Introduction
Papillary thyroid carcinoma (PTC) is the most common
type of differentiated thyroid carcinoma, accounting for more than
80% of all thyroid malignancies, presenting as a frequent type of
cancer in many parts of the world, including China (1–3). An
important characteristic of PTC is that it is prone to spread
through lymphatic ducts, resulting in recurrence, metastases, and
even patient death. Although multi-kinase or tyrosine kinase
inhibitors have been approved for the treatment of
radioiodine-refractory PTC (4), the
therapeutic choices are limited due in part to the lack of
understanding of the molecular characteristics and pathophysiology
of PTC (5,6). Therefore, it is critical to further
understand the molecular characteristics underlying PTC progression
in order to identify useful diagnostic biomarkers as well as
potential targets for therapy.
Squamous cell carcinoma antigens (SCCAs) are members
of the serpin family of endogenous protease inhibitors. The first
variant of SCCA (SCCA1) was initially found to be overexpressed in
squamous cell carcinoma (SCC) of the uterine cervix (7). A previous study showed that SCCA1 and
its isoform, SCCA2, were produced by two tandemly arranged genes
located on chromosome 18q21 (8),
being ~98 and 92% homologous at their nucleotide and amino acid
levels, respectively (9,10). Apart from being present in cervical
SCC, SCCA has been shown to be frequently overexpressed in tumors
of different histological types including breast carcinoma
(11), liver (12) and lung cancer (9,13),
head and neck carcinoma (14), and
esophageal cancer (15). In
addition, circulating SCCA is currently used as a valuable
predictor of node metastasis, response to treatment, and tumor
recurrence (16,17). The SCCA level has been shown to
predict pathological grade, disease stage, recurrence, and response
to both radiotherapy and chemotherapy. SCCA expression has also
been associated with poorly differentiated and advanced metastatic
SCCs (18,19). However, the biological role of SCCA
in PTC and its clinical significance have not been explored.
The Ras family of small GTPases, consisting of three
highly related members, K-Ras, H-Ras and N-Ras, is a central
regulator of growth, proliferation and differentiation processes in
virtually every nucleated cell. Being located in the inner leaflet
of the plasma membrane, Ras GTPases play an important role in the
transmission of signals through interaction with multiple
effectors. Activation of Ras is initiated by cell surface
receptors, which can induce Ras GEFs to exchange GDP with GTP on
Ras. Then Ras stimulates diverse downstream effectors, resulting in
the initiation of an array of cellular signaling networks,
including the RAF-1/MEK/ERK, PI3K/Akt/mTOR and Rac1/JNK pathways
(20–22). Collectively, Ras mutations and
pathway activation induce dramatic changes to cells including
promotion of proliferation, suppression of apoptosis, increased
cell invasiveness and metabolic rewiring (23).
Activating Ras mutations are found in ~25% of all
human tumors, but these three small GTPases are not mutated at
equivalent frequencies in cancer. Eighty-five percent of Ras-driven
cancers have activating mutations in K-Ras, while N-Ras and H-Ras
are mutated in 12 and 3%, respectively, of all cancers (24,25).
Ras mutations are common in pancreatic ductal tumors (26), colorectal tumors (27,28),
PTC (29,30) and lung cancer (31). In PTC, RAS mutations may promote
thyroid tumorigenesis through the verified Ras/Raf/MEK pathway or
through its interaction with the PI3K/AKT pathway (32). In addition, Ras mutations are
associated with tumor metastases in PTC (29,33).
Notably, in our previous study, Ras significantly increased SCCA
protein levels in colon cancer cell lines, and SCCA was found to be
transcriptionally upregulated by oncogenic Ras through the MAPK
pathway (34).
In the present study, we examined, using PTC cells,
xenograft models and PTC patient samples, the role of SCCA and Ras
in PTC progression and metastasis. Our data indicate that SCCA is
upregulated in human PTC tissues and is significantly correlated
with tumor stage. In mice, SCCA overexpression accelerated thyroid
cancer xenograft growth, while SCCA suppression reduced xenograft
growth. Furthermore, in in vitro studies, Ras upregulatedd
SCCA expression and promote cell proliferation, migration and
invasion in PTC cells. Notably, both Ras and SCCA protein are
overexpressed and are significantly associated with tumor stage in
PTC. Moreover, Cox correlation analysis showed that SCCA may be
used as an independent prognostic factor for PTC patients. In
conclusion, these results suggest that SCCA protein upregulated by
Ras accelerates the invasion and metastasis in PTC, and that SCCA
could be utilized as a potential target for PTC treatment.
Materials and methods
Human tissue samples and
follow-up
Human tissue samples were obtained through surgical
resection at Sun Yat-Sen Memorial Hospital of Sun Yat-Sen
University from June, 2006 to July, 2009. All tissue specimens were
collected, frozen and stored in liquid nitrogen until assayed. All
tissue samples were obtained with informed consent, and all
procedures were performed in accordance with the Internal Review
and the Ethics Board of the Sun Yat-Sen Memorial Hospital of Sun
Yat-Sen University. All clinical information was obtained from
patients during follow-up. Moreover, overall survival (OS) was
calculated as the time from the date of diagnosis to the date of
death or the date of the last follow-up (if death did not occur).
Disease-free survival (DFS) was calculated as the time from the
date of surgery to the date of the first recurrence or metastasis
after surgery (in patients with recurrence or metastasis) or to the
date of the last follow-up (in patients without recurrence and
metastasis). Lymph node recurrence-free survival (LNRFS) was
defined as the time from the date of surgery to the date of lymph
node relapse, and distant recurrence-free survival (DRFS) was
defined as the time from the date of surgery to the date of distant
recurrence. Clinical information of the samples is shown in detail
in Table I.
 | Table I.Clinicopathological features of the
papillary thyroid carcinoma (PTC) patients and SCCA expression. |
Table I.
Clinicopathological features of the
papillary thyroid carcinoma (PTC) patients and SCCA expression.
|
|
| SCCA
expression |
|
|
|---|
|
|
|
|
|
|
|---|
| Clinical
features | No. of patients
(N=258) | Low (n=122) n
(%) | High (n=136) n
(%) | χ2 | P-value |
|---|
| Sex |
|
Male | 92 | 43 (46.74) | 49 (53.26) | 0.017 | 0.8956 |
|
Female | 166 | 79 (47.59) | 87 (52.41) |
|
|
| Age, years |
|
<45 | 106 | 52 (49.06) | 54 (50.94) | 0.226 | 0.6344 |
|
≥45 | 152 | 70 (46.05) | 82 (53.95) |
|
|
| Tumor size
(cm) |
| ≤4 | 156 | 89 (57.05) | 67 (42.95) | 19.09 | 0.0001a |
|
>4 | 102 | 33 (32.35) | 69 (67.65) |
|
|
| Extrathyroid
invasion |
| No | 127 | 72 (56.69) | 55 (43.31) | 8.88 | 0.0029a |
|
Yes | 131 | 50 (38.17) | 81 (61.83) |
|
|
| Lymph node
metastasis (LNM) |
| No | 157 | 87 (55.41) | 70 (44.59) | 10.36 | 0.0011a |
|
Yes | 101 | 35 (34.65) | 66 (65.35) |
|
|
| Distant organ
metastasis (DOM) |
| No | 187 | 97 (51.87) | 90 (48.13) | 5.730 | 0.0167a |
|
Yes | 71 | 25 (35.21) | 46 (64.79) |
|
|
| TNM stage |
|
I–II | 120 | 69 (57.50) | 51 (42.50) | 9.38 | 0.0022a |
|
III–IV | 138 | 53 (38.41) | 85 (61.59) |
|
|
Immunohistochemistry (IHC)
SCCA protein expression was analyzed by
immunohistochemistry (IHC) on paraffin-embedded PTC tissue samples
as previously described in our study (35). Briefly, the specimens were cut into
5-µm sections and baked at 65°C for 30 min. The sections were
deparaffinized and antigenic retrieval was carried out. The
sections were treated with 3% hydrogen peroxide in methanol to
quench the endogenous peroxidase activity followed by incubation
with 1% bovine serum albumin to block the nonspecific binding. The
SCCA antibody (cat. no. ab154971, 1:100 dilution; Abcam, Cambridge,
MA, USA) was incubated with the sections overnight at 4°C. After
washing, the tissue sections were treated with biotinylated
secondary antibody (1:2,000; cat. no. 7074; Cell Signaling
Technology, Inc., Danvers, MA, USA) for 60 min at room temperature.
