Introduction
Gastric cancer (GC) continues to impose a
substantial burden on global health. Although notable advances have
been made in elucidating the molecular and cellular events
underlying its onset and progression, this malignancy remains among
the top five causes of cancer-related deaths worldwide (1). Striking geographical disparities exist
in its distribution, with particularly elevated rates in Eastern
populations, where dietary patterns, chronic inflammation linked to
Helicobacter pylori infection, and inherited genetic
alterations exert major influences on disease development (2). Because early clinical manifestations
are often absent or obscure, numerous individuals present with
advanced disease (3,4).
Surgery remains the primary treatment approach for
GC, supplemented with by chemotherapy or radiotherapy when
necessary. However, even with standardized interventions, long-term
prognosis is frequently unfavorable owing to substantial biological
heterogeneity and high recurrence rates (5). Although the American Joint Committee
on Cancer staging framework offers a widely adopted prognostic
reference, marked variability in survival among patients classified
within the same pathological stage highlights its limitations. This
inconsistency underscores the need for additional prognostic
metrics capable of refining risk assessment and supporting more
personalized clinical decision-making.
Chronic systemic inflammation, now recognized as a
defining hallmark of malignant disease, drives multiple aspects of
tumor biology, including initiation, progression and metastatic
spread, through intricate interactions between immune effector
mechanisms and tumor-associated microenvironments (6). Building on this biological axis,
numerous studies have emphasized the prognostic utility of
inflammation-derived indices such as the neutrophil-to-lymphocyte
ratio (NLR), the platelet-to-lymphocyte ratio (PLR) and the
C-reactive protein-to-albumin ratio (CAR), in various human
cancers, including GC (7–9). These markers are attracting increased
attention because they can be readily obtained, are cost-effective,
and integrate both immune and inflammatory states. Ideally,
prognostic indicators should not only predict patient outcomes but
also provide guidance for perioperative decisions, treatment
stratification, and surveillance planning.
Within the category of inflammation-based indices,
the lymphocyte-to-C-reactive protein ratio (LCR) has recently
emerged as a promising candidate. Okugawa et al (6) reported that LCR mirrors both
postoperative and oncological outcomes in colorectal malignancies,
suggesting its broader relevance as a composite index reflecting
immune status, nutritional condition and systemic inflammation
(6). Because lymphocyte activity
and CRP-driven inflammatory signaling are tightly related to tumor
progression, this ratio may capture host-tumor dynamics more
effectively than single-component biomarkers.
Despite these encouraging observations, no
meta-analysis has consolidated the prognostic implications of LCR
in GC. The absence of synthesized evidence hinders the clinical
integration of LCR and limits consensus on the potential role
across different treatment settings. Therefore, a systematic
evaluation is essential to quantify the association of LCR with
survival endpoints and determine whether it can serve as a
standardized prognostic indicator in GC. This evaluation can
strengthen risk stratification paradigms and support more refined
therapeutic planning for this highly aggressive malignancy.
Guided by these considerations, a comprehensive
meta-analysis was performed to investigate the prognostic
significance of circulating LCR in patients with GC. The aim of the
present study was to generate robust evidence that clarifies the
practicality and clinical relevance of this easily obtainable
biomarker and to assess whether it can enhance existing prognostic
systems and facilitate individualized patient management.
Materials and methods
Literature search and study selection
criteria
The present systematic review was undertaken in full
alignment with the PRISMA guidelines for reporting meta-analyses
and systematic syntheses (10). The
protocol of the present meta-analysis was not prospectively
registered in PROSPERO or any other registry. To capture all
relevant evidence, a comprehensive search of PubMed (https://pubmed.ncbi.nlm.nih.gov/), EMBASE
(https://www.embase.com/) and the Cochrane Library
(https://www.cochrane.org/) was
performed, encompassing studies published up to November 18, 2025.
The retrieval strategy employed predetermined terms related to the
LCR ratio. The PubMed search strategy was as follows:
[Lymphocyte-to-C-reactive protein ratio(Title/Abstract)] OR
[Lymphocyte-C-reactive protein ratio(Title/Abstract)] OR
[Lymphocyte/C-reactive protein ratio(Title/Abstract)] OR
[Lymphocyte-to-CRP ratio(Title/Abstract)] OR [Lymphocyte-CRP
ratio(Title/Abstract)] OR [Lymphocyte/CRP ratio(Title/Abstract)].
This strategy was adapted appropriately for EMBASE and the Cochrane
Library according to the syntax and indexing rules of each
database. Furthermore, the reference lists of included articles
were manually screened to identify any additional work not detected
through database queries. To reduce selection bias, two reviewers
independently evaluated the literature, and disagreements were
adjudicated by consultation with a senior investigator.
Studies were included if they met the following
criteria: i) Studies specifically investigating patients with GC,
as defined according to the diagnostic criteria used in the
original reports; ii) studies evaluating the prognostic
significance of pretreatment LCR, with LCR analyzed as a
dichotomized variable; iii) studies reporting survival outcomes,
including overall survival (OS) and/or disease-free survival (DFS);
and iv) studies providing hazard ratios (HRs) with corresponding
95% confidence intervals (CIs), or sufficient data from which these
estimates could be obtained. No additional restriction was imposed
regarding explicit histological confirmation beyond the diagnostic
criteria reported in the original studies. In addition, no minimum
follow-up duration was required, provided that extractable survival
data were available.
Data extraction and quality
evaluation
For each study that met the inclusion criteria, all
pertinent information was systematically gathered, including the
leading author, publication year, duration of the study period,
geographical setting, therapeutic modalities applied, overall
cohort size, and fundamental demographic variables such as age
distribution and sex composition. The thresholds used to categorize
LCR values in individual reports were also recorded. When
available, HRs with corresponding 95% CIs were preferentially
extracted from multivariate Cox regression models to minimize the
influence of potential confounding. If multivariate estimates were
not available, univariate HRs were extracted. When HRs and 95% CIs
were not reported directly but Kaplan-Meier survival curves were
available, the log HR and its standard error were estimated using
the established methods described by Tierney et al (11). Survival probabilities, numbers at
risk, total events and log-rank information were extracted when
available to reconstruct the corresponding HR estimates.
Multivariate estimates were prioritized over reconstructed or
univariate estimates in the quantitative synthesis. When a single
publication reported more than one independent and non-overlapping
cohort with separately available survival estimates, each cohort
was extracted and analyzed as an independent dataset. Specifically,
Xiong et al (12) reported
both a discovery cohort and a validation cohort, which were treated
as two separate cohorts in the quantitative synthesis because they
included distinct patient populations and provided separate
prognostic data (12).
The methodological robustness of the included
observational studies was appraised using the Newcastle-Ottawa
Scale (NOS), a widely accepted instrument for evaluating potential
bias in non-randomized cohort and case-control research (13,14).
Investigations earning six or more points on this scale were
regarded as having satisfactory methodological rigor. Data
extraction and quality assessment were independently performed and
cross-verified by two authors, with any discrepancies resolved by a
senior investigator.
Statistical methods
All quantitative analyses were performed with Stata
(version 18.0; StataCorp LP), and the pooled estimates were
illustrated using forest diagrams. To evaluate variability across
studies, Cochran's Q statistic was applied together with the
I2 metric; heterogeneity was regarded as meaningful when
the I2 value was greater than 50% or when the Q test
yielded a P-value below 0.1 (15).
