Introduction
Lung cancer is one of the most common malignancies
and is the leading cause of cancer-associated mortality worldwide
(1). In Korea, the incidence of lung
cancer has continuously increased and since 2005 it has been the
most frequent cause of cancer-associated mortality in both men and
women (2). Non-small cell lung cancer
(NSCLC) accounts for ~80% of all lung cancer cases, and it includes
adenocarcinoma, squamous cell carcinoma and large cell carcinoma.
Despite the advancements in different treatment strategies,
including surgery, chemotherapy, radiation and their combinations,
the prognosis of NSCLC has not been markedly improved, with a
5-year overall survival rate <20% (3).
The identification of several genetic mutations, the
so-called ‘growth drivers’ of NSCLC carcinogenesis, has led to the
development of targeted cancer therapy and the search for
biological markers for the prediction of therapy responses.
Epidermal growth factor receptor (EGFR) mutation is a key mechanism
of carcinogenesis in certain lung adenocarcinomas since it promotes
the growth and division of tumor cells through sustained activation
of a kinase receptor. Thus, inhibition of EGFR kinase activity with
drugs, such as gefitinib is an example of effective targeted
therapy (4–8). The KRAS gene mutation is considered
crucial for the carcinogenesis of various cancer types, including
NSCLC (9,10). KRAS can act in the downstream part of
the cellular signaling pathways, which is activated by mutant EGFR.
Therefore, increased KRAS activity in tumor cells due to mutations
is a well-known predictor of therapeutic resistance to EGFR
inhibitors; however, to the best of our knowledge, there are no
treatments that directly target KRAS activation yet (11–13). In
2007, a fusion of echinoderm microtubule-associated protein-like 4
(EML4) gene and anaplastic lymphoma kinase (ALK) gene, EML4-ALK,
was identified to be a strong carcinogenic factor leading to cell
proliferation and cancer development by increasing the kinase
activity of the ALK gene (14). The
ALK gene fusion has >20 partners but is most frequently
partnered with EML4 (15–17), and has been reported to occur in 2–10%
of all lung cancer patients, primarily in adenocarcinomas (18–22).
Although the EGFR mutation and ALK fusion may coexist in younger
and non-smoking patients with adenocarcinomas, the simultaneous
occurrence of EGFR mutation and ALK fusion has been reported to be
very rare and considered to be virtually exclusive (23–25).
Concerning the lung adenocarcinomas with EGFR mutation, numerous
studies have reported the clinicopathological features in Korean
patients (26–30); however, there has been a relatively
small number of studies regarding lung cancer cases with ALK fusion
in Korea (21,29–31),
partly because the National Health Insurance Service (NHIS) in
Korea did not start covering ALK inhibitor treatment for advanced
ALK-positive lung cancer until 2015. The first aim of the present
study was to evaluate the status of key driver mutations,
particularly the ALK rearrangement in Korean patients with NSCLC
and the associations with clinicopathological characteristics.
The current diagnostic methods for detection of ALK
fusion include florescence in situ hybridization (FISH),
immunohistochemistry (IHC), reverse transcription-quantitative PCR
(RT-qPCR) and next-generation sequencing (NGS) analyses. Until
recently the ALK FISH was the gold standard of diagnosis and the
ALK IHC or NGS analyses had limited uses as screening or auxiliary
tools. However, FISH has several well-known limitations. It is
labor-intensive, time-consuming and operator-dependent in both
preparation and interpretation processes (32). A number of studies have reported that
ALK IHC produces almost 100% concordant results with ALK FISH,
although there are always some discrepancies (22,33–35). After
the anti-ALK (D5F3) CDx assay (Ventana®) was approved as
a stand-alone ALK diagnostic test by the USA Food and Drug
Administration, a large study in 2017 reported that dichotomous ALK
IHC with D5F3 should be the standard diagnostic test to select
patients with NSCLC who benefit from ALK inhibitor treatment, since
it better predicted the tumor response rate and survival after
crizotinib treatment compared with ALK FISH (36). NGS enables prompt detection of various
genetic alterations, including ALK fusion, and is increasingly
cost-effective; it is expected to overtake the existing ALK
diagnostic tests. An evidence-based guideline for the molecular
diagnosis and treatment of lung cancer, jointly reported by the
International Association for the Study of Lung Cancer (IASLC),
College of American Pathologists (CAP), and Association for
American Molecular Pathology (AMP), recently reported that NGS
panels are preferred over single gene tests to identify other
treatment options beyond ALK, EGFR, and ROS1 inhibitors,
emphasizing the importance of NGS for the detection of genetic
alterations in lung cancer (37). In
Korea, the NHIS recently began to contribute to the cost of NGS
testing for cancer patients; however, it does not yet contribute to
the costs of targeted drug treatments, including ALK inhibitors,
according to the results of NGS analyses, partly due to the
insufficient data on NGS results of Korean patients with cancer.
Therefore, the second aim of the present study was to compare the
different diagnostic tests for ALK fusion in Korean patients with
lung cancer and to investigate the possibility of NGS as a new
standard ALK diagnostic test.
Materials and methods
Case selection and clinical data
collection
A total of 482 NSCLC specimens with ALK gene status
evaluated by FISH were collected and stored in the Biobank of Korea
University Guro Hospital between 2012 and 2018. The glass slides
were reviewed for histological diagnosis and immunohistochemical
features, including ALK (5A4; Novocastra), TTF-1 (8G7G3/1; Dako;
Agilent Technologies, Inc.), and napsin A (polyclonal; Cell
Marque). The formalin-fixed paraffin-embedded (FFPE) tissue blocks
of 10 patients, stored for <3 years to minimize the degradation
of DNA and RNA, were selected for NGS analysis, and consisted of
five ALK FISH-positive and five ALK FISH-negative adenocarcinomas
(38,39). The clinical information included age,
sex, smoking history, cancer stage according to the 8th Edition of
the American Joint Committee on Cancer staging manual, genetic
mutation status and survival. All the glass slides, paraffin blocks
and clinical information were provided by the Human Biobank of
Korea University Guro Hospital, which collects patients' samples
and medical information at the time of biopsies or surgical
excisions of their tumors, with the written informed consent for
future research use. The present study was conducted with the
approval of the Institutional Review Board of Korea University Guro
Hospital (approval no. 2018GR0357).
NGS analysis
HiSeq or MiSeq of Illumina, Inc. and Iron Torrent of
Thermo Fisher Scientific, Inc. are the most widely used NGS
platforms. A number of researchers prefer MiSeq of Illumina, Inc.
due to its high diversity of gene selection and its ability to
obtain large amounts of genetic information. However, when it is
used with customized cancer panels, high quality DNA of ≥200–300 ng
is required. In addition, the device is costly, operator-dependent
and labor-intensive. Whereas, Ion Torrent, even though the
selection range is limited, is cost-effective and can be used with
low quality DNA if the target gene is spared. Sequencing with
Ampliseq Cancer Hotspot Panel enables targeted sequencing from 10
ng of DNA; however, frequent errors and missing copy number
variations (CNVs) are disadvantages (38,40).
Therefore, selection of an appropriate platform depends on the
purpose of the experiment, and the quantity and quality of the DNA
extracted from the available samples. The present study selected
the Miseq system (Illumina, Inc.) with customized cancer panels to
obtain a large amount of genetic information.