After rinsing with PBS, the slides were immersed for 2–5 min in DAB
(3,3′-diaminobenzidine) (Sigma-Aldrich; Merck KGaA, Darmstadt,
Germany) solution, then monitored under a microscope. The reaction
was terminated with distilled water. Slides were then
counterstained with hematoxylin, dehydrated and coverslipped.
IHC staining scores
The quantitative analysis of IHC staining was
performed for SCCA protein expression levels in tissue specimens.
Two experienced investigators scored independently all the slides
using a method previously described (35). Scores considered both the proportion
of positive-staining tumor cells and the staining intensity. The
proportion of positively stained tumor cells was graded as follows:
0 (no positive tumor cells), 1 (10% positive tumor cells), 2
(>10-50% positive tumor cells) and 3 (>50% positive tumor
cells). The cells at each intensity of staining were recorded on a
scale of 0 (no staining), 1 (weak staining, light yellow), 2
(moderate staining, yellowish brown) and 3 (strong staining,
brown). The staining index (SI) was calculated as follows: SI =
staining intensity × proportion of positively stained tumor cells.
Using this method of assessment, we evaluated SCCA expression in
tumor tissues by SI (scored as 0, 1, 2, 3, 4, 6 or 9). Cutoff
values to define the high and low expression of SCCA were chosen
based on a measure of heterogeneity with the log-rank test
statistics with respect to OS. SCCA staining was quantified using a
two-level grade system as follows: 0–3 indicates low expression and
4–9 indicates high expression. Mean optical density (MOD)
represents the strength of staining signals by measuring per
positive pixels.
Cell cultures and interference
assays
K1 and 293T cell lines were obtained from the
American Type Culture Collection (ATCC; Manassas, VA, USA) and
maintained in RPMI-1640 medium (Invitrogen; Thermo Fisher
Scientific, Inc., Waltham, MA, USA) supplementing with 10% fetal
bovine serum (FBS) at 37°C with 5% CO2 according to the
manufacturer's instructions. Ectopic SCCA or Ras expression in the
K1 cell line was achieved using retroviral vectors. Briefly, SCCA
or Ras cDNA was cloned into retroviral transfer plasmid pMSCv to
generate the pMSCv-SCCA or pMSCv-Ras expression vector, which was
co-transfected in 293T cells (ATCC) using standard calcium
phosphate transfection method. Thirty-six hours after the
co-transfection, supernatants were collected and incubated with the
K1 cells for 24 h for the following assays. Knockdown SCCA or Ras
cells were transfected with Lipofectamine 2000 (Invitrogen; Thermo
Fisher Scientific, Inc.) using siRNA (Shanghai GenePharma Co.,
Ltd., Shanghai, China) according to the manufacturer's
instructions. siRNA sequences of the sense strands were as follows:
siSCCA-1, 5′-GCACAACAGATTAAGAAGGTT-3′ and siSCCA-2,
5′-CCGCTGTAGTAGGGATTCGGAT-3′; siRas-1, 5′-GGACGAAUAUGAUCCAACATT-3′
and siRas-2, 5′-UGUUGGAUCAUAUUCGUCCTT-3′.
qPCR assays
RNA was extracted using TRIzol reagent and a reverse
transcription kit following the manufacturer's instructions
(Invitrogen; Thermo Fisher Scientific, Inc.). PCR reactions were
performed under the following conditions: Pre-denaturation at 94°C
for 7 min, denaturation at 94°C for 30 sec, annealing at 55°C for
30 sec, elongation at 72°C for 1 min and elongation at 72°C for 10
min. The primers for quantitative real-time PCR assay were: SCCA,
5′-CATTTGTTTGCTGAAGCCACTAC-3′ and 5′-CATGTTCGAAATCCAGTGATTCC-3′;
GAPDH, 5′-AAGGTCGGAGTCAACGGATTTG-3′ and
5′-CCATGGGTGGAATCATATTGGAA-3. All primers were synthesized by
Shanghai General Biotech, Co., Ltd. (Shanghai, China). GAPDH was
used as an endogenous control. The 2−ΔΔCq method was
used to quantify the relative mRNA amount (36).
Western blot assays
The samples were lysed in RIPA buffer consisting of
20 mM Tris-HCl (pH 7.9), 137 mM NaCl, 5 mM EDTA, 1 mM EGTA, and 1%
Triton X-100 that contained protease inhibitors for 20 min at 4°C,
and total protein concentration was measured using the BCA protein
assay kit (Thermo Fisher Scientific, Inc.). Twenty micrograms of
proteins was separated on a 10% SDS-PAGE and transferred onto
polyvinylidene fluoride (PVDF) membranes (Roche Diagnostics,
Indianapolis, IN, USA). Then, the membranes were blocked in 5% skim
milk in TBS-Tween buffer at room temperature for 2 h and incubated
with a primary antibody against SCCA (dilution 1:1,000; cat. no.
ab154971; Abcam), Ras (dilution 1:1,000; cat. no. 3339; Cell
Signaling Technology, Inc.) or GAPDH (dilution 1:2,000; cat. no.
ab9485; Abcam) at 4°C overnight. Then, the membranes were incubated
with HRP-conjugated secondary antibodies (dilution 1:1,000; cat.
no. 3056; Epitomics, Burlingame, CA, USA) at 4°C for 2 h. The
peroxidase activity was detected using Immobilon Western
Chemiluminescent HRP Substrate (EMD Millipore, Billerica, MA,
USA).
MTT assays
In brief, cell viability was evaluated in accordance
with the MTT method. K1 cells were seeded in 96-well plates at
3×104 ectopic expressed cells/ml and cultured for
pre-selected time-points. Then, the cells were incubated with 10 µl
of 0.5% MTT solution for 4 h at 37°C. The supernatant was
discarded, and 150 µl of dimethyl sulfoxide (DMSO) was added to
each well. The 96-well plates were shaken for 10 min until the
crystals dissolved completely. The absorbance was measured at a
wavelength of 490 nm using a microplate reader (Bio-Rad
Laboratories, Hercules, CA, USA).
Invasion and migration assays
Cells (1×106) were suspended in 200 µl
serum-free medium and seeded in the top chambers of 24-well
Transwell plates (Corning Inc., Corning, NY, USA) coated with 30 µl
Matrigel (BD Biosciences, Franklin Lakes, NJ, USA). The bottom
chambers of the Transwell plates were filled with 600 µl medium
containing 10% FBS. Cells were allowed to migrate for 48 h at 37°C.
After migration, cells in the top chambers were removed using a
cotton swab, and the cells which migrated to the bottom chambers
were fixed in 4% paraformaldehyde and stained with 0.1% crystal
violet (Sigma-Aldrich; Merck KGaA). The fixed and stained cells
were counted in three independent fields under a using an Olympus
BX51 microscope at ×100 magnification (Olympus Corp., Tokyo,
Japan). At least, three chambers were counted for each experiment.
For the migration assay, a similar protocol was followed except for
the replacement of the top chamber of the Transwell plate with an
uncoated chamber. The bottom chamber was filled with 700 µl medium
containing 10% FBS, and cells were allowed to migrate for 24 h.
Xenograft tumor experiments
K1 cells (1×107) with ectopic SSCA
expression were injected into the mammary fat pads of 6- to
8-week-old athymic female nude mice purchased from the Shanghai
Experimental Animal Center (Shanghai, China). Nine mice weighing
23–25 g were used, and they were maintained under SPF conditions at
20–26°C, relative humidity 40–70% and a 12-h light-dark cycle. All
food was treated with high temperature steam disinfection (60 min,
120°C). All water was acidified by hydrochloric acid and adjusted
to a pH between 2.5 and 2.8. All efforts were made to minimize
animal suffering. Tumor growth and progression were monitored for
more than 9 weeks. Tumor size was measured once a week by calipers,
and tumor volume was calculated as: Volume (mm3) =
length × width2 × 0.5. At the end of the experiment,
animals were euthanized by CO2 asphyxiation, and tumors
were carefully resected, weighed and stored for analysis.
