Introduction
Epstein-Barr virus (EBV) is a ubiquitous γ-herpes
virus that maintains a life-long latent infection in B lymphocytes
in over 90% of adults following salivary transmission during
childhood or adolescence (1). Since
its discovery in tumor cells of Burkitt’s lymphoma 40 years ago,
EBV has been associated with various types of cancers, including
lymphoid neoplasms, nasopharyngeal and gastric epithelial
malignancies, and a subset of mesenchymal tumors (1,2).
EBV-associated gastric carcinoma (EBVaGC) accounts for ~10% of
gastric cancer cases (3–5). Gastric cancer has the fourth highest
incidence of all types of cancers worldwide, and the burden of
EBVaGC is estimated at 75,000–90,000 new cases annually,
representing the largest subpopulation among EBV-related tumors
(1,6).
From the viewpoint of the clinical distribution,
EBVaGC presents the distinct characteristics of a male
preponderance, proximal location and high incidence in stump cancer
(3–5,7,8). In
fact, EBVaGC is a heterogeneous histological group consisting of
lymphoepithelioma-like carcinoma (LELC) and conventional
adenocarcinoma (3,4,7). More
than 80% of LELC cases are associated with EBV infection, while
only 5–10% of ordinary adenocarcinoma cases are positive for EBV
infection. The LELC histotype has been demonstrated to present a
significantly favorable prognosis as a result of extensive
infiltration of CD8+ T cells and mature dendritic cells
within these tumors (9–11). Nevertheless, controversy still
exists regarding the prognostic significance of EBV infection
itself. Several studies reported a better prognosis in EBVaGC, but
a favorable outcome may not be observed after adjusting for other
clinicopathological features (11,12).
Other researchers have failed to show that EBVaGC differs from
EBV-negative gastric cancer in terms of survival (8,13–15).
There is a paucity of studies regarding the impact of
clinicopathological factors on survival in EBVaGC. A recent study
showed that advanced stage and histological classification were
meaningful indicators of survival (11).
Since stage I–III gastric cancer patients comprise a
population with diverse outcomes, there is considerable interest in
understanding the predictors of this cancer’s behavior beyond the
Union for International Cancer Control/American Joint Committee on
Cancer (UICC/AJCC) stage. These factors, including the tumor size
and lymph node (LN) ratio, defined as the ratio of metastatic to
retrieved lymph nodes, have not yet been examined specifically in
EBVaGC. Therefore, the present study was conducted to investigate
the prognostic significance of the relevant clinicopathological
parameters in stage I–III EBVaGC and to determine the predictive
factors that would aid in the identification of high-risk patients
who may benefit from adjuvant therapy.
Materials and methods
Case selection
We retrospectively enrolled gastric cancer cases
according to the following criteria: radical resection with lymph
node dissection and final pathologic stage I to III according to
the 2010 UICC/AJCC staging system. From January 1999 to December
2006, 1,020 consecutive surgically resected specimens of gastric
carcinoma were retrieved from the archives of the Department of
Pathology at Chang Chung Memorial Hospital, Linkou, Taiwan.
Clinical information concerning the patient characteristics and
outcome was collected from the medical records. The survival period
was traced until December 31, 2012. The study was approved by the
institutional review board at our hospital.
Tissue microarrays and EBV-encoded small
RNA in situ hybridization
The formalin-fixed and paraffin-embedded tissue
samples were arrayed using an automated tissue-arraying machine
(Beecher ATA-27; Beecher Instruments, Sun Prairie, WI, USA). All
hematoxylin and eosin-stained slides were reviewed to choose
representative tumor areas. Three 1.0-mm tissue cores were taken
from tissue blocks and transferred to receipt blocks. The tissue
microarrays were used for EBV-encoded small RNA (EBER) in
situ hybridization.
EBER in situ hybridization was performed on
tissue microarray slides using the EBV Probe ISH kit from Leica
Microsystems in an automated immunostaining machine (BOND-MAX™;
Leica, Wetzlar, Germany). The procedures were conducted according
to the manufacturer’s instructions. Only cases with universal and
strong nuclear staining within almost all tumor cells were
interpreted as EBV-positive.
Pathological analysis
More than two hematoxylin and eosin-stained slides
of each EBVaGC were reviewed blindly by two pathologists (Dr S.C.
Huang and Dr T.C. Chen) to determine the tumor type. We
subclassified the EBVaGC specimens into LELC, tubular
adenocarcinoma, poorly cohesive adenocarcinoma and mucinous
adenocarcinoma. LELC was defined by the Watanabe’s and Shibata’s
criteria: well circumscribed, undifferentiated carcinoma,
non-desmoplastic stroma with dense lymphoplasmacytic infiltration
(10,16). Tubular adenocarcinoma, poorly
cohesive adenocarcinoma, and mucinous adenocarcinoma were defined
as tumors with >50% of the tumor cells growing in a tubular
pattern, poor cohesion and mucin pools, respectively, according to
WHO classification (17). Mixed
carcinoma was defined as a mixture of tubular adenocarcinoma and
poorly cohesive carcinoma if either component accounted for >10%
of the tumor.
Immunohistochemistry of HER2
We used a HER2 monoclonal antibody (A485, 1:200;
Dako, Carpinteria, CA, USA) for immunostaining. Tissue sections of
EBVaGC were prepared at a thickness of 3-μm and deparaffinized in
xylene and rehydrated in a graded ethanol series. The slides were
submitted to antigen retrieval, antibody incubation and chromogen
counterstaining in an automated immunostainer (BOND-MAX™). Optimal
positive and negative controls were also performed at the same
time. Two experienced pathologists interpreted the HER2 status
according to the recommendation for gastric cancer (18).