For DNA analyses, the paraffin tissue blocks
containing enough, viable tumor cells were selected and sectioned
to a thickness of 10 µm. The DNA was extracted with Qiagen GeneRead
DNA FFPE kit (Qiagen Sciences, Inc.). The sample purity was
evaluated by the absorbance ratio at 260/280 and the samples with a
ratio between 1.8 and 2.1 were considered appropriate for further
analyses. The DNA integrity numbers (DINs) of samples were measured
by Agilent 4200 TapeStation system (Agilent Technologies, Inc.) and
those with a DIN >3 were selected for further analysis. The DNA
library construction, target sequence hybridization and
purification of captured sequences were conducted using
xGen® Lockdown® probes and reagents
(Integrated DNA Technologies, Inc.) and Dynabeads M-270
Streptavidin (Thermo Fisher Scientific, Inc), according to the
manufacturers' protocols. The 80 different oncogenes included in
the DNA hybridization probes are presented in Table SI. Following target hybridization and
purification, the sequencing and analysis of captured DNA fragments
was performed using Illumina MiSeq system with MiSeq Reagent kit v3
(Illumina, Inc.). Sample concentrations were measured using a
Qubit® 3.3 Fluorometer (Thermo Fisher Scientific, Inc.)
and Qubit™ dsDNA HS assay kit (Thermo Fisher Scientific, Inc.). The
final concentrations for sequencing were adjusted to 10–12 pM with
volumes between 350 and 420 µl.
The RNA analyses were conducted through similar
processes to those of the DNA analysis, except for the early
ribosomal RNA (rRNA) removal and complementary DNA (cDNA) library
construction steps. The paraffin tissue blocks were sectioned to a
thickness of 10 µm. Total RNA was extracted with Qiagen RNeasy FFPE
kit (Qiagen Science, Inc.). The sample purity was evaluated by the
absorbance ratio at 260/280 and those with a ratio between 1.8 and
2.1 were considered appropriate for further analyses. The
DV200 of samples, the fraction of RNA >200
nucleotides, was measured with Agilent 4200 TapeStation system
(Agilent Technologies, Inc.) and only those samples with a
DV200>70% were selected for further analysis
according to the manufacturer's guidelines. The rRNA was depleted
from the total RNA samples using NEBNext® rRNA Depletion
kit (New England Biolabs, Inc.), and then the RNA samples were
amplified by RT-PCR to produce cDNA samples. Subsequently, the cDNA
library construction, target sequence hybridization and
purification were conducted using xGen®
Lockdown® probes and reagents (Integrated DNA
Technologies, Inc.) and Dynabeads M-270 Streptavidin (Thermo Fisher
Scientific, Inc.), according to the manufacturers' protocols. The
30 different oncogenes included in the hybridization probes are
presented in Table SII. The
sequencing and analysis of captured cDNA fragments were performed
using Illumina MiSeq system with MiSeq Reagent kit v3 (Illumina,
Inc.), with the same sample concentrations as for the DNA
analysis.
Statistical analysis
Fisher's exact test and Pearson's χ2 test
were used for the statistical analyses. P<0.05 was considered to
indicate a statistically significant difference. To compare
survival data, Kaplan-Meier survival analysis and a log-rank test
were performed. All statistical analyses were performed with SPSS
version 18 (SPSS, Inc.).
Results
Clinicopathological features
Between 2012 and 2018, 482 patients underwent ALK
FISH analysis with small biopsies or surgically excised specimens
of primary or metastatic NSCLC. For all patients, sections from the
FFPE tissue or cell blocks, but no cytological materials or body
fluid samples, were used for FISH or other molecular studies. The
majority of the patients had adenocarcinoma (n=451) and only a
small number had other histological types, including adenosquamous
carcinoma (n=7), squamous cell carcinoma (n=11), large cell
carcinoma (n=8) and pleomorphic carcinoma (n=5). This was partly
because the NHIS in Korea only covers the cost of ALK FISH analysis
for patients with adenocarcinoma histology. The majority of the
patients with other histological types had been suspected of having
adenocarcinoma in small biopsies but confirmed as otherwise in
excised specimens or with additional immunohistochemical studies.
All 39 patients (8.1%) who were diagnosed as ALK FISH-positive had
adenocarcinomas. The mean age of the ALK FISH-positive patients was
60.7 years (range, 34–80 years). This was significantly younger
than the mean age of ALK FISH-negative patients with or without
concurrent EGFR mutation (66.6 years; P<0.001). The male to
female ratio in the ALK FISH-positive patients was 1.44 (23:16),
while it was 1.79 (284:159) in the ALK-negative patients. The
proportion of females was significantly higher in the ALK
FISH-positive patients (P<0.001). The smoking history of the ALK
FISH-positive and -negative patients demonstrated no statistically
significant difference (P>0.5). Of the ALK FISH-positive
patients, 21 were never-smokers, and the remaining 18 had a history
of smoking, ranging between 6 and 200 pack years. However, when the
EGFR mutation-positive patients were removed from the ALK
FISH-negative group, and the ALK FISH-positive group was compared
with the ALK FISH−/EGFR mutation-negative group, the
proportion of never-smokers were significantly higher in ALK
FISH-positive group (P<0.001) (Table
I).
 | Table I.Clinicopathological characteristics
of patients according to the ALK fusion and EGFR mutation
status. |
Table I.
Clinicopathological characteristics
of patients according to the ALK fusion and EGFR mutation
status.
|
| ALK FISH-positive
(n=39) | ALK FISH-negative
and EGFR mutation-negative (n=329) | ALK FISH-negative
and EGFR mutation-positive (n=114) | ALK IHC-positive
(n=74) |
|---|
| Sex |
|
Male | 23 (59.0%) | 198 (60.2%) | 70 (61.4%) | 38 (51.4%) |
|
Female | 16 (41.0%) | 131 (39.8%) | 44 (38.6%) | 36 (48.6%) |
| Smoking
history |
|
|
|
|
|
Never | 21 (53.8%) | 141 (42.9%) | 72 (63.2%) | 39 (52.7%) |
|
Previous or current | 18 (46.2%) | 188 (57.1%) | 42 (36.8%) | 35 (47.3%) |
| Mean age | 60.7 years | 66.5 years | 64.3 years | 63.7 years |
| Nodal
metastasis | 31 (79.5%) | 223 (67.8%) | 72 (63.2%) | 58 (78.4%) |
| Tumor stage |
|
|
|
|
| I | 6
(15.4%) | 83
(25.2%) | 37 (32.5%) | 7 (9.5%) |
| II | 3 (7.7%) | 30 (9.1%) | 15 (13.2%) | 10 (13.5%) |
|
III | 9
(23.1%) | 59
(17.9%) | 21 (18.4%) | 25 (33.8%) |
| IV | 21 (53.8%) | 157 (47.7%) | 41 (36.0%) | 32 (43.2%) |
| 1-year
mortality | 16 (41.0%) |
|
| 31 (41.9%) |
At the time of diagnosis, the ALK FISH-positive
tumors were significantly associated with more frequent nodal
metastases (n=31; 79.5%) compared with ALK FISH-negative cases
(n=295; 66.6%) (P<0.001). A total of 30 ALK FISH-positive
patients (77.0%) had unresectable stage III tumors with mediastinal
metastases or stage IV with distant tumor spread at the time of
diagnosis, whereas among the ALK FISH−/EGFR
mutation-negative (n=215; 65%) and ALK FISH-negative/EGFR
mutation-positive patients (n=62; 54.4%) less proportions exhibited
stage III and IV diseases (P<0.001); and only 6 ALK
FISH-positive patients could undergo a lobectomy for stage I or II
disease. This indicates that ALK FISH-positive cancer cases were
more advanced compared with ALK FISH-negative cases at the time of
diagnosis. In total, 16 ALK FISH-positive patients (41.0%)
succumbed to the disease within 1 year of diagnosis, while 92 ALK
FISH-negative patients (20.8%) succumbed to the disease in the same
period (P<0.001) (Table I). All
patients were treated with surgery, chemotherapy, radiation and
targeted therapeutic agents according to the tumor stage and
genetic mutation status. Of the 39 ALK FISH-positive patients, 12
were treated with ALK inhibitors. Among them, 7 patients received
crizotinib as first-line therapy, whereas the others were treated
with various chemotherapeutic agents and/or radiation before
starting treatment with an ALK inhibitor. No patient could undergo
surgical resection due to the advanced tumor stage. All 12 patients
started ALK inhibitor treatment after 2015, and those who received
first-line ALK inhibitor therapy started after 2017 according to
the NHIS approval for payment. The duration of treatment ranged
between 1 and 24 months. Overall, 1 patient had to stop crizotinib
treatment after 1 month of administration due to severe
hepatotoxicity. Another patient, who had been heavily treated with
various chemotherapeutic regimens and radiation before ALK
inhibitor treatment, demonstrated partial response to crizotinib
and ceritinib for 13 months, then returned to chemotherapy due to
disease progression, succumbed to the disease 3 months later.
