Introduction
Malignant pleural effusion (MPE) is a common
complication of advanced metastatic non-small cell lung cancer
(NSCLC). Abnormal fluid accumulation in the pleural space could
lead to dyspnoea, cough and chest pain, which may eventually impair
the normal function of the heart, and thus threaten patient
survival (1). Since MPE presents
with a high incidence and poor prognosis, characterized by a medium
survival rate of 3 months, one of the highest priorities is to
actively manage the pleural effusion in an attempt to improve the
quality of life of the patients (1,2). The
current mode of therapy for patients with MPE primarily depends on
local treatment, such as tube drainage, chemical pleurodesis and
intrapleural administration of antineoplastic agents such as
doxorubicin, cisplatin, cytarabine, carboplatin, etoposide,
mitomycin C and 5-fluorouracil (3–6). Of
these chemotherapeutic agents, cisplatin is the most commonly used
for the treatment of NSCLC. It is thus the most frequently used
drug for intrapleural therapy of pleural effusions caused by NSCLC
(7). Although the current mode of
therapy can occasionally alleviate the symptoms, the relapse rate
is as high as 50%. In addition, for most patients, no single
treatment approach can achieve a satisfactory effect. Consequently,
there is an urgent need for highly effective combinatorial
therapies.
Vascular endothelial growth factor (VEGF) is an
endothelial cell-specific growth factor that stimulates
vasculogenesis and angiogenesis, and has been shown to be an
essential intermediate in the formation of pleural effusions
(8–10). Synthesis of VEGF by both autocrine
and paracrine pathways (11) has
shown it to be present in multiple solid cancers including NSCLC.
Overexpression of VEGF in NSCLC can enhance its interaction with
VEGF-specific receptors. Occupation of these receptors by VEGF
could further stimulate the production of VEGF by both cancer and
stroma cells, leading to local increases in the levels of VEGF in
MPE.
It is well documented that bevacizumab, a humanized
monoclonal antibody raised against VEGF, is able to directly
inhibit proliferation, migration and differentiation of vascular
endothelial cells. Bevacizumab can also promote apoptosis of
endothelial cells and suppress VEGF-induced neoangiogenesis and
vascular permeability (12). Of
note, bevacizumab has been shown to synergize with chemotherapeutic
agents to block the accumulation of pleural fluid (13–17),
thus making it a promising candidate for the clinical management of
MPE. However, intravenous administration of bevacizumab requires a
much higher dose to achieve a corresponding effect, whose
side-effect might offset the ability of bevacizumab to diminish
effusion (18). Furthermore,
although intrapleural administration is a standard approach for
managing pleural effusion, intrapleural administration of
bevacizumab has not yet been reported for the treatment of MPE as a
consequence of NSCLC. In the present study, we evaluated the
efficacy and safety of local intrapleural administration of a
combination of bevacizumab with cisplatin for the treatment of MPE.
The main purpose of this study was to seek a more efficient
therapeutic approach for the clinical management of these
cancer-associated diseases.
Materials and methods
Research study subjects
This study was approved by the institutional review
board of the First Affiliated Hospital of Chinese PLA Postgraduate
Medical School (Beijing, China) and written informed consent was
obtained from all participants (Approval no. ML25391). Seventy-two
NSCLC subjects (excluding squamous cell carcinoma) with a presence
of excess levels of pleural fluid were enrolled in this study from
August 2009 to December 2011 inclusive. The research study subjects
included 44 males and 28 females with a mean age of 52.50 years
(range, 66–82 years). Primary tumors included adenocarcinoma in 48
cases, alveolar cell carcinoma in 17 cases and large cell carcinoma
in seven cases. The study subjects were randomized into the
bevacizumab group (intrapleural therapy of bevacizumab combined
with cisplatin; n=36), and the cisplatin group (intrapleural
cisplatin therapy alone; n=36). Two study subjects in the cisplatin
group withdrew, including one study subject who was lost to
follow-up after two cycles of chemotherapy, and one study subject
who presented with dual cancer during treatment.
There was no statistically significant difference
(p>0.05) between the two groups in terms of gender, age,
clinical stage and pathological subtype (Table I). The MPE in the study subjects had
been confirmed by imaging such as X-ray, CT scan and type-B
ultrasonic scan in addition to cytological examination. The
enrolled study subjects showed various symptoms including chest
distress, cough and dyspnoea, at different levels.
 | Table IComparison of the clinical
characteristics of the evaluable NSCLC study subjects of the two
treatment groups. |
Table I
Comparison of the clinical
characteristics of the evaluable NSCLC study subjects of the two
treatment groups.
| Bevacizumab (%)
n=36 | Cisplatin (%)
n=34 | P-value |
|---|
| Age |
| ≥50 | 20 (55.56) | 18 (52.9) | >0.05 |
| 18–50 | 16 (44.44) | 16 (46.7) | >0.05 |
| Gender |
| Male | 19 (52.8) | 19 (55.6) | >0.05 |
| Female | 17 (47.2) | 15 (444.1) | >0.05 |
| Clinical stage |
| IV-M1aa | 25 (69.4) | 24 (70.6) | >0.05 |
| IV-M1b | 11 (30.6) | 10 (29.4) | >0.05 |
| Smoker |
| Ever smoker | 22 (61.1) | 21 (61.8) | >0.05 |
| Never smoker | 14 (38.2) | 13 (38.2) | >0.05 |
| EGFR mutation |
| Wild-type | 21 (58.3) | 18 (52.9) | >0.05 |
| Mutand | 15 (41.7) | 16 (47.1) | >0.05 |
| Subtype |
|
Adenocarcinoma | 23 (63.9) | 22 (64.7) | >0.05 |
| Alveolar cell
carcinoma | 9 (25.0) | 9 (26.5) | >0.05 |
| Large cell
carcinoma | 4 (11.1) | 3 (8.8) | >0.05 |
| Kamofsky score |
| ≥80 | 27 (75.0) | 25 (73.5) | >0.05 |
| >60 -
<80a | 9 (25.0) | 9 (26.5) | >0.05 |
| Systematic
treatment history (other regimen) |
| Yes | 25 (69.4) | 23 (67.6) | >0.05 |
| No | 11 (30.6) | 11 (32.4) | >0.05 |
| Local infusion
history |
| Bleomycin
monotherapy | 25 (69.4) | 23 (67.6) | >0.05 |
| No | 11 (30.6) | 11 (32.4) | >0.05 |
The inclusion criteria included the following: a)
advanced NSCLC confirmed histologically or pathologically, but not
including squamous cancer; b) chest X-ray, ultrasonography or CT
scan showing large areas of unilateral or bilateral plural
effusion; c) malignant tumor cells found in the pleural fluid; d)
no intrapleural injection of antineoplastic drugs or hardener
within one month of recruitment to the study; e) Kamofsky score
(KPS) >60, age >18 years at time of recruitment, and a
predicted survival time >3 months; f) no major organ system
dysfunction, and a blood cell count, as well as heart, liver and
kidney test results within a normal range; g) previous chemotherapy
to have been discontinued for >6 weeks prior to admission to
this study.
