Introduction
Both Hodgkin’s and non-Hodgkin’s types of lymphoma
exist. Non-Hodgkin’s lymphomas often invade extra-lymphatic organs,
while Hodgkin’s lymphomas rarely disseminate to extra-lymphatic
organs. More than 25% of non-Hodgkin’s lymphomas originate from
extra-lymphatic organs, approximately 30% of which may involve the
pancreas (1). Primary pancreatic
lymphomas (PPL) are usually non-Hodgkin’s lymphomas and isolated
PPL is quite rare (2). Only three
cases (1.5%) of pancreatic lymphoma were found in a review of 207
cases of malignant pancreatic tumors (3). Clinically, PPL is likely to be
misdiagnosed as pancreatic cancer. However, patients with PPL
require a different therapeutic approach and have a better
prognosis than those with pancreatic adenocarcinoma. Conventional
imaging modalities alone are not able to differentiate between
pancreatic adenocarcinoma and PPL, although the accurate diagnosis
of PPL is crucial.
The development of a new modality such as F-18
2′-deoxy-2fluoro-D-glucose (FDG) positron emission tomography
combined with computed tomography (PET/CT) has contributed to the
evaluation of human cancers and the usefulness of PET/CT has been
well established for lymphoma staging (4,5).
However, few reports are currently available that pertain to PET/CT
diagnosing PPL. In this study, a 56-year-old man with PPL was
examined using PET/CT imaging. Results showed the unique intense
uptake of FDG in the pancreas with atypical findings of malignancy
in the CT scan and magnetic resonance images (MRI).
Patient and methods
A 56-year-old, asymptomatic man was admitted to
Tokai University Hachioji Hospital for further examination
following an abdominal ultrasound study that showed a mass shadow
in the pancreas. A physical examination did not reveal any abnormal
findings or systemic lymphadenopathy. Blood analysis showed a
slight elevation of the serum interluekin-2 receptor (604 ng/ml)
without other abnormalities, including tumor markers such as