Considering that only a small number of patients had tried ALK
inhibitor drugs, and an even lower number had received it as
first-line treatment, it was considered that the influence of
treatment with an ALK inhibitor on the survival of patients would
not be substantial in the present study.
Of the 482 patients evaluated by ALK FISH, 313 were
also evaluated by ALK (5A4) IHC staining. A total of 74 tumors were
positively stained for ALK (23.6%), and among them 27 were also ALK
FISH-positive. The concordance rate between ALK FISH and IHC in the
present study was 81.2%. The clinicopathological features of ALK
IHC-positive patients were similar to those of ALK FISH-positive
patients. The mean age was 63.7 years. At the time of diagnosis, 58
patients had nodal metastases (78.4%) and 57 had stage III or IV
diseases (77.0%). The number of patients who succumbed to the
disease within 1 year of diagnosis was 31 (41.9%) (Table I).
Since all patients suspected of having lung
adenocarcinoma were also evaluated for EGFR mutation status at the
Korea University Guro Hospital, all 482 patients tested for ALK
FISH were also evaluated for EGFR mutation by peptide nucleic acid
(PNA) clamping real-time PCR method, and 114 patients were positive
for EGFR mutation (23.7%). Among the 39 ALK FISH-positive patients,
none were positive for EGFR mutation. The unexpectedly low
EGFR-positive rate in the present study may be because the patients
were first selected among those who underwent ALK FISH analysis and
therefore, not all patients who underwent EGFR mutation tests were
included. Therefore, the clinicopathological features according to
the EGFR mutation status in the present study may also exhibit some
discrepancies with the generally understood characteristics of EGFR
mutation-positive lung cancer. Nevertheless, the comparisons of
clinicopathological features among ALK FISH-positive, ALK
FISH−/EGFR mutation-negative, and EGFR mutation-positive
patients in the present study are summarized in Table I.
Histopathological features
Due to the aforementioned reason, adenocarcinoma
(n=451) was the most frequent histological type of cancer included
in the present study. The glass slides were reviewed for subtype
identification of adenocarcinoma. Numerous patients only had
biopsies and the histological subtypes of the entire tumor could
not be evaluated. Nevertheless, a number of tumors demonstrated
mixed patterns of more than two subtypes, even in small biopsy
specimens. The ALK FISH-positive adenocarcinomas exhibited various
histological subtypes, including solid (n=26), acinar (n=14),
cribriform (n=5), micropapillary (n=5), papillary (n=4), mucinous
(n=4), and enteric (n=1) types. The most frequently observed solid
pattern was present in 66.7% of ALK FISH-positive lung
adenocarcinomas and the proportion was significantly higher
compared with that identified in ALK FISH-negative tumors (38.3%)
irrespective of EGFR mutation status (P<0.0001). Notably, among
the tumors with solid growth pattern, the proportions of ALK
FISH-positive and EGFR mutation-positive cancers demonstrated no
significant difference. The presence of the mucinous type was more
frequent in ALK FISH-positive adenocarcinomas compared with ALK
FISH-negative adenocarcinomas (P=0.0401). The cribriform pattern
was significantly more frequent in ALK FISH-positive
adenocarcinomas (14.3%) compared with in ALK FISH-negative tumors
(5.4%; P<0.001). However, considering the EGFR mutation status,
the difference was maintained only between ALK FISH-positive tumors
and ALK FISH-negative/EGFR mutation-positive adenocarcinomas
(P=0.0121), but not between ALK FISH-positive and ALK
FISH-negative/EGFR mutation-negative cases (P=0.0804). The EGFR
mutation also influenced the presence of acinar, papillary and
lepidic subtypes, which were significantly more frequent in ALK
FISH-negative/EGFR mutation-positive adenocarcinomas compared with
in ALK FISH-positive or ALK FISH-negative/EGFR mutation-negative
tumors. In addition, among the tumors exhibiting acinar, papillary,
or lepidic growth, the presence of EGFR mutation was significantly
more frequent than ALK fusion. The histological subtypes observed
in adenocarcinomas according to the ALK and EGFR mutation status
are summarized in Table II.
| Table II.Histopathologic subtypes of
adenocarcinomas according to the ALK and EGFR mutation status. |
Table II.
Histopathologic subtypes of
adenocarcinomas according to the ALK and EGFR mutation status.
| Histological | ALK FISH-positive
adeno-carcinomas | ALK
FISH-negative/EGFR mutation-negative adenocarcinomas | ALK
FISH-negative/EGFR mutation-positive adenocarcinomas | Ratio of ALK FISH
positive adenocarcinnomas according to the histological | Ratio of EGFR
mutation-positive adenocarcinnomas according |
|---|
| Subtypes | (n=39) (%) | (n=298) (%) | (n=114) (%) | subtype (%) | to the histological
subtype (%) |
| Solid | 26 (66.7) | 131 (44.0) | 27 (23.7) | 14.1 | 14.7 |
| Acinar | 14 (35.9) | 98
(32.9) | 72 (63.2) |
7.6 | 39.1 |
| Papillary | 4
(10.3) | 31
(10.4) | 26 (22.8) |
6.6 | 42.6 |
|
Micro-papillary | 5
(14.3) | 57
(19.1) | 31 (27.2) |
5.4 | 33.3 |
| Cribriform | 5
(14.3) | 16 (5.4) | 2 (1.8) | 21.7 |
8.7 |
| Mucinous | 4
(10.3) | 25 (8.4) | 2 (1.8) | 12.9 |
6.5 |
| Enteric | 1 (2.6) | 3
(1.0) | 0 (0.0) | 25.0 |
0.0 |
| Lepidic | 0 (0.0) | 20 (6.7) | 15 (13.2) |
0.0 | 42.9 |
Immunohistochemical features
The ALK FISH-positive adenocarcinomas were
frequently positive for thyroid transcription factor 1 (TTF-1;
n=34; 87.2%) and napsin A (n=29; 74.4%). TTF-1 expression was
significantly more frequent in ALK FISH-positive tumors than in ALK
FISH-negative/EGFR mutation-negative tumors (P=0.0361), but not
compared with in ALK FISH-negative/EGFR-positive cases (P=0.0544).
Between the ALK FISH-positive and negative tumors, napsin A
expression demonstrated no statistically significant difference
(P=0.0694); however, the ALK FISH-negative/EGFR mutation-positive
adenocarcinomas expressed napsin A significantly more frequently
than ALK FISH-positive adenocarcinomas (P=0.0046), although in both
groups napsin A expression was very frequent (Table III).
| Table III.The immunohistochemical features of
adenocarcinomas according to the ALK fusion and EGFR mutation
status. |
Table III.
The immunohistochemical features of
adenocarcinomas according to the ALK fusion and EGFR mutation
status.
|
| ALK
FISH-positive | ALK
FISH-negative/EGFR mutation-negative | ALK
FISH-negative/EGFR mutation-positive |
|---|
| TTF-1 | 34/39 (87.2%) | 199/279
(71.3%) | 105/109
(96.3%) |
| Napsin | 29/39 (74.4%) | 154/231
(66.7%) | 86/93 (92.5%) |
NGS
The present study analyzed five ALK FISH-positive
and five ALK FISH-negative adenocarcinomas with customized cancer
DNA and RNA panels (Tables SI and
SII). The DNA cancer panel consisted
of 80 genes associated with single nucleotide variant (SNV), CNV,
and insertion and deletion (INDEL) mutations, and the RNA panel
included 30 genes associated with gene translocation and/or fusion.
All samples for DNA analyses revealed >600× coverages, which
were enough to detect variants of 5% frequency. All samples for RNA
analyses revealed 1,000× coverages, enough for detection of gene
fusions.