When substantial divergence among studies was detected, the
DerSimonian-Laird random-effects approach was adopted. By contrast,
datasets exhibiting minimal heterogeneity were synthesized using a
fixed-effects framework based on inverse-variance weighting. To
evaluate whether variations in LCR thresholds influenced the pooled
estimates, an exploratory subgroup analysis was performed according
to the median cut-off value reported by the included studies.
Because no universally accepted LCR threshold has been established
for GC, this analysis was considered exploratory.
Potential publication bias was assessed using Begg's
rank-based test and Egger's regression methodology (15). To determine the stability of the
synthesized effect estimates, sensitivity analyses were performed,
in which each study was removed one at a time before recalculating
the pooled HRs. Statistical significance was defined by a two-sided
P-value of 0.05.
Results
Literature search results
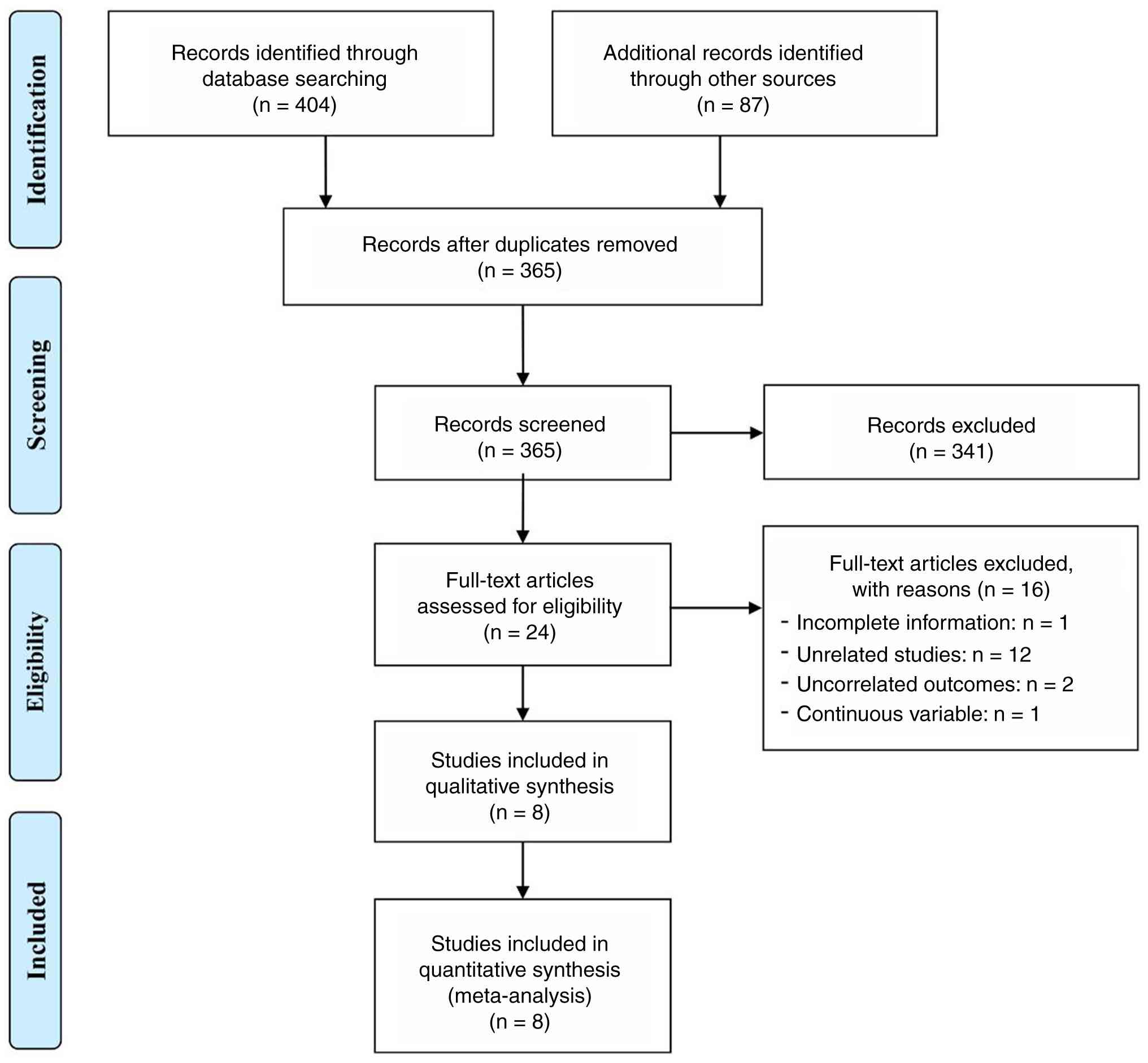
A comprehensive literature search in multiple
electronic databases, complemented by manual screening of reference
lists, yielded 491 articles. After the elimination of 126
duplicates, the remaining articles were evaluated at the title and
abstract levels, leading to the exclusion of 341 articles that did
not fulfill the established selection criteria. Full-text review
was subsequently performed for 24 articles, of which 15 were
removed because they did not meet the eligibility requirements
related to study design, participant characteristics, or reporting
of survival endpoints. In total, eight publications comprising nine
independent cohorts were included in the quantitative synthesis
(12,16–22)
(Fig. 1). Of note, Xiong et
al (12) reported two
independent cohorts, a discovery cohort and a validation cohort,
which were analyzed separately because the patient populations were
non-overlapping and survival estimates were reported
independently.
Characteristics of the included
studies
A comprehensive summary of the principal features of
the included studies is presented in Table I. Altogether, the nine included
studies contributed data from 4,429 patients with GC, with
individual cohort sizes ranging between 123 and 774 participants.
In terms of geographic distribution, four studies were performed in
China, four in Japan, and one in Türkiye. This distribution
highlights the regional pattern of currently available
evidence.
 | Table I.Main characteristics of the studies
included. |
Table I.
Main characteristics of the studies
included.