carcinoembryonic antigen and CA19-9. An abdominal CT scan showed a
5-cm tumor located in the head of pancreas, while an enhanced CT
scan showed a slight increase in the tumor without encasement of
arteries or veins. The MRI showed a mass with homogeneously high
signal intensity on T2-weighted images and low signal intensity on
T1-weighted images with gadolinium enhancement (Fig. 1). The CT and MRI findings described
above suggested not pancreatic cancer but massive pancreatitis.
Endoscopic retrograde cholangiopancreatography did not demonstrate
either stenosis or obstruction of either the main pancreatic or
common bile duct. Informed patient consent was obtained, as well as
approval for the study by an ethics committee of our institute.
The patient underwent 18F-FDG PET/CT
scans. PET/CT imaging was performed with Biograph Duo (Siemens
CTI). The Biograph Duo allows for the simultaneous collection of 64
slices over a span of 15.8 cm with a slice thickness of 2.5 mm and
a transaxial resolution of 6.3 mm. All data were reconstructed with
OSEM image. One hour (early scan) after the intravenous
administration of approximately 3.7 Mbq/kg of 18F-FDG, a
transmission scan using CT for attenuation correction and
anatomical imaging was acquired for 90 sec with a delayed scan
after 2 h. To determine the semi-quantitative FDG uptake, regions
of interest (ROIs) were placed over the lesion, including the
highest uptake area (circular ROI, 1 cm in diameter), and the
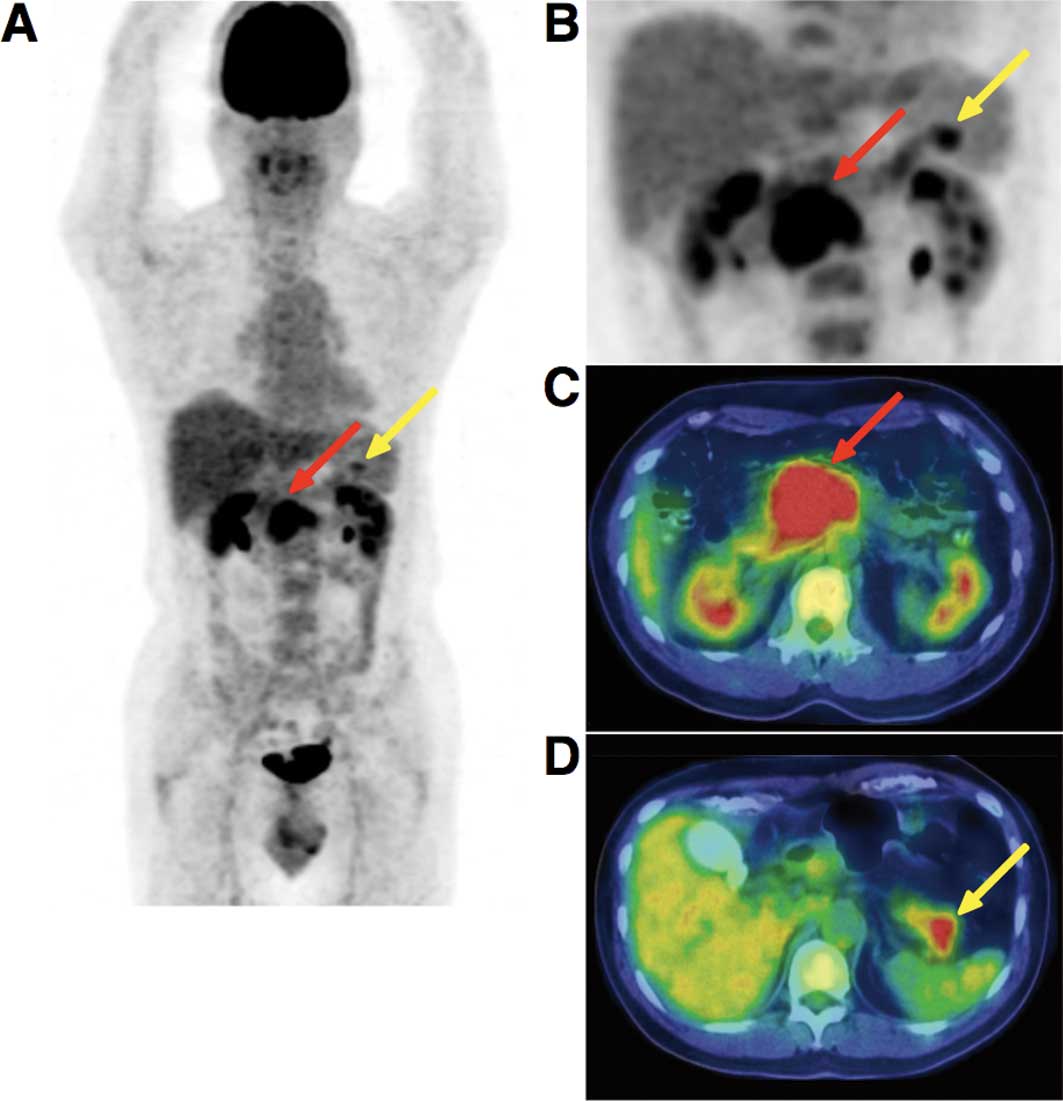
standardized uptake value (SUV) was calculated. The early PET/CT
showed an intense abnormal FDG uptake (SUVmax, 8.67) in the head
and body of the pancreas, and a moderately increased uptake in the
tail of the pancreas (Fig. 2). The
delayed scan demonstrated a more intense FDG uptake (SUVmax, 10.3)
in the pancreas. No other areas showed an abnormal uptake of FDG
apart from the pancreas. The PET/CT findings strongly suggested
malignancy of the pancreas without lymphatic or systemic
metastasis.
