Chemotherapeutics cardiotoxicity is a major concern
for clinicians treating different kinds of cancer, as it seriously
affects their treatment options and the survival of the patient.
The cut-off values for the identification of cardiotoxicity caused
by chemotherapeutics in humans differ between the American and
European guidelines: the definition considers a lower cut-off value
of normality for the left ventricular ejection fraction (LVEF) of
50% in Europe (1) and 53% in the
USA (2). Both Guidelines emphasize
that a drop of LVEF compared to the patient's previous values is
also required. This definition is crucial for patients and
clinicians, as patients presenting this decline in cardio-imaging
indices of cardiac function should be treated with angiotensin
converting enzyme inhibitors (ACEIs) or angiotensin II receptor
blockers (ARBs) in combination with β-blockers (3); nevertheless, modifications of
anticancer treatment in such patients remain a matter of discussion
among different specialists.
In animal studies, where new anticancer substances
are evaluated and different agents are tested to overcome
anticancer drugs cardiotoxicity, identification of the extent of
cardiotoxicity is crucial and necessary for the evaluation of any
favourable effects of the counteracting agent (4). In this regard, cardiac imaging is more
often used at analogy to the clinical setting. Biomarkers and
clinical signs of heart failure are also taken into consideration,
but cardiac imaging in animal studies has gained momentum.
At the same time, other pharmaceutical compounds,
such as anabolic steroids, along with everyday chemicals, such as
metals and pesticides, have been implicated to adversely affect
cardiac pathology causing function impairment (10). Toxicity and risk for human health
posed by chemicals are well controlled at a European level through
a thoroughly developed regulatory network. Nevertheless,
cardiotoxicity is not described as a separate hazard class and no
specific classification criteria are available in order to legally
classify chemicals well in advance as cardiotoxic and avoid
potential long-term cardiovascular complications, which could
significantly burden any national health system.
But, what is considered cardiotoxicity of anticancer
agents and specifically anthracyclines when parameters of cardiac
imaging are monitored in animal studies? Is there a uniformity in
animal models of anthracyclines cardiotoxicity induction and most
importantly, do all studies describe the same decline of myocardial
function? Addressing these issues could be of wider use both in
clinical medicine and practice, when assessing agents employed for
salvation to cardiotoxic complications during oncology treatment,
for example, as well as to regulators, when trying to establish
reference values in echocardiographic function representing
cardiotoxicity induced in animals by chemicals.
In the current in depth review, the identification
of most commonly used metrics of myocardial function in animal
studies of anthracycline induced cardiotoxicity are presented,
along with the range of these values differentiating normal cardiac
function from animals with pathological echocardiographic findings
indicative of anthracycline cardiotoxicity as per author
presentation.
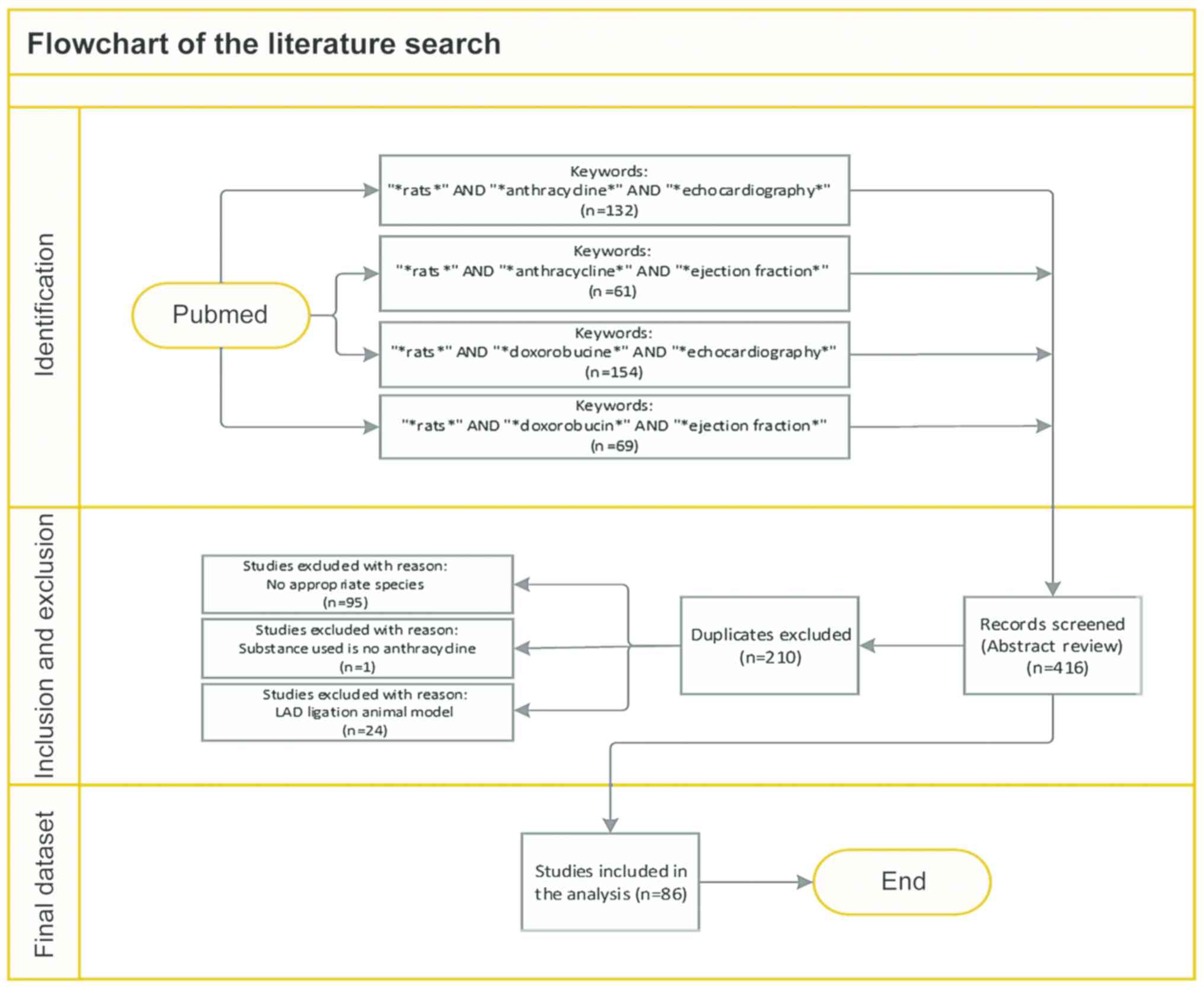
PubMed electronic database was systematically
searched to detect all original research studies published until
March 1, 2020, according to the Preferred Reporting Items for
Systematic Reviews and Meta-analyses (PRISMA) statement (11). The specific literature search
strategy used was: [AND (“*rats*” OR “*doxorubicin* OR
“*echocardiography*” OR “anthracycline” OR “*ejection fraction*”)]
either in the Title, or the Abstracts. The reference list of the
retrieved studies was further evaluated for the relevance of the
subject and the eligibility by screening the titles/abstracts of
full papers. The non-English citations (<5) were reviewed
separately. Animal data only from rat species were assessed, as it
is evident from the search string. All types of citations other
than original research studies (e.g., review articles) were
excluded. Two authors (NG and CT) independently assessed the title
and the abstract content (or both) of each record retrieved to
decide which studies should be further evaluated and extracted all
data. Disagreements were resolved through consensus or by
consultation with a third author (KT). A final draft of the
manuscript was prepared after several revisions and approved by all
authors. In total, 86 published manuscripts on animal studies were
considered for the systematic review (Fig. 1).
Despite the small size of the rat heart and the fast
heart rate, echocardiography is systematically used in the
evaluation of rat heart function (12). Data for 2 main indices of LV
contractility were extracted from the list of studies.
The first index is LV fractional shortening (FS) and
is calculated by the formula: FS (%) = [LV end-diastolic diameter
(LVDd) minus LV end-systolic diameter
(LVDs)]/LVDd × 100.
LVEF is the second and more common, index of LV
contractility. EF can be calculated from the equation: EF (%) =
[(LVDd3 - LVDs3) /
LVDd3] × 100 (13) or from the equation: EF (%) =
(LVEDV-LVESV)/LVEDV × 100, where LVEDV is the LV end-diastolic
volume and LVESV is LV end-systolic volume (12).
