Introduction
Endometrial cancer is the most frequent
gynaecological type of cancer. Hysterectomy with bilateral
oophorectomy and pelvic with or without paraaortic lymphadenectomy
are the primary therapeutic treatments available for endometrial
cancer. Although the therapeutical value of lymphadenectomy is
still under discussion, it is usually necessary to correctly stage
endometrial cancer to determine whether or not adjuvant therapy is
necessary. Since endometrial cancer more frequently occurs in
elderly and overweight patients, the availability of a
preoperative, non-surgical staging method would be beneficial for
these patients. Such a method would reduce morbidity which occurs
inherently with lymphadenectomy.
The growth of solid neoplasms is always accompanied
by neovascularisation. Tumour cells appear to stimulate endothelial
cell proliferation. Moreover, endothelial cells may have an
indirect effect over the rate of tumour growth. Solid tumours are
dependent on angiogenesis for growth when they reach a size of 2–3
mm (1). Tumour and normal
endothelium are distinct at the molecular level. In order to
identify whether molecular markers are differentially expressed in
normal- and tumour-derived endothelium, St Croix et al
performed serial gene expression analyses on human endothelial
cells isolated from normal colonic mucosa or from colorectal
tumours. The authors identified 46 transcripts, named tumour
endothelial markers (TEMs), which were significantly up-regulated
in tumour compared with normal endothelium. Nine (TEM-1 to -9) were
investigated. TEMs are specific to tumour endothelial cells and are
potentially involved in tumour angiogenesis. They are more specific
to tumour cells than other endothelial markers similarly involved
in angiogenesis, such as Von Willebrand factor or CD31 (2). Four of the TEMs (TEM-1, -5, -7 and -8)
are located on the cell surface and, thus, would be accessible to
pharmacological agents (3,4). TEM-5 appears to be a seven-pass
G-protein-coupled transmembrane receptor, whereas TEM-1, -7 and -8
span the membrane once (3).
Several different TEMs have been identified in
various, though mostly colorectal, cancer types. Most of the TEMs
can be detected in normal, non-cancerous samples, but are also
expressed at a higher level in tumour tissues. Only TEM-8 was
almost absent in normal tissues while its expression levels were
significantly raised in colon cancer tissues (5). No information on the expression of
TEMs in the endometrium is available in the literature.
This study aimed to investigate whether normal,
eutopic endometrium expressed TEMs and to analyse whether this
expression was more pronounced in endometrial cancer than in
healthy, intra-uterine control tissues.
Materials and methods
Eutopic endometrium (n=8) was sampled with a soft
catheter (Pipelle de Cornier, Laboratoire CCD, France) from
patients undergoing laparoscopic infertility investigations at the
Department of Obstetrics and Gynaecology. Tumour tissue samples
(endometrial cancers of various stages, n=10) were withdrawn from
the Tumour Bank established at the University of Berne. Solid
tissues (endometrium and carcinomata), previously stored in
RNAlater (Sigma, USA) at −80°C or −150°C for the tumour tissues,
were homogenised using a steel bead, lysed and extracted using a
commercial procedure (SV Total RNA isolation system; Promega, USA)
that included an on-column DNase digestion step before elution.
Different cell lines as well as colon cancer tissue
from three patients were included as positive controls. The MCF-7
cell line was obtained from pleura effusion of breast
adenocarcinoma of a 69-year-old female, and was known to express
high levels of TEM-8 (6). The SW620
cell line was derived from lymph node metastasis of a colon
adenocarcinoma of a 51-year-old male, while the line SW480 was
established from primary colon cancer (7). CACO-2 and DLD-1 were similarly derived
from colon adenocarcinomata (8,9).
The cells were cultured in MEM (Iscove’s
modification with 25 mM Hepes; Gibco Invitrogen, Scotland)
containing fetal bovine serum (10% v/v) and antibiotics/antimycotic
(Gibco) to confluence (37°C, 5% CO2 in air). The
adherent cells were then washed with phosphate-buffered saline and
lysed directly on the plate with the lysis buffer provided in the
SV-RNA extraction kit.
Concentration and purity of the RNA were determined
by spectrophotometry at 260 and 280 nm, and by calculating the
ratio between the two values. RNA samples were selected for further
investigation based on their quality as assessed by capillary
electrophoresis (RNA 6000 Nano Labchip®, Agilent
Technologies, USA) and by their 260/280 nm ratio (>1.9).