Results
Histopathologic study
A laparoscopic examination was performed and biopsy
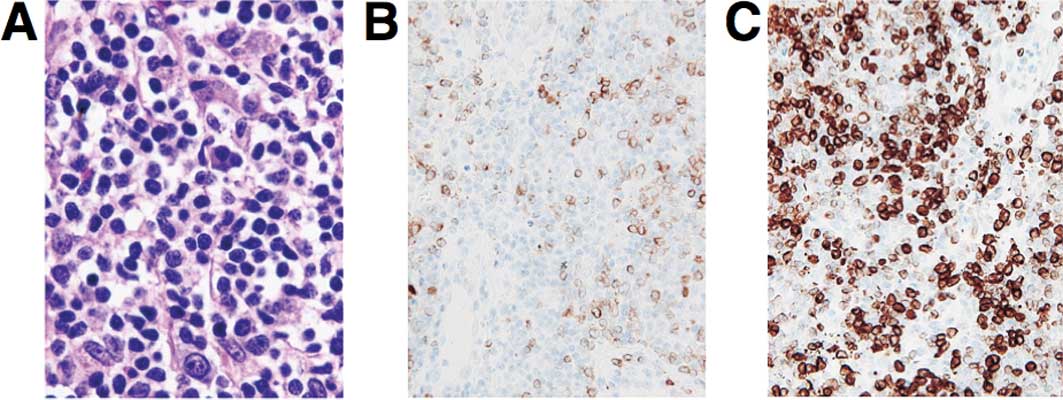
specimens were obtained. Microscopic examination showed diffuse
infiltrative growth of T-lymphoid cells (Fig. 3). Multiple foci of B-lymphoid cells
with small nodular or aggregate features were noted. The B cells
showed a medium to relatively large morphology. The cells were
embedded in the fibrous or hyalinizing stroma. The
immunohistochemical analysis showed that the neoplastic cells were
CD79a(+), CD20(+), BCL-2(+), CD3(−) and CD10(−). The MIB1 (Ki67)
index was ~70–80%. A histopathological examination confirmed the
diagnosis of a low grade B-cell pancreatic lymphoma. The patient
underwent an aspiration biopsy of the bone marrow; however, no
abnormality was noted. He received chemotherapy after surgery.
Discussion
PPL is an extremely rare disease which occurs in the
pancreas, with or without the involvement of peripancreatic lymph
nodes. The clinical manifestation and imaging result of PPL
resembles other pancreatic occupying lesions such as pancreatic
carcinoma. However, unlike carcinomas, PPLs are potentially
treatable even if not found at the early stage. PPL accounts for
fewer than 2% of extra-nodal malignant lymphomas and 0.5% of cases
of pancreatic masses (6,7). Fewer than 150 cases of PPL had been
reported in the literature until 2006 (8).
Imaging results play a key role in the diagnosis of
PPL. Percutaneous ultrasound (US), CT scan and MRI are
well-established procedures used in the evaluation of pancreatic
masses (9,10). CT is the most common imaging
technique used in the detection and characterization of pancreatic
tumors. The CT image of PPL resembles that of pancreatic carcinoma,
including enlargement of the pancreatic head and density changes.
However, fewer signs of invasion of large vessels and metastasis to
the liver and spleen are observed. Pancreatic duct dilation is less
common in PPL compared to pancreatic cancer. Merkle et al
reported that the combination of a bulky localized tumor in the
pancreas without significant dilation of the main pancreatic duct
supports a diagnosis of pancreatic lymphoma as opposed to
adenocarcinoma (11).
MRI findings in PPL usually show homogeneously high
signal intensity on T2-weighted images and low signal intensity on
T1-weighted images (12). Arcari
et al stated that conventional imaging techniques suggest
the suspicion of PPL but are unable to distinguish PPL from
pancreatic adenocarcinoma (13).