Statistical analysis
Statistical analyses were performed with GraphPad
Prism 5.0 (GraphPad Software, Inc., La Jolla, CA, USA). The
Chi-squared test was used to analyze the associations between SCCA
expression and clinicopathological factors. Kaplan-Meier analysis
was used for overall survival (OS), disease-free survival (DFS),
lymph node recurrence-free survival (LNRFS) and distant
recurrence-free survival (DRFS) calculations. Cox regression
analysis determined the prognostic significance and pathologic
characteristics. The correlation between SCCA and Ras mRNA
expression was determined using the Pearson's correlation test. The
comparison of two independent groups was analyzed using Student's
t-tests. Multiple group comparisons were analyzed with one-way
ANOVA and Tukey's post hoc test. All statistical tests were
two-tailed, and P-values <0.05 were considered statistically
significant.
Results
SCCA protein expression correlates
with tumor stage and metastasis in the PTC patient samples
A total of 258 postoperative samples obtained from
patients diagnosed with different stages of PTC, based on the TNM
staging system (37), were
analyzed: Stage I (n=52), stage II (n=68), stage III (n=79) and
stage IV (n=59). The clinical features of the patients with high
and low levels of SCCA expression are summarized in Table I. Low SCCA expression was observed
in 47.29% (122/258) of the samples, while 52.71% (136/258) showed
high SCCA expression levels. In tumors >4 cm, 67.65% (69/102) of
the samples showed high SCCA expression, while only 32.35% (33/102)
of tumors showed low SCCA expression. Moreover, more than 50% of
patients (131/258) showed extra thyroid invasion. Moreover, 39.15%
of patients (101/258) presented with lymph node metastasis (LNM),
and 27.52% of patients (71/258) had distant organ metastasis (DOM).
Based on the TNM staging system, 46.51% of patients (120/258)
presented with a stage I+II disease, and 53.49% of patients
(138/258) with a stage III+IV disease.
As summarized in Table
I, there was a significant correlation between high SCCA
expression and tumor size (P=0.0001), extrathyroid invasion
(P=0.0029), lymph node metastasis (P=0.0011), distant organ
metastasis (P=0.0167), and TNM stage (P=0.0022). These results
indicate that SCCA expression is significantly correlated with
aggressive metastasis and progression in PTC.
Next, we explored whether SCCA expression levels are
correlated with tumor histologic features, by examining 28
non-cancerous tissues and 258 PTC tissues, including 52 stage I, 68
stage II, 79 stage III and 59 stage IV tissues, by IHC. SCCA
expression in non-cancerous tissues was low or non-detected. In
contrast, SCCA protein was highly expressed in higher stages of
PTC, compared with non-cancerous tissues (Fig. 1A). In addition, SCCA expression
increased as the stage of PTC increased. The mean optical density
(MOD) of SCCA staining among non-cancerous tissues and PTC
specimens of different stages is documented in Fig. 1B. Stronger SCCA staining was
observed as the PTC malignant stage degree increased
(P<0.05). In agreement with the IHC results, SCCA mRNA
levels, as determined by qRT-PCR assays, also increased and were
higher as the malignant degree increased (P<0.05;
Fig. 1C). To validate these
findings, we examined SCCA protein expression levels in PTC stages
I to IV by immunoblotting. Compared with lower stage PTC, SCCA
protein expression was markedly strong in higher stage tumors
(Fig. 1D). Noteworthy, there was a
significant correlation between high SCCA expression and lymph node
metastasis, and in most cases a strong SCCA staining was correlated
with tumors with lymph node metastasis (Fig. 1E). Moreover, the primary PTC with
LNM showed high SCCA mRNA level, compared with the tumors without
LNM (P<0.001). Collectively, our findings indicate that
higher SCCA expression levels are associated with PTC stage and
metastasis.
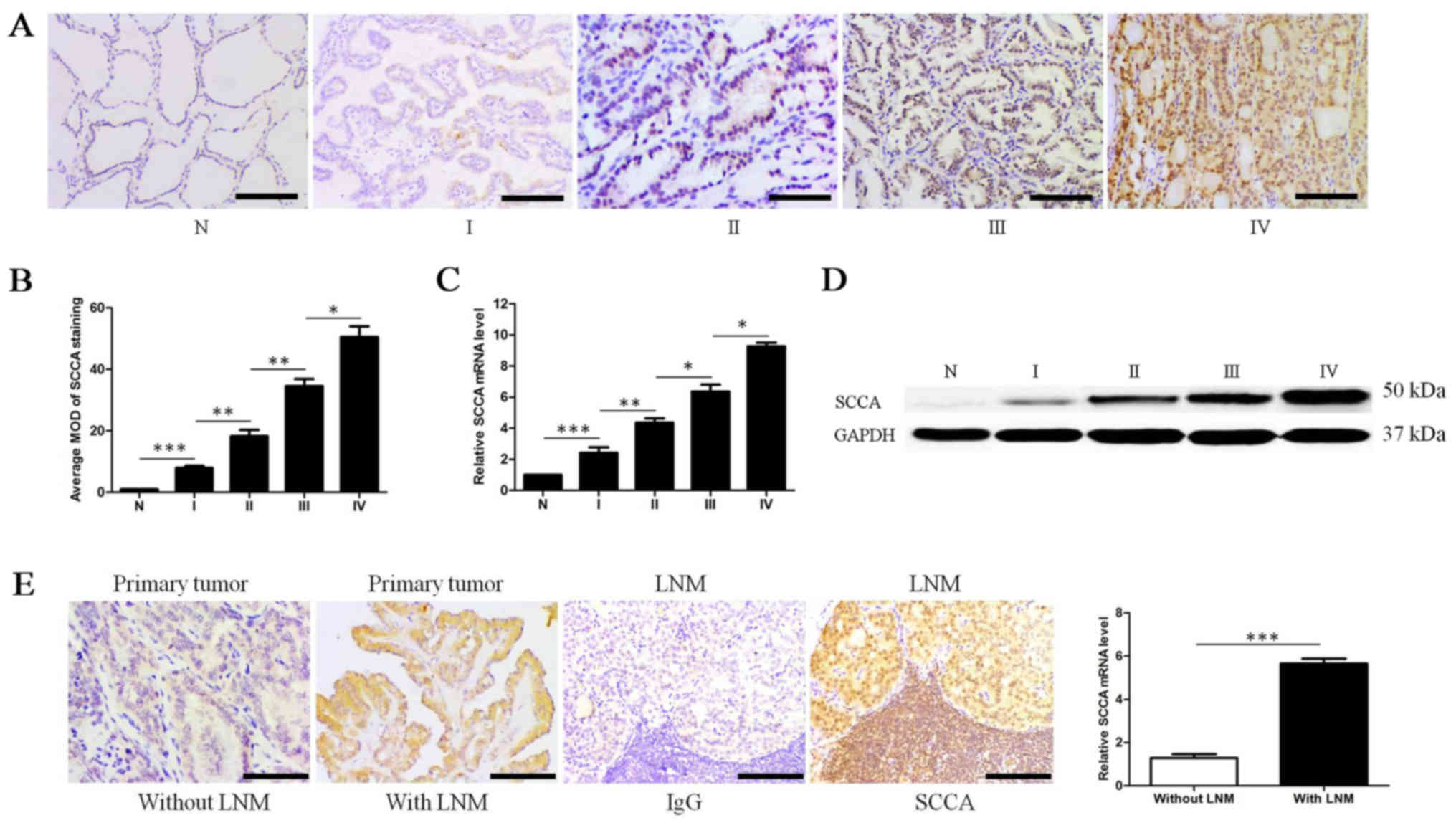 | Figure 1.SCCA expression levels are
significantly correlated with human PTC metastasis and progression.
(A) Representative images from IHC assays of paraffin-embedded
specimens of different stages of PTC and non-cancerous tissues.
