The present study aimed to demonstrate commonality
between the contributing factors (CFs) to coronavirus disease 2019
(COVID-19) and gastrointestinal cancer (GIC), and to demonstrate
that the bases for these superficially different diseases have
important similarities. Much of the underlying motivation for the
present study has been previously presented (1,2) and
is thus not repeated herein.
The virus associated most closely with COVID-19
[severe acute respiratory syndrome (SARS)-coronavirus 2 (CoV-2)] is
transmissible. The occurrence of serious consequences from this
transmission is dependent on the health of the host's immune system
(3–5). In the model proposed by the authors,
these severe consequences of COVID-19 result from the effective
exploitation of a dysfunctional immune system by the SARS-CoV-2
virus. In this exploitive process, genetic disposition and
real-life exposures to multiple toxic stressors, as well as toxic
behaviors, lay the groundwork for immune system dysfunction.
Following SARS-CoV-2 exposure, the dysfunctional immune system is
unable to neutralize the SARS-CoV-2 virus, thereby allowing the
virus to enter and replicate in cells and trigger a chain of
events, ultimately leading to COVID-19 (3,4).
If immune system dysfunction is a/the major factor
in the severity of both infectious and chronic diseases, then a
necessary, although not necessarily sufficient, condition for
prevention and successful longstanding treatment is a reduction of
those factors that contribute to immune system dysfunction. The
virology-centric approach currently used for COVID-19 reflects
damage control for a dysfunctional immune system (e.g., quarantine,
face masks, vaccines, anti-viral treatments, etc.). A
toxicology-centric approach would be aimed at identifying and
removing the CFs to immune system dysfunctionality. Its evidentiary
basis would require going beyond current single-stressor laboratory
experiments to more comprehensive stressor combination experiments
(2,6).
It was hypothesized that the links between CFs to
COVID-19 and GIC are similar, based on independent observations of
chronic disease CFs and COVID-19 CFs. The present study aimed to
examine this hypothesis.
Myriad techniques were developed/exploited and
integrated for the present study, and are explained in detail in
the Data and methods section. Multiple findings resulted from this
approach, although two major demonstrations stand out.
First was the demonstration that a number of crucial
CFs common to GIC and COVID-19 exist. This provides evidence of the
unity of diseases (infectious and chronic) heretofore considered
and treated as separate entities, and is a step along the pathway
to a unified theory of disease.
Second was the demonstration that CFs indirectly
related to COVID-19 (the CF did not appear in the COVID-19 core
literature, but was located in a literature directly related to
COVID-19; e.g., hyperinflammation, hypercoagulation, hypoxia, etc.)
exhibited high promise of being validated eventually as directly
related to COVID-19 (the CF appeared in in the COVID-19 core
literature). Having the ability to identify promising CFs using
literature related directly to the target disease literature is the
mirror image of having the ability to identify promising treatments
for repurposing, and would be of substantial value to researchers,
research managers, research sponsors, and venture capitalists. It
would also serve as an early warning indicator and allow
precautionary preventive steps to be taken for a target disease of
interest before a CF had been confirmed as directly related to that
disease.
The first author and colleagues have been developing
protocols to prevent and reverse chronic diseases (7,8). The
central component of these unique protocols is the identification
and elimination of CFs to these chronic diseases. However, the
question arises of whether the aforementioned approach for
preventing and reversing chronic diseases can be applied
successfully for preventing and reversing communicable diseases
that exploit immune system dysfunction, such as COVID-19.
Over the past two decades, there have been at least
three major coronavirus-based infectious disease
outbreaks/epidemics/pandemics: SARS in 2002–2003; Middle East
respiratory syndrome (MERS), which commenced in 2012; and COVID-19,
which commenced in December, 2019. A comparative analysis of the
clinical and laboratory differences and similarities among
SARS-CoV, MERS-CoV and SARS-CoV-2 (presented in Table I) highlights two points: i) The
most common clinical symptoms (such as fever, cough, myalgia, etc.)
that were present have relatively similar extent in patients with
MERS and SARS-CoV-2; ii) in synchrony, laboratory findings
documented similar alterations of metabolic markers.
The literature data appear to underline various
immunological characteristics among SARS-CoV, MERS-CoV and
SARS-CoV-2 (9). Given the caveat
that the cytokine profile is extremely variable by depending on
numerous factors such as the phase of clinical course, disease
severity, and types of cytokines analyzed; inter alia, it is of
particular interest to mention that the cytokine profile has been
found to be practically unaltered in patients with MERS-CoV who
developed severe disease (10).
Indeed, as previously demonstrated, interferon (IFN)-γ, interleukin
(IL)-10, IL-12p70, IL-12/IL-23p40 and IL-17 were not detected in
the serum of any patients with MERS-CoV during the course of
disease. Only IFN-β, tumor necrosis factor (TNF)-α, transforming
growth factor (TGF)-β3 and IL-1α were detected in a few patients,
although they did not exhibit any significant association with the
clinical course or the severity of illness (10). Hence, these data may suggest a
dominant role of the disrupted cytokine profile, i.e., the
so-called cytokine storm, in determining the disease severity that
affects the SARS patients (11).
Finally, another crucial similarity among them is the demographic
affected most severely: The elderly population and others who have
comorbidities associated with dysfunctional immune systems
(1,3,12–16).
As regards, incidence and prevalence, GIC is a
relatively prevalent cancer. Worldwide, the GIC burden remains high
(19). In the USA, colorectal
cancer was the fourth leading cause of new cancer diagnoses in 2020
(20). Globally, colorectal cancer
also has the fourth highest incidence, with 1.9 million annual
diagnoses (19). Stomach cancer
was the 5th most common diagnosis, with 1.1 million cases (19). The incidence of esophageal cancer
was 604,000 (19).
The risk factors for the development of GIC may be
affected by genetic predisposition, geographic location, infection,
toxic exposures and other medical conditions or treatments
(21–24); however, several risk factors are
modifiable, including diet, physical activity, alcohol consumption
and smoking (25,26). As obesity has become increasingly
prevalent worldwide, increasing associations between obesity and
the risk of GICs have been identified (27). There are likely several mechanisms
involved, including alterations in endocrine signaling, a
relatively high fat and processed meat consumption coupled with a
low fiber intake that influences intestinal microbes and immune
response, and altered inflammatory cytokines from adipose tissue
(27,28).
In its broadest sense, toxicology is the study of
the impact that toxic stimuli and toxic behaviors, as well as their
combinations, can have on all members of the animal kingdom and
their environment. Its two most important components are
epidemiological-type studies to identify potential adverse effects
of candidate toxic stimuli and behaviors, and laboratory studies to
identify mechanisms that link the stimuli to their adverse effects.
Toxic stimuli exposures or toxic behaviors can range from acute to
chronic, and the doses can span a wide spectrum.
It is well documented that exposure to a wide
variety of stimuli, whether they are anthropogenic chemicals (e.g.,
xenobiotics) or lifestyle-related, etc., is associated with an
increased prevalence of chronic diseases. In some cases, the
underlying mechanism includes the dysfunction of the immune system.
Exposure to particulate matters, fossil fuel derivatives, metals,
ultraviolet (UV)-B or ionizing radiation, etc., may contribute to
immunodeficiency, which in turn may contribute to the development
of chronic diseases. This could critically elevate viral epidemic
or even pandemic events and prevalence, such as in the COVID-19
pandemic (3,29), or metabolic disorders (27). A further underlying mechanism may
involve metabolic disorders. Chronic inflammation may be promoted
by the exposure to stressors during a life course, such as
environmental toxicants, processed food (30), infectious agents, overfeeding, or
drugs. The improvement of the immune response and inflammatory
markers may lead to an improved physiological resilience to
disturbances by infectious agents, such as viruses and bacteria,
and may possibly lead to milder COVID-19 symptoms.
The robustness of the immune system appears to play
a pivotal role. It has even been suggested that it may affect
vaccine safety and efficiency (4).
Human host autoimmune pathologies may be triggered due to sequence
similarities between peptides, introduced by vaccines and human
proteins. The protective anti-SARS-CoV-2 antibody immune response
may result in a pathogenic autoimmune attack against a genetically
predisposed human vaccine recipient. Possible stimuli implicated in
the aforementioned mechanism include alcohol consumption, as well
as exposure to various toxic metals (31,32).
The functional improvement of the immune system to
maintain metabolic homeostasis may be achieved by administrating
specific dietary components, such as fibers and polyphenols, as
well as lifestyle changes (e.g., physical exercise), thus
maintaining metabolic homeostasis and preventing disease
development (33).
Similarly, serum zinc, copper and the metabolism of
other biometals, as well as serum metal levels and metal balance
and homeostasis, appear to play a crucial role in the mechanisms
that affect disease severity by interfering with COVID-19
pathogenesis; these may thus be exploited as COVID-19 severity
markers (34).
In previous studies, authors have demonstrated that
the onset and exacerbation of chronic (7) and infectious diseases (3) are greatly affected by toxic
modifiable CFs (with genetic factors having different levels of
influence). The present study demonstrates that there is strong
overlap between the CFs for GIC and COVID-19. Thus, while the
outward manifestations (symptoms) of the two diseases appear to
differ, some fundamental causes are similar. This may be the reason
that the majority of severe consequences of COVID-19 occur in those
patients with high comorbidities; the comorbidities and COVID-19
are two sides of the same coin.
Toxicological components constitute the bulk of
modifiable CFs responsible for GIC and COVID-19. In both cases, the
effects of these toxicological components on the immune system and
circulatory system appear to be major contributors to the symptoms
and outcomes observed, primarily through increases in inflammation
and oxidative stress. Examples of immune system dysfunction center
around the hyperinflammation/cytokine storm and severe allergic
reactions, while circulatory system dysfunction centers around
changes in i) serum properties, such as hypercoagulation; and ii)
cardiovascular markers, such as elevated troponin and D-dimer
levels. In GIC, the interactions between the immune system and the
microbiome (35–38) (Fig.
1) become critical due to the cancer localization in the
digestive tract.
Inflammatory factors and coagulation changes exhibit
similar clinical manifestations in COVID-19 and GIC. In
hospitalized patients with COVID-19, serum IL-6, IL-8, IL-1β and
TNF-α levels are an inflammatory cytokine signature linked to
coagulopathy and are predictive of COVID-19 severity and associated
survival (39,40). Mechanistically, alterations in this
inflammatory cytokine signature and the resulting inflammation and
tissue injury can function as inducers of increased signaling by
thrombin (proteinase-activated) and purinergic receptors, which
promote platelet activation and hypercoagulation events, thus
determining hypercoagulability (41). In particular, it should be
emphasized that increased levels of TNF-α represent a risk
determinant for venous thromboembolism (42).
