Introduction
There were 47,130 cases of endometrial cancer in the
United States in 2012 with fatalities of 8,010. Endometrial cancer
accounts for approximately 6% of all cancers in women (1). The incidence of cervical cancer has
been less frequent in developed countries, as a result of check-ups
and vaccine development (2), the
incidence of endometrial cancer, however, is increasing in these
countries (1,3). Most causes of endometrial cancer are
associated with the effect of estrogen on the endometrium, while
unopposed estrogen in association with obesity is also a major risk
factor (3,4).
Approximately 5% of the endometrial cancer cases are
thought to result from genetic predisposition (5). One of the most important genetic
diseases, Lynch syndrome [hereditary non-polyposis colorectal
cancer (HNPCC)], is a hereditary syndrome associated with familial
cancers, including colorectal cancer and Lynch syndrome-related
cancers, such as endometrial cancer (6). The cause of the disease is the
germline mutation of DNA mismatch repair (MMR) genes MLH1, MSH2,
MSH6 and PMS2, characterized by autosomal dominant
inheritance (7). The risk for
cancer development in Lynch syndrome depends on the cancer type and
is particularly high in colorectal and endometrial cancers. Thus,
in patients with Lynch syndrome the risk of developing colorectal
cancer throughout life is approximately 80% and 40–60% in males and
females, respectively, while that of developing endometrial cancer
throughout life is 40–60%. The risks of developing gastric,
ovarian, small intestine, renal pelvic, ureteral, brain and biliary
tract cancers are 13, 12, ≤5, 4, 4 and 2%, respectively (8,9).
Methods to identify Lynch syndrome-related
endometrial cancer are important for several reasons. First,
endometrial cancer is likely to be the primary cancer in female
individuals with Lynch syndrome and may therefore be managed by
prevention and screening. Endometrial cancer develops first in 51%
of females with Lynch syndrome, followed by colorectal cancer at an
average of 11 years after the onset of endometrial cancer. Thus,
endometrial cancer frequently occurs as a sentinel cancer, with its
identification likely to be useful for the prevention of the
secondary cancer (10). A secondary
reason requiring the identification of useful methods is that the
diagnosis of Lynch syndrome provides a basis for the examination of
gene mutations in family members. In the case of an identical
mutation, appropriate genetic counseling, screening and preventive
therapy are offered to family members.
Examination of the familial history of cancer is
particularly useful for identifying Lynch syndrome-related
endometrial cancer. The Amsterdam II criteria for Lynch syndrome
are based on familial history and age (11). These criteria were developed from
the original Amsterdam criteria, which included only familial
history for colorectal cancer (12). However, certain patients in small
families may not meet the diagnostic criteria, while others with
hMSH6 mutation do not meet the Amsterdam II criteria due to
having developed cancers at an older age (13,14).
Lynch syndrome in women is associated with a relatively early onset
of endometrial cancer (15,16) as well as the development of a
secondary cancer as a double cancer (17). These characteristics should lead to
suspicion of Lynch syndrome.
Microsatellite instability (MSI) reflects
abnormality in DNA MMR (18).
Microsatellites are short DNA repeat sequences that increase or
decrease in number when MMR is dysfunctional. A MSI test is
recommended before examining germline mutation in patients with
suspected Lynch syndrome. MSI is detected in Lynch syndrome caused
by germline mutation and in sporadic endometrial cancer caused by
epigenetic aberrant methylation in the promoter region of
hMLH1(19). However, MSI in
these two diseases is distinguished based on the detection of MMR
protein levels, using a combination of immunohistochemistry (IHC)
and detection of hypermethylation in the hMLH1 promoter
region (20,21). The Bethesda criteria determine the
situation in which a MSI test should be conducted for colorectal
cancer (22). Similar guidelines
have been developed for endometrial cancer (23), although not including items
regarding histopathological findings, in comparison with the
Bethesda criteria.
Tumors in LUS have been found to be frequently
associated with Lynch syndrome (24). The endometrium comprises the
regions: the uterine corpus (UC) and the LUS (25). Endometrial cancer usually develops
in the mucosa of the UC and the uterine fundus, but only
occasionally in the LUS. When a tumor is macroscopically observed
to develop in LUS and expand from the lower UC to the upper cervix,
the disease is defined as LUS cancer (26). Pathologically, LUS cancer is a
poorly differentiated (G3) adenosquamous carcinoma, although the
tumor size is small (26,27–29).
Westin et al first showed a relationship between LUS cancer
and Lynch syndrome in 35 patients with cancer in the uterine
isthmus (24). Decreases were found
in the MSH2 and MSH6 protein levels, using IHC in 10 patients
(29%), including 4 cases with strongly suspected hMSH2
mutations due to high MSI and 1 case with a decreased MLH1 protein
level with no aberrant methylation. These 5 patients (14.2%) met
the Amsterdam II criteria and were diagnosed with Lynch syndrome,
having hMSH2 mutations, MSI and a decreased MSH2 protein
level in IHC (24).