Stage I (n=52), stage II (n=68), stage III (n=79), stage IV (n=59)
and non-cancerous (N) tissues (n=28) (IHC, magnification ×200,
scale bars, 100 µm). (B) SCCA expression is quantified as the mean
optical density (MOD) for SCCA staining among non-cancerous tissues
and various PTC stages (*P<0.05, **P<0.01, ***P<0.001,
one-way ANOVA). (C) SCCA mRNA expression levels in non-cancerous
tissues and PTC stages I to IV using qRT-PCR (*P<0.05,
**P<0.01, ***P<0.001, one-way ANOVA). (D) SCCA protein
expression levels in non-cancerous tissues and PTC stages I to IV
using western blot assay. (E) IHC staining in primary PTC without
lymph node metastasis (LNM), PTC with LNM and metastasis lymph node
(IHC, magnification ×200, scale bars, 100 µm; ***P<0.001,
Student's t-tests). SCCA, squamous cell carcinoma antigen; PTC,
papillary thyroid carcinoma; IHC, immunohistochemistry. |
SCCA expression and patient
survival
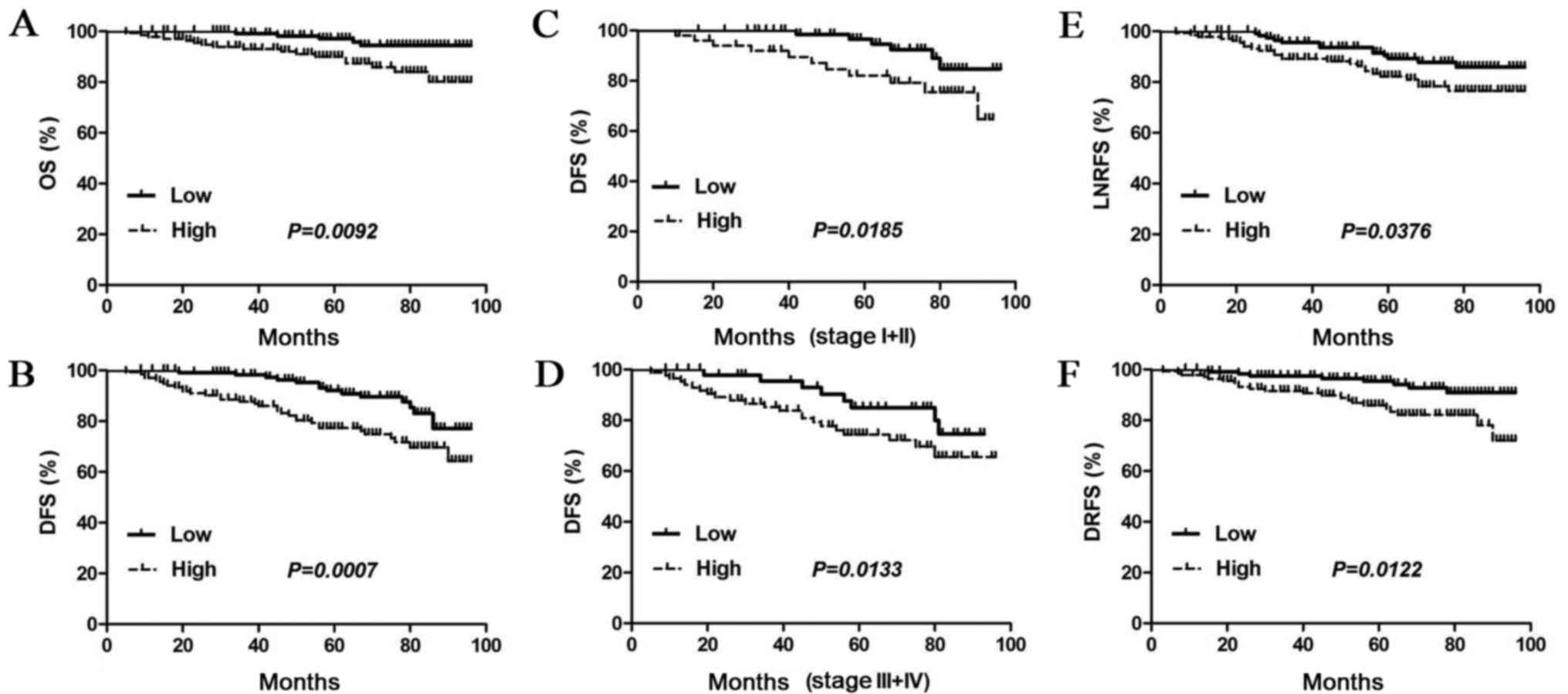
We next investigated whether a correlation exists
between SCCA levels in PTC and patient survival, using Kaplan-Meier
analysis. During the 8-year patient follow-up, the overall survival
(OS) rate was (119/136) 87.5% in the high SCCA expression group,
but it was (117/122) 95.9% in the low SCCA expression group
(P=0.0092; Fig. 2A). Our results
also indicate that SCCA overexpression was significantly correlated
with low disease-free survival (DFS) (P=0.0007; Fig. 2B). The prognostic value of SCCA
expression was also estimated in the various subgroups of PTC
patients, based on the TNM stage. In agreement with our previous
observations, DFS in PTC patients with high SCCA expression was
significantly reduced, compared to those with low SCCA expression
in either stages I+II subgroup (P=0.0185; Fig. 2C) or stages III+IV subgroup
(P=0.0133; Fig. 2D).
Since tumor metastasis plays an important role in
poor prognosis and reduced survival, the correlation was assessed
between SCCA expression and lymph node recurrence-free survival
(LNRFS) and distant recurrence-free survival (DRFS), by the
Kaplan-Meier method. We observed that SCCA expression was
significantly associated with LNRFS (P=0.0376; Fig. 2E) and DRFS (P=0.0122; Fig. 2F).
To determine whether SCCA expression could be
regarded as an independent prognostic factor, a Cox regression
analysis for DFS was performed (Table
II). Moreover, univariate analysis of the clinical features
revealed significant correlation between DFS and tumor size
(P=0.003), lymph node metastasis (LNM) (P=0.001), distant organ
metastasis (DOM) (P=0.012), extrathyroid invasion (P=0.018), SCCA
expression (P<0.001) and TNM stage (P=0.002).
Additionally, using a multivariate analysis, we observed
significant relationships between DFS and tumor size (P=0.015), LNM
(P=0.001), DOM (P=0.026), extrathyroid invasion (P=0.021), SCCA
expression (P<0.001) and TNM stage (P=0.003;
Table III), which were regarded
as significant prognostic factors for PTC patients. Taken together,
our findings indicate that SCCA protein may be considered as a
predictive prognostic factor in PTC patients.
| Table II.Univariate regression analysis of
disease-free survival (DFS) in the papillary thyroid carcinoma
(PTC) cases. |
Table II.
Univariate regression analysis of
disease-free survival (DFS) in the papillary thyroid carcinoma
(PTC) cases.
|
| PTC (N=258) |
|---|
|
|
|
|---|
| Clinical
features | HR (95% CI) | P-value |
|---|
| Age, years |
| 0.651 |
|
<45 | 1 |
|
|
≥45 | 1.975
(1.546–2.372) |
|
| Tumor size, cm |
| 0.003a |
| ≤4 | 1 |
|
|
>4 | 1.352
(0.926–3.356) |
|
| Lymph node
metastasis (LNM) |
| 0.001a |
| No | 1 |
|
|
Yes | 3.239
(1.651–5.563) |
|
| Distant organ
metastasis (DOM) |
| 0.012a |
| No | 1 |
|
|
Yes | 1.225
(0.367–2.328) |
|
| Extrathyroid
invasion |
| 0.018a |
| No | 1 |
|
|
Yes | 1.308
(0.563–3.265) |
|
| SCCA
expression |
|
<0.001a |
|
Low | 1 |
|
|
High | 2.879
(0.432–6.395) |
|
| TNM stage |
| 0.002a |
|
I–II | 1 |
|
|
III–IV | 2.331
(1.247–5.762) |
|
| Table III.Multivariate regression analysis of
disease-free survival (DFS) in the papillary thyroid carcinoma
(PTC) cases. |
Table III.