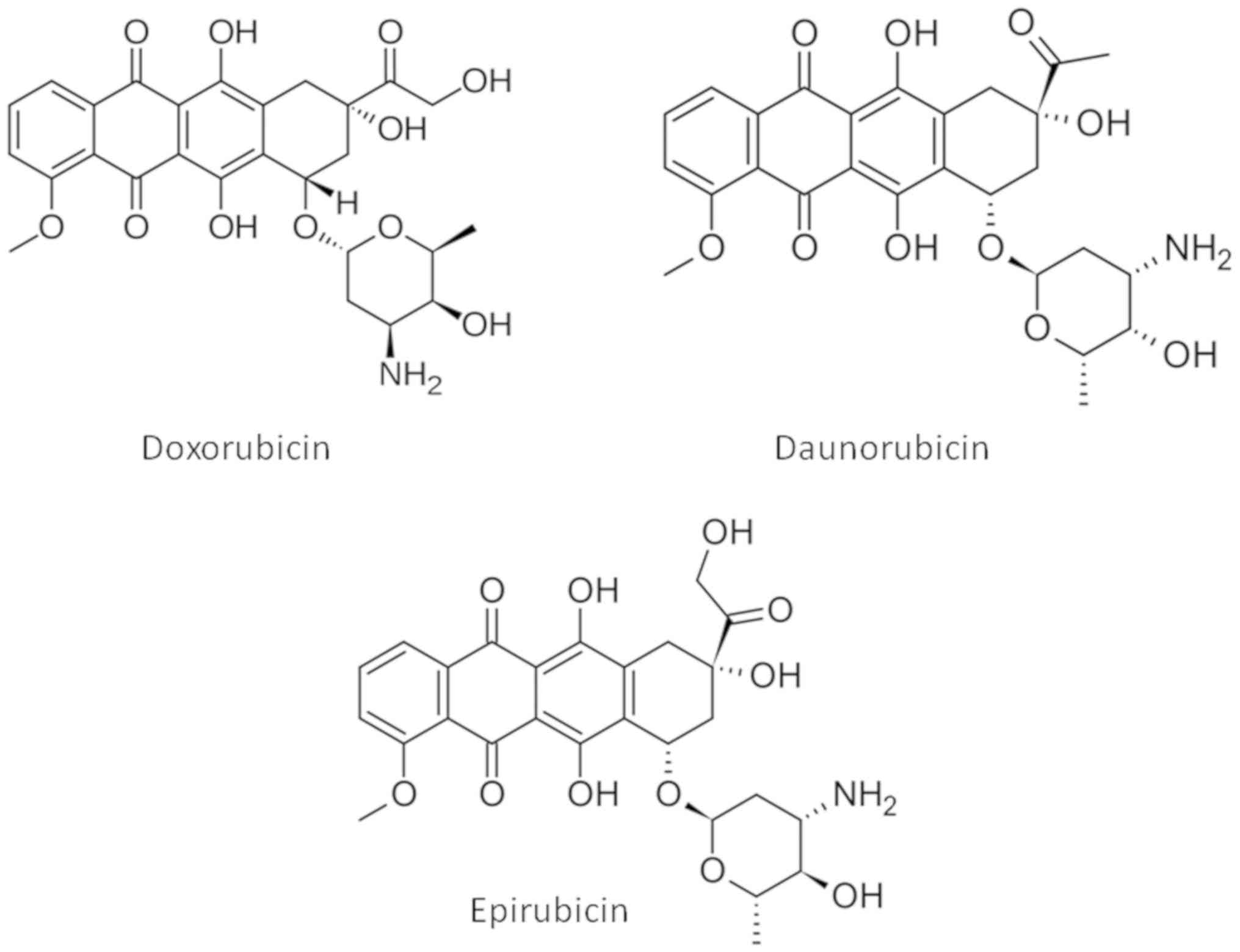
Exposure to anthracyclines suppresses both
echocardiographic indices. In the 86 studies reviewed in the
present report, Doxorubicin is almost universally used to induce
cardiotoxicity, along with Daunorubicin and Epirubicin in two
studies (Table I). The structures
of the three anthracyclines used are presented in Fig. 6. Anthracyclines were administered
with order of appearance either via intraperitoneal injection,
intravenous injection or orally with the feed. The doses were
administered once, twice, three times per week. The duration of the
dose administration spans from one week to ten weeks. In most of
the experiments, the benchmark for terminating the administration
