Introduction
Angiogenesis, the process of new blood vessel
formation from the pre-existing vasculature, is recognized as the
key for tumor growth and progression (1). Solid tumors cannot grow beyond 1–2 mm
in size without a blood supply from the neovasculature (2). In 1971, Folkman (3) first proposed the concept of cancer
treatment via the inhibition of new blood vessel formation in
tumors. Studies of tumor angiogenesis progressed slowly until the
identification of crucial molecules, namely, the vascular
endothelial growth factor (VEGF) family and their cognate receptors
(4). Even though anti-angiogenic
drugs have yielded significant results, extension of
progression-free survival and, in certain cases, overall survival
times are small (5). The benefits
of anti-angiogenic agents are markedly inconsistent among different
tumor types (5). The finding of
inter- and intra-angiogenic heterogeneity may promote the
improvement of the current applications of anti-angiogenic therapy
(6). Thus, the vital issue in the
development of such drugs is the establishment of early clinical
predictors of treatment response in order to predict the patients
that may or may not benefit prior to therapy initiation.
Understanding angiogenic heterogeneity may help guide treatment
strategies.
Integrins, as important mediators in cell-cell and
cell-matrix interactions, serve key roles in angiogenesis and tumor
metastasis (7). Several integrins,
particularly integrin αvβ3, are significantly upregulated in
various types of tumor cells and in activated endothelial cells
during angiogenesis, but these integrins are not at all, or only
slightly, affected in quiescent vessel cells and other normal cells
(8). Therefore, imaging of integrin
αvβ3 expression is a potential method for evaluating tumor
neovascularization. The majority of integrin-targeted imaging
tracers function based on the tripeptide Arg-Gly-Asp (RGD) amino
acid sequence due to its high affinity and specificity for integrin
αvβ3 (9). 18F-alfatide,
with the advantages of easy preparation, one-step labeling and fast
pharmacokinetics in vivo, has been found to be safe
(10). Positron emission tomography
(PET) was chosen as the imaging strategy due to its high
sensitivity to low amounts of tracer and its exquisite specificity
(11). Animal experiments have
shown that 18F-alfatide PET is an effective tracer for
tumor spatial heterogeneity imaging (12), allowing further investigation of the
angiogenic heterogeneity among different tumors. In addition, we
have performed two pilot clinical studies in which
18F-alfatide PET/CT parameters were found to predict
tumor sensitivity to concurrent chemoradiation therapy (CCRT) in
patients with gliomas and advanced non-small cell lung cancer
(NSCLC) (13,14). Therefore, we hypothesized that
18F-alfatide PET may be able to predict anti-angiogenic
responses.
The present animal study aimed to investigate
whether 18F-alfatide PET parameters could be used to
predict the response to anti-angiogenic therapy in a lung
adenocarcinoma A549 ×enograft model, which had a high vessel
density and high αvβ3 expression, and in a prostate cancer PC-3
×enograft model, which had a low vessel density and low αvβ3
expression.
Materials and methods
Drugs
The agents used in the present study were
bevacizumab (Avastin; Roche Diagnostics, Basel, Switzerland),
apatinib (Jiangsu Hengrui Medicine Co., Ltd., Jiangsu, China) and
cisplatin (Qilu Pharmaceutical, Co., Ltd., Jinan, Shandong, China).
Bevacizumab and cisplatin were dissolved in physiological saline.
Apatinib was diluted in 0.5% (w/v) carboxymethyl cellulose and 5%
(w/v) glucose solution.
Cell culture
Human lung adenocarcinoma A549 (high αvβ3
expression) and human prostatic carcinoma PC-3 (low αvβ3
expression) cell lines were purchased from the Type Culture
Collection of the Chinese Academy of Sciences (Shanghai, China).
These two cell lines were grown at 37°C in RPMI-1640 medium
(Invitrogen; Thermo Fisher Scientific, Inc., Waltham, MA, USA)
supplemented with 10% fetal bovine serum and 1% penicillin
streptomycin antibiotic mixture (Invitrogen; Thermo Fisher
Scientific, Inc.) in a humidified incubator (Heraeus Germany GmbH
& Co. KG, Hanau, Germany) with 5% CO2. Cells were
grown as a monolayer and were split or harvested when they reached
80–90% confluence to maintain exponential growth.
Animal models
A total of 2×106 A549 cells or
5×106 PC-3 cells were injected subcutaneously near the
right shoulders of female BALB/c nude mice (n=110; age, 6–8 weeks;
weight, 18–20 g) purchased from the Beijing Hua Fukang
pathogen-free animal breeding facility [approval no. SCXK (Jing)
2009–0008]. A total of 2×106 A549 cells were injected
into the right hind leg for radiotherapy. The tumor size and mouse
body weight were measured every 2 days, and the tumor volume was
calculated with the following formula: Tumor volume = (length ×
width2)/2. The index for evaluating the inhibition in
individuals in the treated groups was the relative tumor growth
ratio, which was calculated according to the following equation:
Treatment/control (T/C) (%) = increase in tumor volume in treated
individuals/mean increase in tumor volume in the control group ×
100 (15). The animal rooms
provided a constant temperature of 26°C, a relative humidity of
50–60% and daylight plus a 12/12-h light/dark cycle. The mice were
fed a laboratory animal diet and sterile water ad libitum.
The maximum tumor volume was ~1,800 mm3 and multiple
tumors were nt observed in any individual animal. A tumor size
>20 mm (2.0 cm) in any direction or weight loss exceeding 10% of
the original weight were considered humane endpoints.
Experimental design and treatment
protocol
A total of 20 size-matched, xenografted
tumor-bearing mice (A549, n=10; PC-3, n=10), with a mean tumor
volume of 100 mm3 1 day prior to the PET imaging, were
used to compare the tumor uptake of 18F-alfatide between
two tumor types and to analyze the angiogenic heterogeneity. The
heterogeneity was represented by the coefficient of variation (CV)
of 18F-alfatide, calculated by dividing the standard
deviation by the mean value.
In an efficacy prediction test, the groups (n=90,
6–8/group) were sized-matched with tumor volumes of 100–200
mm3 1 day prior to the baseline PET imaging. For
anti-angiogenic therapy, A549 and PC-3 ×enografted tumor-bearing
mice were injected with bevacizumab intraperitoneally or
administered apatinib by oral gavage on day 0 after the baseline
imaging. Bevacizumab, at a dose of 20 mg/kg body weight in 200 µl
saline, or vehicle of 200 µl physiological saline, was administered
every 4 days over 2 weeks (four injections). Apatinib, at a dose of
100 mg/kg body weight in 200-µl suspensions, or the vehicle of 200
µl 0.5% (w/v) carboxymethyl cellulose and 5% (w/v) glucose
solution, was administered once daily for 2 weeks.