| First author,
year | Country | Number | Age, years | Male/female, n | Stage
information | Treatments | During the
study | Cut-off | NOS score | (Refs.) |
|---|
| Matsunaga et
al, 2023 | Japan | 101 | 65.1±11.0 | 79/22 | - | Chemotherapy |
01/2017-04/2022 | 13895 | 7 | (19) |
| Aoyama et
al, 2022 | Japan | 480 | 68
(32–90)b | 318/162 | - | Gastrectomy | 2013-2017 | 7000 | 8 | (17) |
| Wang et al,
2025 | China | 763 | 59.1±11.9 | 534/229 | TNM stage
I/II/III/IV: 64/149/274/276 | NA |
04/2013-12/2022 | 6452 | 6 | (22) |
| Xiong et al,
2022 (Discovery cohort) | China | 774 | 62.3
(57–70)a | 639/135 | TNM stage I/II/III:
157/243/374 | Gastrectomy |
04/2011-02/2016 | 6000 | 7 | (12) |
| Xiong et al,
2022 (Validation cohort) | China | 575 | ≥65/<65:
274/301 | 439/136 | TNM stage
I–III | Gastrectomy |
03/2016-09/2019 | 6000 | 7 | (12) |
| Miyatani et
al, 2022 | Japan | 455 | ≥75/<75:
157/298 | 332/123 | Stage I/II–III:
307/148 | Gastrectomy | 2005-2018 | 23800 | 7 | (20) |
| Angin et al,
2021 | Türkiye | 123 | 65.4±10.2 | 83/40 | - | Gastrectomy |
01/2010-12/2015 | 1931 | 6 | (16) |
| Okugawa et
al, 2019 | Japan | 551 | 65.4
(18–90)b | 387/164 | TNM stage
I/II/III/IV: 296/86/87/82 | Gastrectomy | 2001-2011 | 8350 | 7 | (21) |
| Cheng et al,
2020 | China | 607 | - | 196/411 | T1-T4 | Gastrectomy |
01/2013-06/2019 | 6300 | 7 | (18) |
Regarding treatment context, seven studies focused
specifically on patients undergoing surgical treatment, whereas the
remaining two studies included individuals receiving multimodal
therapy. All studies adopted a retrospective observational
framework, a design that, despite certain inherent constraints,
enabled the extraction of detailed clinical information and
laboratory parameters.
Quality assessment based on the NOS yielded scores
ranging from 6 to 8, suggesting a generally low risk of bias and
reinforcing confidence in the robustness of the synthesized
findings. Overall, these study characteristics reflect high
methodological quality and provide essential context for
interpreting subsequent meta-analysis results.
Pooled analysis of the association
between LCR and OS
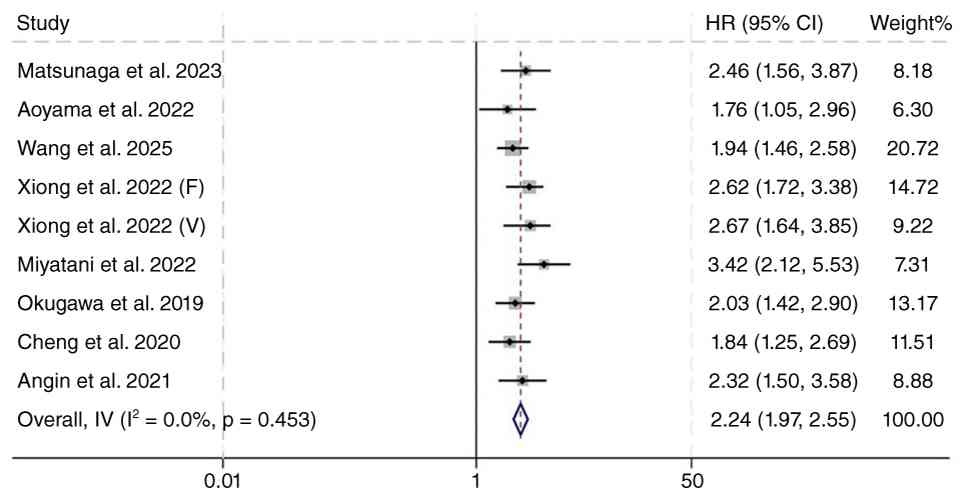
A total of nine studies fulfilled the eligibility
criteria, contributing data from 4,429 individuals diagnosed with
GC. In each dataset, patients were categorized into high- and
low-LCR groups based on the cut-off values specified in the
respective studies. When these data were synthesized, a pronounced
survival disadvantage emerged for individuals with reduced LCR
values. The pooled hazard ratio for OS was 2.24 (95% CI, 1.97–2.55;
P<0.001), indicating that the mortality risk in low-LCR patients
was more than twice that in high-LCR patients (Fig. 2).
To assess the consistency of these findings across
studies, heterogeneity was examined using both Cochran's Q
statistic and the I2 index. Neither metric suggested
meaningful variability: The Q test showed no statistical
significance, and the I2 value was 0% (P=0.453). This
absence of detectable heterogeneity suggested that the effect
estimates were highly concordant among included analyses.
Consequently, a fixed-effects modeling approach was selected as the
most appropriate framework for deriving the final pooled
results.
Sensitivity analysis and publication
bias of the association between LCR and OS
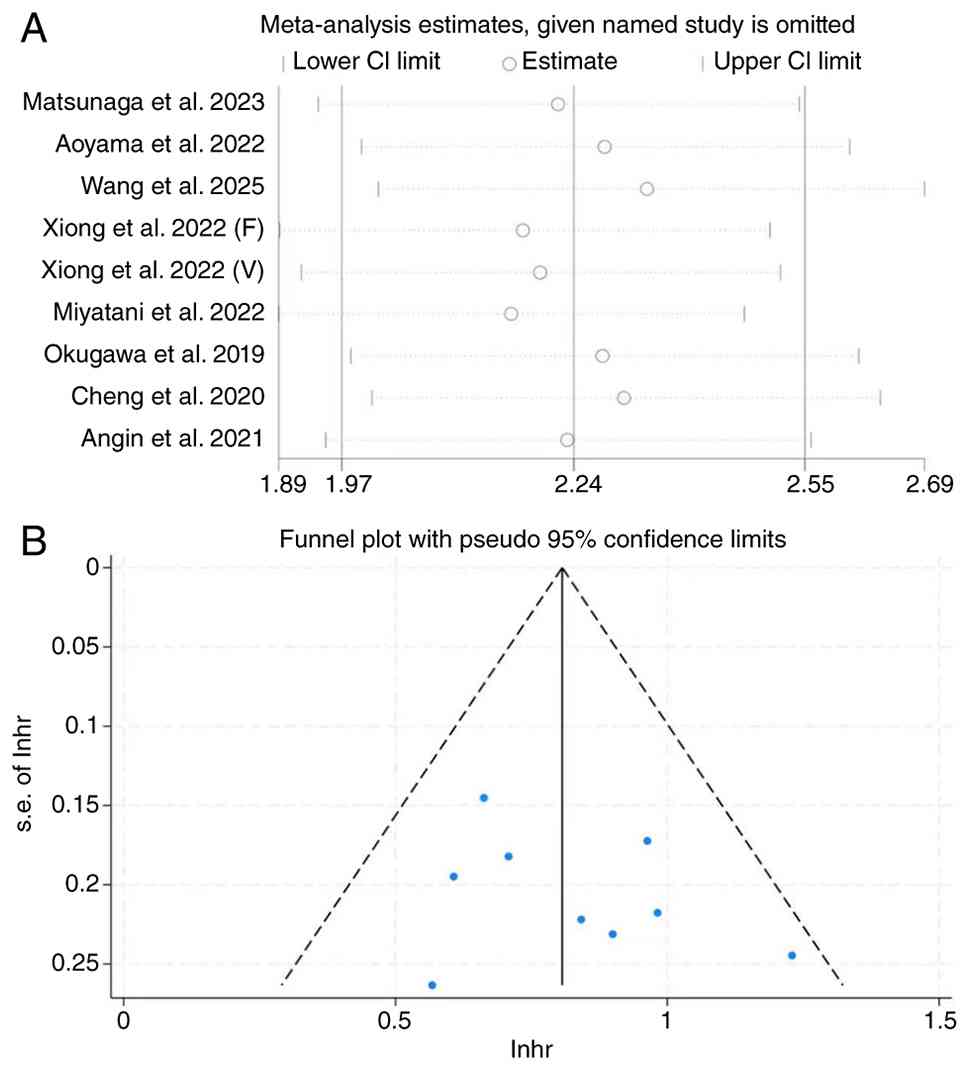
To evaluate the robustness of the pooled effect, a
leave-one-out sensitivity analysis was conducted, in which each
study was removed sequentially and the overall HR recalculated.