The exclusion criteria included: a) history of
allergy to biological agents; b) under current treatment with other
antineoplastic agents; c) no detectable lesions; d) uncontrolled
metastasis to the central nervous system; e) major organ
dysfunction, such as congestive heart failure, malignant
arrhythmia, angina requiring long-term medication, heart valve
diseases, myocardial infarction and refractory hypertension; f)
pregnant or breastfeeding women; g) infected wound; and h) history
of refractory psychiatric diseases.
The criteria for withdrawal included: a) patients
requesting withdrawal; b) stage III/IV adverse reactions related to
bevacizumab therapy; c) poor study subject compliance; and d)
disease progression. In addition, bevacizumab was discontinued if
any of the following conditions occurred: a) wound dehiscence that
needed intervention and associated complications; b) severe
bleeding; c) severe arterial thrombus; d) hypertension crisis or
hypertensive encephalopathy; e) reversible posterior
leukoencephalopathy syndrome; and f) nephrotic syndrome.
Treatment protocol
After draining the pleural fluid by thoracentesis,
study subjects were given intrapleural administration of either a
combination of 30 mg of cisplatin plus 300 mg of bevacizumab or 30
mg of cisplatin monotherapy. After 2 h of bed rest, study subjects
were asked to turn over every 15 min, in order to encourage full
access of the delivered drugs to the chest wall. This treatment was
given every two weeks. The tumor markers were examined at the end
of the first treatment cycle. Detailed records of the responses
following treatment were made by weekly blood monitoring and type-B
ultrasonic tests. The end point of this study was the completion of
3 cycles of treatment. One week after the first intrapleural
therapy, the enrolled NSCLC study subjects were given more than 3
cycles of conventional chemotherapy comprising paclitaxel (175
mg/m2) and carboplatin (AUC=6).
Evaluation of the standard of efficacy
and safety
Recent objective responses were determined according
to a previous study (19). Complete
remission (CR) was considered when the accumulated fluid had
disappeared and was stable for at least four weeks; partial
remission (PR) was considered when >50% of the accumulated fluid
had disappeared, symptoms had improved, and the remaining fluid had
failed to increase for at least four weeks; remission not obvious
(NC) was considered when <50% of the accumulated fluid had
disappeared; progression (PD) was considered when the accumulated
fluid had increased. The total efficiency was calculated by taking
the sum of CR+PR. At the same time, the median progression-free
survival (PFS) and the median overall survival (OS) were assessed.
Adverse reactions were evaluated by the Common Toxicity Evaluation
Criteria (CTC) according to the National Cancer Institute (NCI).
Qualify of Life (QOL) was evaluated by the Kanofsky score
(KPS).
Quantitation of VEGF by enzyme-linked
immunosorbent assay (ELISA)
Pleural fluid was centrifuged at 4,000 rpm for 10
min at 4°C, following which the supernatant was collected and
assessed by ELISA using the VEGF-A ELISA kit (USCN), according to
the manufacturer’s instructions. The assay plates were read using a
Microplate Reader (Bio-Rad, model 550). Carcinoembryonic antigen
(CEA) was determined by a chemiluminescence method.
Quantitative RT-PCR for VEGF-A
Cells (~105–106) were
subjected to total RNA extraction using TRIzol reagent (Invitrogen
Corp., Carlsbad, CA, USA). For RT-PCR, first-strand cDNA was
synthesized from 0.2 to 1.0 μg of total RNA with an oligo-dT primer
(Gibco), according to the manufacturer’s instructions. The
sequences of the VEGF-A primers were: forward
5′-ctacctccaccatgccaagt-3′, reverse 5′-aaatgctttc
tccgctctga-3′.
Statistical analysis
Results are expressed as the means ± standard error
of the mean. Data were analyzed by the χ2 test and the
rank sum test using SPSS 11.0 software. p<0.05 was considered to
indicate a statistically significant difference.
Results
Short-term effect
The 70 evaluable enrolled study subjects had
completed at least one cycle of treatment. The response rate for
the combination therapy group was 83.33% (30/36 study subjects),
while that for the cisplatin alone therapy group was 50.00% (17/34
study subjects). There was a statistically significant difference
between the two groups in terms of stratification of MPE
(p<0.05) (Table II). Following
2–3 cycles of treatment, the response rate was significantly
increased in the bevacizumab group (Table III). However, the response rate
only increased after 4 or more cycles of treatment in the cisplatin
monotherapy group (Table III).
Statistical analysis was not performed here due to the relatively
small case numbers.
| Table IIComparison of the efficacy between
the bevacizumab and cisplatin groups. |
Table II
Comparison of the efficacy between
the bevacizumab and cisplatin groups.
| Group | n | CR | PR | NC/PD | OR (%) |
|---|
| Cisplatin | 34 | 2 | 15 | 17 | 50.00 |
| Bevacizumab | 36 | 17 | 13 | 6 | 83.33 |
| Table IIITreatment cycles of intrapleural
infusion in the bevacizumab and cisplatin groups. |
Table III
Treatment cycles of intrapleural
infusion in the bevacizumab and cisplatin groups.