Multivariate regression analysis of
disease-free survival (DFS) in the papillary thyroid carcinoma
(PTC) cases.
|
| PTC (N=258) |
|---|
|
|
|
|---|
| Clinical
features | HR (95% CI) | P-value |
|---|
| Tumor size, cm |
| 0.015a |
| ≤4 | 1 |
|
|
>4 | 1.326
(0.128–3.876) |
|
| Lymph node
metastasis (LNM) |
| 0.001a |
| No | 1 |
|
|
Yes | 2.213
(1.868–5.387) |
|
| Distant organ
metastasis (DOM) |
| 0.026a |
| No | 1 |
|
|
Yes | 1.653
(0.238–3.552) |
|
| Extrathyroid
invasion |
| 0.021a |
| No | 1 |
|
|
Yes | 1.763
(0.342–3.652) |
|
| SCCA
expression |
|
<0.001a |
|
Low | 1 |
|
|
High | 3.487
(1.863–6.238) |
|
| TNM stage |
| 0.003a |
|
I–II | 1 |
|
|
III–IV | 2.365
(1.339–5.382) |
|
SCCA promotes PTC growth in vitro and
in vivo
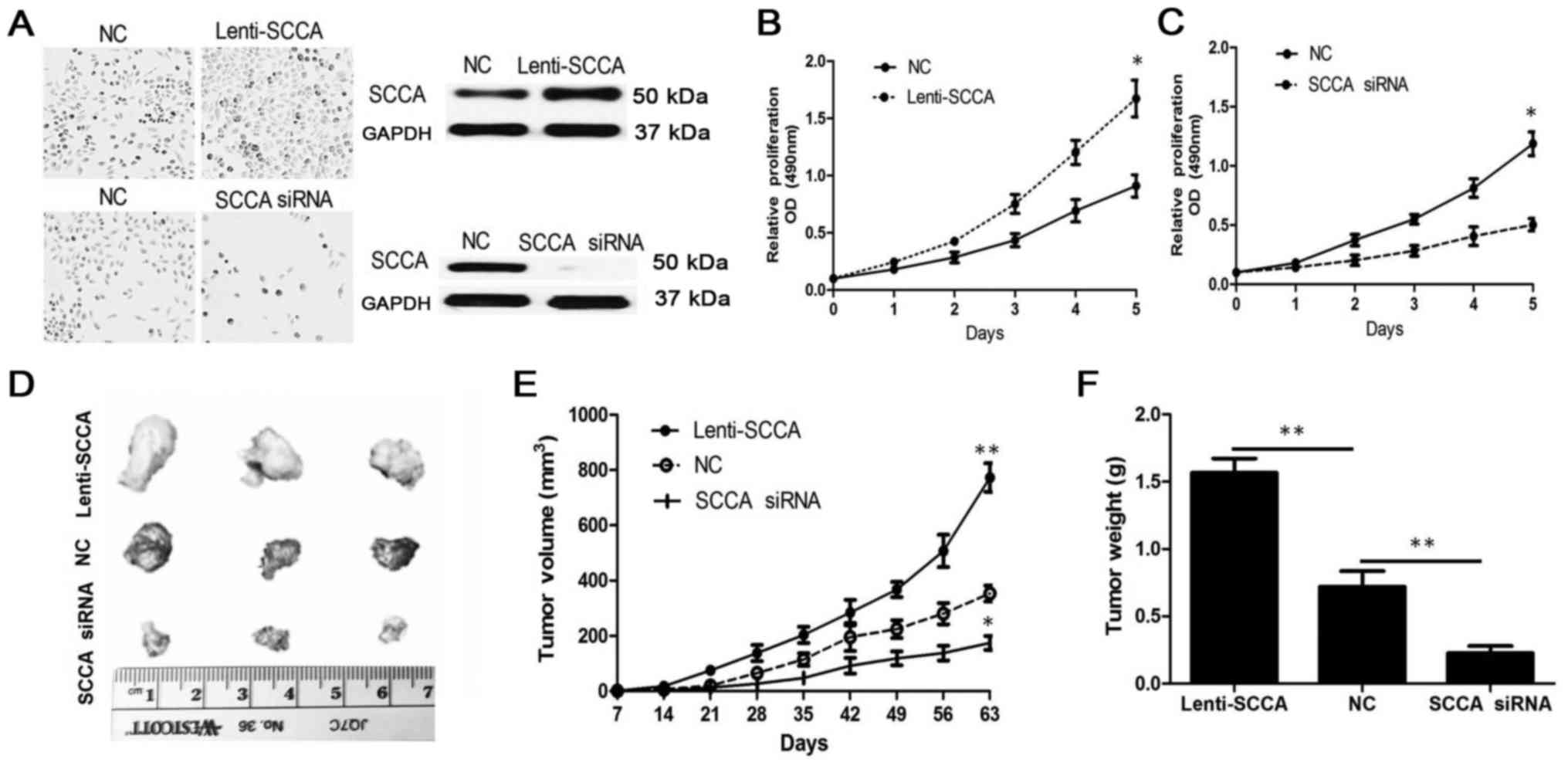
To evaluate whether SCCA plays an important role in
tumor growth, we performed SCCA overexpression and knockdown assays
using plasmid and specific siRNAs (Fig.
3A). SCCA overexpression significantly promoted K1 thyroid
cancer cell proliferation. In contrast, SCCA knockdown
significantly inhibited cell proliferation as demonstrated using
MTT assays in vitro (P<0.05; Fig. 3B and C). To assess whether SCCA was
involved in PTC growth in vivo, we performed a tumor
xenograft model using K1 cells, expressing different levels of SCCA
protein. Representative images of the xenograft tumors at 9 weeks
are shown (Fig. 3D). Nine weeks
following implantation, tumors in which SCCA was knocked-down
showed a reduced xenograft volume, while tumors with overexpressed
SCCA had accelerated growth, compared to the control
(P<0.05; Fig. 3E). In
agreement, SCCA knockdown decreased tumor weight, while SCCA
overexpression significantly increased tumor weight
(P<0.01; Fig. 3F). Taken
together, our data indicate that SCCA knockdown inhibits tumor
growth, suggesting that SCCA protein could represent a target for
PTC therapy.
SCCA promotes thyroid cancer cell K1
invasiveness in vitro
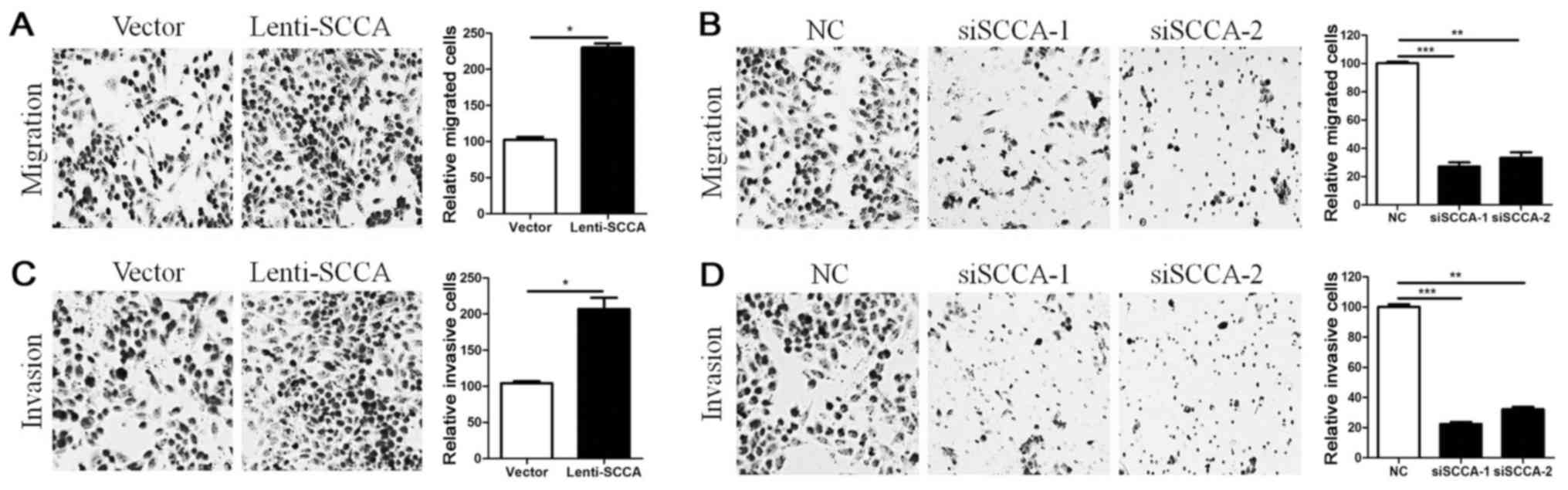
Tumor invasiveness is significantly correlated with
aggressive metastasis (6). To
determine whether the SCCA protein plays an important role in tumor
invasion, we performed migration and invasion assays in K1 cells
with overexpressed or silenced SCCA. Overexpression of SCCA
significantly increased K1 thyroid cancer cell migration, while
SCCA knockdown significantly reduced the migratory capability of
the K1 cells (P<0.05; Fig. 4A
and B). In addition, SCCA overexpression significantly promoted
the invasive capability of K1 thyroid cancer cells, while SCCA
knockdown significantly inhibited the invasion of K1 cells
(P<0.05; Fig. 4C and D).