was the proof of cardiac toxicity. The echocardiography values
suggest that there is no specific dose regime threshold which
indicates the establishment of the effect, but it is specific to
each experiment and probably dependent on other factors such as age
and general condition of the animals.
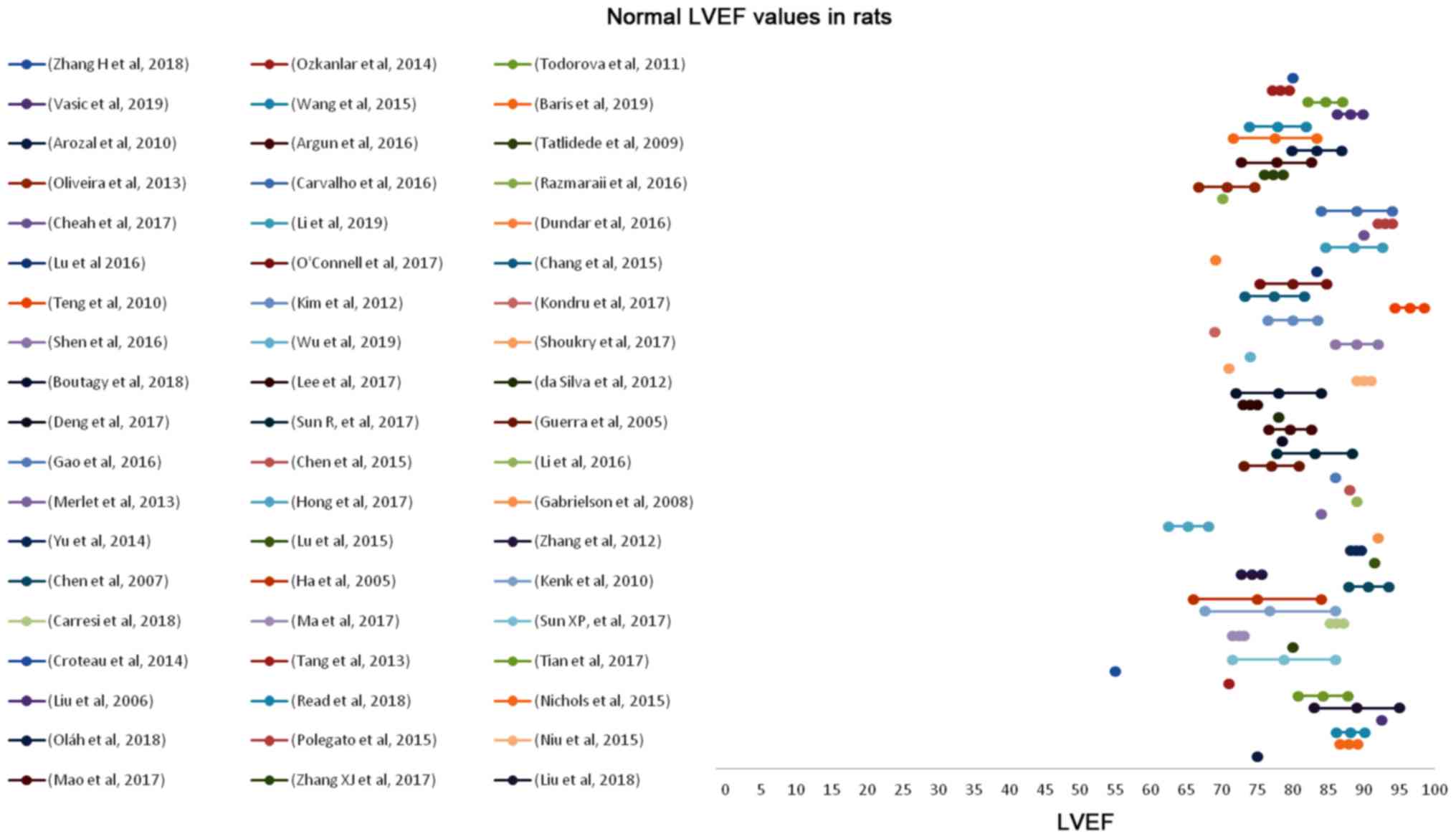
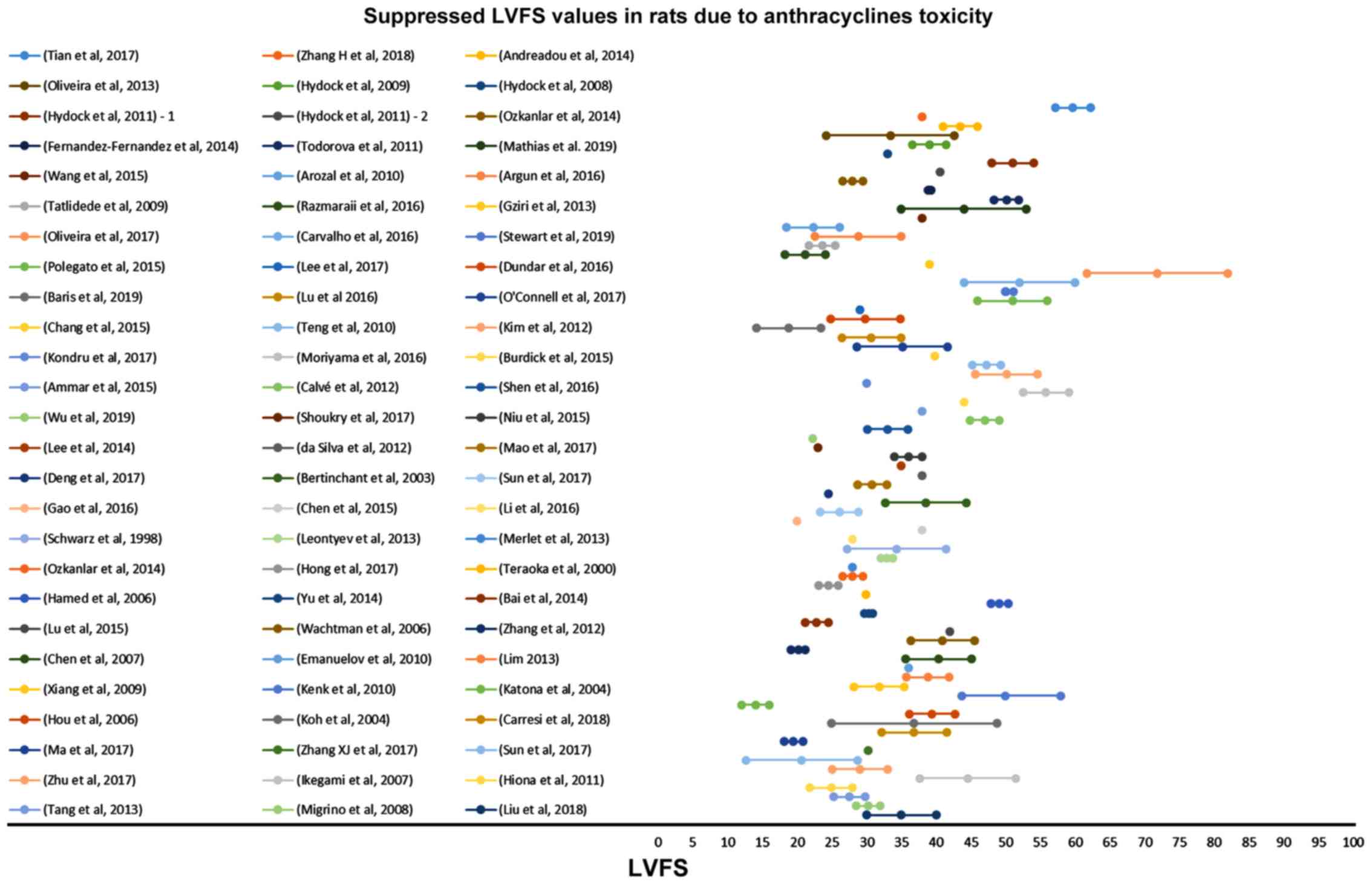
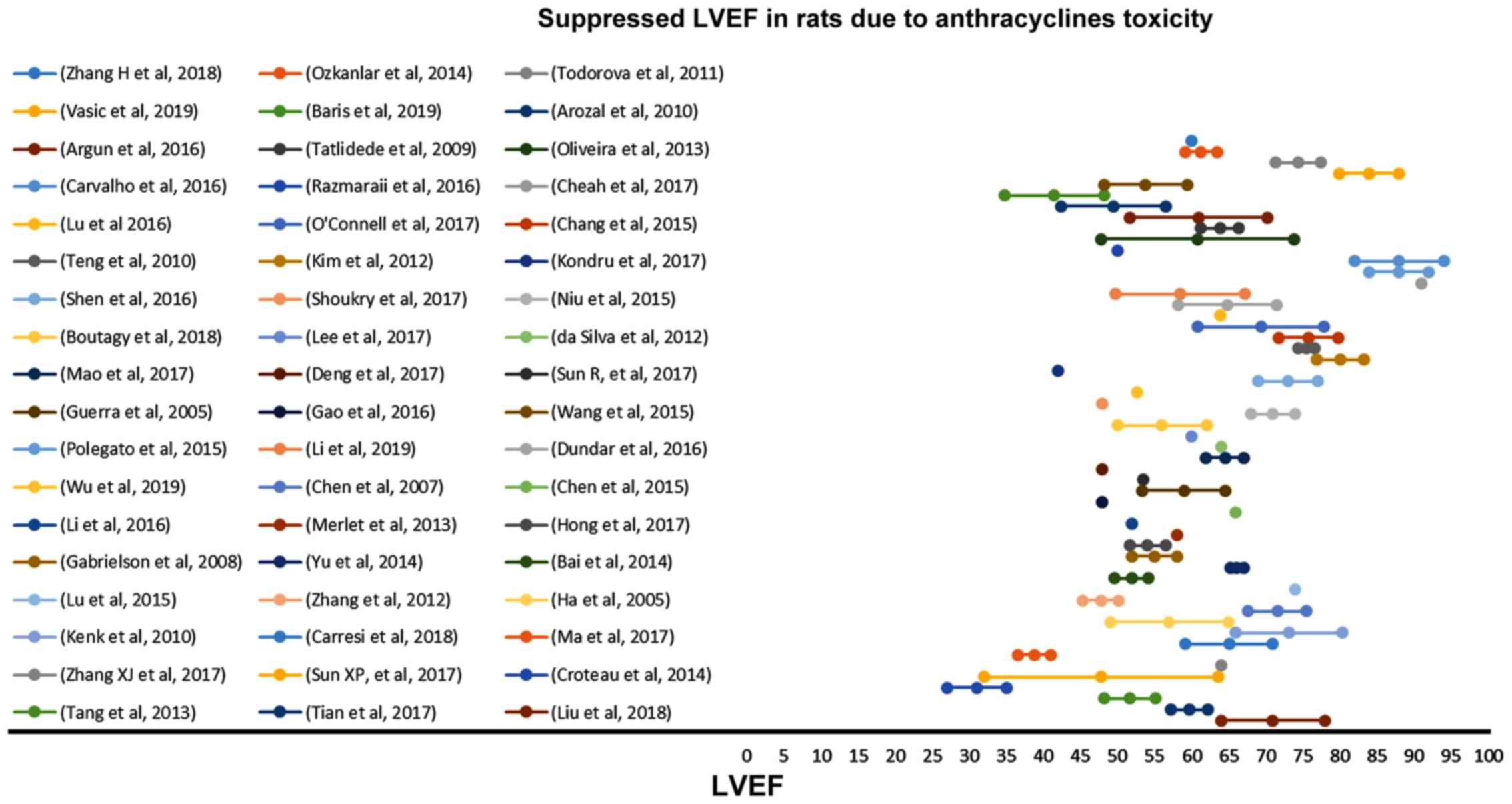
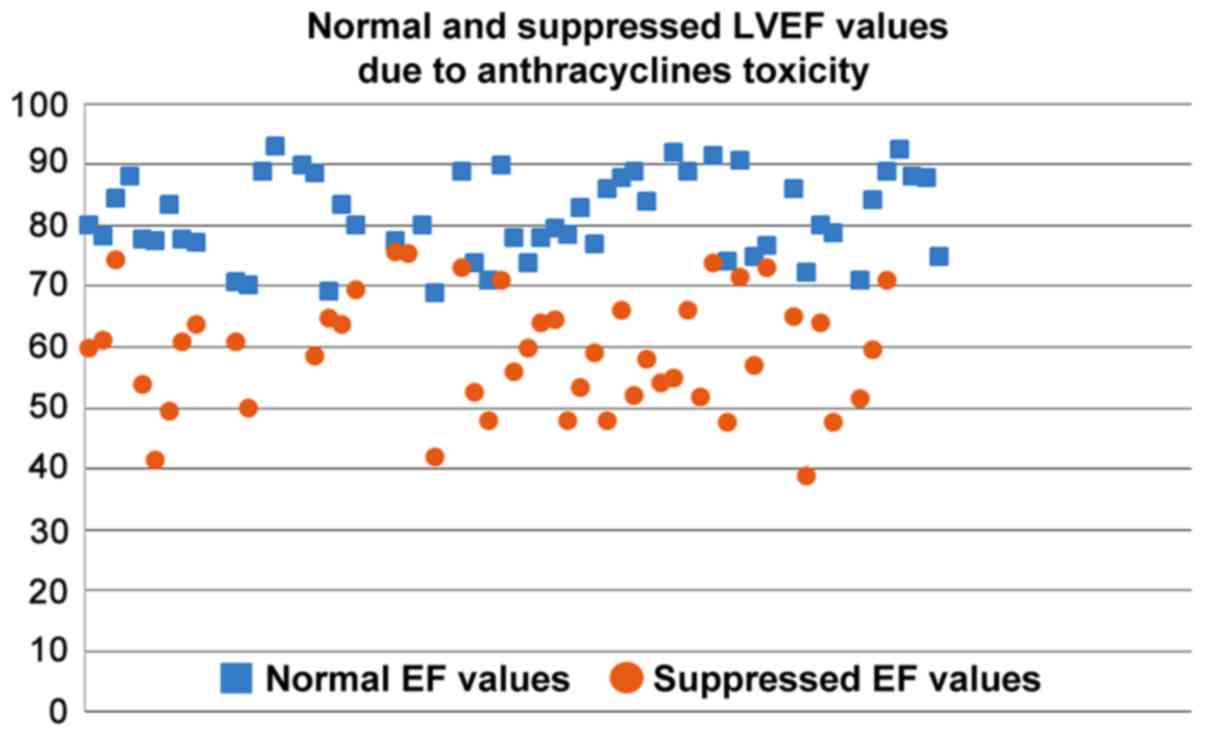
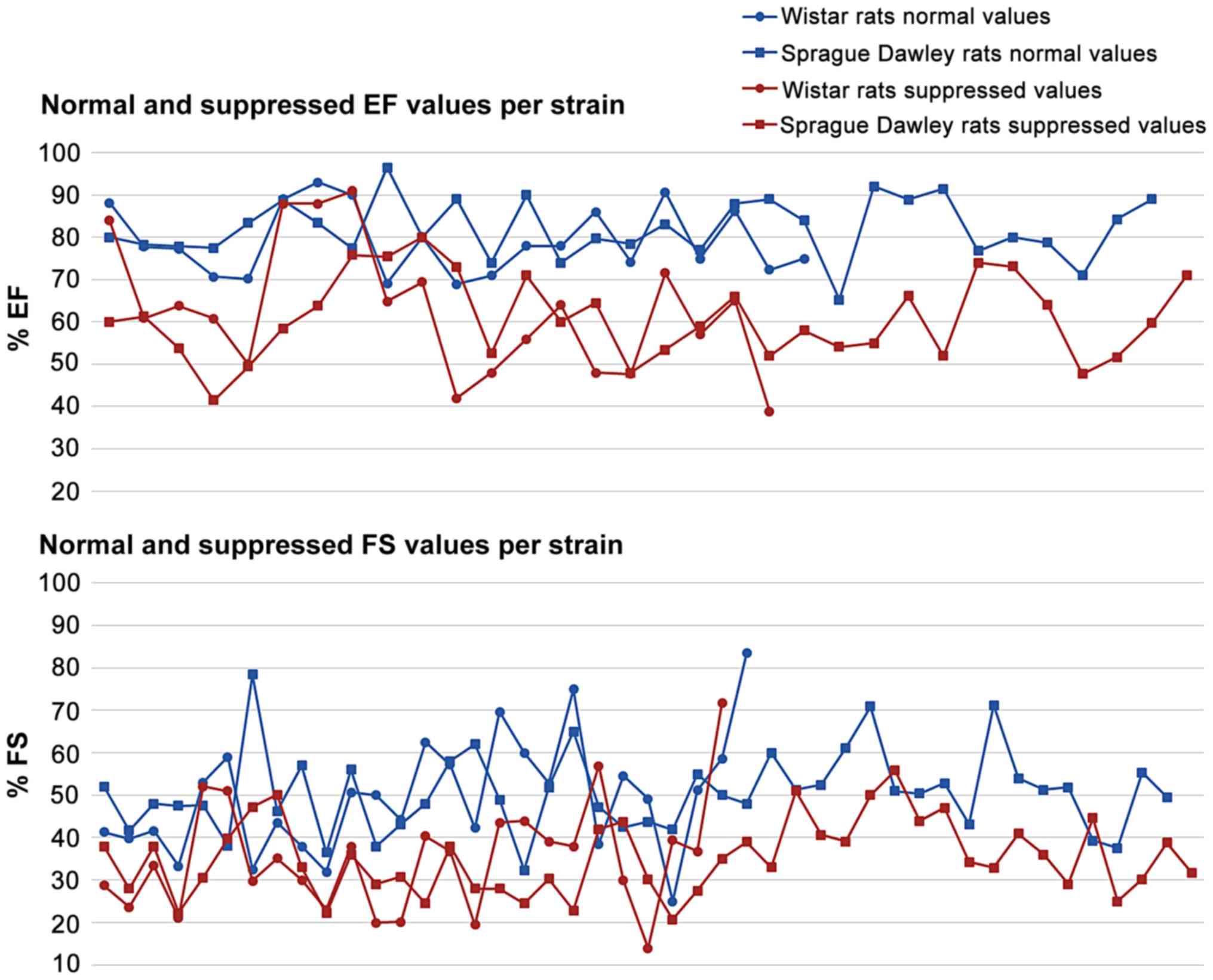
The suppressed %EF values reported from rats after
anthracyclines administration vary from 31 to 91% (Fig. 4). EF values 50–80% are reported in
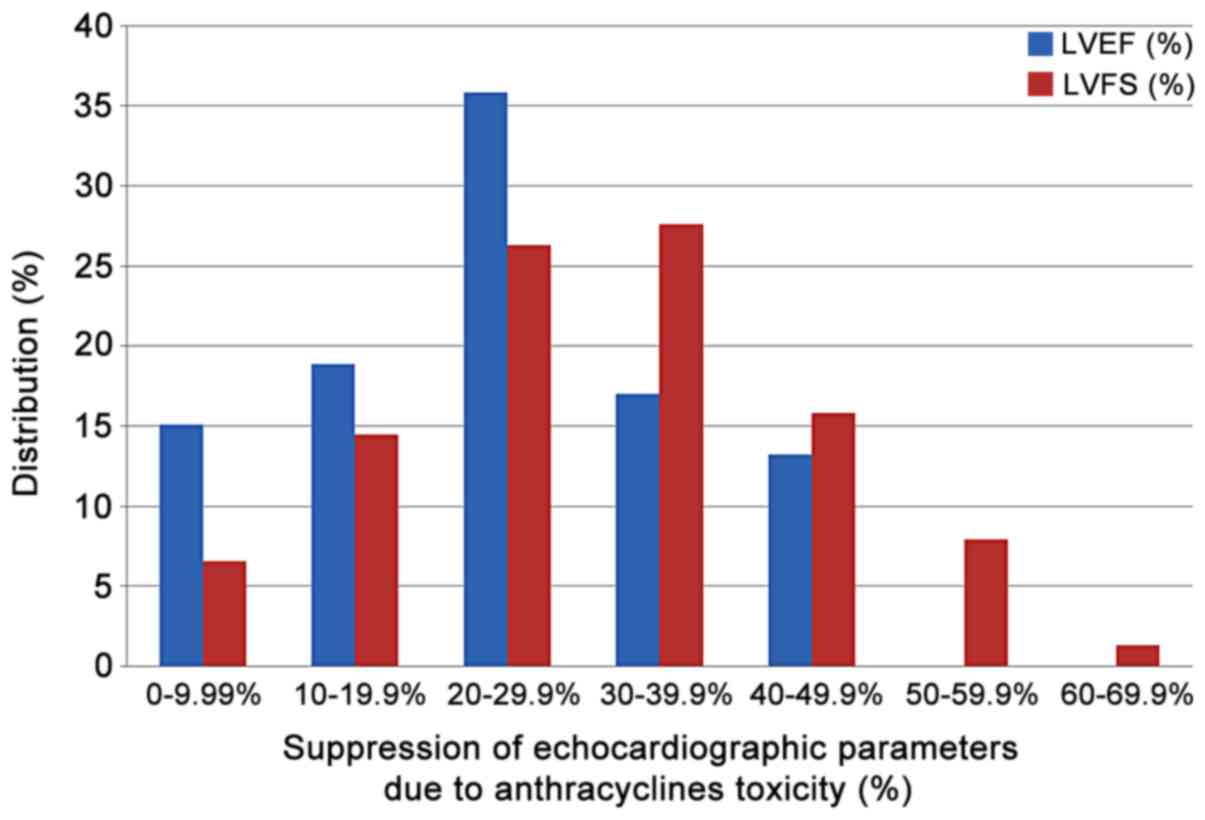
72.3% of the studies reviewed. Suppression of the %EF due to
