Introduction
Lung cancer (LC) is one of the most prevalent
malignant tumors in China. In 2022, ~1.06 million new cases of LC
were diagnosed in China, with an incidence rate of 149.54 per
100,000 and a mortality rate of 102.97 per 100,000, ranking first
among malignant tumors in terms of cancer-related mortality
(1). Brain metastasis (BM) is one
of the most serious complications affecting patient prognosis and
quality of life, and represents the most common form of distant
metastasis in LC, occurring in ~20–65% of patients with LC during
the course of disease (2,3). Lung adenocarcinoma (LUAD), a subtype
of non-small cell lung cancer (NSCLC) arising from the pulmonary
glandular epithelium, accounts for ~50% of all LC cases (4). Approximately 30% of patients with LUAD
develop BM, which is a leading cause of treatment failure (5). Early detection and intervention of BM
is therefore considered essential for improving the prognosis of
patients with LUAD.
Epidermal growth factor receptor (EGFR) mutation is
among the most frequently identified driver gene alterations in
NSCLC, particularly in Asian populations (6). A total of ~40–50% of patients with
LUAD in Asia harbor deleterious mutations in the EGFR gene
(7). The specific mutation site and
type are key determinants for selecting targeted therapies, such as
EGFR tyrosine kinase inhibitors (TKIs) (8). Third-generation EGFR TKIs have
demonstrated definite efficacy in treating BM in patients with
NSCLC with EGFR mutations (9).
Several clinical studies have suggested that certain EGFR mutation
subtypes may increase the risk of BM in LC, although most were
limited by small sample sizes (10–12).
However, evidence directly confirming the relationship between
specific EGFR mutations and BM development in LUAD remains scarce,
and qualitative assessment of EGFR mutation status alone cannot
serve as a real-time quantitative marker for monitoring disease
progression (13). In the present
study, the impact of EGFR mutation subtypes on BM risk in LUAD was
analyzed and EGFR mutation status was integrated with serum
LC-related biomarkers to develop a combined predictive approach.
This combined method was evaluated for its utility in auxiliary
diagnosis and risk stratification of BM in LUAD, with the aim of
providing a quantitative and dynamic tool for early detection and
clinical intervention.
Materials and methods
Study population
This study retrospectively enrolled 615 patients
with LUAD, including 401 with BM and 214 without BM, matched by age
and sex. Between June 2021 and June 2024, patients with LUAD who
developed BM were consecutively identified from the medical records
of the First Affiliated Hospital of Guangzhou Medical University
(Guangzhou, China); a control group of patients with LUAD without
BM was subsequently selected from the same institution during the
same period, matched to the BM group by age and sex. LUAD diagnosis
was established by a pathologist and respiratory physicians based
on histopathological examination of lung biopsy specimens. BM
diagnosis was established by a multidisciplinary team comprising
neurologists, radiologists and respiratory physicians, based on
findings from contrast-enhanced 3.0T MRI or detection of tumor
cells in the cerebrospinal fluid. All patients in the non-BM group
also underwent contrast-enhanced 3.0T MRI, with the absence of BM
confirmed on the basis of negative imaging findings, thereby
ensuring that BM status was determined by standardized imaging
assessment across all enrolled patients. The primary inclusion
criterion was a confirmed diagnosis of primary LC in the absence of
other concurrent malignancies. The exclusion criteria were as
follows: i) History of psychiatric complaints, disturbance of
consciousness, dementia, central nervous system (CNS) infection or
other conditions associated with impaired brain function; ii)
severe hepatic or renal dysfunction; and iii) absence of key
diagnostic examinations required for clinical diagnosis. All
participants provided written informed consent for the collection,
processing and analysis of blood samples and clinical data for
research and publication purposes. This study was conducted in
accordance with the principles of the Declaration of Helsinki and
was approved by the Ethics Committee of the First Affiliated
Hospital of Guangzhou Medical University (approval no.
GZMC2021-06-1237; Fig. S1).
Peripheral blood collection and
detection
Blood samples from patients in the BM group were
collected within 3 days of BM diagnosis; this sampling window was
intended to ensure that collection preceded the initiation of
BM-specific treatments, including corticosteroids, whole-brain
radiotherapy and stereotactic radiosurgery. Blood samples from
patients in the non-BM group were collected at the time of initial
LUAD diagnosis, prior to the initiation of any antitumor therapy,
representing a treatment-naive baseline state. All samples were
collected in the morning under fasting conditions and stored in
anticoagulant-containing polypropylene tubes. Plasma was separated
by centrifugation at 500 × g for 10 min at 4°C. Serum samples were
processed for LC biomarker detection within 24 h of collection;
remaining samples were stored at −80°C. The LC biomarkers assessed
included neuron-specific enolase (NSE), carcinoembryonic antigen
(CEA), cancer antigen 125 (CA125), CA153 and cytokeratin 19
fragment (CYFRA21-1). CEA concentrations were measured by
electrochemiluminescence immunoassay using a commercial kit
(Architect CEA Reagent Kit; Abbott Diagnostics Division), whereas
NSE, CA125, CA153 and CYFRA21-1 concentrations were determined by
immunoradiometric assay using commercially available kits
(Cytokeratin 19 Fragment IRMA Kit and NSE IRMA Kit; Beckman
Coulter, Inc.). The procedure followed the manufacturer's
instructions, as reported previously (14). The upper reference limits were as
follows: NSE, 16.30 ng/ml; CEA, 5.00 ng/ml; CA125, 35.00 U/ml;
CA153, 25.00 U/ml; and CYFRA21-1, 3.30 ng/ml. Each sample was
measured in triplicate and the mean value was used for subsequent
analyses. No samples were subjected to repeated freeze-thaw
cycles.
DNA extraction and sequencing
Total DNA was extracted from formalin-fixed,
paraffin-embedded tumor tissue using a QIAamp DNA Tissue Kit
(Qiagen GmbH), following previously described methods (15). DNA purity was assessed by
spectrophotometric measurement of the 260/280 nm absorbance ratio
using a NanoDrop 2000 spectrophotometer (Thermo Fisher Scientific,
Inc.). Targeted next-generation sequencing was performed by Burning
Rock Biotech, a commercial clinical laboratory certified by the
Clinical Laboratory Improvement Amendments and accredited by the
College of American Pathologists (15). A commercial capture panel targeting
520 genes of the human genome (OncoScreen Plus; Burning Rock
Biotech) was used for target enrichment according to the
manufacturer's protocol. DNA fragments of 200–400 bp were purified
using a Bioanalyzer 2100 (Agilent Technologies, Inc.), hybridized
with capture probes, selected with magnetic beads and amplified.
Library sequencing was performed on the NextSeq 500 platform
(Illumina, Inc.), with a mean sequencing depth of ~1,000 ×. Further
methodological details were reported previously (15).
Nomogram construction and
validation
A total of 9 candidate variables were initially
entered into a multivariate analysis, encompassing TNM staging
components (T stage, N stage and other tissue metastases as a
surrogate for distant metastatic burden), EGFR exon 19 deletion
(19del) mutation status, and five serum biomarkers (NSE, CEA,
CA125, CA153 and CYFRA21-1). M stage was excluded to avoid
collinearity with the outcome variable, as BM itself constitutes M1
disease by definition. Bidirectional stepwise selection based on
the Akaike information criterion (AIC) was applied to identify the
optimal variable subset; T stage was eliminated during this process
and eight variables were retained in the final model (AIC=439.42).
A nomogram was subsequently constructed using these variables to
predict BM risk in patients with LUAD (16). Calibration curve and receiver
operating characteristic (ROC) curve analyses were used to evaluate
the calibration and discriminatory ability of the nomogram,
respectively, and decision curve analysis (DCA) was performed to
assess its clinical utility. Subsequently, 10-fold cross-validation
was performed for the internal validation of the nomogram. The
original dataset was randomly partitioned into 10 equal subsets; at
each iteration, 9 subsets were pooled for model training and the
remaining subset was withheld for validation, with this process
repeated 10 times. The mean area under the ROC curve (AUC),
sensitivity and specificity across the 10 validation iterations
were calculated to assess the generalizability of the model. A
web-based calculator was also developed (https://clinicalnomogram.shinyapps.io/BMsPredictionApp/)
to facilitate the clinical application of the nomogram, providing
individualized BM probability estimates based on patient-specific
variable inputs.
Statistical analysis
Statistical analyses were performed using GraphPad
Prism (version 8.0.2; Dotmatics), SPSS (version 19.0; SPSS, Inc.)
and R (version 4.1.0; R Foundation for Statistical Computing). Key
R packages used included rms, pROC, ResourceSelection and caret.