Such a scheme of altered inflammatory factors
leading to coagulation disorders appears to be reflected in GIC. In
fact, alterations in the levels of IL-8, IL-10 and TNF-α may play
crucial roles in the development of gastric cancer (43); TNF-α/TNFR1 signaling promotes
gastric tumorigenesis (44); TNF-α
gene promoter polymorphisms are linked to a risk of developing
venous thromboembolism (45). In
essence, alterations in a selected cytokine profile and, in
particular, in the levels of TNF-α appear to be a main factor of
hyperinflammation and hypercoagulopathy in both COVID-19 and
GIC.
The toxicological components included in the present
study cover toxic lifestyles (diet, activity, sleep, substance
abuse, etc.), medical procedures (drugs, diagnostics, surgery,
non-drug therapies, etc.), bio-organisms (fungi, mold, parasites,
viruses, bacteria, etc.), environments, occupations, psychosocial
events and socioeconomic environments. The laboratory-based
evidence for the toxicity of the majority of toxic substances is
obtained through single-stressor laboratory experiments, which
under-represent real-world effects. The combinations of toxic
stimuli reflect real-world exposures, and the doses of substances
that can cause damage in combinations are lower than those that can
cause damage in single-stressor experiments of those substances.
Each of these factors plays a key role in such chronic exposure
paradigms, revealing the importance of required further toxic
evaluations in order to discover possible routes that would
eventually lead to a human risk.
The rapidly growing body of scientific evidence on
COVID-19 indicates that in order for a patient to exhibit serious
symptoms and side-effects, an underlying dysfunction of the immune
system is necessary. Various factors, including genetic
predisposition and exposure to toxic stimuli, aid the virus in
rendering the immune system vulnerable.
Literature-related discovery and innovation (LRDI).
LRDI has been previously described in detail (46–48),
and only the essential features relevant to the present study (the
discovery component of LRDI: LRD) will be summarized herein. LRD
and its subset literature-based discovery (LBD) link two or more
disparate literatures to produce discovery. In the medical world,
the main application of LRD has been to identify novel treatments
for disease (48,49), also known as treatment repurposing.
The LRD process uses pattern matching to link the disparate
literatures.
For example, a disease of interest may have
hyperinflammation, hypercoagulation and hypoxia as its main
characteristics. In that case, the non-disease of interest
literature would be searched for records that contain various
combinations of hyperinflammation, hypercoagulation and hypoxia. If
the purpose of the search is to identify novel treatments for the
disease of interest, then substances/behaviors (in the retrieved
records) that reduce hyperinflammation, hypercoagulation and
hypoxia would be viewed as candidate treatments for the disease of
interest. If the purpose of the search is to identify novel CFs for
the disease of interest, then substances/behaviors (in the
retrieved records) that increase hyperinflammation,
hypercoagulation and hypoxia would be viewed as candidate CFs for
the disease of interest.
The characteristics mentioned above can be specified
at a number of different hierarchical levels of detail. Consider
inflammatory bowel disease (IBD), which encompasses chronic
inflammatory GI disorders categorized most commonly as Crohn's
disease (CD) and ulcerative colitis (UC). IBD is described in more
detail in prior studies (2,48). A
previous IBD treatment repurposing study by the first author and
colleagues mainly used specific biomarkers and their desired
directions of value change (e.g., reduce IL-β AND/OR reduce IL-6
AND/OR reduce C reactive protein, etc.) as the pattern to identify
records that may contain novel IBD treatments (48).
The present study used three separate literatures to
identify CFs common to GIC and COVID-19 (see Appendix S1 for the
queries used to retrieve these three literatures). First was a
mature GIC core literature spanning 1990-early 2021, and it was
used to identify CFs that had a direct impact on GIC (i.e., the CF
was contained in a GIC core literature record(s). Second was a
predominately nascent COVID-19 literature (whose main component was
focused strictly on COVID-19 and was primarily ≤9 months old, and
whose very minor component included other coronaviruses), and it
was used to identify CFs that had a direct impact on COVID-19.
Third was a mature literature linked to, but not contained within,
the COVID-19 core literature. This linked literature was used to
identify CFs that had an indirect impact on COVID-19, and was
called the discovery literature. These latter CFs affected the
entities that linked this related literature to the COVID-19 core
literature. For example, if a key characteristic of the COVID-19
core literature is immune system dysfunction, and immune system
dysfunction is a link to this third literature, then a CF to immune
system dysfunction identified in the third literature, but not
contained in the COVID-19 core literature, has the potential to
impact COVID-19 indirectly through the immune system dysfunction
link from the non-COVID-19 literature to the COVID-19
literature.
Commonality was determined between i) CFs that
impacted GIC directly; and ii) CFs that impacted COVID-19 directly
and indirectly using a streamlined dot-product approach to identify
the CFs that impacted COVID-19 and GIC directly, and a
literature-related discovery approach to identify the CFs that
impacted COVID-19 indirectly. Modifiable CFs that contribute to
both GIC and COVID-19 were identified.
The COVID-19 core literature was viewed as
insufficient for the identification of the COVID-19 CFs due to its
nascency and immediacy. The main emphases of the COVID-19 core
literature titles are the following: i) Containing the pandemic;
ii) identifying the major abnormal biomarker values and symptoms of
patients hospitalized with COVID-19; iii) repurposing and testing
treatments; iv) developing and testing vaccines; v) assessing the
effects of the pandemic on behaviors, medical treatments and
procedures; and vi) reviews of treatments, vaccines, restrictions,
etc. In brief, the COVID-19 core literature as of early March,
2021, was mainly focused on disease/viral containment rather than
prevention.
As of March, 2021, there has been insufficient time
to conduct the lengthy laboratory experiments relating CFs to
COVID-19 or to conduct the longer-term epidemiological studies
required to reveal these associations. Therefore, a more mature
intermediate literature that shares commonalities with important
aspects of the COVID-19 core literature, and includes the
longer-term studies that can demonstrate links of immune system
dysfunction consequences to CFs, is required. While the results of
the present study demonstrate a substantial number of GIC and
COVID-19 direct impact CFs that overlapped, it was considered that
far more overlaps between GIC and COVID-19 were possible using the
discovery approach. This was the purpose of the third (discovery)
literature that was generated.
There were three general themes of articles
retrieved from the third (discovery) literature associated with
potential CFs for impacting COVID-19 indirectly, although not every
third literature article retrieved reflected each theme (some
articles reflected only one of the themes; some reflected two, and
some reflected all three). The first was increasing vulnerability
to infectious disease; the second was exacerbating the seriousness
of an existing infectious disease; the third was adversely
impacting biomarkers that reflected coagulation, hypoxia, etc., as
well as biomarkers that reflected immune system dysfunction. All
else being equal, the prioritization of the selection of the
potential discovery CFs for inclusion in the present study followed
the order above.
There is no guarantee that a CF that produces any
one of the three adverse effects listed above, or all three
simultaneously, will have the same adverse impact for COVID-19. The
reasoning for selection is that if the CF had this adverse effect,
or a combination of adverse effects, for another infectious
disease, there is greater likelihood that it could have a similar
effect on COVID-19, all else being equal. The potential COVID-19
adverse effect(s) need(s) to be demonstrated in an
experiment/clinical trial.
In 2014, the first author published a study
demonstrating theme commonalities between Parkinson's disease (PD;
neurodegenerative) and CD (autoimmune) using phrase matching and
bibliographic coupling (shared references) between the two disease
literatures (50). Due to the
strong emphasis on shared references, the commonality of PD and CD
at a more fundamental mechanism level was demonstrated. Combining
these two approaches for identifying commonality (CF commonality
and bibliographic coupling/phrase matching) could provide deeper
understanding at different levels of commonality between GIC and
COVID-19.
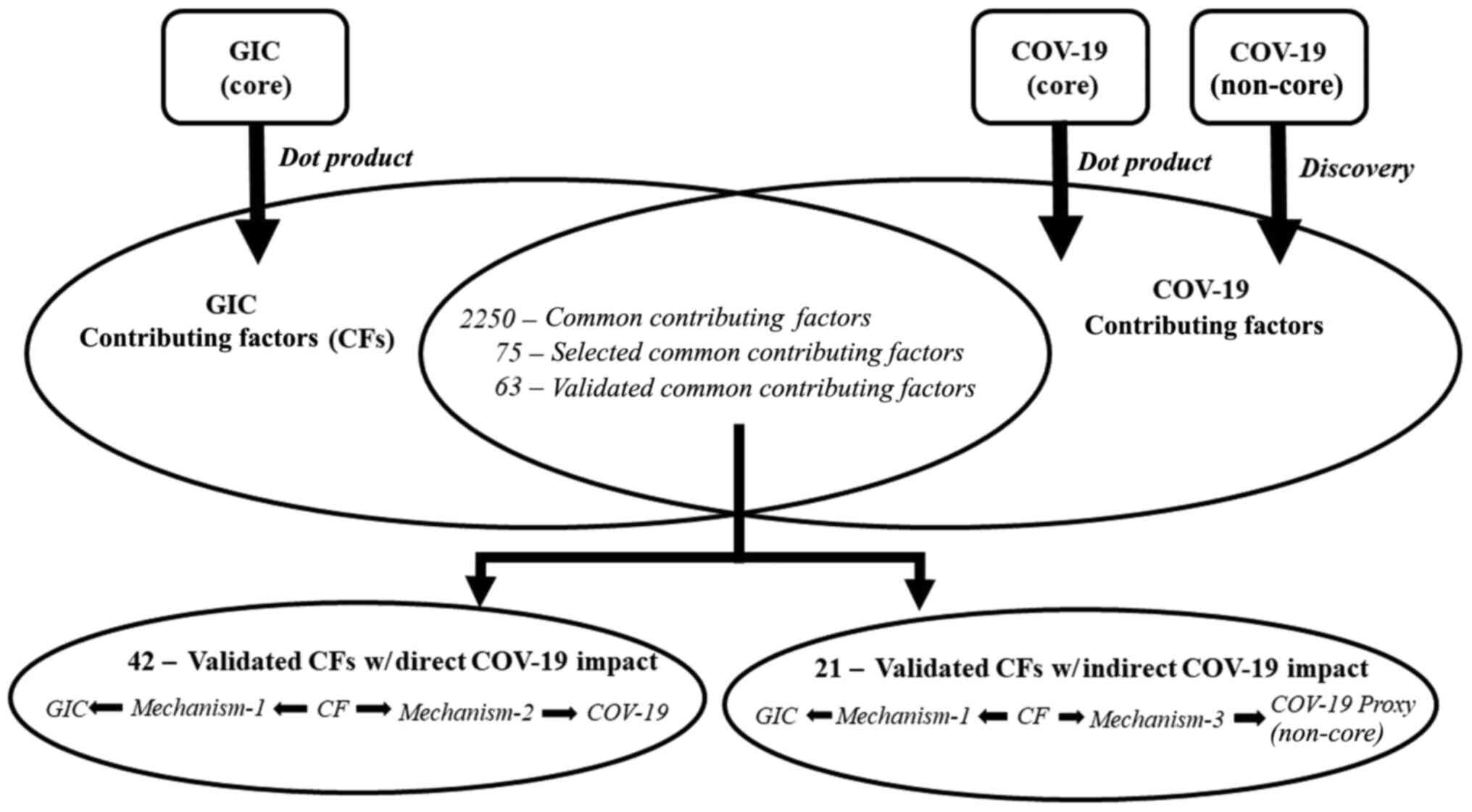
The streamlined method used to identify common CFs
that impact GIC and COVID-19 directly (these are CFs that are found
in the core literatures for GIC and COVID-19) for the present study
is termed a dot-product approach (1,2).