anthracycline administration varies from 10 to 40% compared to the
normal values in more than two thirds of the studies reviewed
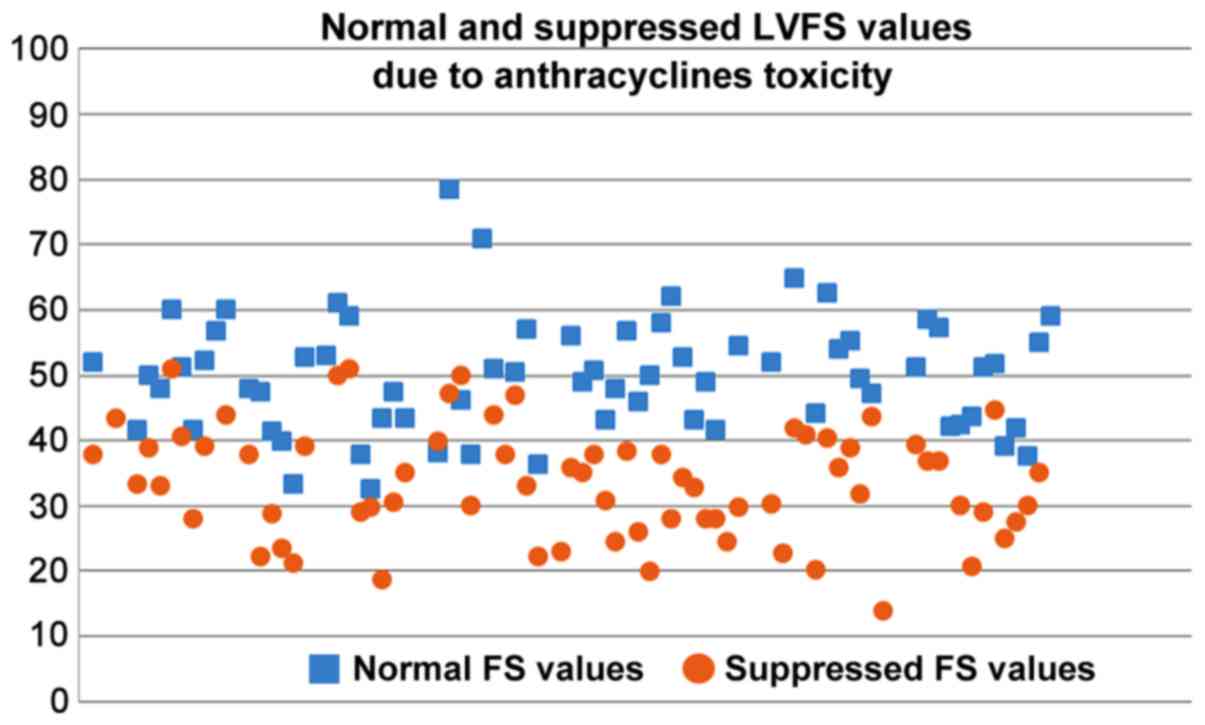
(71.7%) (Fig. 7). On the other
hand, suppressed %FS values ranging from 14 to 71.8%, present a
more narrow distribution (%FS values 20–50% in 84.6% of the
studies). As shown in Fig. 7, a
more equal distribution of the %FS suppression due to anthracycline
toxicity is observed with approximately one fourth of the studies
reporting 20–30% and 30–40% suppression, respectively. It is
evident from Figs 8 and 9 that normal and suppressed %EF and %FS
values separate sufficiently well. The rat strain does not seem to
influence either the normal or the suppressed %EF and %FS values
(Fig. 10).