Collectively, these data suggest that SCCA protein may be
associated with tumor metastasis.
Ras/SCCA pathway activation enhances
tumor proliferation and invasion
Genetic alterations in the mitogen-associated
protein kinase (MAPK) pathway play an important role in the
progression of PTC (29). In
addition, BRAF point mutations, RET/PTC oncogene rearrangements,
and RAS point mutations are frequent in advanced PTC and are
associated with poor prognosis (6,29,38).
Previously, it was shown that Ras activation upregulated SCCA
protein levels in colon cancer cell lines (34). However, whether Ras upregulates SCCA
protein in PTC remains unclear. For this reason, to determine
whether Ras upregulates SCCA protein to promote PTC progression, we
analyzed SCCA expression using an RAS overexpression plasmid and
specific siRas in vitro. Ras overexpression significantly
increased SCCA protein level, while Ras silencing markedly
decreased the SCCA protein level (Fig.
5A and B). In concordance, knockdown of Ras markedly decreased
SCCA mRNA levels, while Ras overexpression increased the mRNA level
of SCCA (P<0.01; Fig. 5C and
D). Moreover, Ras overexpression significantly enhanced K1
thyroid cancer cell proliferation and invasion in vitro,
while knockdown of Ras significantly suppressed cell proliferation
and invasion (P<0.01; Fig. 5E
and F). Noteworthy, Ras and SCCA mRNA expression levels
increased from stage I to IV with similar style in PTC tissues by
qRT-PCR assay (Fig. 5G). Moreover,
SCCA mRNA levels were significantly correlated with Ras levels in
PTC tissues (Fig. 5H, r=0.9449,
P<0.0001). Taken together, these results indicate that Ras could
upregulate SCCA expression to promote PTC proliferation and
invasion.
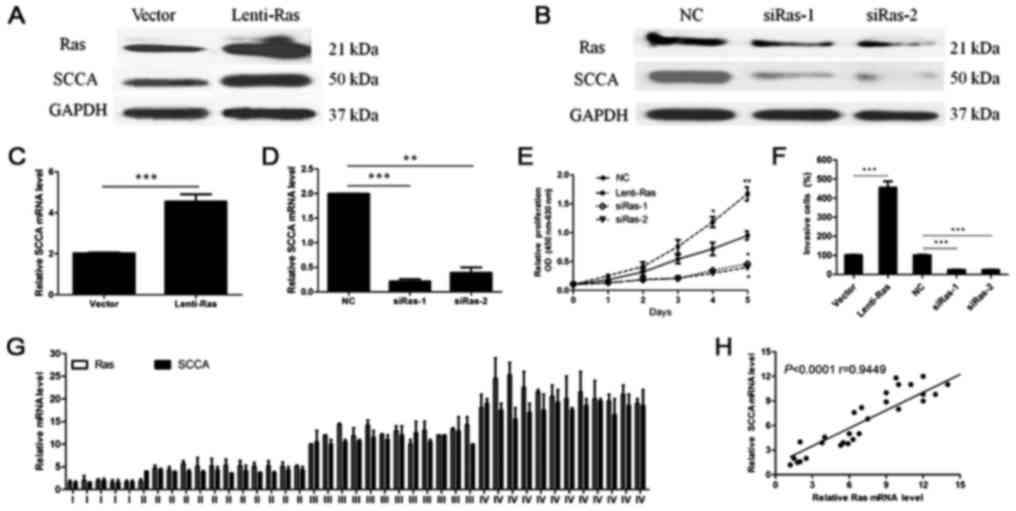 | Figure 5.Ras upregulates SCCA protein and
promotes PTC growth and invasion. (A and B) Ras overexpression
significantly increased SCCA protein levels, whereas Ras knockdown
markedly reduced SCCA expression. (C and D) Ras overexpression
increased SCCA mRNA levels, while Ras knockdown significantly
decreased SCCA mRNA levels (**P<0.01, ***P<0.001, Student's
t-tests or one-way ANOVA). (E and F) Ras overexpression
significantly promoted K1 cell proliferation and invasion, while
Ras knockdown significantly inhibited cell proliferation and
invasion in vitro (*P<0.05, **P<0.01, ***P<0.001,
one-way ANOVA). (G) Ras and SCCA mRNA expression increased from
stage I to IV in PTC tissues with a similar tendency by qRT-PCR,
including 5 stage I, 12 stage II, 12 stage III and 12 stage IV
samples. (H) SCCA expression is positively correlated with Ras
levels in PTC tissues (n=41, r=0.9449, P<0.0001). SCCA, squamous
cell carcinoma antigen; PTC, papillary thyroid carcinoma. |
Discussion
PTC, the most common cancer of the endocrine system,
accounts for the highest number of thyroid cancer cases diagnosed
in recent decades (39). Even
though PTC is usually curable and has a 5-year survival rate higher
than 95%, in some circumstances, PTC de-differentiates and becomes
aggressive, resulting in a poor prognosis. Therefore, novel PTC
biomarkers are needed to better predict patient prognosis and to
facilitate the development of personalized therapies for PTC
patients. In the present study, we identified SCCA as a critical
growth regulator and a target marker of PTC.
SCCA protein is a member of the serine protease
inhibitor family of proteins. Initially identified as an important
marker for advanced carcinomas of the cervix (18), SCCA has now been shown to have a
critical function in many cancer types, including breast (11), liver (12,16),
lung (13), head and neck carcinoma
(14), and esophageal cancers
(15). In agreement, we observed
that SCCA levels were significantly overexpressed in PTC, and were
correlated with the clinicopathological features of PTC. In
agreement with previous research, SCCA overexpression was
associated with high-grade breast carcinoma and was correlated with
estrogen receptor/progesterone receptor double-negative tumors as
well as with a poor prognosis for breast cancer patients (34).
To directly evaluate whether SCCA is critical to
tumor growth, we performed a genetic approach to knockdown and
overexpress SCCA in PTC cells. SCCA knockdown markedly inhibited
the proliferation of K1 thyroid cancer cells, while SCCA
overexpression accelerated xenograft tumor growth. Furthermore,
SCCA overexpression significantly increased K1 thyroid cancer cell
migration and invasion, while SCCA suppression reduced the
migratory and invasive capability of K1 cells. Similar observations
have been described in breast and cervical cancers, where SCCA was
associated with both advanced stage and strong invasive breast
carcinoma (11), and also
positively correlated with para-aortic lymph node metastasis in
cervical cancer (40). Moreover,
SCCA levels have also been shown to coincide to a degree with tumor
infiltration and frequency of lymph node metastasis in both
cervical and esophageal squamous cell carcinomas (41,42).
Mechanistically, it has been shown that SCCA increased tumor
invasiveness by promoting oncogenic transformation and
epithelial-mesenchymal transition (EMT) in breast cancer (43). Collectively, these findings support
a role for SCCA in PTC growth and invasiveness.