Lists of known toxic substances were aggregated from myriad
(mainly) government agencies, and combined with lists of CFs
identified in our previous disease studies (7,8).
This combination produced a final list of >13,000 CFs
potentially impacting disease. While this is certainly a large
number of potential CFs, it undoubtedly omits additional CFs that a
well-resourced study could have identified.
A core literature query was defined for GIC, applied
to PubMed, and the resultant retrieval (~275,000 records with
abstracts, covering the period between 1990-early 2021) was
imported into VantagePoint (VP) text analysis software (www.theVantagePoint.com; V12 Pro/64). This GIC
core literature query is shown in Appendix S1. The title and
abstract phrases of the retrieved records were parsed in VP,
resulting in lists of numerous phrases. The same procedure was
followed for the COVID-19 core literature (~88,000 records with
abstracts, covering the period between 1990-early 2021); the
COVID-19 core literature query is also shown in Appendix S1.
The external list of >13,000 phrases of potential
CFs was intersected with the parsed list of abstract phrases in the
GIC and COVID-19 core literatures to generate the subset of the
13,000+ phrases relevant to each core literature. There were ~4,400
candidate CFs that impacted GIC directly, and ~2,800 candidate CFs
(candidate means they are potential CFs, but need to be validated
as actual CFs) that impacted COVID-19 directly. These two
intersected lists of direct impact CFs were compared, and the
candidate direct impact CFs in common between GIC and COVID-19 were
identified. Approximately 2,250 candidate direct impact CFs in
common were identified, albeit some being variants of the same
concept. However, this is a very conservative estimate of candidate
direct impact CFs in common, for the reasons shown in Appendix
S2.
The dot-product approach described above produced
CFs that impacted GIC and COVID-19 directly (using articles
contained in the core literatures only). However, as the numbers
above indicate, there were ~2,150 CFs that impacted GIC directly,
but did not impact COVID-19 directly. The myriad reasons for CF
underestimation summarized in Appendix S2 could explain this
observation, particularly given the nascency of the majority of the
COVID-19 core literature relative to the time required to
demonstrate CF-disease linkages in laboratory experiments. This led
to the decision to include an approach for identifying CFs that
impacted COVID-19 indirectly.
One method for identifying indirect impacts of CFs
on a given disease is with use of the discovery component of LRDI.
This has been used successfully to generate CF discovery in chronic
kidney disease (CKD) (8) and
Alzheimer's disease (AD) (7). It
has also been used to generate treatment discovery (treatment
repurposing) for CKD (8) and AD
(7), as well as for IBD (34). A variant of this discovery approach
was developed for the present study.
In previous studies, patterns of biomarkers,
symptoms, etc., in a disease core literature that were associated
with that disease were extracted and applied to the larger
non-disease literature to identify substances and behaviors that
produced these patterns (7,8) (as
described in the Introduction). Following the analyses of the
retrievals, a number of these substances and behaviors were
classified as potential CFs to the disease of interest, and needed
to be validated through experiments and/or epidemiological studies.
There were no constraints placed on the substances and
behaviors.
The present study aimed to select, from the ~2,150
substances and behaviors, CFs impacting GIC directly and not
impacting COVID-19 directly. The study also aimed to ascertain
whether evidence existed in the non-COVID-19 literature to validate
that at least some of the substances selected could be viewed as
candidate CFs for indirect impact of COVID-19 (CF discovery, or CF
repurposing, analogous to treatment repurposing). The present study
used a modified version of recent discovery queries previously
demonstrated (49) that required
retrievals to contain the CF under consideration (this modified
version of the discovery query is shown in Appendix S1). For
purposes of completeness, this approach was eventually applied to
all the CFs selected for display purposes, and the results are
presented in Table II.
The phrases in common between GIC and COVID-19
should be viewed as candidate CFs, which must be validated as
actual CFs by detailed analysis. There was also the question of how
many validated CFs are required to support the hypothesis of common
causation between the two diseases. There are two main criteria to
be considered in making the selection. The first criterion is the
numbers of CFs in common. The second criterion is the importance of
the CFs in contributing to the disease.
In the case that the system operation is determined
mainly by a few significant factors, as in a number of large and
complex systems, then a handful of such significant factors is all
that would be required to support the hypothesis. If no such
significant factors stand out, then further CFs would be required
to support the hypothesis of common cause.
For GIC and COVID-19, there were significant factors
that stood out, and these were the foundation of the validation
selection process. A balance/trade-off between the two major
selection criteria resulted in the selection of 63 common phrases
between GIC and COVID-19 to be validated as CFs. These 63 phrases
included those deemed most significant and spanning the
five-category taxonomy we have developed for classifying modifiable
CFs to disease: Lifestyle, iatrogenic, biotoxins,
occupational/environmental, psychosocial/socioeconomic (7). Genetics was not included, since the
CFs in the current definition were viewed as modifiable, indicating
that they were relatively controllable.
Given the shortcomings of the COVID-19 core
literature from the perspective of insufficient causation studies
(as described above), the present study also included CFs that
impacted COVID-19 indirectly. This would also demonstrate the novel
CF discovery technique developed for the present study. In total 21
of the 63 candidate CFs were selected as indirect impact CFs and
validated as proof of concept. A schematic diagram of the study
protocol and approach used is presented in Fig. 2.
The 63 GIC direct impact CFs in common with the
COVID-19 direct and indirect impact CFs selected for validation are
presented in Table II. The
detailed record excerpts demonstrating the links between the CFs
and disease are presented in Appendix S3.
The results of the present study conclusively
demonstrate the wide range of CFs in common between GIC and
COVID-19. The next section addresses some of the numerous
mechanisms considered responsible for these links, followed by a
section that demonstrates how these common CF results provide the
basis for a unified theory of infectious and chronic disease.
The operational implication of the results is that
strengthening the immune system against both infectious and
autoimmune diseases requires the discipline to i) remove exposure
to a broad range of toxic substances; and ii) eliminate toxic
behaviors.
It would be of interest to determine some of the
mechanisms that link CFs identified in the present study with GIC
and COVID-19. The following brief analysis examines the role of
advanced glycation end products (AGEs), high-fat diets (HFDs),
cooked red meat, excessive alcohol consumption and a sedentary
lifestyle in contributing to, and/or exacerbating, GIC.
A dietary context appears to contribute to and
sustain the global burden of GICs (51). Among the CFs, a main role is played
by AGEs that can activate the NLR family pyrin domain containing 3
(NLRP3) inflammasome (52). This
not only determines the colonic inflammation environment for
carcinogenesis (53), but also
impairs innate immune response in macrophages (35), thereby contributing to the tumor
escape from innate immunosurveillance (54,55).
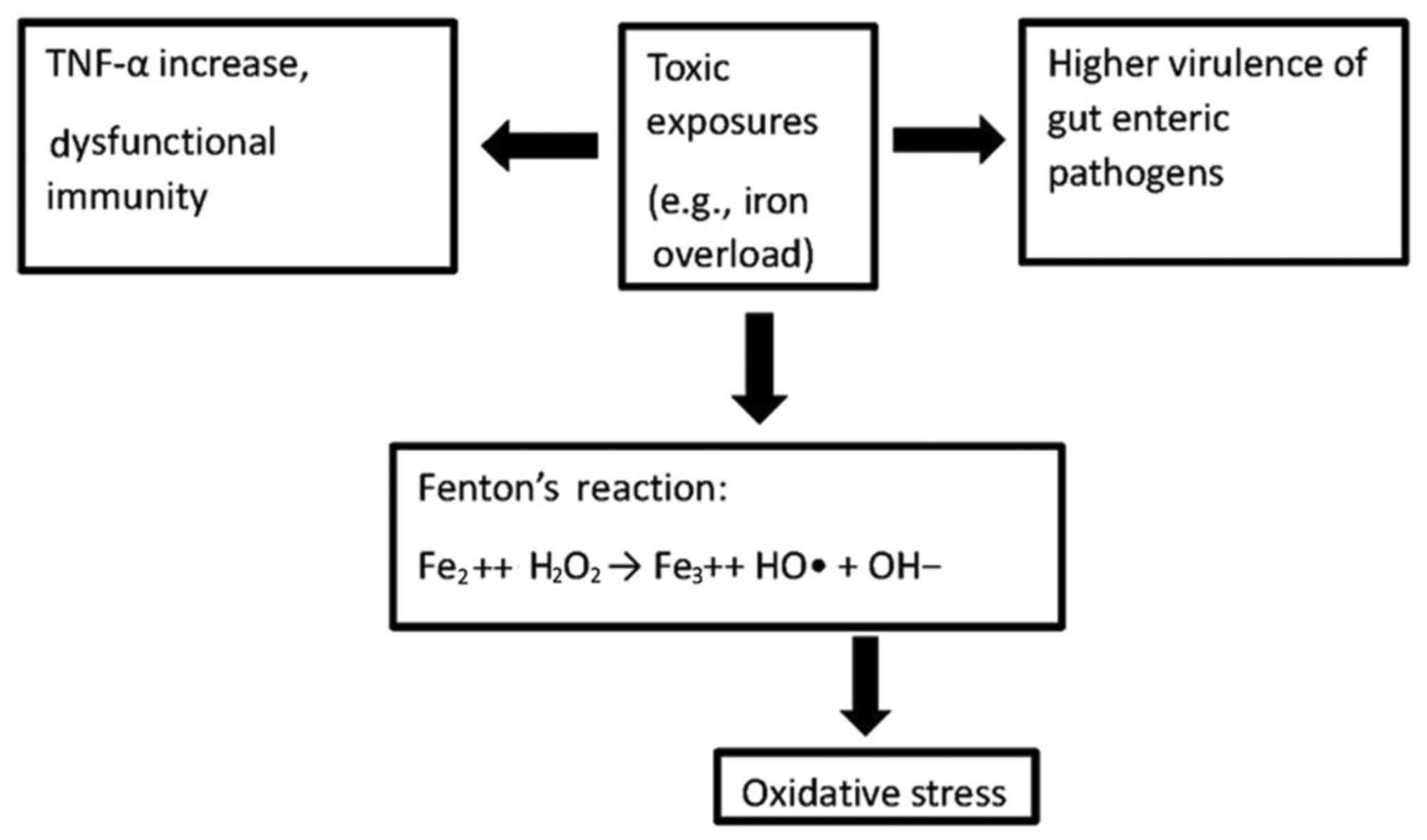
Another crucial dietary CF in GI carcinogenesis is
represented by the consumption of high amounts of cooked red meat.