This procedure tested whether any single dataset disproportionately
affected the combined estimate. The results showed that the
exclusion of individual studies produced negligible changes in both
effect size and direction, indicating strong internal consistency
across the included analyses (Fig.
3A). Although minor fluctuations were observed, the overall
pattern remained stable. Removing the study by Miyatani et
al (20) produced the lowest
risk estimate (HR=2.16; 95% CI: 1.89–2.50; P<0.001), whereas
omission of the dataset from Wang et al (22) resulted in the highest estimate
(HR=2.33; 95% CI: 2.01–2.69; P<0.001). Importantly, all
recalculated values were directionally aligned and statistically
significant, demonstrating that no single investigation materially
shaped the final outcome. Collectively, these findings confirm that
the observed association between low LCR levels and unfavorable OS
in GC is highly robust and not driven by outlier studies. This
reinforces the methodological reliability of the quantitative
synthesis.
To further evaluate potential distortions arising
from selective publication, Begg's rank correlation and Egger's
regression tests were applied. Neither test identified significant
evidence of bias, with P-values of 0.466 and 0.350, respectively.
This conclusion was supported by the symmetrical appearance of the
funnel plot, which likewise indicated the absence of
publication-related skewness (Fig.
3B).
Subgroup analyses of the association
between LCR and OS
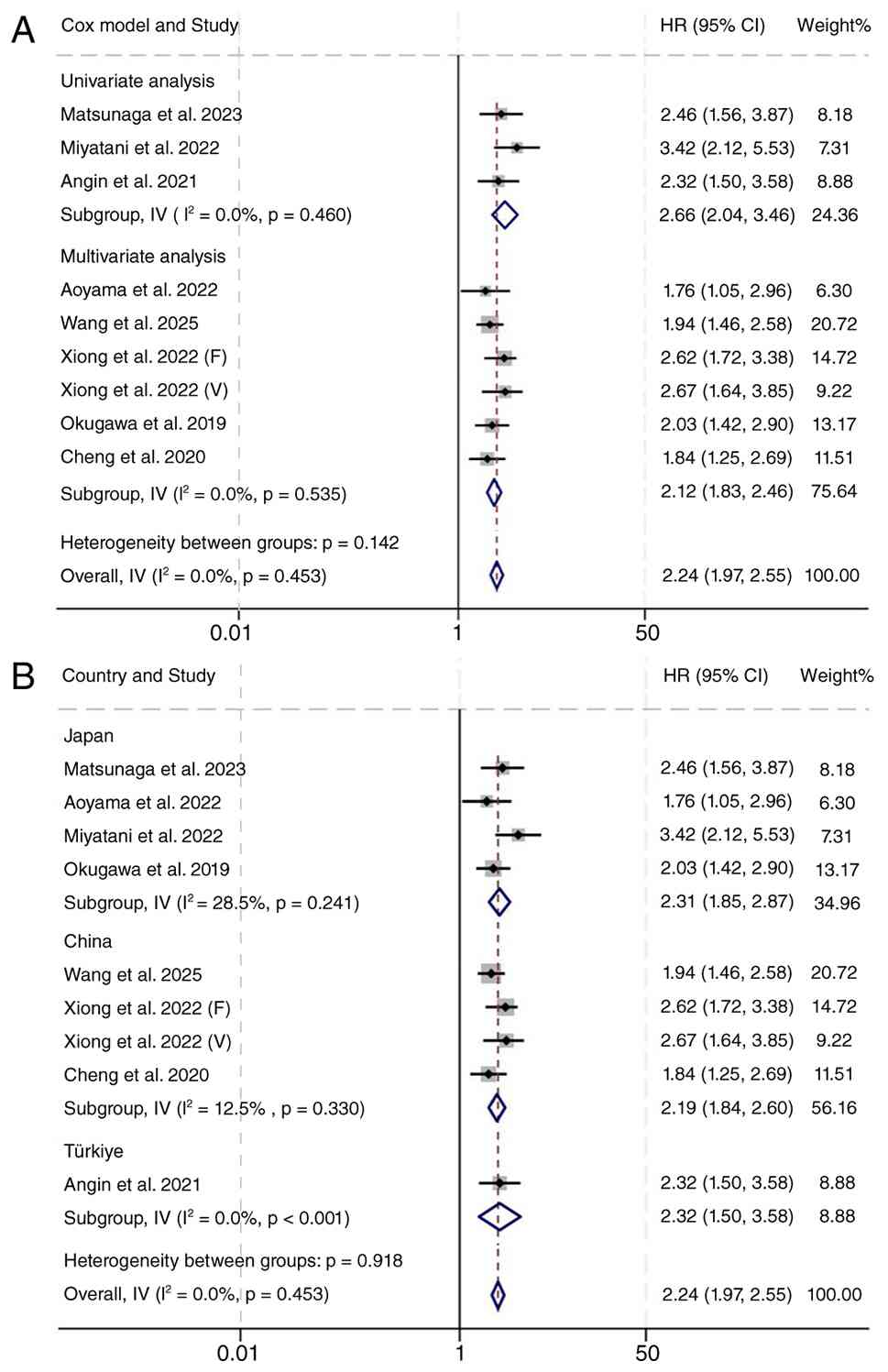
To determine whether the prognostic value of LCR was
influenced by analytical approach, region, or treatment strategy, a
series of predefined subgroup analyses were performed. When
stratified by the source of effect estimates, the association
between reduced LCR and adverse OS remained highly consistent.
Effect sizes derived from univariate analyses indicated a
substantial survival disadvantage for patients with low LCR levels
(HR=2.66; 95% CI: 2.04–3.46; P<0.001), and this relationship
persisted even after adjustment for confounding factors in
multivariate models (HR=2.12; 95% CI: 1.83–2.46; P<0.001)
(Fig. 4A). These findings suggest
that the prognostic relevance of LCR is robust and not dependent on
statistical modeling choices.