A 300 ng RNA sample was reverse transcribed with the
Archive® Kit (Applied Biosystems, USA) in one batch in
an incubation of 10 min at 25°C and 60 min at 37°C, and the
resulting cDNA was stored at −30°C until further use. Quantitative
(real-time) polymerase chain reaction (PCR) was performed with
TaqMan® primer/probes (Assay-on-demand®,
Applied Biosystems) for TEM-1, -2, -6, -7, -7r and -8. The PCR
reactions were run on an ABI PRISM® SDS 7900 HT
thermocycler (Applied Biosystems). GAPDH, β-actin and ribosomal
protein L13A (RPL13A) were used as control or reference genes.
Matrix metalloproteinase-2 (MMP-2) and glycodelin (PP14) were
determined as well. Primer and TEM data are summarised in Table I.
 | Table ISummary of tumour endothelial markers
and primer characteristics. |
Table I
Summary of tumour endothelial markers
and primer characteristics.
| Marker | Name | AB gene no. | Amplicon size
(bp) |
|---|
| TEM-1 | Endosialin,
CD248 | Hs00535574_s1 | 81 |
| TEM-2 | RASD family member
2 | Hs00374755_m1 | 84 |
| TEM-6 | Tensin 3 | Hs00224228_m1 | 60 |
| TEM-7 | Plexin domain
containing 1 | Hs00220723_m1 | 58 |
| TEM-7r | Plexin domain
containing 2 | Hs00262350_m1 | 109 |
| TEM-8 | Anthrax toxin
receptor 1 | Hs00216777_m1 | 67 |
| GAPDH | AP dehydrogenase | Hs99999905_m1 | 122 |
| β-actin | β-actin | Hs00242273_m1 | 93 |
| L13A | Ribosomal protein
L13A | Hs01926559_g1 | 105 |
| PP14 | Glycodelin | Hs00171462_m1 | 109 |
| MMP-2 | Metalloproteinase
2 | Hs00234422_m1 | 93 |
Results
Among the six endothelial tumour markers
investigated, TEM-1, -6 and -8 showed the highest expression level
(per ng of reverse transcribed RNA) over all the groups of cells
and tissues. The different positive controls (cell lines and
biopsies of colon carcinomata) showed expression levels which