Indeed, consuming red meat equates to introducing hemoglobin and
its degradation products, heme and iron, in non-hematopoietic
tissues (63). Iron can generate
severe oxidative stress via the Fenton reaction, thus causing
severe inflammatory pathologies and eventually leading to cancer
(63–65). Moreover, the iron load is a crucial
factor in colorectal carcinogenesis as it can trigger the
macrophage expression of TNF-α-converting enzyme (TACE; also known
as ADAM17) (66,67). The tolerable iron upper intake
level (UL) for adults is 45 mg/day of iron, a level based on
gastrointestinal distress as an adverse effect. The median dietary
intake of iron is ~16–18 mg/day for males and 12 mg/day for females
(https://www.ncbi.nlm.nih.gov/books/NBK222309/).
TACE is a sheddase (membrane-bound enzyme) that cuts
and sheds the membrane-bound precursor of TNF-α to its mature
soluble form (68). In other
words, a cytokine storm is unleashed, given that TNF-α is the
master regulator of inflammatory cytokine production (69).
Such a sequence of potent inflammatory events can be
further enhanced by alcohol consumption. In fact, the iron-induced
oxidative stress and inflammation are potentiated by excessive
alcohol abuse that results in further dysregulated iron homeostasis
at the hepatic level and heightened TACE induction and activity
(66).
In this pathological scenario dominated by
inflammation and oxidative stress, a sedentary lifestyle also plays
a role. Indeed, sedentary behavior relates to chronic inflammation
and colorectal cancer development, while physical activity plays a
protective role (70,71). The molecular basis of the
protection exerted by physical activity appears to reside in a
transcriptional factor, the peroxisome proliferator-activated
receptor γ co-activator 1α (PGC-1α), the level of which is enhanced
by physical activity (72). In
fact, PGC-1α regulates proteins involved in the antioxidant defense
and lowers the expression of inflammatory markers (73).
On the whole, these five CFs, namely AGEs, HFDs, red
meat, alcohol consumption and sedentary behavior, suffice to
explain much of the 2018 epidemiological data reporting an
estimated 4.8 million new cases of GICs and 3.4 million related
deaths worldwide, with GI cancers accounting for 26% of the global
cancer incidence and 35% of all cancer-related deaths (51).
The present study is the third one by the first
author and colleagues examining the CFs common to COVID-19 and a
chronic disease (1,2). As time has proceeded, and the
COVID-19 core literature has increased in size, other CFs linked to
COVID-19 have emerged and commonality of CFs to chronic disease has
increased. This trend is expected to continue.
All three studies have demonstrated the existence of
numerous potential CFs common to the two types of disease, and at
least 50 common CFs have been validated in each study. Many of the
common infectious disease-chronic disease CFs are also common among
the three studies. For the CFs that have been validated, myriad
common factors include lifestyle (e.g., dietary content, vitamin
and mineral deficiencies, food processing and preparation,
exercise, sleep, substance abuse, etc.), occupational/environmental
(air pollution, water pollution, heavy metals, agrochemicals,
occupational chemicals, ionizing and non-ionizing radiations,
etc.), and psychosocial/socioeconomic (myriad forms of stress,
adverse childhood experiences, isolation, low income, etc.)
factors. Iatrogenic factors are mixed; substances/radiations that
are beneficial for treating one disease may exacerbate other
diseases. Biotoxins are mixed as well, particularly since some
viruses associated with disease enhancement are also used as
vectors for drug/treatment delivery.
In the case that the majority of the important CFs
to COVID-19 are important CFs to the associated chronic diseases
examined, as increasingly appears to be the case with the growth of
the COVID-19 literature, the question remains of what could be
concluded about the similarity of these infectious and chronic
diseases.
One important conclusion is that for the prevention
of either type of disease, the CFs identified and validated must be
eliminated/reduced as broadly, deeply, and rapidly as possible.
A second important conclusion is that, if it is
assumed that the symptoms characteristic of either disease
represent the host's response to the CFs, the same fundamental
disease can have myriad manifestations exhibited through the
symptoms. Thus, treating the host's manifestation of the disease
(symptoms) is different from treating the disease. The
manifestations can be suppressed, but the disease perseveres. Only
elimination of the CFs, as outlined in the previous paragraph, has
the potential to eliminate the disease (and its associated damages)
at its core (assuming that the damages resulting from the disease
are not irreversible and the host does not have a strong genetic
predisposition to the disease).
There may be treatments for COVID-19 and GIC that
overlap; however, there may also be treatments that are
antagonistic. As demonstrated in prior sections and the biomedical
literature (39–45), inflammatory and coagulation factors
exhibit clinical manifestations in both COVID-19 and GIC.
Treatments that reduce inflammation and coagulation should be
beneficial to both diseases, and could possibly overlap.
Conversely, immunosuppressants (used in myriad cancer treatments)
tend to increase vulnerability to infectious diseases. In general,
if the removal of a potential cause is defined as one type of
treatment, then one potential class of overlapping treatments will
be the removal of the CFs in common between GIC and COVID-19.
The third conclusion relates to the different
external manifestations of disease, even though the CFs have a
strong commonality. In the case of the existence of a high
commonality between the CFs to GIC and COVID-19, the question would
arise as to why one group of individuals manifests COVID-19
symptoms and another group manifests GIC symptoms (although in
actuality the vast majority of individuals experiencing the most
severe forms of COVID-19 are those with multiple chronic disease
comorbidities, exhibiting symptoms of both types of diseases).
There are at least two explanations for this.
Individuals have different genetic structures and different
predispositions (particularly as regards responses to CFs), and
their external manifestations would be expected to differ. Second,
CFs have temporal and dosage components (among others), so the CF
‘signature’ of each individual differs, even following exposure to
the same type of CF. As a simple example, one individual who smokes
may develop lung cancer, another may develop CD, another may
develop myocardial infarction, another may develop COVID-19 and
another may remain healthy. In real-life, individuals are exposed
to myriad combinations of CFs. Depending on the complex structure
of temporal and dosage components of each CF and the nature of
interactions among CFs, different external manifestations of the
exposure combinations would be expected.
It may be possible that the analysis and treatment
of these infectious and chronic diseases have been performed using
the wrong ‘coordinate system’. These diseases have been viewed from
the perspective of their external manifestations (symptoms) rather
than the perspective of their CFs. When ‘coordinates’ are switched
from symptoms to CFs, and focus is placed on treatments and
preventative measures to alter the CFs rather than the symptoms, a
unified approach for resolving the dichotomy between these two
types of diseases and, most importantly, eliminating their
prevalence, may be presented. Obviously, in the case that symptoms
become life-threatening or may result in permanent damage,
short-term tactical treatments are required; however, for the
intermediate or long-term, preventive measures are necessary.
The findings of the present study suggest a need for
a paradigmatic shift in medical approaches to disease. The current
approach to both infectious and chronic disease in Western medicine
is often external-treatment-based (i.e., providing a drug, vaccine,
radiation, surgery, etc.) to reduce symptoms without sufficiently
addressing the underlying modifiable factors that enabled the
disease to emerge. The present study highlights modifiable factors
(toxic exposures and behaviors) that contribute to disease
pathogenesis via various mechanisms of immune dysfunction, and
demonstrates CF commonality between GIC and COVID-19. Eliminating
these factors as comprehensively and rapidly as possible is
prudent, and perhaps should be pursued in parallel with
treatment.
Not applicable.
No funding was received.
All data generated or analyzed during this study are
included in this published article and in the supplementary
material.
RNK contributed to the conception of the study, as
well as in data analysis and in the writing of the manuscript. MBB
participated in data analysis, validation of the results, and in
the preparation of the tables. DK participated in data analysis and
in the writing of the manuscript. DRS contributed to query
development, background development, and in the writing and editing
of the manuscript. LK contributed to data analysis, as well as in
the study design, and in the writing, and editing of the
manuscript. ALP contributed to the conception and design of the
study, as well as in the writing and editing of the manuscript. ND
contributed to the design of the study, as well as in the drafting,
writing and editing of the manuscript. AT contributed to the
critical revision of the study, as well as in the design, drafting
writing, and editing of the manuscript. DAS contributed to the
design of the study, as well as in the revision, writing and
editing of the manuscript. RNK and MBB confirm the authenticity of
all the raw data. All the authors have read and approved the final
version of the manuscript.
Not applicable.
Not applicable.
DAS is the Editor-in-Chief for the journal, but had
no personal involvement in the reviewing process, or any influence
in terms of adjudicating on the final decision, for this article.