Statistical analysis
Statistical analysis was performed on an SPSS
platform (version 17; SPSS, Chicago, IL, USA). The associations
between the clinicopathological characteristics and the EBV status
were evaluated by independent t-test, Pearson’s χ2 or
Fisher exact test, according to the variable type. A multivariate
logistic regression model was applied to the variables with a
p-value <0.05 in the univariate analysis. For the comparison of
LELC and non-LELC EBVaGC, the Mann-Whitney U test was employed for
some continuous variables, including age, size and LN ratio. The
overall survival was measured from the date of surgery to the date
of death. Kaplan-Meier estimate was performed to calculate the
overall survival, and the statistical significance of different
variables was examined by the log-rank test. The Cox proportional
hazard regression model was undertaken to determine the independent
prognostic factors. Two-sided p-values were calculated, and
p<0.05 was considered to be significant for all statistical
analyses.
Results
Patient characteristics and pathological
findings
A total of 52 EBVaGCs (5.1%) were identified by EBER
in situ hybridization from 1,020 stage I–III gastric
cancers. The clinical and pathologic features of the cases of
EBVaGC and EBV-negative gastric cancer are summarized in Table I. The EBVaGC cases included 43 men
and 9 women with a mean age of 64.83 years. The multivariate
logistic regression analysis demonstrated that EBVaGC had a male
predominance [odds ratio (OR) 3.120, 95% confidence interval (CI)
1.473–6.612, p=0.003] and a higher incidence in stump cancers (OR
5.957, 95% CI 2.423–14.648, p<0.0001) and poorly differentiated
adenocarcinoma (OR 2.494, 95% CI 1.249–4.981, p=0.010) in
comparison to EBV-negative gastric cancer. The EBVaGCs tended to
occur more frequently in the proximal and middle portion than
EBV-negative gastric cancer (57.7 vs. 32.0%), although the
multivariate analysis failed due to the occurrence of
non-convergence in the logistic regression models. No significant
difference was found in regards to patient age, Lauren’s
classification, depth of invasion, metastatic node number,
UICC/AJCC stage, lymphovascular permeation, perineural invasion and
Helicobacter infection status between the EBVaGCs and
EBV-negative gastric cancer. The tumor size and LN ratio were also
not significantly different.
 | Table IClinicopathological findings of stage
I–III gastric cancer patients classified by EBV status. |
Table I
Clinicopathological findings of stage
I–III gastric cancer patients classified by EBV status.
| EBV status | Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Parameters | Negative
(n=968) | Positive
(n=52) | P-value | Odds ratio | 95% CI | P-value |
|---|
| Age (years), mean ±
SD | 63.65±13.51 | 64.83±11.02 | 0.536 | | | |