Among the patients with ALK FISH-positive
adenocarcinomas, two cases of EML4-ALK translocation were detected,
which were also positive in the ALK IHC analysis. However, three
ALK FISH-positive tumors demonstrated no RNA fusion abnormalities.
In total, 1 patient exhibited an EGFR L858R mutation, which was not
detected in PNA clamping, and another had an ERBB2 exon 20
insertion (A775_G776 in YVMA) which had not been tested before.
Among the ALK FISH-negative patients, none exhibited ALK fusion in
NGS. Furthermore, 1 patient was identified to have TPM3-NTRK1
translocation, which had not been tested before. One EGFR exon 19
deletion which had also been detected in PNA clamping, one ERBB2
exon 20 insertion (A775_G776 in YVMA) and one KRAS G12D mutation
were identified in 1 patient each. Since the KRAS or ERBB2 mutation
test has not been allowed in patients with lung cancer by the NHIS
in Korea, the majority of patients in the present study, including
those with KRAS G12D or ERBB exon 20 insertion detected by NGS, had
not been tested before. The comparison of the results of ALK FISH,
ALK IHC, EGFR PNA clamping and NGS analysis are summarized in
Table IV. The results of ALK FISH,
ALK IHC and NGS demonstrated significant differences, and the EGFR
PNA clamping and NGS DNA analysis also demonstrated some
discordance. Considering the NGS results only, patients with ALK
fusion-positive adenocarcinomas exhibited no mutations in other
oncogenes such as EGFR, BRAF, and KRAS; however, those with no ALK
alteration demonstrated frequent genetic mutations in EGFR, ERBB2
and KRAS, even with the small number of cases tested.
| Table IV.Comparison of the results of ALK
FISH, ALK IHC, EGFR PNA clamping and NGS analysis. |
Table IV.
Comparison of the results of ALK
FISH, ALK IHC, EGFR PNA clamping and NGS analysis.
|
|
|
|
|
|
| NGS analysis |
|---|
|
|
|
|
|
|
|
|
|---|
|
| Sex | Age | ALK FISH | ALK IHC | EGFR PNA
clamping | RNA | DNA |
|---|
| Case 1 | M | 63 | Positive (18/50;
36.0%) | Positive | Wild | EML4-ALK | None |
| Case 2 | F | 53 | Positive (8/50;
16.0%) | Negative | Wild | None | EGFR L858R |
| Case 3 | F | 53 | Positive (8/50;
16.0%) | Negative | Wild | None | ERBB2 Ins |
| Case 4 | F | 74 | Positive (11/50;
22.0%) | Positive | Wild | None | None |
| Case 5 | F | 44 | Positive (25/50;
50%) | Positive | Wild | EML4-ALK | None |
| Case 6 | F | 71 | Negative | Negative | 19Del | None | EGFR 19 Del |
| Case 7 | M | 53 | Negative | Negative | Wild | TPM3-NTRK1 | None |
| Case 8 | F | 49 | Negative | Negative | Wild | None | KRAS G12D |
| Case 9 | F | 53 | Negative | Negative | Wild | None | ERBB2 Ins |
| Case 10 | F | 73 | Negative | Positive | Wild | None | None |
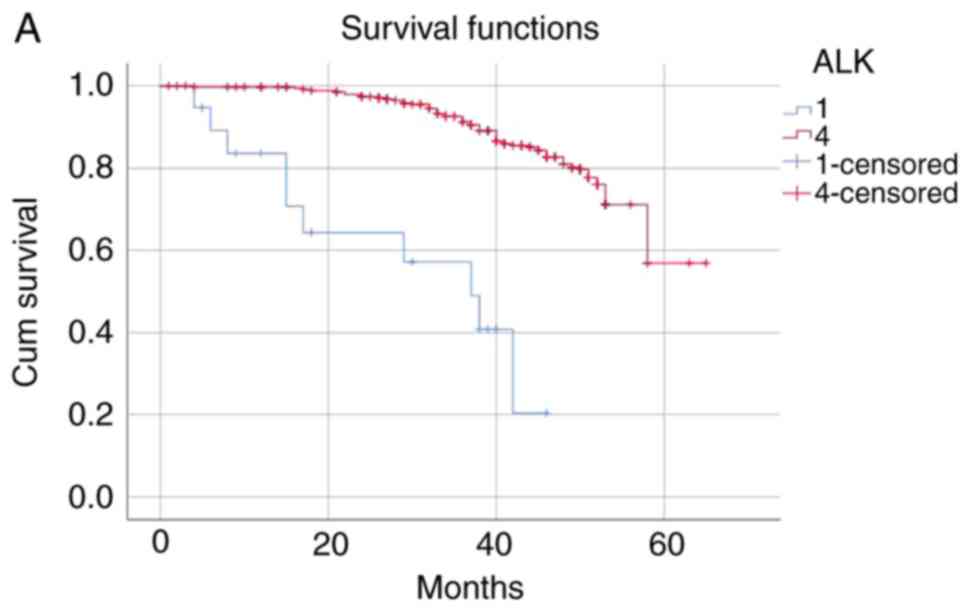
Survival analysis
The patients were categorized into the following
four groups according to the ALK fusion detection methods and their
results: i) Both ALK FISH- and ALK IHC-positive (n=27); ii) only
ALK FISH-positive (n=12); iii) only ALK IHC-positive (n=47); and
iv) both ALK FISH− and ALK IHC-negative (n=227). The
mean survival time of the ALK FISH−/IHC-positive group
was 40.42 months and that of the ALK FISH−/IHC-negative
group was 56.96 months. The negative group survived significantly
longer than the positive group (P<0.001). The mean survival time
was 34.41 months in the ALK FISH-negative/IHC-positive group and
40.72 months in the ALK FISH-positive/IHC-negative group,
indicating that the only ALK IHC-positive patients died
significantly earlier than the only ALK FISH-positive patients
(P<0.001; Table V and Fig. 1). The median follow-up time was 46.35
months.
| Table V.The mean survival months of patients
according to the ALK fusion detection methods and their
results. |
Table V.
The mean survival months of patients
according to the ALK fusion detection methods and their
results.
|
|
|
| 95% confidence
interval |
|---|
|
|
|
|
|
|---|
| Patient group | Mean | Standard error | Lower bound | Upper bound |
|---|
| 1 | 30.172 | 3.713 | 22.896 | 37.449 |
| 2 | 40.718 | 3.446 | 33.963 | 47.473 |
| 3 | 34.412 | 2.020 | 30.452 | 38.372 |
| 4 | 56.962 | 1.270 | 54.472 | 59.451 |
Discussion
In 2018, the World Conference on Lung Cancer
reported the results of the first interim analysis from the ALTA-1L
study, which compared the next-generation ALK inhibitor brigatinib
and the traditional first-line ALK inhibitor drug crizotinib
(41,42). ALTA-1L was a phase III, randomized,
open-labeled, comparative, multicenter, international study with
275 participants who had ALK fusion-positive, locally advanced or
metastatic NSCLC and had not been previously treated with an ALK
inhibitor. The primary endpoint, progression-free survival (PFS),
assessed by a double-blinded independent central review, was
significantly longer among patients who received brigatinib than
those who received crizotinib. The estimated 12-month PFS was 67%
[95% confidence interval (CI), 56–75] in the brigatinib group and
43% (95% CI, 32–53) in the crizotinib group, and brigatinib was
associated with a 51% lower risk of disease progression or
mortality compared with crizotinib [(hazard ratio, 0.49; 95% CI,
0.33–0.74); P<0.001]. Currently, three ALK target therapeutic
drugs have been approved in Korea, crizotinib
(Xalkori®), alectinib (Alecensa®), and
ceritinib (Zykadia®). Only crizotinib was approved as a
first-line drug, while the other drugs are limited to second-line
treatment. With the results of the ALTA-1L trial, there is an
expected shift in generations among ALK target drugs in Korea.