PPL is a rare disease with non-specific symptoms, laboratory tests
and imaging examination results (14). Therefore, the final diagnosis of PPL
should depend on a histopathological examination. The first choice
for PPL treatment should be a combination of chemotherapy and
radiotherapy as opposed to surgery. The development of FDG-PET/CT
contributes to the evaluation of human cancer staging and the
usefulness of PET/CT has been well established for lymphoma staging
(5), whereas only one report
regarding PET findings in PPL was previously published (15). Yoon et al reported that
FDG-PET imaging, and not PET/CT, showed round intense FDG uptake in
the center of the midabdomen in a patient with PPL. However,
results of the PET/CT imaging for a 56-year-old man examined in our
study showed a unique intense uptake of FDG in the pancreas as well
as atypical findings of malignancy from a CT scan and MRI. The
results therefore show that further accumulation and analysis of
PET/CT images of PPL may provide additional and novel information
to the data currently available from conventional imaging such as
US, CT and MRI for the evaluation of pancreatic tumors.
Acknowledgements
We thank Mr. Kenji Kawai for his technical
assistance.
References
|
1
|
Behrns KE, Sarr MG and Strickler JG:
Pancreatic lymphoma: is it a surgical disease? Pancreas. 9:662–667.
1994. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Freeman C, Berg JW and Cutler SJ:
Occurrence and prognosis of extranodal lymphomas. Cancer.
29:252–260. 1972. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Reed K, Vose PC and Jarstfer BS:
Pancreatic cancer: 30 year review (1947–1977). Am J Surg.
138:929–933. 1979.PubMed/NCBI
|
|
4
|
Weiler-Sagie M, Bushelev O, Epelbaum R,
Dann EJ, Haim N, Avivi I, Ben-Barak A, Ben-Arie Y, Bar-Shalom R and
Israel O: (18)F-FDG avidity in lymphoma readdressed: a study of 766
patients. J Nucl Med. 51:25–30. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Cronin CG, Swords R, Truong MT,
Viswanathan C, Rohren E, Giles FJ, O’Dwyer M and Bruzzi JF:
Clinical utility of PET/CT in lymphoma. AJR Am J Roentgenol.
194:W91–W103. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zucca E, Roggero E, Bertoni F and Cavalli
F: Primary extranodal non-Hodgkin’s lymphomas. Part 1:
gastrointestinal, cutaneous and genitourinary lymphomas. Ann Oncol.
8:727–737. 1997.
|
|
7
|
Boni L, Benevento A, Dionigi G, Cabrini L
and Dionigi R: Primary pancreatic lymphoma. Surg Endosc.
16:1107–1108. 2002. View Article : Google Scholar
|
|
8
|
Saif MW: Primary pancreatic lymphomas. J
Pancreas. 7:262–273. 2006.
|
|
9
|
McNulty NJ, Francis IR, Platt JF, Cohan
RH, Korobkin M and Gebremariam A: Multi-detector row helical CT of
the pancreas: effect of contrast-enhanced multiphasic imaging on
enhancement of the pancreas, peripancreatic vasculature, and
pancreatic adenocarcinoma. Radiology. 220:97–102. 2001. View Article : Google Scholar
|
|
10
|
Kelekis NL and Semelka RC: MRI of
pancreatic tumors. Eur Radiol. 7:875–886. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Merkle EM, Bender GN and Brambs HJ:
Imaging findings in pancreatic lymphoma: differential aspects. AJR
Am J Roentgenol. 174:671–675. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Masui T, Katayama M, Kobayashi S and
Shimizu S: MR imaging of primary malignant lymphoma of the
pancreas. Radiat Med. 23:213–215. 2005.PubMed/NCBI
|
|
13
|
Arcari A, Anselmi E, Bernuzzi P, Berte R,
Lazzaro A, Moroniz CF, Trabacchi E, Vallisa D, Vercelli A and
Cavanna L: Primary pancreatic lymphoma. Report of five cases.
Haematologica. 90:ECR092005.
|
|
14
|
Lin H, Li SD, Hu XG and Li ZS: Primary
pancreatic lymphoma: report of six cases. World J Gastroenterol.
12:5064–5067. 2006.PubMed/NCBI
|
|
15
|
Yoon SN, Lee MH and Yoon JK: F-18 FDG
positron emission tomography findings in primary pancreatic
lymphoma. Clin Nucl Med. 29:574–575. 2004. View Article : Google Scholar : PubMed/NCBI
|