| Group | Treatment
cycle | Response (n) | CR | PR | Percentage (%) |
|---|
| Bevacizumab
(n=36) | 2 | 13 | 5 | 8 | 36.11 |
| 3 | 15 | 11 | 4 | 41.67 |
| ≥4 | 2 | 1 | 1 | 5.56 |
| Cisplatin
(n=34) | 2 | 2 | 0 | 2 | 5.88 |
| 3 | 4 | 0 | 4 | 11.77 |
| ≥4 | 11 | 2 | 9 | 32.35 |
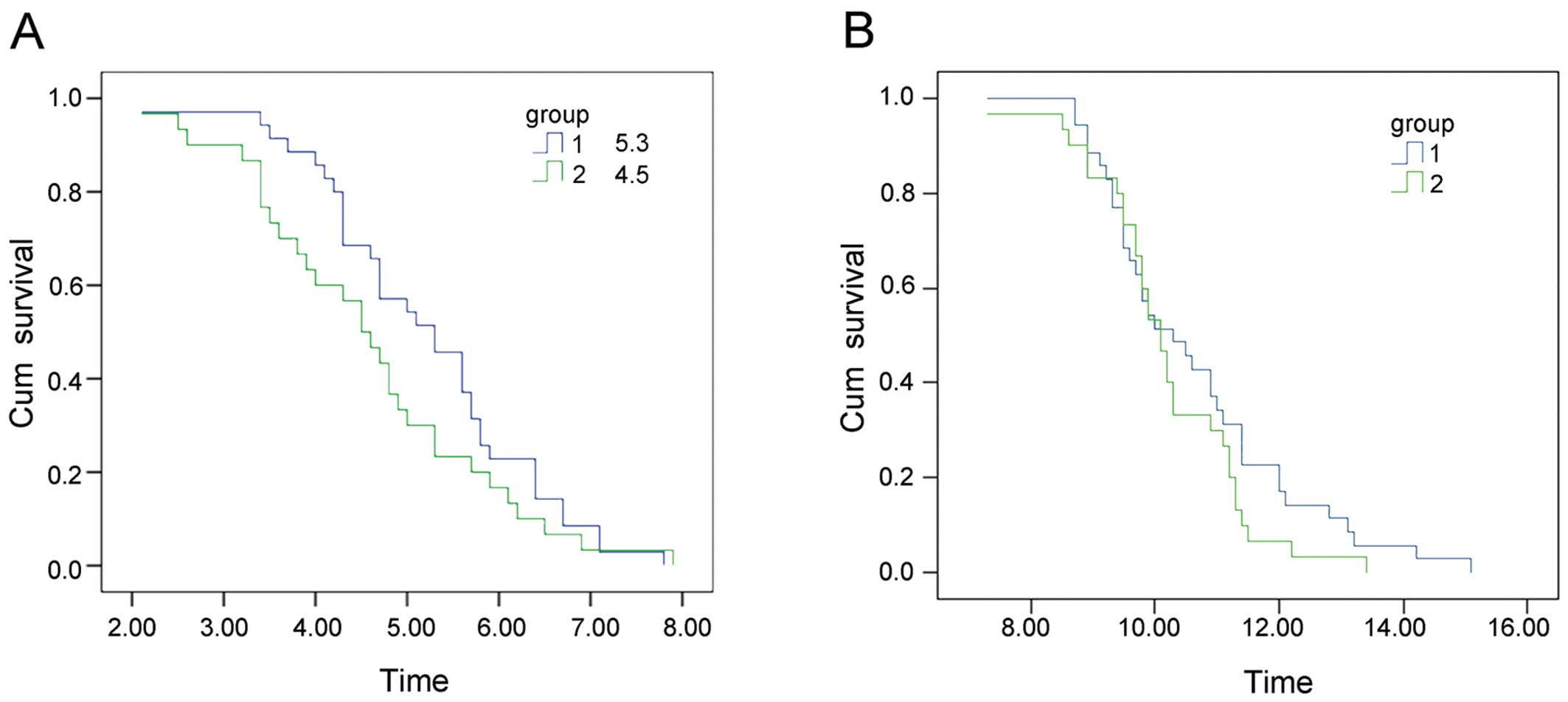
Long-term effect
The median PFS was found to be 5.3 months for the
bevacizumab combination group and 4.5 months for the cisplatin
alone group. This observation indicated that the addition of
bevacizumab to the therapeutic regime could significantly extend
the PFS of the study subjects presenting with MPE (p<0.05)
(Fig. 1A). The median survival time
was found to be 10.3 and 10.1 months, respectively, in the two
groups (p>0.05) (Fig. 1B).
Quality of life (QOL)
Of the 36 study subjects in the combination therapy
group, 30 study subjects were found to have an improved QOL
(83.33%), one study subject showed a stable QOL, and one study
subject showed a reduced QOL. In the cisplatin monotherapy group,
only 50.00% (15 cases) of the study subjects showed an improvement
in their QOL.
Toxicity
There was no evidence of significantly increased
toxicity following systemic chemotherapy in combination with
intrapleural therapy. The major side-effects of bevacizumab
treatment included bleeding and high blood pressure. Although the
study subjects in both groups presented symptoms such as
neutropenia, nausea, vomiting and diarrhea, all of the symptoms
were typical side-effects of chemotherapy rather than being
exclusively associated with bevacizumab treatment. Although one of
the study subjects showed nasal mucous membrane bleeding, this
observation did not affect follow-up treatment. The incidence of
hypertension was also significantly higher in the combination
therapy group (p<0.05). However, observation of hypertension in
this group fell into stage I and II (although one case required
oral antihypertensive therapy) and no subject withdrew from the
study due to toxicity. No significant difference in grade III–IV
adverse side-effects was seen between the two groups (Table IV).
| Table IVComparison of toxicity between the
bevacizumab and cisplatin groups. |
Table IV
Comparison of toxicity between the
bevacizumab and cisplatin groups.
| | Grade |
|---|
| |
|
|---|
| Group | Toxicity | 0 | 1 | 2 | 3 | 4 |
|---|
| Bevacizumab
(n=36) | Leucocytopenia | 12 | 9 | 10 | 4 | 1 |
| Nausea and
vomiting | 19 | 12 | 5 | 0 | 0 |
| Diarrhea | 30 | 4 | 2 | 0 | 0 |
| Rhinorrhagia | 34 | 2 | 0 | 0 | 0 |
| Hemoptysis or
gastrointestinal bleeding | 36 | 0 | 0 | 0 | 0 |
| Hypertension | 27 | 7 | 2 | 0 | 0 |
| Proteinuria | 34 | 2 | 0 | 0 | 0 |
| Cisplatin
(n=34) | Leucocytopenia | 12 | 8 | 9 | 4 | 1 |
| Nausea and
vomiting | 17 | 12 | 4 | 1 | 0 |
| Diarrhea | 28 | 3 | 2 | 1 | 0 |
| Rhinorrhagia | 34 | 0 | 0 | 0 | 0 |
| Hemoptysis or
gastrointestinal bleeding | 34 | 0 | 0 | 0 | 0 |
| Hypertension | 32 | 2 | 0 | 0 | 0 |
| Proteinuria | 34 | 0 | 0 | 0 | 0 |
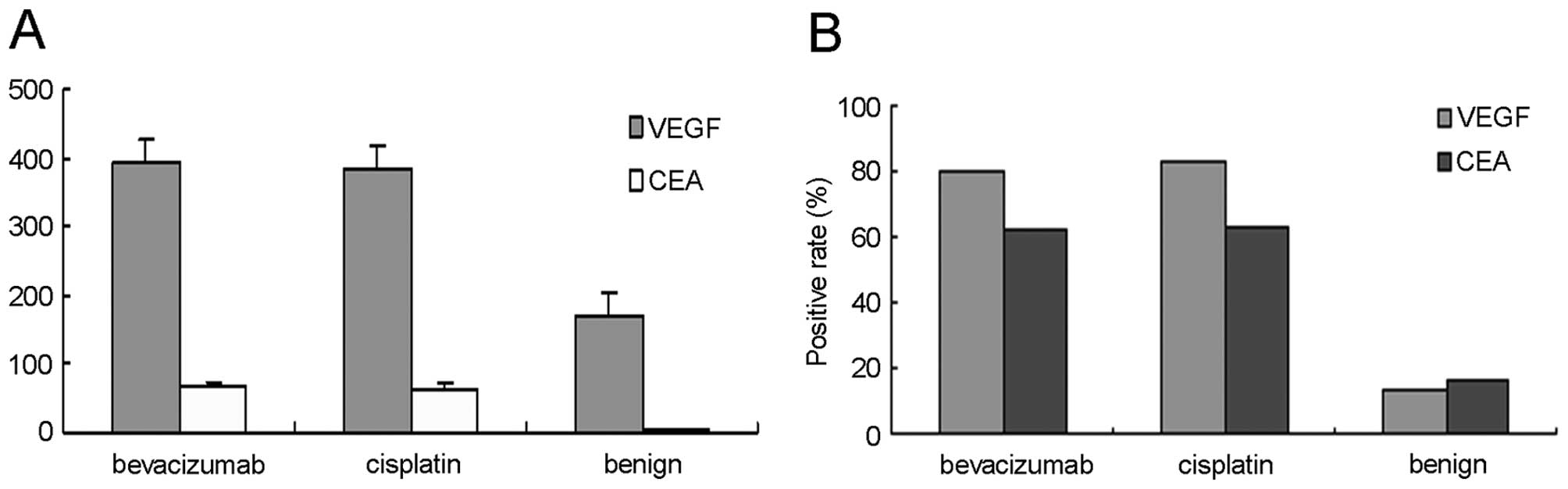
Levels and positive rate of VEGF-A and
CEA
The levels and positive rates of VEGF-A and CEA seen