To balance the effects of the two drugs in the
combined treatment, preliminary experiments (n=3) were performed to
determine whether cisplatin, at a dose of 5 mg/kg body weight
(injected intraperitoneally every 3 days for five injections), and
radiotherapy of 5 Gy at a time (once a week, two times), could
produce similar effects to those of the treatment protocol of
bevacizumab over 2 weeks by comparing the tumor volumes between the
experimental and control groups (data not shown). In the combined
therapy, mice bearing A549 ×enografts received chemotherapy or
radiotherapy 2 h after bevacizumab in order to obtain a better
curative effect during vascular normalization (16). For the radiation treatment, the mice
were anesthetized, the tumor-bearing leg was positioned in the
radiation field and a lead cover protected the rest of the body.
Irradiation was performed with 6 MeV of X-rays using a linear
accelerator (X-RAD 225; Varian Medical Systems, Inc., Palo Alto,
CA, USA). The dose was administered at the measured depth. The
schedule of laboratory assignments is shown in Fig. 1.
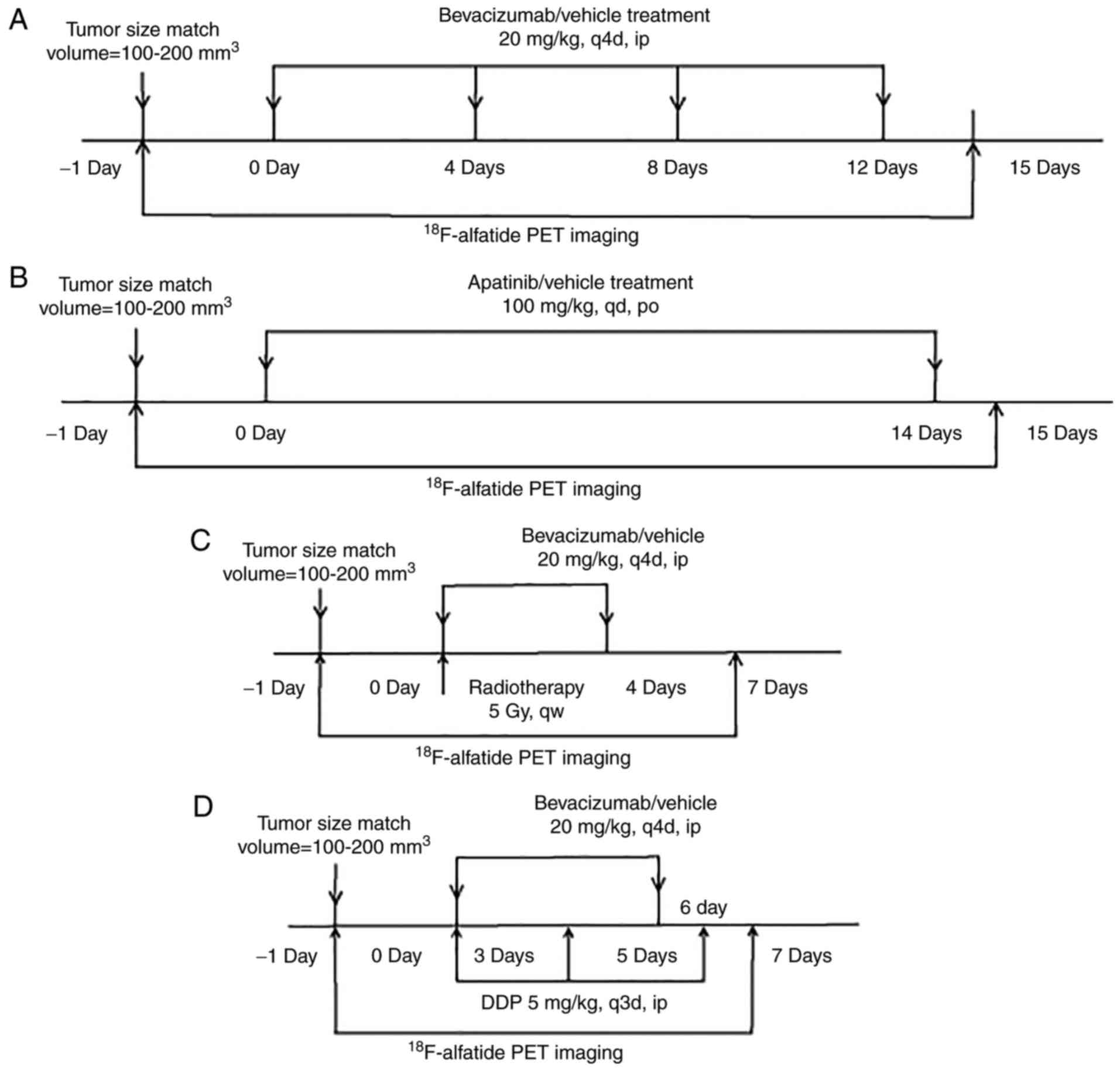 | Figure 1.Treatment protocols for (A)
bevacizumab, (B) apatinib, (C) bevacizumab combined with
radiotherapy and (D) bevacizumab combined with DDP, and the imaging
protocol are shown. Tumor size was calculated on the basis of
caliper measurements according the formula: (length ×
width2)/2. DDP, cisplatin; q4d, every four days; qd,
once a day; qw, once a week; ip, intraperitoneal injection; po,
oral administration; PET, positron emission tomography. |
Micro-PET imaging protocol
18F-alfatide micro-PET scans were
performed for all 20 tumor-bearing mice when the tumor volume of
each mouse reached ~100 mm3 for the heterogeneity
analysis, at 0 and 15 days for anti-angiogenic treatment, and at 0
and 7 days for the combined therapy following the initiation of
treatment. A simple lyophilized kit for labeling the PRGD2 peptide
was purchased from the Jiangsu Atomic Energy Laboratory (Jiangsu,
China), and the synthesis process was performed according to a
previously published method (17).
The radiochemical purity of the 18F-alfatide exceeded
95%, and its specific radioactivity exceeded 37 GBq (1,000
mCi)/µmol. All the micro-PET images were obtained with an Inveon
PET scanner (Siemens Preclinical Solutions, LLC, Knoxville, TN,
USA) using 18F-alfatide. With the assistance of the
positioning laser from the Inveon system, each tumor-bearing mouse
was placed with its tumor located in the center of the field of
view to achieve the highest imaging sensitivity.