The other authors declare that they have no competing
interests.
|
1
|
Kostoff RN, Briggs MB, Kanduc D, Porter AL
and Buchtel HA: Communicable Diseases are not Communicable! Georgia
Institute of Technology. 2020. https://smartech.gatech.edu/handle/1853/63805
|
|
2
|
Kostoff RN, Briggs MB, Kanduc D, Shores
DR, Kovatsi L, Vardavas AI and Porter AL: Common contributing
factors to COVID-19 and inflammatory bowel disease. Toxicol Rep.
8:1616–1637. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kostoff RN, Briggs MB, Porter AL,
Hernandez AF, Abdollahi M, Aschner M and Tsatsakis A: The
under-reported role of toxic substance exposures in the COVID-19
pandemic. Food Chem Toxicol. 145:1116872020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kostoff RN, Kanduc D, Porter AL, Shoenfeld
Y, Calina D, Briggs MB, Spandidos DA and Tsatsakis A: Vaccine- and
natural infection-induced mechanisms that could modulate vaccine
safety. Toxicol Rep. 7:1448–1458. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gorji A and Khaleghi Ghadiri M: Potential
roles of micronutrient deficiency and immune system dysfunction in
the coronavirus disease 2019 (COVID-19) pandemic. Nutrition.
82:1110472021. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kostoff RN, Goumenou M and Tsatsakis A:
The role of toxic stimuli combinations in determining safe exposure
limits. Toxicol Rep. 5:1169–1172. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kostoff RN, Porter AL and Buchtel HA:
Prevention and reversal of Alzheimer's disease: treatment protocol.
Georgia Institute of Technology. 2018. https://smartech.gatech.edu/handle/1853/59311
|
|
8
|
Kostoff RN and Patel U: Literature-related
discovery and innovation: Chronic kidney disease. Technol Forecast
Soc Change. 91:341–351. 2015. View Article : Google Scholar
|
|
9
|
Liu J, Xie W, Wang Y, Xiong Y, Chen S, Han
J and Wu Q: A comparative overview of COVID-19, MERS and SARS:
Review article. Int J Surg. 81:1–8. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zhang YY, Li BR and Ning BT: The
Comparative Immunological Characteristics of SARS-CoV, MERS-CoV,
and SARS-CoV-2 Coronavirus Infections. Front Immunol. 11:20332020.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kim ES, Choe PG, Park WB, Oh HS, Kim EJ,
Nam EY, Na SH, Kim M, Song KH, Bang JH, et al: Clinical Progression
and Cytokine Profiles of Middle East Respiratory Syndrome
Coronavirus Infection. J Korean Med Sci. 31:1717–1725. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Qin C, Zhou L, Hu Z, Zhang S, Yang S, Tao
Y, Xie C, Ma K, Shang K, Wang W and Tian D-S: Dysregulation of
Immune Response in Patients With Coronavirus 2019 (COVID-19) in
Wuhan, China. Clin Infecti Dis. 71:762–768. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu
Y, Zhang L, Fan G, Xu J, Gu X, et al: Clinical features of patients
infected with 2019 novel coronavirus in Wuhan, China. Lancet.
395:497–506. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Liu Y, Yang Y, Zhang C, Huang F, Wang F,
Yuan J, Wang Z, Li J, Li J, Feng C, et al: Clinical and biochemical
indexes from 2019-nCoV infected patients linked to viral loads and
lung injury. Sci China Life Sci. 63:364–374. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Mo P, Xing Y, Xiao Y, Deng L, Zhao Q, Wang
H, Xiong Y, Cheng Z, Gao S, Liang K, et al: Clinical
characteristics of refractory COVID-19 pneumonia in Wuhan, China.
Clin Infect Dis. ciaa2702020. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Qian GQ, Yang NB, Ding F, Ma AHY, Wang ZY,
Shen YF, Shi CW, Lian X, Chu JG, Chen L, et al: Epidemiologic and
clinical characteristics of 91 hospitalized patients with COVID-19
in Zhejiang, China: a retrospective, multi-centre case series.
QJM-Int J Med. 113:474–481. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
NaturePortfolio Gastrointestinal cancer, .
https://www.nature.com/subjects/gastrointestinal-cancerMarch
21–2021
|
|
18
|
National Institutes of Health, .
Gastrointestinal Neoplasms. https://www.ncbi.nlm.nih.gov/mesh/?term=GASTROINTESTINAL+NEOPLASMS)March
24–2021
|
|
19
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global Cancer Statistics 2020:
GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36
Cancers in 185 Countries. CA Cancer J Clin. 71:209–249. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Cancer Stat Facts: Colorectal Cancer:
National Cancer Institute Surveillance, Epidemoiology, and End
Results Program. https://seer.cancer.gov/statfacts/html/common.htmlMarch
3–2021
|
|
21
|
Yusefi AR, Bagheri Lankarani K, Bastani P,
Radinmanesh M and Kavosi Z: Risk Factors for Gastric Cancer: A
Systematic Review. Asian Pac J Cancer Prev. 19:591–603.
2018.PubMed/NCBI
|
|
22
|
Poorolajal J, Moradi L, Mohammadi Y,
Cheraghi Z and Gohari-Ensaf F: Risk factors for stomach cancer: A
systematic review and meta-analysis. Epidemiol Health.
42:e20200042020. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Castro C, Peleteiro B and Lunet N:
Modifiable factors and esophageal cancer: Asystematic review of
published meta-analyses. J Gastroenterol. 53:37–51. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lichtenstern CR, Ngu RK, Shalapour S and
Karin M: Immunotherapy, Inflammation and Colorectal Cancer. Cells.
9:6182020. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Marmol I, Sanchez-de-Diego C, Pradilla
Dieste A, Cerrada E and Rodriguez Yoldi MJ: Colorectal Carcinoma: A
General Overview and Future Perspectives in Colorectal Cancer. Int
J Mol Sci. 18:19720017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
World Cancer Research Fund/American
Institute for Cancer Research, . Diet, Nutrition, Physical Activity
and Cancer: A Global Perspective. Continuous Update Project Expert
Report 2018. www.dietandcancerreport.org.
|
|
27
|
Murphy N, Jenab M and Gunter MJ: Adiposity
and gastrointestinal cancers: Epidemiology, mechanisms and future
directions. Nat Rev Gastroenterol Hepatol. 15:659–670. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zhou E and Rifkin S: Colorectal Cancer and
Diet: Risk Versus Prevention, Is Diet an Intervention?
Gastroenterol Clin North Am. 50:101–111. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Tsatsakis A, Petrakis D, Nikolouzakis TK,
Docea AO, Calina D, Vinceti M, Goumenou M, Kostoff RN, Mamoulakis
C, Aschner M and Hernández AF: COVID-19, an opportunity to
reevaluate the correlation between long-term effects of
anthropogenic pollutants on viral epidemic/pandemic events and
prevalence. Food Chem Toxicol. 141:1114182020. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Margină D, Ungurianu A, Purdel C,
Tsoukalas D, Sarandi E, Thanasoula M, Tekos F, Mesnage R, Kouretas
D and Tsatsakis A: Chronic Inflammation in the Context of Everyday
Life: Dietary Changes as Mitigating Factors. Int J Environ Res
Public Health. 17:41352020. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Calina D, Hartung T, Mardare I, Mitroi M,
Poulas K, Tsatsakis A, Rogoveanu I and Docea AO: COVID-19 pandemic
and alcohol consumption: Impacts and interconnections. Toxicol Rep.
8:529–535. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Skalny AV, Lima TRR, Ke T, Zhou JC,
Bornhorst J, Alekseenko SI, Aaseth J, Anesti O, Sarigiannis DA,
Tsatsakis A, et al: Toxic metal exposure as a possible risk factor
for COVID-19 and other respiratory infectious diseases. Food Chem
Toxicol. 146:1118092020. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Margină D, Ungurianu A, Purdel C,
Nițulescu GM, Tsoukalas D, Sarandi E, Thanasoula M, Burykina TI,
Tekos F, Buha A, et al: Analysis of the intricate effects of
polyunsaturated fatty acids and polyphenols on inflammatory
pathways in health and disease. Food Chem Toxicol. 143:1115582020.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Skalny AV, Timashev PS, Aschner M, Aaseth
J, Chernova LN, Belyaev VE, Grabeklis AR, Notova SV, Lobinski R,
Tsatsakis A, et al: Serum Zinc, Copper, and Other Biometals Are
Associated with COVID-19 Severity Markers. Metabolites. 11:2442021.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Lee JK, Shin JH, Gwag BJ and Choi EJ: Iron
accumulation promotes TACE-mediated TNF-α secretion and
neurodegeneration in a mouse model of ALS. Neurobiol Dis. 80:63–69.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Menghini R, Fiorentino L, Casagrande V,
Lauro R and Federici M: The role of ADAM17 in metabolic
inflammation. Atherosclerosis. 228:12–17. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Winterbourn CC: Toxicity of iron and
hydrogen peroxide: The Fenton reaction. Toxicol Lett 82–83.
969–974. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Yilmaz B and Li H: Gut Microbiota and
Iron: The Crucial Actors in Health and Disease. Pharmaceuticals
(Basel). 11:982018. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Del Valle DM, Kim-Schulze S, Huang HH,
Beckmann ND, Nirenberg S, Wang B, Lavin Y, Swartz TH, Madduri D,
Stock A, et al: An inflammatory cytokine signature predicts
COVID-19 severity and survival. Nat Med. 26:1636–1643. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Rad F, Dabbagh A, Dorgalaleh A and Biswas
A: The Relationship between Inflammatory Cytokines and Coagulopathy
in Patients with COVID-19. J Clin Med. 10:20202021. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Sriram K and Insel PA: Inflammation and
thrombosis in COVID-19 pathophysiology: Proteinase-activated and
purinergic receptors as drivers and candidate therapeutic targets.
Physiol Rev. 101:545–567. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Reitsma PH and Rosendaal FR: Activation of
innate immunity in patients with venous thrombosis: The Leiden
Thrombophilia Study. J Thromb Haemost. 2:619–622. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Lu W, Pan K, Zhang L, Lin D, Miao X and
You W: Genetic polymorphisms of interleukin (IL)-1B, IL-1RN, IL-8,
IL-10 and tumor necrosis factor {alpha} and risk of gastric cancer
in a Chinese population. Carcinogenesis. 26:631–636. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Oshima H, Ishikawa T, Yoshida GJ, Naoi K,
Maeda Y, Naka K, Ju X, Yamada Y, Minamoto T, Mukaida N, et al:
TNF-α/TNFR1 signaling promotes gastric tumorigenesis through
induction of Noxo1 and Gna14 in tumor cells. Oncogene.