in the pleural effusion are shown in Fig. 2. The difference between the two
groups of NSCLC study subjects treated with either cisplatin
monotherapy or combined therapy with bevacizumab and cisplatin was
not statistically significant (p>0.05). The tumor marker CEA
showed a significant difference between the study subjects
presenting with MPE and those presenting with benign effusion
(p<0.01). Treatment with bevacizumab and cisplatin significantly
decreased VEGF levels in the pleural fluid compared to that of the
cisplatin monotherapy group before and after the respective
treatments (p<0.01).
Relationship between VEGF expression and
response rate
The VEGF positive status of the study subjects was
determined when the pleural VEGF was higher than the normal maximum
value of 300.6 pg/l. This was a value generated from a previous
study which included 30 patients presenting with benign pleural
effusions (unpublished data). The CEA-positive status was
determined by comparison with the conventional standard value of
pleural effusion (5 ng/l).
Bevacizumab was particularly efficient in the
treatment of study subjects that were VEGF-positive (p<0.01)
(Table V). Of the six VEGF negative
study subjects, five showed no response to bevacizumab treatment,
which suggested that bevacizumab therapy was specific to
VEGF-positive patients. There were also five study subjects who
were negative for CEA, but positive for VEGF yet showed an
acceptable response to bevacizumab therapy (Table V). Of the 15 CEA-negative study
subjects, five were refractory to bevacizumab, while among the
bevacizumab-refractory study subjects, five presented as
CEA-positive, indicating that CEA was not a specific marker for
bevacizumab treatment. Analysis of the 25 study subjects who were
initially resistant to intrapleural therapy with bleomycin revealed
that combination therapy with bevacizumab plus cisplatin provoked
highly responsive regression of pleural effusion in 22 study
subjects, an observation which may support an association between
the VEGF-positive status and the actual response of study subjects
to bevacizumab.
| Table VRelationship between efficacy and
expression of VEGF and CEA in the bevacizumab group. |
Table V
Relationship between efficacy and
expression of VEGF and CEA in the bevacizumab group.
| VEGF (n=36) | CEA (n=36) |
|---|
|
|
|
|---|
| Positive | Negative | Positive | Negative |
|---|
| CR | 17 | 0 | 12 | 5 |
| PR | 12 | 1 | 8 | 5 |
| NC/PD | 1 | 5 | 1 | 5 |
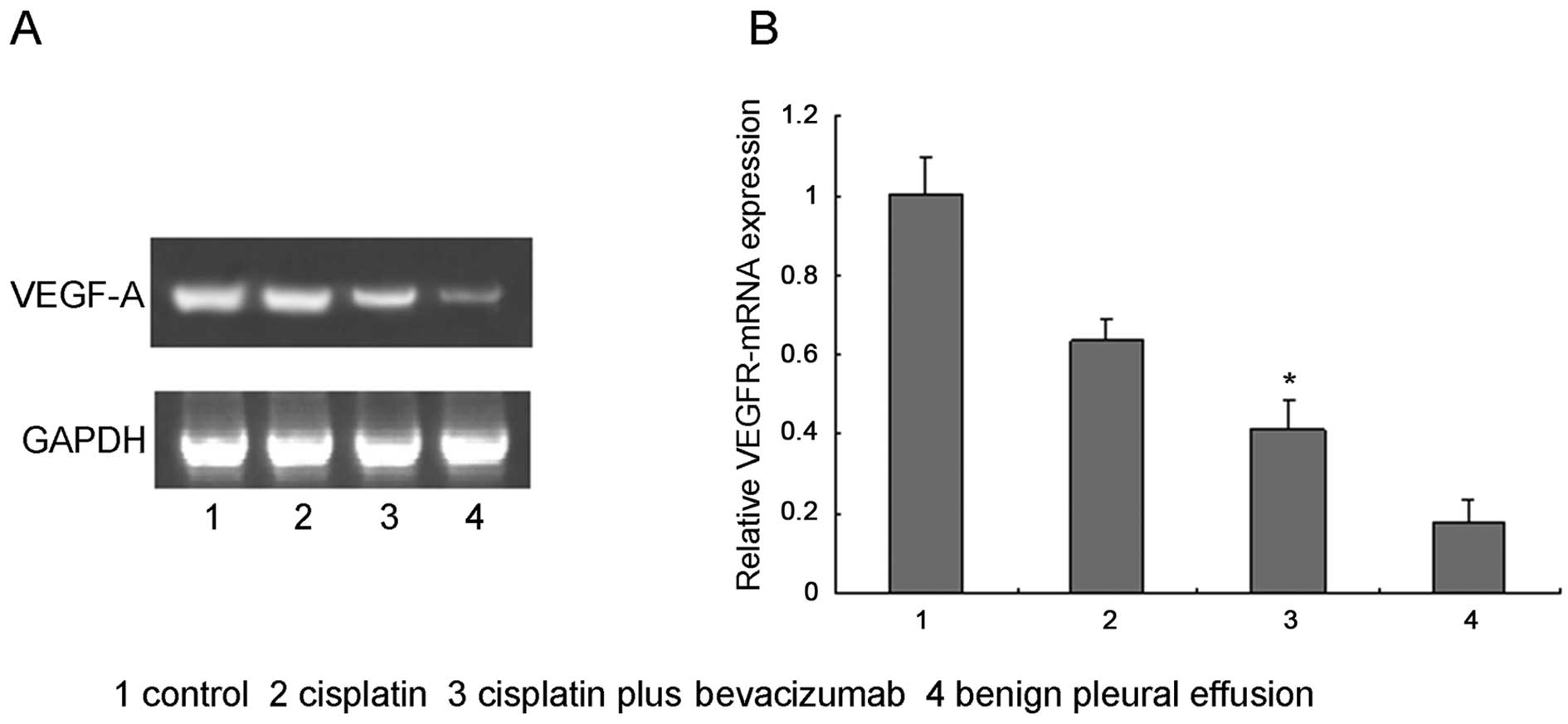
mRNA expression of VEGF-A in pleural
effusion
The pleural VEGF-A mRNA was significantly lower in
study subjects treated with combination therapy as compared with
subjects treated with cisplatin alone, as determined by real-time
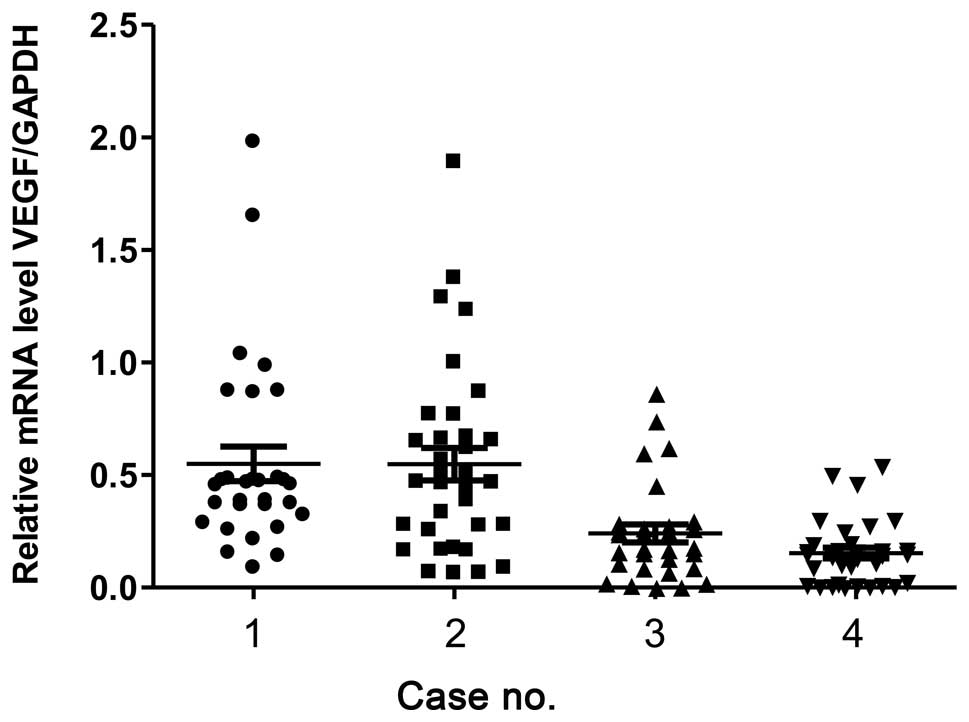
RT-PCR (Fig. 3). The expression
levels of VEGF-A mRNA (log copy number/μg) normalized to the
internal control GAPDH in samples without therapy (before therapy),
with cisplatin monotherapy and with combined cisplatin plus
bevacizumab therapy were found to be 0.54±0.12, 0.24±0.041 and
0.15±0.029, respectively. Expression of VEGF-A was significantly