In the case that LUS cancer is found to occur
frequently in patients with Lynch syndrome in additional
large-scale studies, it might be added to the clinical
characteristics used to identify Lynch-related endometrial cancer.
Therefore, we conducted the first study on the relationship between
the clinicopathological characteristics of LUS cancer and Lynch
syndrome in Asian patients.
Materials and methods
Case selection
The subjects were patients diagnosed with
endometrial cancer, who underwent hysterectomy in our hospital
between January, 2002 and July, 2010. Based on pathology reports,
patients were divided into LUS and non-LUS groups. The criterion
for the diagnosis of LUS cancer was the macroscopic observation of
a tumor developing in the LUS and expanding from the lower uterine
corpus to the upper cervix. Patients with tumors in the LUS or in
any other region and those with cancer spreading from the fundus to
the endocervix, for whom the site of cancer onset was unclear were
excluded from the study.
Clinical data were collected from patient records.
Surgical staging was determined based on the criteria of the 1988
International Federation of Gynecology and Obstetrics (FIGO)
Classification or the Guidelines for Endometrial Cancer published
by the Japan Society of Obstetrics and Gynecology. Pathological
evaluation was performed with hematoxylin and eosin staining. Lynch
syndrome was diagnosed using the Amsterdam II criteria. This study
was conducted after the approval of the institutional review
board.
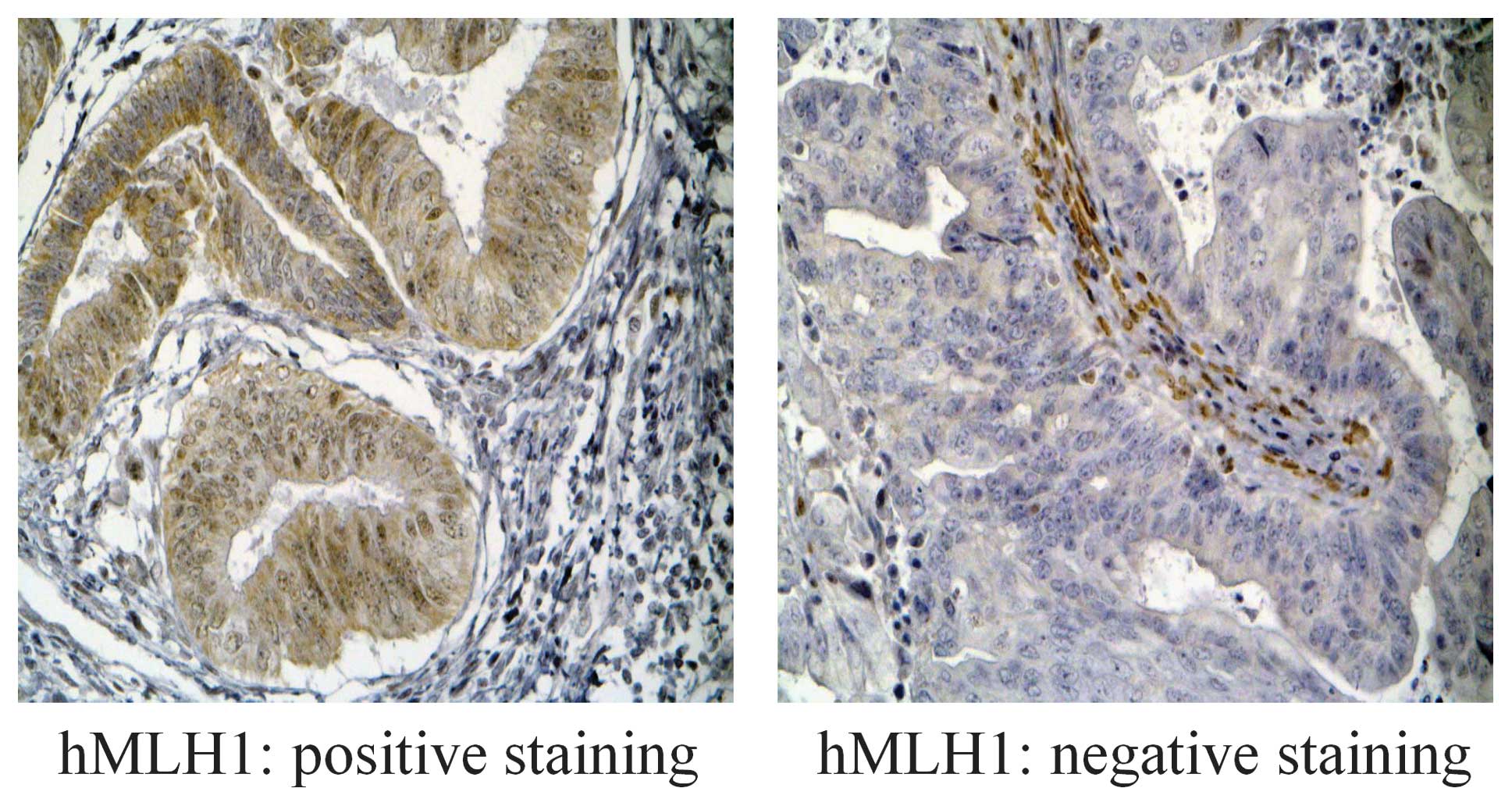
Immunohistochemistry
Immunohistochemical staining was performed on 2-μm
sections of formalin-fixed, paraffin-embedded tissues using
standard procedures. Slides were cleaned in xylene and dehydrated
in graded alcohol. Antigen retrieval was performed with a 10-min
microwave treatment in 10 mM citrate buffer, pH 7.0. Endogenous
peroxidase was blocked by dipping sections in 0.3%
H2O2 in methanol for 10 min. Slides were
incubated with mouse monoclonal antibody to hMLH1 (clone G168-15;
Pharmingen, San Diego, CA, USA) (1:30), mouse monoclonal antibody
to hMSH6 (clone 44; BD Transduction Laboratories, San Jose, CA,
USA) (1:500), or rabbit polyclonal antibody to hMSH2 (SC-494; Santa
Cruz Biotechnology, Santa Cruz, CA, USA) (1:200) for 90 min at room
temperature. Immunostaining was performed using the
avidin-biotin-peroxidase complex method with an Elite ABC kit
(Vector Laboratories, Burlingame, CA, USA), using
3,3′-diaminobenzidine as a chromogen and
H2O2. Slides were counterstained with
hematoxylin, dehydrated in graded alcohol, dried and coverslipped.