varied from 0 to the level of GAPDH expression. The controls are
shown in Table II as a percentage
of the GAPDH expression level for that particular tumour
marker.
| Table IIGene expression levels for different
tumour endothelial markers in human cell lines and biopsies of
colon cancer tissue. |
Table II
Gene expression levels for different
tumour endothelial markers in human cell lines and biopsies of
colon cancer tissue.
| GAPDH | TEM-1 | TEM-2 | TEM-6 | TEM-7 | TEM-7r | TEM-8 |
|---|
| Cell line |
| SW620 | 100 | 27.5 | 13.4 | 65.4 | 0.0 | 0.0 | 78.0 |
| SW480 | 100 | 18.3 | 41.6 | 59.4 | 18.2 | 0.0 | 75.1 |
| DLD-1 | 100 | 23.7 | 14.8 | 64.0 | 7.5 | 25.1 | 100.1 |
| CACO-2 | 100 | 50.2 | 0.0 | 62.0 | 3.0 | 14.7 | 14.0 |
| MCF-7 | 100 | 19.9 | 45.0 | 52.3 | 34.0 | 35.5 | 78.2 |
| Colon cancer
tissue |
| No. 504 | 100 | 4.8 | 0.0 | 45.1 | 0.0 | 5.3 | 7.7 |
| No. 516 | 100 | 10.4 | 1.5 | 37.8 | 14.7 | 26.3 | 38.1 |
| No. 564 | 100 | 32.6 | 0.0 | 37.8 | 16.5 | 22.8 | 35.4 |
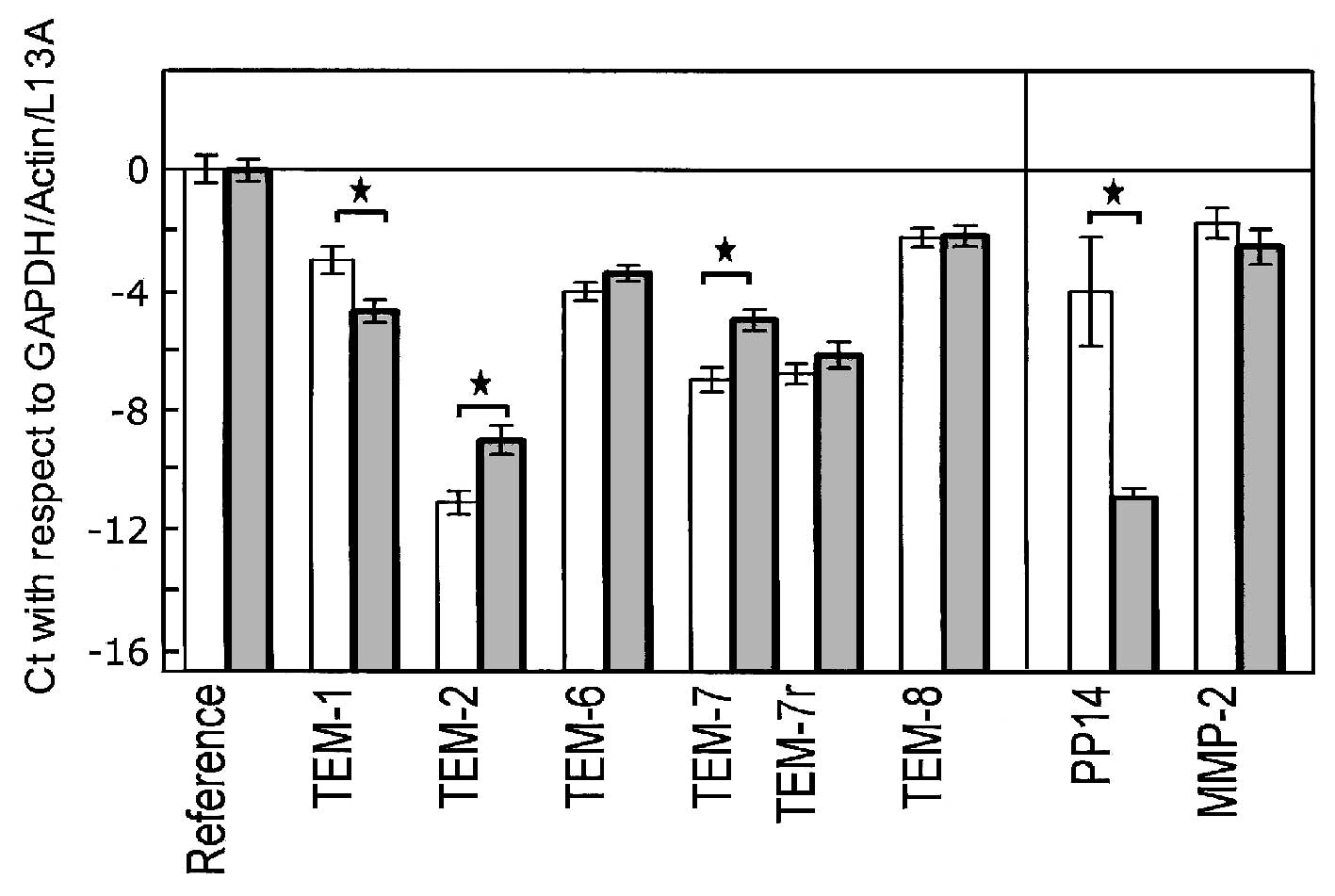
In endometrium, TEM-1 showed a higher expression
level (lower Ct value) in the normal healthy tissues than in the
tumour samples. For all other TEMs, however, we found a marginally
higher expression in the cancer samples than in the normal
endometria. The raw Ct values are shown in Table III for the two groups of tissues.
Statistical significance for the difference in gene expression
between healthy and cancerous endometrium was achieved for TEM-1,
-2 and -7. The results were normalised against GAPDH, β-actin and
L13A (Fig. 1).
| Table IIIRaw Ct values obtained in quantitative
PCR for 6 tumour endothelial markers and 3 reference genes. |
Table III
Raw Ct values obtained in quantitative
PCR for 6 tumour endothelial markers and 3 reference genes.