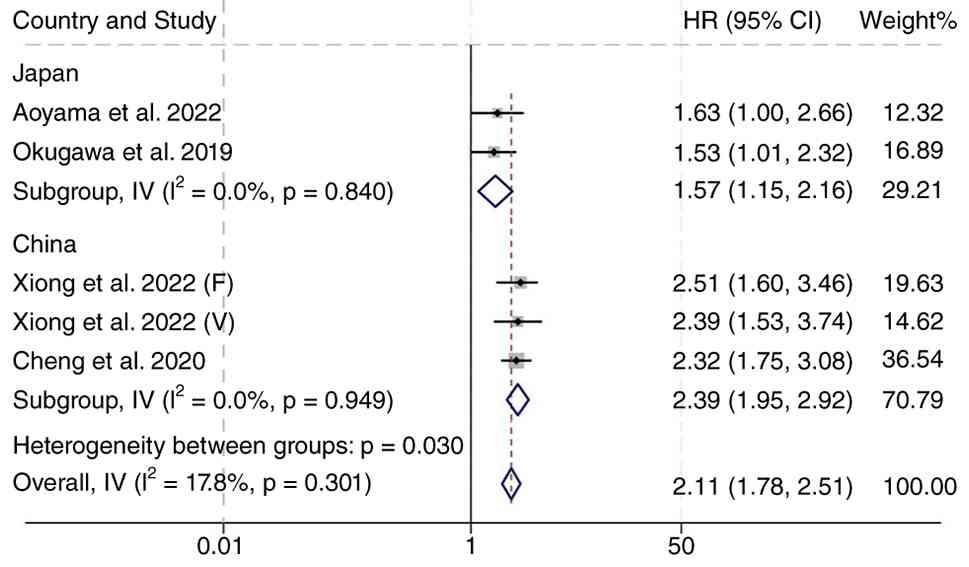
Geographically stratified analyses further
reinforced this conclusion. In studies conducted in Japan, low LCR
values were strongly associated with inferior OS, with a pooled HR
of 2.31 (95% CI: 1.85–2.87; P<0.001). A similar magnitude of
risk was observed among cohorts from China, where low LCR remained
a significant predictor of poor survival (HR=2.19; 95% CI:
1.84–2.60; P<0.001) (Fig. 4B).
The consistent effect across regions suggests that the prognostic
value of LCR transcends geographic and demographic variability.
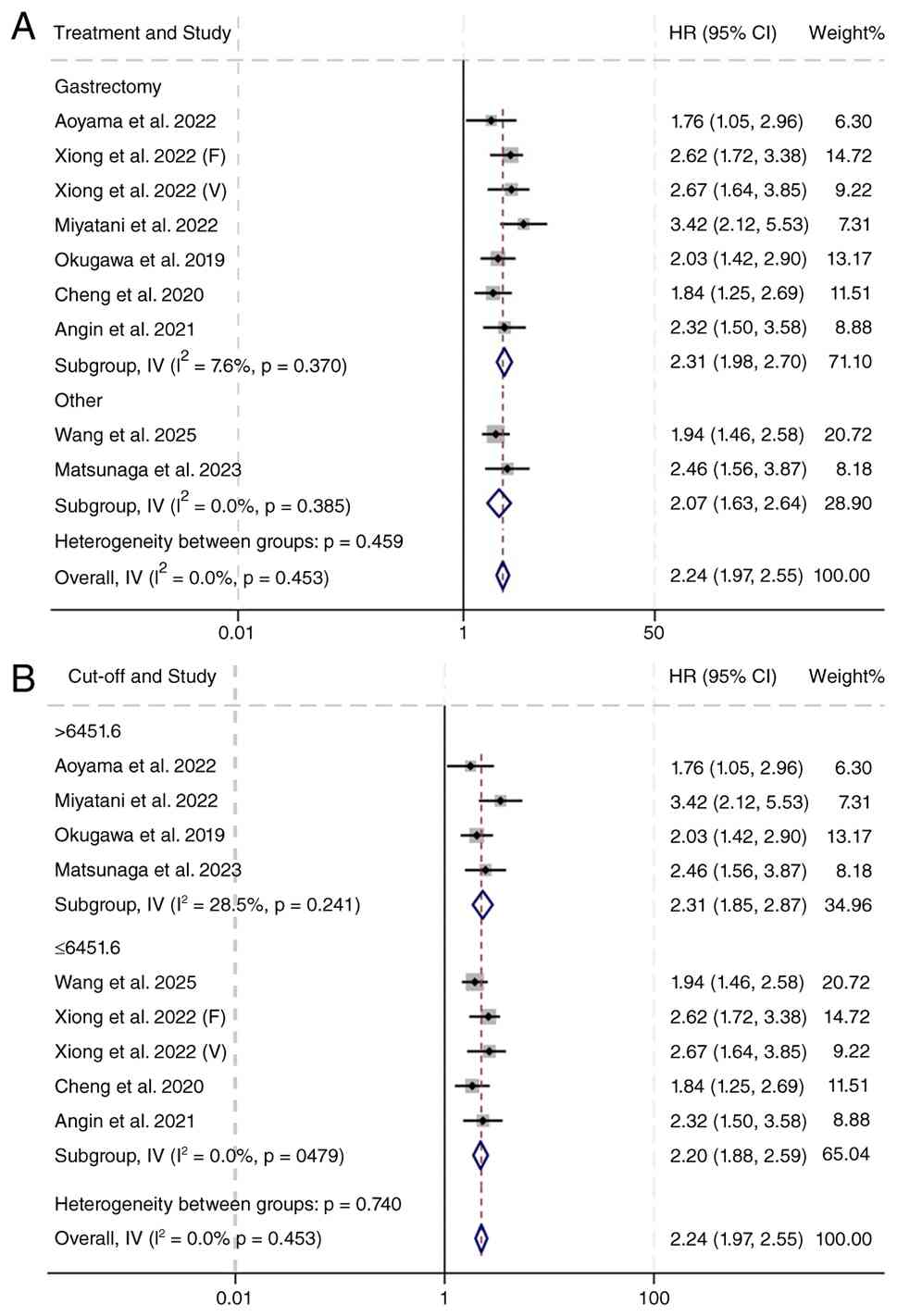
It was further examined whether treatment modality
and LCR cut-off value influenced the prognostic association between
LCR and OS. In the treatment-based subgroup analysis, low LCR
remained significantly associated with unfavorable OS both in
patients undergoing gastrectomy (HR=2.31; 95% CI: 1.98–2.70;
P<0.001) and in those receiving other treatment modalities
(HR=2.07; 95% CI: 1.63–2.64; P<0.001; Fig. 5A). Similarly, when studies were
stratified by the median LCR cut-off value, the association
remained significant in both the high cut-off group (>6451.6:
HR=2.31; 95% CI: 1.85–2.87; P<0.001) and the low cut-off group
(≤6451.6: HR=2.20; 95% CI: 1.88–2.59; P<0.001; Fig. 5B).
Collectively, the subgroup analyses provide
compelling evidence that the prognostic effect of low LCR is
consistent across diverse analytical frameworks, geographic
populations, cut-off and clinical management strategies. These
findings highlight the potential of LCR as a broadly applicable
biomarker for risk stratification in GC.