lower following treatment with either cisplatin monotherapy or with
combined cisplatin plus bevacizumab (p<0.05) (Fig. 4). There was also no difference in
the basal expression of VEGF-A in both treatment groups (p=0.97)
(Fig. 4). In addition, both
treatment approaches were found to markedly decrease the mRNA
expression levels of VEGF-A (p<0.01) in the study subjects.
However, the extent to which VEGF-A mRNA decreased was much greater
in subjects that had received the combination therapy compared to
the subjects that had received cisplatin monotherapy (p<0.01).
This observation suggested that bevacizumab could significantly
reduce the levels of VEGF-A mRNA.
Discussion
Approximately 70–80% of patients with NSCLC are
diagnosed at relatively advanced stages (stage IIIB to IV) of their
disease, with a 5-year survival rate for NSCLC of less than 5%
(1). Malignant pleural effusion
(MPE) is seen in more than 50% of patients presenting with NSCLC
(1,2). The mortality rate of patients with MPE
is very high (19). The detection
of MPE can be a clinical indicator of local invasion or systemic
metastasis of advanced lung cancer.
The current mode of therapy for patients with MPE
involves primarily local treatment, such as tube drainage, chemical
pleurodesis and intrapleural administration of antineoplastic
agents, accompanied by the addition of a diuretic and albumin, and
restricted intake of salt and water. Among these therapeutic
approaches, intrapleural infusion is an important approach for
managing pleural effusion. The drugs that are used intrapleurally
include cisplatin, which can directly target tumor cells and
stimulate chemical pleurisy to reduce the pleural effusion
(20). However, as the ability of
intrapleural chemotherapy to penetrate the tumor is restricted to
only a few millimetres (21), the
response rates are often disappointing, with an effectiveness of
0–66% (22). Furthermore, the
clinical outcome of current modes of therapy is unstable and while
they can occasionally alleviate the symptoms, there is no eventual
benefit in patient survival.
It has been demonstrated that in cancer patients the
reabsorption of pleural fluid is blocked due to vascular and/or
lymph node metastasis. By contrast, tumor cells can also secrete
various growth factors which could lead to the local overexpression
of VEGF, and thus contribute to elevated capillary permeability and
fluid release from the capillary beds (10,23–27).
VEGF is a well-characterized angiogenic factor, with
VEGF-A serving a prominent role in this regard, which on binding to
its cognate receptors, primarily VEGFR-2, can increase vascular
permeability, stimulate proliferation of vascular endothelial
cells, promote the efflux of intravascular biological matrices,
inhibit apoptosis of endothelial cells and activate enzymes that
degrade the extracellular matrix. VEGF is thus able to facilitate
the growth and extension of neovascularization. The ability of VEGF
to promote vascular permeability renders it a key instigator of MPE
(28,29). The elevated efflux of plasma
proteins provides the microenvironment a suitable matrix for the
formation of pleural effusions (30–32).
