Introduction
Hepatocellular carcinoma (HCC), the fifth most
common cancer worldwide, is not only a highly aggressive carcinoma
of the liver but is also the third leading cause of cancer-related
mortality (1). Hepatitis B virus,
hepatitis C virus, and chronic heavy alcohol consumption leading to
liver cirrhosis remain the most important causes (2). Few target molecules have been
identified that enable the diagnosis of HCC with a high sensitivity
and specificity, particularly in the early clinical stages of HCC.
Currently α-fetoprotein (AFP) is widely used as a surveillance and
detection test for HCC, despite its limited performance,
particularly in early-stage HCC (3). Other molecular markers, for example,
lectin-bound AFP (4), glypican-3
(5) and des-γ carboxyprothrombin
(6) have been proposed for HCC
detection. However, an ideal marker for HCC diagnosis and prognosis
has not yet been identified. Development of novel biomarkers for
the early diagnosis and prognosis of HCC is vital.
Our previous studies demonstrated that cancer serum
contains antibodies that react with a unique group of autologous
cellular antigens called tumor-associated antigens (TAAs), whose
abnormal regulation or excessive expression are closely related to
carcinogenesis (7,8). The TAAs in blood circulation rapidly
degrade, and their use in early cancer diagnosis has been hampered
by false-positive rates in the normal population. In contrast,
autoantibodies can identify aberrant cellular antigens in
carcinogenesis and serve as markers for cancer detection and
surveillance since anti-TAA autoantibodies are more stable
(9). Furthermore, the absence of
these autoantibodies in normal individuals and non-cancer
conditions makes them potential markers for different types of
cancer (7). For example, p62, a
fetal protein absent in adult tissues, is recognized as a TAA. The
anti-p62 autoantibodies were found to be positive in 21% of HCC
patients but negative in controls (10).
Osteopontin (OPN) is a secreted phosphorylated and
glycosylated protein, which is expressed widely and has multiple
functions in cell adhesion and migration (11), antiapoptosis (12), immune and inflammatory responses
(13,14), calcification (15) and suppression of nitric oxide
synthase (16). In addition, it is
also known as secreted phosphoprotein 1 (SPP1). In normal liver
tissue, OPN is expressed in bile duct epithelium, stellate cells,
and Kupffer cells but not in normal hepatocytes (17). Recent studies have confirmed that
OPN plays an important role in carcinogenesis and metastasis
(18,19). In many types of cancer, including
breast (20), lung (21), colon (22) and kidney cancer (23) elevated expression of OPN was found
to be associated with carcinogenesis, progression, metastasis and
poor prognosis. Other studies further found elevated expression
levels of serum OPN in HCC compared to liver cirrhosis (LC),
chronic hepatitis (CH) and normal human serum (NHS) groups
(24,25). However, little is known concerning
the role of the autoantibody against OPN in HCC and its
relationship with the prognosis of HCC patients.
In the present study, the autoantibody response to
OPN in HCC and control groups was analyzed by enzyme-linked
immunosorbent assay (ELISA) and indirect immunofluorescence assay.
Immunohistochemistry (IHC) with an HCC tissue array was also
investigated to understand OPN protein expression profiles. In
addition, the relationship between OPN expression and overall
survival (OS) of HCC patients was analyzed to investigated the role
of OPN in the prognosis of HCC patients.
Materials and methods
Serum samples from 148 HCC patients, 32 patients
with CH, 32 patients with LC, and 75 normal controls were collected
at The First Affiliated Hospital of Xi’an Jiaotong University
(China) from 2011 to 2013. This study was approved by the Ethics
Committee of The First Affiliated Hospital of Xi’an Jiaotong
University. All HCC serum samples (n=148) had been collected before
patients were treated with chemotherapy, radiotherapy or surgery,
and were pathologically confirmed. The normal controls were
negative for the hepatitis virus and had no evidence of malignancy.
All blood samples were collected in vacuum tubes, clotted at room
temperature for 30 min, and then centrifuged at 3,000 rpm for 5
min. The suspension was distributed into 300-μl aliquots each and
stored at −80°C until analysis. The general information for these
patients was available (Table I),
and AFP levels of 140 of the 148 HCC serum samples were assessed by
ELISA assay.
 | Table ICharacteristics of the patients for
ELISA assay. |
Table I
Characteristics of the patients for
ELISA assay.
| Group | Male/Female | Age range
(years) | Mean age
(years) | Viral
infection |
|---|
|
|---|
| HBV | HCV | HBV+HCV | No virus |
|---|
| NHS | 52/23 | 16–82 | 51.41 | 0 | 0 | 0 | 75 |
| LC | 28/4 | 27–65 | 45.91 | 27 | 3 | 0 | 2 |
| CH | 17/15 | 34–73 | 49.09 | 21 | 10 | 1 | 0 |
| HCC | 123/25 | 14–78 | 52.95 | 127 | 8 | 1 | 12 |
Indirect enzyme-linked immunosorbent
assay (ELISA)
Microtiter plates (96-well; Corning, NY, USA) were
coated overnight at 4°C with 100 μl/well recombinant osteopontin
protein (R&D, Minneapolis, MN, USA) at a final concentration of
1.0 μg/ml in phosphate-buffered saline (PBS). Then the plates were
blocked with 1% bovine serum albumin (BSA) in PBS, 300 μl/well, for
2 h at room temperature with gentle shaking. Following 4-time
washes with PBST (0.1% Tween-20 in PBS), 100 μl/well diluted human
serum (1:50) in 1% BSA/PBS was incubated for 2 h at room
temperature in the antigen-coated wells with gentle shaking. Plates
were washed 4 times again followed by 100 μl/well of HRP-conjugated
goat antihuman IgG (1:4000 diluted) for 1 h. After 4 washes, 100
μl/well of tetramethylbenzidine (TMB) was added and the reaction
was stopped by adding 50 μl 2 M sulphuric acid
(H2SO4). The optical density (OD) of each
well was read at a wavelength of 405 nm, and the mean OD of 75
NHS+3SD was designated as a cutoff value for a positive
reaction.