Non-normally distributed data are presented as median
(interquartile range), while normally distributed data are
expressed as mean ± standard deviation. Categorical data were
expressed as n (%). Group comparisons were performed using the
Mann-Whitney U test, Kruskal-Wallis test or chi-square test, as
appropriate for the data distribution. Logistic regression was used
to identify factors independently associated with BM in patients
with LUAD. ROC curves and the corresponding area under the curve
(AUC) values were generated to evaluate and compare the predictive
performance of individual and combined markers for BM. The net
reclassification improvement (NRI) and integrated discrimination
improvement (IDI) were calculated to quantitatively compare the
discriminative ability of the nomogram with that of the TNM staging
model. The optimal cut-off value for each serum biomarker was
determined by maximizing the Youden index (sensitivity +
specificity-1) on the training set ROC curves: NSE, 18.18 ng/ml;
CEA, 6.01 ng/ml; CA125, 19.59 U/ml; CA153, 14.82 U/ml; and
CYFRA21-1, 4.17 ng/ml. A post-hoc power analysis was conducted for
the primary comparison of BM incidence between 19del and non-19del
groups within a chi-square test framework (Cohen's w=0.10; N=615;
achieved power, 70.3%; α=0.05). A two-sided P<0.05 was
considered to indicate statistical significance for all
analyses.
Results
The distribution of patients with EGFR
mutations does not change in LUAD with BM
In accordance with the inclusion and exclusion
criteria, 401 patients with LUAD with BM and 214 patients without
BM were recruited, matched by age [BM group: Median, 61 years
(range, 24–88 years); non-BM group: Median, 60 years (range, 30–93
years)] and sex [BM group: 55.4% male; non-BM group: 49.5% male]
and were well-balanced with respect to smoking history [BM group:
9.2% (37/401); non-BM group: 9.3% (20/214); P=0.961; Table SI]. Demographic and
clinicopathological characteristics, including pathologic stage,
primary tumor status, lymph node metastasis and number of BMs, were
recorded for all enrolled patients. The proportion of patients with
other tissue metastases was significantly higher in the BM group
than in the non-BM group (54.1 vs. 22.0%, P<0.001), whereas the
overall distribution of EGFR mutations did not differ significantly
between groups (P>0.999; Table
SI). These findings suggest that BM development in LUAD may be
associated with enhanced tumor invasiveness; however, the lack of a
significant difference in overall EGFR mutation distribution
indicates that distinct mutation subtypes may exert differential
effects on BM risk, warranting further subtype-level analysis.
Serum concentrations of NSE, CEA, CA125, CA153 and CYFRA21-1 were
subsequently measured in all patients. As shown in Fig. S2, serum levels of NSE, CEA, CA125,
CA153 and CYFRA21-1 were significantly elevated in patients with BM
compared with those in the non-BM group, by 1.44-, 4.93-, 3.33-,
2.13- and 2.30-fold, respectively (all P<0.0001), suggesting
potential predictive value for BM in clinical settings. To further
characterize these relationships, patients were stratified into
four subgroups according to BM and EGFR mutation status. As shown
in Fig. 1A-E, serum levels of all
five biomarkers were significantly elevated in both BM subgroups
compared with both non-BM subgroups (all P<0.0001), while EGFR
mutation status exerted no significant effect within either the
non-BM or BM stratum (all P>0.9999). The sole exception was
CA153 (Fig. 1D), for which a modest
but statistically significant difference was observed between
EGFR-mutated and non-mutated patients within the non-BM group
(P=0.038), but not within the BM group. Collectively, these results
indicate that elevation of all five serum biomarkers was primarily
driven by BM status rather than EGFR mutation status. Nevertheless,
the complex interplay among BM, EGFR mutations and serum biomarkers
suggests that subtype-level analysis of EGFR mutations may help
elucidate underlying mechanisms.
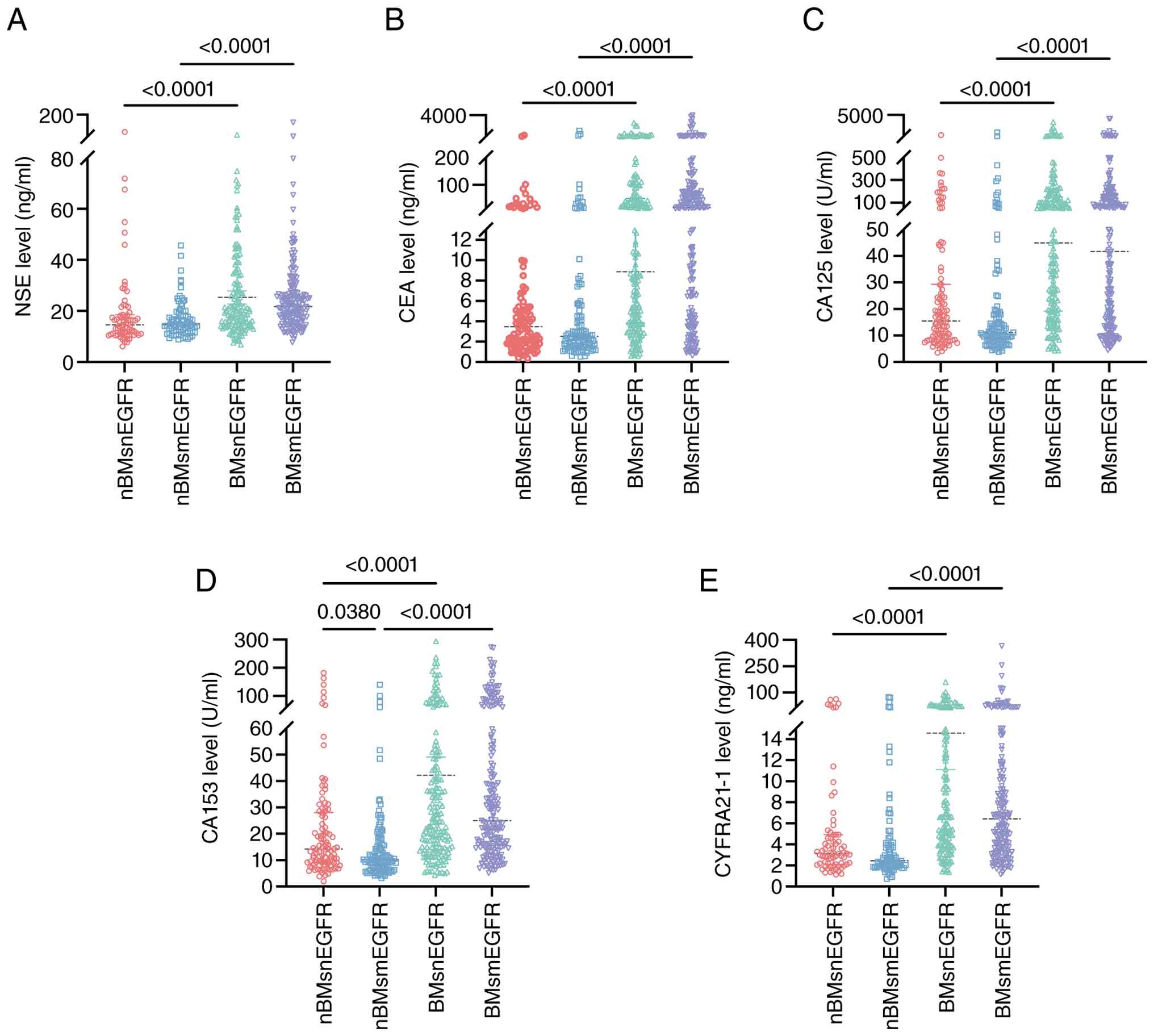 | Figure 1.Lung cancer biomarker concentrations
in patients with LUAD with EGFR mutations. The concentrations of
(A) NSE, (B) CEA, (C) CA125, (D) CA153 and (E) CYFRA21-1 in the
serum of different LUAD groups were detected. Patients were
stratified into four groups according to BM and EGFR mutation
status: nBMsnEGFR, non-BM without EGFR mutation; nBMsmEGFR, non-BM
with EGFR mutation; BMsnEGFR, BM without EGFR mutation; BMsmEGFR,
BM with EGFR mutation. The data are presented in scatter plots and
the median is shown by a horizontal line. P-values are shown above
the comparison brackets. Comparisons between groups were performed
with the Kruskal-Wallis test and Dunn's multiple-comparisons test.
