Introduction
Cancer is the primary cause of death in the world,
and the main cause of cancer-associated death is cancer metastasis,
which arises following dissemination of cancer cells from the
primary tumor (1). The disseminated
cancer cells in blood circulation are defined as circulating tumor
cells (CTCs) that are carried around the human body by the
bloodstream and colonize at secondary sites forming metastatic
tumors (2). It is difficult to
isolate CTCs due to their rarity in the peripheral blood of
patients with cancer, and only 1–100 CTCs can be detected from
1×109 hematological cells in 1 ml human whole blood
(3,4). The majority of single CTCs are
apoptotic owing to their loss of cell adherence and the shear
forces in the bloodstream. Only a rare subset of aggregated CTC
clusters (2–50 CTCs) are capable of surviving in the bloodstream
(5). Compared to a single CTC, CTC
clusters have enhanced metastatic potential, and the presence of
CTC clusters is closely associated with shorter progression-free
survival and overall survival in various types of metastatic cancer
(6,7). The isolated CTCs or CTC clusters from
the liquid biopsy samples are considered to represent the molecular
characteristics of the primary tumor, and culturing of CTC-derived
tumors may provide valuable information on drug sensitivity and
immune epitope prediction. Growing evidence has also demonstrated
the clinical significance of isolated CTCs or CTC clusters in
cancer prognosis, treatment response and recurrence (8–11).
Strategies for isolation and enhancement of CTCs can
be classified into two major categories: Antibody-antigen
affinity-based methods and isolation devices based on the physical
characteristics of cancer cells (12). The only system approved by the US
Food and Drug Administration (FDA) for detecting CTCs is the
CellSearch® system which relies on targeting the
epithelial cell adhesion molecule (EpCAM) epitope to isolate CTCs
(13). The primary limitation of
antibody-antigen affinity-based methods is the low detection rates,
as both the expression levels and types of cancer cell biomarkers
are highly dynamic and heterogeneous during cancer progression.
Sample preparation of existing CTC isolation methods may also
severely damage CTC clusters and fail to preserve their integrity
(14). Another strategy for
isolation of CTCs is based on the physical characteristics of
cancer cells, such as size, density and dielectric properties
(15–17). Among these methods, conventional
size-based filtration has been frequently used for CTC isolation
(18). The majority of CTCs are
significantly larger than blood cells and thus can be isolated
using a polycarbonate membrane with a pore size of 8 µm (19). Conventional size-based filtration
methods are more widely used in practice due to the ease of
operation and low cost, and previous reports have indicated that
the size-based filtration may be a more accurate method for
predicting patient prognosis in certain types of cancer (20,21).
However, filter clogging, and a high degree of damage are the
limitations of conventional filtration methods, which limit more
widespread clinical use.
To overcome filter clogging and enhance the
filtering efficiency, in the present study, an electromagnetic
vibration-based filtration (eVBF) device was developed that could
isolate rare CTCs and CTC clusters from clinical blood samples of
patients with cancer. The eVBF device utilized an electromagnetic
force to generate a periodic vibration that prevented filter
clogging and enhanced the filtering efficiency. Based on the
optimized parameters of the eVBF device, CTCs were successfully
isolated from spiked human whole blood samples. The efficiency of
CTC recovery with this device was >80%. The eVBF device was also
used to isolate CTCs or CTC clusters in clinical blood samples of
patients with gastric cancer, and the sensitivity of detection of
CTCs using this method was 100%. Finally, the eVBF device was also
deemed suitable for continuous flow isolation of CTCs from
large-volume blood samples, suggesting that it may be potentially
suitable for detecting or capturing CTCs in the human body. Thus,
the eVBF device represents a novel and robust technique that can
efficiently isolate CTCs or CTC clusters for downstream
analysis.
Materials and methods
Materials and reagents
Filters were purchased from Whatman (GE Healthcare).
The polycarbonate membrane (8 µm) was purchased from EMD
Millipore. CK8 FITC-conjugated antibodies (cat. no. 11-9938),
CK18/19 Alexa Fluor 488-conjugated antibodies (cat. nos. 53-9815
and 53-9898), EpCAM FITC-conjugated antibodies (cat. no. 11-5791)
and CD45 PE-conjugated antibodies (cat. no. 12-0459) were purchased
from Thermo Fisher Scientific, Inc. CellTracker Green CMFDA dye and
Hoechst dye were purchased from Thermo Fisher Scientific, Inc.
RPMI-1640 medium was purchased from Hyclone (GE Healthcare). FBS
was purchased from Shanghai ExCell Biology, Inc. All other reagents
were of analytical grade.
Design and fabrication of the eVBF
device
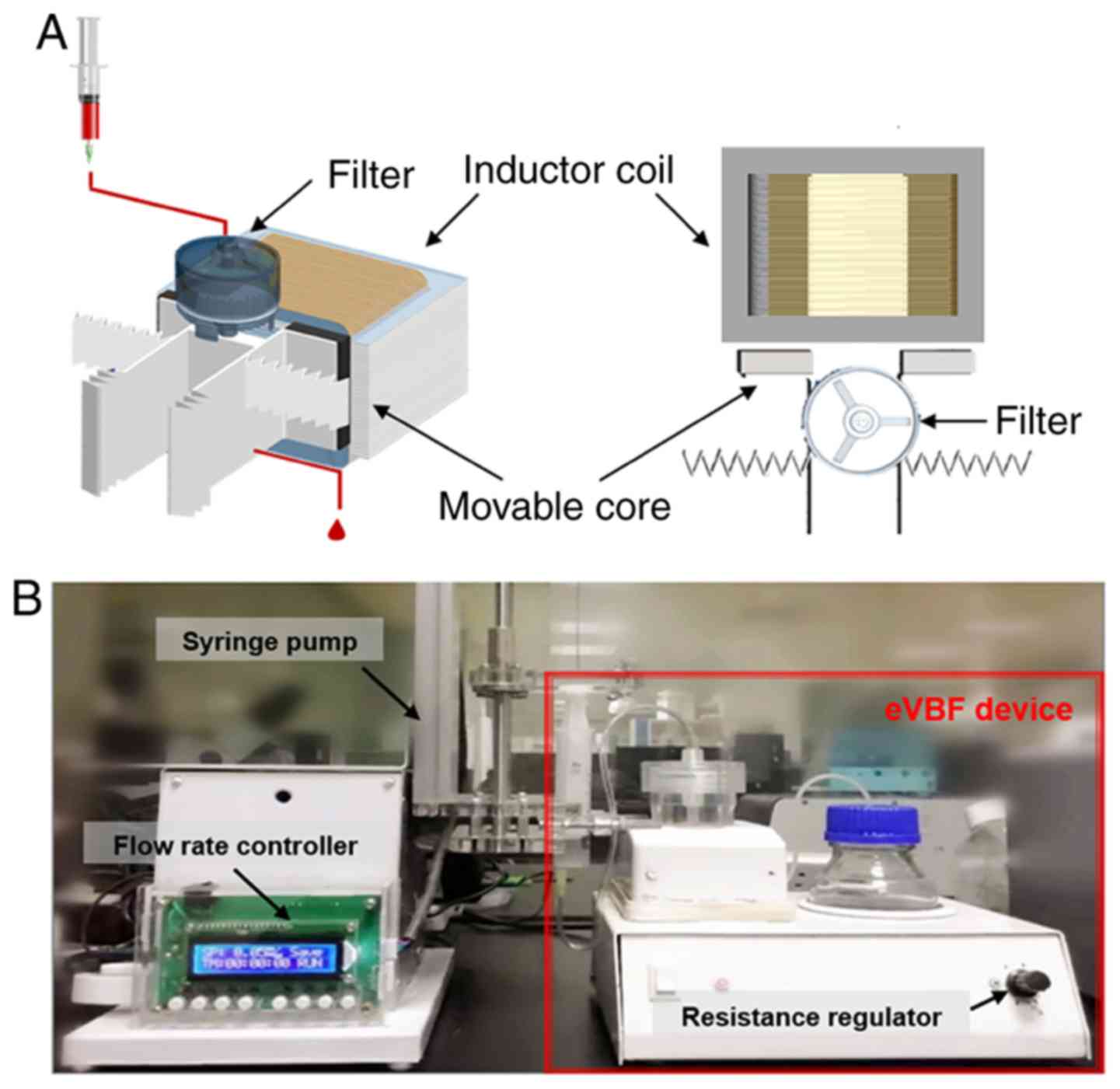
This device was composed of an electromagnetic
vibration system and a filtration system. The filtration system
included a vertical filter with two chambers: A sample loading
chamber with one inlet and a fluidic waste chamber with one outlet
at the bottom of the filter (Fig.