33:3820–3829. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Roselli M, Ferroni P, Rolfo C, Peeters M,
Palmirotta R, Formica V, Ludovici G, Laudisi A, De Marchis ML, La
Farina F, et al: TNF-α gene promoter polymorphisms and risk of
venous thromboembolism in gastrointestinal cancer patients
undergoing chemotherapy. Ann Oncol. 24:2571–2575. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Kostoff RN, Block JA, Solka JL, Briggs MB,
Rushenberg RL, Stump JA, Johnson D, Lyons TJ and Wyatt JR:
Literature-Related Discovery. Annu Rev Inf Sci Technol. 43:241–285.
2009. View Article : Google Scholar
|
|
47
|
Kostoff RN: Literature-related discovery
and innovation - update. Technol Forecast Soc Change. 79:789–800.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Kostoff RN, Briggs MB and Shores DR:
Treatment repurposing for inflammatory bowel disease using
literature-related discovery and innovation. World J Gastroenterol.
26:4889–4899. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Kostoff RN: Treatment Repurposing using
Literature-related Discovery. J Scientometr Res. 8:S74–S84. 2019.
View Article : Google Scholar
|
|
50
|
Kostoff RN: Literature-related discovery:
common factors for Parkinson's Disease and Crohn's Disease.
Scientometrics. 100:623–657. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Arnold M, Abnet CC, Neale RE, Vignat J,
Giovannucci EL, McGlynn KA and Bray F: Global Burden of 5 Major
Types of Gastrointestinal Cancer. Gastroenterology. 159:335–349.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Kong X, Lu AL, Yao XM, Hua Q, Li XY, Qin
L, Zhang HM, Meng GX and Su Q: Activation of NLRP3 Inflammasome by
Advanced Glycation End Products Promotes Pancreatic Islet Damage.
Oxid Med Cell Longev. 2017:96925462017. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Geicu OI, Stanca L, Voicu SN, Dinischiotu
A, Bilteanu L, Serban AI and Calu V: Dietary AGEs involvement in
colonic inflammation and cancer: insights from an in vitro
enterocyte model. Sci Rep. 10:25742020. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Son S, Hwang I, Han SH, Shin JS, Shin OS
and Yu JW: Advanced glycation end products impair NLRP3
inflammasome-mediated innate immune responses in macrophages. J
Biol Chem. 292:20437–20448. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Wilczynski JR and Duechler M: How do
Tumors Actively Escape from Host Immunosurveillance? Arch Immunol
Ther Exp (Warsz). 58:435–448. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Kim M and Park K: Dietary Fat Intake and
Risk of Colorectal Cancer: A Systematic Review and Meta-Analysis of
Prospective Studies. Nutrients. 10:19632018. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Padidar S, Farquharson AJ, Williams LM,
Kearney R, Arthur JR and Drew JE: High-fat diet alters gene
expression in the liver and colon: links to increased development
of aberrant crypt foci. Dig Dis Sci. 57:1866–1874. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Han J, Jiang Y, Liu X, Meng Q, Xi Q,
Zhuang Q, Han Y, Gao Y, Ding Q and Wu G: Dietary Fat Intake and
Risk of Gastric Cancer: A Meta-Analysis of Observational Studies.
PLoS One. 10:e01385802015. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Duan Y, Zeng L, Zheng C, Song B, Li F,
Kong X and Xu K: Inflammatory Links Between High Fat Diets and
Diseases. Front Immunol. 9:26492018. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Fujiyama Y, Hokari R, Miura S, Watanabe C,
Komoto S, Oyama T, Kurihara C, Nagata H and Hibi T: Butter feeding
enhances TNF-α production from macrophages and lymphocyte adherence
in murine small intestinal microvessels. J Gastroenterol Hepatol.
22:1838–1845. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Ralston JC, Lyons CL, Kennedy EB, Kirwan
AM and Roche HM: Fatty Acids and NLRP3 Inflammasome-Mediated
Inflammation in Metabolic Tissues. Stover PJ and Balling R: Annu
Rev Nutrition. 37:77–102. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Karasawa T, Kawashima A, Usui-Kawanishi F,
Watanabe S, Kimura H, Kamata R, Shirasuna K, Koyama Y, Sato-Tomita
A, Matsuzaka T, et al: Saturated Fatty Acids Undergo Intracellular
Crystallization and Activate the NLRP3 Inflammasome in Macrophages.
Arterioscler Thromb Vasc Biol. 38:744–756. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Kruger C and Zhou Y: Red meat and colon
cancer: A review of mechanistic evidence for heme in the context of
risk assessment methodology. Food Chem Toxicol. 118:131–153. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Sun H, Zhang C, Cao S, Sheng T, Dong N and
Xu Y: Fenton reactions drive nucleotide and ATP syntheses in
cancer. J Mol Cell Biol. 10:448–459. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Toyokuni S: Iron and carcinogenesis: From
Fenton reaction to target genes. Redox Rep. 7:189–197. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Chua ACG, Klopcic B, Lawrance IC, Olynyk
JK and Trinder D: Iron: An emerging factor in colorectal
carcinogenesis. World J Gastroenterol. 16:663–672. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Maras JS, Das S, Sharma S, Sukriti S,
Kumar J, Vyas AK, Kumar D, Bhat A, Yadav G, Choudhary MC, et al:
Iron-Overload triggers ADAM-17 mediated inflammation in Severe
Alcoholic Hepatitis. Sci Rep. 8:102642018. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Moss ML, Jin SLC, Milla ME, Burkhart W,
Carter HL, Chen WJ, Clay WC, Didsbury JR, Hassler D, Hoffman CR, et
al: Cloning of a disintegrin metalloproteinase that processes
precursor tumour-necrosis factor-alpha. Nature. 385:733–736. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Parameswaran N and Patial S: Tumor
Necrosis Factor-α Signaling in Macrophages. Crit Rev Eukaryot Gene
Expr. 20:87–103. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Derry MM, Raina K, Agarwal C and Agarwal
R: Identifying molecular targets of lifestyle modifications in
colon cancer prevention. Front Oncol 2013. 3:1192013.PubMed/NCBI
|
|
71
|
Durko L and Malecka-Panas E: Lifestyle
Modifications and Colorectal Cancer. Curr Colorectal Cancer Rep.
10:45–54. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Handschin C and Spiegelman BM: The role of
exercise and PGC1 alpha in inflammation and chronic disease.
Nature. 454:463–469. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Olesen J, Kiilerich K and Pilegaard H:
PGC-1 alpha-mediated adaptations in skeletal muscle. Pflugers Arch.
460:153–162. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Holly JMP, Biernacka K, Maskell N and
Perks CM: Obesity, Diabetes and COVID-19: An Infectious Disease
Spreading From the East Collides With the Consequences of an
Unhealthy Western Lifestyle. Front Endocrinol (Lausanne).
11:5828702020. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Traore K, Arama C, Medebielle M, Doumbo O
and Picot S: Do advanced glycation end- products play a role in
malaria susceptibility? Parasite. 23:152016. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Na H-K and Lee JY: Molecular Basis of
Alcohol-Related Gastric and Colon Cancer. Int J Mol Sci.
18:11162017. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Bailey KL, Samuelson DR and Wyatt TA:
Alcohol use disorder: A pre-existing condition for COVID-19?
Alcohol. 90:11–17. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Arvers P: Alcohol consumption and lung
damage: Dangerous relationships. Rev Mal Respir. 35:1039–1049.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Lin CL, Liu TC, Wang YN, Chung CH and
Chien WC: The Association Between Sleep Disorders and the Risk of
Colorectal Cancer in Patients: A Population-based Nested
Case-Control Study. In Vivo. 33:573–579. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Silva FRD, Guerreiro RC, Andrade HA,
Stieler E, Silva A and de Mello MT: Does the compromised sleep and
circadian disruption of night and shiftworkers make them highly
vulnerable to 2019 coronavirus disease (COVID-19)? Chronobiol Int.
37:607–617. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Rosselot AE, Hong CI and Moore SR: Rhythm
and bugs: circadian clocks, gut microbiota, and enteric infections.
Curr Opin Gastroenterol. 32:7–11. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Sinha R and Rothman N: Role of well-done,
grilled red meat, heterocyclic amines (HCAs) in the etiology of
human cancer. Cancer Lett. 143:189–194. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Jaarin K, Mustafa MR and Leong XF: The
effects of heated vegetable oils on blood pressure in rats.
Clinics. 66:2125–2132. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Ocvirk S, Wilson AS, Appolonia CN, Thomas
TK and O'Keefe SJD: Fiber, Fat, and Colorectal Cancer: New Insight
into Modifiable Dietary Risk Factors. Curr Gastroenterol Rep.
21:62. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Batchu SN, Kaur H, Yerra VG, Advani SL,
Kabir MG, Liu Y, Klein T and Advani A: Lung and Kidney ACE2 and
TMPRSS2 in Renin-Angiotensin System Blocker-Treated Comorbid
Diabetic Mice Mimicking Host Factors That Have Been Linked to
Severe COVID-19. Diabetes. 70:759–771. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Las Heras V, Clooney AG, Ryan FJ,
Cabrera-Rubio R, Casey PG, Hueston CM, Pinheiro J, Rudkin JK,
Melgar S, Cotter PD, et al: Short-term consumption of a high-fat
diet increases host susceptibility to Listeria monocytogenes
infection. Microbiome. 7:72019. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Berlau J, Glei M and Pool-Zobel B: Colon
cancer risk factors from nutrition. Anal Bioanal Chem. 378:737–743.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Rouget A, Vardon-Bounes F, Lorber P,
Vavasseur A, Marion O, Marcheix B, Lairez O, Balardy L, Fourcade O,
Conil JM, et al: Prevalence of malnutrition in coronavirus disease
19: The NUTRICOV study. Br J Nutr. 126:1296–1303. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Taylor AK, Cao W, Vora KP, De La Cruz J,
Shieh WJ, Zaki SR, Katz JM, Sambhara S and Gangappa S: Protein
Energy Malnutrition Decreases Immunity and Increases Susceptibility
to Influenza Infection in Mice. J Infect Dis. 207:501–510. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Pillay V, Isaacson C, Mothobi P, Hale M,
Tomar LK, Tyagi C, Altini M, Choonara YE and Kumar P: Carcinogenic
nitrosamines in traditional beer as the cause of oesophageal
squamous cell carcinoma in black South Africans. S Afr Med J.