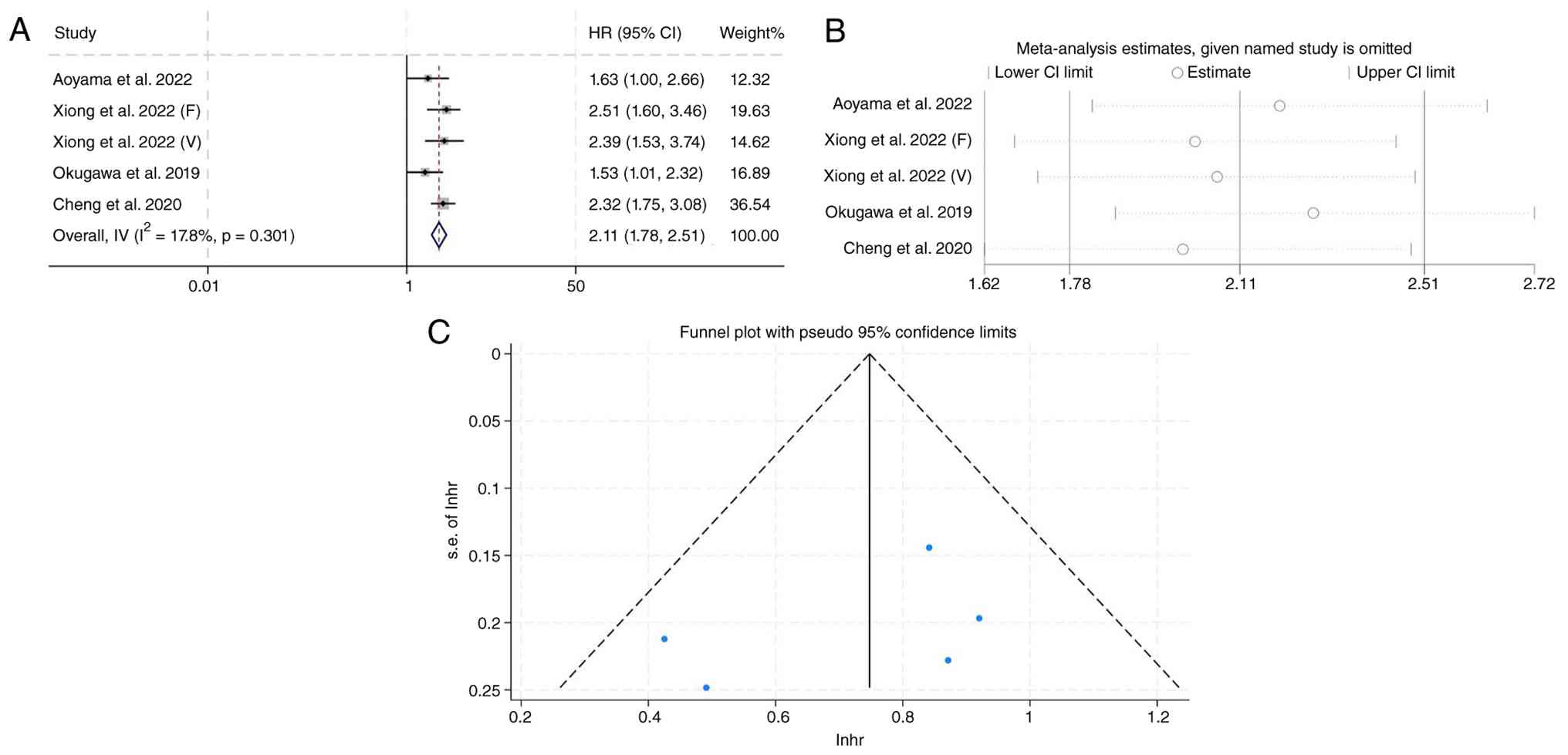
Pretreatment LCR and DFS
A total of five eligible studies, encompassing 2,987
individuals diagnosed with GC, were included to investigate the
prognostic significance of pretreatment LCR in relation to DFS. In
each cohort, patients were stratified into high- and low-LCR
subgroups based on the cut-off values defined by the original
studies. When these datasets were quantitatively synthesized, low
pretreatment LCR was consistently associated with a markedly
increased risk of earlier recurrence. The pooled HR for DFS was
2.11 (95% CI: 1.78–2.51; P<0.001), indicating that patients with
reduced LCR levels experienced substantially shorter DFS compared
with those with higher levels (Fig.
6A).
Between-study heterogeneity was minimal. Cochran's Q
test did not reach statistical significance, and the I2
statistic was 0% (P=0.301), demonstrating that the effect estimates
were highly concordant across all included cohorts. Owing to this
strong consistency, a fixed-effect model was adopted to generate
the final summary estimate. These findings collectively suggest
that LCR may serve as a simple and clinically accessible biomarker
capable of identifying patients at elevated risk for early
relapse.
Sensitivity analyses further supported the
robustness of the pooled results. Sequential omission of individual
studies revealed no material changes in the magnitude or direction
of the hazard ratio, confirming that the association between
reduced LCR and inferior DFS was not driven by any single dataset
(Fig. 6B).
Evaluation of publication bias using Begg's rank
correlation and Egger's regression also demonstrated no
statistically significant evidence of small-study effects (Begg's
P=0.462; Egger's P=0.391). The symmetrical appearance of the funnel
plot provided additional reassurance that the synthesized results
were unlikely to be influenced by selective reporting practices
(Fig. 6C). Geographically
stratified analyses further reinforced this conclusion (Fig. 7).
Overall, these findings reinforce the prognostic
value of pretreatment LCR for predicting disease recurrence in GC
and highlight its potential role as a readily applicable tool for
risk stratification.
Discussion
The present meta-analysis is the first to
comprehensively assess the prognostic significance of LCR in GC. It
was found that lower LCR values consistently indicated poorer
survival. Because LCR is derived from routine laboratory
measurements, it provides a readily obtainable, reproducible, and
economical metric that can complement current prognostic
frameworks. Individuals with lower LCR values tended to exhibit a
higher risk of postoperative relapse or rapid tumor progression,
indicating the potential of this index to refine risk
stratification and support more personalized therapeutic
decision-making.
The biological significance of LCR as a prognostic
indicator is reinforced by evidence highlighting the combined roles
of lymphocyte-driven immune activity and CRP-mediated inflammatory
signaling in oncogenesis. Lymphocyte abundance has been recognized
as a prognostic marker in multiple cancers, including breast,
colorectal and pancreatic malignancies (23,24).
In addition, specific lymphocyte subsets infiltrating the tumor,
such as CD8+ cytotoxic cells and memory T-cell
populations, have been associated with more favorable clinical
outcomes (25), highlighting the
importance of cellular immunity in maintaining antitumor
surveillance.
CRP, by contrast, is a classical acute-phase
reactant synthesized by hepatocytes under interleukin-2-dependent
regulation (26). Compared with
other inflammatory markers, CRP exhibits more stable kinetic
behavior during inflammation (26).
Its elevation, frequently observed in colorectal, pulmonary and GCs
(27), has been associated with
adverse pathological features, such as nodal involvement, deeper
gastric wall invasion and distant metastasis. Since Virchow first
elucidated the conceptual link between inflammation and neoplasia
in the nineteenth century (28),
the complexity of tumor-host inflammatory interactions remains
incompletely defined.
Inflammation within the tumor microenvironment
promotes leukocyte apoptosis and margination, resulting in
lymphopenia (29). Reduced
lymphocyte counts have been associated with poor outcomes in
various malignancies (30,31), consistent with the hypothesis that
weakened immunosurveillance accelerates tumor evolution and
metastatic dissemination. Elevated levels of proinflammatory
mediators further promote angiogenesis and metastatic capability.
Consequently, systemic inflammation in cancer is usually marked by
increased neutrophil and monocyte counts accompanied by decreased
lymphocyte counts, indicating enhanced inflammatory activity
alongside compromised adaptive immunity.