1). The vertical filter was fixed on the center of the two
movable cores of electromagnetic vibration. This electromagnetic
vibrator adopted a half-wave rectifier and a magnetic inductor coil
to produce the electromagnetic force that drove the vertical filter
to vibrate cyclically. The polycarbonate membrane (8 µm) was
placed in the membrane holder of the vertical filter (diameter 25
mm). The effluent blood cells from the fluidic waste chamber were
collected in a collecting bottle via a catheter.
Cell culture and blood
preparation
Human gastric cancer cells (AGS) were used to mimic
CTCs. AGS cells were cultured in RPMI-1640 media supplemented with
10% FBS, maintained at 37°C, in a humidified atmosphere with 5%
CO2 atmosphere. AGS cells were labeled with CellTracker
Green CMFDA dye. Whole blood samples, obtained from healthy
volunteers, were used as the spiked blood samples.
Evaluation of the eVBF device using
human cancer cells spiked into whole blood samples
To evaluate the isolation efficiency of the eVBF
device for CTCs, AGS cells pre-stained with CellTracker Green CMFDA
dye were spiked into whole blood samples obtained from healthy
individuals. Prepared blood samples were pumped into the loading
chamber via a syringe pump. Spiked blood samples were injected into
the upper chamber of the filter followed by filtration with a
controlled amplitude or flow rate. The effluent blood cells from
the fluidic waste chamber were collected in a collecting bottle.
After the filtering process was complete, the filter membrane was
disassembled from the vertical filter and washed with PBS.
Subsequently, the washing buffer containing the CTCs was collected
for further analysis.
Isolation of CTCs from clinical blood
samples of patients with cancer
To evaluate the clinical applicability of the eVBF
device, whole peripheral blood samples were obtained from 20
patients (11 male and 9 female patients; age range, 46–79 years)
with gastric cancer from January 2017 to December 2018. The present
study was approved by the Ethics Committee of Xijing Hospital of
Air Force Medical University (Xi'an, China). The cells which had
been isolated using the eVBF device were analyzed by
immunofluorescent staining. The collected cell fractions were fixed
with 4% paraformaldehyde, followed by permeabilization with 0.1%
Triton X-100, and blocked with 5% BSA. Subsequently, the cells were
incubated with CK8/18/19 antibodies, EpCAM antibodies, CD45
antibodies, and cellular nuclei were counterstained with Hoechst.
The imaging and counting of the isolated cells were performed using
a fluorescence microscope (Olympus Corp.; original magnification,
×200) and analyzed with Olympus cellSens software (version 1.6;
Olympus Corp.). CTCs were identified by observing the morphology of
cancer cells and the expression of biomarkers associated with
cancer cells. Cells which exhibited a rounded or elliptical
morphology with a large nucleolus ratio, positive expression of
CK8/18/19 or EpCAM (green), and negative expression of CD45 (red)
were considered CTCs.
Statistical analysis
Statistical analysis was performed using GraphPad
Prism version 7.0 (GraphPad Software, Inc.). Data are expressed as
the mean ± standard deviation. Differences between two
groups were analyzed using a Student's t-test. Comparisons of
multiple groups were analyzed using one-way analysis of variance
(ANOVA) test with post hoc Student-Newman-Keuls test. P<0.05 was
considered to indicate a statistically significant difference. All
model diagrams were generated using 3D Studio MAX 2016 (Autodesk,
Inc.).
Results
Working principle and characterization
of the eVBF device
The complete isolation system of the eVBF device is
shown in Fig. 1. The device
consists of a vertical filter with two chambers, and one
electromagnetic vibrator with two movable cores (Fig. 1A). The polycarbonate membrane with
an 8-µm pore size was placed in the membrane holder of the vertical
filter. It has been previously reported that a polycarbonate
membrane with an 8-µm pore size is optimal for isolation of CTCs
(19). In the present study, human
gastric cancer AGS cells were used as a model for CTC isolation.
AGS cells range in diameter from 9–20 µm which are larger than the
cell size of erythrocytes or the majority of white blood cells
(WBCs) as previously described (22,23).
During the filtering process, blood samples were filled in a
syringe pump and pumped through the eVBF device under different
flow rates. Furthermore, the electromagnetic vibrator of the eVBF
device could drive the filter to generate periodic vibration during
the filtering process, which promoted the CTCs on the membrane to
vibrate and re-disperse into the cell suspension. CTCs were caught
by the membrane whereas the blood cells such as erythrocytes and
WBCs passed through the membrane and were collected at the bottom
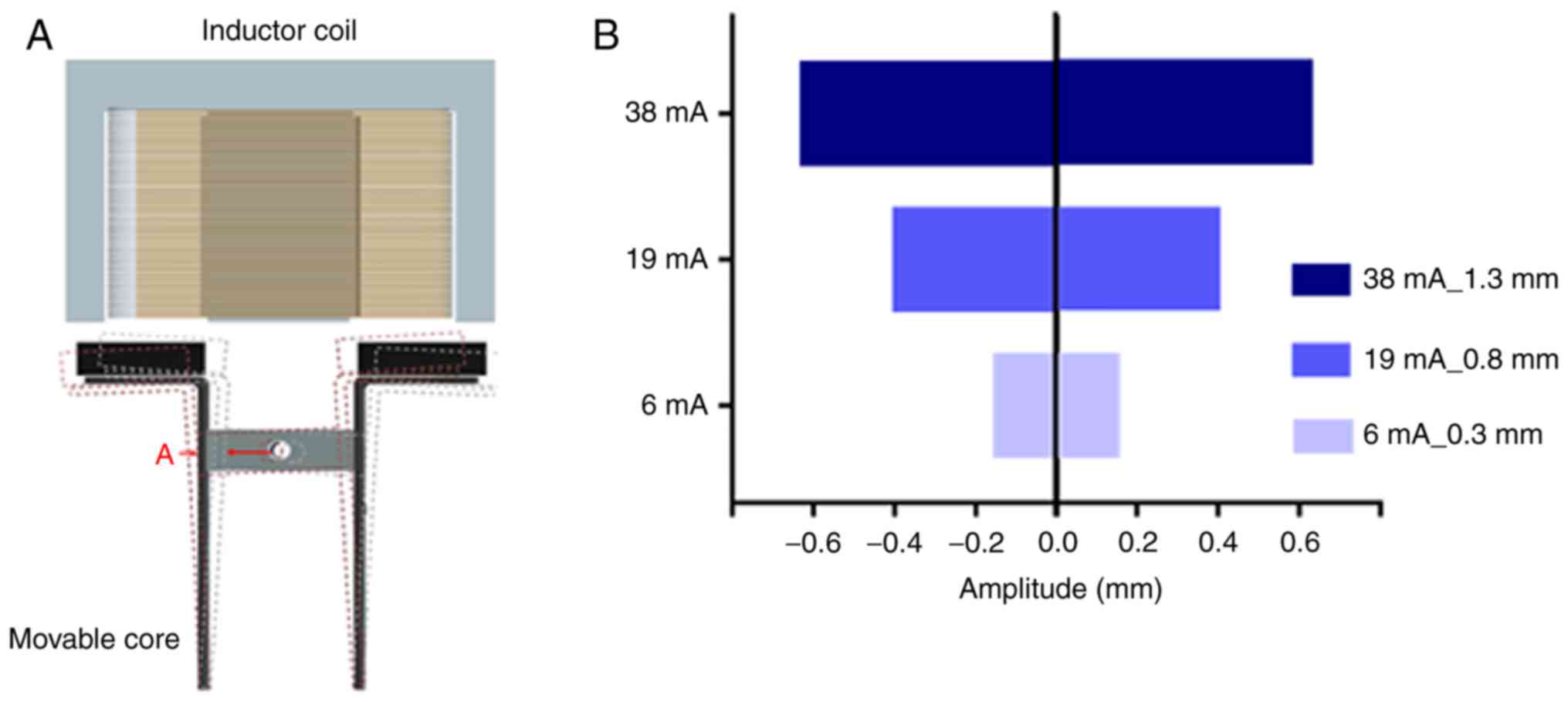
chamber. The vibration performance of the eVBF device was verified
and the vibrating amplitude of the movable core was assessed by
adjusting the resistance regulator (Fig. 1B and 2A). When the minimum current was 6 mA, the
amplitude was only 0.3 mm. When the current was 19 mA, the
amplitude of the movable core was 0.8 mm. When the current reached
38 mA, the amplitude reached 1.3 mm (Fig. 2B).