Bevacizumab is a humanized monoclonal antibody
against VEGF-A, which is able to specifically block the binding of
VEGF-A to its receptor, and, by doing so, induces the degradation
of existing tumor blood vessels and normalization of the remaining
blood vessels (33). Bevacizumab
can also substantially suppress the continuous growth and
metastasis of tumor cells by repressing angiogenesis in the tumor
tissues (34). Bevacizumab has been
approved and recommended by the FDA in the treatment of certain
types of metastatic cancer, including colon, breast and kidney
tumors, as well as glioblastoma multiforme. The role of bevacizumab
in suppressing malignant progression of pleural effusion has only
recently been elucidated, and suggests that treatment with
bevacizumab, either as monotherapy or in combination with other
chemotherapeutic agents, could be useful in the treatment of
malignant pleural effusion (10,11).
In addition, preclinical studies and clinical research, although
still quite limited, have demonstrated that by inhibiting VEGF,
treatment with bevacizumab may represent an effective way to
prevent local fluid accumulation. To date, it has not been shown
whether intrapleural bevacizumab therapy can be applied to MPE as a
consequence of NSCLC.
On the basis of the aforementioned discussion, we
compared the efficacy and safety of intrapleural combination
therapy with bevacizumab and cisplatin with that of cisplatin
monotherapy on MPE. Our results indicated that the intrapleural
combination therapy of bevacizumab and cisplatin directed a very
promising short-term effect, with a response rate of 85.71%, a
value which was significantly higher than that of cisplatin
monotherapy (56.67%).
Our results are consistent with a recent report that
showed that pleural effusion could be markedly reduced by treatment
with bevacizumab in combination with carboplatin and paclitaxel in
a 63-year-old patient presenting with lung cancer (35). Similarly, intravenous or
intraperitoneal administration of bevacizumab has been shown to be
highly effective in the treatment of malignant ascites, at least in
studies where only a limited number of study subjects were assessed
(18,36–38).
We also showed that 88.57% of subjects presenting
with both NSCLC and MPE overexpressed VEGF following treatment with
bevacizumab. Additionally, study subjects that displayed originally
high VEGF expression levels showed a more improved response than
those subjects that were VEGF-negative.
The response rate for CEA-positive patients was
found to be 57.1%, where five subjects that were negative for CEA
but positive for VEGF showed a satisfactory response to
bevacizumab. By contrast, among the bevacizumab-resistant subjects,
three were found to be CEA-positive, and this observation indicated
that CEA was not a specific marker for bevacizumab treatment.
Analysis of the 25 subjects who were initially
resistant to chemotherapy showed that treatment with a combination
of bevacizumab plus cisplatin provoked regression of pleural
effusion in 22 of the 25 subjects. This observation further
supported the hypothesis that bevacizumab is highly effective in
the subjects that were considered VEGF-positive. Furthermore, in
most cases, the pleural effusion was well controlled after one or
two treatment cycles, and the stratification of effusion was
reduced following three cycles of treatment.
The median progression-free survival (PFS) for both
treatment groups showed a significant difference, and indicated
that the addition of bevacizumab to the therapeutic regimen may
significantly extend the PFS of patients with MPE. Although the
patients receiving bevacizumab treatment survived longer, the
median survival (OS) for the two groups did not show any
statistically significant difference. This could be due to the
difference of the second-line treatment that some of the study
subjects received.
Quantitative analysis of VEGF mRNA suggested that
there was no difference in basal VEGF expression between subjects
that had received any therapy. However, there was a significant
difference between the subjects that had received combination
therapy and the subjects that were treated with cisplatin
monotherapy.
We also found that the VEGF mRNA levels in patients
administered bevacizumab treatment were significantly lower than
those found in subjects treated with cisplatin monotherapy. This
observation suggested that bevacizumab may have downregulated
VEGF-A gene expression, thereby inhibiting cell proliferation and
migration, factors that are required for neoangiogenesis. This
finding also suggested that bevacizumab may have suppressed the
permeability of blood vessels, thereby eliminating the accumulation
of pleural fluid. We suggest that this is likely the underlying
mechanism by which bevacizumab inhibits the formation of MPE. Our
results further confirmed the clinical significance of detecting
VEGF mRNA and protein as biomarkers for the clinical management of
MPE with bevacizumab.
Overexpression of VEGF in tumor tissues is
associated with the metastatic potential of tumors and their rate
of survival (39,40). Thus, elevation in the serum levels
of VEGF and overexpression of VEGF within the tumor tissue are
considered to be associated with NSCLC staging and prognosis
(41,42). Of note, MPE that is caused by NSCLC
also shows substantial increases in the levels of VEGF and its
concentration exceeds that found in serum. By contrast, pleural
effusion that is caused by lung infections, heart failure or
cirrhosis of the liver does not appear to upregulate VEGF (43–48).
Additionally, previous studies have shown that VEGF is the most
highly overexpressed cytokine among 21 cytokines and chemokines
that have been identified in both benign and malignant pleural
effusion (31,49,50).
Markedly, the concentration of VEGF found in MPE can be considered
an independent prognostic factor for tumor PFS and total survival.
VEGF has been found to be associated with the sensitivity of tumors
to chemotherapeutic agents. Therefore, treatment with an antibody
specific to VEGF in patients with high levels of VEGF in the
pleural effusion suggests that VEGF can be considered a biomarker
for bevacizumab treatment of MPE (18,51,52).
Our study provides evidence that combination therapy
with intrapleural bevacizumab and cisplatin can efficiently treat
MPE caused by NSCLC. This combination therapy can readily diminish
effusion, with a positive health outcome for the patient. During
this study, we did not detect any severe side-effects, indicating
that this line of therapy is well tolerated. The combination
therapy used in our study was able to control pleural effusion
within a short period of time. Although mild hypertension was
detected, it never exceeded grade II. We did not observe any
proteinuria, thrombosis, gastrointestinal or pulmonary bleeding.
Also, we did not have a single research study subject withdraw from
the study due to toxicity. Although current evidence demonstrates
that intrapleural bevacizumab does not lead to specific risks, we
still recommend that some precautions be taken when managing
patients with a significant tumor burden or in patients where
squamous cell carcinoma is found in the main bronchus or in
patients receiving surgery in the latter stages of the disease.
Treatment with intrapleural delivery of bevacizumab
and cisplatin combination therapy is reliable, safe and feasible;
it provides a novel approach for the management of MPE, and
warrants further investigation. Our study demonstrated that the
VEGF levels found in the pleural effusions of benign disease were
markedly lower than those found in lung cancer. Moreover, VEGF
expression can be significantly downregulated by intrapleural
delivery of bevacizumab in lung cancer patients. This latter
observation supports the theory that bevacizumab suppresses MPE by
mechanisms dependent, in part, on the inhibition of VEGF
expression.