A normal nuclear staining pattern was detected for hMLH1, hMSH2 and
hMSH6, while nuclei in the stromal cells were used as internal
positive controls (Fig. 1).
MSI analysis
DNA was extracted from paraffin-embedded tumor
tissue and normal tissue using DEXPAT (Takara, Shiga, Japan) for
use in polymerase chain reaction (PCR) assays. DNA samples were
analyzed using five microsatellite primers, recommended by the
National Cancer Institute (NCI), which amplified D2S123, D5S376,
D17S250, BAT25 and BAT26. The PCR primers for these regions were
purchased from Research Genetics (Huntsville, AL, USA). The
antisense primers contained a fluorescent marker, Cy5 amidite
(indodicarbocyanine), at their 5′ ends. AmpliTaq polymerase and
AmpliTaq buffer (Perkin-Elmer, Boston, MA, USA) were used in the
PCR, in which 1 μl of sample DNA (template, 0.1 μg/μl) was added to
24 μl of premixture (distilled water, 16.125 μl; 1.25 mmol/l dNTP,
4 μl; 10× BPCR buffer, 2.5 μl; optical density (OD) 2.2 forward
primer, 0.625 μl; OD 2.2 reverse primer, 0.625 μl; and Taq
polymerase, 0.125 μl) in a total reaction volume of 25 μl. Forward
and reverse primers specific for the D2S123, D5S376, D17S250, BAT25
and BAT26 regions were used. DNA denaturation at 95°C for 5 min was
followed by 40 cycles for 30 sec at 95°C, 40 sec at 55°C and 40 sec
at 72°C. The reaction mixture was then heated to 72°C for 7 min,
cooled and stored at 4°C. The PCR products were combined with size
markers, denatured for 5 min at 80°C, and then electrophoresed in
6% Long Ranger 7 M urea denaturing gel on an AFL red DNA sequencer
(Amersham Pharmacia Biotech, Tokyo, Japan). DNA fragment sizes were
analyzed using gene scanning software (Allele Links; Amersham
Pharmacia Biotech). Tumors showing an allelic shift at ≥2 markers
were classified as MSI-H, while tumors with an allelic shift at 1
marker were classified as MSI-L, and those with no allelic shift at
any marker as microsatellite stable (MSS).
Methylation-specific PCR (MSP)
DNA (1 μg) extracted from paraffin-embedded tumor
tissue was diluted with 50 μl of distilled water and incubated in
5.5 μl of 3 N NaOH at 37°C for 15 min. To this solution, 30 μl of
10 mM hydroquinone (Sigma, St. Louis, MO, USA) and 520 μl of 3 M
sodium bisulfite (prepared at pH 5.5 with 10 N NaOH, Sigma) were
added with mixing. Mineral oil was laid over the solution to
prevent evaporation and the solution was incubated overnight at
50°C. The lower layer of the solution was then mixed with 1 ml of
Clean-up Resin (Promega, Madison, WI, USA) and injected into a
column. After rinsing with 2 ml of 80% isopropanol, the mixture was
centrifuged at 15,000 rpm for 3 min to completely remove
isopropanol. Then, 50 μl of hot (70°C) distilled water was added
and the mixture was centrifuged at 15,000 rpm for 2 min to elute
DNA. The DNA was then incubated with 5.5 μl of 2 N NaOH at 37°C for
20 min. Then, 66 μl of 5 N ammonium acetate and 243 μl of 95%
ethanol were added and the mixture was incubated at −80°C for 1 h
and centrifuged at 15,000 rpm for 30 min to precipitate DNA. The
supernatant (>50 μl) was removed and 1 ml of 60% ethanol was
added. The mixture was centrifuged at 15,000 rpm for 30 min and
rinsed. The precipitated DNA was dried in air and dissolved in 20
μl of distilled water. The DNA solution (2 μl) was used as the MSP
template. In the PCR assay, AmpliTaq Gold & 10× PCR
buffer/MgCl2 with dNTP (Applied Biosystems, Foster City,
CA, USA) were used and the results were analyzed with a GeneAmp PCR
System 9700 (Applied Biosystems). The primer sequences were 5′-ACG
TAG ACG TTT TAT TAG GGT CGC-3′ (sense) and 5′-CCT CAT CGT AAC TAC
CCG CG-3′ (antisense), 159 bp. Primer sequences for the
unmethylated reaction were 5′-TTT TGA TGT AGA TGT TTT ATT AGG GTT
GT-3′ (sense) and 5′-ACC ACC TCA TCA TAA CTA CCC ACA-3′
(antisense), 165 bp. PCR was performed for 35 cycles (94, 60 and
72°C, each for 30 sec).