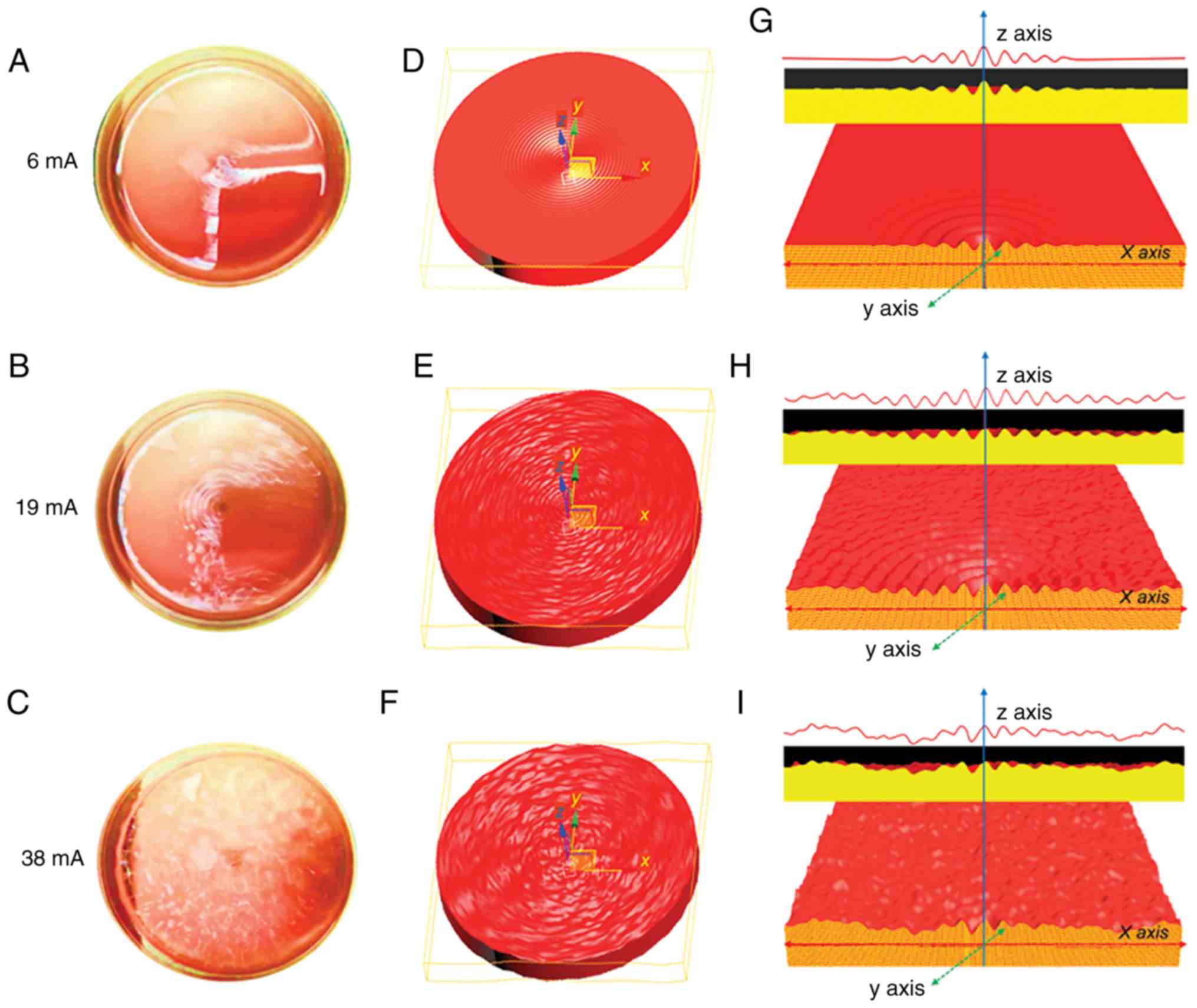
To examine the practical isolation parameters of the
eVBF device for CTC isolation, the effects of amplitude on the
vibration were determined. Cell culture dishes with blood samples
were used to substitute the vertical filter. It was shown that the
vibration of liquid appeared in the central part of the blood
suspension under low-amplitude conditions (6 mA) (Fig. 3A, D and G). As the amplitude was
enhanced (19 mA), the intensity of the vibration was further
strengthened. The range of vibration expanded from the center to
the edge, but the vibration intensity of the surrounding area was
lower than that of the central region (Fig. 3B, E and H). When the amplitude
intensity was increased to the maximum value of 38 mA, the
vibration of liquid also reached its maximum. Under these
conditions, a high-strength vibration formed over the entire blood
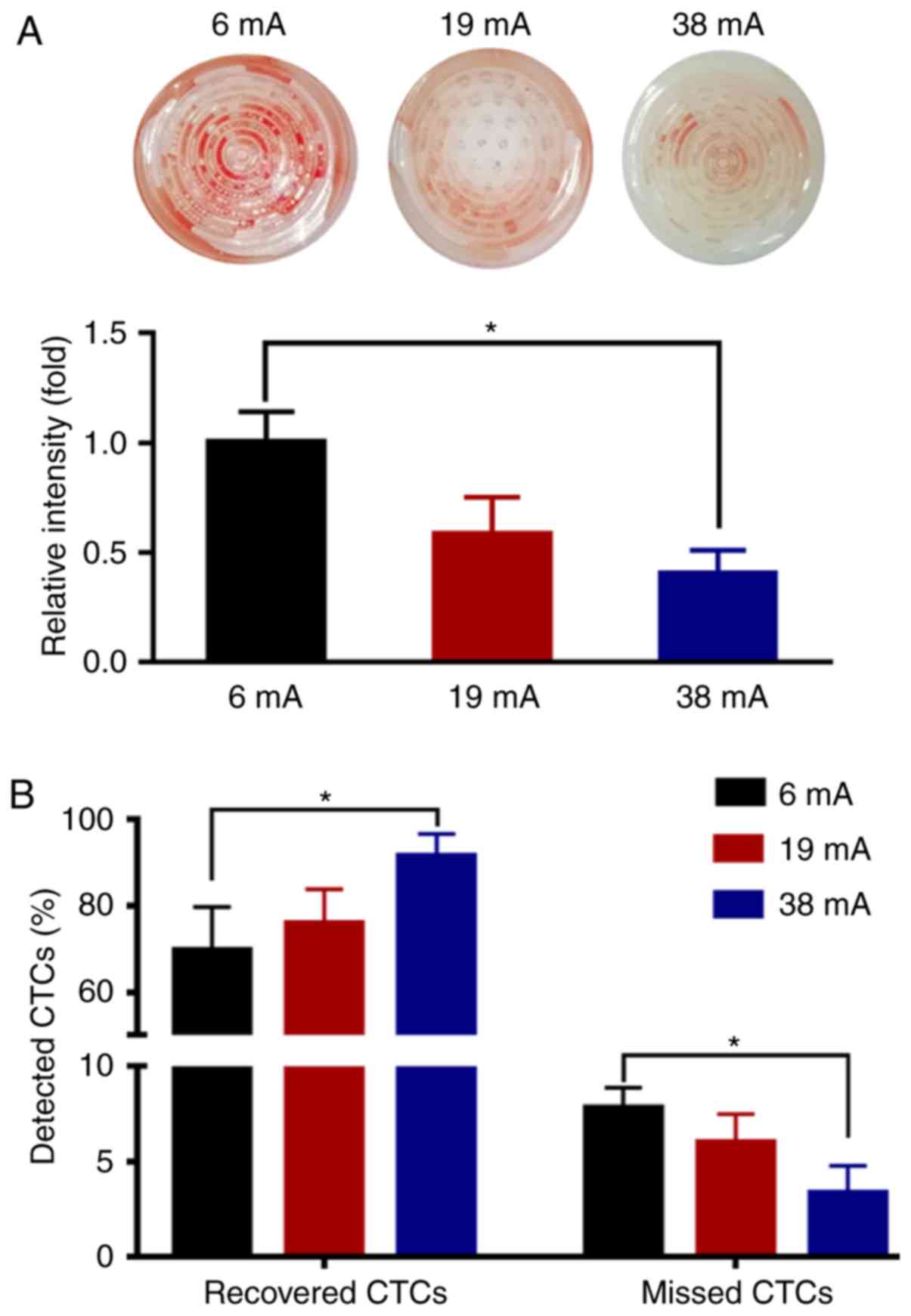
suspension from the center to the edge (Fig. 3C, F and I). To further investigate
the effects of vibration on the blood suspension, the blood samples
were filtered using the 8-µm filter membrane of the eVBF
device with different vibration amplitudes. After the filtering
process was finished, the intensity of the red color of the
residual blood cells on the membrane was assessed. As shown in
Fig. 4A, the intensity of the
residual blood cells on the membrane under low-amplitude (6 mA) was
60% higher compared with the high-amplitude (38 mA) filtration.