Only 11 studies used an acute administration scheme,
with 3–20 mg/kg bw anthracycline single injection either
intravenously or intraperitoneally. Most of the studies used a
prolonged administration period, from 2 weeks (33 studies) up to 10
weeks, and cumulative doses ranging from 1 to 20 mg/kg bw. All
dosage schemes were carefully selected to induce cardiotoxicity and
did not seem to affect the suppression of %EF and %FS
monitored.
Myocardial contractility suppression due to
anthracycline administration is of increasing interest and
represents a major challenge in the clinical setting. At the same
time in a preclinical stage it serves as a model for the assessment
of both new chemotherapeutic and cardioprotective agents to be
introduced in clinical practice. The myocardial toxicity of
anthracyclines is known to be affected by sex and age, along with a
number of cardiovascular risk factors and comorbidities (99). It is found that anthracycline
related congestive heart failure reaches 10% of patients older than
65 years at usual doses (100).
While in early studies it was thought that EF cannot accurately
predict congestive heart failure attributed to doxorubicin
(100), current perspective is
that anthracycline-related cardiotoxicity is manifested by a
progressive continuous decline in LVEF (1) and identifying subclinical myocardial
dysfunction related to anthracycline treatment has great
therapeutic implications (2).
Preclinical animal studies are essential in cancer
chemotherapy research along with the evaluation of the cardiotoxic
propensity of the chemotherapeutic agents. The current
recommendations for prevention of cardiac events from cancer
chemotherapies are largely based on recommendations. The American
Society of Clinical Oncology, for example, recommends active
screening and prevention of modifiable cardiovascular risk factors,
such as tobacco use, high blood pressure, high cholesterol, alcohol
use, obesity and physical inactivity (101). A well characterized animal model
for defining cardiotoxicity due to chemotherapy and the treatment
thereof is of great importance for clinical practice, as it will
enable physicians to base their decisions not only on epidemiology
but also on observations developed using concrete data from animal
studies.
In the present review, the range of the main
echocardiographic indices, namely EF and FS, used in describing
anthracycline cardiotoxicity in rats was summarized along with the
normal values of the said indices presented in the respective
studies. In the graphic representation, it seems that normal and
suppressed values due to anthracyclines administration for the two
echocardiographic indices are well separated. This provides the
first evidence for the possibility of setting a cut-off point for
defining anthracycline cardiotoxicity in rats with an in-depth
future meta-analysis.
In the current study a wide range of EF and FS
decline due to anthracycline administration was observed. However,
the trends of the said decline are easily identified, especially
for FS values, thus rendering the establishment of minimum cut off
values of decline feasible. The question remains, as it has also
been identified for humans, whether the absolute suppressed values
of EF and FS, combined or separately, or the % suppression caused
by anthracyclines should be used to describe cardiotoxicity, and
which of the two approaches could be more effective in prevention.
In our study, it seems that setting a range for % suppression of EF
and FS could be more efficient in identifying early cardiotoxicity
by counteracting the intra-individual variation of the absolute
values.
In the current in depth review analysis, we did not
identify differences between rat strains in terms of suppressed EF
and FS values due to anthracycline administration. This is an
interesting finding as it seems that the usual strains used in rat
studies are equally prone to the cardiotoxic anthracycline
potential. In animal models of genetically programmed hypertension
and heart failure, it is found that doxorubicin administration did
not lead to lower myocardial contractility compared to
non-genetically modified strains (102). In addition, in the current
systematic review, acute and chronic anthracyclines cardiotoxicity
models were found equally potent in inducing cardiotoxicity based
on evaluated echocardiographic indices.
Currently, when assessing chemicals toxicity,
cardiac effects if monitored and detected in animal studies, mainly
on the tissue level, are considered by the authorities, but
cardiotoxicity, as such, is not described as a separate hazard
class of chemical substances through the available regulations,
both at a European level and world-wide. Therefore, chemicals other
than pharmaceutical agents are recognised to be cardiotoxic after
having exerted such deleterious effects on humans, based on
epidemiological studies. In a previous review of our research team,
the cardiac pathology and function impairment due to exposure to
pesticides revealed that several cardiovascular complications have
been reported in animal models including electrocardiogram
abnormalities, myocardial infarction, impaired systolic and
diastolic performance and histopathological findings, such as
haemorrhage, vacuolization, signs of apoptosis and degeneration
(103). In addition, there is
evidence that short and/or long-term exposure to anabolic
androgenic steroids is linked to a variety of cardiovascular
complications which could be identified by using echocardiography
or biochemical markers (10,104,105).
The published data suggest clearly that there is a need to
establish regulatory criteria for assessing cardiotoxicity as an
inherent property of a chemical substance well in advance, and
characterize the risk of exposure to such chemicals through a
well-developed regulatory network based on animal models, as is the
case for other human health hazard classes, such as
carcinogenicity. Regulatory established criteria will enable
international organizations to early identify cardiotoxic effects
and classify chemicals in order to avoid long-term cardiovascular
complications. Specific classification criteria should be developed
based on anatomical, histopathological, echocardiographic and
biochemical criteria in animals developed in a way that could
exclude confounding factors in the development of the observed
cardiotoxicity. The results of the present study are promising in
identifying echocardiographic criteria in rats for the
establishment of cardiotoxicity. Further studies and meta-analyses
are needed in order to evaluate other species, commonly used in
research, and explore the possibility of early recognizing the
onset of cardiotoxicity, possibly through monitoring of biochemical
markers based on understanding of the mode of action.
No funding was received.
All authors have read and approved the final version
of this manuscript. This report is part of the PhD Thesis of NG
supervised by DS, KTo and DK and performed in the University of
Thessaly. NG: organization and performing of the research,
collecting data, writing of the research article. KT, CT:
conceptualization of the project, setting criteria for the
research, verification of the results, reviewing the manuscript,
the statistics and the reference list, overall project management.
RR, HN, GENK, JLCMD: data extraction, evaluation of the results,
statistical analysis. DAS, DS, KTo, DK, CT: overall project
overview, data assessment, evaluation of the results, evaluation of
the applicability of the findings, reviewing and writing of the
research article and plan assessment.
DAS is the Editor-in-Chief for the journal, but had
no personal involvement in the reviewing process, or any influence
in terms of adjudicating on the final decision, for this article.
The positions and opinions presented in this article are those of
the authors (NG, GENK, JLCMD) alone and are not intended to
represent the views or any official position or scientific works of
the European Agencies EFSA and ECHA. The other authors declare that
they have no competing interests.
|
1
|
Zamorano JL, Lancellotti P, Rodriguez
Muñoz D, Aboyans V, Asteggiano R, Galderisi M, Habib G, Lenihan DJ,
Lip GYH, Lyon AR, et al ESC Scientific Document Group, : 2016 ESC
Position Paper on cancer treatments and cardiovascular toxicity
developed under the auspices of the ESC Committee for Practice
Guidelines: The Task Force for cancer treatments and cardiovascular
toxicity of the European Society of Cardiology (ESC). Eur Heart J.
37:2768–2801. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Plana JC, Galderisi M, Barac A, Ewer MS,
Ky B, Scherrer-Crosbie M, Ganame J, Sebag IA, Agler DA, Badano LP,
et al: Expert consensus for multimodality imaging evaluation of
adult patients during and after cancer therapy: A report from the
American Society of Echocardiography and the European Association
of Cardiovascular Imaging. J Am Soc Echocardiogr. 27:911–939. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Pardo Sanz A and Zamorano JL:
‘Cardiotoxicity’: time to define new targets? Eur Heart J.
41:1730–1732. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Park CJ, Branch ME, Vasu S and Melendez
GC: The role of cardiac MRI in animal models of cardiotoxicity:
hopes and challenges. J Cardiovasc Transl Res. Apr 4–2020.(Epub
ahead of print). View Article : Google Scholar
|
|
5
|
Sobczuk P, Czerwinska M, Kleibert M and
Cudnoch-Jedrzejewska A: Anthracycline-induced cardiotoxicity and
renin-angiotensin-aldosterone system-from molecular mechanisms to
therapeutic applications. Heart Fail Rev. May 30–2020.(Epub ahead
of print). View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hashemzaei M, Karami SP, Delaramifar A,
Sheidary A, Tabrizian K, Rezaee R, Shahsavand S, Arsene AL,
Tsatsakis AM and Mohammad S: Anticancer effects of
co-administration of daunorubicin and resveratrol in MOLT-4, U266
B1 and RAJI cell lines. Farmacia. 64:36–42. 2016.
|
|
7
|
Iranshahi M, Barthomeuf C, Bayet-Robert M,
Chollet P, Davoodi D, Piacente S, Rezaee R and Sahebkar A:
Drimane-type sesquiterpene coumarins from ferula gummosa fruits
enhance doxorubicin uptake in doxorubicin-resistant human breast
cancer cell line. J Tradit Complement Med. 4:118–125. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Schwarz ER, Pollick C, Dow J, Patterson M,
Birnbaum Y and Kloner RA: A small animal model of non-ischemic
cardiomyopathy and its evaluation by transthoracic
echocardiography. Cardiovasc Res. 39:216–223. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Robert J: Preclinical assessment of
anthracycline cardiotoxicity in laboratory animals: Predictiveness
and pitfalls. Cell Biol Toxicol. 23:27–37. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Germanakis I, Tsarouhas K, Fragkiadaki P,
Tsitsimpikou C, Goutzourelas N, Champsas MC, Stagos D, Rentoukas E
and Tsatsakis AM: Oxidative stress and myocardial dysfunction in
young rabbits after short term anabolic steroids administration.