Cell lines and cell extracts
Ten different cancer cell lines, human
hepatocellular carcinoma cell lines (HepG2 and Hep3B), human breast
cancer cell lines (MCF-7 and MDA-MB-453), human cervical cancer
cell lines (HeLa and SiHa), human colorectal cancer cell line
(HCT116), non-small cell lung cancer cell line (H1299), prostate
cancer cell line (C42), and human epidermal carcinoma cell line
(A431), were obtained from the Department of Transformation Medical
Center of Xi’an Jiaotong University. Cancer cells were solubilized
in extraction buffer supplemented with the protease inhibitor
cocktail.
Western blotting
Cancer cell lysates were electrophoresed on 12%
SDS-PAGE and transferred to polyvinylidene fluoride (PVDF)
membranes. The membranes were blocked with 5% non-fat milk in
Tris-buffered saline (TBS) at 37°C for 3 h and then incubated
overnight at 4°C with a 1:1,000 dilution of the rabbit monoclonal
anti-SPP1 antibody (Epitomics, Burlingame, CA, USA) and a 1:5,000
dilution of the mouse monoclonal anti-β-actin antibody
(Sigma-Aldrich, St. Louis, MO, USA). HRP-conjugated goat
anti-rabbit IgG and HRP-conjugated goat anti-mouse IgG (both at
1:2,000; Abcam Inc, Cambridge, MA, USA) were used as secondary
antibodies. An enhanced chemiluminescence kit (Millipore
Corporation, Billerica, MA, USA) was used to detect the
immunoreactive bands.
Absorption of antibodies with recombinant
protein
The serum was incubated with recombinant OPN protein
(the final concentration of the protein diluted with HCC serum was
0.01 μg/μl) overnight at 4°C, and then centrifuged at 10,000 ×
g for 15 min. The supernatant was the pre-absorbed serum
used for the immunofluorescence assay.
Indirect immunofluorescence assay
(IIFA)
HeLa cells (2×104 cells/ml) were cultured
in 12-well plates, after 24 h, serum (1:1) and pre-absorbed serum
(1:1) were incubated with these HeLa antigen substrates overnight
at 4°C. FITC-conjugated goat anti-human IgG (Protein Tech Group,
Inc., Chicago, IL, USA) was used as the secondary antibody at a
1:20 dilution. Fluorescence microscope (Leica DM1000, Germany) was
used for examination.
Immunohistochemical (IHC) analysis of the
tissue assay slides
HCC tissue array slides (including 90 HCC tissue
specimens) with information regarding clinicopathological
characteristics comprising age, gender, clinical stage, pathology
grade, and prognosis information were commercially purchased (Outdo
Biotech Co., Ltd., Shanghai, China). This tissue assay was used to
detect the expression of OPN in HCC specimens and identify the
relevant prognostic factors. The protocol for IHC was carried out
as previously described (26). The
primary antibody was rabbit monoclonal anti-SPP1 antibody (1:120
dilution; Epitomics).
Three independent pathologists evaluated and scored
the IHC staining. Scoring of cytoplasmic OPN staining was based on
both the staining intensity and extent according to a previous
report (27). Microscopically, each
section was observed randomly in 10 high-power fields (x40
magnification), each of which included 100 cells. First, the
staining extent was scored according to the proportion of positive
tumor cells: 0, 0%; 1, 1–25%; 2, 26–50%; 3, 51–75%; and 4, 76–100%.
Second, the staining intensity was scored: 0, no cell staining; 1,
weak staining; 2, moderate staining; 3, strong staining. Finally,
scores were calculated by multiplying the intensity and extent
scores and the results were divided as follows: negative (‘I’,
score: 0–1), weak positive (‘II’, score: 2–4), moderate positive
(‘III’, score: 5–8) and strong positive (‘IV’, score: 9–12).
Staining results were also divided into negative expression and
positive expression for further study.
Statistical analysis
We adopted SPSS version 18.0 (SPSS Inc., Chicago,
IL, USA) for Windows to analyze the data. The mean OD value of each
group was compared using the Mann-Whitney U test and the frequency
of the autoantibody to OPN in each group of patient serum was
compared by means of the χ2 test with Fisher’s exact
test. Comparison of the clinicopathological parameters with OPN
expression was conducted by the two-tailed Mann-Whitney U test. The
survival curve was estimated using the Kaplan-Meier method, and the
prognostic significance of these markers was analyzed by log-rank
test. Univariate and multivariate Cox regression analyses were
performed to analyze the relevant prognostic factors. Two-tailed
P-values <0.05 were considered to indicate statistically
significant differences.
Results
Frequency and titer of the autoantibodies
against OPN in HCC, LC, CH and NHS groups
Recombinant human OPN protein was used in ELISA as a
coated antigen with which to detect autoantibodies against OPN in
serum samples from 148 HCC patients, 32 CH patients, 32 LC patients
and 75 healthy individuals. The mean titer of the autoantibodies
against serum OPN in the NHS group was 0.768±0.266, the mean + 3SD
of the NHS samples (1.566) was used as a cutoff value. Table II shows that the prevalence of
autoantibodies against OPN was 12.8% (19/148) in HCC, 15.6% (5/32)
in LC, 3.1% (1/32) in CH and 0% (0/75) in the NHS group. Compared
with these 4 groups, the prevalence of anti-OPN autoantibodies in
the HCC (P=0.001) and LC (P=0.002) group was significantly higher
than that in the NHS groups. As shown in Fig. 1, the titer of the autoantibodies
against OPN in the 4 groups was different (P=0.001). The titer in
the HCC and LC groups was higher than that in the NHS group (both
P=0.000). The average titer of the anti-OPN autoantibodies was
1.015±0.502, 1.087±0.498, 0.902±0.328 and 0.768±0.266 in the HCC,
LC, CH, and NHS group, respectively. In fact, of the 148 HCC
patients, 140 patients were tested for both AFP and anti-OPN
autoantibody levels by ELISA. The AFP level in 84 (60%) HCC
patients was >100 ng/ml, whereas in 75 (53.6%) HCC patients the
level was >200 ng/ml. When both AFP and anti- OPN autoantibody
were used simultaneously as biomarkers, 91 (65%) HCC patients (AFP
>100 ng/ml) were positive, and 83 (59.3%) HCC patients (AFP
>200 ng/ml) were positive, respectively.