18F-alfatide PET scans were performed 1 h
after tail-vein injection of 18F-alfatide (2.4–3.5 MBq),
under isoflurane anesthesia with 1.5% isoflurane in 100% oxygen at
a flow rate of 1.5 l/min. Prior to the 18F-alfatide PET
scanning, the mice were prohibited from drinking water for at least
4 h. The PET images were reconstructed and analyzed by the OSEM-3D
IAM software program (IS_v1.4.3 SP1; Siemens Preclinical Solutions,
LLC).
Image analysis
Two experienced nuclear medicine physicians examined
all the images using a double-blinded approach and aimed to reach a
consensus. If no consensus was reached, the third chief physician
decided the treatment response. Regions of interest (ROIs) were
drawn over the tumor using vendor software (IS_v1.4.3 SP1; Siemens
Healthineers, Erlangen, Germany) on decay-corrected, whole-body
transverse images with a threshold of 40%, and a set of data that
included the ROImax and the mean was obtained. The
standardized uptake value (SUV) of each tumor was calculated as the
maximal or mean trace uptake of the ROIs according to the following
formula: [measured activity concentration (Bq/ml) × body weight
(g)]/injected activity (Bq). A circular region of 5×5 mm, which was
manually contoured in the liver, a relatively large and less active
organ, on each transverse PET image was defined as the non-target
reference. The tumor-to-normal tissue (T/N) ratio was calculated by
taking the ratio of the tumor SUVmax to the liver
SUVmax (18).
Three-dimensional ROIs were drawn using the TrueD
tool kit (Siemens Preclinical Solutions, LLC), which involved
several imperative manual adjustments. The SUVmean and
SUVmax were acquired by calculating the average of the
SUVmean and the SUVmax of the planar ROIs
drawn on three discontinuous transaxial PET slices, respectively
(6). The CV of each group was
calculated by the following formula: Standard deviation (SD)/the
mean value of the SUVmean.
Statistical analysis
All data were analyzed using GraphPad Prism 7.0
(GraphPad Software, Inc., La Jolla, CA, USA) and are presented as
the mean ± SD. The significance of statistical differences between
the two groups was determined by Student's t-tests. One-way
analysis of variance and Bonferroni's post hoc test were required
for multiple comparisons. Within each group, linear regression
analysis was used to evaluate the associations. P<0.05 was
considered to indicate a statistically significant difference.
Results
Tumor uptake of
18F-alfatide and angiogenesis heterogeneity between the
A549 and PC-3 models
As illustrated in Fig.
2, the SUVmean and T/N ratios of
18F-alfatide in the A549 models were significantly
higher than those in the PC-3 models (SUVmean, 0.64±0.07
and 0.25±0.02, respectively; P<0.00001; T/N, 2.76±0.62 and
0.82±0.11, respectively; P<0.00001). The variation coefficients
of the 10 tumors in the A549 and PC-3 models were 11.44 and 9.21%,
respectively, for the SUVmean, and 22.28 and 13.15%, respectively,
for the T/N ratios, indicating that there was inter- and
intra-angiogenic heterogeneity among the A549 and PC-3 ×enografted
tumors.
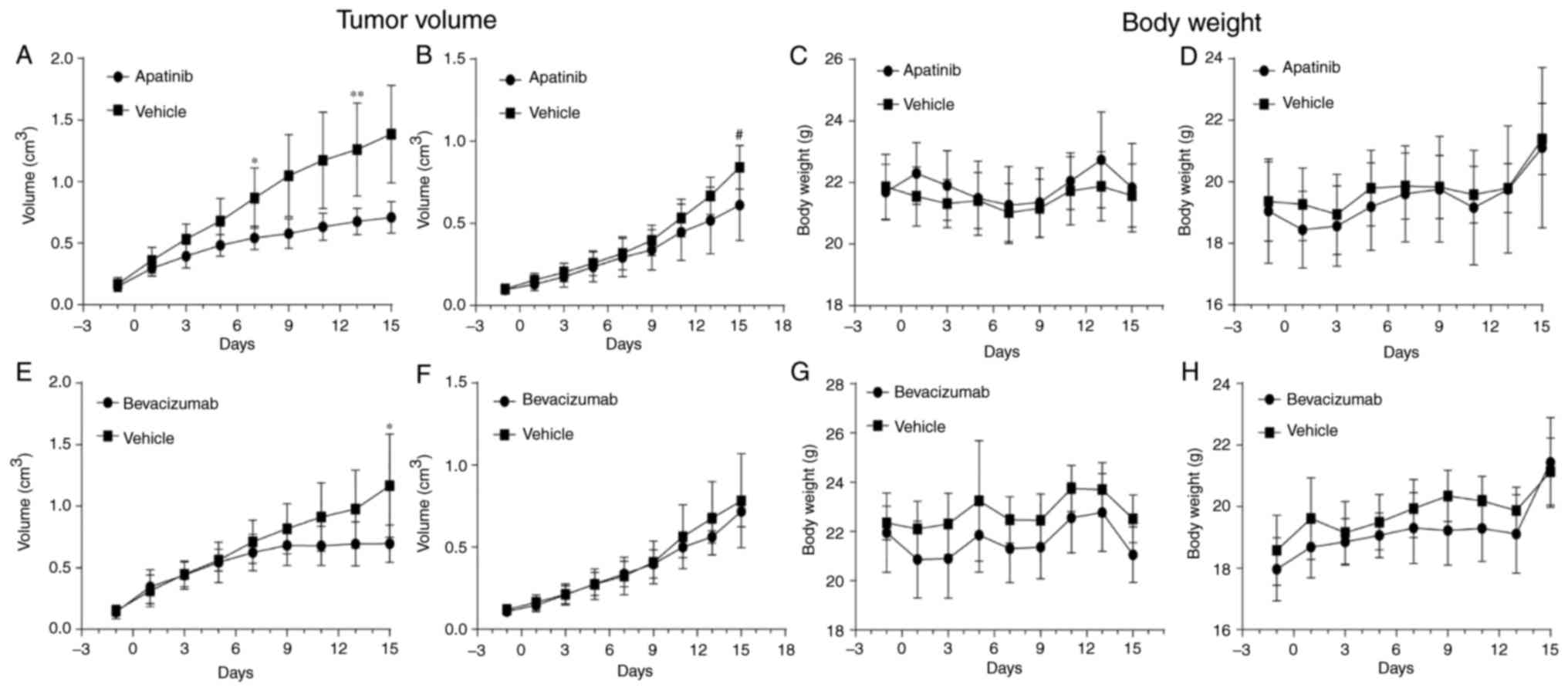
Comparison of tumor responses in the
two animal models following anti-angiogenic treatment
The ratio of the tumor growth (T/C) following
treatment with the anti-angiogenic drugs was lower in the A549
×enografted tumors compared with that in the PC-3 tumors (apatinib,
47±11.46 and 69±26.74%, respectively, P=0.052; bevacizumab,
57.80±13.82 and 90.27±13.09%, respectively, P=0.001). With regard
to tumor responses (Fig. 3),
Fig. 3A, B, E and F compares the
angiogenic responses of the A549 and PC-3 groups by analyzing the
tumor growth curves for the vehicle and the same anti-angiogenic
drug. Among the A549 groups receiving anti-angiogenic therapy,
there was a significant decrease in tumor volume beginning at day 7
in the apatinib-treated models (P<0.01) and at day 15 in the
bevacizumab-treated models (P<0.01) compared with that in the
vehicle-treated controls. This response occurred earlier than that
in the PC-3 groups, in which the significant difference in tumor
volume occurred at day 15 (P<0.05) in the apatinib-treated
models, while no significant difference was observed in the
bevacizumab-treated models. The difference between the tumor
volumes in the apatinib- and vehicle-treated models was greater
(P<0.001 at day 13) in the A549 group than in the PC-3 group. As
shown in Fig. 3C, D, G and H,
neither apatinib nor bevacizumab had toxic effects on the mice,
indicated by the absence of significant weight loss compared with
that in the control groups.
