrera-Serna B and Fuentes-Barria H: Impact of
adipose tissue on the development and progression of breast cancer:
A crucial perspective. Nutrición Hospitalaria. 41:5182024.(In
Spanish). PubMed/NCBI
|
|
24
|
EPD, . The Eukaryotic Promoter Database.
October 28–2025https://epd.expasy.org/epd/
|
|
25
|
Deng G, Song GA, Pong E, Sleisenger M and
Kim YS: Promoter methylation inhibits APC gene expression by
causing changes in chromatin conformation and interfering with the
binding of transcription factor CCAAT-binding factor. Cancer Res.
64:2692–2698. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Vu TL, Nguyen TT, Doan VTH and Vo LTT:
Methylation profiles of BRCA1, RASSF1A and GSTP1 in Vietnamese
women with breast cancer. Asian Pac J Cancer Prev. 19:1887–1893.
2018.PubMed/NCBI
|
|
27
|
Lobanova O, Medvedieva N, Fishchuk L,
Dubitska O, Cheshuk V, Vereshchako R, Zakhartseva L, Rossokha Z and
Gorovenko N: Methylation of promoter region of BRCA1 gene versus
pathogenic variants of gene: Risk factor or clinical marker of
breast cancer. Breast Cancer Res Treat. 196:505–515. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Hassani H, Talaiezadeh A, Tahmasebi
Birgani M and Bijanzadeh M: Evaluation of BRCA1 gene promoter
methylation status in sporadic breast cancer patients in southwest
of Iran. Asian Pac J Cancer Prev. 24:811–817. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Jagtap SV and Jagtap SS: Methylation of
BRCA1 promoter in sporadic breast cancer. Indian J Med Res.
158:85–87. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Li Q, Wei W, Jiang YI, Yang H and Liu J:
Promoter methylation and expression changes of BRCA1 in cancerous
tissues of patients with sporadic breast cancer. Oncol Lett.
9:1807–1813. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Hsu NC, Huang YF, Yokoyama KK, Chu PY,
Chen FM and Hou MF: Methylation of BRCA1 promoter region is
associated with unfavorable prognosis in women with early-stage
breast cancer. PLoS One. 8:e562562013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Oubaddou Y, Oukabli M, Fenniche S,
Elktaibi A, Elochi MR, Al Bouzidi A, Qmichou Z, Dakka N, Diorio C,
Richter A, et al: BRCA1 promoter hypermethylation in malignant
breast tumors and in the histologically normal adjacent tissues to
the tumors: Exploring its potential as a biomarker and its clinical
significance in a translational approach. Genes (Basel).
14:16802023. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Panagopoulou M, Panou T, Gkountakos A,
Tarapatzi G, Karaglani M, Tsamardinos I and Chatzaki E: BRCA1 &
BRCA2 methylation as a prognostic and predictive biomarker in
cancer: Implementation in liquid biopsy in the era of precision
medicine. Clin Epigenetics. 16:1782024. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
García AM: Evaluation of the methylation
status of the BMP6 gene promoter in breast tissue and serum levels
of BMP6 protein in Mexican women with breast cancer (unpublished
PhD thesis) (In Spanish). Universidad de Guadalajara; 2023
|
|
35
|
Liu J, Huang B, Ding F and Li Y:
Environment factors, DNA methylation, and cancer. Environ Geochem
Health. 45:7543–7568. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Maleknia M, Ahmadirad N, Golab F, Katebi Y
and Haj Mohamad Ebrahim Ketabforoush A: DNA methylation in cancer:
Epigenetic view of dietary and lifestyle factors. Epigenet
Insights. 16:251686572311998932023. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Duthie SJ: Epigenetic modifications and
human pathologies: Cancer and CVD. Proc Nutr Soc. 70:47–56. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Kader F and Ghai M: DNA methylation-based
variation between human populations. Mol Genet Genomics. 292:5–35.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Domingo-Relloso A, Huan T, Haack K,
Riffo-Campos AL, Levy D, Fallin MD, Terry MB, Zhang Y, Rhoades DA,
Herreros-Martinez M, et al: DNA methylation and cancer incidence:
lymphatic-hematopoietic versus solid cancers in the Strong Heart
Study. Clin Epigenetics. 13:432021. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Ferlay J, Ervik M, Lam F, Laversanne M,
Colombet M, Mery L, Piñeros M, Znaor A, Soerjomataram I and Bray F:
Global Cancer Observatory: Cancer Today. International Agency for
Research on Cancer; Lyon: 2024, https://gco.iarc.who.int/media/globocan/factsheets/cancers/20-breast-fact-sheet.pdfMay
29–2026
|
|
41
|
Elhanani O, Ben Uri R and Keren L: Spatial
profiling technologies illuminate the tumor microenvironment.
Cancer Cell. 41:404–420. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Daraei A, Izadi P, Khorasani G, Nafissi N,
Naghizadeh MM, Meysamie A, Mansoori Y, Nariman-Saleh-Fam Z, Bastami
M, Saadatian Z, et al: A methylation signature at the CpG island
promoter of estrogen receptor beta (ER-β) in breasts of women may
be an early footmark of lack of breastfeeding and nulliparity.
Pathol Res Pract. 218:1533282021. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Zhu X, Leav I, Leung YK, Wu M, Liu Q, Gao
Y, McNeal JE and Ho SM: Dynamic regulation of estrogen
receptor-beta expression by DNA methylation during prostate cancer
development and metastasis. Am J Pathol. 164:2003–2012. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Arai T, Miyoshi Y, Kim SJ, Taguchi T,
Tamaki Y and Noguchi S: Association of GSTP1 CpG islands
hypermethylation with poor prognosis in human breast cancers.
Breast Cancer Res Treat. 100:169–176. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Song B, Wang L, Zhang Y, Li N, Dai H, Xu
H, Cai H and Yan J: Combined detection of HER2, Ki67, and GSTP1
genes on the diagnosis and prognosis of breast cancer. Cancer
Biother Radiopharm. 34:85–90. 2019.PubMed/NCBI
|