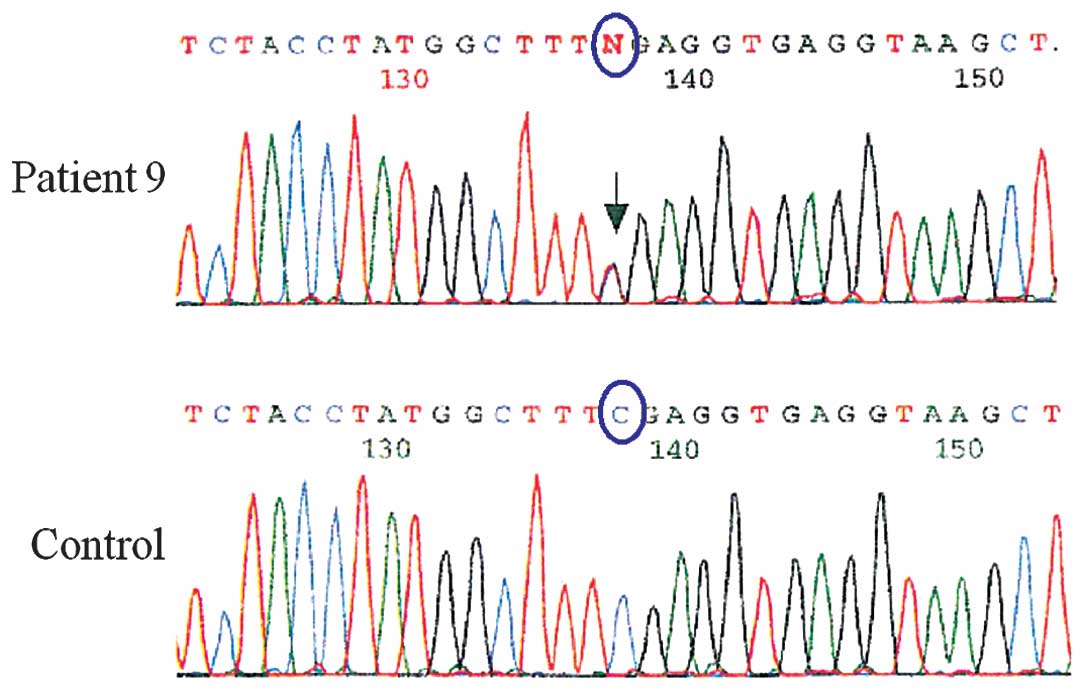
Mutation detection
A mutation in hMLH1 was detected in case 9,
which was MSI-H and negative for DNA hypermethylation in the
hMLH1 promoter. Peripheral leukocyte DNA was extracted and
the hMLH1 mutation was analyzed by direct sequencing with
primers, as previously described (13). DNA yielding altered bands was
automatically sequenced and the result compared with the normal DNA
sequence.
Statistical analysis
Statistical analysis was performed using the IBM
SPSS Statistics 19 software. Clinical and pathological variables
were compared in the two groups using χ2 and Student's
t-test. P<0.05 was considered to indicate a statistically
significant difference.
Results
Clinical background
The subjects were 625 patients diagnosed with
endometrial cancer, who underwent hysterectomy in our hospital
between January, 2002 and July, 2010. Pathological reports were
evaluated and 9 (1.4%) patients were diagnosed in the LUS group.
Table I shows the clinical
background of these 9 patients and of an additional 27, randomly
selected from the non-LUS group. The patients in the LUS group were
significantly younger (44.4 vs. 59.5 years old, P=0.001) and had a
significantly lower BMI (18.5 vs. 22.7 kg/m2, P=0.002).