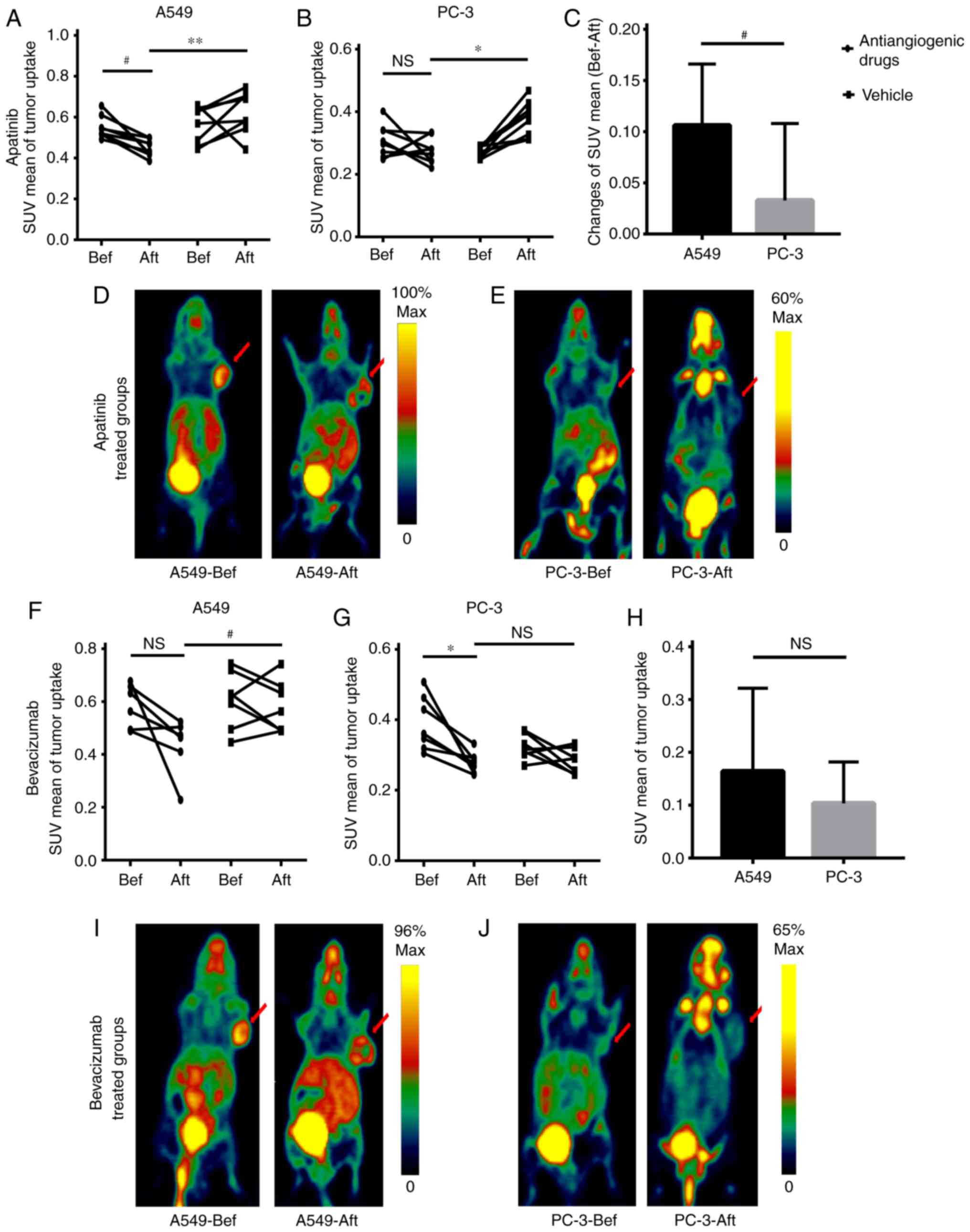
In Fig. 4, the
responses to the same anti-angiogenic drugs were compared between
the A549 and PC-3 groups by analyzing the SUVmean of the
tumors prior to and following treatment. In the A549 lung
adenocarcinomas treated by apatinib, the SUVmeans
decreased significantly (P<0.01), and a significant difference
between the anti-angiogenic drug- and vehicle-treated models
(P<0.001) was observed following treatment. In the PC-3 prostate
tumors, only apatinib caused a significant difference in the
SUVmean between the treatment and control models
(P<0.01) following treatment. Bevacizumab caused a slight
decrease in the SUVmean in the treatment group (P=0.06)
and a significant difference between the treatment models and
control models (P<0.05). However, bevacizumab only caused a
significant decrease of SUVmean in the treatment group
(P<0.01).
Fig. 4C and H
compares the changes in the SUVmean of
18F-alfatide following anti-angiogenic therapy in the
two xenografted tumor-bearing animal models. The degree of tumor
response to apatinib or bevacizumab therapy, assessed by the tumor
uptake changes of 18F-alfatide (19), was higher in A549 lung
adenocarcinomas than in PC-3 prostate tumors. Only
SUVmean changes in the tumors following apatinib
treatment exhibited a significant difference between the A549 and
PC-3 groups (P<0.05). Fig. 4D, E, I
and J show the differences in tumor uptake intuitively.