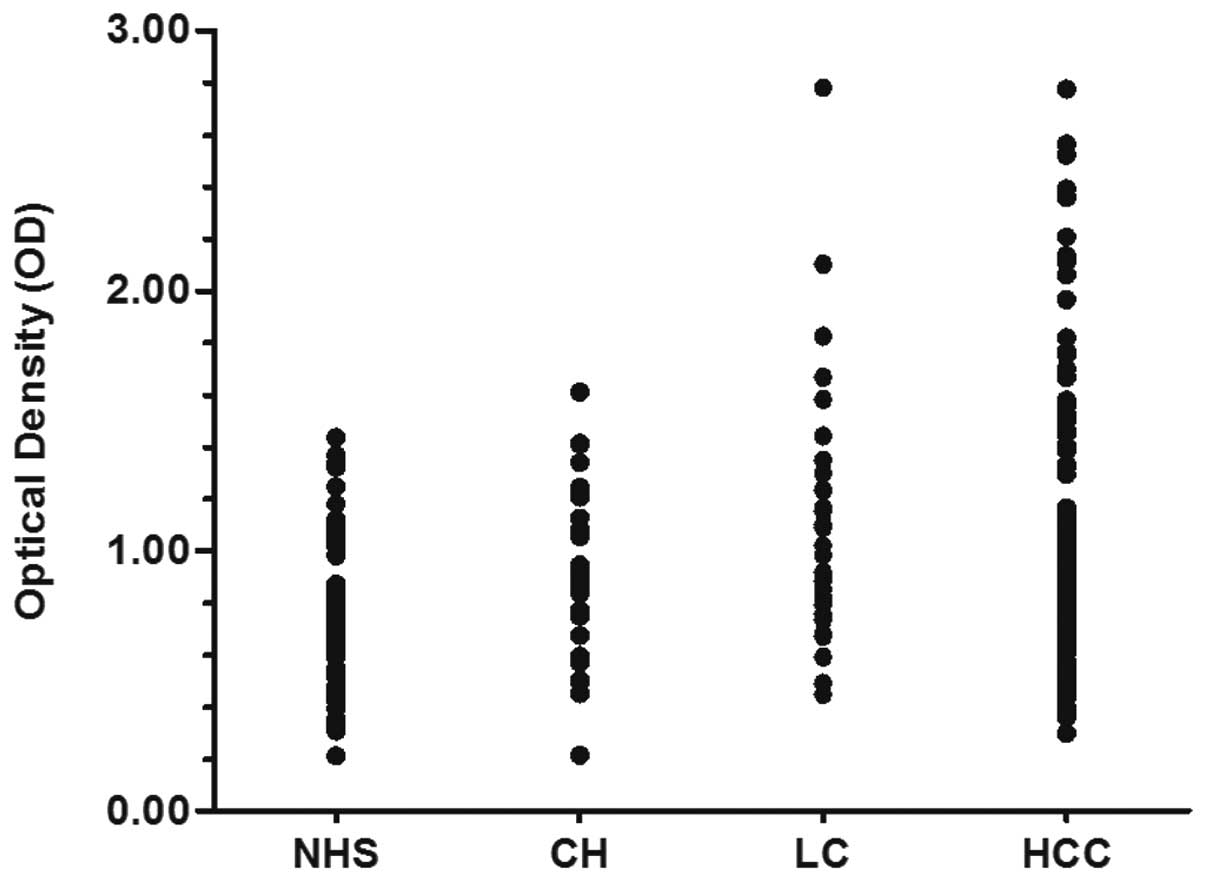 | Figure 1Titer of anti-OPN autoantibodies in
human serum samples by ELISA. The range of antibody titers to OPN
was expressed as optical density (OD) obtained from ELISA. The mean
titer of NHS, CH, LC and HCC was 0.768, 0.902, 1.087 and 1.02,
respectively. The mean + 3SD of the NHS samples was used as a
cutoff value. Titer of anti-OPN in LC and HCC was much higher than
that in the NHS group (P<0.001). OPN, osteopontin; NHS, normal
human serum; CH, chronic hepatitis; LC, liver cirrhosis; HCC,
hepatocellular carcinoma. |
| Table IIFrequency of the autoantibody against
OPN in human serum samples by ELISA. |
Table II
Frequency of the autoantibody against
OPN in human serum samples by ELISA.