| Gender | | | 0.001 | | | |
| Male | 567 (58.6) | 43 (82.7) | | 3.120 | 1.473–6.612 | 0.003 |
| Female | 401 (41.4) | 9 (17.3) | | 1 | | |
| Stump cancer | | | <0.0001 | | | |
| Yes | 21 (2.2) | 10 (19.2) | | 5.957 | 2.423–14.648 | <0.001 |
| No | 947 (97.8) | 42 (80.8) | | 1 | | |
|
Localizationa | | | <0.001 | | | |
| Upper | 149 (15.4) | 20 (38.5) | | | | |
| Middle | 161 (16.6) | 10 (19.2) | | | | |
| Lower | 620 (64.0) | 21 (40.4) | | | | |
| Diffuse | 38 (3.9) | 1 (1.9) | | | | |
| Tumor size, mean ±
SD (cm) | 4.43±3.17 | 4.44±2.36 | 0.966 | | | |
|
Differentiation | | | 0.010 | | | |
| Well/moderate | 397 (41.0) | 12 (23.1) | | 1 | | |
| Poor | 571 (59.0) | 40 (76.9) | | 2.494 | 1.249–4.981 | 0.010 |
| Lauren’s
classification | | | 0.120 | | | |
| Intestinal | 489 (50.5) | 25 (48.1) | | | | |
| Diffuse | 365 (37.7) | 16 (30.8) | | | | |
| Mixed | 114 (11.8) | 11 (21.2) | | | | |
| Depth of
invasion | | | 0.039 | | | |
| T1/T2 | 360 (37.2) | 12 (23.1) | | 1 | | |
| T3/T4 | 608 (62.8) | 40 (76.9) | | 1.233 | 0.604–2.520 | 0.565 |
| Nodal status | | | 0.753 | | | |
| N0 | 384 (39.7) | 17 (32.7) | | | | |
| N1 | 133 (13.7) | 7 (13.5) | | | | |
| N2 | 154 (15.9) | 10 (19.2) | | | | |
| N3 | 297 (30.7) | 18 (34.6) | | | | |
| Stage | | | 0.179 | | | |
| I | 283 (29.2) | 9 (17.3) | | | | |
| II | 177 (18.3) | 11 (21.2) | | | | |
| III | 508 (52.5) | 32 (61.5) | | | | |
| LN ratio, mean ±
SD | 0.21±0.27 | 0.19±0.21 | 0.702 | | | |
| Lymphatic
invasionb | | | 0.204 | | | |
| No | 475 (49.4) | 21 (40.4) | | | | |
| Yes | 486 (50.6) | 31 (59.6) | | | | |
| Vascular
invasionb | | | 0.863 | | | |
| No | 838 (87.7) | 46 (88.5) | | | | |
| Yes | 118 (12.3) | 6 (11.5) | | | | |
| Perineural
invasionb | | | 0.892 | | | |
| No | 505 (52.9) | 28 (53.8) | | | | |
| Yes | 450 (47.1) | 24 (46.2) | | | | |
| HP infection | | | 0.462 | | | |
| No | 771 (80.5) | 44 (84.6) | | | | |
| Yes | 187 (19.5) | 8 (15.4) | | | | |
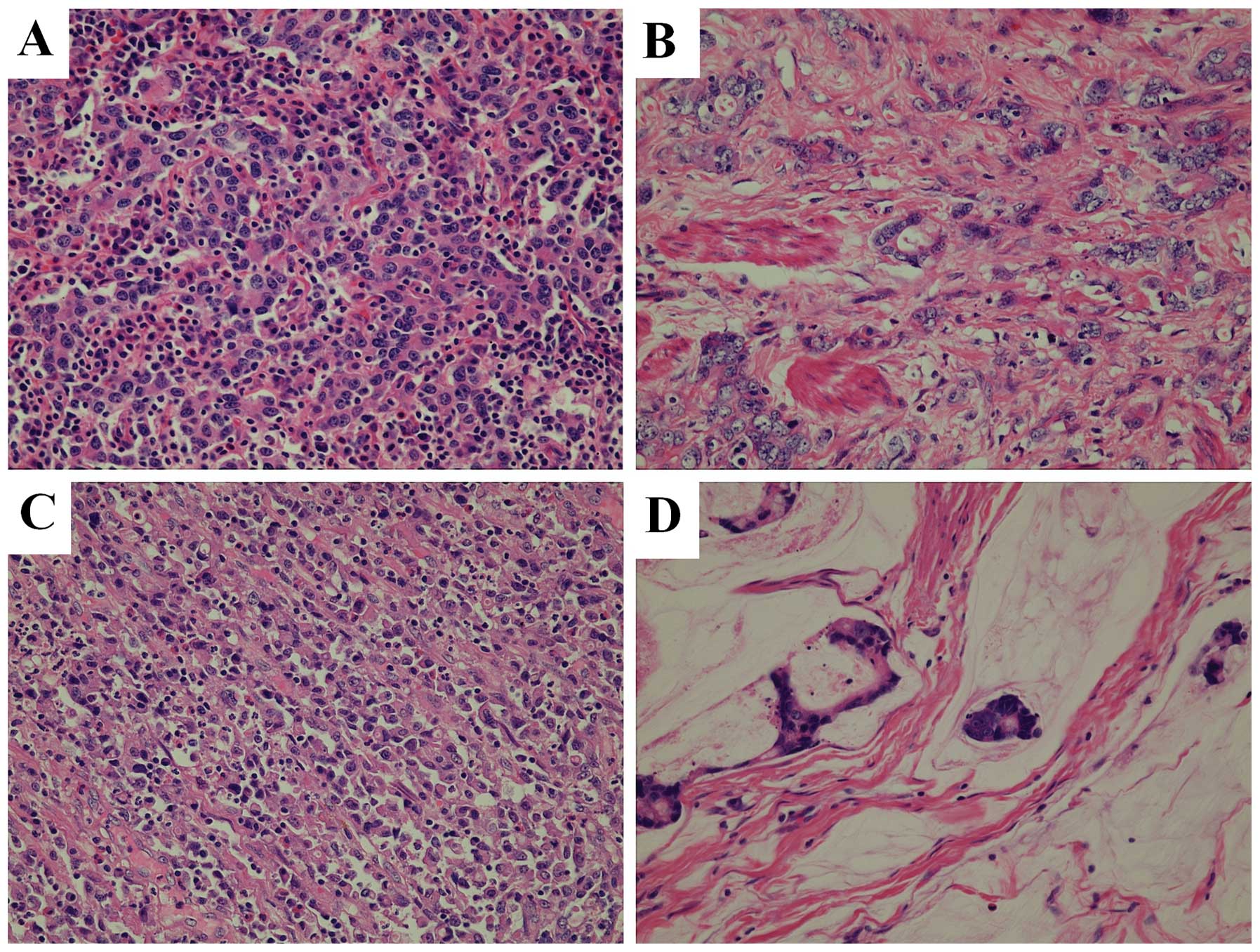
The 52 cases of EBVaGC were further subclassified
into 19 LELC cases (36.5%) and 33 non-LELC cases (63.5%) (Fig. 1). The 33 non-LELC EBVaGC cases
consisted of 29 cases of tubular adenocarcinoma (87.9%), 1 case of
poorly cohesive carcinoma (3.0%), 1 case of mucinous adenocarcinoma
(3.0%) and 2 cases of mixed carcinoma (6.1%). After excluding 1
case that suffered from surgical mortality, the clinicopathological
parameters of LELC and non-LELC in the 51 cases of EBVaGC were not
significantly different, with the exception of tumor
differentiation (p=0.004) (Table
II).
| Table IIClinicopathological findings of stage
I–III EBV-associated gastric cancer patients classified by tumor
histology. |
Table II
Clinicopathological findings of stage
I–III EBV-associated gastric cancer patients classified by tumor
histology.