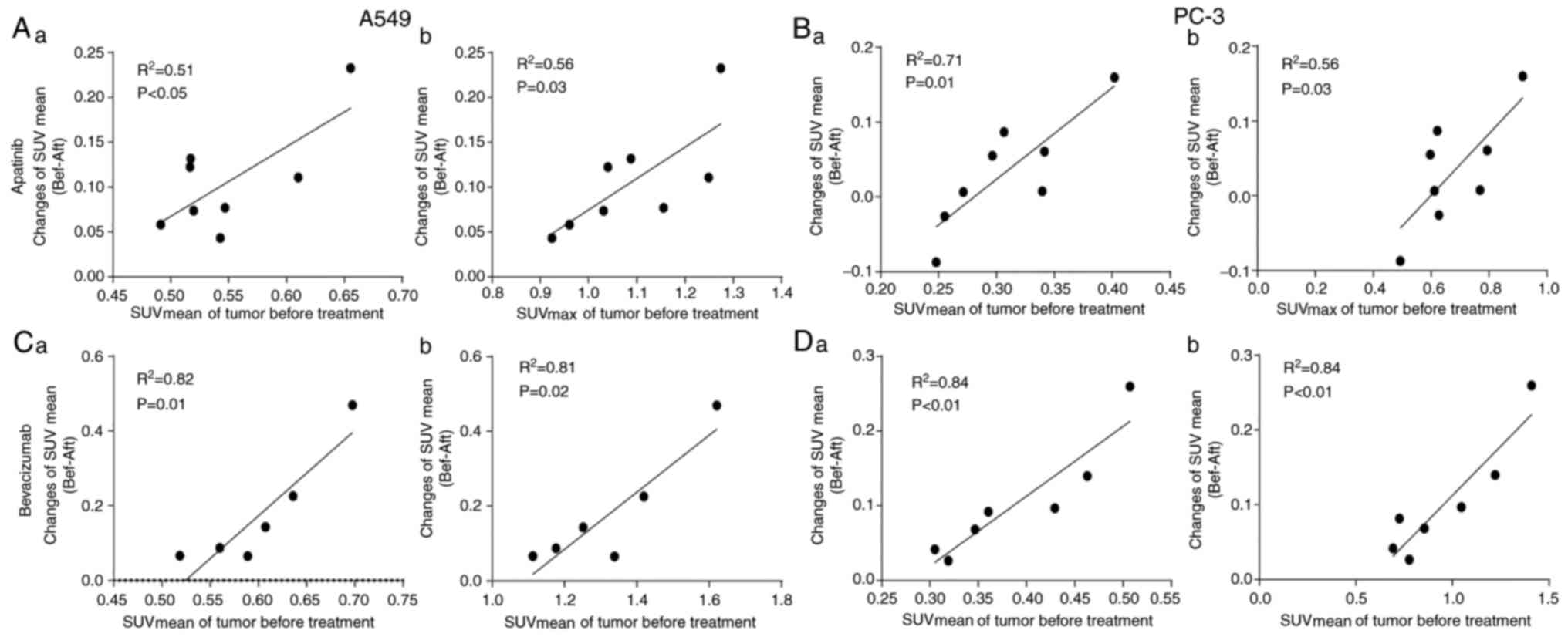
Association between tumor response and
tumor uptake prior to treatment with anti-angiogenic therapy
The median of the SUVmean prior to
treatment in the apatinib and bevacizumab groups (A549 and PC-3
were included in both groups) was 0.47 and 0.52, respectively. As
shown in Table I, the ratios of the
individuals whose tumor growth ratio was less than the T/C were
greater in the higher SUVmean groups than in the lower
SUVmean groups. Fig. 5
shows plots of the SUVmean changes (i.e., the
therapeutic effect) following anti-angiogenic therapy against the
SUVmean and SUVmax in the A549 and PC-3
models at the time of diagnosis. The SUVmean changes
were calculated by deducting the SUVmean of
18F-alfatide on day 15 from the SUVmean on
day 0 for the same animal. There was a significant positive linear
association between SUVmean changes and the tumor uptake
prior to treatment in the apatinib-treatment groups
(R2=0.51, P<0.05 for SUVmean prior to
treatment and R2=0.56, P=0.03 for SUVmax in
the A549 models; R2=0.71, P=0.01 for SUVmean
and R2=0.56, P=0.03 for SUVmax in the PC-3
models). With bevacizumab treatment, there was a higher positive
linear association between SUVmean changes and the tumor
uptake prior to treatment (R2=0.82, P=0.01 for
SUVmean and R2=0.81, P=0.02 for
SUVmax in the A549 models; R2=0.84, P<0.01
for SUVmean and R2=0.84, P<0.01 for
SUVmax in the PC-3 models).
 | Table I.Inhibition of tumor growth by
apatinib and bevacizumab. |
Table I.
Inhibition of tumor growth by
apatinib and bevacizumab.
|
|
| Ratio of
individuals <T/C (%) |
|
|---|
|
|
|
|
|
|---|
| Antiangiogenic
drugs | SUVmean
prior to treatment | <90% | <80% | <70% | <60% | <50% | <40% | P-value |
|---|
| Apatinib | >0.47 |
|
| 100 | 87.50 | 62.5 | 37.5 | 0.052 |
|
| <0.47 |
|
| 62.5 | 37.5 | 12.5 | 12.5 |
|
| Bevacizumab | >0.52 | 100 | 85.71 | 71.43 |
|
|
| 0.006 |
|
| <0.52 | 50 | 16.67 | 0 |
|
|
|
|
Association between tumor response and
tumor uptake prior to treatment with anti-angiogenic therapy
combined with chemotherapy or radiotherapy
As shown in Fig. 6A and
F, there was a significant decrease in tumor volume in the
combined bevacizumab and cisplatin-treated models compared with
that in the vehicle-treated models beginning at day 7 (P<0.05),
and the same effect was found with bevacizumab combined with
radiotherapy at day 5 (P<0.01). In Fig. 6B and G, bevacizumab combined with
cisplatin treatment is shown to have a toxic effect on the mice, as
shown by the significant weight loss on the 7th day (P<0.05),
and bevacizumab combined with radiotherapy did not have this
effect. Fig. 6C, D, H and I shows
the linear association between the SUVmean changes
following treatment with bevacizumab combined with either cisplatin
or radiotherapy and the uptake of 18F-alfatide by the
tumor prior to treatment in the A549 models. There was a
significant positive linear association between the
SUVmean changes and the SUVmean prior to
treatment in the combined bevacizumab and cisplatin-treated models
(R2=0.84, P<0.01) and a moderate linear association
between the SUVmean changes and other parameters prior
to treatment (R2=0.60, P=0.02 for SUVmax). In
mice treated with bevacizumab combined with radiotherapy, the
SUVmean changes were associated with the
SUVmean prior to treatment (R2=0.93,
P<0.0001) and with the SUVmax (R2=0.52,
P=0.04) prior to treatment.