| Type of serum | No. tested | Autoantibody to
OPN, n (%) |
|---|
| HCC | 148 | 19 (12.8)b |
| LC | 32 | 5 (15.6)a |
| CH | 32 | 1 (3.1) |
| NHS | 75 | 0 (0.0) |
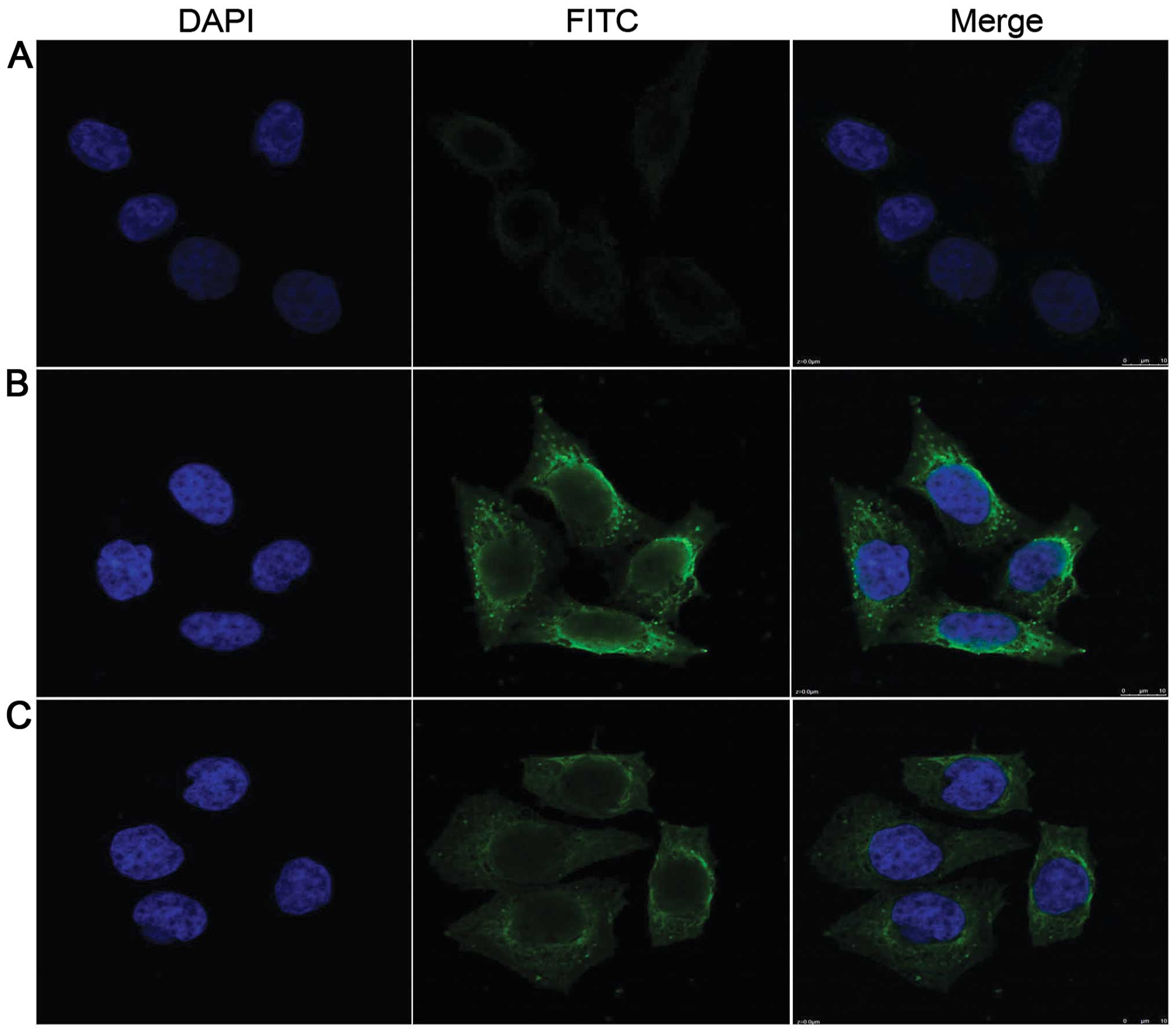
Perinuclear intense staining pattern
detected in HeLa cells by indirect immunofluorescence assay with
representative positive HCC serum
Indirect immunofluorescence was used to confirm the
reactivity of OPN autoantibodies in HCC serum samples and the
intracellular location of OPN. In this assay, HeLa cell slides and
HCC serum samples with anti-OPN-positive expression in ELISA were
selected. As shown in Fig. 2, HCC
serum samples with anti-OPN-positive expression had a perinuclear
staining pattern. When the same HCC serum samples were pre-absorbed
by recombinant OPN protein, the fluorescent staining was
significantly reduced.
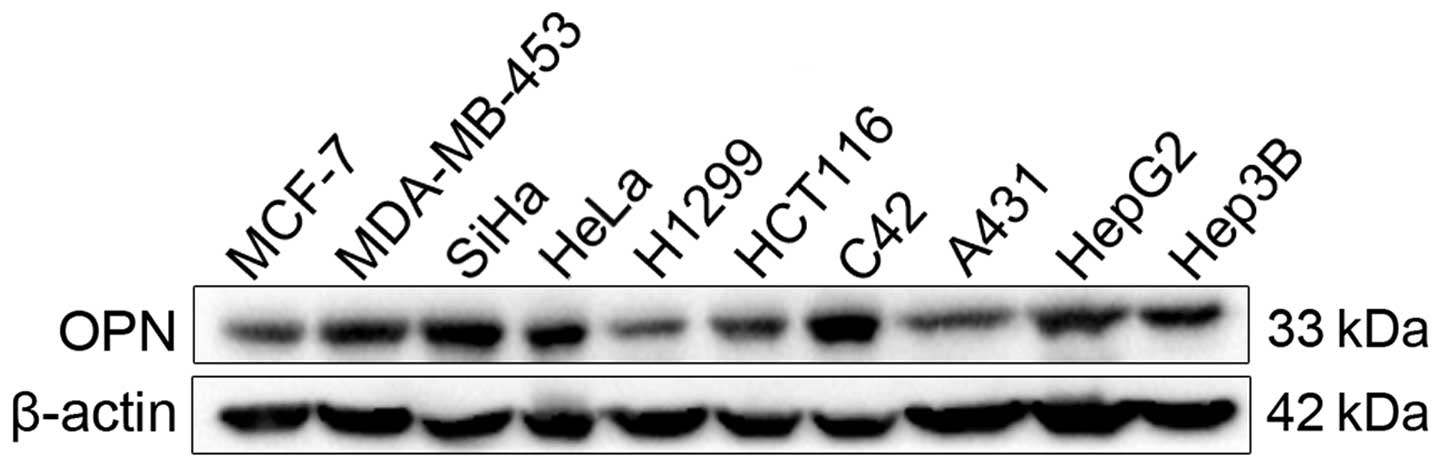
OPN expression in the different cancer
cell lines
OPN contributes to carcinogenesis and metastasis. To
determine the expression levels of OPN protein in different tumor
cell lines, 10 tumor cell lines (MCF-7, MDA-MB-453, SiHa, HeLa,
H1299, HCT116, C42, A431, HepG2, Hep3B) were cultured, and analyzed
by western blotting. As shown in Fig.
3, MCF-7, H1299, HCT116 and A431 cancer cell lines showed
relatively weaker reactive bands compared to those cell lines that
had strong reactivity such as MDA-MB-453, SiHa, HeLa, C42, HepG2
and Hep3B.