Cesarean section had been performed in 2 patients (22.2%) in the
LUS group and in 1 patient (3.7%) in the non-LUS group, with no
statistically significant difference between these groups. There
were also no statistically significant differences in the frequency
of delivery or in the rates of infertility and diabetes between
these groups.
 | Table IClinical characteristics of LUS and
non-LUS tumors. |
Table I
Clinical characteristics of LUS and
non-LUS tumors.
| LUS tumor | Non-LUS tumor | P-value |
|---|
| Median age
(years) | 44.4
(34.2–54.6)a | 59.48
(55.8–63.1)a | 0.001 |
| Median BMI
(g/m2) | 18.5
(17.0–19.9)a | 22.7
(21.2–24.1)a | 0.002 |
| Median parity | 1.1
(0.3–1.9)a | 1.5
(1.1–1.9)a | 0.267 |
|
| No. of
patients | % | No. of
patients | % | P-value |
|
| Cesarean
section |
| No | 7 | 77.7 | 26 | 96.2 | 0.082 |
| Yes | 2 | 22.2 | 1 | 3.7 | |
| Infertility |
| No | 8 | 88.8 | 26 | 96.2 | 0.401 |
| Yes | 1 | 11.1 | 1 | 3.7 | |
| Diabetes |
| No | 8 | 88.8 | 23 | 85.1 | 0.781 |
| Yes | 1 | 11.1 | 4 | 14.8 | |
Pathological characteristics
A comparison of the pathological characteristics of
the LUS and non-LUS cases is shown in Table II. The histological type was
endometrioid in 8 (88.8%) and adenosquamous in 1 (11.1%) of the LUS
cases. There were no statistically significant differences in
histology, grade, stage, rates of vascular invasion and lymph node
metastasis or the depth of myometrial invasion between the 2
groups.
| Table IIPathologic characteristics of LUS and
non-LUS tumors. |
Table II
Pathologic characteristics of LUS and
non-LUS tumors.
| LUS tumor | Non-LUS tumor | |
|---|
|
|
| |
|---|
| No. (N=9) | % | No. (N=27) | % | P-value |
|---|
| Histology | | | | | 0.728 |
| Endometrioid | 8 | 88.8 | 25 | 92.5 | |
|
Non-endometrioid | 1 | 11.1 | 2 | 7.4 | |
| Histological
grade | | | | | 0.832 |
| 1 | 5 | 55.5 | 13 | 48.1 | |
| 2 | 3 | 33.3 | 7 | 25 | |
| 3 | 1 | 11.1 | 6 | 22.2 | |
| Vascular
invasion | | | | | 0.841 |
| Positive | 6 | 66.6 | 17 | 62.9 | |
| Negative | 3 | 33.3 | 10 | 37 | |
| Myometrial
invasion | | | | | 0.401 |
| negative | 1 | 11.1 | 1 | 3.7 | |
| <1/3 | 3 | 33.3 | 12 | 44.4 | |
| 1/3-1/2 | 3 | 33.3 | 4 | 14.8 | |
| >1/2 | 2 | 22.2 | 10 | 37 | |
| Lymph node
metastasis | | | | | 0.579 |
| Negative | 7 | 77.7 | 19 | 73 | |
| Positive | 2 | 22.2 | 7 | 26.9 | |
| Stage | | | | | 0.665 |
| I/II | 6 | 66.6 | 18 | 66.6 | |
| III/IV | 3 | 33.3 | 9 | 33.3 | |
Microsatellite status and IHC
characteristics
A comparison of the microsatellite status and IHC
findings for the LUS and non-LUS groups are shown in Table III. The microsatellite status was
MSI-H in 2 LUS cases (22.2%) and MSI-L in 1 (11.1%), and MSI-H in 7
non-LUS cases (25.9%). Loss of expression of hMLH1 was detected in
4 LUS cases (44.4%) and 4 non-LUS cases (14.8%). Loss of expression
of hMSH2 was not detected in LUS patients, although was found in 4
non-LUS cases (14.8%). Loss of expression of hMLH6 was detected in
1 LUS case (11.1%) and 11 non-LUS cases (40.7%). No statistically
significant differences were found in the microsatellite status and
IHC findings between the 2 groups.
| Table IIIMicrosatellite status and
immunohistochemical (IHC) characteristics of LUS and non-LUS
tumors. |
Table III
Microsatellite status and
immunohistochemical (IHC) characteristics of LUS and non-LUS
tumors.
| LUS tumor | Non-LUS tumor | |
|---|
|
|
| |
|---|
| No. | % | No. | % | P-value |
|---|
| MSI | | | | | 0.39 |
| MSI-H | 2 | 22.2 | 7 | 25.9 | |
| MSI-L | 1 | 11.1 | 0 | 0 | |
| MSS | 6 | 66.6 | 20 | 74 | |
| IHC |
| Loss of hMLH1
expression | 4 | 44.4 | 4 | 14.8 | 0.66 |
| Loss of hMSH2
expression | 0 | 0 | 4 | 14.8 | 0.66 |
| Loss of hMSH6
expression | 1 | 11.1 | 11 | 40.7 | 0.41 |
Lynch syndrome and LUS cancer
The microsatellite status, IHC findings for MMR
genes, status of DNA hypermethylation of the hMLH1 promoter
and the Amsterdam II criteria for the 9 LUS patients are shown in
Table IV. These 9 patients had
hMSH2 expression in IHC. Cases 2 and 8 had a decreased hMLH1
protein level and were MSI-H and MSI-L, respectively.