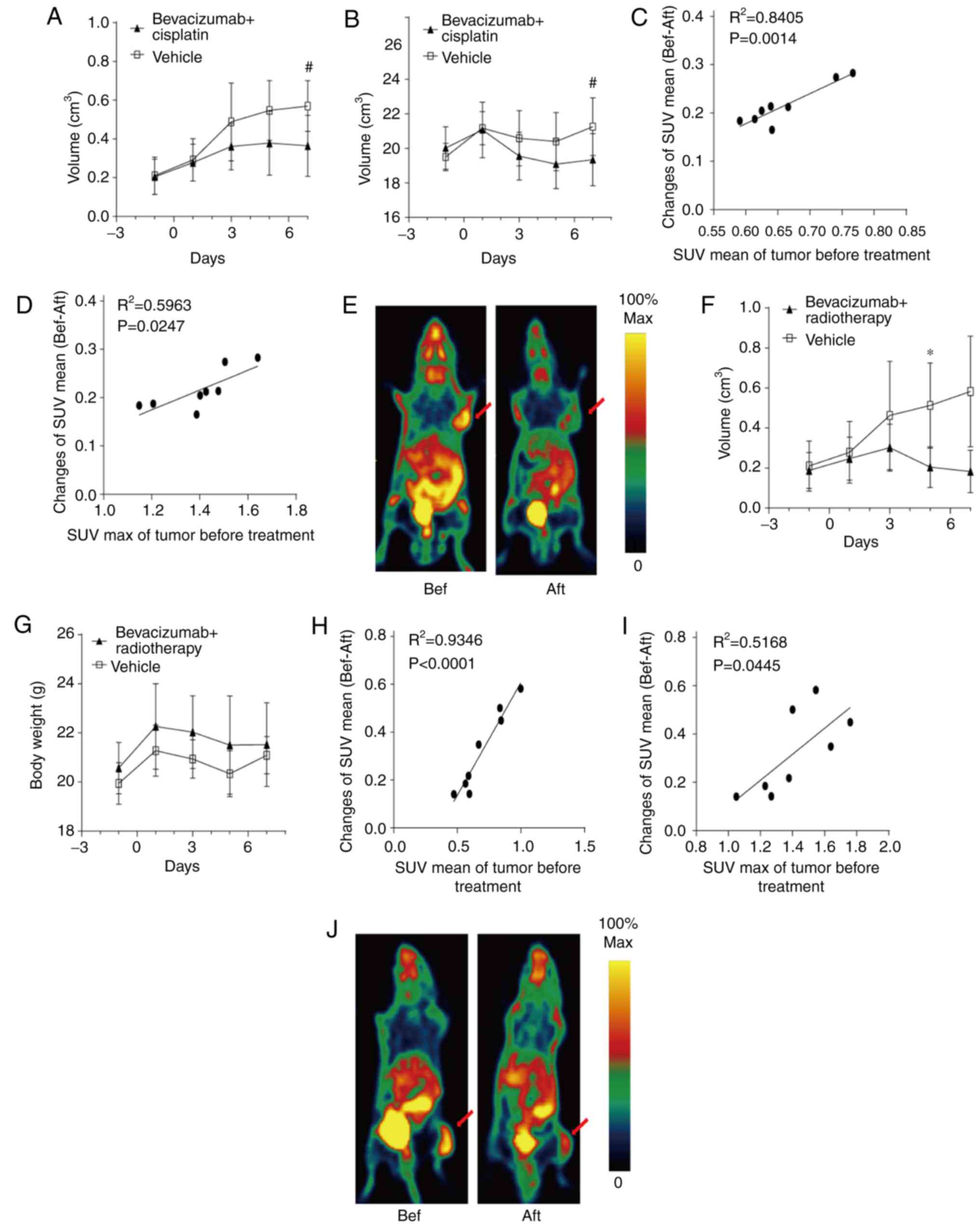 | Figure 6.(A) Tumor growth curves, (B) body
weight changes, linear associations between the SUVmean
changes following treatment with (C) SUVmean and (D)
SUVmax prior to treatment, and (E) PET imaging for
vehicle-(n=8) and bevacizumab combined with cisplatin-(5 mg/kg) in
the xenografted A549 lung adenocarcinoma model. (F) Tumor growth
curves, (G) body weight changes, linear associations between the
SUVmean changes following treatment with (H)
SUVmean and (I) SUVmax prior to treatment,
and (J) PET imaging for vehicle-(n=8) and bevacizumab combined with
radiotherapy (5Gy)-treated groups in the xenografted A549 lung
adenocarcinoma model. PET imaging of tumor-bearing mice was
performed prior to and following treatment with the anti-angiogenic
drugs. Tumor volume was determined by caliper measurements. Body
weight was measured using scales once every 2 days. The red arrow
indicates the tumor. *P<0.01 and #P<0.05,
significantly different from the vehicle-treated group.
SUVmean, mean standardized uptake value;
SUVmax, maximum SUV; Bev, bevacizumab. |
Discussion
In the present study, it was found that the
anti-angiogenic treatment response of tumors with high uptake of
RGD tracers was better than that of the low-uptake tumors. This
result was consistent with the results of the study by Ji et
al (19), in which the degree
of tumor response to linifanib therapy was associated with αvβ3
expression levels prior to treatment. In clinical studies, Iagaru
et al (20) first found that
decreases of >50% in SUVmax and angiogenic volumes,
assessed by fluorine 18 2-fluoropropionyl-labeled PEGylated dimeric
arginine-glycine-aspartic acid peptide
(18F-FPPRGD2) uptake, at 1 week after
bevacizumab administration predicted good outcomes, while decreases
of <15% predicted poor prognoses in patients with glioblastoma
multiforme. Subsequently, it was further confirmed that changes in
18F-FPPRGD2 uptake as early as 1 week after
bevacizumab administration may be able to predict the outcome of
treatment in patients with cervical and ovarian cancer (21). However, all these results were
completely contrary to the results of a previous study (14), which demonstrated that tumor uptake
in 18F-alfatide PET/CT was higher in non-responders than
in responders following CCRT. In the present study, the correlation
between tumor uptake prior to treatment and the degree of treatment
response in the bevacizumab groups was higher than that in the
apatinib groups. The correlation decreased to a moderate level in
the bevacizumab combined with chemoradiotherapy group, but remained
high in the bevacizumab combined with radiotherapy group. The
abnormal structure of neovascularization and the different
mechanisms of action of different drugs may be the reason for the
opposing conclusions.
Tumor vessels are dilated, tortuous and
heterogeneous in their spatial distributions, and are characterized
by large inter-endothelial junctions, an increased number of
fenestrations and a lack of a normal basement membrane, which makes
flow resistance and the hydrostatic and oncotic pressures almost
equal between the intravascular and extravascular spaces (22,23).