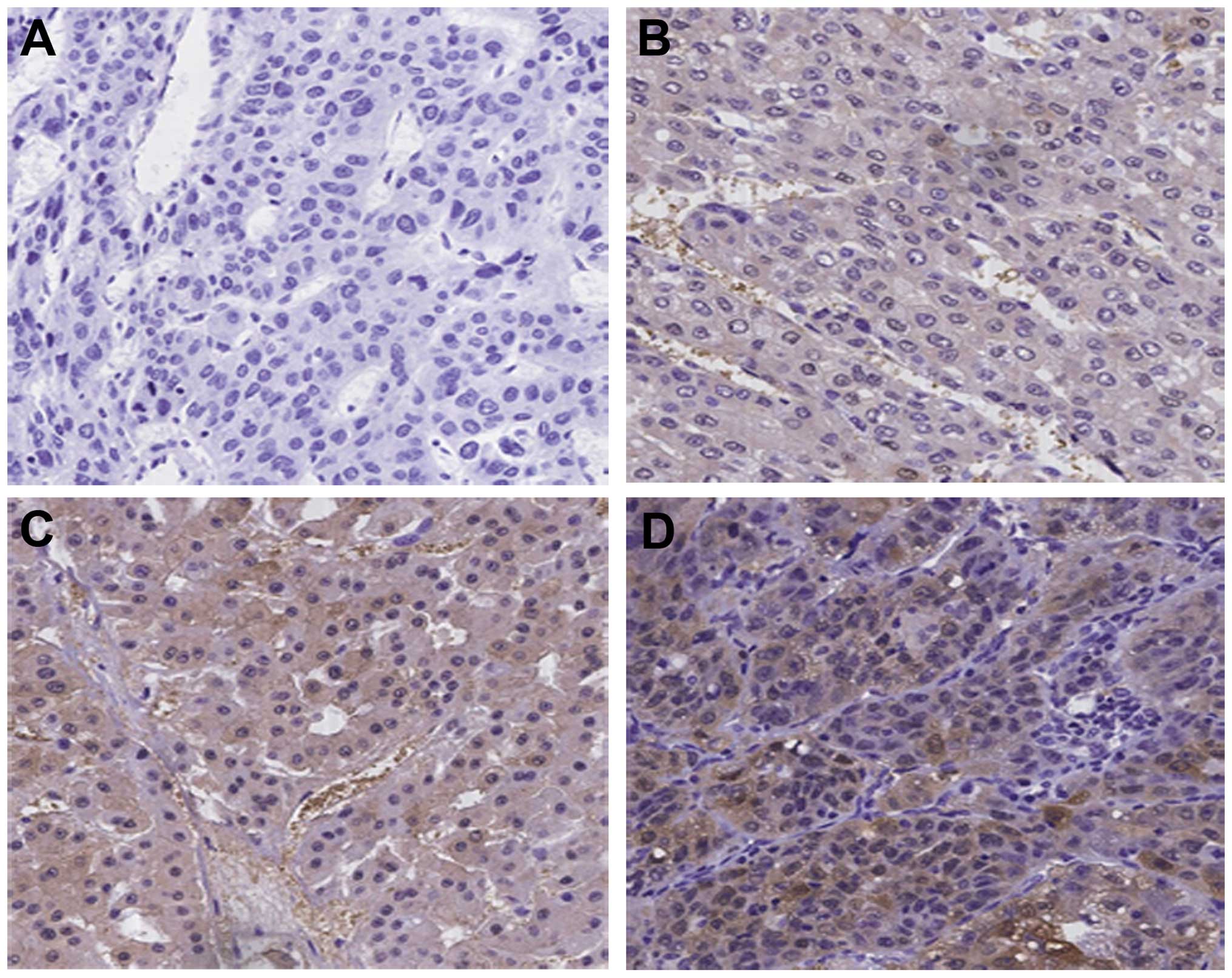
Expression of OPN in hepatocellular
carcinoma tissues
Expression of OPN protein in the HCC tissues was
examined by immunohistochemistry with tissue array slides. The
monoclonal anti-OPN antibody was used as a primary antibody to
detect the expression of OPN. The expression of OPN showed no
correlation with clinical and pathological characteristics such as
age, gender, tumor size, histological grade, capsular infiltration
and portal vein invasion (P<0.05). The patients included 77
males and 13 females, with a mean age of 54.51±9.49 years (range
18–73 years). The expression of OPN protein in the HCC tissues is
shown in Fig. 4. Of the total 90
HCC specimens, 59 HCC samples (65.6%) were positive for OPN
staining and OPN-positive staining was observed in the cytoplasm of
the cancer cells. However, there was no significant correlation
between patient age, gender, tumor size, tumor differentiation
grade and OPN expression.