Investigations regarding the development of new drugs targeting ALK
or other genetic alterations in cancer are proceeding rapidly and
frequently as joint research with large pharmaceutical companies
occurs. However, compared with the fast evolution of ALK-targeting
treatment, the development of diagnostic methods of ALK aberration
has been slow. Until recently, ALK FISH has been used as the gold
standard for the detection of ALK fusion, and ALK IHC or NGS have
only been used as screening tools or adjunctive diagnostic methods.
Only recently has the Ventana® anti-ALK (D5F3) CDx assay
been considered a more advanced diagnostic method compared with
traditional ALK IHC, and it has been approved in Korea as an
ALK-testing method for selecting patients eligible for crizotinib.
In the case of NGS, although it is the newest technology, with
continuous development of platforms and data analysis methods
enabling rapid and simultaneous detection of various genetic
alterations including ALK fusion, its use has been minimal due to
the high cost and incomplete coverage by the NHIS in Korea.
Prompt and accurate diagnosis of genetic alterations
including ALK fusion can provide patients with the administration
of appropriate drugs and thereby improve disease prognosis.
Therefore, the present study investigated clinical,
histopathological and immunohistochemical features that may be
associated with ALK alteration and searched for other genetic
changes that may accompany ALK fusion in NSCLC. The present study
also investigated whether NGS, the promising, new method, could
replace the traditional method of ALK FISH for the detection of
ALK-positive NSCLC. Both ALK fusion and EGFR mutation were more
frequent in tumors in never-smokers. The ALK IHC- or ALK
FISH-positive tumors were similarly associated with younger patient
age, female patients, frequent nodal metastases and advanced stage
(III or IV) at the time of diagnosis and higher 1-year mortality.
The more advanced disease with frequent nodal and distant
metastases at the time of diagnosis could explain the higher 1-year
mortality and shorter survival in patients with ALK fusion-positive
adenocarcinomas; however, definite evidence that ALK fusion was an
independent poor prognostic factor was not identified in the
present study. Several studies have attempted to clarify whether
ALK fusion is an independent risk factor for poor prognosis in
cancers; however, the results have been inconsistent thus far
(18,43,44).
Although the positive rates of TTF-1 and napsin A
immunohistochemical staining were significantly higher than those
of other antibodies in ALK fusion-positive tumors, the relevance of
these markers to ALK fusion could not be demonstrated since both
TTF-1 and napsin A are well-known markers for lung adenocarcinoma
and are also expressed in quite a high proportion of
adenocarcinomas with no ALK fusion. However, in 2017, a study
reported that the overall survival was significantly longer in
stage IV patients with TTF-1-positive adenocarcinomas than in
patients with TTF-1-negative tumors (18 vs. 9 months) (45). Considering that the patients with ALK
fusion-positive cancers frequently had either advanced stage III or
IV diseases, TTF-1 may act as a marker with prognostic value in
these patients.
Although the NGS analysis in the present study
revealed no concurrent mutations in EGFR, BRAF, and KRAS in the ALK
fusion-positive adenocarcinomas, and historically ALK rearrangement
is considered a virtually exclusive event with other driver
mutations (23,25,44),
several studies have revealed that more than two driver mutations
can occur in a small portion of lung adenocarcinomas (24,29,46). In
ALK fusion-negative tumors, different types of EGFR-activating
mutations, ERBB2 insertion, KRAS mutation and TPM3-NTRK1 fusion
were detected by NGS in one, two, one and one cases, respectively.
It may have been due to the small number of cases submitted to the
NGS analysis in the present study that no concurrent mutations were
detected in ALK fusion-positive tumors. The NTRK1 gene, which
encodes the high-affinity nerve growth factor receptor TRKA
protein, has been known to fuse with various partners at low
frequency and act as an oncogenic driver in different malignancies,
including lung adenocarcinoma, colorectal adenocarcinoma, papillary
thyroid carcinoma, neuroblastoma, prostate adenocarcinoma, and
breast carcinoma (47–49). NPM3-NTRK1 is a type of oncogenic TRK1
fusion gene, which can be detected in various cancers, including
lung adenocarcinoma, colorectal carcinoma and papillary thyroid
carcinoma, and it is inhibited by TRK1 inhibitors, such as
entrectinib and larotrectinib (50–54). The
ERBB2 mutations, known as oncogenic drivers, are identified in 2–4%
of NSCLCs, particularly adenocarcinomas of young and non-smoking
women (55–57). Constitutive activation of ERBB2 gene
by mutation causes overexpression of HER2 protein and subsequent
activation of downstream PI3K/AKT and MEK/ERK signaling pathways,
which leads to carcinogenesis (58).
The ERBB exon 20 insertion identified in the present study is
understood to be the most common type of ERBB2 mutation in lung
cancer (57,59,60).
Studies evaluating the possibility of HER2-targeted treatment for
lung cancer have been conducted and it may be possible that
HER2-targeted antibodies or tyrosine kinase inhibitors could be a
novel therapeutic approach for lung cancer in the future (61–63).
Simultaneous detection of multiple oncogenic alterations, such as
TRK1 fusion or ERBB2 mutation, is one of the strongest advantages
of NGS testing. No genetic changes had been previously detected in
those tumors with NPM3-TRK rearrangement or ERBB2 mutation prior to
NGS in the present study.
Concerning the EGFR mutation, the results of NGS
demonstrated a 90% agreement with those of the PNA clamping method.
However, three out of five ALK FISH-positive tumors were negative
in the NGS RNA panel analysis. The diagnostic agreement rate
between ALK FISH and NGS RNA panel analysis was only 70%, while the
agreement rate between ALK IHC and NGS was 80% (Table IV). Although the number of patients
submitted to NGS analysis was small, such discrepancies among the
three detection methods for ALK fusion cast doubts on the
reliability of various detection methods and the overwhelming
excellence of any one approach. Investigating the three ALK
FISH-positive but NGS-negative cases more closely, it was
identified that the rearrangement-positive cells, i.e., with
abnormal split signals under fluorescence microscopy, were 16% each
in two cases and 22% in the other case, all falling within or close
to the range of borderline positivity of 10 to 20% (Table IV), which has been known as the
primary source of discrepancy between FISH and other modalities
(64,65). The ALK IHC results in these patients
were negative in two and positive in one. The FFPE blocks selected
for NGS analysis were relatively fresh and contained enough viable
tumor cells. The quantity and quality of the RNA samples were
sufficient for NGS analyses. Therefore, in those two patients with
ALK FISH-positive/ALK IHC-negative/NGS-negative tumors, it was
assumed that the results of ALK FISH were false-positive. The
borderline FISH positivity of 16% and the concordant negativity in
ALK IHC and NGS also seemed supportive of this conclusion. These
patients did not receive ALK inhibitor therapy. However, the third
patient with ALK FISH-positive/ALK IHC-positive/NGS-negative
disease started crizotinib treatment based on the FISH result and
exhibited partial response and stable disease for 13 months prior
to commencement of this study. Therefore, it was concluded that the
NGS result was false-negative in this patient. The targeted RNA
sequencing by NGS is known to be sensitive enough to detect gene
fusions with FFPE tissue (39).
However, various factors, including fixation time, specimen size
during fixation, and storage temperature and duration, can
influence the RNA quality from FFPE samples (39,66).
Although the RNA sample of the third patient was extracted from the
FFPE block stored at consistent room temperature for only 13 months
and exhibited a DV200 value sufficiently high for
Illumina sequencing, it still could have been degraded in the
process of fixation and storage due to some unknown causes. The
present study used stored FFPE tissue blocks that were not expected
to be used for NGS analysis. However, if NGS is used routinely for
the detection of genetic alterations and all specimens are
processed from the fixation step to minimize the degradation of
genetic material and submitted to NGS analysis without prolonged
storage, it is expected that the test accuracy would be improved.