| Tumor type | |
|---|
|
| |
|---|
| Parameters | LELC (n=18) | Non-LELC
(n=33) | P-value |
|---|
| Age (years), median
(range) | 62 (44–81) | 70 (39–80) | 0.253 |
| Gender | | | 0.703 |
| Male | 14 (77.8) | 28 (984.8) | |
| Female | 4 (22.2) | 5 (15.2) | |
| Stump cancer | | | 0.727 |
| Yes | 4 (22.2) | 6 (18.2) | |
| No | 14 (77.8) | 27 (81.8) | |
| Localization | | | 0.322 |
| Upper | 5 (27.8) | 15 (45.5) | |
| Middle | 3 (16.7) | 7 (21.2) | |
| Lower | 10 (55.6) | 10 (30.3) | |
| Diffuse | 0 | 1 (3.0) | |
| Tumor size (cm),
median (range) | 3.8 (1.0–6.0) | 4.5 (0.8–14.0) | 0.161 |
|
Differentiation | | | 0.004 |
| Well/moderate | 0 | 12 (36.4) | |
| Poor | 18 (100.0) | 21 (63.6) | |
| Lauren’s
classification | | | 0.106 |
| Intestinal | 5 (27.8) | 19 (57.6) | |
| Diffuse | 7 (38.9) | 9 (27.3) | |
| Mixed | 6 (33.3) | 5 (15.2) | |
| Depth of
invasion | | | 0.304 |
| T1/T2 | 6 (33.3) | 6 (18.2) | |
| T3/T4 | 12 (66.7) | 27 (81.8) | |
| Nodal status | | | 0.282 |
| N0 | 9 (50.0) | 8 (24.2) | |
| N1 | 2 (11.1) | 5 (15.2) | |
| N2 | 3 (16.7) | 6 (18.2) | |
| N3 | 4 (22.2) | 14 (42.4) | |
| Stage | | | 0.189 |
| I | 5 (27.8) | 4 (12.1) | |
| II | 5 (27.8) | 6 (18.2) | |
| III | 8 (44.4) | 23 (69.7) | |
| LN ratio, median
(range) | 0.03 (0–0.57) | 0.19 (0–0.81) | 0.116 |
| Lymphatic
invasion | | | 0.244 |
| No | 9 (50.0) | 11 (33.3) | |
| Yes | 9 (50.0) | 22 (66.7) | |
| Vascular
invasion | | | 0.078 |
| No | 18 (100.0) | 27 (81.8) | |
| Yes | 0 | 6 (18.2) | |
| Perineural
invasion | | | 0.147 |
| No | 12 (66.7) | 15 (45.5) | |
| Yes | 6 (33.3) | 18 (54.5) | |
| HP infection | | | 0.686 |
| No | 15 (83.3) | 29 (87.9) | |
| Yes | 3 (16.7) | 4 (12.1) | |
HER2 immunohistochemistry
Only one case of the 52 EBVaGCs (1.9%) demonstrated
HER2 overexpression (strong intensity, score 3+).
Survival analysis
According to the available survival data, the mean
survival duration for the 51 cases of EBVaGC and the 943 cases of
EBV-negative gastric cancer was 87.74 (95% CI 70.37–105.11) and
88.1 (95% CI 84.09–92.12) months, respectively. The follow-up
duration for the 51 cases of EBVaGC ranged from 1.2 to 166 months
(median 45.04 months). EBV infection itself was not a prognostic
factor in stage I–III gastric cancer (p=0.977) (Fig. 2). According to the survival analysis
of EBVaGC, the log-rank analysis revealed that tumor location,
tumor size >5 cm, depth of tumor invasion, number of lymph node
metastasis, LN ratio, lymphovascular invasion, perineural invasion
and LELC subtype reached statistical significance as prognostic
factors (Table III). In the Cox
proportional hazard model, tumor size >5 cm [hazard ratio (HR)
2.884, 95% CI 1.129–7.365, p=0.027], LN ratio >0.15 (HR 19.352,
95% CI 4.383–85.441, p<0.0001), and non-LELC subtypes (HR
12.178, 95% CI 2.135–69.474, p=0.005) had an unfavorable effect on
survival. However, the depth of tumor invasion and nodal status
lost their statistical significance (p=0.834 and 0.844,
respectively). Tumor location was excluded due to the occurrence of
the monotone likelihood, and the maximum likelihood estimation did
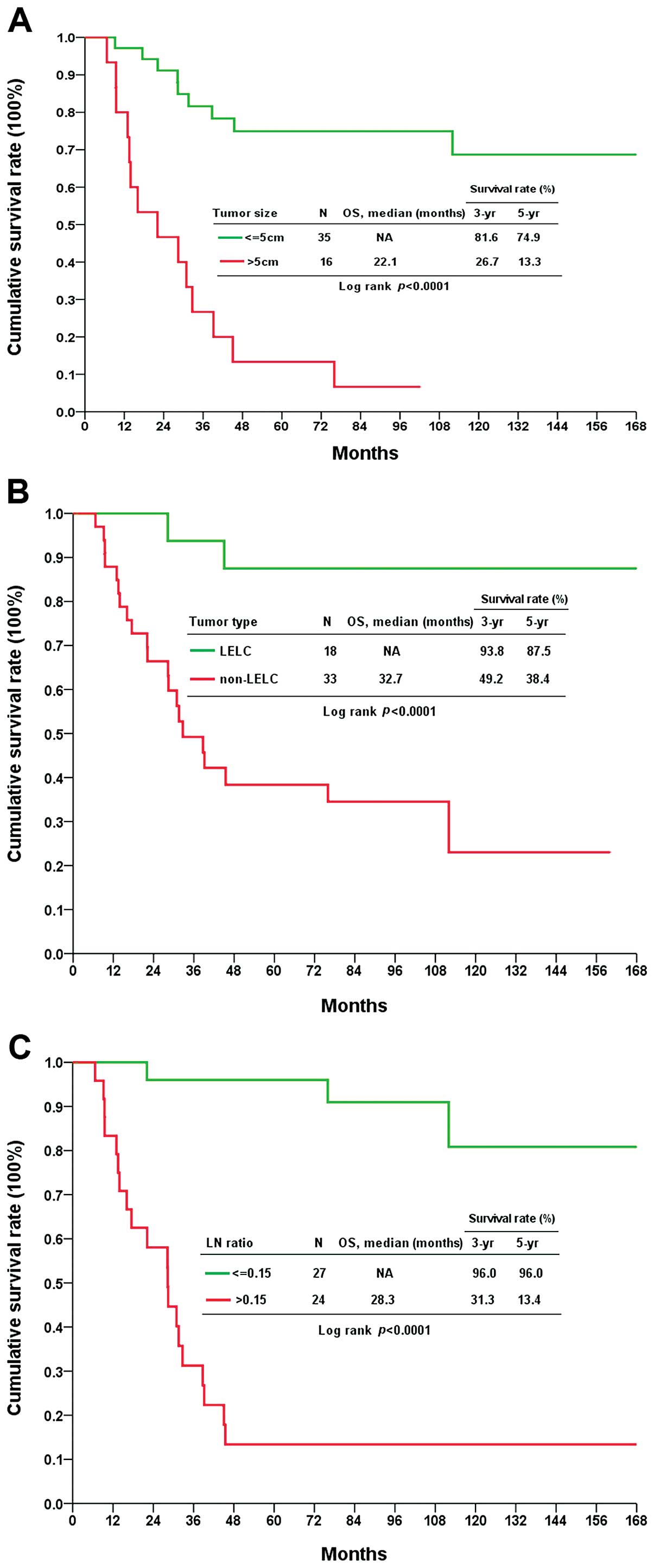
not exist. The median survival for cases with a tumor size >5 cm
was 22.1 months with a 5-year survival rate of 13.3% compared to
74.9% in tumors with a size ≤5 cm (Fig.