105:656–658. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Thomas P, Fugmann R, Aranyi C, Barbera P,
Gibbons R and Fenters J: The effect of dimethylnitrosamine on host
resistance and immunity. Toxicol Appl Pharmacol. 77:219–229. 1985.
View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Seiwert N, Heylmann D, Hasselwander S and
Fahrer J: Mechanism of colorectal carcinogenesis triggered by heme
iron from red meat. Biochim Biophys Acta Rev Cancer.
1873:1883342020. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Kamyari N, Soltanian AR, Mahjub H and
Moghimbeigi A: Diet, Nutrition, Obesity, and Their Implications for
COVID-19 Mortality: Development of a Marginalized Two-Part Model
for Semicontinuous Data. JMIR Public Health Surveill. 7:e227172021.
View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Tappel A: Heme of consumed red meat can
act as a catalyst of oxidative damage and could initiate colon,
breast and prostate cancers, heart disease and other diseases. Med
Hypotheses. 68:562–564. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Kerr J, Anderson C and Lippman SM:
Physical activity, sedentary behaviour, diet, and cancer: an update
and emerging new evidence. Lancet Oncol. 18:E457–E471. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Hamer M, Kivimaki M, Gale CR and Batty GD:
Lifestyle Risk Factors for Cardiovascular Disease in Relation to
COVID-19 Hospitalization: A Community-Based Cohort Study of 387,109
Adults in UK. medRxiv. May 13–2020.(Epub ahead of print). doi:
10.1101/2020.05.09.20096438.
|
|
97
|
Stravinskas Durigon T, MacKenzie B,
Carneiro Oliveira-Junior M, Santos-Dias A, De Angelis K, Malfitano
C, Kelly da Palma R, Moreno Guerra J, Damaceno-Rodrigues NR, Garcia
Caldini E, et al: Aerobic Exercise Protects from Pseudomonas
aeruginosa-Induced Pneumonia in Elderly Mice. J Innate Immun.
10:279–290. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Dekker E, Tanis PJ, Vleugels JLA, Kasi PM
and Wallace MB: Colorectal cancer. Lancet. 394:1467–1480. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Rahman A and Sathi NJ: Risk factors of the
severity of COVID-19: A meta-analysis. Int J Clin Pract.
75:e139162021. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Duffney PF, Embong AK, McGuire CC,
Thatcher TH, Phipps RP and Sime PJ: Cigarette smoke increases
susceptibility to infection in lung epithelial cells by
upregulating caveolin-dependent endocytosis. PLoS One.
15:e02321022020. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Zhang Z and Zhang X: Salt Taste
Preference, Sodium Intake and Gastric Cancer in China. Asian Pac J
Cancer Prev. 12:1207–1210. 2011.PubMed/NCBI
|
|
102
|
Post A, Dullaart RPF and Bakker SJL: Is
low sodium intake a risk factor for severe and fatal COVID-19
infection? Eur J Int Med. 75:1092020. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Targonski R, Sadowski J, Price S and
Targonski R: Sodium-induced inflammation-an invisible player in
resistant hypertension. Hypertension Res. 43:629–633. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Gholipour M, Islami F, Roshandel G,
Khoshnia M, Badakhshan A, Moradi A and Malekzadeh R: Esophageal
Cancer in Golestan Province, Iran: A Review of Genetic
Susceptibility and Environmental Risk Factors. Middle East J Dig
Dis. 8:249–266. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Baillargeon J, Polychronopoulou E, Kuo YF
and Raji MA: The Impact of Substance Use Disorder on COVID-19
Outcomes. Psychiatr Serv. 72:578–581. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Yang L, Chen X, Simet SM, Hu G, Cai Y, Niu
F, Kook Y and Buch SJ: Reactive Oxygen Species/Hypoxia-Inducible
Factor-1 alpha/Platelet-Derived Growth Factor-BB Autocrine Loop
Contributes to Cocaine-Mediated Alveolar Epithelial Barrier Damage.
Am J Respir Cell Mol Biol. 55:736–748. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Pereira F, Jesus Larriba M and Munoz A:
Vitamin D and colon cancer. Endocr Relat Cancer. 19:R51–R71. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Meltzer DO, Best TJ, Zhang H, Vokes T,
Arora V and Solway J: Association of Vitamin D Status and Other
Clinical Characteristics With COVID-19 Test Results. JAMA Netw
Open. 3:e20197222020. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Mandell EW, Ryan S, Seedorf GJ, Gonzalez
T, Smith BJ, Fleet JC and Abman SH: Maternal Vitamin D Deficiency
Causes Sustained Impairment of Lung Structure and Function and
Increases Susceptibility to Hyperoxia-induced Lung Injury in Infant
Rats. Am J Respir Cell Mol Biol. 63:79–91. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Xie Y, Zhao Y, Shi L, Li W, Chen K, Li M,
Chen X, Zhang H, Li T, Matsuzawa-Ishimoto Y, et al: Gut epithelial
TSC1/mTOR controls RIPK3-dependent necroptosis in intestinal
inflammation and cancer. J Clin Invest. 130:2111–2128. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
111
|
Butler MJ and Barrientos RM: The impact of
nutrition on COVID-19 susceptibility and long-term consequences.
Brain Behav Immun. 87:53–54. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
112
|
Kramer B, França LM, Zhang Y, Paes AMA,
Gerdes AM and Carrillo-Sepulveda MA: Western diet triggers
Toll-like receptor 4 signaling-induced endothelial dysfunction in
female Wistar rats. Am J Physiol Heart Circ Physiol.
315:H1735–H1747. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
113
|
Worthley DL, Ruszkiewicz A, Davies R,
Moore S, Nivison-Smith I, Bik To L, Browett P, Western R, Durrant
S, So J, et al: Human Gastrointestinal Neoplasia-Associated
Myofibroblasts Can Develop from Bone Marrow-Derived Cells Following
Allogeneic Stem Cell Transplantation. Stem Cells. 27:1463–1468.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
114
|
Huang J, Lin H, Wu Y, Fang Y, Kumar R,
Chen G and Lin S: COVID-19 in posttransplant patients-report of 2
cases. AmJ Transplant. 20:1879–1881. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Gowdy KM, Martinu T, Nugent JL, Manzo ND,
Zhang HL, Kelly FL, Holtzman MJ and Palmer SM: Impaired CD8(+) T
cell immunity after allogeneic bone marrow transplantation leads to
persistent and severe respiratory viral infection. Transplant
Immunol. 32:51–60. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
116
|
Gong CS, Yoo MW, Kim BS, Hwang S, Kim KH,
Yook JH, Kim BS and Lee SG: De Novo Gastric Cancer After Liver
Transplantation. Ann Transplant. 21:386–391. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
117
|
Garrido I, Liberal R and Macedo G: Review
article: COVID-19 and liver disease-what we know on 1st May 2020.
Aliment Pharmacol Ther. 52:267–275. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
118
|
Laici C, Gamberini L, Bardi T, Siniscalchi
A, Reggiani MLB and Faenza S: Early infections in the intensive
care unit after liver transplantation-etiology and risk factors: A
single-center experience. Transpl Infect Dis. 20:e128342018.
View Article : Google Scholar : PubMed/NCBI
|
|
119
|
Cheung KS, Chan EW, Wong AYS, Chen L, Wong
ICK and Leung WK: Long-term proton pump inhibitors and risk of
gastric cancer development after treatment for Helicobacter
pylori: A population-based study. Gut. 67:28–35. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
120
|
Almario CV, Chey WD and Spiegel BMR:
Increased Risk of COVID-19 Among Users of Proton Pump Inhibitors.
Am J Gastroenterol. 115:1707–1715. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
121
|
Canani RB, Cirillo P, Roggero P, Romano C,
Malamisura B, Terrin G, Passariello A, Manguso F, Morelli L and
Guarino A: Working Group on Intestinal Infections of the Italian
Society of Pediatric Gastroenterology, HepatologyNutrition
(SIGENP): Therapy with gastric acidity inhibitors increases the
risk of acute gastroenteritis and community-acquired pneumonia in
children. Pediatrics. 117:e817–e820. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
122
|
Roshan MHK, Tambo A and Pace NP: The role
of testosterone in colorectal carcinoma: pathomechanisms and open
questions. EPMA J. 7:222016. View Article : Google Scholar : PubMed/NCBI
|
|
123
|
Erfinanda L, Ravindran K, Kohse F, Gallo
K, Preissner R, Walther T and Kuebler WM: Oestrogen-mediated
upregulation of the Mas receptor contributes to sex differences in
acute lung injury and lung vascular barrier regulation. Eur
Respirat J. 57:20009212021. View Article : Google Scholar
|
|
124
|
Thabet HS, Thabet SS, Ali NM and Ahmed NS:
Effects of ovariectomy and thyroidectomy on course and outcome of
Trichinella spiralis infection rat. Egypt Soc Parasitol. 38:29–46.
2008.PubMed/NCBI
|
|
125
|
Sheridan J, Tosetto M, Gorman J,
O'Donoghue D, Sheahan K, Hyland J, Mulcahy H, Gibbons D and
O'Sullivan J: Effects of radiation on levels of DNA damage in
normal non-adjacent mucosa from colorectal cancer cases. J
Gastrointest Cancer. 44:41–45. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
126
|
Song K, Gong H, Xu B, Dong X, Li L, Hu W,
Wang Q, Xie Z, Rao Z, Luo Z, et al: Association between recent
oncologic treatment and mortality among patients with carcinoma who
are hospitalized with COVID-19: A multicenter study. Cancer.
127:437–448. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
127
|
Gowda SSN, Raviraj R, Nagarajan D and Zhao
W: Radiation-induced lung injury: impact on macrophage
dysregulation and lipid alteration - a review. Immunopharmacol
Immunotoxicol. 41:370–379. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
128
|
Balhareth A, Reynolds IS, Solon JG, Harte
EG, Boland F, O'Sullivan JM, Burke JP, Little D and McNamara DA:
Thirty-seven-year Population-based Study of Colorectal Cancer Rates
in Renal Transplant Recipients in Ireland. Transplant Proc.