Taken together, these data suggest that vibration with a
high-amplitude (38 mA) can promote blood cell filtration and reduce
cell clogging.
Optimization of the eVBF device using
human cancer cells spiked into whole blood
To analyze the effects of vibration on the
selectivity of the filter membrane for cells, 1×105
fluorescently labeled AGS cells were spiked into 10 ml unlabeled
whole blood samples from healthy donors (1×104 cancer
cells/ml) and these samples were isolated using the eVBF device. As
shown in Fig. 4B, when applying a
low-amplitude vibration (6 mA), 69.67±10.02% of the cancer cells
were recovered by the membrane. As the clogging appeared and
progressed, 8.00±1.00% of the cancer cells became deformed and
finally passed through the membrane which resulted in missed
detection of CTCs. Under a medium amplitude or high-amplitude
conditions (19 or 38 mA, respectively), the recovered rate of
cancer cells isolated by the filter membrane was increased from
76.00±7.76 to 91.67±5.13%, respectively, and the missed rate of
cancer cells passing through the membrane was reduced from
6.00±1.50 to 3.67±1.15%, respectively (Fig. 4B). Together, these results indicate
that the device may improve the isolation efficiency of CTCs and
reduce the missed detection rate of CTCs.
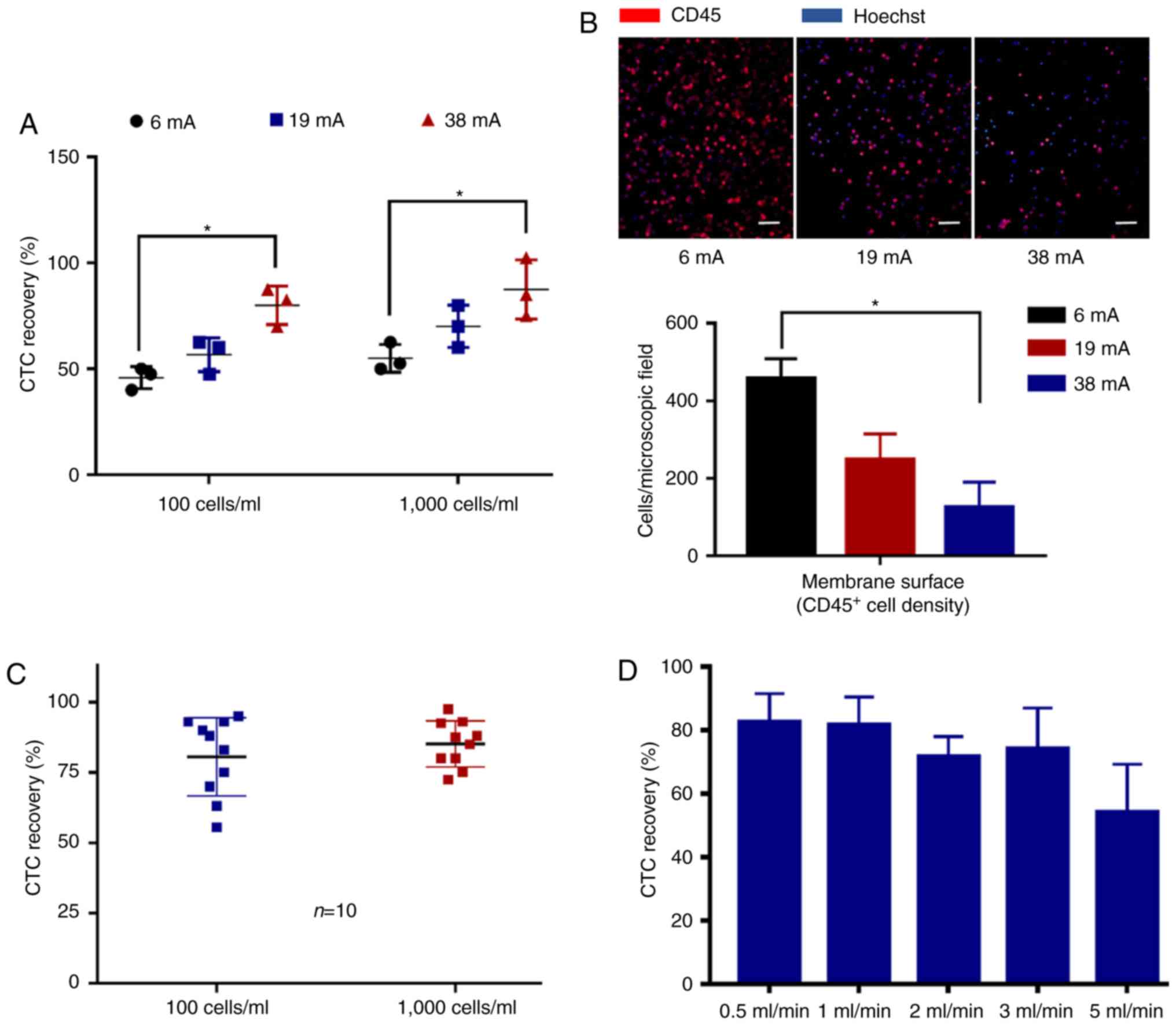
To determine the recovery rate of the eVBF device
for rare cancer cells, fluorescently labeled AGS cells were spiked
into undiluted whole blood samples from healthy donors, at either
~100 cancer cells/ml or ~1,000 cancer cells/ml. After the filtering
process was complete, the residual blood cells (such as WBCs) on
the filter membrane were washed and detected using
immunofluorescent staining with CD45 antibodies. As shown in
Fig. 5A and B, the high-amplitude
(38 mA) vibration of the eVBF device improved the recovery rate of
CTCs while reducing the background WBC count. Isolated experiments
under high-amplitude (38 mA) conditions were repeated 10 times. The
average recovered efficiency of the 100 and 1,000 AGS cells was
80.55±13.93 and 85.10±8.15%, respectively (Fig. 5C). The effects of flow rate
(throughput) for CTC isolation were further observed. The flow rate
of the eVBF device was set at 0.5, 1, 2, 3 and 5 ml/min. As shown
in Fig. 5D, the flow rate of the
eVBF device affected the recovery rate of CTCs. These results also
indicated that as the flow rate increased, the recovery rate of
CTCs decreased. Compared with a flow rate of 1 ml/min, the lower
flow rate of 0.5 ml/min had no significant effect on the recovery
rate of CTCs. Together, these results suggest that the optimal
conditions for use of the eVBF device for isolation of CTCs were a
high-amplitude vibration (38 mA) and a high throughput (1
ml/min).