LUAD, lung adenocarcinoma; NSE, neuron-specific enolase; CYFRA21-1,
cytokeratin 19 fragment; BM, brain metastasis. |
The 19del mutation is associated with
increased risk of BM in patients with LUAD
All 615 patients with LUAD were classified into
three subgroups according to EGFR genotype: 19del, 21L858R and
other genotypes. Baseline clinicopathological characteristics,
including pathologic stage, primary tumor status, lymph node
metastasis and other tissue metastases, were comparable among the
three genotype groups (Table SII).
Compared with other genotypes, the 19del mutation was associated
with a significantly higher BM rate (105/142, 73.9% vs. 296/473,
62.6%, P=0.013), while the 21L858R mutation showed a trend toward a
lower BM rate that did not reach statistical significance (P=0.083;
Table SII).
Patients were further stratified into four subgroups
according to BM and 19del mutation status. As shown in Fig. 2A-E, serum levels of all five
biomarkers were significantly elevated in both BM subgroups
compared with both non-BM subgroups (all P<0.0001), whereas no
significant difference was observed between 19del and non-19del
subjects within either the non-BM or BM stratum (all
P>0.999).
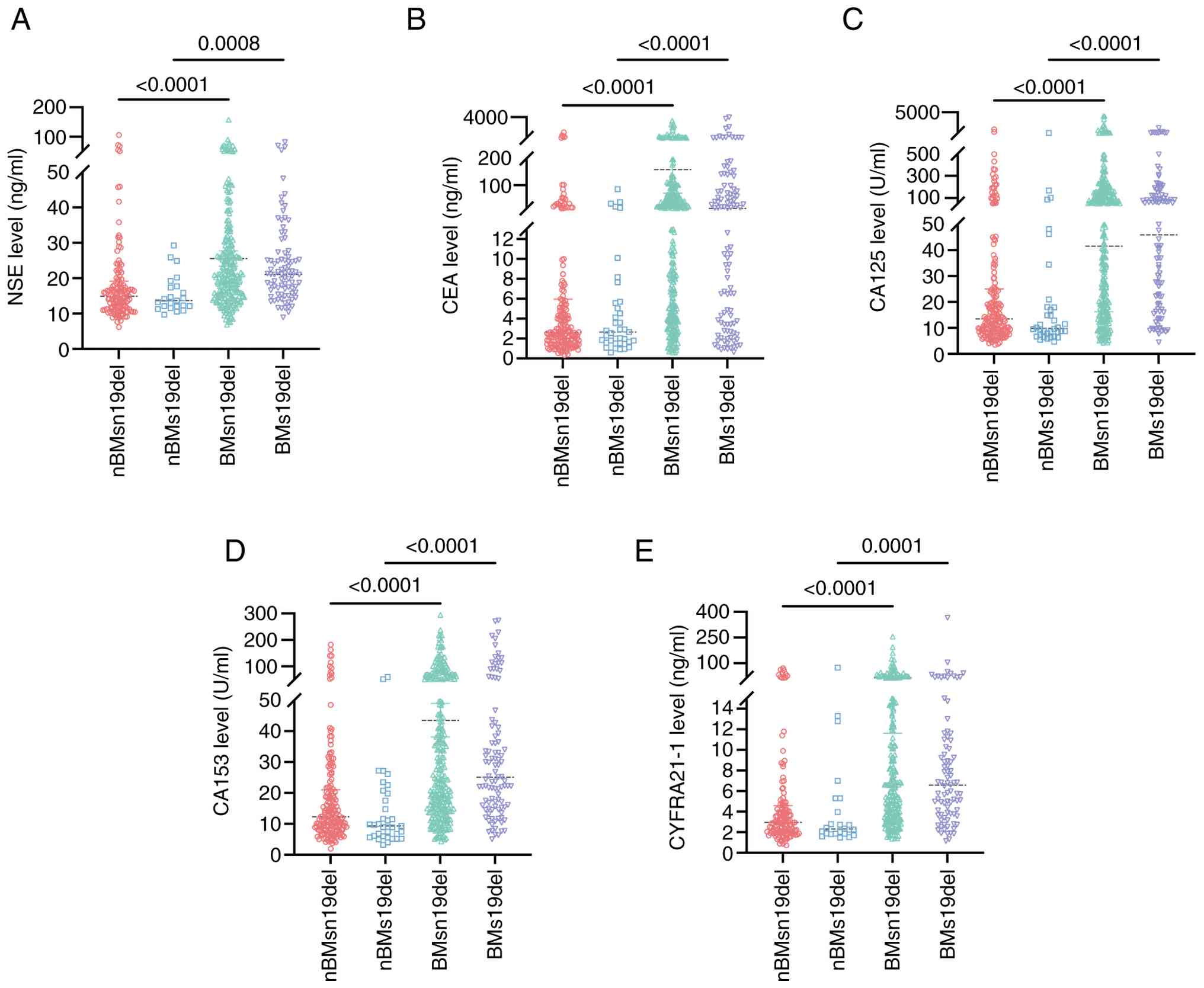 | Figure 2.Lung cancer biomarker concentrations
in patients with lung adenocarcinoma with the 19del mutation. The
concentrations of (A) NSE, (B) CEA, (C) CA125, (D) CA153 and (E)
CYFRA21-1 in the serum of patients with 19del mutation or BM were
detected. Patients were stratified into four groups according to BM
and 19del mutation status: nBMsn19del, non-BM without 19del;
nBMs19del, non-BM with 19del; BMsn19del, BM without 19del;
BMs19del, BM with 19del. The data are presented in scatter plots
and the median is shown by a horizontal line. P-values are shown
above the comparison brackets. Comparisons between groups were
performed with the Kruskal-Wallis test and Dunn's multiple
comparisons test. NSE, neuron-specific enolase; CYFRA21-1,
cytokeratin 19 fragment; BM, brain metastasis; 19del, exon 19
deletion. |
Univariate logistic regression analysis was
performed with BM status as the dependent variable and nine
candidate variables as independent variables, including primary
tumor stage, lymph node metastasis, other tissue metastasis, EGFR
19del status and five serum biomarkers (NSE, CEA, CA125, CA153 and
CYFRA21-1). All nine variables were significantly associated with
BM in the univariate analysis (Table
SIII). Among these, lymph node metastasis showed a stepwise
increase in BM risk with advancing N stage (vs. N0: N1, OR=4.24;
N2, OR=10.01; N3, OR=12.31; all P<0.001), and EGFR 19del was
independently associated with elevated BM risk (OR=2.10, 95% CI:
1.25–3.51, P=0.005). All five serum biomarkers were also
significantly associated with BM (all P<0.001; Table SIII). In the multivariate analysis,
five variables were independently associated with BM: N stage (N1,
N2 and N3 vs. N0), EGFR 19del, NSE, CEA and CYFRA21-1 (Table SIII). These results suggest that
the EGFR 19del mutation is independently associated with an
elevated risk of BM in LUAD, and that the concurrent elevation of
serum NSE, CEA, CA125, CA153 and CYFRA21-1 reflects increased tumor
burden at the time of BM development.
EGFR mutations combined with LC
biomarkers for the prediction of BM in LUAD
Building on the above findings, the predictive
performance of serum biomarkers for BM was further evaluated within
EGFR mutation-defined subgroups. In the overall cohort, ROC curve
analysis yielded AUC values of 0.709, 0.756, 0.739, 0.742 and 0.751
for NSE, CEA, CA125, CA153 and CYFRA21-1, respectively, as
individual biomarkers (Fig. S3).
Following stratification by EGFR mutation status, AUC values in the
EGFR-mutated subgroup increased substantially for NSE, CEA and
CA153, reaching 0.746, 0.781 and 0.800, respectively, while those
for CA125 and CYFRA21-1 showed modest changes, reaching 0.753 and
0.763. Further stratification by the 19del subtype yielded
additional AUC gains for CA125 and CA153 in the 19del subgroup,
reaching 0.803 and 0.815, respectively, while AUC values for NSE,
CEA and CYFRA21-1 showed modest changes, reaching 0.775, 0.750 and
0.772, respectively (Fig. 3). These
results indicate that stratifying patients by EGFR mutation status
improves the BM predictive performance of serum biomarkers compared
with biomarkers alone, and that further stratification by the 19del
subtype yields additional gains for selected biomarkers. These
findings suggest that distinct EGFR mutation subtypes exert
differential effects on biomarker-based BM prediction in LUAD.