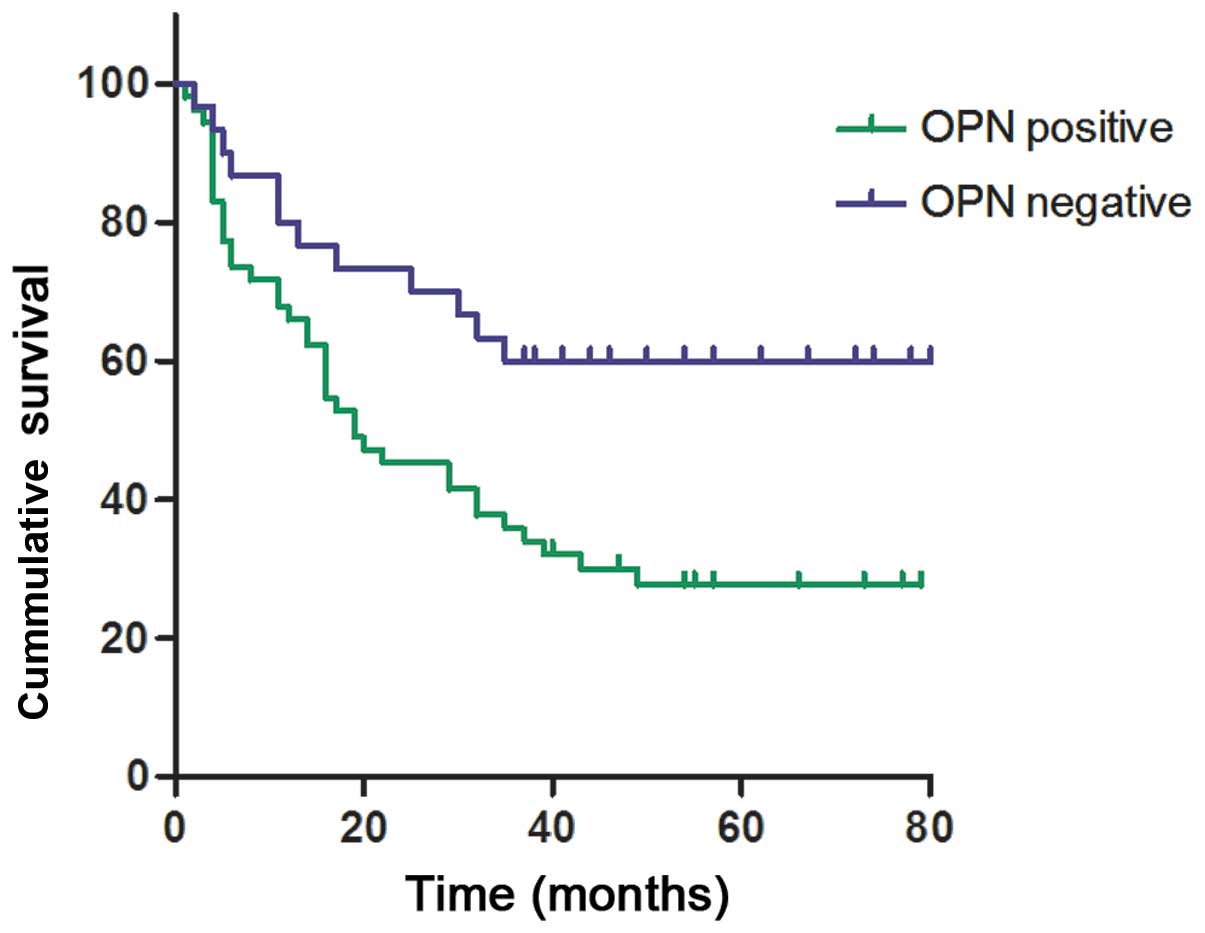
Furthermore, the HCC patients of the tissue array
slides were followed up over the course of 3–7 years (7 patients
were lost to follow-up). At the end of the follow-up period, 33 HCC
patients were alive and 50 HCC patients were deceased. We further
analyzed the relationship between OPN expression and overall
survival (OS) of the HCC patients. Mean OS was 39.37±23.48 months
in the HCC patients with negative OPN expression. In contrast, mean
OS in the patients with positive OPN expression was 28.81±24.22
months. OPN expression was significantly correlated with OS of the
HCC patients (Table III).
Kaplan-Meier curve and log-rank test showed that HCC patients with
positive OPN expression had shorter OS than those with negative OPN
expression (P<0.01) (Fig. 5).
Overexpression of OPN in HCC is an independent prognostic factor
for OS of these HCC patients. Cox multivariate analysis showed that
OPN-positive expression and tumor size were prognostic factors
(Table IV), and the hazard ratio
of OPN expression was 2.099 (95% CI 1.086–4.059; P=0.02).
Collectively, these data indicate that HCC patients with
OPN-positive expression have a poor prognosis.
| Table IIIUnivariate analysis of the
associations between prognostic variables and overall survival in
the HCC patients. |
Table III
Univariate analysis of the
associations between prognostic variables and overall survival in
the HCC patients.
| Markers | n | P-value (OS) |
|---|
| Age (years) | | 0.893 |
| ≤55 | 45 | |
| >55 | 38 | |
| Gender | | 0.367 |
| Male | 70 | |
| Female | 13 | |
| Tumor size
(cm) | | 0.012 |
| ≤5 | 35 | |
| >5 | 47 | |
| Histological
grade | | 0.432 |
| I–II | 52 | |
| III | 31 | |
| Capsular
infiltration | | 0.035 |
| With | 2 | |
| Without | 81 | |
| Portal vein
invasion | | 0.016 |
| With | 6 | |
| Without | 77 | |
| Lymph node
metastasis | | 0.257 |
| With | 1 | |
| Without | 82 | |
| OPN | | 0.009 |
| Positive | 53 | |
| Negative | 30 | |
| Table IVMultivariate analysis of overall
survival according to the Cox model. |
Table IV
Multivariate analysis of overall
survival according to the Cox model.
| | | | 95% CI for
Exp(B) | | |
|---|
| | | |
| | |
|---|
| Factors | B | S.E. | Exp(B) | Lower | Upper | Wald | P-value |
|---|
| OPN | 0.742 | 0.336 | 2.099 | 1.086 | 4.059 | 4.859 | 0.020 |
| Tumor size | 0.049 | 0.020 | 1.050 | 1.009 | 1.093 | 5.675 | 0.028 |
Discussion
OPN is an arginine-glycine-aspartate
(RGD)-containing acidic member of the small integrin-binding ligand
N-linked glycoprotein (SIBLING) family of proteins. Various tissues
including brain, liver, lung, bone, kidney can produce this
protein, and it can be detected in different fluids, for example,
blood, urine, milk and seminal fluid (28). Previous studies found that OPN can
be produced by activated lymphocytes and macrophages as an early
T-cell activation factor and plays a role as a cytokine (29,30).
OPN is also a protein with diverse functions due to its different
functional domains, such as calcium-binding domain, aspartate-rich
domain, heparin-binding domain, thrombin cleavage site, α9β1/α4β1
domain as well as an integrin-binding RGD motif (31). The multifunction OPN has been
revealed in promoting tumor formation and prognosis. It exerts
these functions through direct binding to integrin and/or CD44, and
the subsequent activation of various pathways leads to an increased
malignant phenotype (32). Other
studies have also reported the related signaling pathways and
mechanisms of OPN. For example, OPN protein can trigger the
mitogen-activated protein kinase pathway (MAPK) to promote tumor
growth and matastasis, while the effect can be reversed through the
knockdown of OPN expression (33).
OPN can also induce NF-κB activity through phosphorylation and
degradation of IκBα by activating IKK that ultimately triggers the
activation of pro-MMP-2 (34).
OPN is an attractive potential tumor marker, since
it functions not only as an immobilized extracellular matrix
molecule but also as a secreted form in body fluids including
serum. Previous studies have demonstrated that OPN is overexpressed
with invasion and metastasis in a wide variety of human
malignancies including HCC (20,21,24).