Poor blood flow and elevated interstitial fluid pressure hinder the
delivery of therapeutic drugs and oxygen to tumor tissues.
Bevacizumab, a recombinant humanized monoclonal antibody that
blocks human VEGF from binding to its receptors, could interfere
with the ability of a tumor to recruit new blood vessels by binding
soluble VEGF in the blood and has no direct effect on the growth of
tumor cells in vitro (24).
As a result, the anti-angiogenic efficiency of bevacizumab may be
less affected by vascular structure and function. However, the
abnormal microenvironment in tumors could hinder the efficacy of
chemotherapeutic drugs, which must pass through the vascular wall
to directly act on tumor cells (25). The same is true with radiotherapy in
terms of blocking oxygen. It is presumed that it is more difficult
for chemotherapeutic drugs and oxygen to reach a tumor with
increased immature tumor neovascularization. This may be the reason
why tumor uptake in 18F-alfatide PET/CT prior to
treatment was higher in non-responders than in responders
(P<0.01) (13,14). The negative association between
tumor uptake of 18F-alfatide prior to treatment and the
degree of the chemoradiotherapy response may reduce the
treatment-response association of bevacizumab to a moderate one in
the bevacizumab combined with chemotherapy group. In the
bevacizumab combined with radiotherapy group, the tumor volumes
following therapy were so small that the tumor uptake was very low.
Therefore, the SUVmean changes in a tumor mainly depend
on the SUVmean prior to treatment. This may have led to
the high association between the SUVmean prior to
treatment and the response to bevacizumab combined with
radiotherapy. Apatinib, an inhibitor of VEGFR-2 tyrosine kinase
that targets the intracellular ATP-binding site of the receptor,
would also be affected, in that it could inhibit tumor cell growth
and tumor angiogenesis during in vitro experiments (15). The partial effect of apatinib on
antitumor cells may also be influenced by the abnormal neovascular
structure. The different mechanisms of action may be the reason for
the different degrees of association between the uptake of
RGD-based tracers by tumors and the effects of anti-angiogenic
therapies.
From the present study, intertumoral angiogenic
heterogeneity was found between A549 lung adenocarcinoma and PC-3
prostate cancer, which was indicated by higher levels of tracer
uptake in A549 tumors than in PC-3 ×enografted tumors. Intratumor
angiogenic heterogeneity (CV) also existed among the groups and was
higher in the A549 group than in the PC-3 group. RGD-based tracer
targeting of αvβ3 has already been used in the diagnosis of
malignant tumors (10,26,27)
and in predicting the efficacy of CCRT in NSCLC (13,14).
Low 68Ga-RGD2 uptake and poor αvβ3 expression
in SCLC may have led to the conclusion that αvβ3-targeted therapy
is not adequate for the majority of SCLC patients. Clinical
research of cilengitide (a type of RGD peptide targeted to αvβ3)
was supported in NSCLC, and the treated tumors were characterized
by high angiogenesis. However, the relatively conspicuous
intratumor angiogenic heterogeneity of NSCLC made the therapeutic
response to cilengitide susceptible to variations between
individuals (6,20). Therefore, such inter- and
intratumoral angiogenic heterogeneity highlights the importance of
patient selection prior to αvβ3-targeted or anti-angiogenic
therapy. Kang et al (6)
found that the apparent intratumoral angiogenic heterogeneity in
NSCLC and SCLC primary lesions was similar (CV: 36.2 vs. 36.3%),
although the SUVs of 68Ga-RGD2 in NSCLC
primary lesions were significantly higher than those in SCLC
(P<0.0001) (6). From the present
study, it was found that the CV of the A549 tumor group (high
angiogenesis) was greater than that of the PC-3 group (low
angiogenesis). This result may indicate that more attention should
be paid to the difference in the responses of high angiogenesis
tumors.
There were several limitations to this study. First,
the A549 and PC-3 lines represent different cancer types, and this
could easily raise questions regarding the validity of this
experimental scheme with regard to the treatment efficacy in
different tumor types from the same type of cancer. These two
xenografted tumor-bearing animal models (A549 with relatively high
integrin αvβ3 expression in the tumor cells and tumor
neovasculature; and PC-3 with low integrin αvβ3 expression in the
tumor cells and neovasculature) were verified in previous studies,
and it was indeed difficult to find two tumor cell lines of
xenografted tumors with significantly different uptakes in RGD PET
or SPECT from the same tumor type (28,29).
Second, xenografted tumors are relatively homogeneous. The CVs of
the tumor uptake in the present study may not be able to completely
replace tumor heterogeneity in clinical settings.
In conclusion, in this study, data was obtained
supporting the fact that the use of 18F-alfatide PET may
be a valid and useful pretreatment screening tool to identify
individuals who would benefit from anti-angiogenic drug-containing
therapy. The inter- and intra-angiogenic heterogeneity highlighted
the importance of individual selection prior to anti-angiogenic
therapy. Further clinical evaluations in large cohorts are required
to confirm these preliminary findings.
Acknowledgements
The authors specially thank Professor Hongbo Huang
(Jiangsu Key Laboratory of Molecular Nuclear Medicine, Jiangsu
Institute of Nuclear Medicine, Wuxi, China) for providing
assistance with the micro-PET imaging of the mice.
Funding
The present study was partially funded by the
Shandong Key Research and Development Plan (grant nos. 2017CXGC1209
and 2017GSF18164), the Outstanding Youth Natural Science Foundation
of Shandong Province (grant no. JQ201423), the Jinan Clinical
Medicine Science and Technology Innovation Plan (grant no.
201704095), the National Natural Science Foundation of China (grant
nos. 81472812 and 81372413) and the National Key Research and
Development Program of China (grant no. 2016YFC0904700).
Availability of data and materials
The datasets obtained during the current study are
available from the corresponding author on reasonable request.
Authors' contributions
JY and SY conceived the study, and participated in
its design. JL participated in the experiments and drafted the
manuscript. DW contributed to the sample collection and
interpretation of the data. XS performed the statistical analysis.
XM and JL performed the nuclear medicine experiments. SY revised
the manuscript. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
This study was performed with the approval of the
Shandong Cancer Hospital and Institute Ethical Committee, and all
the experiments were performed according to the National Institutes
of Health Guide for the Care and Use of Laboratory Animals
(publication no. 85-23, revised 1985).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Folkman J: Role of angiogenesis in tumor
growth and metastasis. Semin Oncol. 29 6 Suppl 16:S15–S18. 2002.