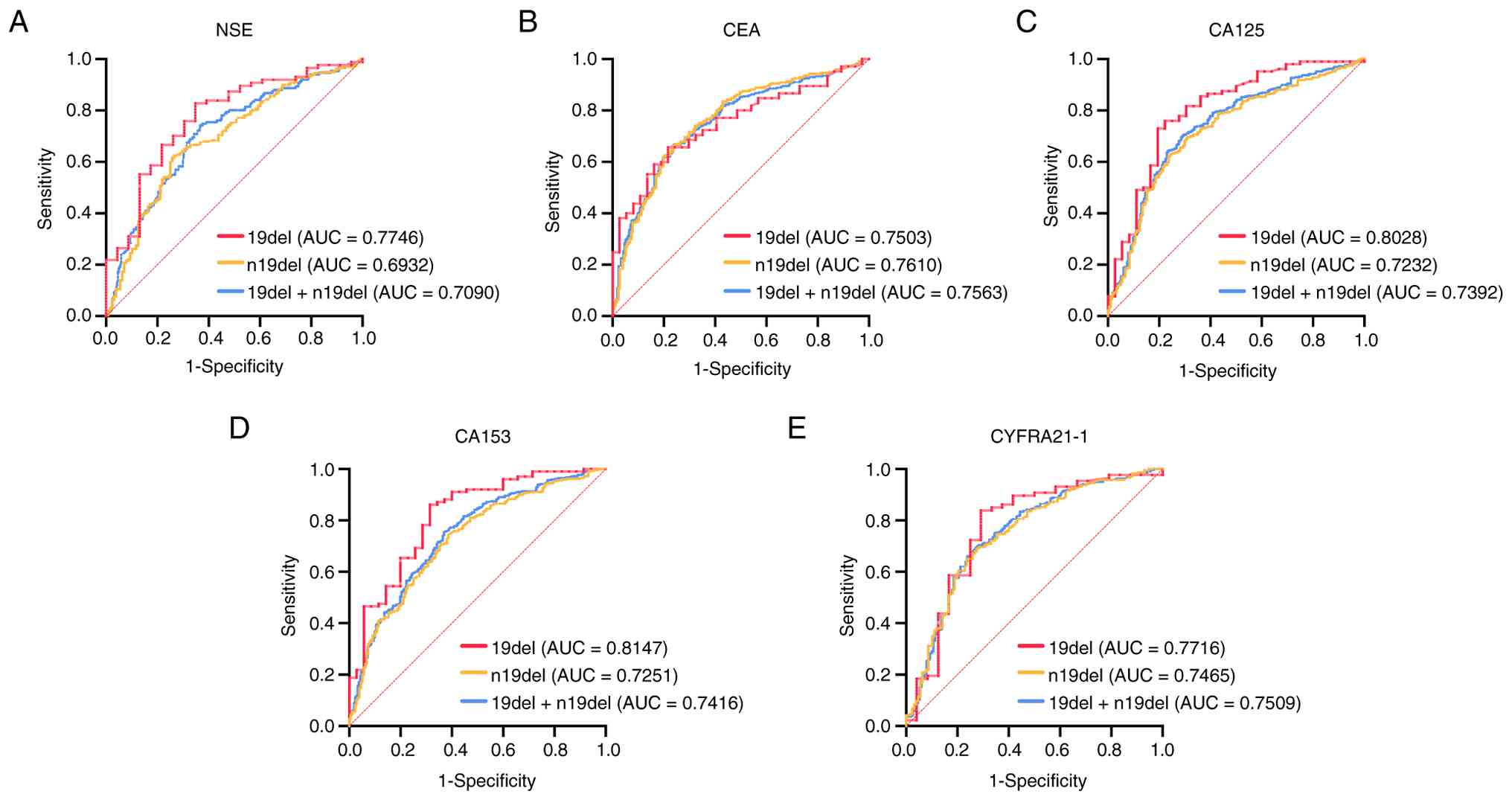 | Figure 3.ROC curves of 19del combined with
lung cancer biomarkers for the prediction of BM in patients with
LUAD. ROC curves of serum levels of (A) NSE, (B) CEA, (C) CA125,
(D) CA153 and (E) CYFRA21-1 were generated to distinguish BM in
patients with LUAD. The three subgroups are shown: 19del, patients
harboring the exon 19 deletion; n19del, patients without the exon
19 deletion; 19del+n19del, the overall cohort. ROC, receiver
operating characteristic; AUC, area under the ROC curve; NSE,
neuron-specific enolase; CYFRA21-1, cytokeratin 19 fragment; BM,
brain metastasis; 19del, exon 19 deletion; LUAD, lung
adenocarcinoma. |
Combining biomarkers for the
prediction of BM in LUAD
A combined approach incorporating EGFR mutation
status and serum concentrations of NSE, CEA, CA125, CA153 and
CYFRA21-1 was evaluated for BM prediction. ROC curve analysis of
the combined approach in the overall cohort yielded an AUC of
0.776. Following stratification by EGFR mutation status, the AUC
increased to 0.820 in the EGFR-mutated subgroup and further to
0.871 in the 19del subgroup (Fig.
4). These findings demonstrate that the combined approach
outperforms individual biomarkers for BM prediction in LUAD, with
the performance further enhanced in EGFR mutation-enriched
subgroups.
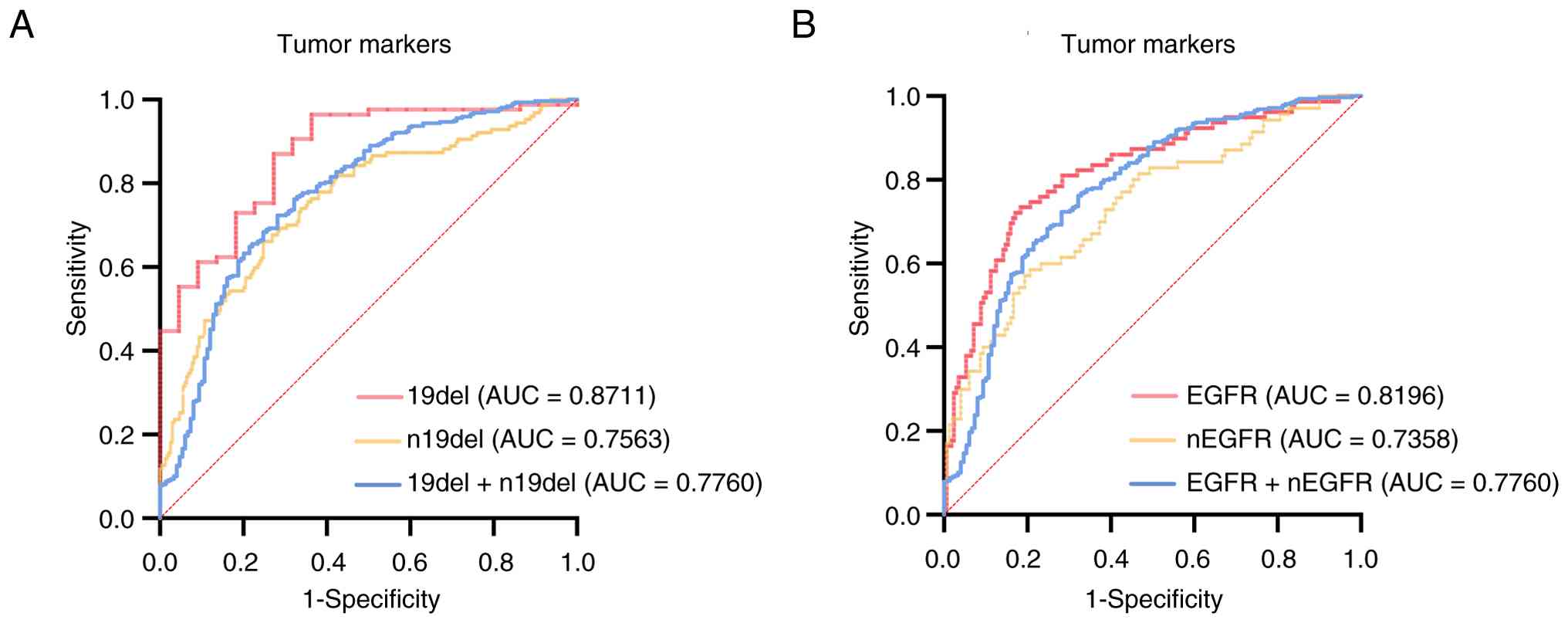 | Figure 4.ROC curves of the combined method for
the prediction of brain metastasis in lung adenocarcinoma. ROC
curves of combined tumor markers, including NSE, CEA, CA125, CA153
and CYFRA21-1, were analyzed in subgroups of (A) 19del and (B) EGFR
mutations. ROC, receiver operating characteristic; AUC, area under
the ROC curve; NSE, neuron-specific enolase; CYFRA21-1, cytokeratin
19 fragment; 19del, exon 19 deletion. |
Verification of the prediction
formulation of BM in LUAD
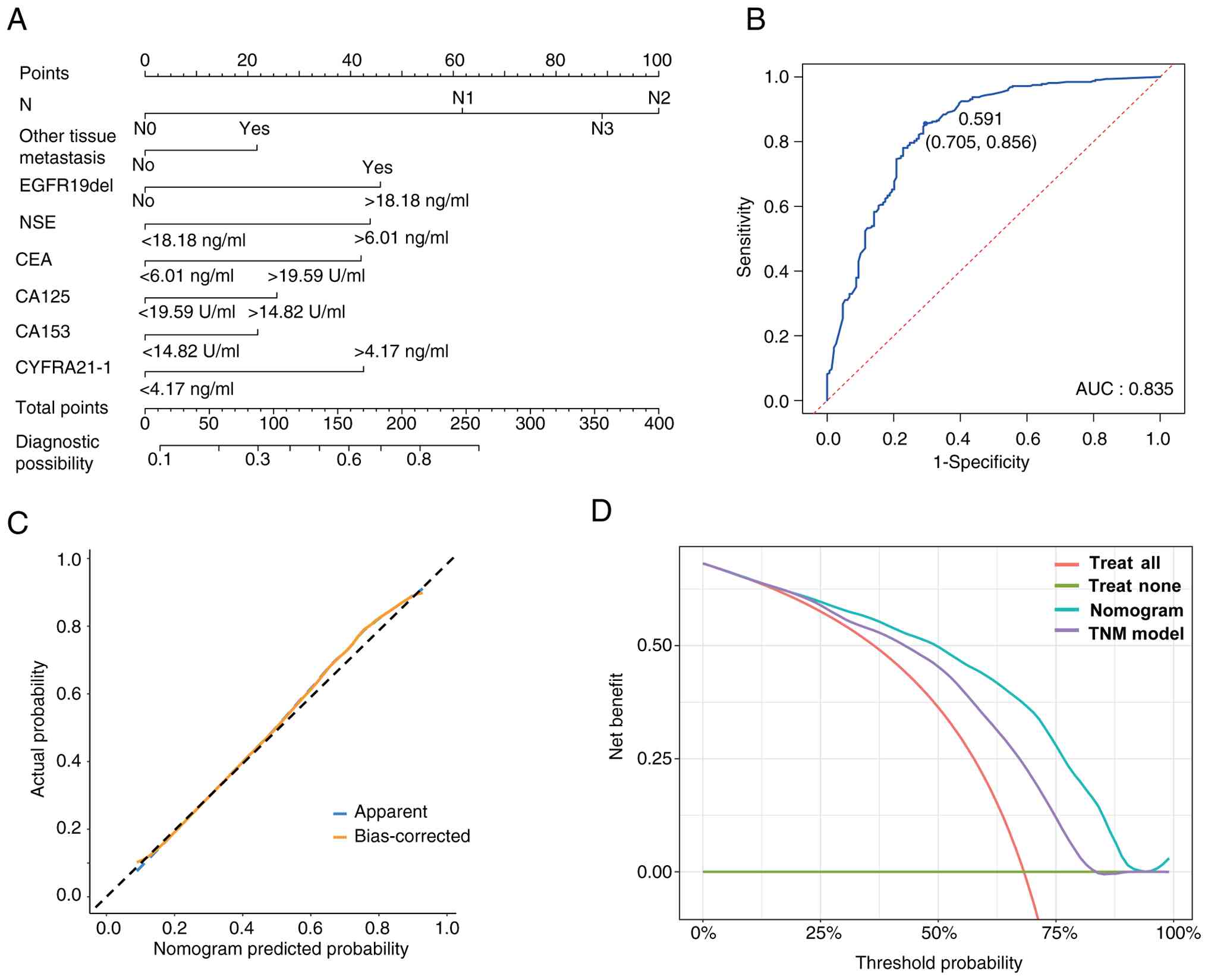
Multivariate logistic regression analysis identified
eight variables independently associated with BM in patients with
LUAD, including N stage, other tissue metastasis, EGFR 19del, NSE,
CEA, CA125, CA153 and CYFRA21-1. The resulting risk prediction
formula was as follows: Logit (P)=−2.4028 + 1.0930(N1) + 1.7697(N2)
+ 1.5743(N3) + 0.3853 (other tissue metastasis) + 0.8107(EGFR
19del) + 0.7753 (NSE >18.18 ng/ml) + 0.7440 (CEA > 6.01
ng/ml) + 0.4539 (CA125 >19.59 U/ml) + 0.3879 (CA153 >14.82
U/ml) + 0.7526 (CYFRA21-1 >4.17 ng/ml), with an optimal
probability cutoff of 0.591. A nomogram incorporating these eight
variables was constructed for individualized BM risk prediction
(Fig. 5A). In the 10-fold
cross-validation, the nomogram achieved a mean AUC of 0.814,
sensitivity of 0.564 and specificity of 0.906 across the 10
iterations (Table SIV). The
nomogram achieved an AUC of 0.835 on the training set ROC curve
(Fig. 5B). Calibration curves
demonstrated close agreement between predicted and observed BM
frequencies across the cohort, confirming good model calibration
(Fig. 5C). DCA demonstrated that
the nomogram provided greater net clinical benefit than the TNM
staging model across a wide range of threshold probabilities
(Fig. 5D). Furthermore, compared
with the TNM-only model, the nomogram yielded an NRI of 0.210
(P<0.001) and an IDI of 0.147 (P<0.001), indicating that
incorporation of EGFR 19del mutation status and the five serum
biomarkers significantly improved the predictive performance over
TNM staging alone.