The role of OPN in cancer has recently attracted attention. Our
study showed that OPN was expressed at a higher level in
MDA-MB-453, SiHa, HeLa, C42, HepG2 and Hep3B cell lines, while
expressed relatively weaker in MCF-7, H1299, HCT116 and A431 cell
lines. In addition, an immunohistochemistry assay was further used
to detect the OPN protein expression profiles. Most importantly,
the data showed that the OS of HCC patients with OPN-positive
expression was 28.81±24.22 months which was significantly shorter
than 39.37±23.48 months of HCC patients with OPN-negative
expression. Furthermore, multivariate analysis showed that OPN
overexpression was the strongest independent adverse prognostic
factor for OS. Taken together, these results suggest that
overexpression of OPN in HCC is related to poor prognosis of HCC
patients, which is consistent with the findings of previous
studies. Collectively, OPN may be considered as an independent
prognostic marker of HCC. Further studies have found that OPN is
related to capsular infiltration and portal vein invasion (25,27).
Yet, our study did not find a relationship due to the limited
pathological information or the small sample size.
However, the role of anti-OPN autoantibody levels in
HCC patients is not clearly known although elevated anti-OPN
autoantibodies have been detected in prostate cancer (35) and rheumatoid arthritis (36). In the present study, we demonstrated
that 12.8% of HCC patients expressed autoantibodies against OPN,
and the frequency and the mean titer of the anti-OPN antibodies in
HCC serum samples were higher than these values in normal human
serum (NHS). However, there was no statistical differences between
the HCC group and the LC group or the chronic hepatitis (CH) group,
which may be because of the limited patient population of the two
groups. Notably, when both the anti-OPN antibody and α-fetoprotein
(AFP) were used as diagnostic biomarkers simultaneously, the
sensitivity of HCC diagnosis reached 65%, which was higher than
that using the single anti-OPN autoantibody or AFP as a biomarker.
Moreover, indirect immunofluorescence assay was also used to
confirm the immune response of the anti-OPN autoantibody in HCC
serum samples to recombinant OPN protein. Collectively, these data
indicate that the anti-OPN autoantibody may be a potential
diagnostic marker for HCC, particularly in conjunction with
AFP.
In conclusion, we identified a high level of
anti-OPN autoantibody in HCC serum samples and the poor prognosis
of HCC patients with OPN-positive expression. It is plausible that
OPN and the anti-OPN autoantibody are closely correlated to HCC;
both may play an important role in the diagnosis and prognosis of
HCC. Further studies with large sample size and detailed
pathological information are warranted, and research aimed to
investigate the mechanisms of OPN and the anti-OPN autoantibody in
carcinogenesis, progression and metastasis will also be
proposed.
Acknowledgements
We thank Huixun Ren at the Xi’an Jiaotong University
School of Medicine for his help.
Abbreviations:
|
HCC
|
hepatocellular carcinoma
|
|
OPN
|
osteopontin
|
|
CH
|
chronic hepatitis
|
|
NHS
|
normal human serum
|
|
AFP
|
α-fetoprotein
|
|
SPP1
|
secreted phosphoprotein 1
|
|
ELISA
|
enzyme-linked immunosorbent assay
|
|
IHC
|
immunohistochemistry
|
|
IIFA
|
indirect immunofluorescence assay
|
|
OS
|
overall survival
|
|
TAAs
|
tumor-associated antigens
|
|
PVDF
|
polyvinylidene fluoride
|
|
TBS
|
Tris-buffered saline
|
|
RGD
|
arginine-glycine-aspartate
|
|
SIBLING
|
small integrin-binding ligand N-linked
glycoprotein
|
|
MAPK
|
mitogen-activated protein kinase
pathway
|
References
|
1
|
Gomaa AI, Khan SA, Toledano MB, Waked I
and Taylor-Robinson SD: Hepatocellular carcinoma: Epidemiology,
risk factors and pathogenesis. World J Gastroenterol. 14:4300–4308.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Parikh S and Hyman D: Hepatocellular
cancer: a guide for the internist. Am J Med. 120:194–202. 2007.
View Article : Google Scholar
|
|
3
|
Behne T and Copur MS: Biomarkers for
hepatocellular carcinoma. Int J Hepatol. 2012:8590762012.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cheng J, Wang W, Zhang Y, et al:
Prognostic role of pre-treatment serum AFP-L3% in hepatocellular
carcinoma: systematic review and meta-analysis. PloS One.
9:e870112014.PubMed/NCBI
|
|
5
|
Chen M, Li G, Yan J, et al: Reevaluation
of glypican-3 as a serological marker for hepatocellular carcinoma.
Clin Chim Acta. 423:105–111. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Song P, Feng X, Zhang K, et al:
Perspectives on using des-gamma-carboxyprothrombin (DCP) as a serum
biomarker: facilitating early detection of hepatocellular carcinoma
in China. Hepatobiliary Surg Nutr. 2:227–231. 2013.PubMed/NCBI
|
|
7
|
Zhu Q, Liu M, Dai L, et al: Using
immunoproteomics to identify tumor-associated antigens (TAAs) as
biomarkers in cancer immunodiagnosis. Autoimmun Rev. 12:1123–1128.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zhang Y, Ying X, Han S, et al:
Autoantibodies against insulin-like growth factor binding protein-2
as a serological biomarker in the diagnosis of lung cancer. Int J
Oncol. 42:93–100. 2013.PubMed/NCBI
|
|
9
|
Tan EM: Autoantibodies as reporters
identifying aberrant cellular mechanisms in tumorigenesis. J Clin
Invest. 108:1411–1415. 2001. View
Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zhang JY, Chan EK, Peng XX and Tan EM: A
novel cytoplasmic protein with RNA-binding motifs is an autoantigen
in human hepatocellular carcinoma. J Exp Med. 189:1101–1110. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Liaw L, Skinner MP, Raines EW, Ross R,
Cheresh DA, Schwartz SM and Giachelli CM: The adhesive and
migratory effects of osteopontin are mediated via distinct cell
surface integrins. Role of alpha v beta 3 in smooth muscle cell
migration to osteopontin in vitro. J Clin Invest. 95:713–724. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Malyankar UM, Scatena M, Suchland KL, Yun
TJ, Clark EA and Giachelli CM: Osteoprotegerin is an alpha vbeta
3-induced, NF-kappa B-dependent survival factor for endothelial
cells. J Biol Chem. 275:20959–20962. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chen F, Liu H, Shen Q, et al: Osteopontin:
participation in inflammation or mucosal protection in inflammatory
bowel diseases? Dig Dis Sci. 58:1569–1580. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yang M, Ramachandran A, Yan HM, et al:
Osteopontin is an initial mediator of inflammation and liver injury
during obstructive cholestasis after bile duct ligation in mice.