| Gene (Reference of
TEM) | Healthy endometrium
(n=8) | Endometrial cancer
(n=10) | P-value |
|---|
| Reference |
| GAPDH | 21.42±1.16 | 21.35±1.47 | NS |
| β-Actin | 21.53±1.50 | 21.43±0.85 | NS |
| L13A | 26.87±0.94 | 27.16±1.05 | NS |
| Tumour endothelial
markers |
| TEM-1 | 26.28±1.41 | 27.97±1.22 | 0.015 |
| TEM-2 | 34.25±1.09 | 32.28±1.53 | 0.007 |
| TEM-6 | 27.31±0.83 | 26.70±0.82 | NS |
| TEM-7 | 30.26±1.16 | 28.26±1.12 | 0.002 |
| TEM-7r | 30.06±0.99 | 29.42±1.40 | NS |
| TEM-8 | 25.51±1.59 | 25.46±1.58 | NS |
| Other genes |
| Glycodelin | 27.30±5.10 | 34.18±1.09 | <0.001 |
| MMP-2 | 25.02±1.42 | 25.83±1.84 | NS |
For glycodelin the differential expression between
the two groups of endometrium was much more pronounced, with the Ct
difference at 6.84 after normalisation, corresponding to a 114-fold
down-regulation in carcinoma compared to healthy tissue. No
differential expression was observed for MMP-2.
When the results for the endometrial tumour samples
were analysed with respect to FIGO staging, no correlation between
this stage and the levels of TEM-1, -6 and -8 expression was noted.
The studied TEMs, with the exception of TEM-6, showed the highest
expression in FIGO stage I. Only one tissue sample was assigned to
be FIGO stage IV. Therefore, statistical analysis was not possible.
However, the expression levels for the 6 investigated TEMs were
lower in this sample than in the remaining TEMs which were
expressed in FIGO stages I to III (data not shown).
Discussion
The production of TEM-8 by the MCF-7 cell line
(6) was confirmed. This cell line
also expressed the remaining TEMs studied, and the same was the
case for DLD-1. Table II shows the
values in relation to GAPDH expression. The other colon
adenocarcinoma-derived cell lines expressed the different TEMs to a
varying extent, indicating the specificity of the assays and the
cell lines, and thus validating this study. SW480/SW620 lines
expressed high levels of TEM-6 and -8, but no or little TEM-7/-7r.
CACO-2 expressed no TEM-2 and little TEM-7/-7r, but large levels of
TEM-1 and -6 (Table II). In the 3
tested colon cancer tissue samples, TEM-6 showed the highest
expression level, followed by TEM-8 (Table II), the latter confirming published
data (5) and thus fulfilling the
role of a positive control in this study. TEM-2 expression was low
or undetectable.
We examined the possible expression of TEMs in human
endometrium and endometrial cancer, specifically endometrial
adenocarcinoma, as performed by Davies et al with human
breast cancer (6). The authors
concluded that elevated levels of TEM-1, -7r and -9 (but not TEM-2,
-4, -5, -6 and -7) are associated with either nodal involvement
and/or disease progression, which may therefore have a prognostic
value in breast cancer. Furthermore, the authors showed that TEMs
appeared to be expressed in normal tissues as well. In their study,
TEM-7r and -8 were significantly raised in breast cancer tissues
compared with normal background tissues (10). In contrast, in our study, TEM-2 and
-7 were significantly raised in endometrial cancer tissues compared
with normal endometrium from healthy women. Rmali et al
found that TEM-1, -7, -7r and -8 were significantly raised in colon
cancer tissues compared with normal background tissues from the
same patients. The same TEMs showed an association with both nodal
involvement and disease progression (5). We did not repeat these investigations
but have used breast cancer tissue for validation of our QPCR
setup. TEM-8 was reported to be raised in breast and colon cancer
tissues (5,10,11).
However, as regards the endometrium, we did not observe a
significantly increased TEM-8 gene expression in cancer tissue
compared to healthy tissue. This indicates that TEM-8 shows a
certain level of tissue specificity independent of the presence of
cancer. Glycodelin (PP14) was shown to be negatively associated
with ovarian cancer (12), i.e., it
is a marker of differentiation which is lost in advanced cancer
stages. A large fraction of ovarian cancers are of the endometroid
type. In this study, glycodelin gene expression was determined and
found to be strongly decreased in cancerous compared to healthy
endometrium, which is in agreement with the previously mentioned
report (12), thus validating the
selection of our tissue samples. Moreover, glycodelin was found to
reduce proliferation of endometrial carcinoma cells in vitro
(13). MMP-2 expression, on the
other hand, did not differ between the two tissue types, as
confirmed by a recent report (14).