Isolation of CTCs and CTC clusters
from blood samples of gastric cancer patients using the eVBF
device
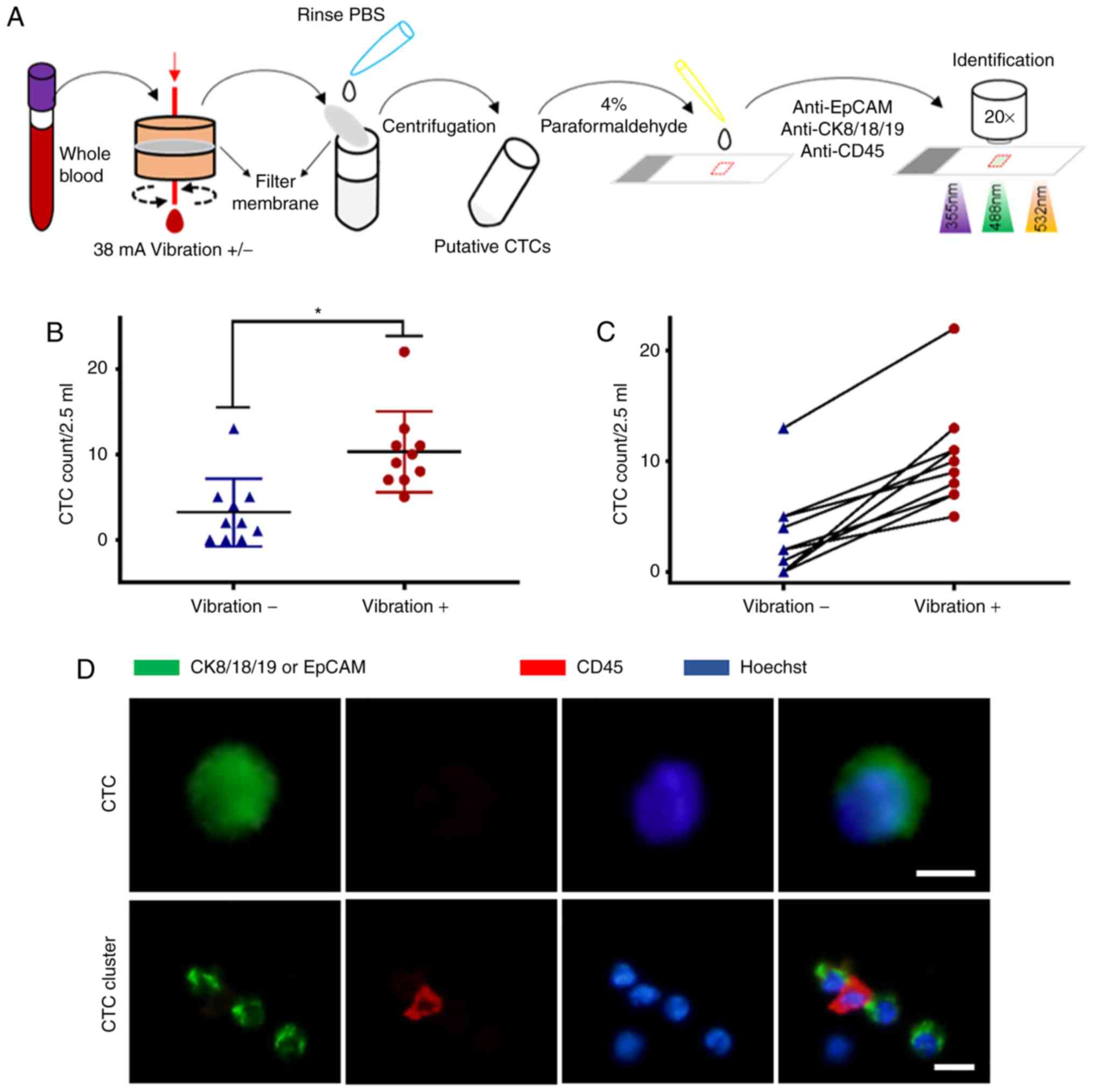
To evaluate the clinical applicability of the eVBF
device, 5-ml blood samples were collected from 10 patients with
gastric cancer. The collected blood samples were divided into two
equal parts: One tube for conventional filtration and the other
tube for filtration using the eVBF device (Fig. 6A). The isolated cells were
identified using immunofluorescent staining. Cells that showed a
round or elliptical morphology with a large nucleolus ratio,
positive expression of CK8/18/19 or EpCAM (green), and negative
expression of CD45 (red) were considered CTCs. The clinical
information and CTC count for each patient are presented in
Table I. CTCs were detected in 10
out of 10 (100%) patient blood samples using the eVBF device, and 7
out of 10 (70%) of the patient blood samples using a conventional
filtration method. (Fig. 6B and C).
The enumeration of isolated CTCs using the eVBF device ranged
between 5–22 tumor cells in 2.5 ml of blood, and the enumeration of
isolated CTCs using the conventional filtration method ranged
between 1–13 tumor cells in 2.5 ml of blood. Representative
immunofluorescent staining images of single CTCs are shown in
Fig. 6D. To evaluate the capability
of the eVBF device for isolation of CTC clusters, 5-ml blood
samples were collected from another 10 patients with gastric
cancer. CTC clusters were identified in 4 of 10 (40%) patients with
gastric cancer. As shown in Fig.
6D, the integrity of CTC clusters was preserved using this
device. Therefore, compared with conventional filtration methods,
the eVBF device more effectively isolated CTCs or CTC clusters from
whole blood samples of patients with gastric cancer compared with
conventional filtration methods.
 | Table I.Clinical information of the 10
patients with gastric cancer and the numbers of CTCs detected. |
Table I.
Clinical information of the 10
patients with gastric cancer and the numbers of CTCs detected.
|
|
|
|
|
| CTC count |
|---|
|
|
|
|
|
|
|
|---|
| Patient ID | Age (years) | Sex | Clinical
diagnosis | Clinical
treatment | Conventional
filtration | eVBF device |
|---|
| 1 | 67 | Male | Gastric cancer | After
operation | 4 | 10 |
| 2 | 60 | Female | Gastric cancer | Before
operation | 5 | 11 |
| 3 | 46 | Male | Gastric cancer | After
operation | 13 | 22 |
| 4 | 79 | Male | Gastric cancer | Before
operation | 5 | 9 |
| 5 | 79 | Male | Gastric cancer | After
operation | 1 | 8 |
| 6 | 65 | Female | Gastric cancer | After
operation | 0 | 13 |
| 7 | 51 | Male | Gastric cancer | After
operation | 0 | 11 |
| 8 | 52 | Male | Gastric cancer | Before
operation | 2 | 7 |
| 9 | 54 | Male | Gastric cancer | After
operation | 2 | 5 |
| 10 | 51 | Female | Gastric cancer | After
operation | 0 | 7 |
Continuous flow isolation of CTCs from
whole blood using the eVBF device
Owing to the extremely low concentration of CTCs in
the peripheral bloodstream, isolated CTCs within a limited volume
(5–10 ml) of blood samples may reduce the accuracy of detection
(24). Methods for continuous flow
isolation of CTCs in vivo have been demonstrated that may
overcome this limitation (25,26).