Toxicol Lett. 224:186–195. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Shao JS, Sierra OL, Cohen R, et al:
Vascular calcification and aortic fibrosis: a bifunctional role for
osteopontin in diabetic arteriosclerosis. Arterioscler Thromb Vasc
Biol. 31:1821–1833. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hwang SM, Lopez CA, Heck DE, Gardner CR,
Laskin DL, Laskin JD and Denhardt DT: Osteopontin inhibits
induction of nitric oxide synthase gene expression by inflammatory
mediators in mouse kidney epithelial cells. J Biol Chem.
269:711–715. 1994.PubMed/NCBI
|
|
17
|
Kawashima R, Mochida S, Matsui A, et al:
Expression of osteopontin in Kupffer cells and hepatic macrophages
and Stellate cells in rat liver after carbon tetrachloride
intoxication: a possible factor for macrophage migration into
hepatic necrotic areas. Biochem Biophys Res Commun. 256:527–531.
1999. View Article : Google Scholar
|
|
18
|
Hahne JC, Meyer SR, Kranke P, et al:
Studies on the role of osteopontin-1 in endometrial cancer cell
lines. Strahlenther Onkol. 189:1040–1048. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ramachandran S, Kwon KY, Shin SJ, et al:
Regulatory role of osteopontin in malignant transformation of
endometrial cancer. Mol Biol Rep. 40:3623–3629. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Li NY, Weber CE, Mi Z, Wai PY, Cuevas BD
and Kuo PC: Osteopontin up-regulates critical
epithelial-mesenchymal transition transcription factors to induce
an aggressive breast cancer phenotype. J Am Coll Surg. 217:17–26.
2013. View Article : Google Scholar
|
|
21
|
Yu TT, Han ZG, Shan L, Tao J, Zhang T,
Yuan SF and Shen HL: Expression of osteopontin in non-small cell
lung cancer and correlative relation with microvascular density.
Asian Pac J Cancer Prev. 15:29–32. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Huang J, Pan C, Hu H, Zheng S and Ding L:
Osteopontin-enhanced hepatic metastasis of colorectal cancer cells.
PloS One. 7:e479012012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Righi L, Bollito E, Ceppi P, et al:
Prognostic role of bone sialoprotein in clear cell renal carcinoma.
Anticancer Res. 33:2679–2687. 2013.PubMed/NCBI
|
|
24
|
Shang S, Plymoth A, Ge S, et al:
Identification of osteopontin as a novel marker for early
hepatocellular carcinoma. Hepatology. 55:483–490. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Abu El Makarem MA, Abdel-Aleem A, Ali A,
Saber R, Shatat M, Rahem DA and Sayed D: Diagnostic significance of
plasma osteopontin in hepatitis C virus-related hepatocellular
carcinoma. Ann Hepatol. 10:296–305. 2011.PubMed/NCBI
|
|
26
|
Shao Q, Ren P, Li Y, et al: Autoantibodies
against glucose-regulated protein 78 as serological diagnostic
biomarkers in hepatocellular carcinoma. Int J Oncol. 41:1061–1067.
2012.PubMed/NCBI
|
|
27
|
Xie H, Song J, Du R, et al: Prognostic
significance of osteopontin in hepatitis B virus-related
hepatocellular carcinoma. Dig liver Dis. 39:167–172. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ramaiah SK and Rittling S:
Pathophysiological role of osteopontin in hepatic inflammation,
toxicity, and cancer. Toxicol Sci. 103:4–13. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
O’Regan AW, Nau GJ, Chupp GL and Berman
JS: Osteopontin (Eta-1) in cell-mediated immunity: teaching an old
dog new tricks. Immunol Today. 21:475–478. 2000.PubMed/NCBI
|
|
30
|
Shinohara ML, Jansson M, Hwang ES, Werneck
MB, Glimcher LH and Cantor H: T-bet-dependent expression of
osteopontin contributes to T cell polarization. Proc Natl Acad Sci
USA. 102:17101–17106. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Denhardt DT, Noda M, O’Regan AW, Pavlin D
and Berman JS: Osteopontin as a means to cope with environmental
insults: regulation of inflammation, tissue remodeling, and cell
survival. J Clin Invest. 107:1055–1061. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Cao DX, Li ZJ, Jiang XO, et al:
Osteopontin as potential biomarker and therapeutic target in
gastric and liver cancers. World J Gastroenterol. 18:3923–3930.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Sun BS, Dong QZ, Ye QH, et al:
Lentiviral-mediated miRNA against osteopontin suppresses tumor
growth and metastasis of human hepatocellular carcinoma.
Hepatology. 48:1834–1842. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Philip S and Kundu GC: Osteopontin induces
nuclear factor kappa B-mediated promatrix metalloproteinase-2
activation through I kappa B alpha/IKK signaling pathways, and
curcumin (diferulolylmethane) down-regulates these pathways. J Biol
Chem. 278:14487–14497. 2003. View Article : Google Scholar
|
|
35
|
Tilli TM, Silva EA, Matos LC, et al:
Osteopontin is a tumor autoantigen in prostate cancer patients.
Oncol Lett. 2:109–114. 2011.PubMed/NCBI
|
|
36
|
Sakata M, Tsuruha JI, Masuko-Hongo K, et
al: Autoantibodies to osteopontin in patients with osteoarthritis
and rheumatoid arthritis. J Rheumatol. 28:1492–1495.
2001.PubMed/NCBI
|