Discussion
BM is a critical complication that significantly
affects the survival and prognosis of patients with LC (2,17).
Early identification and risk monitoring of BM may provide a
critical window for timely intervention and help prevent disease
progression in patients with LC (18,19).
On the basis of its distinct pathological characteristics and high
BM incidence, LUAD was selected as the study population. Given that
EGFR mutations contribute to tumor development and guide targeted
therapy selection, it was hypothesized that specific mutation
subtypes may differentially influence BM risk and accordingly, a
subtype-level analysis was conducted. To identify a clinically
applicable marker for BM risk assessment, the EGFR mutation status
was integrated with serum LC-related biomarkers to develop a
combined predictive approach and its performance was evaluated in
patients with LUAD. A nomogram incorporating the identified
predictors was subsequently constructed and internally validated.
In summary, this study aimed to identify reliable biomarkers for
early BM risk stratification in LUAD and to develop a combined
approach integrating qualitative and quantitative indicators for
individualized BM prediction.
EGFR plays a central physiological role in
regulating epithelial tissue development and homeostasis, and
serves as a key driver of tumorigenesis, particularly in LC and
glioblastoma (20–22). As a member of the ErbB family of
receptor tyrosine kinases, EGFR regulates multiple downstream
signaling pathways, including the Ras/MAPK, PI3K/AKT, phospholipase
C/protein kinase C and STAT pathways (20,23,24).
These EGFR-mediated pathways are critical regulators of cell
proliferation, apoptosis, migration and survival-processes central
to LC progression (23,25). Clinical studies have demonstrated
that patients with EGFR-mutated NSCLC face a substantially elevated
risk of developing BM (26–28). In one cohort study, the cumulative
BM incidence among patients with EGFR-mutated NSCLC reached 47% at
3 years and 53% at 5 years (29).
Gene-targeted therapies, such as EGFR TKIs, suppress EGFR-mediated
signaling and have become a cornerstone of LC treatment (30). EGFR TKIs have demonstrated efficacy
in controlling CNS progression and are recommended for the
treatment of BM, including leptomeningeal metastases (31–33).
The efficacy of EGFR TKIs against BM has been further supported by
several landmark phase III trials, including FLAURA, AENEAS and
FURLONG (34–36). Collectively, these findings
underscore the pivotal role of EGFR signaling in BM development in
LC. An epidemiological study reported that activating EGFR
mutations are present in at least 50% of Asian patients with NSCLC
(37). EGFR mutation status is
increasingly recognized as a clinically important biomarker in LC
(38). In the present study, the
distribution of EGFR mutations was compared between BM and non-BM
groups in a Chinese LUAD cohort of 615 patients and no significant
difference in the overall proportion of EGFR-mutated patients was
found between groups. This finding suggests that different EGFR
mutation subtypes may exert distinct functional effects on BM
development, as individual mutations differ in their impact on EGFR
signaling activity. Therefore, precise subtype-level classification
of EGFR mutations is essential for a more nuanced understanding of
their respective roles in BM development.