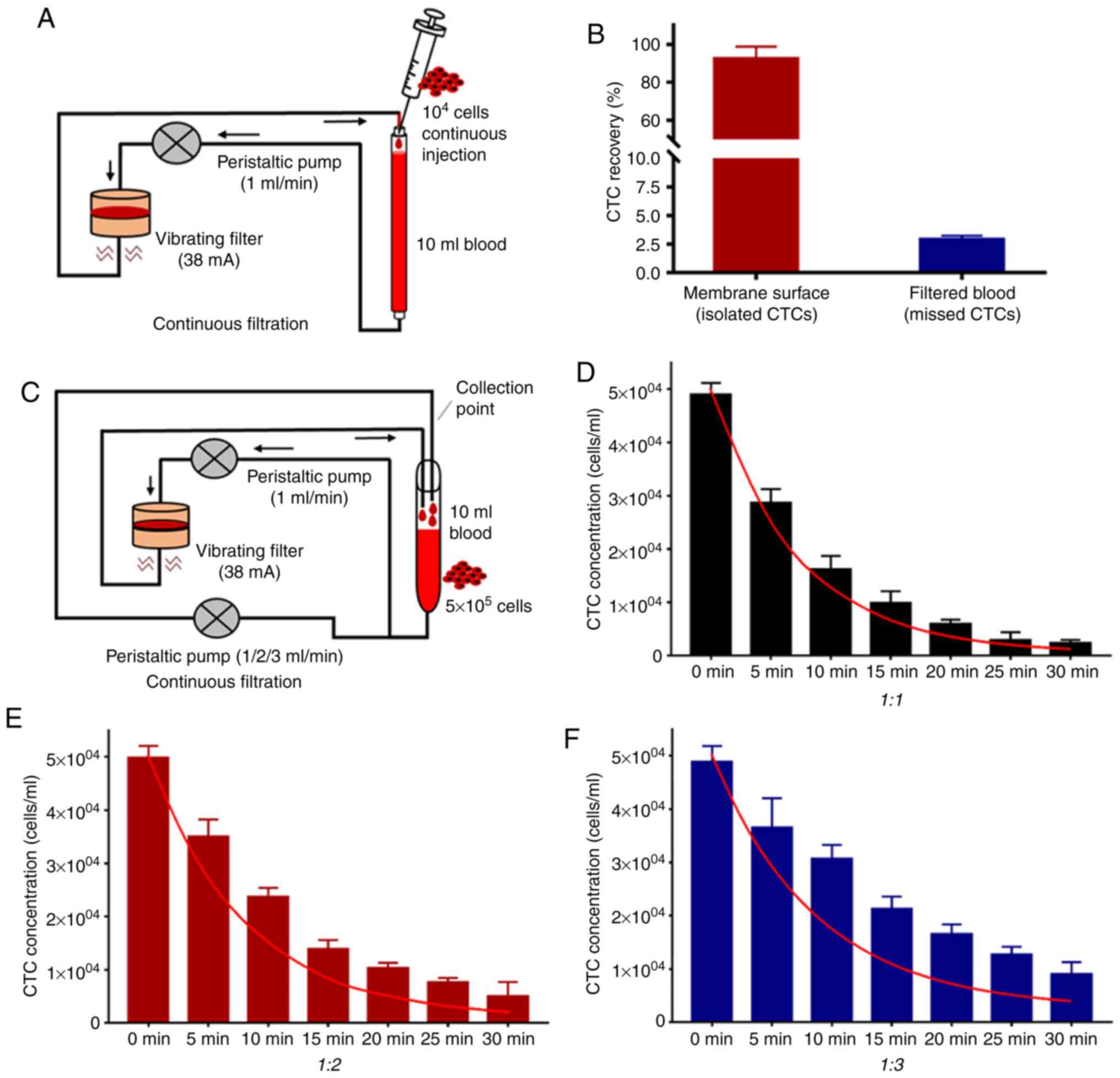
To explore the capability of the eVBF device to isolate CTCs from
large-volume blood samples (>100 ml), a peristaltic pump was
used to control the flow rate at 1 ml/min. This peristaltic pump
also pumped the blood flow through the eVBF device (Fig. 7A). Subsequently, a syringe pump was
used to continuously inject 1×104 fluorescently labeled
AGS cells into the blood flow (10 ml undiluted whole blood samples)
for 120 min (equal to total 120 ml blood samples and ~80 cancer
cells/ml) to simulate the CTCs in the bloodstream. As shown in
Fig. 7B, the average recovery rate
of CTCs was 92.50±6.32%. When the filtering process was completed,
the average residual rates of CTCs in the bloodstream was
2.93±0.30% (Fig. 7B). The other 5%
of CTCs may have remained in the pipeline or were lost during the
filtering process. Taken together, these results suggest that the
eVBF device is suitable for isolation of CTCs in large volumes of
blood samples due to effective reduction of cell clogging.
To simulate the complicated blood circuit of humans,
the blood flow system described above was expanded upon by adding
another peristaltic pump to simulate blood reflux. Subsequently,
5×105 fluorescently labeled AGS cells were injected into
10 ml of undiluted whole blood samples. One part of this mixture
was passed through the eVBF device at a flow rate of 1 ml/min,
whereas the other part of the blood flow was retransferred without
passing through the eVBF device at a flow rate of 1, 2 or 3 ml/min
(Fig. 7C). The concentrations of
residual CTCs in the blood flow system were measured at different
time points (every 5 min for a total of 30 min) to evaluate the
ability of the eVBF device to isolate CTCs. As the reflux rate
increased, the blood flow pumped into the eVBF device was reduced,
and more CTCs remained in the blood flow that was unfiltered by
eVBF device. As the filtering time increased, the residual number
of CTCs in the blood flow decreased gradually (Fig. 7D-F). Furthermore, the actual
reduction of CTCs in the blood flow was lower than the theoretical
value (red curve) at different filtering time points.
Under different filtering time points (t), the
calculation of the theoretical value of the residual concentration
of CTCs in the blood flow (Ct) is described by equation
1: Ct=C°[V/(1+V]N, where C0
represents the initial concentration of CTCs in the blood flow. The
flow rate of the blood loop through the eVBF device was 1 ml/min,
and the flow rate of the blood loop without the eVBF device was V
ml/min. The total velocity of blood circulation was (V+1) ml/min.
Theoretically, all CTCs passing through the eVBF device may be
intercepted by the filter membrane. When the filtering time is t
min, the actual filtration period (N) is described by equation 2:
N=t(V+1)/10. Thus, the theoretical value of the residual
concentration of CTCs in the blood flow (Ct) could be
represented as equation 1 and equation 2. When the flow rate of
blood reflux increased, the residual amount of CTCs in the blood
flow also increased (Fig. 7D-F).
Together, these results suggest that this device significantly
reduced the total content of CTCs in the bloodstream. However, to
achieve the desired isolated rate of CTCs, the filtering time, the
filter membrane area or the blood samples passed through the eVBF
device should be increased suitably.
Discussion
Conventional size-based filtration is a tumor
biomarker-independent method for isolation of CTCs, and the
advantages of this technique mainly include simple structure,
convenient operation and low cost (27). However, the primary challenge of
conventional filtration methods is cell clogging, which results in
a low enrichment efficiency of CTCs. Severe cell clogging can form
on the surface of the filter membrane when using conventional
filtration methods, which may cause cancer cells to become deformed
and pass through the membrane pores, resulting in a lowering of the
detection rate of CTCs. To eliminate cell deformation, and to
improve enrichment efficiency of CTCs, the conventional filtration
method usually requires formaldehyde to fix the blood samples, but
the fixation step can affect the downstream analyses of CTCs, such
as cellular and molecular assays (28). The majority of improved filtration
methods for CTC isolation are primarily modifications of
traditional filter membranes to overcome the problems of low
recovery and cell fixation (27–29).
However, these methods require microfabrication and special
materials, and the preparation processes of membranes are complex
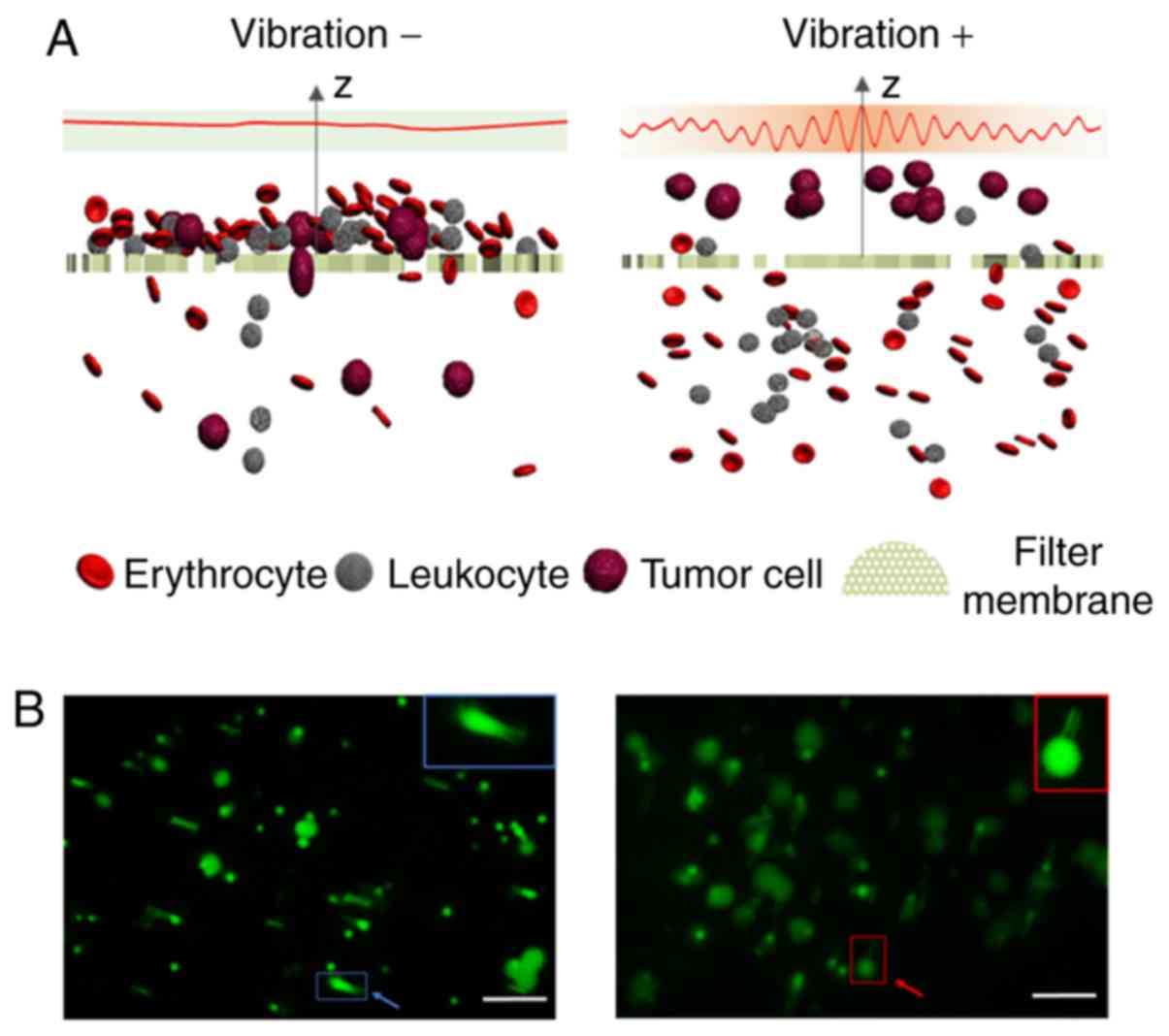
and expensive. In the present study, a simple and inexpensive eVBF
device was developed for isolation of CTCs with traditional
polycarbonate membranes without the use of any antibodies, chemical
regents or any pretreatment processes. Periodic vibration generated
by the eVBF device improved the enrichment efficiency of
conventional filtration methods by preventing cell clogging. Due to
the prevention of cell clogging, CTCs were not deformed and thus
captured by the membrane (Fig. 8).