Hypermethylation of the hMLH1 promoter was detected in the
two patients. Case 9 had decreased hMLH1 in IHC, while the DNA
methylation of the hMLH1 promoter was not detected, despite
the MSI-H status. Since the patient had a family history of cancer
and met the Amsterdam II criteria, she was diagnosed with Lynch
syndrome. Germ cell mutation of hMLH1 was examined using
peripheral blood lymphocytes and mutation from CGA to TGA was
detected in codon 100 in exon 3 (Fig.
2).
| Table IVIHC and MSI and methylation status of
LUS patients. |
Table IV
IHC and MSI and methylation status of
LUS patients.
| IHC | | | | |
|---|
|
| | | | |
|---|
| Pt | hMLH1 | hMSH2 | hMSH6 | MSI | hMLH1
hypermethylation | Age | Amsterdam II
criteria |
|---|
| 1 | − | + | + | MSS | − | 62 | Negative |
| 2 | − | + | − | MSI-H | + | 35 | Negative |
| 3 | + | + | + | MSS | − | 46 | Negative |
| 4 | + | + | + | MSS | − | 39 | Negative |
| 5 | + | + | + | MSS | − | 26 | Negative |
| 6 | + | + | + | MSS | − | 69 | Negative |
| 7 | + | + | + | MSS | − | 41 | Negative |
| 8 | − | + | + | MSI-L | + | 40 | Negative |
| 9 | − | + | + | MSI-H | − | 42 | Positive |
Discussion
In the present study, the incidence of LUS was 9
(1.4%) of the 625 patients with endometrial cancer, who underwent
hysterectomy. This incidence is lower than the 3–6.3% rates of LUS
cancer among the cases of endometrial cancer in previous studies
(24,26,27).
The patients with LUS cancer in this study were significantly
younger than those with non-LUS endometrial cancer. At present, the
largest study conducted comprised 35 patients with LUS cancer and
79 with non-LUS endometrial cancer. The mean onset ages were 54.2
and 62.9 years, respectively, indicating younger patients in the
LUS group (24). In a study of
patients with endometrial cancer aged ≤50 years, LUS cancer was
present in 18% (16/88) (28).
However, other small-scale studies have not shown similar results
(26).
Endometrial cancer is classified into types I and
II, with type I being estrogen-dependent. Obesity increases insulin
resistance as well as the risk of endometrial cancer, due to an
elevated blood estradiol level. Thus, BMI ≥25 doubles, while ≥30
triples the risk of endometrial cancer (30). Nulliparity, amenorrhea and
infertility cause long-term stimulation by estrogen and are
considered to be risks for endometrial cancer. In this study, BMI
in the LUS group was significantly lower than that in the non-LUS
group. The lower rate of obesity suggests that LUS cancer does not
have the typical properties of type I endometrial cancer. Hachisuga
et al found that the incidence of menstrual irregularity,
nulliparity, infertility and polycystic ovary syndrome was
significantly lower in the 16 patients with LUS cancer, compared
with 72 patients with non-LUS endometrial cancer, suggesting that
LUS cancer is not a typical type I endometrial cancer (28). In the present study, no difference
was evident in the incidence of diabetes and infertility between
the LUS and non-LUS groups.
Previous pathological findings demonstrated that a
histological adenosquamous carcinoma, a higher grade (26–28)
and muscle invasion (24,27,28,31)
are common in LUS cancer. However, there was no significant
difference in the pathological findings between LUS and non-LUS
endometrial cancer in our patients.
The MSI-positive frequency in this study was 22.2%
in the LUS and 25.9% in the non-LUS groups, with no statistically
significant difference between the groups. Similar MSI-positive
frequencies of 29% (127/441) and 21.7% (118/543) have been reported
in previous studies that mainly included cases with
hypermethylation of the hMLH1 promoter (20,21).
In this study, hMLH2 expression in IHC was detected
in all the patients with LUS cancer. These findings differ
considerably from those of Westin et al who demonstrated a
decreased hMSH2 and hMSH6 expression in 25.7% (9/35) of the cases
(24). We found a decreased hMLH1
expression in 44.4% (4/9) of our cases of LUS cancer, with
epigenetic suppression due to DNA hypermethylation of the
hMLH1 promoter detected in 2 cases (22.2%). This finding
suggests that DNA hypermethylation of hMLH1 also induces LUS
cancer. A decreased hMSH6 expression was present in 11.1% (1/9) of
the cases, while case 2 also had MSI-H. The MSI-positive rate
associated with a reduced hMSH6 expression is usually lower
than that for hMLH1 and hMSH2, while hMSH6
knockout mice have been shown to have a negative MSI (32). However, the effect of a reduced
hMSH6 expression on MSI is unclear since case 2 also showed
hypermethylation of hMLH1.
The incidence of Lynch syndrome in the LUS group was
11.1% (1/9) in this study, which is higher than the previously
reported incidences of 1–2% for Lynch syndrome in patients with
various types of endometrial cancer (20,21,33).