Currently, considering the discrepancies among the results of ALK
FISH, IHC and NGS, it can be concluded that no one detection method
is completely reliable. Therefore, it would be reasonable to more
frequently add other testing methods to ALK FISH for the accurate
diagnosis of ALK fusion-positive lung cancer, even though the ALK
FISH has been considered the standard diagnostic method for a long
time.
The present study assumed that the ALK test results
would be more reliable when two different modalities, for example
FISH and IHC, agreed with each other. Thus, during Kaplan-Meier
survival analysis, it was reasonably concluded that ALK
fusion-positive lung cancer had a worse prognosis compared with ALK
fusion-negative disease; the mean survival time was 30.17 months in
patients with tumors positive for both ALK FISH and IHC and 56.96
months in those with tumors negative for both ALK FISH and IHC.
However, in certain patients the results of ALK FISH and IHC were
discordant, and the mean survival time was 40.72 months in ALK
FISH-positive/IHC-negative patients and 34.41 in ALK
FISH-negative/IHC-positive patients. The present study considered
the possibility that this difference in the survival periods could
reflect the accuracy of FISH and IHC tests, and the ALK
IHC-positive group could include more ALK fusion-positive patients
than the ALK FISH-positive group. However, also considering that
the positive rate of ALK IHC was much higher in the present study
than the previously determined ALK fusion-positive rate in lung
cancer (19–24), the ALK FISH-negative/IHC-positive
group may also include a number of false-positive cases. The
shorter survival period could be due to other clinicopathological
features, such as frequent nodal metastasis and advanced stage,
which were frequent in this group. This high positive rate of ALK
IHC was the result of staining with clone 5A4. It was hypothesized
that the relatively weak stainability of this clone in NSCLC could
have made it difficult to differentiate between weakly stained
tumor cells and background staining, resulting in frequent
false-positive cases (67).
Nonetheless, the present study suggests that ALK
FISH and IHC should be used together for more accurate results, and
NGS analysis with an advantage of simultaneous detection of
different mutations could also be considered an alternative to ALK
FISH as the diagnostic standard. In the present study, TPM3-NTRK1
fusion or ERBB2 mutation, which were not anticipated at the time of
diagnosis, were first detected in NGS analysis with a rather high
frequency even in the small number of cases submitted. Even if a
patient is known to have TPM3-NTRK1 fusion, they would not be able
to receive tyrosine kinase inhibitor treatment, such as
entrectinib, in Korea due to the lack of drug approval and coverage
by the NHIS. Likewise, patients with ERBB2 mutations would not have
access to HER2-targeted drugs at the time of diagnosis. However,
considering the speed of the discovery of new therapeutic targets
and the development of appropriate drugs, additional NGS results,
even with no proper treatment at the time of diagnosis, would be
helpful for future treatment decisions while monitoring the
progress of the patient.
The present study confirmed that ALK-rearranged lung
adenocarcinomas have characteristic clinical, histological and
immunohistochemical features. Rapid and accurate diagnosis of ALK
rearrangement is closely associated with the treatment and
prognosis of patients. The present results emphasized that in
practice ALK testing should be diversified; ALK FISH and IHC should
be used concurrently to complement each other, and NGS analysis
could be a good alternative of FISH. These conclusions were in
agreement with the new molecular testing guideline for the
selection of lung cancer patients for treatment with targeted
tyrosine kinase inhibitors, which was jointly reported by
IASLC/AMP/CAP, in that the role of ALK IHC and/or NGS analysis
could be expanded further in clinical practice (39).
Supplementary Material
Supporting Data
Acknowledgements
We are sincerely grateful to Dr Ensel Oh for her
technical advice on selecting an appropriate next-generation
sequencing platform and troubleshooting during experiments.
Funding
Not applicable.
Availability of data and material
The datasets used and analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
BKS designed the study and reviewed and analyzed the
histological and immunohistochemical features of submitted cases.
WCC reviewed and analyzed the clinical data of patients, conducted
statistical analyses, and performed the experiments. HKK
contributed to the analysis and interpretation of the experimental
and clinical data. All authors drafted, reviewed, edited, read and
approved the manuscript and agree to be accountable for all aspects
of the research in ensuring that the accuracy or integrity of any
part of the work are appropriately investigated and resolved.
Ethics approval and consent to
participate
This study was conducted with the approval of the
Institutional Review Board of Korea University Guro Hospital
(Approval no. 2018GR0357). The clinical information including age,
sex, smoking history, cancer stage, genetic mutation status and
survival was obtained through the Human Biobank of Korea University
of Guro Hospital, without identifiable personal data, according to
the approved protocol by the Institutional Review Board of Korea
University Guro Hospital.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
National Cancer Information Center (NCIC),
. Main Cancer Mortality Fraction in 2017. https://cancer.go.kr/lay1/S1T645C647/contents.do
|
|
3
|
Noone AM, Howlader N, Krapcho M, Miller D,
Brest A, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, et al:
SEER Cancer Statistics Review, 1975–2015National Cancer Institute;
Bethesda, MD: 2017
|
|
4
|
Fukui T and Mitsudomi T: Mutations in the
epidermal growth factor receptor gene and effects of EGFR-tyrosine
kinase inhibitors on lung cancers. Gen Thorac Cardiovasc Surg.
56:97–103. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Tamura K, Okamoto I, Kashii T, Negoro S,
Hirashima T, Kudoh S, Ichinose Y, Ebi N, Shibata K, Nishimura T, et
al: Multicentre prospective phase II trial of gefitinib for
advanced non-small cell lung cancer with epidermal growth factor
receptor mutations: Results of the West Japan thoracic oncology
group trial (WJTOG0403). Br J Cancer. 98:907–914. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mitsudomi T and Yatabe Y: Mutations of the
epidermal growth factor receptor gene and related genes as
determinants of epidermal growth factor receptor tyrosine kinase
inhibitors sensitivity in lung cancer. Cancer Sci. 98:1817–1824.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lee DH, Han JY, Yu SY, Kim HY, Nam BH,
Hong EK, Kim HT and Lee JS: The role of gefitinib treatment for
Korean never-smokers with advanced or metastatic adenocarcinoma of
the lung: A prospective study. J Thorac Oncol. 1:965–971. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Marchetti A, Martella C, Felicioni L,
Barassi F, Salvatore S, Chella A, Camplese PP, Iarussi T, Mucilli
F, Mezzetti A, et al: EGFR mutations in non-small-cell lung cancer:
Analysis of a large series of cases and development of a rapid and
sensitive method for diagnostic screening with potential
implications on pharmacologic treatment. J Clin Oncol. 23:857–865.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bos JL: Ras oncogenes in human cancer: A
review. Cancer Res. 49:4682–4689. 1989.PubMed/NCBI
|
|
10
|
Rodenhuis S, van de Wetering ML, Mooi WJ,
Evers SG, van Zandwijk N and Bos JL: Mutational activation of the
K-ras oncogene. A possible pathogenetic factor in adenocarcinoma of
the lung. N Engl J Med. 317:929–935. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhao XD, Deng HB, Lu CL, Bao YX, Lu X and
Deng LL: Association of EGFR and KRAS mutations with expression of
p-AKT, DR5 and DcR1 in non-small cell lung cancer. Neoplasma.
64:182–191. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Campos-Parra AD, Zuloaga C, Manriquez ME,
Avilés A, Borbolla-Escoboza J, Cardona A, Meneses A and Arrieta O:
KRAS mutation as the biomarker of response to chemotherapy and
EGFR-TKIs in patients with advanced non-small cell lung cancer:
Clues for its potential use in second-line therapy decision making.
Am J Clin Oncol. 38:33–40. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Johnson ML, Sima CS, Chaft J, Paik PK, Pao
W, Kris MG, Ladanyi M and Riely GJ: Association of KRAS and EGFR
mutations with survival in patients with advanced lung
adenocarcinomas. Cancer. 119:356–362. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Soda M, Choi YL, Enomoto M, Takada S,
Yamashita Y, Ishikawa S, Fujiwara S, Watanabe H, Kurashina K,
Hatanaka H, et al: Identification of the transforming EML4-ALK
fusion gene in non-small-cell lung cancer. Nature. 448:561–566.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hong M, Kim RN, Song JY, Choi SJ, Oh E,
Lira ME, Mao M, Takeuchi K, Han J, Kim J and Choi YL: HIP1-ALK, a
novel fusion protein identified in lung adenocarcinoma. J Thorac
Oncol. 9:419–422. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Hallberg B and Palmer RH: Mechanistic
insight into ALK receptor tyrosine kinase in human cancer biology.