The only FDA-approved technique for CTC isolation is the
CellSearch® system which relies on the detection of the
expression of the cell surface epithelial marker EpCAM to isolate
CTCs from whole blood. However, the expression of EpCAM is often
downregulated or absent in malignant epithelial CTCs undergoing
epithelial-to-mesenchymal transition or in malignancies of
non-epithelial origin (30).
Compared with the FDA-approved CellSearch® system, the
eVBF device is not dependent on the expression of cell surface
markers. Thus, the eVBF device is able to capture sub-populations
of CTCs with malignant potential that may be more suitable for
phenotype identification and downstream analysis.
In patients with gastric cancer, the eVBF device
exhibited 30% better clinical sensitivity compared with
conventional filtration methods. The enumeration of isolated CTCs
using the eVBF device (2–8.8 CTCs per ml) was significantly higher
compared with conventional filtration methods (0.4–5.2 CTCs per
ml). These results indicate that the conventional filtration method
leads to the loss of CTCs, and the eVBF device could reduce this
loss rate. The presence and high numbers of CTC clusters have been
demonstrated, and is associated with a poor prognosis in patients
with gastric cancer. CTC clusters are considered to possess a
higher metastatic potential compared with single CTCs (31). Therefore, CTC clusters may also
serve as biomarkers for indicating cancer prognosis and monitoring
cancer metastasis. CTC clusters were isolated and identified using
the eVBF device in 40% (4/10) of patients with gastric cancer. The
majority of existing technologies for isolation of CTCs are
designed to isolate single CTCs and the pretreatment procedures of
these methods may affect the integrity of CTC clusters (14). However, the eVBF device can isolate
CTC clusters from the whole blood of cancer patients and the intact
CTC clusters isolated by the eVBF device can be used for downstream
studies, such as molecular characterization and functional
analysis.
CTCs are extremely rare in the peripheral
bloodstream of humans. It is important to acquire the maximum
number of CTCs from a blood sample for an accurate representation
of the CTCs present (24). In in
vitro methods for detection of CTCs, the volume of blood
samples used for detection is limited to 5–10 ml, which may result
in sampling bias and reduce the accuracy of the detection methods.
To avoid sampling errors, CTCs should be isolated from considerably
larger volumes of blood samples (32,33).
In the present study, it was demonstrated that the eVBF device
could isolate CTCs from a large volume of blood sample
(high-throughput 1 ml/min, >100 ml blood sample), and the
recovery rate was maintained at ~90%. The currently available in
vivo enrichment strategies for CTC isolation have potential for
monitoring the dynamics of CTCs continuously and preventing cancer
metastasis in humans. However, the human blood circulatory system
is very complicated, such as the differences in blood flow between
the arteries and veins, the differences of blood flow in different
organs, and capillary barriers, which may affect the spatial and
temporal distributions of CTCs within the blood circulation of
humans (34). Therefore, in
vivo CTC isolation technologies are still experimental, and it
is difficult to translate these technologies from the laboratory to
clinical practice. These factors can also affect the clinical
application of the eVBF device for continuous flow isolation of
CTCs in vivo. Detailed animal studies or preclinical studies
on the eVBF device application in vivo are thus
required.
In summary, a simple, inexpensive and robust eVBF
device for isolation of rare CTCs and CTC clusters was developed.
Periodic vibration generated by the eVBF device improves
conventional filtration methods for CTC isolation by preventing
filter clogging. In addition, this device enables high-throughput
and continuous flow isolation of CTCs without the need for
antibodies, chemical regents or any pretreatment processes. Further
optimization and characterization of the eVBF device is required;
however, the device possesses clinical potential for real-time
monitoring of cancer, which may improve patient outcomes and assist
in improving our understanding of CTC biology.
Acknowledgements
Not applicable.
Funding
This research was funded by the National Key R&D
Program of China (no. 2017YFC1308600), the National Natural Science
Foundation of China (no. 81301513), the Natural Science Foundation
of Shaanxi Province of China (no. 2018JM7032) and the Key Projects
of State Key Laboratory of Cancer Biology (no. CBSKL2014Z06).
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
AX, MX, GJ and ZL designed this study. AX, MX, FR,
LW, ZY, DL and QJ performed the experiments and collected and
analyzed the data. AX, MX and ZL wrote and revised the manuscript.
All authors read and approved the final manuscript and agree to be
accountable for all aspects of the research in ensuring that the
accuracy or integrity of any part of the work are appropriately
investigated and resolved.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
Xijing Hospital of Air Force Medical University (Xi'an, China).
Patient consent for publication
Informed consent was obtained from each patient or
healthy volunteer before blood sample collection.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
ANOVA
|
analysis of variance
|
|
CK
|
cytokeratin
|
|
CMFDA
|
chloromethylfluorescein diacetate
|
|
CTC
|
circulating tumor cell
|
|
EpCAM
|
epithelial cell adhesion molecule
|
|
eVBF
|
electromagnetic vibration-based
filtration
|
|
FDA
|
US food and drug administration
|
|
FITC
|
fluorescein isothiocyanate
|
|
PBS
|
phosphate-buffered saline
|
|
PE
|
phycoerythrin
|
|
WBC
|
white blood cell
|
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2019. CA Cancer J Clin. 69:7–34. 2019. View Article : Google Scholar
|
|
2
|
Ortiz V and Yu M: Analyzing circulating
tumor cells one at a time. Trends Cell Biol. 28:764–775. 2018.
View Article : Google Scholar :
|
|
3
|
Wang S, Liu K, Liu J, Yu ZT, Xu X, Zhao L,
Lee T, Lee EK, Reiss J, Lee YK, et al: Highly efficient capture of
circulating tumor cells by using nanostructured silicon substrates
with integrated chaotic micromixers. Angew Chem Int Ed Engl.
50:3084–3088. 2011. View Article : Google Scholar :
|
|
4
|
Alix-Panabières C and Pantel K: Challenges
in circulating tumour cell research. Nat Rev Cancer. 14:623–631.
2014. View
Article : Google Scholar
|
|
5
|
Aceto N, Bardia A, Miyamoto DT, Donaldson
MC, Wittner BS, Spencer JA, Yu M, Pely A, Engstrom A, Zhu H, et al:
Circulating tumor cell clusters are oligoclonal precursors of
breast cancer metastasis. Cell. 158:1110–1122. 2014. View Article : Google Scholar :
|
|
6
|
Hou JM, Krebs MG, Lancashire L, Sloane R,
Backen A, Swain RK, Priest LJ, Greystoke A, Zhou C, Morris K, et
al: Clinical significance and molecular characteristics of
circulating tumor cells and circulating tumor microemboli in
patients with small-cell lung cancer. J Clin Oncol. 30:525–532.