3A). LELC EBVaGC had a 5-year survival rate of 87.5%, which was
superior to the non-LELC cases with a 5-year survival rate of 38.4%
and a median survival of 32.7 months (Fig. 3B). Cases with an LN ratio >0.15
had a median survival of 28.3 months and a 13.4% 5-year survival
rate, whereas cases with an LN ratio ≤0.15 had a 96.0% 5-year
survival rate (Fig. 3C).
| Table IIISurvival analysis of patients with
stage I–III EBV-associated gastric cancer. |
Table III
Survival analysis of patients with
stage I–III EBV-associated gastric cancer.
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|---|
| Clinicopathological
factors | Mean survival
(months) | 95% CI | P-value | Hazard ratio | 95% CI | P-value |
|---|
| Age (years) | | | 0.116 | | | |
| ≤65 (n=25) | 120.81 | 91.59–150.03 | | | | |
| >65 (n=26) | 79.73 | 51.57–107.90 | | | | |
| Gender | | | 0.859 | | | |
| Male (n=42) | 101.62 | 77.56–125.68 | | | | |
| Female (n=9) | 80.24 | 49.32–111.15 | | | | |
| Locationa | | | <0.0001 | | | |
| Upper (n=20) | 79.68 | 49.76–109.61 | | | | |
| Middle (n=10) | 102.77 | 60.51–145.02 | | | | |
| Lower (n=20) | 119.82 | 86.44–153.21 | | | | |
| Diffuse (n=1) | 6.67 | 6.67–6.67 | | | | |
| Tumor size
(cm) | | | <0.0001 | | | |
| ≤5 (n=35) | 135.28 | 112.41–158.14 | | 1 | | |
| >5 (n=16) | 30.58 | 17.45–43.71 | | 2.884 | 1.129–7.365 | 0.027 |
|
Differentiation | | | 0.892 | | | |
| Well/moderate
(n=12) | 86.48 | 51.27–121.69 | | | | |
| Poor (n=39) | 105.19 | 80.19–130.20 | | | | |
| Histological
classification | | | <0.0001 | | | |
| LELC (n=18) | 158.97 | 136.27–181.68 | | 1 | | |
| Non-LELC
(n=33) | 67.04 | 44.61–89.47 | | 12.178 | 2.135–69.474 | 0.005 |
| Depth of
invasion | | | 0.032 | | | 0.834 |
| T1/T2 (n=12) | 145.23 | 118.37–172.09 | | | | |
| T3/T4 (n=39) | 90.10 | 65.54–114.65 | | | | |
| Nodal status | | | <0.0001 | | | 0.844 |
| N0 (n=17) | 160.30 | 145.92–174.69 | | | | |
| N1 (n=7) | 116.73 | 86.43–147.03 | | | | |
| N2 (n=9) | 79.00 | 27.26–131.93 | | | | |
| N3 (n=18) | 37.42 | 20.87–53.98 | | | | |
| LN ratio | | | <0.0001 | | | |
| ≤0.15 (n=27) | 151.83 | 134.94–168.72 | | 1 | | |
| >0.15
(n=24) | 44.72 | 22.92–66.51 | | 19.352 | 4.383–85.441 | <0.0001 |
| Lymphatic
invasion | | | 0.001 | | | 0.699 |
| No (n=20) | 146.21 | 123.60–168.81 | | | | |
| Yes (n=31) | 72.10 | 46.34–97.87 | | | | |
| Vascular
invasion | | | 0.003 | | | 0.935 |
| No (n=45) | 114.57 | 91.82–137.31 | | | | |
| Yes (n=6) | 36.97 | 6.17–67.77 | | | | |
| Perineural
invasion | | | 0.002 | | | 0.464 |
| No (n=27) | 132.40 | 106.92–157.88 | | | | |
| Yes (n=24) | 63.63 | 36.68–90.58 | | | | |
| HP infection | | | 0.846 | | | |
| No (n=44) | 101.76 | 79.04–124.47 | | | | |
| Yes (n=7) | 104.29 | 42.14–166.44 | | | | |
Discussion
In the present study, EBVaGC constituted 5.1% of the
cases of stage I–III gastric cancer and was associated with
demographic features that have been described in previous studies.
According to a large-scale meta-analysis of 70 studies including
15,952 cases of gastric cancer, EBVaGC had a prevalence estimate of
8.7% (95% CI 7.5–10.0%, range 1.33–19.9%) (5). The meta-analysis revealed that EBVaGC
presented a 2-fold higher incidence in males (11.1%) than in
females and occurred twice as often in the gastric cardia or corpus
than in the antrum (13.6 or 13.1 vs. 5.2%) compared to EBV-negative
gastric cancers. Stump cancer had a 4-fold higher incidence of EBV
positivity (35.1%). The above results are similar to the finding of
our study, which revealed a male preponderance and a higher
incidence in stump cancer. Regarding the location in the stomach,
EBVaGC seems to occur more frequently in the upper third and less
frequently in the lower third than EBV-negative gastric cancer. No
significant difference was observed in prevalence between the
intestinal, diffuse and mixed tumor types. In addition, the present
study revealed that poorly differentiated carcinoma has a higher
likeliness of EBV positivity. Taiwan is an endemic area for
nasopharyngeal cancer, which is also associated with EBV infection.