We conclude that intrapleural combinatorial therapy
with bevacizumab and cisplatin represents a novel treatment option
for MPE. Intrapleural infusion does not necessarily impart an
additional burden to the patients since it is also a routine
therapeutic approach for pleural effusion. The preclinical and
clinical study for intrapleural bevacizumab therapy has been
successful and has also yielded some promising outcomes (53,54).
Our findings provide further evidence to an accumulating body of
studies supporting the use of bevacizumab therapy, and suggest that
intrapleural bevacizumab therapy could provide long-lasting effects
in patients with MPE associated with advanced NSCLC. In addition,
our investigation suggests that biomonitoring VEGF expression
levels could be a reliable bioindicator of the clinical
effectiveness of bevacizumab therapy.
Acknowledgements
This study was supported by grants from the National
Health Research Foundation (no. W2010BX055), the National Natural
Science Foundation of China (no. 81000994), the Chinese Wu Jie-ping
Medical Foundation (no. 320.6750.1083), the Beijing Municipal
Science and Technology Commission (no. Z121107001012080), and the
National Natural Science Outstanding Youth Foundation of China (no.
39825111). The authors thank Dr Ye Qinong and Dr Sun Junzhong
(Institute of Molecular Biology Medicine, Beijing, China), and Dr
Ye Chuanzhong (Vanderbilt Epidemiology Center and Institute for
Medical Center North, Nashville, TN, USA) for their helpful
advice.
References
|
1
|
Sanz N, Aguado P, de Agustin JC, et al:
Parapneumonic effussion. A review of 33 cases over 6 years. Cir
Pediatr. 18:77–82. 2005.(In Spanish).
|
|
2
|
Ramalingam S and Belani C: Systemic
chemotherapy for advanced non-small cell lung cancer: recent
advances and future directions. Oncologist. 13(Suppl 1): 5–13.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Masuno T, Kishimoto S, Ogura T, et al: A
comparative trial of LC9018 plus doxorubicin and doxorubicin alone
for the treatment of malignant pleural effusion secondary to lung
cancer. Cancer. 68:1495–1500. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Rusch VW, Figlin R, Godwin D and
Piantadosi S: Intrapleural cisplatin and cytarabine in the
management of malignant pleural effusions: a Lung Cancer Study
Group trial. J Clin Oncol. 9:313–319. 1991.PubMed/NCBI
|
|
5
|
Luh KT, Yang PC, Kuo SH, Chang DB, Yu CJ
and Lee LN: Comparison of OK-432 and mitomycin C pleurodesis for
malignant pleural effusion caused by lung cancer. A randomized
trial. Cancer. 69:674–679. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tohda Y, Iwanaga T, Takada M, et al:
Intrapleural administration of cisplatin and etoposide to treat
malignant pleural effusions in patients with non-small cell lung
cancer. Chemotherapy. 45:197–204. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ishida A, Miyazawa T, Miyazu Y, et al:
Intrapleural cisplatin and OK432 therapy for malignant pleural
effusion caused by non-small cell lung cancer. Respirology.
11:90–97. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Senger DR, Galli SJ, Dvorak AM, Perruzzi
CA, Harvey VS and Dvorak HF: Tumor cells secrete a vascular
permeability factor that promotes accumulation of ascites fluid.
Science. 219:983–985. 1983. View Article : Google Scholar
|
|
9
|
Fontanini G, Faviana P, Lucchi M, et al: A
high vascular count and overexpression of vascular endothelial
growth factor are associated with unfavourable prognosis in
operated small cell lung carcinoma. Br J Cancer. 86:558–563. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sack U, Hoffmann M, Zhao XJ, et al:
Vascular endothelial growth factor in pleural effusions of
different origin. Eur Respir J. 25:600–604. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kobold S, Hegewisch-Becker S, Oechsle K,
Jordan K, Bokemeyer C and Atanackovic D: Intraperitoneal VEGF
inhibition using bevacizumab: a potential approach for the
symptomatic treatment of malignant ascites? Oncologist.
14:1242–1251. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ferrara N, Gerber HP and LeCouter J: The
biology of VEGF and its receptors. Nat Med. 9:669–676. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Pichelmayer O, Zielinski C and Raderer M:
Response of a nonmalignant pleural effusion to bevacizumab. N Engl
J Med. 353:740–741. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Neragi-Miandoab S: Malignant pleural
effusion, current and evolving approaches for its diagnosis and
management. Lung Cancer. 54:1–9. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Cohen MH, Gootenberg J, Keegan P and
Pazdur R: FDA drug approval summary: bevacizumab (Avastin) plus
Carboplatin and Paclitaxel as first-line treatment of
advanced/metastatic recurrent nonsquamous non-small cell lung
cancer. Oncologist. 12:713–718. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ribeiro SC, Vargas FS, Antonangelo L, et
al: Monoclonal anti-vascular endothelial growth factor antibody
reduces fluid volume in an experimental model of inflammatory
pleural effusion. Respirology. 14:1188–1193. 2009.
|
|
17
|
Teixeira LR, Vargas FS, Acencio MM, et al:
Blockage of vascular endothelial growth factor (VEGF) reduces
experimental pleurodesis. Lung Cancer. 74:392–395. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Pichelmayer O, Gruenberger B, Zielinski C
and Raderer M: Bevacizumab is active in malignant effusion. Ann
Oncol. 17:18532006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sahn SA: Management of malignant pleural
effusions. Monaldi Arch Chest Dis. 56:394–399. 2001.PubMed/NCBI
|
|
20
|
Musani AI: Treatment options for malignant
pleural effusion. Curr Opin Pulm Med. 15:380–387. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Los G, Mutsaers PH, van der Vijgh WJ,
Baldew GS, de Graaf PW and McVie JG: Direct diffusion of
cis-diamminedichloroplatinum(II) in intraperitoneal rat tumors
after intraperitoneal chemotherapy: a comparison with systemic
chemotherapy. Cancer Res. 49:3380–3384. 1989.PubMed/NCBI
|
|
22
|
Walker-Renard PB, Vaughan LM and Sahn SA:
Chemical pleurodesis for malignant pleural effusions. Ann Intern
Med. 120:56–64. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Aslam N and Marino CR: Malignant ascites:
new concepts in pathophysiology, diagnosis, and management. Arch
Intern Med. 161:2733–2737. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Grove CS and Lee YC: Vascular endothelial
growth factor: the key mediator in pleural effusion formation. Curr
Opin Pulm Med. 8:294–301. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Patane S, Marte F, Di Bella G and Davi M:
Pericardial effusion with elevated serum carbohydrate antigen 125
levels and ovarian tumor mass. Int J Cardiol. 127:e105–e107. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Yokoyama T, Tanaka A, Kato S and Aizawa H:
Multiple myeloma presenting initially with pleural effusion and a
unique paraspinal tumor in the thorax. Intern Med. 47:1917–1920.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Chen Y, Liang B, Zhao YJ, Wang SC, Fan YB
and Wu GP: Transcription expression and clinical significance of
vascular endothelial growth factor mRNA and endostatin mRNA in
pleural effusions of patients with lung cancer. Diagn Cytopathol.