2012. View Article : Google Scholar
|
|
7
|
Giuliano M, Shaikh A, Lo HC, Arpino G, De
Placido S, Zhang XH, Cristofanilli M, Schiff R and Trivedi MV:
Perspective on circulating tumor cell clusters: Why it takes a
village to metastasize. Cancer Res. 78:845–852. 2018. View Article : Google Scholar
|
|
8
|
Chikaishi Y, Yoneda K, Ohnaga T and Tanaka
F: EpCAM-independent capture of circulating tumor cells with a
‘universal CTC-chip’. Oncol Rep. 37:77–82. 2017. View Article : Google Scholar
|
|
9
|
Abdallah EA, Braun AC, Flores BCTCP, Senda
L, Urvanegia AC, Calsavara V, Fonseca de Jesus VH, Almeida MFA,
Begnami MD, Coimbra FJF, et al: The potential clinical implications
of circulating tumor cells and circulating tumor microemboli in
gastric cancer. Oncologist. 24:e854–e863. 2019. View Article : Google Scholar :
|
|
10
|
Chen JY, Tsai WS, Shao HJ, Wu JC, Lai JM,
Lu SH, Hung TF, Yang CT, Wu LC, Chen JS, et al: Sensitive and
specific biomimetic lipid coated microfluidics to isolate viable
circulating tumor cells and microemboli for cancer detection. PLoS
One. 11:e01496332016. View Article : Google Scholar :
|
|
11
|
Warkiani ME, Khoo BL, Wu L, Tay AK, Bhagat
AA, Han J and Lim CT: Ultra-fast, label-free isolation of
circulating tumor cells from blood using spiral microfluidics. Nat
Protoc. 11:134–148. 2016. View Article : Google Scholar
|
|
12
|
Kaiser J: Medicine. Cancer's circulation
problem. Science. 327:1072–1074. 2010. View Article : Google Scholar
|
|
13
|
Yu M, Bardia A, Wittner BS, Stott SL, Smas
ME, Ting DT, Isakoff SJ, Ciciliano JC, Wells MN, Shah AM, et al:
Circulating breast tumor cells exhibit dynamic changes in
epithelial and mesenchymal composition. Science. 339:580–584. 2013.
View Article : Google Scholar :
|
|
14
|
Sarioglu AF, Aceto N, Kojic N, Donaldson
MC, Zeinali M, Hamza B, Engstrom A, Zhu H, Sundaresan TK, Miyamoto
DT, et al: A microfluidic device for label-free, physical capture
of circulating tumor cell clusters. Nat Methods. 12:685–691. 2015.
View Article : Google Scholar :
|
|
15
|
Warkiani ME, Guan G, Luan KB, Lee WC,
Bhagat AA, Chaudhuri PK, Tan DS, Lim WT, Lee SC, Chen PC, et al:
Slanted spiral microfluidics for the ultra-fast, label-free
isolation of circulating tumor cells. Lab Chip. 14:128–137. 2014.
View Article : Google Scholar
|
|
16
|
Li M and Anand RK: High-throughput
selective capture of single circulating tumor cells by
dielectrophoresis at a wireless electrode array. J Am Chem Soc.
139:8950–8959. 2017. View Article : Google Scholar
|
|
17
|
Wang K, Zhou L, Zhao S, Cheng Z, Qiu S, Lu
Y, Wu Z, Abdel Wahab AHA, Mao H and Zhao J: A microfluidic platform
for high-purity separating circulating tumor cells at the
single-cell level. Talanta. 200:169–176. 2019. View Article : Google Scholar
|
|
18
|
Vona G, Sabile A, Louha M, Sitruk V,
Romana S, Schütze K, Capron F, Franco D, Pazzagli M, Vekemans M, et
al: Isolation by size of epithelial tumor cells: A new method for
the immunomorphological and molecular characterization of
circulatingtumor cells. Am J Pathol. 156:57–63. 2000. View Article : Google Scholar :
|
|
19
|
Hao SJ, Wan Y, Xia YQ, Zou X and Zheng SY:
Size-based separation methods of circulating tumor cells. Adv Drug
Deliv Rev. 125:3–20. 2018. View Article : Google Scholar
|
|
20
|
Farace F, Massard C, Vimond N, Drusch F,
Jacques N, Billiot F, Laplanche A, Chauchereau A, Lacroix L,
Planchard D, et al: A direct comparison of CellSearch and ISET for
circulating tumour-cell detection in patients with metastatic
carcinomas. Br J Cancer. 105:847–853. 2011. View Article : Google Scholar :
|
|
21
|
De Giorgi V, Pinzani P, Salvianti F,
Panelos J, Paglierani M, Janowska A, Grazzini M, Wechsler J,
Orlando C, Santucci M, et al: Application of a filtration- and
isolation-by-size technique for the detection of circulating tumor
cells in cutaneous melanoma. J Invest Dermatol. 130:2440–2447.
2010. View Article : Google Scholar
|
|
22
|
Coumans FA, van Dalum G, Beck M and
Terstappen LW: Filter characteristics influencing circulating tumor
cell enrichment from whole blood. PLoS One. 8:e617702013.
View Article : Google Scholar :
|
|
23
|
Shapiro HM, Schildkraut ER, Curbelo R,
Laird CW, Turner B and Hirschfeld T: Combined blood cell counting
and classification with fluorochrome stains and flow
instrumentation. J Histochem Cytochem. 24:396–401. 1976. View Article : Google Scholar
|
|
24
|
Li P, Mao Z, Peng Z, Zhou L, Chen Y, Huang
PH, Truica CI, Drabick JJ, El-Deiry WS, Dao M, et al: Acoustic
separation of circulating tumor cells. Proc Natl Acad Sci USA.
112:4970–4975. 2015. View Article : Google Scholar
|
|
25
|
Galanzha EI, Menyaev YA, Yadem AC,
Sarimollaoglu M, Juratli MA, Nedosekin DA, Foster SR,
Jamshidi-Parsian A, Siegel ER, Makhoul I, et al: In vivo liquid
biopsy using cytophone platform for photoacoustic detection of
circulating tumor cells in patients with melanoma. Sci Transl Med.
11(pii): eaat58572019. View Article : Google Scholar
|
|
26
|
Saucedo-Zeni N, Mewes S, Niestroj R,
Gasiorowski L, Murawa D, Nowaczyk P, Tomasi T, Weber E, Dworacki G,
Morgenthaler NG, et al: A novel method for the in vivo
isolation of circulating tumor cells from peripheral blood of
cancer patients using a functionalized and structured medical wire.
Int J Oncol. 41:1241–1250. 2012.
|
|
27
|
Zheng S, Lin H, Liu JQ, Balic M, Datar R,
Cote RJ and Tai YC: Membrane microfilter device for selective
capture, electrolysis and genomic analysis of human circulating
tumor cells. J Chromatogr A. 1162:154–161. 2007. View Article : Google Scholar
|
|
28
|
Zheng S, Lin HK, Lu B, Williams A, Datar
R, Cote RJ and Tai YC: 3D microfilter device for viable circulating
tumor cell (CTC) enrichment from blood. Biomed Microdevices.
13:203–213. 2011. View Article : Google Scholar
|
|
29
|
Lin E, Cao T, Nagrath S and King MR:
Circulating tumor cells: Diagnostic and therapeutic applications.
Annu Rev Biomed Eng. 20:329–352. 2018. View Article : Google Scholar
|
|
30
|
Iliescu FS, Poenar DP, Yu F, Ni M, Chan
KH, Cima I, Taylor HK, Cima I and Iliescu C: Recent advances in
microfluidic methods in cancer liquid biopsy. Biomicrofluidics.
13:0415032019. View Article : Google Scholar
|
|
31
|
Zheng X, Fan L, Zhou P, Ma H, Huang S, Yu
D, Zhao L, Yang S, Liu J, Huang A, et al: Detection of circulating
tumor cells and circulating tumor microemboli in gastric cancer.
Transl Oncol. 10:431–441. 2017. View Article : Google Scholar :
|
|
32
|
Galanzha EI, Shashkov EV, Kelly T, Kim JW,
Yang L and Zharov VP: In vivo magnetic enrichment and multiplex
photoacoustic detection of circulating tumour cells. Nat
Nanotechnol. 4:855–860. 2009. View Article : Google Scholar :
|
|
33
|
Zhang H, Jia Z, Wu C, Zang L, Yang G, Chen
Z and Tang B: In vivo capture of circulating tumor cells based on
transfusion with a vein indwelling needle. ACS Appl Mater
Interfaces. 7:20477–20484. 2015. View Article : Google Scholar
|
|
34
|
Plaks V, Koopman CD and Werb Z: Cancer.
Circulating tumor cells. Science. 341:1186–1188. 2013. View Article : Google Scholar
|