In a more recent publication, MMP-2 expression was found to be
lower in endometrial cancer than in endometriotic or healthy
proliferative endometrial tissue (15).
With the exception of the known up-regulation of
TEM-8 at the mRNA and protein levels in endothelial cells by
interleukin-1 (16), the role of
TEMs in tumour-associated angiogenesis and the factors which are
able to regulate the expression of TEMs in human endothelial and
cancer cells are unknown. The dependence of neoplasms on
neovascularisation was previously identified and has subsequently
led to substantial research efforts on tumour angiogenesis. Folkman
et al described a tumour angiogenesis factor (TAF) which was
isolated from human and animal tumours, and which was not found in
normal tissues, with the exception of placenta. TAF was shown to
stimulate the rapid formation of new capillaries in animals
(1,17). There are many factors (soluble,
membrane-bound, biomechanical) which stimulate angiogenesis in
normal and tumour tissues, as well as other factors which inhibit
tumour angiogenesis (18).
Angiogenesis normally occurs during fetal growth and development,
but rarely occurs in adults, except during the ovarian cycle
(corpus luteum formation) and in physiological repair processes
such as wound healing (19–21). Focusing on TEM-1 to -9, St Croix
et al showed in their analysis by in situ
hybridization that the expression of TEM transcripts were
associated with the endothelium of cancer types in the corpus
luteum and granulation tissue of healing wounds, with the exception
of TEM-8 which was not detectable in the corpus luteum (2). Furthermore, Carson-Walter et al
identified the counterparts of TEM-1, -5, -7, -7r and -8 in mice
(3).
The case numbers in our study are small.
Consequently, further investigation on the specificity and
significance of TEMs in endometrial and other gynaecological cancer
types should be undertaken with larger sample numbers. The role of
endothelial products at the protein level should also be
investigated. Anti-TEM antibodies are commercially available for
some but not all TEMs studied here, and for these a specific
immunoassay (e.g., ELISA) could be developed for the quantitative
expression of TEMs at the protein level. The antibodies can also be
used to show by immunohistochemistry whether epithelial and/or
stromal cells would express TEMs. Davies et al did not
detect any TEM-8 in the MCF-7 cell line (6). The human endometrium is one of the few
adult tissues that develops new capillaries from existing
microvessels, which then undergo maturation and remodelling. This
process is regulated primarily by the circulating steroids
oestrogen and progesterone (22,23).
If development in a sensitive immunoanalytical detection method for
TEMs at the protein level occurs, the expression of TEMs in the
different stages of the menstrual cycle may be analysed and
compared. Moreover, if the expression of TEMs is dependent on sex
hormones, it would be interesting to investigate whether this
influence is direct or secondary, as in the case of the
up-regulation of the vascular endothelial growth factor (VEGF)
receptor Flk-1/KDR by estradiol, secondary to the up-regulation of
VEGF expression (24).
Acknowledgements
We thank Professor Rolf Jaggi for his help with the
PCR, Daniel Müllener for providing the tumour tissue samples from
the University of Berne Tumour Bank and Anne Vaucher, Andrea Oberli
and Anne Baltzer for their help with technical laboratory
issues.
References
|
1
|
Folkman J: Tumor angiogenesis: Therapeutic
implications. N Engl J Med. 285:1182–1186. 1971. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
St Croix B, Rago C, Velculescu V, et al:
Genes expressed in human tumor endothelium. Science. 289:1197–1201.
2000.PubMed/NCBI
|
|
3
|
Carson-Walter EB, Watkins DN, Nanda A,
Vogelstein B, Kinzler KW and St Croix B: Cell surface tumour
endothelial markers are conserved in mice and humans. Cancer Res.
61:6649–6655. 2001.PubMed/NCBI
|
|
4
|
Nanda A and St Croix B: Tumour endothelial
markers: new targets for cancer therapy. Curr Opin Oncol. 16:44–49.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Rmali KA, Puntis MC and Jiang WG:
Prognostic values of tumor endothelial markers in patients with
colorectal cancer. World J Gastroenterol. 11:1283–1286. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Davies G, Rmali KA, Watkins G, Mansel RE,
Mason MD and Jiang WG: Elevated levels of tumour endothelial
marker-8 in human breast cancer and its clinical significance. Int
J Oncol. 29:1311–1317. 2006.PubMed/NCBI
|
|
7
|
Leibovitz A, Stinson JC, McCombs WB, McCoy
CE, Mazur KC and Mabry ND: Classification of human colorectal
adenocarcinoma cell lines. Cancer Res. 36:4562–4569.