View Article : Google Scholar
|
|
2
|
Folkman J: Angiogenesis in cancer,
vascular, rheumatoid and other disease. Nat Med. 1:27–31. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Folkman J: Tumor angiogenesis: Therapeutic
implications. N Engl J Med. 285:1182–1186. 1971. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ferrara N and Kerbel RS: Angiogenesis as a
therapeutic target. Nature. 438:967–974. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jayson GC, Kerbel R, Ellis LM and Harris
AL: Antiangiogenic therapy in oncology: Current status and future
directions. Lancet. 388:518–529. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kang F, Wang Z, Li G, Wang S, Liu D, Zhang
M, Zhao M, Yang W and Wang J: Inter-heterogeneity and
intra-heterogeneity of αvβ3 in non-small cell
lung cancer and small cell lung cancer patients as revealed by
68Ga-RGD2 PET imaging. Eur J Nucl Med Mol
Imaging. 44:1520–1528. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Niu G and Chen X: Why integrin as a
primary target for imaging and therapy. Theranostics. 1:30–47.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Danhier F, Le Breton AL and Préat V:
RGD-based strategies to target alpha(v) beta(3) integrin in cancer
therapy and diagnosis. Mol Pharm. 9:2961–2973. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chen H, Gang N, Hua W and Chen X: Clinical
application of radiolabeled RGD peptides for PET imaging of
integrin αvβ3. Theranostics. 6:78–92. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gao S, Wu H, Li W, Zhao S, Teng X, Lu H,
Hu X, Wang S, Yu J and Yuan S: A pilot study imaging integrin αvβ3
with RGD PET/CT in suspected lung cancer patients. Eur J Nucl Med
Mol Imaging. 42:2029–2037. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Massoud TF and Gambhir SS: Molecular
imaging in living subjects: Seeing fundamental biological processes
in a new light. Genes Dev. 17:545–580. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wei YC, Gao Y, Zhang J, Fu Z, Zheng J, Liu
N, Hu X, Hou W, Yu J and Yuan S: Stereotactic comparison study of
18F-alfatide and 18F-FDG PET imaging in an
LLC tumor-bearing C57BL/6 mouse model. Sci Rep. 6:287572016.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zhang H, Liu N, Gao S, Hu X, Zhao W, Tao
R, Chen Z, Zheng J, Sun X, Xu L, et al: Can a novel
18F-ALF-NOTA-PRGD2 PET/CT predict the treatment
sensitivity of concurrent chemoradiotherapy in patients with newly
diagnosed glioblastoma? J Nucl Med. 57:524–529. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Luan X, Huang Y, Gao S, Sun X, Wang S, Ma
L, Teng X, Lu H, Yu J and Yuan S: 18F-alfatide PET/CT
may predict short-term outcome of concurrent chemoradiotherapy in
patients with advanced non-small cell lung cancer. Eur J Nucl Med
Mol Imaging. 43:2336–2342. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Tian S, Quan H, Xie C, Guo H, Lü F, Xu Y,
Li J and Lou L: YN968D1 is a novel and selective inhibitor of
vascular endothelial growth factor receptor-2 tyrosine kinase with
potent activity in vitro and in vivo. Cancer Sci. 102:1374–1380.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Becker S, Bohn P, Bouyeure-Petit AC,
Modzelewski R, Gensanne D, Picquenot JM, Dubray B and Vera P:
Bevacizumab enhances efficiency of radiotherapy in a lung
adenocarcinoma rodent model: Role of αvβ3 imaging in determining
optimal window. Nucl Med Biol. 42:923–930. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wan W, Guo N, Pan D, Yu C, Weng Y, Luo S,
Ding H, Xu Y, Wang L, Lang L, et al: First experience of
18F-alfatide in lung cancer patients using a new
lyophilized kit for rapid radiofluorination. J Nucl Med.
54:691–698. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hu M, Xing L, Mu D, Yang W, Yang G, Kong L
and Yu J: Hypoxia imaging with 18F-fluoroerythronitroimidazole
integrated PET/CT and immunohistochemical studies in non-small cell
lung cancer. Clin Nucl Med. 38:591–596. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ji S, Zheng Y, Shao G, Zhou Y and Liu S:
Integrin αvβ3-targeted radiotracer
99mTc-3P-RGD2 useful for noninvasive
monitoring of breast tumor response to antiangiogenic linifanib
therapy but not anti-integrin αvβ3 RGD2 therapy.
Theranostics. 3:816–830. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Iagaru A, Mosci C, Mittra E, Zaharchuk G,
Fischbein N, Harsh G, Li G, Nagpal S, Recht L and Gambhir SS:
Glioblastoma multiforme recurrence: An exploratory study of
18F FPPRGD2 PET/CT. Radiology. 277:497–506.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Minamimoto R, Karam A, Jamali M,
Barkhodari A, Gambhir SS, Dorigo O and Iagaru A: Pilot prospective
evaluation of 18F-FPPRGD2 PET/CT in patients
with cervical and ovarian cancer. Eur J Nucl Med Mol Imaging.
43:1047–1055. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tong RT, Boucher Y, Kozin SV, Winkler F,
Hicklin DJ and Jain RK: Vascular normalization by vascular
endothelial growth factor receptor 2 blockade induces a pressure
gradient across the vasculature and improves drug penetration in
tumors. Cancer Res. 64:3731–3736. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Jain RK: Determinants of tumor blood flow:
A review. Cancer Res. 48:2641–2658. 1988.PubMed/NCBI
|
|
24
|
Kim KJ, Li B, Winer J, Armanini M, Gillett
N, Phillips HS and Ferrara N: Inhibition of vascular endothelial
growth factor-induced angiogenesis suppresses tumour growth in
vivo. Nature. 362:841–844. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Fukumura D and Jain RK: Tumor
microvasculature and microenvironment: Targets for
anti-angiogenesis and normalization. Microvasc Res. 74:72–84. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kang F, Wang S, Tian F, Zhao M, Zhang M,
Wang Z, Li G, Liu C, Yang W, Li X, et al: Comparing the diagnostic
potential of 68Ga-Alfatide II and 18F-FDG in
differentiating between non-small cell lung cancer and
tuberculosis. J Nucl Med. 57:672–677. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Iagaru A, Mosci C, Shen B, Chin FT, Mittra
E, Telli ML and Gambhir SS: 18F-FPPRGD2
PET/CT: Pilot phase evaluation of breast cancer patients.
Radiology. 273:549–559. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zhou Y, Kim YS, Lu X and Liu S: Evaluation
of 99mTc-labeled cyclic RGD dimers: Impact of cyclic RGD
peptides and 99mTc chelates on biological properties.
Bioconjug Chem. 23:586–595. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Zhou Y, Kim YS, Chakraborty S, Shi J, Gao
H and Liu S: 99mTc-labeled cyclic RGD peptides for
noninvasive monitoring of tumor integrin αVβ3
expression. Mol Imaging. 10:386–397. 2011. View Article : Google Scholar : PubMed/NCBI
|