The data gathered at our institute indicated that EBVaGC was a rare
(1/6, 16.6%) event of secondary cancer in patients with
nasopharyngeal cancer in Taiwan (19). Furthermore, the incidence of EBVaGC
is similar worldwide, with 8.3% in Asia, 9.2% in Europe and 9.9% in
America (5). EBV-associated gastric
cancer and nasopharyngeal cancer express latency I and latency II
protein, respectively (1,2). EBVaGC may be a universal and distinct
variant of gastric cancer with characteristic clinical features
that are independent from nasopharyngeal cancer.
In addition, our results showed that EBV infection
itself seems not to be a prognostic factor, and risk stratification
by tumor size, histological classification, and LN ratio may help
identify high-risk patients. According to the literature, a
favorable outcome was observed only in those cases categorized as
LELC, and EBV infection itself was not associated with any survival
advantage (10,11,13–15).
Our results also support this prevailing opinion. LELC-type EBVaGC
presents a striking benefit for both the 3- and 5-year survival
rate. This unique histological subtype is distinguished by the
presence of a non-desmoplastic stroma infiltrated with an abundance
of lymphocytes and plasma cells (10,16).
These extensive intratumoral inflammatory components are composed
of activated cytotoxic T, nature killer and mature dendritic cells
(9,15,20).
The T cell infiltration has been correlated to intratumoral
FoxP3-positive regulatory T cells (21). Some authors hypothesized that the
intratumoral inflammatory reaction represents an effective host
immune reaction against tumor cells (9,20,22).
In colon, breast and lung malignancies, tumor-infiltrating
lymphocytes also express a cytotoxic T-cell phenotype and are
related to a survival advantage (22).
Likewise, the intratumoral inflammation pattern and
intensity have been reported to influence the survival of EBVaGC
patients (9,11,22).
Song et al purported that a typical Crohn’s disease-like
lymphocytic reaction may share a similar morphology with LELC on
the basis of the similar survival benefit in both groups (11). Grogg et al found that
increased lymphocyte infiltration of the tumor indicated a better
prognosis as EBVaGC had a higher lymphocyte count (450/10 HPF) than
EBV-negative gastric cancer (21/10 HPF) (22). The amount of intratumoral T and
dendritic cells was also more plentiful in EBVaGC without lymph
node metastasis than in EBVaGC with node metastasis (9). Although the underlying mechanism of
the antitumor immune reaction is not well elucidated, the accurate
classification of EBVaGC into LELC or non-LELC is not only
associated with patient prognosis but also implies a different
tumor-host interaction.
Tumor size has been regarded as an important
prognostic factor due to its close relationship to histological
grade, UICC/AJCC stage, vascular invasion and neural permeation
(23). We observed that a tumor
size >5 cm is an independent parameter of poor prognosis in
stage I–III EBVaGC instead of the depth of tumor invasion. EBVaGC
frequently grows in ulcerated or saucer-like tumors featured by
well-delineated and pushing borders (7,10,16).
This macroscopic pattern corresponds to a microscopic expanding
front rather than to infiltrative invasion. EBVaGC may follow a
different encroachment fashion from EBV-negative gastric cancer.
That may be why tumor size is a powerful predictor. Indeed, tumor
size is a paramount component for UICC/AJCC tumor stage in some
malignancies, including lung and breast cancers (24). For gastric cancer, some authors have
found that tumor size is a simple prognostic indicator and could
even improve the accuracy of UICC/AJCC staging for gastric cancer
(25,26). Due to the heterogeneity of gastric
cancer, tumor size may be a significant outcome indicator in some
subgroups, such as EBVaGC, as shown by the present study.
The LN ratio is an emerging parameter that may be
more useful than UICC/AJCC lymph node stage due to its consistent
prognostic power whenever the type of lymphadenectomy or total
number of resected nodes varies (27–30).
This study suggests that an LN ratio >0.15 is an independent and
powerful predictor that is superior to the UICC/AJCC nodal status
in stage I–III EBVaGC. The mean number of harvested lymph nodes
from the EBVaGC group in our study was 30.5 with 6 cases having a
total of <15 lymph nodes (11.8%) (data not shown). An LN ratio
>0.15 retained its statistical significance in the Cox
regression multivariate analysis and had the strongest hazard ratio
compared with the other factors. Most previous studies have divided
LN ratio into categories corresponding to 0, 1–9, 10–25 and >25%
to stratify patient risk, which is intended to imitate the
AJCC/UICC node status (27,28). Our data demonstrated that a simple
threshold of 0.15 could achieve considerable discernability for
patient outcome. Metastatic foci of EBVaGC in lymph nodes still
maintain an EBV genome (9). The
occurrence of node metastasis does not signify tumor escape by
virus deletion, but it may imply alteration of the tumor to lose
the target antigen or to attenuate the immune defense. Indeed, a
better prognosis observed in EBVaGC has been attributed to less
lymph node involvement (12). The
relationship between tumor molecular alteration and lymph node
metastasis still requires further study, but the LN ratio may be
used as another simple approach to predict this host-tumor
interaction and its effect on patient outcome.
EBV is thought to play a critical role, not only in
stimulation of an immunologic reaction, but also in gastric
carcinogenesis. Through the presentation of an undefined antigen,
EBV attracts strikingly numerous lymphocytes and plasma cells that
are intimately admixed with tumor cells by upregulation of major
histocompatibility complex class II molecules and IL1-β cytokines
(9,31). Aside from the differences in protein
expression and chromosomal aberrations compared with EBV-negative
counterparts, EBVaGC exhibits characteristic molecular features,
including a global and non-random CpG island methylation
epigenotype, which is activated by DNMT1 through the
phosphorylation of STAT3 from viral LMP2A effect (7,32–36).