The 19del is among the most common activating
mutations in EGFR, accounting for 85–90% of sensitizing mutations,
and is strongly associated with LUAD histology (39,40).
The most prevalent 19del variants are clustered within the 746–750
amino acid range, while other EGFR mutation types include the L858R
point mutation and uncommon variants such as G719S, L861Q and
C-helix deletions (41–43). LUAD patients harboring common 19del
variants demonstrate a favorable response to TKI treatment in ~75%
of cases, along with superior progression-free and overall
survival, although response rates are lower in patients with the
rare C-helix deletion subtype (44–46).
Compared with patients harboring L858R or uncommon mutations, those
with 19del mutations generally achieve better clinical outcomes
(44,45). A study using 19del-mutant LC cell
lines demonstrated that EGFR-TKIs effectively suppress EGFR pathway
activation, including downstream AKT and ERK signaling (47). These findings indicate that the
19del mutation exerts distinct effects on EGFR function in the
pathogenesis of LUAD. Clinical studies have further demonstrated
that 19del may serve as a favorable prognostic biomarker in LUAD
(40). However, BM represents a
well-established indicator of poor prognosis in LUAD, and its
relationship with the 19del mutation has remained to be elucidated.
In the present study, it was found that patients with LUAD
harboring 19del mutations had a significantly higher BM rate than
those with other EGFR genotypes.
These findings suggest that 19del may enhance the
invasive ability of LUAD cells. A prior in vitro study
demonstrated that ectopic expression of mutated EGFR-including
constructs harboring either the 19del or the L858R point
mutation-induced epithelial-to-mesenchymal transition-like
morphological changes and promoted cell migration in LUAD cells,
effects not observed with wild-type EGFR; consistent with these
findings, vimentin expression was significantly elevated in
EGFR-mutated clinical tumor specimens compared with wild-type
counterparts, supporting a biological basis for enhanced tumor cell
dissemination (48). Notably, the
two common EGFR mutation subtypes displayed comparable migratory
potential in vitro, suggesting that differences in intrinsic
invasive capacity alone may not fully account for the elevated BM
risk associated with 19del observed in the present study. A
complementary explanation is that the prolonged overall survival
conferred by 19del mutations may extend the temporal window for
intracranial dissemination and colonization, particularly given the
limited blood-brain barrier penetration of first-generation
EGFR-TKIs (48,49). At the molecular level, sustained
activation of EGFR-mediated signaling pathways-including RAS/MAPK
and PI3K/AKT-upregulates matrix metalloproteinase expression and
promotes extracellular matrix degradation, potentially facilitating
tumor cell transgression across the blood-brain barrier (49). The precise molecular mechanisms
specifically linking 19del to elevated BM risk warrant dedicated
investigation in future in vitro and in vivo studies
(50). From a clinical perspective,
the elevated BM risk associated with 19del appears to contradict
the favorable prognosis previously reported for this mutation
subtype; however, this discrepancy may be attributable to the
pronounced efficacy of TKI therapy in 19del-mutated LUAD, whereby
targeted treatment partially suppresses the invasive phenotype
induced by this mutation, ultimately contributing to improved
overall outcomes (51,52).
An ideal dynamic indicator for the real-time
evaluation, prediction and monitoring of BM risk remains lacking in
clinical practice. EGFR mutation status may assist in BM risk
prediction in LUAD but cannot serve as a real-time quantitative
monitoring index (53). Serum
biomarkers-including NSE, CEA, CA125, CA153 and CYFRA21-1-have been
employed as quantitative indices for LC risk assessment based on
their measurable serum concentrations (54,55).
Among single biomarkers-including CA-125, CA-199, CA-153,
α-fetoprotein and CEA-CYFRA21-1 demonstrated the highest diagnostic
performance for ocular metastasis in patients with LC with
hypertension, achieving a sensitivity of 77.6%, specificity of
87.0% and AUC of 0.875 (56).
Another study demonstrated that a combination of CA-125, CA-153 and
CYFRA21-1 could facilitate the diagnosis of ocular metastasis in
male patients with LC, achieving an AUC of 0.859 (57). In the context of BM, baseline serum
concentrations of CEA, CYFRA21-1 and NSE, evaluated as individual
indices, have also been associated with prognosis in patients with
LC with BM (58,59). However, most prior studies focused
on the predictive value of individual serum biomarkers for BM
without incorporating the EGFR mutation genotype. In the present
study, quantitative serum biomarker data were integrated with
qualitative EGFR mutation genotype information to develop a
combined approach for BM risk prediction. The results demonstrated
that these serum biomarkers exhibited meaningful predictive value
for BM in LUAD and their integration with EGFR mutation
status-particularly 19del-yielded an improved predictive
performance, as reflected by higher AUC values across subgroup
analyses. These findings suggest that integrating EGFR mutation
subtype information with serum biomarker profiling may provide a
more precise approach for BM risk stratification in clinical
practice.
Of note, the present study has several limitations.
First, it was a single-center retrospective study in which matching
was performed only for age and sex; prior treatment exposure before
blood collection cannot be fully excluded in patients with
metachronous BM, representing an inherent limitation of the
retrospective design. Second, the timing of enhanced MRI was
determined by attending clinicians based on individual clinical
presentation rather than a standardized surveillance protocol, and
the possibility of missed diagnoses in asymptomatic patients cannot
be entirely excluded. Third, the sample size of the 19del subgroup
was relatively limited (n=142), and subgroup-level ROC analyses
should be interpreted as exploratory and hypothesis-generating,
pending confirmation in larger prospective cohorts. Fourth, the
model was validated internally through 10-fold cross-validation
without an independent external validation cohort, which limits the
definitive assessment of its generalizability. Fifth, this study
was conducted in a Chinese cohort with a substantially higher EGFR
mutation prevalence than Western populations, and the biomarker
cutoff values were optimized using the Youden index in this cohort;
both the model's applicability and the cutoff thresholds may
require recalibration before use in populations with different
genetic backgrounds, and prospective validation in multiethnic
cohorts is warranted.
In conclusion, patients with LUAD harboring EGFR
19del mutations demonstrated a significantly elevated risk of BM
compared with those carrying other mutation subtypes. Elevated
serum concentrations of NSE, CEA, CA125, CA153 and CYFRA21-1 were
associated with increased BM risk in patients with LUAD. The
combined nomogram integrating EGFR 19del mutation status with five
serum biomarkers demonstrated robust discriminatory performance and
may serve as an effective tool for individualized BM risk
stratification in LUAD. This approach offers a feasible framework
combining quantitative serum indices with qualitative genetic
information, and warrants prospective validation in multicenter
cohorts to confirm its clinical applicability.
Supplementary Material
Supporting Data
Supporting Data
Acknowledgements
Not applicable.
Funding
This work was supported by the National Natural Science
Foundation of China (grant no. 81701254) and the General Project of
Basic and Applied Basic Research of Guangzhou Bureau of Science and
Technology (grant no. 02-408-2501-2235).
Availability of data and materials
The data generated in this study may be requested
from the corresponding author.
Authors' contributions
MM conceived and designed the study and interpreted
the experiments. MM wrote the main manuscript text. HL and LW
performed the data analysis and statistical modeling, constructed
the nomogram and web-based calculator, and prepared the figures.
XZ, YH, HD and ZL reviewed the medical records, extracted and
verified the clinical and laboratory data, and maintained the study
database. HL and MM checked and confirmed the authenticity of all
the raw data. All authors reviewed the manuscript and have read and
approved the final manuscript.
Ethics approval and consent to
participate
The First Affiliated Hospital of Guangzhou Medical
University Ethics Committee approved this study (approval no.