Thus, the current small-scale study is the first to show a
relationship between LUS cancer and Lynch syndrome in Asian
patients. In their study, Westin et al found that the
hMSH2 mutation was causative in all the LUS cancer patients
with Lynch syndrome (24); however,
the hMLH1 mutation was found to be causative in our study.
This finding is the first evidence that LUS cancer is likely to
develop due to the germline mutation of hMLH1, thereby
enhancing the possibility of the causative mutation being different
in various ethnicities.
The prognosis of LUS cancer has been examined in two
small-scale studies (26,28). Patients with Lynch syndrome and
concomitant colorectal cancer usually have a good prognosis
(34,35). The prognosis of endometrial cancer
in patients with Lynch syndrome has not been established, the
findings for colorectal cancer, however, suggest that the prognosis
of LUS cancer may be good for patients with Lynch syndrome.
Notably, a comparative study on germline MMR mutation- or
hMLH1 hypermethylation-induced endometrial cancer showed an
older onset age with fewer grade 1 and more grade 3 cases in the
hypermethylation group (36).
Therefore, the possible association of hMLH1
hypermethylation with LUS cancer demonstrated in this study
suggests a worse prognosis for LUS cancer associated with Lynch
syndrome. LUS cancer is rare and relatively few cases have been
described, thus, additional large-scale studies are required to
establish the characteristics of this disease.
Acknowledgements
The authors gratefully acknowledge grant support
from the Japan Society for the Promotion of Science (JSPS) through
a Grant-in-Aid for Scientific Research (KAKENHI); a Grant-in-Aid
for Scientific Research (B) (22390313), a Grant-in-Aid for
Scientific Research (C) (22591866) and a Grant-in-Aid for Young
Scientists (B) (21791573); the Ichiro Kanehara Foundation; and the
Keio University Medical Science Fund through a Research Grant for
Life Sciences and Medicine.
References
|
1
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics. CA Cancer J Clin. 62:10–29. 2012.
|
|
2
|
Forouzanfar MH, Foreman KJ, Delossantos
AM, et al: Breast and cervical cancer in 187 countries between 1980
and 2010: a systematic analysis. Lancet. 378:1461–1484. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Saso S, Chatterjee J, Georgiou E, Ditri
AM, Smith JR and Ghaem-Maghami S: Endometrial cancer. BMJ.
343:3954. 2011. View Article : Google Scholar
|
|
4
|
Brinton LA, Berman ML, Mortel R, et al:
Reproductive, menstrual, and medical risk factors for endometrial
cancer: results from a case-control study. Am J Obstet Gynecol.
167:1317–1325. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gruber SB and Thompson WD: A
population-based study of endometrial cancer and familial risk in
younger women. Cancer and Steroid Hormone Study Group. Cancer
Epidemiol Biomarkers Prev. 5:411–417. 1996.PubMed/NCBI
|
|
6
|
Lynch HT and de la Chapelle A: Hereditary
colorectal cancer. N Engl J Med. 348:919–932. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Peltomäki P: Role of DNA mismatch repair
defects in the pathogenesis of human cancer. J Clin Oncol.
21:1174–1179. 2003.PubMed/NCBI
|
|
8
|
Dunlop MG, Farrington SM, Carothers AD, et
al: Cancer risk associated with germline DNA mismatch repair gene
mutations. Hum Mol Genet. 6:105–110. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Aarnio M, Sankila R, Pukkala E, et al:
Cancer risk in mutation carriers of DNA-mismatch-repair genes. Int
J Cancer. 81:214–218. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lu KH, Dinh M, Kohlmann W, et al:
Gynecologic cancer as a ‘sentinel cancer’ for women with hereditary
nonpolyposis colorectal cancer syndrome. Obstet Gynecol.
105:569–574. 2005.
|
|
11
|
Vasen HF, Watson P, Mecklin JP and Lynch
HT: New clinical criteria for hereditary nonpolyposis colorectal
cancer (HNPCC, Lynch syndrome) proposed by the International
Collaborative Group on HNPCC. Gastroenterology. 116:1453–1456.
1999. View Article : Google Scholar
|
|
12
|
Vasen HF, Mecklin JP, Khan PM and Lynch
HT: The International Collaborative Group on Hereditary
Non-Polyposis Colorectal Cancer (ICG-HNPCC). Dis Colon Rectum.
34:424–425. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Banno K, Susumu N, Hirao T, et al:
Identification of germline MSH2 gene mutations in endometrial
cancer not fulfilling the new clinical criteria for hereditary
nonpolyposis colorectal cancer. Cancer Genet Cytogenet. 146:58–65.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hendriks YMC, Wagner A, Morreau H, et al:
Cancer risk in hereditary nonpolyposis colorectal cancer due to
MSH6 mutations: impact on counseling and surveillance.
Gastroenterology. 127:17–25. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Berends MJW, Wu Y, Sijmons RH, et al:
Toward new strategies to select young endometrial cancer patients
for mismatch repair gene mutation analysis. J Clin Oncol.