Considering the unique host-tumor interaction and the molecular
alterations detected in EBVaGC, our data suggest that the use of
the histological classification, tumor size, and LN ratio could
discriminate the prognosis of patients with stage I–III EBVaGC. For
therapeutic options that utilize virus-host interactions in
EBV-associated tumors, demethylating agents, such as 5-azacytidine,
can induce lytic infection of EBV, leading to lysis of the infected
tumor cells, by restoring the expression of the BMRF1, BZLF1 and
BRLF1 genes after removing promoter methylation (37,38).
These novel antitumor drugs may provide a maximal survival benefit
to those high-risk patients with a large tumor size, non-LELC
tumors or a high LN ratio.
It is important to characterize the tumor pathway
and processes for personalized medicine. The present study is one
of our serial investigations aimed at the molecular classification
of gastric cancers. EBVaGC and HER-2-overexpressing gastric cancers
may represent distinct subsets since only one EBVaGC case had HER-2
overexpression. The incidence of 1.9% was much lower than that of
6.1% in the general population of gastric cancer, as demonstrated
in our previous study (39). In
addition, the low incidence of HER2 amplification is also
consistent with the results reported by a Korean group (1/123,
0.8%) (11).
In conclusion, we conducted a large-scale study
involving 1,020 stage I–III gastric cancer cases from a single
institute. We identified 52 cases of EBVaGC. EBVaGC showed a male
preponderance and a higher incidence in stump cancer and poorly
differentiated carcinoma. The survival analysis suggested that
tumor size, LELC classification, and LN ratio were important
prognostic factor. These influential factors most likely reflect
EBVaGC’s unique mode of carcinogenesis and host-tumor interaction
and should be considered in the identification of high-risk
patients who may benefit from adjuvant regimens or virus-specific
treatments.
Acknowledgements
We thank the Tissue Bank, Chang Gung Memorial
Hospital, for excellent tissue processing. This study was supported
by a grant from the Department of Health (DOH99-TD-C-111-006), a
grant from the National Science Council (101-2320-B-182A-008), and
a grant from the Chang Gung Memorial Hospital (CMRPG340547,
CMRPG3B1192 and CMRPG3A1182).
References
|
1
|
Young LS and Rickinson AB: Epstein-Barr
virus: 40 years on. Nat Rev Cancer. 4:757–768. 2004.PubMed/NCBI
|
|
2
|
Deyrup AT: Epstein-Barr virus-associated
epithelial and mesenchymal neoplasms. Hum Pathol. 39:473–483. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Shibata D and Weiss LM: Epstein-Barr
virus-associated gastric adenocarcinoma. Am J Pathol. 140:769–774.
1992.PubMed/NCBI
|
|
4
|
Tokunaga M, Land CE, Uemura Y, Tokudome T,
Tanaka S and Sato E: Epstein-Barr virus in gastric carcinoma. Am J
Pathol. 143:1250–1254. 1993.PubMed/NCBI
|
|
5
|
Murphy G, Pfeiffer R, Camargo MC and
Rabkin CS: Meta-analysis shows that prevalence of Epstein-Barr
virus-positive gastric cancer differs based on sex and anatomic
location. Gastroenterology. 137:824–833. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Parkin DM, Bray F, Ferlay J and Pisani P:
Global cancer statistics, 2002. CA Cancer J Clin. 55:74–108. 2005.
View Article : Google Scholar
|
|
7
|
Fukayama M and Ushiku T: Epstein-Barr
virus-associated gastric carcinoma. Pathol Res Pract. 207:529–537.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tokunaga M, Uemura Y, Tokudome T, et al:
Epstein-Barr virus related gastric cancer in Japan: a molecular
patho-epidemiological study. Acta Pathol Jpn. 43:574–581.
1993.PubMed/NCBI
|
|
9
|
van Beek J, zur Hausen A, Snel SN, et al:
Morphological evidence of an activated cytotoxic T-cell infiltrate
in EBV-positive gastric carcinoma preventing lymph node metastases.
Am J Surg Pathol. 30:59–65. 2006.PubMed/NCBI
|
|
10
|
Watanabe H, Enjoji M and Imai T: Gastric
carcinoma with lymphoid stroma. Its morphologic characteristics and
prognostic correlations. Cancer. 38:232–243. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Song HJ, Srivastava A, Lee J, et al: Host
inflammatory response predicts survival of patients with
Epstein-Barr virus-associated gastric carcinoma. Gastroenterology.
139:84–92. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
van Beek J, zur Hausen A, Klein Kranenbarg
E, et al: EBV-positive gastric adenocarcinomas: a distinct
clinicopathologic entity with a low frequency of lymph node
involvement. J Clin Oncol. 22:664–670. 2004.PubMed/NCBI
|
|
13
|
Park ES, Do IG, Park CK, et al:
Cyclooxygenase-2 is an independent prognostic factor in gastric
carcinoma patients receiving adjuvant chemotherapy and is not
associated with EBV infection. Clin Cancer Res. 15:291–298. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Chang MS, Lee HS, Kim CW, Kim YI and Kim
WH: Clinicopathologic characteristics of Epstein-Barr
virus-incorporated gastric cancers in Korea. Pathol Res Pract.
197:395–400. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kijima Y, Ishigami S, Hokita S, Koriyama
C, Akiba S, Eizuru Y and Aikou T: The comparison of the prognosis
between Epstein-Barr virus (EBV)-positive gastric carcinomas and
EBV-negative ones. Cancer Lett. 200:33–40. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Shibata D, Tokunaga M, Uemura Y, Sato E,
Tanaka S and Weiss LM: Association of Epstein-Barr virus with
undifferentiated gastric carcinomas with intense lymphoid
infiltration. Lymphoepithelioma-like carcinoma. Am J Pathol.