Food Chem Toxicol. 61:101–105. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Moher D, Shamseer L, Clarke M, Ghersi D,
Liberati A, Petticrew M, Shekelle P and Stewart LA; PRISMA-P Group,
: Preferred reporting items for systematic review and meta-analysis
protocols (PRISMA-P) 2015 statement. Syst Rev. 4:12015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zacchigna S, Paldino A, Falcao-Pires I,
Daskalopoulos EP, Dal Ferro M, Vodret S, Lesizza P, Cannatà A,
Daniela Miranda-Silva D, et al: Toward standardization of
echocardiography for the evaluation of left ventricular function in
adult rodents: a position paper of the ESC Working Group on
Myocardial Function. Cardiovasc Res. May 4–2020.(Epub ahead of
print). View Article : Google Scholar
|
|
13
|
Liu J and Rigel DF: Echocardiographic
examination in rats and mice. Methods Mol Biol. 573:139–155. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhang H, Lu X, Liu Z and Du K:
Rosuvastatin reduces the pro-inflammatory effects of adriamycin on
the expression of HMGB1 and RAGE in rats. Int J Mol Med.
42:3415–3423. 2018.PubMed/NCBI
|
|
15
|
Tian XQ, Ni XW, Xu HL, Zheng L, ZhuGe DL,
Chen B, Lu CT, Yuan JJ and Zhao YZ: Prevention of
doxorubicin-induced cardiomyopathy using targeted MaFGF mediated by
nanoparticles combined with ultrasound-targeted MB destruction. Int
J Nanomedicine. 12:7103–7119. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Andreadou I, Mikros E, Ioannidis K, Sigala
F, Naka K, Kostidis S, Farmakis D, Tenta R, Kavantzas N, Bibli SI,
et al: Oleuropein prevents doxorubicin-induced cardiomyopathy
interfering with signaling molecules and cardiomyocyte metabolism.
J Mol Cell Cardiol. 69:4–16. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Oliveira MS, Melo MB, Carvalho JL, Melo
IM, Lavor MSI, Gomes DA, de Goes AM and Melo MM: Doxorubicin
cardiotoxicity and cardiac function improvement after stem cell
therapy diagnosed by strain echocardiography. J Cancer Sci Ther.
5:52–57. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hydock DS, Lien CY and Hayward R:
Anandamide preserves cardiac function and geometry in an acute
doxorubicin cardiotoxicity rat model. J Cardiovasc Pharmacol Ther.
14:59–67. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Fernandez-Fernandez A, Carvajal DA, Lei T
and McGoron AJ: Chemotherapy-induced changes in cardiac capillary
permeability measured by fluorescent multiple indicator dilution.
Ann Biomed Eng. 42:2405–2415. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Todorova VK, Kaufmann Y and Klimberg VS:
Increased efficacy and reduced cardiotoxicity of metronomic
treatment with cyclophosphamide in rat breast cancer. Anticancer
Res. 31:215–220. 2011.PubMed/NCBI
|
|
21
|
Vasić M, Lončar-Turukalo T, Tasić T, Matić
M, Glumac S, Bajić D, Popović B and Japundžić-Žigon N:
Cardiovascular variability and β-ARs gene expression at two stages
of doxorubicin-induced cardiomyopathy. Toxicol Appl Pharmacol.
362:43–51. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Mathias LMBS, Alegre PHC, Dos Santos IOF,
Bachiega T, Figueiredo AM, Chiuso-Minicucci F, Fernandes AA, Bazan
SGZ, Minicucci MF, Azevedo PS, et al: Euterpe oleracea Mart.
(Açai) supplementation attenuates acute doxorubicin-induced
cardiotoxicity in rats. Cell Physiol Biochem. 53:388–399. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wang X, Chen L, Wang T, Jiang X, Zhang H,
Li P, Lv B and Gao X: Ginsenoside Rg3 antagonizes
adriamycin-induced cardiotoxicity by improving endothelial
dysfunction from oxidative stress via upregulating the Nrf2-ARE
pathway through the activation of akt. Phytomedicine. 22:875–884.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Arozal W, Watanabe K, Veeraveedu PT,
Thandavarayan RA, Harima M, Sukumaran V, Suzuki K, Kodama M and
Aizawa Y: Effect of telmisartan in limiting the cardiotoxic effect
of daunorubicin in rats. J Pharm Pharmacol. 62:1776–1783. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Argun M, Üzüm K, Sönmez MF, Özyurt A,
Derya K, Çilenk KT, Unalmış S, Pamukcu Ö, Baykan A, Narin F, et al:
Cardioprotective effect of metformin against doxorubicin
cardiotoxicity in rats. Anatol J Cardiol. 16:234–241.
2016.PubMed/NCBI
|
|
26
|
Tatlidede E, Sehirli O, Velioğlu-Oğünc A,
Cetinel S, Yeğen BC, Yarat A, Süleymanoğlu S and Sener G:
Resveratrol treatment protects against doxorubicin-induced
cardiotoxicity by alleviating oxidative damage. Free Radic Res.
43:195–205. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Razmaraii N, Babaei H, Mohajjel Nayebi A,
Assadnassab G, Ashrafi Helan J and Azarmi Y: Crocin treatment
prevents doxorubicin-induced cardiotoxicity in rats. Life Sci.
157:145–151. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Gziri MM, Pokreisz P, De Vos R, Verbeken
E, Debiève F, Mertens L, Janssens SP and Amant F: Fetal rat hearts
do not display acute cardiotoxicity in response to maternal
Doxorubicin treatment. J Pharmacol Exp Ther. 346:362–369. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Oliveira LF, O'Connell JL, Carvalho EE,
Pulici ECC, Romano MMD, Maciel BC and Simões MV: Comparison between
radionuclide ventriculography and echocardiography for
quantification of left ventricular systolic function in rats
exposed to doxorubicin. Arq Bras Cardiol. 108:12–20.
2017.PubMed/NCBI
|
|
30
|
Carvalho PB, Gonçalves AF, Alegre PH,
Azevedo PS, Roscani MG, Bergamasco CM, Modesto PN, Fernandes AA,
Minicucci MF, Paiva SA, et al: Pamidronate attenuates oxidative
stress and energetic metabolism changes but worsens functional
outcomes in acute doxorubicin-induced cardiotoxicity in rats. Cell
Physiol Biochem. 40:431–442. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Stewart LK, Smoak P, Hydock DS, Hayward R,
O'Brien K, Lisano JK, Boeneke C, Christensen M and Mathias A: Milk
and kefir maintain aspects of health during doxorubicin treatment
in rats. J Dairy Sci. 102:1910–1917. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Polegato BF, Minicucci MF, Azevedo PS,
Carvalho RF, Chiuso-Minicucci F, Pereira EJ, Paiva SA, Zornoff LA,
Okoshi MP, Matsubara BB, et al: Acute doxorubicin-induced
cardiotoxicity is associated with matrix metalloproteinase-2
alterations in rats. Cell Physiol Biochem. 35:1924–1933. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Lee KH, Cho H, Lee S, Woo JS, Cho BH, Kang
JH, Jeong YM, Cheng XW and Kim W: Enhanced-autophagy by exenatide
mitigates doxorubicin-induced cardiotoxicity. Int J Cardiol.
232:40–47. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Cheah HY, Šarenac O, Arroyo JJ, Vasić M,
Lozić M, Glumac S, Hoe SZ, Hindmarch CCT, Murphy D, Kiew LV, et al:
Hemodynamic effects of HPMA copolymer based doxorubicin conjugate:
A randomized controlled and comparative spectral study in conscious
rats. Nanotoxicology. 11:210–222. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Li X, Xu G, Wei S, Zhang B, Yao H, Chen Y,
Liu W, Wang B, Zhao J and Gao Y: Lingguizhugan decoction attenuates
doxorubicin-induced heart failure in rats by improving TT-SR
microstructural remodeling. BMC Complement Altern Med. 19:3602019.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Dundar HA, Kiray M, Kir M, Kolatan E,
Bagriyanik A, Altun Z, Aktas S, Ellidokuz H, Yilmaz O, Mutafoglu K,
et al: Protective effect of acetyl-L-carnitine against
doxorubicin-induced cardiotoxicity in wistar albino rats. Arch Med
Res. 47:506–514. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Barış VO, Gedikli E, Yersal N, Müftüoğlu S
and Erdem A: Protective effect of taurine against
doxorubicin-induced cardiotoxicity in rats: Echocardiographical and
histological findings. Amino Acids. 51:1649–1655. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Lu PP, Ma J, Liang XP, Guo CX, Yang YK,
Yang KQ, Shen QM, Ma LH and Zhou XL: Xinfuli improves cardiac
function, histopathological changes and attenuate cardiomyocyte
apoptosis in rats with doxorubicin-induced cardiotoxicity. J
Geriatr Cardiol. 13:968–972. 2016.PubMed/NCBI
|
|
39
|
O'Connell JL, Romano MM, Campos Pulici EC,
Carvalho EEV, de Souza FR, Tanaka DM, Maciel BC, Salgado HC,
Fazan-Júnior R, Rossi MA, et al: Short-term and long-term models of
doxorubicin-induced cardiomyopathy in rats: A comparison of
functional and histopathological changes. Exp Toxicol Pathol.