GZMC2021-06-1237). All procedures were carried out in accordance
with the hospital's policies. All participants provided written
informed consent for the collection, processing and analysis of
blood samples and clinical data for research and publication
purposes.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
AIC
|
Akaike information criterion
|
|
AUC
|
area under the curve
|
|
BM
|
brain metastasis
|
|
CA125
|
cancer antigen 125
|
|
CA153
|
cancer antigen 153
|
|
CEA
|
carcinoembryonic antigen
|
|
CNS
|
central nervous system
|
|
CYFRA21-1
|
cytokeratin 19 fragment
|
|
DCA
|
decision curve analysis
|
|
EGFR
|
epidermal growth factor receptor
|
|
IDI
|
integrated discrimination
improvement
|
|
LC
|
lung cancer
|
|
LUAD
|
lung adenocarcinoma
|
|
NRI
|
net reclassification improvement
|
|
NSCLC
|
non-small cell lung cancer
|
|
NSE
|
neuron-specific enolase
|
|
ROC
|
receiver operating characteristic
|
|
TKI
|
tyrosine kinase inhibitor
|
|
19del
|
exon 19 deletion
|
References
|
1
|
Zheng RS, Chen R, Han BF, Wang SM, Li L,
Sun KX, Zeng HM, Wei WW and He J: Cancer incidence and mortality in
China, 2022. Zhonghua Zhong Liu Za Zhi. 46:221–231. 2024.(In
Chinese). PubMed/NCBI
|
|
2
|
Thawani R, Fakhoury K and Becker KD: Cause
of mortality in patients with lung cancer and brain metastasis. J
Clin Oncol. 38:e21743. 2020. View Article : Google Scholar
|
|
3
|
Ernani V and Stinchcombe TE: Management of
brain metastases in non-small-cell lung cancer. J Oncol Pract.
15:563–570. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Howlader N, Forjaz G, Mooradian MJ, Meza
R, Kong CY, Cronin KA, Mariotto AB, Lowy DR and Feuer EJ: The
effect of advances in lung-cancer treatment on population
mortality. N Engl J Med. 383:640–649. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Duma N, Santana-Davila R and Molina JR:
Non-small cell lung cancer: Epidemiology, screening, diagnosis, and
treatment. Mayo Clin Proc. 94:1623–1640. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Suda K, Mitsudomi T, Shintani Y, Okami J,
Ito H, Ohtsuka T, Toyooka S, Mori T, Watanabe SI, Asamura H, et al:
Clinical impacts of EGFR mutation status: Analysis of 5780
surgically resected lung cancer cases. Ann Thorac Surg.
111:269–276. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhang YL, Yuan JQ, Wang KF, Fu XH, Han XR,
Threapleton D, Yang ZY, Mao C and Tang JL: The prevalence of EGFR
mutation in patients with non-small cell lung cancer: A systematic
review and meta-analysis. Oncotarget. 7:78985–78993. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Johnson M, Garassino MC, Mok T and
Mitsudomi T: Treatment strategies and outcomes for patients with
EGFR-mutant non-small cell lung cancer resistant to EGFR tyrosine
kinase inhibitors: Focus on novel therapies. Lung Cancer.
170:41–51. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cooper AJ, Sequist LV and Lin JJ:
Third-generation EGFR and ALK inhibitors: Mechanisms of resistance
and management. Nat Rev Clin Oncol. 19:499–514. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Thomas NJ, Myall NJ, Sun F, Patil T,
Mushtaq R, Yu C, Sinha S, Pollom EL, Nagpal S, Camidge DR, et al:
Brain metastases in EGFR- and ALK-positive NSCLC: Outcomes of
central nervous system-penetrant tyrosine kinase inhibitors alone
versus in combination with radiation. J Thorac Oncol. 17:116–129.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Porta R, Sánchez-Torres JM, Paz-Ares L,
Massutí B, Reguart N, Mayo C, Lianes P, Queralt C, Guillem V,
Salinas P, et al: Brain metastases from lung cancer responding to
erlotinib: The importance of EGFR mutation. Eur Respir J.
37:624–631. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hsu F, De Caluwe A, Anderson D, Nichol A,
Toriumi T and Ho C: EGFR mutation status on brain metastases from
non-small cell lung cancer. Lung Cancer. 96:101–107. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Liao L, Ji X, Ge M, Zhan Q, Huang R, Liang
X and Zhou X: Characterization of genetic alterations in brain
metastases from non-small cell lung cancer. FEBS Open Bio.
8:1544–1552. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhang Z, Yuan F, Chen R, Li Y, Ma J, Yan
X, Wang L, Zhang F, Tao H, Guo D, et al: Dynamics of serum tumor
markers can serve as a prognostic biomarker for chinese advanced
non-small cell lung cancer patients treated with immune checkpoint
inhibitors. Front Immunol. 11:11732020. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Xie X, Qiu G, Chen Z, Liu T, Yang Y, You
Z, Zeng C, Lin X, Xie Z, Qin Y, et al: Characteristics and
prognosis of EGFR mutations in small cell lung cancer patients in
the NGS era. Clin Transl Oncol. 26:434–445. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Schoenfeld DA and Richter JR: Nomograms
for calculating the number of patients needed for a clinical trial
with survival as an endpoint. Biometrics. 38:163–170. 1982.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Page S, Milner-Watts C, Perna M, Janzic U,
Vidal N, Kaudeer N, Ahmed M, McDonald F, Locke I, Minchom A, et al:
Systemic treatment of brain metastases in non-small cell lung
cancer. Eur J Cancer. 132:187–198. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Chen BT, Jin T, Ye N, Mambetsariev I,
Daniel E, Wang T, Wong CW, Rockne RC, Colen R, Holodny AI, et al:
Radiomic prediction of mutation status based on MR imaging of lung
cancer brain metastases. Magn Reson Imaging. 69:49–56. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Chen S, Hua X, Jia J, Wu Y, Wei S, Xu L,
Han S, Zhang H and Zhu X: Risk factors for brain metastases in
patients with non-small cell lung cancer: A meta-analysis of 43
studies. Ann Palliat Med. 10:3657–3672. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Oprita A, Baloi SC, Staicu GA, Alexandru
O, Tache DE, Danoiu S, Micu ES and Sevastre AS: Updated insights on
EGFR signaling pathways in glioma. Int J Mol Sci. 22:5872021.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Du Z, Brown BP, Kim S, Ferguson D, Pavlick
DC, Jayakumaran G, Benayed R, Gallant JN, Zhang YK, Yan Y, et al:
Structure-function analysis of oncogenic EGFR kinase domain
duplication reveals insights into activation and a potential
approach for therapeutic targeting. Nat Commun. 12:13822021.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Romano R and Bucci C: Role of EGFR in the
nervous system. Cells. 9:18872020. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Uribe ML, Marrocco I and Yarden Y: EGFR in
cancer: Signaling mechanisms, drugs, and acquired resistance.
Cancers (Basel). 13:27482021. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Cheng WL, Feng PH, Lee KY, Chen KY, Sun
WL, VanHiep N, Luo CS and Wu SM: The role of EREG/EGFR pathway in
tumor progression. Int J Mol Sci. 22:128282021. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sigismund S, Avanzato D and Lanzetti L:
Emerging functions of the EGFR in cancer. Mol Oncol. 12:3–20. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Piper-Vallillo AJ, Sequist LV and
Piotrowska Z: Emerging treatment paradigms for EGFR-mutant lung
cancers progressing on osimertinib: A Review. J Clin Oncol.
38:2926–2936. 2020. View Article : Google Scholar
|
|
27
|
Hayashi H, Nadal E, Gray JE, Ardizzoni A,
Caria N, Puri T and Grohe C: Overall treatment strategy for
patients with metastatic NSCLC with activating EGFR mutations. Clin
Lung Cancer. 23:e69–e82. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Singh R, Lehrer EJ, Ko S, Peterson J, Lou
Y, Porter AB, Kotecha R, Brown PD, Zaorsky NG and Trifiletti DM:
Brain metastases from non-small cell lung cancer with EGFR or ALK
mutations: A systematic review and meta-analysis of
multidisciplinary approaches. Radiother Oncol. 144:165–179. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Rangachari D, Yamaguchi N, VanderLaan PA,
Folch E, Mahadevan A, Floyd SR, Uhlmann EJ, Wong ET, Dahlberg SE,
Huberman MS and Costa DB: Brain metastases in patients with
EGFR-mutated or ALK-rearranged non-small-cell lung cancers. Lung
Cancer. 88:108–111. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Girard N: New strategies and novel
combinations in EGFR TKI-resistant non-small cell lung cancer. Curr
Treat Options Oncol. 23:1626–1644. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ma J, Pang X, Zhang S, Huang L, Sun L and
Han C: First-line treatment of EGFR-mutated non-small cell lung
cancer with brain metastases: A systematic review and
meta-analysis. Sci Rep. 14:229012024. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Pecci F, Cantini L, Metro G, Ricciuti B,
Lamberti G, Farooqi AA and Berardi R: Non-small-cell lung cancer:
How to manage EGFR-mutated disease. Drugs Context. 11:2022–4-1.