139:469–474. 1991.PubMed/NCBI
|
|
17
|
Lauwers GY, Carneiro F, Graham DY, et al:
Gastric carcinoma. WHO Classification of Tumours of the Digestive
System. Bosman FT, Carneiro F, Hruban RH and Theise ND: IARC; Lyon:
pp. 48–58. 2010
|
|
18
|
Hofmann M, Stoss O, Shi D, et al:
Assessment of a HER2 scoring system for gastric cancer: results
from a validation study. Histopathology. 52:797–805. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wang CC, Chen ML, Hsu KH, et al: Second
malignant tumors in patients with nasopharyngeal carcinoma and
their association with Epstein-Barr virus. Int J Cancer.
87:228–231. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Minamoto T, Mai M, Watanabe K, et al:
Medullary carcinoma with lymphocytic infiltration of the stomach.
Clinicopathologic study of 27 cases and immunohistochemical
analysis of the subpopulations of infiltrating lymphocytes in the
tumor. Cancer. 66:945–952. 1990. View Article : Google Scholar
|
|
21
|
Haas M, Büttner M, Rau TT, Fietkau R,
Grabenbauer GG and Distel LV: Inflammation in gastric
adenocarcinoma of the cardia: how do EBV infection, Her2
amplification and cancer progression influence tumor-infiltrating
lymphocytes? Virchows Arch. 458:403–411. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Grogg KL, Lohse CM, Pankratz VS, Halling
KC and Smyrk TC: Lymphocyte-rich gastric cancer: associations with
Epstein-Barr virus, microsatellite instability, histology, and
survival. Mod Pathol. 16:641–651. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yokota T, Ishiyama S, Saito T, et al: Is
tumor size a prognostic indicator for gastric carcinoma? Anticancer
Res. 22:3673–3677. 2002.PubMed/NCBI
|
|
24
|
Edge SB, Byrd DR, Compton CC, Fritz AG, et
al: AJCC Cancer Staging Manual. 7th edition. Springer; New York,
NY: pp. 117–126. 2010
|
|
25
|
Saito H, Osaki T, Murakami D, et al:
Macroscopic tumor size as a simple prognostic indicator in patients
with gastric cancer. Am J Surg. 192:296–300. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lu J, Huang CM, Zheng CH, Li P, Xie JW,
Wang JB and Lin JX: Consideration of tumor size improves the
accuracy of TNM predictions in patients with gastric cancer after
curative gastrectomy. Surg Oncol. 22:167–171. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Xu DZ, Geng QR, Long ZJ, et al: Positive
lymph node ratio is an independent prognostic factor in gastric
cancer after d2 resection regardless of the examined number of
lymph nodes. Ann Surg Oncol. 16:319–326. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Marchet A, Mocellin S, Ambrosi A, et al:
The ratio between metastatic and examined lymph nodes (N ratio) is
an independent prognostic factor in gastric cancer regardless of
the type of lymphadenectomy: results from an Italian multicentric
study in 1853 patients. Ann Surg. 245:543–552. 2007. View Article : Google Scholar
|
|
29
|
Persiani R, Rausei S, Antonacci V, Biondi
A, Casella F, Ciccoritti L and D’Ugo D: Metastatic lymph node
ratio: a new staging system for gastric cancer. World J Surg.
33:2106–2111. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Inoue K, Nakane Y, Iiyama H, et al: The
superiority of ratio-based lymph node staging in gastric carcinoma.
Ann Surg Oncol. 9:27–34. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Chong JM, Sakuma K, Sudo M, et al:
Interleukin-1β expression in human gastric carcinoma with
Epstein-Barr virus infection. J Virol. 76:6825–6831. 2002.
|
|
32
|
Lee HS, Chang MS, Yang HK, Lee BL and Kim
WH: Epstein-barr virus-positive gastric carcinoma has a distinct
protein expression profile in comparison with Epstein-barr
virus-negative carcinoma. Clin Cancer Res. 10:1698–1705. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
zur Hausen A, van Grieken NC, Meijer GA,
et al: Distinct chromosomal aberrations in Epstein-Barr
virus-carrying gastric carcinomas tested by comparative genomic
hybridization. Gastroenterology. 121:612–618. 2001.PubMed/NCBI
|
|
34
|
Chang MS, Uozaki H, Chong JM, et al: CpG
island methylation status in gastric carcinoma with and without
infection of Epstein-Barr virus. Clin Cancer Res. 12:2995–3002.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Chong JM, Sakuma K, Sudo M, et al: Global
and non-random CpG-island methylation in gastric carcinoma
associated with Epstein-Barr virus. Cancer Sci. 94:76–80. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Hino R, Uozaki H, Murakami N, et al:
Activation of DNA methyltransferase 1 by EBV latent membrane
protein 2A leads to promoter hypermethylation of PTEN gene
in gastric carcinoma. Cancer Res. 69:2766–2774. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Fu DX, Tanhehco Y, Chen J, et al:
Bortezomib-induced enzyme-targeted radiation therapy in
herpesvirus-associated tumors. Nat Med. 14:1118–1122. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Jung EJ, Lee YM, Lee BL, Chang MS and Kim
WH: Lytic induction and apoptosis of Epstein-Barr virus-associated
gastric cancer cell line with epigenetic modifiers and ganciclovir.
Cancer Lett. 247:77–83. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Hsu JT, Chen TC, Tseng JH, et al: Impact
of HER-2 overexpression/amplification on the prognosis of gastric
cancer patients undergoing resection: a single-center study of
1,036 patients. Oncologist. 16:1706–1713. 2011. View Article : Google Scholar : PubMed/NCBI
|