40:287–291. 2012. View
Article : Google Scholar : PubMed/NCBI
|
|
28
|
Folkman J, Merler E, Abernathy C and
Williams G: Isolation of a tumor factor responsible for
angiogenesis. J Exp Med. 133:275–288. 1971. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Mohammed KA, Nasreen N, Hardwick J, Logie
CS, Patterson CE and Antony VB: Bacterial induction of pleural
mesothelial monolayer barrier dysfunction. Am J Physiol Lung Cell
Mol Physiol. 281:L119–L125. 2001.PubMed/NCBI
|
|
30
|
Folkman J: Tumor angiogenesis and tissue
factor. Nat Med. 2:167–168. 1996. View Article : Google Scholar
|
|
31
|
Zebrowski BK, Yano S, Liu W, et al:
Vascular endothelial growth factor levels and induction of
permeability in malignant pleural effusions. Clin Cancer Res.
5:3364–3368. 1999.PubMed/NCBI
|
|
32
|
Strizzi L, Catalano A, Vianale G, et al:
Vascular endothelial growth factor is an autocrine growth factor in
human malignant mesothelioma. J Pathol. 193:468–475. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Presta LG, Chen H, O’Connor SJ, et al:
Humanization of an anti-vascular endothelial growth factor
monoclonal antibody for the therapy of solid tumors and other
disorders. Cancer Res. 57:4593–4599. 1997.PubMed/NCBI
|
|
34
|
Shaheen RM, Tseng WW, Vellagas R, et al:
Effects of an antibody to vascular endothelial growth factor
receptor-2 on survival, tumor vascularity, and apoptosis in a
murine model of colon carcinomatosis. Int J Oncol. 18:221–226.
2001.
|
|
35
|
Hama M, Komatsu Y and Hachiya T: A case of
lung cancer showing marked reduction of pleural effusion by
bevacizumab in combination with carboplatin and paclitaxel. Gan To
Kagaku Ryoho. 38:1877–1879. 2011.(In Japanese).
|
|
36
|
Numnum TM, Rocconi RP, Whitworth J and
Barnes MN: The use of bevacizumab to palliate symptomatic ascites
in patients with refractory ovarian carcinoma. Gynecol Oncol.
102:425–428. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Hamilton CA, Maxwell GL, Chernofsky MR,
Bernstein SA, Farley JH and Rose GS: Intraperitoneal bevacizumab
for the palliation of malignant ascites in refractory ovarian
cancer. Gynecol Oncol. 111:530–532. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Kesterson JP, Mhawech-Fauceglia P and Lele
S: The use of bevacizumab in refractory ovarian granulosa-cell
carcinoma with symptomatic relief of ascites: a case report.
Gynecol Oncol. 111:527–529. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Volm M, Koomagi R and Mattern J:
Prognostic value of vascular endothelial growth factor and its
receptor Flt-1 in squamous cell lung cancer. Int J Cancer.
74:64–68. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Kassim SK, El-Salahy EM, Fayed ST, et al:
Vascular endothelial growth factor and interleukin-8 are associated
with poor prognosis in epithelial ovarian cancer patients. Clin
Biochem. 37:363–369. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Kumar H, Heer K, Lee PW, et al:
Preoperative serum vascular endothelial growth factor can predict
stage in colorectal cancer. Clin Cancer Res. 4:1279–1285.
1998.PubMed/NCBI
|
|
42
|
Matsuyama W, Hashiguchi T, Mizoguchi A, et
al: Serum levels of vascular endothelial growth factor dependent on
the stage progression of lung cancer. Chest. 118:948–951. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Cheng D, Rodriguez RM, Perkett EA, et al:
Vascular endothelial growth factor in pleural fluid. Chest.
116:760–765. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Kraft A, Weindel K, Ochs A, et al:
Vascular endothelial growth factor in the sera and effusions of
patients with malignant and nonmalignant disease. Cancer.
85:178–187. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Thickett DR, Armstrong L and Millar AB:
Vascular endothelial growth factor (VEGF) in inflammatory and
malignant pleural effusions. Thorax. 54:707–710. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Yanagawa H, Takeuchi E, Suzuki Y, Ohmoto
Y, Bando H and Sone S: Vascular endothelial growth factor in
malignant pleural effusion associated with lung cancer. Cancer
Immunol Immunother. 48:396–400. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Verheul HM, Hoekman K, Jorna AS, Smit EF
and Pinedo HM: Targeting vascular endothelial growth factor
blockade: ascites and pleural effusion formation. Oncologist.
5(Suppl 1): 45–50. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Ishimoto O, Saijo Y, Narumi K, et al: High
level of vascular endothelial growth factor in hemorrhagic pleural
effusion of cancer. Oncology. 63:70–75. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Kishiro I, Kato S, Fuse D, Yoshida T,
Machida S and Kaneko N: Clinical significance of vascular
endothelial growth factor in patients with primary lung cancer.
Respirology. 7:93–98. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Momi H, Matsuyama W, Inoue K, et al:
Vascular endothelial growth factor and proinflammatory cytokines in
pleural effusions. Respir Med. 96:817–822. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Harlozinska A, Sedlaczek P, Kulpa J, et
al: Vascular endothelial growth factor (VEGF) concentration in sera
and tumor effusions from patients with ovarian carcinoma.
Anticancer Res. 24:1149–1157. 2004.PubMed/NCBI
|
|
52
|
Rudlowski C, Pickart AK, Fuhljahn C, et
al: Prognostic significance of vascular endothelial growth factor
expression in ovarian cancer patients: a long-term follow-up. Int J
Gynecol Cancer. 16(Suppl 1): 183–189. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Watanabe M, Boyer JL and Crystal RG:
AAVrh.10-mediated genetic delivery of bevacizumab to the pleura to
provide local anti-VEGF to suppress growth of metastatic lung
tumors. Gene Ther. 17:1042–1051. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Konner JA, Grabon DM, Gerst SR, et al:
Phase II study of intraperitoneal paclitaxel plus cisplatin and
intravenous paclitaxel plus bevacizumab as adjuvant treatment of
optimal stage II/III epithelial ovarian cancer. J Clin Oncol.
29:4662–4668. 2011. View Article : Google Scholar
|