1976.PubMed/NCBI
|
|
8
|
Fogh J: Submission of Caco-2 cell line to
the American Type Culture Collection (ATCC). J Natl Cancer Inst.
58:221–226. 1977.
|
|
9
|
Dexter DL, Barbosa JA and Calabresi P:
N,N-dimethylformamide-induced alteration of cell culture
characteristics and loss of tumorigenicity in cultured human colon
carcinoma cells. Cancer Res. 39:1020–1025. 1979.
|
|
10
|
Davies G, Cunnick GH, Mansel RE, Mason MD
and Jiang WG: Levels of expression of endothelial markers specific
to tumour-associated endothelial cells and their correlation with
prognosis in patients with breast cancer. Clin Exp Metastasis.
21:31–37. 2004. View Article : Google Scholar
|
|
11
|
Rmali KA, Watkins G, Harrison G, Parr C,
Puntis MCA and Jiang WG: Tumour endothelial marker 8 (TEM-8) in
human colon cancer and its association with tumour progression. Eur
J Surg Oncol. 30:948–953. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Mandelin E, Lassus H, Seppala M, et al:
Glycodelin in ovarian serous carcinoma: association with
differentiation and survival. Cancer Res. 63:6258–6264.
2003.PubMed/NCBI
|
|
13
|
Koistinen H, Seppala M, Nagy B, Tapper J,
Knuutila S and Koistinen R: Glycodelin reduces carcinoma-associated
gene expression in endometrial adenocarcinoma cells. Am J Obstet
Gynecol. 193:1955–1960. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Bogusiewicz M, Stryjecka M and Rechberger
T: Activity of matrix metalloproteinases -2 and -9 (MMP-2 and
MMP-9) and content of their tissue inhibitors in endometrial cancer
- a preliminary study. Ginekol Pol. 78:366–372. 2007.PubMed/NCBI
|
|
15
|
Shaco-Levy R, Sharabi S, Benharroch D,
Piura B and Sion-Vardy N: Matrix metalloproteinases -2 and -9,
E-cadherin and beta-catenin expression in endometriosis, low-grade
endometrial carcinoma and non-neoplastic eutopic endometrium. Eur J
Obstet Gynecol Reprod Biol. 139:226–232. 2008. View Article : Google Scholar
|
|
16
|
Rmali KA, Al-Rawi MA, Parr C, Puntis MC
and Jiang WG: Up-regulation of tumour endothelial marker-8 by
interleukin-1β and its impact in IL-1β induced angiogenesis. Int J
Mol Med. 14:75–80. 2004.PubMed/NCBI
|
|
17
|
Folkman J, Merler E, Abernathy C and
Williams G: Isolation of a tumor factor responsible for
angiogenesis. J Exp Med. 133:275–288. 1971. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Papetti M and Herman IM: Mechanisms of
normal and tumour-derived angiogenesis. Am J Physiol Cell Physiol.
282:947–970. 2002. View Article : Google Scholar
|
|
19
|
Folkman J and Klagsbrun M: Angiogenic
factors. Science. 235:442–447. 1987. View Article : Google Scholar
|
|
20
|
Reynolds L, Killilea SD and Redmer DA:
Angiogenesis in the female reproductive system. FASEB J. 6:886–892.
1992.PubMed/NCBI
|
|
21
|
Reynolds L and Redmer DA: Expression of
the angiogenic factors, basic fibroblast growth factor and vascular
endothelial growth factor in the ovary. J Anim Sci. 76:1671–1681.
1998.PubMed/NCBI
|
|
22
|
Gargett CE and Rogers PA: Human
endometrial angiogenesis. Reproduction. 121:181–186. 2001.
View Article : Google Scholar
|
|
23
|
Krikun G, Schatz F and Lockwood CJ:
Endometrial angiogenesis: from physiology to pathology. Ann NY Acad
Sci. 1034:27–35. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hervé MA, Meduri G, Petit FG, Domet TS,
Lazennec G, Mourah S and Perrot M: Regulation of the vascular
endothelial growth factor (VEGF) receptor Flk-1/KDR by estradiol
through VEGF in uterus. J Endol. 188:91–99. 2006.PubMed/NCBI
|