Nat Rev Cancer. 13:685–700. 2013. View
Article : Google Scholar : PubMed/NCBI
|
|
17
|
Togashi Y, Soda M, Sakata S, Sugawara E,
Hatano S, Asaka R, Nakajima T, Mano H and Takeuchi K: KLC1-ALK: A
novel fusion in lung cancer identified using a formalin-fixed
paraffin-embedded tissue only. PLoS One. 7:e313232012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zheng D, Wang R, Zhang Y, Pan Y, Cheng X,
Cheng C, Zheng S, Li H, Gong R, Li Y, et al: Prevalence and
clinicopathological characteristics of ALK fusion subtypes in lung
adenocarcinomas from Chinese populations. J Cancer Res Clin Oncol.
142:833–843. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Barlesi F, Mazieres J, Merlio JP,
Debieuvre D, Mosser J, Lena H, Ouafik L, Besse B, Rouquette I,
Westeel V, et al: Routine molecular profiling of patients with
advanced non-small-cell lung cancer: Results of a 1-year nationwide
programme of the French cooperative thoracic intergroup (IFCT).
Lancet. 387:1415–1426. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Vidal J, Clave S, de Muga S, González I,
Pijuan L, Gimeno J, Remón J, Reguart N, Viñolas N, Gironés R, et
al: Assessment of ALK status by FISH on 1000 Spanish non-small cell
lung cancer patients. J Thorac Oncol. 9:1816–1820. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kim TJ, Park CK, Yeo CD, Park K, Rhee CK,
Kim J, Kim SJ, Lee SH, Lee KY and Yoon HK: Simultaneous diagnostic
platform of genotyping EGFR, KRAS, and ALK in 510 Korean patients
with non-small-cell lung cancer highlights significantly higher ALK
rearrangement rate in advanced stage. J Surg Oncol. 110:245–251.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ali G, Proietti A, Pelliccioni S, Niccoli
C, Lupi C, Sensi E, Giannini R, Borrelli N, Menghi M, Chella A, et
al: ALK rearrangement in a large series of consecutive non-small
cell lung cancers: Comparison between a new immunohistochemical
approach and fluorescence in situ hybridization for the screening
of patients eligible for crizotinib treatment. Arch Pathol Lab Med.
138:1449–1458. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zhang X, Zhang S, Yang X, Yang J, Zhou Q,
Yin L, An S, Lin J, Chen S, Xie Z, et al: Fusion of EML4 and ALK is
associated with development of lung adenocarcinomas lacking EGFR
and KRAS mutations and is correlated with ALK expression. Mol
Cancer. 9:1882010. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Xu CW, Cai XY, Shao Y, Li Y, Shi MW, Zhang
LY, Wang L, Zhang YP, Wang LP and Tian YW: A case of lung
adenocarcinoma with a concurrent EGFR mutation and ALK
rearrangement: A case report and literature review. Mol Med Rep.
12:4370–4375. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wong DW, Leung EL, So KK, Tam IY, Sihoe
AD, Cheng LC, Ho KK, Au JS, Chung LP, Pik Wong M, et al: The
EML4-ALK fusion gene is involved in various histologic types of
lung cancers from nonsmokers with wild-type EGFR and KRAS. Cancer.
115:1723–1733. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kim HJ, Choi EY, Jin HJ and Shin KC:
Relationship between EGFR mutations and clinicopathological
features of lung adenocarcinomas diagnosed via small biopsies.
Anticancer Res. 34:3189–3195. 2014.PubMed/NCBI
|
|
27
|
Lim JU, Yeo CD, Rhee CK, Kim YH, Park CK,
Kim JS, Kim JW, Lee SH, Kim SJ, Yoon HK, et al: Chronic obstructive
pulmonary disease-related non-small-cell lung cancer exhibits a low
prevalence of EGFR and ALK Driver Mutations. PLoS One.
10:e01423062015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Bae NC, Chae MH, Lee MH, Kim KM, Lee EB,
Kim CH, Park TI, Han SB, Jheon S, Jung TH and Park JY: EGFR, ERBB2,
and KRAS mutations in Korean non-small cell lung cancer patients.
Cancer Genet Cytogenet. 173:107–113. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Lee T, Lee B, Choi YL, Han J, Ahn MJ and
Um SW: Non-small cell lung cancer with concomitant EGFR, KRAS, and
ALK mutation: Clinicopathologic features of 12 cases. J Pathol
Transl Med. 50:197–203. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Ha SY, Choi SJ, Cho JH, Choi HJ, Lee J,
Jung K, Irwin D, Liu X, Lira ME, Mao M, et al: Lung cancer in
never-smoker Asian females is driven by oncogenic mutations, most
often involving EGFR. Oncotarget. 6:5465–5474. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lee B, Lee T, Lee SH, Choi YL and Han J:
Clinicopathologic characteristics of EGFR, KRAS, and ALK
alterations in 6,595 lung cancers. Oncotarget. 7:23874–23884.
2016.PubMed/NCBI
|
|
32
|
Thunnissen E, Bubendorf L, Dietel M,
Elmberger G, Kerr K, Lopez-Rios F, Moch H, Olszewski W, Pauwels P,
Penault-Llorca F and Rossi G: EML4-ALK testing in non-small cell
carcinomas of the lung: A review with recommendations. Virchows
Arch. 461:245–257. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Yatabe Y: ALK FISH and IHC: You cannot
have one without the other. J Thorac Oncol. 10:548–550. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Savic S, Diebold J, Zimmermann AK, Jochum
W, Baschiera B, Grieshaber S, Tornillo L, Bisig B, Kerr K and
Bubendorf L: Screening for ALK in non-small cell lung carcinomas:
5A4 and D5F3 antibodies perform equally well, but combined use with
FISH is recommended. Lung Cancer. 89:104–109. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Cabillic F, Gros A, Dugay F, Begueret H,
Mesturoux L, Chiforeanu DC, Dufrenot L, Jauffret V, Dachary D,
Corre R, et al: Parallel FISH and immunohistochemical studies of
ALK status in 3244 non-small-cell lung cancers reveal major
discordances. J Thorac Oncol. 9:295–306. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
van der Wekken AJ, Pelgrim R, 't Hart N,
Werner N, Mastik MF, Hendriks L, van der Heijden EHFM,
Looijen-Salamon M, de Langen AJ, Staal-van den Brekel J, et al:
Dichotomous ALK-IHC is a better predictor for ALK inhibition
outcome than traditional ALK-FISH in advanced non-small cell lung
cancer. Clin Cancer Res. 23:4251–4258. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Lindeman NI, Cagle PT, Aisner DL, Arcila
ME, Beasley MB, Bernicker EH, Colasacco C, Dacic S, Hirsch FR, Kerr
K, et al: Updated molecular testing guideline for the selection of
lung cancer patients for treatment with targeted tyrosine kinase
inhibitors: Guideline from the college of American pathologists,
the international association for the study of lung cancer, and the
association for molecular pathology. J Mol Diagn. 20:129–159. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Jennings LJ, Arcila ME, Corless C,
Kamel-Reid S, Lubin IM, Pfeifer J, Temple-Smolkin RL, Voelkerding
KV and Nikiforova MN: Guidelines for validation of next-generation
sequencing-based oncology panels: A joint consensus recommendation
of the association for molecular pathology and college of American
pathologists. J Mol Diagn. 19:341–365. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
von Ahlfen S, Missel A, Bendrat K and
Schlumpberger M: Determinants of RNA quality from FFPE samples.