These mechanistic findings align with the findings
of studies investigating inflammation-based biomarkers. Among these
biomarkers, the NLR has been thoroughly examined in GC, with
elevated preoperative levels consistently associated with shortened
survival and more advanced disease (32,33).
Similarly, other inflammation-based indices, such as PLR, LMR and
CAR, have shown prognostic value in multiple tumor types (34–37).
Notably, emerging evidence suggests that markers integrating both
inflammatory burden and lymphocyte status can outperform
traditional single-parameter indices. Studies on colorectal cancer
have reported that LCR provides superior prognostic discrimination
compared with other inflammation-based indices (6,38,39).
The results of the present study are consistent with these
findings.
From a clinical perspective, LCR has several
practical advantages. It can be calculated easily from routine
blood tests, is inexpensive, and does not require specialized
equipment or additional invasive procedures. Therefore, LCR may be
useful as an adjunct to existing prognostic systems, such as tumor
stage, pathological features and treatment-related factors.
Patients with low pretreatment LCR may represent a higher-risk
population who require closer surveillance, more individualized
perioperative management, or more intensive follow-up strategies.
However, LCR should not be considered a replacement for established
staging systems. Instead, it may provide complementary prognostic
information and help refine risk assessment when used together with
conventional clinicopathological parameters.
Several limitations should be considered when
interpreting the current findings. First, all included studies were
retrospective, which may increase the risk of selection bias and
unmeasured confounding. Although multivariate estimates were
preferentially extracted when available, residual confounding could
not be completely excluded. Second, the protocol of the present
meta-analysis was not prospectively registered, which should be
acknowledged when considering the methodological transparency of
the present systematic review. Third, most included cohorts were
derived from East Asian populations, particularly China and Japan.
Ethnicity-related differences, dietary habits, Helicobacter
pylori prevalence, screening practices, baseline nutritional
and inflammatory status, stage distribution at diagnosis, and
regional treatment strategies may influence both LCR levels and
survival outcomes. Differences in lymphadenectomy extent,
perioperative or adjuvant chemotherapy, postoperative surveillance,
and supportive care may also affect the prognostic performance of
LCR. Therefore, extrapolation of these findings to Western and
other non-East Asian populations should be made cautiously.
Another important limitation is the lack of a
standardized LCR cut-off value among the included studies. Although
our exploratory subgroup analysis showed that the association
between low LCR and unfavorable OS remained significant across
different cut-off subgroups, the optimal threshold for clinical use
remains undetermined. Variation in cut-off values may affect
clinical interpretation and limit direct application in routine
practice. Future prospective multicenter studies with standardized
measurement methods and predefined LCR thresholds are needed to
validate the present findings and establish an appropriate cut-off
value for patients with GC. In addition, some studies provided HRs
from different statistical models, and reconstructed estimates from
Kaplan-Meier curves may introduce measurement uncertainty when
directly reported HRs were unavailable.
In conclusion, the present meta-analysis indicated
that a reduced LCR was consistently associated with poor survival
outcomes, including both overall and DFS, in GC. As an inexpensive
and readily obtainable biomarker, LCR offers robust prognostic
value across diverse analytical methods, clinical settings and
geographic regions. Its strong and stable predictive performance
suggests that LCR may serve as a valuable adjunct to current
staging systems, aiding in more precise risk stratification and
individualized patient management. Nonetheless, prospective
multicenter studies with standardized LCR thresholds are warranted
to validate these findings and facilitate its broader clinical
application.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
KL and LC conceived and designed the study,
performed data collection, statistical analysis and interpretation,
drafted the manuscript, and critically revised the manuscript. Both
authors have read and approved the final version of the manuscript.
KL and LC confirm the authenticity of all the raw data.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Bray F, Laversanne M, Sung H, Ferlay J,
Siegel RL, Soerjomataram I and Jemal A: Global cancer statistics
2022: GLOBOCAN estimates of incidence and mortality worldwide for
36 cancers in 185 countries. CA Cancer J Clin. 74:229–263.
2024.PubMed/NCBI
|
|
2
|
Usui Y, Taniyama Y, Endo M, Koyanagi YN,
Kasugai Y, Oze I, Ito H, Imoto I, Tanaka T, Tajika M, et al:
Helicobacter pylori, Homologous-recombination genes, and gastric
cancer. N Engl J Med. 388:1181–1190. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Manohar SM: At the crossroads of TNF α
signaling and cancer. Curr Mol Pharmacol.
17:e0609232207582024.PubMed/NCBI
|
|
4
|
Zhang X, Jin M, Yao X, Liu J, Yang Y,
Huang J, Jin G, Liu S and Zhang B: Upregulation of LncRNA WT1-AS
inhibits tumor growth and promotes autophagy in gastric cancer via
suppression of PI3K/Akt/mTOR pathway. Curr Mol Pharmacol.
17:e187614293183982024. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Lee JH, Chang KK, Yoon C, Tang LH, Strong
VE and Yoon SS: Lauren histologic type is the most important factor
associated with pattern of recurrence following resection of
gastric adenocarcinoma. Ann Surg. 267:105–113. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Okugawa Y, Toiyama Y, Yamamoto A,
Shigemori T, Ide S, Kitajima T, Fujikawa H, Yasuda H, Hiro J,
Yoshiyama S, et al: Lymphocyte-C-reactive protein ratio as
promising new marker for predicting surgical and oncological
outcomes in colorectal cancer. Ann Surg. 272:342–351. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Gao Q, Quan M, Zhang L, Ran Y, Zhong J and
Wang B: Neutrophil-To-Lymphocyte ratio as a prognostic indicator in
thyroid cancer. Cancer Control. 31:107327482413090482024.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zhang L, Feng J, Kuang T, Chai D, Qiu Z,
Deng W, Dong K, Zhao K and Wang W: Blood biomarkers predict
outcomes in patients with hepatocellular carcinoma treated with
immune checkpoint Inhibitors: A pooled analysis of 44 retrospective
sudies. Int Immunopharmacol. 118:1100192023. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chen XD, Mao CC, Wu RS, Zhang WT, Lin J,
Sun XW, Chi CH, Lou N, Wang PF, Shen X, et al: Use of the
combination of the preoperative platelet-to-lymphocyte ratio and
tumor characteristics to predict peritoneal metastasis in patients
with gastric cancer. PLoS One. 12:e01750742017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Page MJ, McKenzie JE, Bossuyt PM, Boutron
I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan
SE, et al: The PRISMA 2020 statement: An updated guideline for
reporting systematic reviews. BMJ. 372:n712021. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tierney JF, Stewart LA, Ghersi D, Burdett
S and Sydes MR: Practical methods for incorporating summary
time-to-event data into meta-analysis. Trials. 8:162007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Xiong J, Hu H, Kang W, Li Y, Jin P, Shao
X, Li W and Tian Y: Peking prognostic score, based on preoperative
sarcopenia status, is a novel prognostic factor in patients with
gastric cancer. Front Nutr. 9:9102712022. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Stang A: Critical evaluation of the
Newcastle-Ottawa scale for the assessment of the quality of
nonrandomized studies in meta-analyses. Eur J Epidemiol.