69:213–219. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Chang SA, Lim BK, Lee YJ, Hong MK, Choi JO
and Jeon ES: A novel angiotensin type I receptor antagonist,
Fimasartan, prevents Doxorubicin-induced cardiotoxicity in rats. J
Korean Med Sci. 30:559–568. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Teng LL, Shao L, Zhao YT, Yu X, Zhang DF
and Zhang H: The beneficial effect of n-3 polyunsaturated fatty
acids on doxorubicin-induced chronic heart failure in rats. J Int
Med Res. 38:940–948. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Kim YH, Kim M, Park SM, Kim SH, Lim SY,
Ahn JC, Song WH and Shim WJ: Discordant impairment of
multidirectional myocardial deformation in rats with Doxorubicin
induced cardiomyopathy. Echocardiography. 29:720–728. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Kondru SK, Potnuri AG, Allakonda L and
Konduri P: Histamine 2 receptor antagonism elicits protection
against doxorubicin-induced cardiotoxicity in rodent model. Mol
Cell Biochem. 441:77–88. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Moriyama T, Kemi M and Horie T: Elevated
cardiac 3-deoxyglucosone, a highly reactive intermediate in
glycation reaction, in doxorubicin-induced cardiotoxicity in rats.
Pathophysiology. 23:237–242. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Burdick J, Berridge B and Coatney R:
Strain echocardiography combined with pharmacological stress test
for early detection of anthracycline induced cardiomyopathy. J
Pharmacol Toxicol Methods. 73:15–20. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Ammar HI, Sequiera GL, Nashed MB, Ammar
RI, Gabr HM, Elsayed HE, Sareen N, Rub EA, Zickri MB and Dhingra S:
Comparison of adipose tissue- and bone marrow-derived mesenchymal
stem cells for alleviating doxorubicin-induced cardiac dysfunction
in diabetic rats. Stem Cell Res Ther. 6:1482015. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Calvé A, Haddad R, Barama SN, Meilleur M,
Sebag IA and Chalifour LE: Cardiac response to doxorubicin and
dexrazoxane in intact and ovariectomized young female rats at rest
and after swim training. Am J Physiol Heart Circ Physiol.
302:H2048–H2057. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Shen LJ, Lu S, Zhou YH, Li L, Xing QM and
Xu YL: Developing a rat model of dilated cardiomyopathy with
improved survival. J Zhejiang Univ Sci B. 17:975–983. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Wu Z, Zhao X, Miyamoto A, Zhao S, Liu C,
Zheng W and Wang H: Effects of steroidal saponins extract from
Ophiopogon japonicus root ameliorates doxorubicin-induced chronic
heart failure by inhibiting oxidative stress and inflammatory
response. Pharm Biol. 57:176–183. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Shoukry HS, Ammar HI, Rashed LA, Zikri MB,
Shamaa AA, Abou Elfadl SG, Rub EA, Saravanan S and Dhingra S:
Prophylactic supplementation of resveratrol is more effective than
its therapeutic use against doxorubicin induced cardiotoxicity.
PLoS One. 12:e01815352017. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Niu QY, Li ZY, Du GH and Qin XM: (1)H NMR
based metabolomic profiling revealed doxorubicin-induced systematic
alterations in a rat model. J Pharm Biomed Anal. 118:338–348. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Boutagy NE, Wu J, Cai Z, Zhang W, Booth
CJ, Kyriakides TC, Pfau D, Mulnix T, Liu Z, Miller EJ, et al: In
vivo reactive oxygen species detection with a novel positron
emission tomography tracer, 18F-DHMT, allows for early detection of
anthracycline-induced cardiotoxicity in rodents. JACC Basic Transl
Sci. 3:378–390. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Lee PJ, Rudenko D, Kuliszewski MA, Liao C,
Kabir MG, Connelly KA and Leong-Poi H: Survivin gene therapy
attenuates left ventricular systolic dysfunction in doxorubicin
cardiomyopathy by reducing apoptosis and fibrosis. Cardiovasc Res.
101:423–433. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
da Silva MG, Mattos E, Camacho-Pereira J,
Domitrovic T, Galina A, Costa MW and Kurtenbach E: Cardiac systolic
dysfunction in doxorubicin-challenged rats is associated with
upregulation of MuRF2 and MuRF3 E3 ligases. Exp Clin Cardiol.
17:101–109. 2012.PubMed/NCBI
|
|
55
|
Mao C, Hou X, Wang B, Chi J, Jiang Y,
Zhang C and Li Z: Intramuscular injection of human umbilical
cord-derived mesenchymal stem cells improves cardiac function in
dilated cardiomyopathy rats. Stem Cell Res Ther. 8:182017.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Deng B, Wang JX, Hu XX, Duan P, Wang L, Li
Y and Zhu QL: Nkx2.5 enhances the efficacy of mesenchymal stem
cells transplantation in treatment heart failure in rats. Life Sci.
182:65–72. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Bertinchant JP, Polge A, Juan JM,
Oliva-Lauraire MC, Giuliani I, Marty-Double C, Burdy JY,
Fabbro-Peray P, Laprade M, Bali JP, et al: Evaluation of cardiac
troponin I and T levels as markers of myocardial damage in
doxorubicin-induced cardiomyopathy rats, and their relationship
with echocardiographic and histological findings. Clin Chim Acta.
329:39–51. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Sun R, Wang J, Zheng Y, Li X, Xie T, Li R,
Liu M, Cao Y, Lu L, Zhang Q, et al: Traditional Chinese medicine
baoxin decoction improves cardiac fibrosis of rats with dilated
cardiomyopathy. Exp Ther Med. 13:1900–1906. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Guerra J, De Jesus A, Santiago-Borrero P,
Roman-Franco A, Rodríguez E and Crespo MJ: Plasma nitric oxide
levels used as an indicator of doxorubicin-induced cardiotoxicity
in rats. Hematol J. 5:584–588. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Gao Y, Yang H, Fan Y, Li L, Fang J and
Yang W: Hydrogen-rich saline attenuates cardiac and hepatic injury
in doxorubicin rat model by inhibiting inflammation and apoptosis.
Mediators Inflamm. 2016:13203652016. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Chen Y, Tang Y, Xiang Y, Xie YQ, Huang XH
and Zhang YC: Shengmai injection improved doxorubicin-induced
cardiomyopathy by alleviating myocardial endoplasmic reticulum
stress and caspase-12 dependent apoptosis. BioMed Res Int.
2015:9526712015.PubMed/NCBI
|
|
62
|
Li H, Mao Y, Zhang Q, Han Q, Man Z, Zhang
J, Wang X, Hu R, Zhang X, Irwin DM, et al: Xinmailong mitigated
epirubicin-induced cardiotoxicity via inhibiting autophagy. J
Ethnopharmacol. 192:459–470. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Leontyev S, Schlegel F, Spath C, Schmiedel
R, Nichtitz M, Boldt A, Rübsamen R, Salameh A, Kostelka M, Mohr FW,
et al: Transplantation of engineered heart tissue as a biological
cardiac assist device for treatment of dilated cardiomyopathy. Eur
J Heart Fail. 15:23–35. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Merlet N, Piriou N, Rozec B, Grabherr A,
Lauzier B, Trochu JN and Gauthier C: Increased beta2-adrenoceptors
in doxorubicin-induced cardiomyopathy in rat. PLoS One.
8:e647112013. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Ozkanlar Y, Aktas MS, Turkeli M, Erturk N,
Oruc E, Ozkanlar S, Kirbas A, Erdemci B and Aksakal E: Effects of
ramipril and darbepoetin on electromechanical activity of the heart
in doxorubicin-induced cardiotoxicity. Int J Cardiol. 173:519–521.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Hong YM, Lee H, Cho MS and Kim KC:
Apoptosis and remodeling in adriamycin-induced cardiomyopathy rat
model. Korean J Pediatr. 60:365–372. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Teraoka K, Hirano M, Yamaguchi K and
Yamashina A: Progressive cardiac dysfunction in adriamycin-induced
cardiomyopathy rats. Eur J Heart Fail. 2:373–378. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Hamed S, Barshack I, Luboshits G, Wexler
D, Deutsch V, Keren G and George J: Erythropoietin improves
myocardial performance in doxorubicin-induced cardiomyopathy. Eur
Heart J. 27:1876–1883. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Gabrielson KL, Mok GS, Nimmagadda S, Bedja
D, Pin S, Tsao A, Wang Y, Sooryakumar D, Yu SJ, Pomper MG, et al:
Detection of dose response in chronic doxorubicin-mediated cell
death with cardiac technetium 99m annexin V single-photon emission
computed tomography. Mol Imaging. 7:132–138. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Yu Q, Li Q, Na R, Li X, Liu B, Meng L,
Liutong H, Fang W, Zhu N and Zheng X: Impact of repeated
intravenous bone marrow mesenchymal stem cells infusion on
myocardial collagen network remodeling in a rat model of
doxorubicin-induced dilated cardiomyopathy. Mol Cell Biochem.