Lymph node metastasis is one of the most important
clinical features in treatment determination and prognosis for
cancer patients, including PTC. In PTC, despite being highly
curable and presenting a 10-year survival rate of more than 90%,
lymph node metastasis, especially in the neck, occurs in 20–50% of
all tumor patients and regional recurrence was observed in 5–20% of
patients who underwent total thyroidectomy (2). Our findings indicate a significant
correlation between high SCCA expression and lymph node metastasis,
and in most cases we observed a strong SCCA staining in primary
tumors with lymph node metastasis. In agreement, lymph node
metastasis has been shown to be the main factor affecting the
5-year overall survival rate of cervical cancer patients (44). The prognosis of cervical carcinoma
with common iliac lymph node metastasis was even poorer, with the
5-year overall survival rate of 25–47.8% (45). Moreover, the primary PTC with LNM
showed a higher SCCA mRNA level compared with the tumors without
LNM, suggesting that SCCA overexpression could be associated with
PTC stage and metastasis. Previous observation also suggested that
the SCCA level in serum is a prediction factor for lymph node
metastasis (46).
The Ras signaling pathway, a highly complex
signaling pathway, regulates tumor initiation and progression.
Recent evidence supports the notion that Ras oncoproteins
participate in the acquisition of tumor cells with EMT plasticity,
enhanced metastatic potential and poor patient survival (47). In thyroid cancer, BRAF and Ras
mutations as well as RET rearrangements recently have been given a
great deal of attention as novel prognostic markers for thyroid
carcinoma. Ras mutations seem to favorably activate the PI3K/AKT
pathway in thyroid tumorigenesis, as suggested by the preferential
association of RAS mutations with AKT phosphorylation in thyroid
cancers (38,48). We observed that Ras overexpression
significantly increased SCCA protein levels, while Ras knockdown
markedly decreased SCCA protein levels. Noteworthy, Ras and SCCA
mRNA expression levels increased from stage I to IV with similar
style in PTC tissues. Furthermore, SCCA mRNA levels were
significantly associated with the Ras levels in PTC tissues. These
results indicate that Ras enhances SCCA expression to promote PTC
proliferation and invasion.
In conclusion, our results indicate a critical role
for SCCA in PTC growth and invasion. SCCA protein is overexpressed
in PTC tissues, correlating with clinical stage and metastasis in
PTC. SCCA protein may be a predictive prognostic factor in PTC
patients. Moreover, activation of the Ras/SCCA pathway plays an
important role in promoting cancer cell proliferation and
metastasis in PTC.
Acknowledgements
Not applicable.
Funding
The present study was supported by grants from the
National Natural Science Foundation of China (no. 81702654) and the
Natural Science Foundation of Guangdong Province (no.
2017A030313642).
Availability of data and materials
The datasets used during the present study are
available from the corresponding author upon reasonable
request.
Authors' contributions
DL, YL and SL conceived the research project,
designed the experiments and edited the manuscript. DL, WZ, GGM, HL
and NO edited the manuscript and provided overall support for the
experimental process. DL, LT, ZD and XP performed the experiments
and collected the clinical samples. DL, ML and YZ analyzed the
results and conducted the statistical analysis of data. DL, YL and
GGM wrote and revised the manuscript. All authors read and approved
the manuscript and agree to be accountable for all aspects of the
research in ensuring that the accuracy or integrity of any part of
the work are appropriately investigated and resolved.
Ethics approval and consent to
participate
The present study was performed in accordance with
the policies of the Institutional Research Ethics Committee of Sun
Yat-Sen Memorial Hospital. Written informed consent was obtained
from the study participants at the Sun Yat-Sen Memorial Hospital of
Guangzhou City. All animal experiments were carried out under the
guidelines of the Sun Yat-Sen University Committee for Use and Care
of Laboratory Animals and approved by the Animal Experimentation
Ethics Committee of Sun Yat-Sen University.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no conflict of
interest.
Glossary
Abbreviations
Abbreviations:
|
SCCA
|
squamous cell carcinoma antigen
|
|
PTC
|
papillary thyroid carcinoma
|
|
LNM
|
lymph node metastasis
|
|
FBS
|
fetal bovine serum
|
|
IHC
|
immunohistochemistry
|
|
MOD
|
mean optical density
|
|
MAPK
|
mitogen-associated protein kinase
|
|
OS
|
overall survival
|
|
DFS
|
disease-free survival
|
|
LNRFS
|
lymph node recurrence-free
survival
|
|
DRFS
|
distant recurrence-free survival
|
References
|
1
|
Kim MJ, Won JK, Jung KC, Kim JH, Cho SW,
Park DJ and Park YJ: Clinical characteristics of subtypes of
follicular variant papillary thyroid carcinoma. Thyroid.
28:311–318. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sipos JA and Mazzaferri EL: Thyroid cancer
epidemiology and prognostic variables. Clin Oncol (R Coll Radiol).
22:395–404. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zheng R, Zeng H, Zhang S and Chen W:
Estimates of cancer incidence and mortality in China, 2013. Chin J
Cancer. 36:662017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Schmidbauer B, Menhart K, Hellwig D and
Grosse J: Differentiated thyroid cancer-treatment: State of the
art. Int J Mol Sci. 18(pii): E12922017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Nasef HO, Nixon IJ and Wreesmann VB:
Optimization of the risk-benefit ratio of differentiated thyroid
cancer treatment. Eur J Surg Oncol. 44:276–285. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chmielik E, Rusinek D, Oczko-Wojciechowska
M, Jarzab M, Krajewska J, Czarniecka A and Jarzab B: Heterogeneity
of thyroid cancer. Pathobiology. 85:117–129. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kato H, Morioka H, Aramaki S and Torigoe
T: Radioimmunoassay for tumor-antigen of human cervical squamous
cell carcinoma. Cell Mol Biol Incl Cyto Enzymol. 25:51–56.
1979.PubMed/NCBI
|
|
8
|
Schneider SS, Schick C, Fish KE, Miller E,
Pena JC, Treter SD, Hui SM and Silverman GA: A serine proteinase
inhibitor locus at 18q21.3 contains a tandem duplication of the
human squamous cell carcinoma antigen gene. Proc Natl Acad Sci USA.
92:3147–3151. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Vassilakopoulos T, Troupis T, Sotiropoulou
C, Zacharatos P, Katsaounou P, Parthenis D, Noussia O, Troupis G,
Papiris S, Kittas C, et al: Diagnostic and prognostic significance
of squamous cell carcinoma antigen in non-small cell lung cancer.
Lung Cancer. 32:137–144. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Guido M, Roskams T, Pontisso P, Fassan M,
Thung SN, Giacomelli L, Sergio A, Farinati F, Cillo U and Rugge M:
Squamous cell carcinoma antigen in human liver carcinogenesis. J
Clin Pathol. 61:445–447. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Catanzaro JM, Guerriero JL, Liu J, Ullman
E, Sheshadri N, Chen JJ and Zong WX: Elevated expression of
squamous cell carcinoma antigen (SCCA) is associated with human
breast carcinoma. PLoS One. 6:e190962011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Pontisso P: Role of SERPINB3 in
hepatocellular carcinoma. Ann Hepatol. 13:722–727. 2014.PubMed/NCBI
|
|
13
|
Zhao W, Yu H, Han Z, Gao N, Xue J and Wang
Y: Clinical significance of joint detection of serum CEA, SCCA, and
bFGF in the diagnosis of lung cancer. Int J Clin Exp Pathol.
8:9506–9511. 2015.PubMed/NCBI
|
|
14
|
Deng Z, Hasegawa M, Yamashita Y, Matayoshi
S, Kiyuna A, Agena S, Uehara T, Maeda H and Suzuki M: Prognostic
value of human papillomavirus and squamous cell carcinoma antigen
in head and neck squamous cell carcinoma. Cancer Sci.
103:2127–2134. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zheng X, Xing S, Liu XM, Liu W, Liu D, Chi
PD, Chen H, Dai SQ, Zhong Q, Zeng MS, et al: Establishment of using
serum YKL-40 and SCCA in combination for the diagnosis of patients
with esophageal squamous cell carcinoma. BMC Cancer. 14:4902014.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Guarino M, Di Costanzo GG, Gallotta A,
Tortora R, Paneghetti L, Auriemma F, Tuccillo C, Fassina G,
Caporaso N and Morisco F: Circulating SCCA-IgM complex is a useful
biomarker to predict the outcome of therapy in hepatocellular
carcinoma patients. Scand J Clin Lab Invest. 77:448–453. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Chen X, Wang X, He H, Liu Z, Hu JF and Li
W: Combination of circulating tumor cells with serum
carcinoembryonic antigen enhances clinical prediction of non-small
cell lung cancer. PLoS One. 10:e01262762015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Brioschi PA, Bischof P, Delafosse C and
Krauer F: Squamous-cell carcinoma antigen (SCC-A) values related to
clinical outcome of pre-invasive and invasive cervical carcinoma.