25:603–605. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhang L, Wang K, Liu R, Kuang T, Chen C,
Yao F and Wang W: Body composition as a prognostic factor in
cholangiocarcinoma: A meta-analysis. Nutr J. 23:1452024. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhang L, Li X, Wang K, Wu M, Liu W and
Wang W: Prognostic impact of body composition in hepatocellular
carcinoma patients with immunotherapy. Ann Med. 56:23950622024.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Angin YS, Yildirim M, Dasiran F and Okan
I: Could lymphocyte to C-reactive protein ratio predict the
prognosis in patients with gastric cancer? ANZ J Surg.
91:1521–1527. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Aoyama T, Nakazano M, Nagasawa S, Hara K,
Komori K, Tamagawa H, Maezawa Y, Segami K, Kano K, Ogata T, et al:
The association of the lymphocyte-to-c-reactive-protein ratio with
gastric cancer patients who receive curative treatment. In Vivo.
36:482–489. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cheng CB, Zhang QX, Zhuang LP and Sun JW:
Prognostic value of lymphocyte-to-C-reactive protein ratio in
patients with gastric cancer after surgery: A multicentre study.
Jpn J Clin Oncol. 50:1141–1149. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Matsunaga T, Saito H, Fukumoto Y, Kuroda
H, Taniguchi K, Takahashi S, Osaki T, Iwamoto A, Fukuda K, Shimizu
S, et al: The prognostic impact of the lymphocyte-to-C-reactive
protein ratio in patients with unresectable or recurrent advanced
gastric cancer treated with first- and second-line treatment. Surg
Today. 53:940–948. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Miyatani K, Sawata S, Makinoya M, Miyauchi
W, Shimizu S, Shishido Y, Matsunaga T, Yamamoto M, Tokuyasu N,
Takano S, et al: Combined analysis of preoperative and
postoperative lymphocyte-C-reactive protein ratio precisely
predicts outcomes of patients with gastric cancer. BMC Cancer.
22:6412022. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Okugawa Y, Toiyama Y, Yamamoto A,
Shigemori T, Ichikawa T, Yin C, Suzuki A, Fujikawa H, Yasuda H,
Hiro J, et al: Lymphocyte-to-C-reactive protein ratio and score are
clinically feasible nutrition-inflammation markers of outcome in
patients with gastric cancer. Clin Nutr. 39:1209–1217. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wang Y, Zhang X, Liu C, Shi J, Liu T, Chen
Y, Zheng X, Bu Z and Shi H: Combined assessment of inflammation and
food intake contributes to prognostic stratification of gastric
cancer. Front Oncol. 15:16698382025. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Toss MS, Miligy I, Al-Kawaz A, Alsleem M,
Khout H, Rida PC, Aneja R, Green AR, Ellis IO and Rakha EA:
Prognostic significance of tumor-infiltrating lymphocytes in ductal
carcinoma in situ of the breast. Mod Pathol. 31:1226–1236. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wild AT, Ye X, Ellsworth SG, Smith JA,
Narang AK, Garg T, Campian J, Laheru DA, Zheng L, Wolfgang CL, et
al: The association between chemoradiation-related lymphopenia and
clinical outcomes in patients with locally advanced pancreatic
adenocarcinoma. Am J Clin Oncol. 38:259–265. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Trédan O, Manuel M, Clapisson G, Bachelot
T, Chabaud S, Bardin-dit-Courageot C, Rigal C, Biota C, Bajard A,
Pasqual N, et al: Patients with metastatic breast cancer leading to
CD4+ T cell lymphopaenia have poor outcome. Eur J Cancer.
49:1673–1682. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Pepys MB and Hirschfield GM: C-reactive
protein: A critical update. J Clin Invest. 111:1805–1812. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kim DK, Oh SY, Kwon HC, Lee S, Kwon KA,
Kim BG, Kim SG, Kim SH, Jang JS, Kim MC, et al: Clinical
significances of preoperative serum interleukin-6 and C-reactive
protein level in operable gastric cancer. BMC Cancer. 9:1552009.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Balkwill F and Mantovani A: Inflammation
and cancer: Back to Virchow? Lancet. 357:539–545. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Grivennikov SI, Greten FR and Karin M:
Immunity, inflammation, and cancer. Cell. 140:883–899. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Clark EJ, Connor S, Taylor MA, Madhavan
KK, Garden OJ and Parks RW: Preoperative lymphocyte count as a
prognostic factor in resected pancreatic ductal adenocarcinoma. HPB
(Oxford). 9:456–460. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lim DV, Woo WH, Lim JX, Loh XY, Soh HT,
Lim SYA, Lee ZY, Yow HY, Hamzah SB, Sellappans R and Foo JB:
Targeting mutant-p53 for cancer treatment: Are we there yet? Curr
Mol Pharmacol. 17:e1409232210422024. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Wang SC, Chou JF, Strong VE, Brennan MF,
Capanu M and Coit DG: Pretreatment neutrophil to lymphocyte ratio
independently predicts disease-specific survival in resectable
gastroesophageal junction and gastric adenocarcinoma. Ann Surg.
263:292–297. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Hsu JT, Liao CK, Le PH, Chen TH, Lin CJ,
Chen JS, Chiang KC and Yeh TS: Prognostic value of the preoperative
neutrophil to lymphocyte ratio in resectable gastric cancer.
Medicine (Baltimore). 94:e15892015. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Sensi B, Angelico R, Toti L, Conte L,
Coppola A, Tisone G and Manzia TM: Mechanism potential and concerns
of immunotherapy for hepatocellular carcinoma and liver
transplantation. Curr Mol Pharmacol. 17:e187614293107032024.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Mano Y, Shirabe K, Yamashita Y, Harimoto
N, Tsujita E, Takeishi K, Aishima S, Ikegami T, Yoshizumi T,
Yamanaka T and Maehara Y: Preoperative neutrophil-to-lymphocyte
ratio is a predictor of survival after hepatectomy for
hepatocellular carcinoma: A retrospective analysis. Ann Surg.
258:301–305. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Liu Z, Jin K, Guo M, Long J, Liu L, Liu C,
Xu J, Ni Q, Luo G and Yu X: Prognostic value of the CRP/Alb ratio,
a novel inflammation-based score in pancreatic cancer. Ann Surg
Oncol. 24:561–568. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Shimada H, Takiguchi N, Kainuma O, Soda H,
Ikeda A, Cho A, Miyazaki A, Gunji H, Yamamoto H and Nagata M: High
preoperative neutrophil-lymphocyte ratio predicts poor survival in
patients with gastric cancer. Gastric Cancer. 13:170–176. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Suzuki S, Akiyoshi T, Oba K, Otsuka F,
Tominaga T, Nagasaki T, Fukunaga Y and Ueno M: Comprehensive
comparative analysis of prognostic value of systemic inflammatory
biomarkers for patients with stage II/III colon cancer. Ann Surg
Oncol. 27:844–852. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Okugawa Y, Toiyama Y, Fujikawa H, Ide S,
Yamamoto A, Omura Y, Yin C, Kusunoki K, Kusunoki Y, Yasuda H, et
al: Prognostic potential of lymphocyte-C-reactive protein ratio in
patients with rectal cancer receiving preoperative
chemoradiotherapy. J Gastrointest Surg. 25:492–502. 2021.
View Article : Google Scholar : PubMed/NCBI
|