387:279–285. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Bai J, Gu R, Wang B, Zhang N, Kang L and
Xu B: Overexpression of integrin-linked kinase improves cardiac
function in a rat model of doxorubicin-induced chronic heart
failure. Zhonghua Xin Xue Guan Bing Za Zhi. 42:225–229. 2014.(In
Chinese). PubMed/NCBI
|
|
72
|
Lu XL, Tong YF, Liu Y, Xu YL, Yang H,
Zhang GY, Li XH and Zhang HG: Gαq protein carboxyl terminus
imitation polypeptide GCIP-27 improves cardiac function in chronic
heart failure rats. PLoS One. 10:e01210072015. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Wachtman LM, Browning MD, Bedja D, Pin S
and Gabrielson KL: Validation of the use of long-term indwelling
jugular catheters in a rat model of cardiotoxicity. J Am Assoc Lab
Anim Sci. 45:55–64. 2006.PubMed/NCBI
|
|
74
|
Zhang J, Zhang L, Wu Q, Liu H and Huang L:
Recombinant human brain natriuretic peptide therapy combined with
bone mesenchymal stem cell transplantation for treating heart
failure in rats. Mol Med Rep. 7:628–632. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Chen X, Chen Y, Bi Y, Fu N, Shan C, Wang
S, Aslam S, Wang PW and Xu J: Preventive cardioprotection of
erythropoietin against doxorubicin-induced cardiomyopathy.
Cardiovasc Drugs Ther. 21:367–374. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Ha JW, Kang SM, Pyun WB, Lee JY, Ahn MY,
Kang WC, Jeon TJ, Chung N, Lee JD and Cho SH: Serial assessment of
myocardial properties using cyclic variation of integrated
backscatter in an adriamycin-induced cardiomyopathy rat model.
Yonsei Med J. 46:73–77. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Emanuelov AK, Shainberg A, Chepurko Y,
Kaplan D, Sagie A, Porat E, Arad M and Hochhauser E: Adenosine A3
receptor-mediated cardioprotection against doxorubicin-induced
mitochondrial damage. Biochem Pharmacol. 79:180–187. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Lim SC: Interrelation between expression
of ADAM 10 and MMP 9 and synthesis of peroxynitrite in doxorubicin
induced cardiomyopathy. Biomol Ther (Seoul). 21:371–380. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Hydock DS, Lien CY, Schneider CM and
Hayward R: Exercise preconditioning protects against
doxorubicin-induced cardiac dysfunction. Med Sci Sports Exerc.
40:808–817. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Xiang P, Deng HY, Li K, Huang G-Y, Chen Y,
Tu L, Ng PC, Pong NH, Zhao H, Zhang L, et al: Dexrazoxane protects
against doxorubicin-induced cardiomyopathy: Upregulation of Akt and
Erk phosphorylation in a rat model. Cancer Chemother Pharmacol.
63:343–349. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Kenk M, Thackeray JT, Thorn SL, Dhami K,
Chow BJ, Ascah KJ, DaSilva JN and Beanlands RS: Alterations of pre-
and postsynaptic noradrenergic signaling in a rat model of
adriamycin-induced cardiotoxicity. J Nucl Cardiol. 17:254–263.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Katona M, Boros K, Sántha P, Ferdinandy P,
Dux M and Jancsó G: Selective sensory denervation by capsaicin
aggravates adriamycin-induced cardiomyopathy in rats. Naunyn
Schmiedebergs Arch Pharmacol. 370:436–443. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Hydock DS, Parry TL, Jensen BT, Lien CY,
Schneider CM and Hayward R: Effects of endurance training on
combined goserelin acetate and doxorubicin treatment-induced
cardiac dysfunction. Cancer Chemother Pharmacol. 68:685–692. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Hou XW, Son J, Wang Y, Ru YX, Lian Q,
Majiti W, Amazouzi A, Zhou YL, Wang PX and Han ZC: Granulocyte
colony-stimulating factor reduces cardiomyocyte apoptosis and
improves cardiac function in adriamycin-induced cardiomyopathy in
rats. Cardiovasc Drugs Ther. 20:85–91. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Hydock DS, Lien CY, Jensen BT, Schneider
CM and Hayward R: Exercise preconditioning provides long-term
protection against early chronic doxorubicin cardiotoxicity. Integr
Cancer Ther. 10:47–57. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Koh E, Nakamura T and Takahashi H:
Troponin-T and brain natriuretic peptide as predictors for
adriamycin-induced cardiomyopathy in rats. Circ J. 68:163–167.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Carresi C, Musolino V, Gliozzi M, Maiuolo
J, Mollace R, Nucera S, Maretta A, Sergi D, Muscoli S, Gratteri S,
et al: Anti-oxidant effect of bergamot polyphenolic fraction
counteracts doxorubicin-induced cardiomyopathy: Role of autophagy
and c-kitposCD45negCD31neg cardiac stem cell activation. J Mol Cell
Cardiol. 119:10–18. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Ma H, Kong J, Wang YL, Li JL, Hei NH, Cao
XR, Yang JJ, Yan WJ, Liang WJ, Dai HY, et al:
Angiotensin-converting enzyme 2 overexpression protects against
doxorubicin-induced cardiomyopathy by multiple mechanisms in rats.
Oncotarget. 8:24548–24563. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Zhang XJ, Cao XQ, Zhang CS and Zhao Z:
17β-estradiol protects against doxorubicin-induced cardiotoxicity
in male Sprague-Dawley rats by regulating NADPH oxidase and
apoptosis genes. Mol Med Rep. 15:2695–2702. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Sun XP, Wan LL, Yang QJ, Huo Y, Han YL and
Guo C: Scutellarin protects against doxorubicin-induced acute
cardiotoxicity and regulates its accumulation in the heart. Arch
Pharm Res. 40:875–883. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Zhu HJ, Han ZY, He SF, Jin S-Y, Xu S-J,
Fang X-D and Zhang Y: Specific MicroRNAs comparisons in hypoxia and
morphine preconditioning against hypoxia-reoxgenation injury with
and without heart failure. Life Sci. 170:82–92. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Croteau E, Tremblay S, Gascon S,
Dumulon-Perreault V, Labbé SM, Rousseau JA, Cunnane SC, Carpentier
AC, Bénard F and Lecomte R: [(11)C]-Acetoacetate PET imaging: A
potential early marker for cardiac heart failure. Nucl Med Biol.
41:863–870. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Ikegami E, Fukazawa R, Kanbe M, Watanabe
M, Abe M, Watanabe M, Kamisago M, Hajikano M, Katsube Y and Ogawa
S: Edaravone, a potent free radical scavenger, prevents
anthracycline-induced myocardial cell death. Circ J. 71:1815–1820.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Hiona A, Lee AS, Nagendran J, Xie X,
Connolly AJ, Robbins RC and Wu JC: Pretreatment with
angiotensin-converting enzyme inhibitor improves
doxorubicin-induced cardiomyopathy via preservation of
mitochondrial function. J Thorac Cardiovasc Surg. 142:396–403.e3.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Tang DX, Zhao HP, Pan CS, Liu YY, Wei XH,
Yang XY, Chen YY, Fan JY, et al: QiShenYiQi pills, a compound
Chinese medicine, ameliorates doxorubicin-induced myocardial
structure damage and cardiac dysfunction in rats. Evid Based
Complement Alternat Med: eCAM. 2013:4805972013. View Article : Google Scholar
|
|
96
|
Migrino RQ, Aggarwal D, Konorev E,
Brahmbhatt T, Bright M and Kalyanaraman B: Early detection of
doxorubicin cardiomyopathy using two-dimensional strain
echocardiography. Ultrasound Med Biol. 34:208–214. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Liu Y, Xu W, Xiong Y, Du G and Qin X:
Evaluations of the effect of HuangQi against heart failure based on
comprehensive echocardiography index and metabonomics.
Phytomedicine. 50:205–212. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Liu X, Gu X, Li Z, Li X, Li H, Chang J,
Chen P, Jin J, Xi B, Chen D, et al: Neuregulin-1/erbB-activation
improves cardiac function and survival in models of ischemic,
dilated, and viral cardiomyopathy. J Am Coll Cardiol. 48:1438–1447.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Cadeddu Dessalvi C, Pepe A, Penna C,
Gimelli A, Madonna R, Mele D, Monte I, Novo G, Nugara C, Zito C, et
al: Sex differences in anthracycline-induced cardiotoxicity: The
benefits of estrogens. Heart Fail Rev. 24:915–925. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Swain SM, Whaley FS and Ewer MS:
Congestive heart failure in patients treated with doxorubicin: A
retrospective analysis of three trials. Cancer. 97:2869–2879. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Blanter JB and Frishman WH: The preventive
role of angiotensin converting enzyme inhibitors/angiotensin-II
receptor blockers and β-adrenergic blockers in anthracycline- and
trastuzumab-induced cardiotoxicity. Cardiol Rev. 27:256–259. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Sharkey LC, Radin MJ, Heller L, Rogers LK,
Tobias A, Matise I, Wang Q, Apple FS and McCune SA: Differential
cardiotoxicity in response to chronic doxorubicin treatment in male
spontaneous hypertension-heart failure (SHHF), spontaneously
hypertensive (SHR), and Wistar Kyoto (WKY) rats. Toxicol Appl
Pharmacol. 273:47–57. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Georgiadis N, Tsarouhas K, Tsitsimpikou C,
Vardavas A, Rezaee R, Germanakis I, Tsatsakis A, Stagos D and
Kouretas D: Pesticides and cardiotoxicity. Where do we stand?
Toxicol Appl Pharmacol. 353:1–14. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Vasilaki F, Tsitsimpikou C, Tsarouhas K,
Germanakis I, Tzardi M, Kavvalakis M, Ozcagli E, Kouretas D and
Tsatsakis AM: Cardiotoxicity in rabbits after long-term nandrolone
decanoate administration. Toxicol Lett. 241:143–151. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Achar S, Rostamian A and Narayan SM:
Cardiac and metabolic effects of anabolic-androgenic steroid abuse
on lipids, blood pressure, left ventricular dimensions, and rhythm.
Am J Cardiol. 106:893–901. 2010. View Article : Google Scholar : PubMed/NCBI
|