Int J Cancer. 47:376–379. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Cao L, Wang X, Li S, Zhi Q, Wang Y, Wang
L, Li K and Jiang R: PD-L1 is a prognostic biomarker in resected
NSCLC patients with moderate/high smoking history and elevated
serum SCCA level. J Cancer. 8:3251–3260. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Downward J: Targeting RAS signalling
pathways in cancer therapy. Nature Rev Cancer. 3:11–22. 2003.
View Article : Google Scholar
|
|
21
|
Schmukler E, Kloog Y and Pinkas-Kramarski
R: Ras and autophagy in cancer development and therapy. Oncotarget.
5:577–586. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ye K, Li J, Li X, Chang S and Zhang Z:
Ang1/Tie2 induces cell proliferation and migration in human
papillary thyroid carcinoma via the PI3K/AKT pathway. Oncol Lett.
15:1313–1318. 2018.PubMed/NCBI
|
|
23
|
Pylayeva-Gupta Y, Grabocka E and Bar-Sagi
D: RAS oncogenes: Weaving a tumorigenic web. Nature Rev Cancer.
11:761–774. 2011. View Article : Google Scholar
|
|
24
|
Cox AD and Der CJ: Ras history: The saga
continues. Small GTPases. 1:2–27. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Frodyma D, Neilsen B, Costanzo-Garvey D,
Fisher K and Lewis R: Coordinating ERK signaling via the molecular
scaffold Kinase Suppressor of Ras. F1000Res. 6:16212017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Eser S, Schnieke A, Schneider G and Saur
D: Oncogenic KRAS signalling in pancreatic cancer. Br J Cancer.
111:817–822. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Margonis GA, Kim Y, Sasaki K, Samaha M,
Amini N and Pawlik TM: Codon 13 KRAS mutation predicts patterns of
recurrence in patients undergoing hepatectomy for colorectal liver
metastases. Cancer. 122:2698–2707. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Christensen TD, Palshof JA, Larsen FO,
Poulsen TS, Høgdall E, Pfeiffer P, Jensen BV, Yilmaz MK and Nielsen
D: Associations between primary tumor RASBRAFPIK3CA mutation
status and metastatic site in patients with chemo-resistant
metastatic colorectal cancer. Acta Oncol. 57:1057–1062. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Zaballos MA and Santisteban P: Key
signaling pathways in thyroid cancer. J Endocrinol. 235:R43–R61.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Liang J, Cai W, Feng D, Teng H, Mao F,
Jiang Y, Hu S, Li X, Zhang Y, Liu B and Sun ZS: Genetic landscape
of papillary thyroid carcinoma in the Chinese population. J Pathol.
244:215–226. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Sanclemente M, Francoz S, Esteban-Burgos
L, Bousquet-Mur E, Djurec M, Lopez-Casas PP, Hidalgo M, Guerra C,
Drosten M, Musteanu M, et al: c-RAF ablation induces regression of
advanced Kras/Trp53 mutant lung adenocarcinomas by a
mechanism independent of MAPK signaling. Cancer cell. 33:217–228.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Xing M: Genetic alterations in the
phosphatidylinositol-3 kinase/Akt pathway in thyroid cancer.
Thyroid. 20:697–706. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ning L, Rao W, Yu Y, Liu X, Pan Y, Ma Y,
Liu R, Zhang S, Sun H and Yu Q: Association between the KRAS
gene polymorphisms and papillary thyroid carcinoma in a Chinese Han
population. J Cancer. 7:2420–2426. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Catanzaro JM, Sheshadri N, Pan JA, Sun Y,
Shi C, Li J, Powers RS, Crawford HC and Zong WX: Oncogenic Ras
induces inflammatory cytokine production by upregulating the
squamous cell carcinoma antigens SerpinB3/B4. Nat Commun.
5:37292014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Luo D, Chen H, Li X, Lu P, Long M, Peng X,
Lin S, Tan L, Zhu Y, Ouyang N, et al: Activation of the ROCK1/MMP-9
pathway is associated with the invasion and poor prognosis in
papillary thyroid carcinoma. Int J Oncol. 51:1209–1218. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2ΔΔCT method. Methods.
25:402–408. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Haugen BR, Alexander EK, Bible KC, Doherty
GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM,
Schlumberger M, et al: 2015 Αmerican thyroid association management
guidelines for adult patients with thyroid nodules and
differentiated thyroid cancer: The american thyroid association
guidelines task force on thyroid nodules and differentiated thyroid
cancer. Thyroid. 26:1–133. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Ming J, Liu Z, Zeng W, Maimaiti Y, Guo Y,
Nie X, Chen C, Zhao X, Shi L, Liu C, et al: Association between
BRAFRAS mutations, and RET rearrangements and the
clinical features of papillary thyroid cancer. Int J Clin Exp
Pathol. 8:15155–15162. 2015.PubMed/NCBI
|
|
39
|
La Vecchia C, Malvezzi M, Bosetti C,
Garavello W, Bertuccio P, Levi F and Negri E: Thyroid cancer
mortality and incidence: A global overview. Int J Cancer.
136:2187–2195. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Han X, Wen H, Ju X, Chen X, Ke G, Zhou Y,
Li J, Xia L, Tang J, Liang S, et al: Predictive factors of
para-aortic lymph nodes metastasis in cervical cancer patients: A
retrospective analysis based on 723 para-aortic lymphadenectomy
cases. Oncotarget. 8:51840–51847. 2017.PubMed/NCBI
|
|
41
|
Markovina S, Wang S, Henke LE, Luke CJ,
Pak SC, DeWees T, Pfeifer JD, Schwarz JK, Liu W, Chen S, et al:
Serum squamous cell carcinoma antigen as an early indicator of
response during therapy of cervical cancer. Br J Cancer. 118:72–78.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Fassan M, Realdon S, Vianello L, Quarta S,
Ruol A, Castoro C, Scarpa M, Zaninotto G, Guzzardo V, Chiarion
Sileni V, et al: Squamous cell carcinoma antigen (SCCA) is
up-regulated during Barrett's carcinogenesis and predicts
esophageal adenocarcinoma resistance to neoadjuvant chemotherapy.
Oncotarget. 8:24372–24379. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Sheshadri N, Catanzaro JM, Bott AJ, Sun Y,
Ullman E, Chen EI, Pan JA, Wu S, Crawford HC, Zhang J, et al:
SCCA1/SERPINB3 promotes oncogenesis and epithelial-mesenchymal
transition via the unfolded protein response and IL6 signaling.
Cancer Res. 74:6318–6329. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Huang L, Zheng M, Liu JH, Xiong Y, Ding H,
Tang L and Wang HY: Risk factors and prognosis of IB-IIB cervical
carcinoma with common iliac lymph node metastasis. Chin J Cancer.
29:431–435. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Aoki Y, Sasaki M, Watanabe M, Sato T,
Tsuneki I, Aida H and Tanaka K: High-risk group in node-positive
patients with stage IB IIA, and IIB cervical carcinoma after
radical hysterectomy and postoperative pelvic irradiation. Gynecol
Oncol. 77:305–309. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Yoon SM, Shin KH, Kim JY, Seo SS, Park SY,
Moon SH and Cho KH: Use of serum squamous cell carcinoma antigen
for follow-up monitoring of cervical cancer patients who were
treated by concurrent chemoradiotherapy. Radiat Oncol. 5:782010.
View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Tripathi K and Garg M: Mechanistic
regulation of epithelial-to-mesenchymal transition through RAS
signaling pathway and therapeutic implications in human cancer. J
Cell Commun Signal. 12:513–527. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Jeong SH, Hong HS, Kwak JJ and Lee EH:
Analysis of RAS mutation and PAX8/PPARg rearrangements in
follicular-derived thyroid neoplasms in a Korean population:
Frequency and ultrasound findings. J Endocrinol Invest. 38:849–857.
2015. View Article : Google Scholar : PubMed/NCBI
|