2022. View Article : Google Scholar
|
|
33
|
Kwon BS, Cho YH, Yoon SK, Lee DH, Kim SW,
Kwon DH, Lee JC and Choi CM: Impact of clinicopathologic features
on leptomeningeal metastasis from lung adenocarcinoma and treatment
efficacy with epidermal growth factor receptor tyrosine kinase
inhibitor. Thorac Cancer. 11:436–442. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Shi Y, Chen G, Wang X, Liu Y, Wu L, Hao Y,
Liu C, Zhu S, Zhang X, Li Y, et al: Furmonertinib (AST2818) versus
gefitinib as first-line therapy for Chinese patients with locally
advanced or metastatic EGFR mutation-positive non-small-cell lung
cancer (FURLONG): A multicentre, double-blind, randomised phase 3
study. Lancet Respir Med. 10:1019–1028. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Lu S, Dong X, Jian H, Chen J, Chen G, Sun
Y, Ji Y, Wang Z, Shi J, Lu J, et al: AENEAS: A randomized phase III
trial of aumolertinib versus gefitinib as first-line therapy for
locally advanced or metastatic non-small-cell lung cancer with EGFR
Exon 19 deletion or L858R mutations. J Clin Oncol. 40:3162–3171.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Ohe Y, Ramalingam S, Reungwetwattana T,
Chewaskulyong B, Dechaphunkul A, Lee KH, Imamura F, Nogami N, Cheng
Y and Cho BC: Osimertinib vs standard of care EGFR-TKI as
first-line treatment in patients with EGFRm advanced NSCLC: FLAURA.
Ann Oncol. 28:x1252017. View Article : Google Scholar
|
|
37
|
Shi Y, Au JSK, Thongprasert S, Srinivasan
S, Tsai CM, Khoa MT, Heeroma K, Itoh Y, Cornelio G and Yang PC: A
prospective, molecular epidemiology study of EGFR mutations in
Asian patients with advanced non-small-cell lung cancer of
adenocarcinoma histology (PIONEER). J Thorac Oncol. 9:154–162.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Lim C, Tsao MS, Le LW, Shepherd FA, Feld
R, Burkes RL, Liu G, Kamel-Reid S, Hwang D, Tanguay J, et al:
Biomarker testing and time to treatment decision in patients with
advanced nonsmall-cell lung cancer. Ann Oncol. 26:1415–1421. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Zhang Y, Ma Y, Li Y, Shen X, Yu Y, Pan Y,
Zhang Y, Yu S, Zheng D, Zhao Y, et al: Are exon 19 deletions and
L858R different in early stage lung adenocarcinoma? J Cancer Res
Clin Oncol. 144:165–171. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Peng X, Long X, Liu L, Zeng L, Yang H,
Jiang W, Liao D, Li K, Wang J and Lizaso A: Clinical impact of
uncommon epidermal growth factor receptor exon 19
insertion-deletion variants on epidermal growth factor
receptor-tyrosine kinase inhibitor efficacy in non-small-cell lung
cancer. Eur J Cancer. 141:199–208. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Xu CW, Lei L, Wang WX, Lin L, Zhu YC, Wang
H, Miao LY, Wang LP, Zhuang W, Fang MY, et al: Molecular
characteristics and clinical outcomes of EGFR exon 19 C-Helix
deletion in non-small cell lung cancer and response to EGFR TKIs.
Transl Oncol. 13:1007912020. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Vyse S and Huang PH: Targeting EGFR exon
20 insertion mutations in non-small cell lung cancer. Signal
Transduct Target Ther. 4:52019. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Gu W, Lu Z, Shi S, Ma J, Lu G, Deng W,
Ding R and Bu F: Molecular characteristics of EGFR exon 19 deletion
subtypes in NSCLC patients. J Clin Oncol. 39:8530. 2021. View Article : Google Scholar
|
|
44
|
Meador CB, Sequist LV and Piotrowska Z:
Targeting EGFR exon 20 insertions in non-small cell lung cancer:
Recent advances and clinical updates. Cancer Discov. 11:2145–2157.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Russo A, Franchina T, Ricciardi G,
Battaglia A, Picciotto M and Adamo V: Heterogeneous responses to
epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors
(TKIs) in patients with uncommon EGFR mutations: New insights and
future perspectives in this complex clinical scenario. Int J Mol
Sci. 20:14312019. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Schrock AB, Frampton GM, Herndon D,
Greenbowe JR, Wang K, Lipson D, Yelensky R, Chalmers ZR, Chmielecki
J, Elvin JA, et al: Comprehensive genomic profiling identifies
frequent drug-sensitive EGFR exon 19 deletions in NSCLC not
identified by prior molecular testing. Clin Cancer Res.
22:3281–3285. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Lu Z, Yi Y, Wang L, Luo Y, Luo D, Xiong L,
Shu Y, Luo H, Li J, Zhu W, et al: Non-small cell lung cancer cells
with uncommon EGFR exon 19delins variants respond poorly to
third-generation EGFR inhibitors. Transl Oncol. 39:1018342024.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Hsiao SH, Chou YT, Lin SE, Hsu RC, Chung
CL, Kao YR, Liu HE and Wu CW: Brain metastases in patients with
non-small cell lung cancer: The role of mutated-EGFRs with an exon
19 deletion or L858R point mutation in cancer cell dissemination.
Oncotarget. 8:53405–53418. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Wang H, Wang L, Gao N, Li H, Yang F, Liu
Z, Li H and Li X: Advances in the treatment of brain metastases in
EGFR-mutant non-small cell lung cancer. Lung Cancer.
206:1086412025. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Yenerall P, Kittler R and Minna J:
Structure-based classification of EGFR mutations informs inhibitor
selection for lung cancer therapy. Cancer Cell. 39:1455–1457. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Ju JS, Huang ACC, Tung PH, Huang CH, Chiu
TH, Wang CC, Ko HW, Chung FT, Hsu PC, Fang YF, et al: Brain
metastasis, EGFR mutation subtype and generation of EGFR-TKI
jointly influence the treatment outcome of patient with EGFR-mutant
NSCLC. Sci Rep. 13:203232023. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Huang LT, Zhang SL, Han CB and Ma JT:
Impact of EGFR exon 19 deletion subtypes on clinical outcomes in
EGFR-TKI-Treated advanced non-small-cell lung cancer. Lung Cancer.
166:9–16. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Wang G, Wang B, Wang Z, Li W, Xiu J, Liu Z
and Han M: Radiomics signature of brain metastasis: Prediction of
EGFR mutation status. Eur Radiol. 31:4538–4547. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Liu Y, Dai S, Liu Z, He L, Zhu L, Qin Z,
Fan H, Fang F, Xie Y and Peng X: Serum tumor markers and outcomes
in lung cancer patients with brain metastases: A retrospective
longitudinal cohort study. Transl Lung Cancer Res. 13:2282–2295.
2024. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Wu H, Wang Q, Liu Q, Zhang Q, Huang Q and
Yu Z: The serum tumor markers in combination for clinical diagnosis
of lung cancer. Clin Lab. 66:2020. View Article : Google Scholar
|
|
56
|
Tang J, Ge QM, Huang R, Shu HY, Su T, Wu
JL, Pan YC, Liang RB, Zhang LJ, Shao Y and Yu Y: Clinical
significance of CYFRA21-1, AFP, CA-153, CEA, and CA-199 in the
diagnosis of lung cancer ocular metastasis in hypertension
population. Front Cardiovasc Med. 8:6705942021. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Li B, Yuan Q, Zou YT, Su T, Lin Q, Zhang
YQ, Shi WQ, Liang RB, Ge QM, Li QY and Shao Y: CA-125, CA-153, and
CYFRA21-1 as clinical indicators in male lung cancer with ocular
metastasis. J Cancer. 11:2730–2736. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Cedrés S, Nuñez I, Longo M, Martinez P,
Checa E, Torrejón D and Felip E: Serum tumor markers CEA,
CYFRA21-1, and CA-125 are associated with worse prognosis in
advanced non-small-cell lung cancer (NSCLC). Clin Lung Cancer.
12:172–179. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Zhang L, Liu D, Li L, Pu D, Zhou P, Jing
Y, Yu H, Wang Y, Zhu Y, He Y, et al: The important role of
circulating CYFRA21-1 in metastasis diagnosis and prognostic value
compared with carcinoembryonic antigen and neuron-specific enolase
in lung cancer patients. BMC Cancer. 17:962017. View Article : Google Scholar : PubMed/NCBI
|