PLoS One. 2:e12612007. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Glenn TC: Field guide to next-generation
DNA sequencers. Mol Ecol Resour. 11:759–769. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Camidge R, Kim HR, Ahn M, Yang JC, Han J,
Lee J, Hochmair M, Li JY, Chang G, Lee K, et al: PL02.03 brigatinib
vs crizotinib in patients with ALK inhibitor-naive advanced ALK+
NSCLC: First report of a phase 3 trial (ALTA-1L). J Thorac Oncol.
13:S184–S185. 2018. View Article : Google Scholar
|
|
42
|
Camidge DR, Kim HR, Ahn MJ, Yang JC, Han
JY, Lee JS, Hochmair MJ, Li JY, Chang GC, Lee KH, et al: Brigatinib
versus Crizotinib in ALK-positive non-small-cell lung cancer. N
Engl J Med. 379:2027–2039. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Yang P, Kulig K, Boland JM,
Erickson-Johnson MR, Oliveira AM, Wampfler J, Jatoi A, Deschamps C,
Marks R, Fortner C, et al: Worse disease-free survival in
never-smokers with ALK+ lung adenocarcinoma. J Thorac Oncol.
7:90–97. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Wu SG, Kuo YW, Chang YL, Shih JY, Chen YH,
Tsai MF, Yu CJ, Yang CH and Yang PC: EML4-ALK translocation
predicts better outcome in lung adenocarcinoma patients with
wild-type EGFR. J Thorac Oncol. 7:98–104. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Schilsky JB, Ni A, Ahn L, Datta S, Travis
WD, Kris MG, Chaft JE, Rekhtman N and Hellmann MD: Prognostic
impact of TTF-1 expression in patients with stage IV lung
adenocarcinomas. Lung Cancer. 108:205–211. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Won JK, Keam B, Koh J, Cho HJ, Jeon YK,
Kim TM, Lee SH, Lee DS, Kim DW and Chung DH: Concomitant ALK
translocation and EGFR mutation in lung cancer: A comparison of
direct sequencing and sensitive assays and the impact on
responsiveness to tyrosine kinase inhibitor. Ann Oncol. 26:348–354.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Gatalica Z, Xiu J, Swensen J and Vranic S:
Molecular characterization of cancers with NTRK gene fusions. Mod
Pathol. 32:147–153. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Ardini E, Bosotti R, Borgia AL, De Ponti
C, Somaschini A, Cammarota R, Amboldi N, Raddrizzani L, Milani A,
Magnaghi P, et al: The TPM3-NTRK1 rearrangement is a recurring
event in colorectal carcinoma and is associated with tumor
sensitivity to TRKA kinase inhibition. Mol Oncol. 8:1495–1507.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Vaishnavi A, Capelletti M, Le AT, Kako S,
Butaney M, Ercan D, Mahale S, Davies KD, Aisner DL, Pilling AB, et
al: Oncogenic and drug-sensitive NTRK1 rearrangements in lung
cancer. Nat Med. 19:1469–1472. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Drilon A, Laetsch TW, Kummar S, DuBois SG,
Lassen UN, Demetri GD, Nathenson M, Doebele RC, Farago AF, Pappo
AS, et al: Efficacy of larotrectinib in TRK fusion-positive cancers
in adults and children. N Engl J Med. 378:731–739. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Chen Y and Chi P: Basket trial of TRK
inhibitors demonstrates efficacy in TRK fusion-positive cancers. J
Hematol Oncol. 11:782018. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Rolfo C and Raez L: New targets bring hope
in squamous cell lung cancer: Neurotrophic tyrosine kinase gene
fusions. Lab Invest. 97:1268–1270. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Amatu A, Sartore-Bianchi A and Siena S:
NTRK gene fusions as novel targets of cancer therapy across
multiple tumour types. ESMO Open. 1:e0000232016. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Farago AF, Le LP, Zheng Z, Muzikansky A,
Drilon A, Patel M, Bauer TM, Liu SV, Ou SH, Jackman D, et al:
Durable clinical response to entrectinib in NTRK1-rearranged
non-small cell lung cancer. J Thorac Oncol. 10:1670–1674. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Liu Z, Wu L, Cao J, Yang Z, Zhou C, Cao L,
Wu H, Shen H, Jin M, Zhang Y, et al: Clinical characterization of
ERBB2 exon 20 insertions and heterogeneity of outcomes responding
to afatinib in Chinese lung cancer patients. Onco Targets Ther.
11:7323–7331. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Pillai RN, Behera M, Berry LD, Rossi MR,
Kris MG, Johnson BE, Bunn PA, Ramalingam SS and Khuri FR: HER2
mutations in lung adenocarcinomas: A report from the lung cancer
mutation consortium. Cancer. 123:4099–4105. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Sonobe M, Manabe T, Wada H and Tanaka F:
Lung adenocarcinoma harboring mutations in the ERBB2 kinase domain.
J Mol Diagn. 8:351–356. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Spector NL and Blackwell KL: Understanding
the mechanisms behind trastuzumab therapy for human epidermal
growth factor receptor 2-positive breast cancer. J Clin Oncol.
27:5838–5847. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Lee JW, Soung YH, Kim SY, Nam SW, Park WS,
Wang YP, Jo KH, Moon SW, Song SY, Lee JY, et al: ERBB2 kinase
domain mutation in the lung squamous cell carcinoma. Cancer Lett.
237:89–94. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Stephens P, Hunter C, Bignell G, Edkins S,
Davies H, Teague J, Stevens C, O'Meara S, Smith R, Parker A, et al:
Lung cancer: Intragenic ERBB2 kinase mutations in tumours. Nature.
431:525–526. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Liu S, Li S, Hai J, Wang X, Chen T, Quinn
MM, Gao P, Zhang Y, Ji H, Cross DAE and Wong KK: Targeting HER2
aberrations in non-small cell lung cancer with osimertinib. Clin
Cancer Res. 24:2594–2604. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
de Langen AJ, Jebbink M, Hashemi SMS,
Kuiper JL, de Bruin-Visser J, Monkhorst K, Thunnissen E and Smit
EF: Trastuzumab and paclitaxel in patients with EGFR mutated NSCLC
that express HER2 after progression on EGFR TKI treatment. Br J
Cancer. 119:558–564. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Mazieres J, Barlesi F, Filleron T, Besse
B, Monnet I, Beau-Faller M, Peters S, Dansin E, Früh M, Pless M, et
al: Lung cancer patients with HER2 mutations treated with
chemotherapy and HER2-targeted drugs: Results from the European
EUHER2 cohort. Ann Oncol. 27:281–286. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
von Laffert M, Stenzinger A, Hummel M,
Weichert W, Lenze D, Warth A, Penzel R, Herbst H, Kellner U,
Jurmeister P, et al: ALK-FISH borderline cases in non-small cell
lung cancer: Implications for diagnostics and clinical decision
making. Lung Cancer. 90:465–471. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Ilie MI, Bence C, Hofman V, Long-Mira E,
Butori C, Bouhlel L, Lalvée S, Mouroux J, Poudenx M, Otto J, et al:
Discrepancies between FISH and immunohistochemistry for assessment
of the ALK status are associated with ALK ‘borderline’-positive
rearrangements or a high copy number: A potential major issue for
anti-ALK therapeutic strategies. Ann Oncol. 26:238–244. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Heyer EE, Deveson IW, Wooi D, Selinger CI,
Lyons RJ, Hayes VM, O'Toole SA, Ballinger ML, Gill D, Thomas DM, et
al: Diagnosis of fusion genes using targeted RNA sequencing. Nat
Commun. 10:13882019. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Ibrahim M, Parry S, Wilkinson D, Bilbe N,
Allen D, Forrest S, Maxwell P, O'Grady A, Starczynski J, Tanier P,
et al: ALK immunohistochemistry in NSCLC: Discordant staining can
impact patient treatment regimen. J Thorac Oncol. 11:2241–2247.
2016. View Article : Google Scholar : PubMed/NCBI
|