21:4364–4370. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lu KH, Schorge JO, Rodabaugh KJ, et al:
Prospective determination of prevalence of lynch syndrome in young
women with endometrial cancer. J Clin Oncol. 25:5158–5164. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Millar AL, Pal T, Madlensky L, et al:
Mismatch repair gene defects contribute to the genetic basis of
double primary cancers of the colorectum and endometrium. Hum Mol
Genet. 8:823–829. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Boland CR, Thibodeau SN, Hamilton SR, et
al: A National Cancer Institute Workshop on Microsatellite
Instability for cancer detection and familial predisposition:
development of international criteria for the determination of
microsatellite instability in colorectal cancer. Cancer Res.
58:5248–5257. 1998.
|
|
19
|
Simpkins SB, Bocker T, Swisher EM, et al:
MLH1 promoter methylation and gene silencing is the primary cause
of microsatellite instability in sporadic endometrial cancers. Hum
Mol Genet. 8:661–666. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Goodfellow PJ, Buttin BM, Herzog TJ, et
al: Prevalence of defective DNA mismatch repair and MSH6 mutation
in an unselected series of endometrial cancers. Proc Natl Acad Sci
USA. 100:5908–5913. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hampel H, Frankel W, Panescu J, et al:
Screening for Lynch syndrome (hereditary nonpolyposis colorectal
cancer) among endometrial cancer patients. Cancer Res.
66:7810–7817. 2006. View Article : Google Scholar
|
|
22
|
Umar A, Boland CR, Terdiman JP, et al:
Revised Bethesda Guidelines for hereditary nonpolyposis colorectal
cancer (Lynch syndrome) and microsatellite instability. J Natl
Cancer Inst. 96:261–268. 2004. View Article : Google Scholar
|
|
23
|
Lancaster JM, Powell CB, Kauff ND, et al:
Society of Gynecologic Oncologists Education Committee statement on
risk assessment for inherited gynecologic cancer predispositions.
Gynecol Oncol. 107:159–162. 2007. View Article : Google Scholar
|
|
24
|
Westin SN, Lacour RA, Urbauer DL, et al:
Carcinoma of the lower uterine segment: a newly described
association with Lynch syndrome. J Clin Oncol. 26:5965–5971. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Normal histology of the uterus and
fallopian tubes. Histology for Pathologists. Sternberg S: 2nd
edition. Lippincott-Raven Publishers; Philadelphia: pp. 879–927.
1997
|
|
26
|
Jacques SM, Qureshi F, Ramirez NC, Malviya
VK and Lawrence WD: Tumors of the uterine isthmus:
clinicopathologic features and immunohistochemical characterization
of p53 expression and hormone receptors. Int J Gynecol Pathol.
16:38–44. 1997. View Article : Google Scholar
|
|
27
|
Hachisuga T, Kaku T and Enjoji M:
Carcinoma of the lower uterine segment. Clinicopathologic analysis
of 12 cases. Int J Gynecol Pathol. 8:26–35. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Hachisuga T, Fukuda K, Iwasaka T, Hirakawa
T, Kawarabayashi T and Tsuneyoshi M: Endometrioid adenocarcinomas
of the uterine corpus in women younger than 50 years of age can be
divided into two distinct clinical and pathologic entities based on
anatomic location. Cancer. 92:2578–2584. 2001.
|
|
29
|
Masuda K, Banno K, Yanokura M, et al:
Carcinoma of the lower uterine segment (LUS): clinicopathological
characteristics and association with Lynch syndrome. Curr Genomics.
12:25–29. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Calle EE, Rodriguez C, Walker-Thurmond K
and Thun MJ: Overweight, obesity, and mortality from cancer in a
prospectively studied cohort of U.S. adults. N Engl J Med.
348:1625–1638. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Watanabe Y, Nakajima H, Nozaki K, et al:
Clinicopathologic and immunohistochemical features and
microsatellite status of endometrial cancer of the uterine isthmus.
Int J Gynecol Pathol. 20:368–373. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Edelmann L and Edelmann W: Loss of DNA
mismatch repair function and cancer predisposition in the mouse:
animal models for human hereditary nonpolyposis colorectal cancer.
Am J Med Genet C Semin Med Genet. 129:91–99. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ollikainen M, Abdel-Rahman WM, Moisio A-L,
et al: Molecular analysis of familial endometrial carcinoma: a
manifestation of hereditary nonpolyposis colorectal cancer or a
separate syndrome? J Clin Oncol. 23:4609–4616. 2005. View Article : Google Scholar
|
|
34
|
Watson P, Lin KM, Rodriguez-Bigas MA, et
al: Colorectal carcinoma survival among hereditary nonpolyposis
colorectal carcinoma family members. Cancer. 83:259–266. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Lanspa SJ, Lynch HT, Smyrk TC, et al:
Colorectal adenomas in the Lynch syndromes. Results of a
colonoscopy screening program. Gastroenterology. 98:1117–1122.
1990.PubMed/NCBI
|
|
36
|
Broaddus RR, Lynch HT, Chen L-M, et al:
Pathologic features of endometrial carcinoma associated with HNPCC:
a comparison with sporadic endometrial carcinoma. Cancer.
106:87–94. 2006. View Article : Google Scholar : PubMed/NCBI
|