50:3434–3439. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
129
|
Caillard S, Chavarot N, Francois H,
Matignon M, Greze C, Kamar N, Gatault P, Thaunat O, Legris T,
Frimat L, et al: Is COVID-19 infection more severe in kidney
transplant recipients? Am J Transplant. 21:1295–1303. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
130
|
Kinnunen S, Karhapaa P, Juutilainen A,
Finne P and Helantera I: Secular Trends in Infection-Related
Mortality after Kidney Transplantation. Clin J Am Soc Nephrol.
13:755–762. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
131
|
Cai ZZ, Xu JG, Zhou YH, Zheng JH, Lin KZ,
Zheng SZ, Ye MS, He Y, Liu CB and Xue ZX: Human
cytomegalovirus-encoded US28 may act as a tumor promoter in
colorectal cancer. World J Gastroenterol. 22:2789–2798. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
132
|
Moss P: ‘The ancient and the new’: is
there an interaction between cytomegalovirus and SARS-CoV-2
infection? Immun Ageing. 17:142020. View Article : Google Scholar : PubMed/NCBI
|
|
133
|
Zhou W, Xi D, Shi Y, Wang L, Zhong H,
Huang Z, Liu Y, Tang Y, Lu N, Wang Y, et al: MicroRNA-1929-3p
participates in murine cytomegalovirus-induced hypertensive
vascular remodeling through Ednra/NLRP3 inflammasome activation.
Int J Mol Med. 47:719–731. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
134
|
Chang C and Worrell SG: Viruses and
esophageal cancer. Dis Esophagus. 33:doaa0362020. View Article : Google Scholar : PubMed/NCBI
|
|
135
|
Shrock E, Fujimura E, Kula T, Timms RT,
Lee IH, Leng Y, Robinson ML, Sie BM, Li MZ, Chen Y, et al: Viral
epitope profiling of COVID-19 patients reveals cross-reactivity and
correlates of severity. Science. 370:eabd42502020. View Article : Google Scholar : PubMed/NCBI
|
|
136
|
Sartori E, Calistri A, Salata C, Del
Vecchio C, Palù G and Parolin C: Herpes simplex virus type 2
infection increases human immunodeficiency virus type 1 entry into
human primary macrophages. Virol J. 8:2662011. View Article : Google Scholar : PubMed/NCBI
|
|
137
|
Wu F, Groopman JD and Pestka JJ: Public
Health impacts of foodborne mycotoxins. Klaenhammer TR: Annu Rev
Food Sci Technol. 5:351–372. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
138
|
Liu D, Ge L, Wang Q, Su J, Chen X, Wang C
and Huang K: Low-level contamination of deoxynivalenol: A threat
from environmental toxins to porcine epidemic diarrhea virus
infection. Environ Int. 143:1059492020. View Article : Google Scholar : PubMed/NCBI
|
|
139
|
Li M, Harkema JR, Islam Z, Cuff CF and
Pestka JJ: T-2 toxin impairs murine immune response to respiratory
reovirus and exacerbates viral bronchiolitis. Toxicol Appl
Pharmacol. 217:76–85. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
140
|
Jeong CH, Kwon HC, Cheng WN, Kim DH, Choi
Y and Han SG: Aluminum exposure promotes the metastatic proclivity
of human colorectal cancer cells through matrix metalloproteinases
and the TGF-beta/Smad signaling pathway. Food Chem Toxicol.
141:1114022020. View Article : Google Scholar : PubMed/NCBI
|
|
141
|
Omran GA: Hematological and immunological
impairment following in-utero and postnatal exposure to aluminum
sulfate in female offspring of albino rats. Immunopharmacol
Immunotoxicol. 41:40–47. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
142
|
Moulahoum H, Boumaza BMA, Ferrat M and
Djerdjouri B: Arsenic trioxide exposure accelerates colon
preneoplasic aberrant crypt foci induction regionally through
mitochondrial dysfunction. Toxicol Res. 7:182–190. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
143
|
Zeng HL, Yang Q, Yuan P, Wang X and Cheng
L: Associations of essential and toxic metals/metalloids in whole
blood with both disease severity and mortality in patients with
COVID-19. FASEB J. 35:e213922021. View Article : Google Scholar : PubMed/NCBI
|
|
144
|
Zhang WH, Huang J, Feng M, Tong YQ, Guan
XH, Jiang HW and Wei S: Elevated Arsenic Exposure Is Associated
with an Increased Risk of Chronic Hepatitis B Virus Infection:
NHANES (2003–2014) in US Adults. Curr Med Sci. 38:610–617. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
145
|
Di Ciaula A: Asbestos ingestion and
gastrointestinal cancer: a possible underestimated hazard. Expert
Rev Gastroenterol Hepatol. 11:419–425. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
146
|
Musk AW, de Klerk N, Reid A, Hui J,
Franklin P and Brims F: Asbestos-related diseases. Int J Tuberc
Lung Dis. 24:562–567. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
147
|
Talibov M, Sormunen J, Hansen J, Kjaerheim
K, Martinsen JI, Sparen P, Tryggvadottir L, Weiderpass E and
Pukkala E: Benzene exposure at workplace and risk of colorectal
cancer in four Nordic countries. Cancer Epidemiol. 55:156–161.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
148
|
Luo Y, Yan J and McClure S: Distribution
of the environmental and socioeconomic risk factors on COVID-19
death rate across continental USA: A spatial nonlinear analysis.
Environ Sci Pollut Res Int. 28:6587–6599. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
149
|
Hosgood HD III, Zhang L, Shen M, Berndt
SI, Vermeulen R, Li G, Yin S, Yeager M, Yuenger J, Rothman N, et
al: Association between genetic variants in VEGF, ERCC3 and
occupational benzene haematotoxicity. Occup Environ Med.
66:848–853. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
150
|
Morinaga K, Oshima A and Hara I: Multiple
primary cancers following exposure to benzidine and beta
naphthylamine. Am J Ind Med. 3:243–246. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
151
|
Hu H, Zheng Y, Wen X, Smith SS, Nizomov J,
Fishe J, Hogan WR, Shenkman EA and Bian J: An external
exposome-wide association study of COVID-19 mortality in the United
States. Sci Total Environ. 768:144832. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
152
|
Luster MI, Tucker AN, Hayes HT, Pung OJ,
Burka T, McMillan R and Eling T: Immunosuppressive effects of
benzidine in mice - evidence of alterations in arachidonic-acid
metabolism. J Immunol. 135:2754–2761. 1985.PubMed/NCBI
|
|
153
|
Bolli A, Bulzomi P, Galluzzo P, Acconcia F
and Marino M: Bisphenol A Impairs Estradiol-induced Protective
Effects Against DLD-1 Colon Cancer Cell Growth. IUBMB Life.
62:684–687. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
154
|
Zahra A, Sisu C, Silva E, De Aguiar Greca
SC, Randeva HS, Chatha K, Kyrou I and Karteris E: Is There a Link
between Bisphenol A (BPA), a Key Endocrine Disruptor, and the Risk
for SARS-CoV-2 Infection and Severe COVID-19? J Clin Med.
9:32962020. View Article : Google Scholar : PubMed/NCBI
|
|
155
|
Abedelhaffez AS, El-Aziz EAA, Aziz MAA and
Ahmed AM: Lung injury induced by Bisphenol A: A food contaminant,
is ameliorated by selenium supplementation. Pathophysiology.
24:81–89. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
156
|
Naji S, Issa K, Eid A, Iratni R and Eid
AH: Cadmium Induces Migration of Colon Cancer Cells: Roles of
Reactive Oxygen Species, P38 and Cyclooxygenase-2. Cell Physiol
Biochem. 52:1517–1534. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
157
|
Zeng HL, Zhang B, Wang X, Yang Q and Cheng
L: Urinary trace elements in association with disease severity and
outcome in patients with COVID-19. Environ Res. 194:1106702021.
View Article : Google Scholar : PubMed/NCBI
|
|
158
|
Krueger WS and Wade TJ: Elevated blood
lead and cadmium levels associated with chronic infections among
non-smokers in a cross-sectional analysis of NHANES data. Environ
Health. 15:162016. View Article : Google Scholar : PubMed/NCBI
|
|
159
|
Jacobi CA, Sabat R, Bohm B, Zieren HU,
Volk HD and Müller JM: Pneumoperitoneum with carbon dioxide
stimulates growth of malignant colonic cells. Surgery. 121:72–78.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
160
|
Duarte CM, Jaremko L and Jaremko M:
Hypothesis: Potentially Systemic Impacts of Elevated CO2
on the Human Proteome and Health. Front Public Health.
8:5433222020. View Article : Google Scholar : PubMed/NCBI
|
|
161
|
Kato K, Kawai T, Fujii M, Bunai Y, Shima H
and Takahashi M: Enhancing effect of preadministration of carbon
tetrachloride on methylazoxymethanol acetate-induced intestinal
carcinogenesis. J Toxicol Sci. 10:289–294. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
162
|
Unsal V, Cicek M and Sabancilar İ:
Toxicity of carbon tetrachloride, free radicals and role of
antioxidants. Rev Environ Health. Sep 24–2020.(Epub ahead of
print). doi: 10.1515/reveh-2020-0048. PubMed/NCBI
|
|
163
|
Mills PK and Yang RC: Agricultural
exposures and gastric cancer risk in Hispanic farm workers in
California. Environ Res. 104:282–289. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
164
|
Tryphonas H, Bondy G, Hodgen M, Coady L,
Parenteau M, Armstrong C, Hayward S and Liston V: Effects of
cis-nonachlor, trans-nonachlor and chlordane on the immune system
of Sprague-Dawley rats following a 28-day oral (gavage) treatment.
Food Chemi Toxicol. 41:107–118. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
165
|
El-Tawil AM: Colorectal cancers and
chlorinated water. World J Gastrointest Oncol. 8:402–409. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
166
|
Bornstein SR, Voit-Bak K, Schmidt D,
Morawietz H, Bornstein AB, Balanzew W, Julius U, Rodionov RN,
Biener AM, Wang J, et al: Is There a Role for Environmental and
Metabolic Factors Predisposing to Severe COVID-19? Horm Metab Res.
52:540–546. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
167
|
Gao S, Wang Y, Zhang P, Dong Y and Li B:
Subacute oral exposure to dibromoacetic acid induced immunotoxicity
and apoptosis in the spleen and thymus of the mice. Toxicol Sci.
105:331–341. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
168
|
McDorman KS, Chandra S, Hooth MJ, Hester
SD, Schoonhoven R and Wolf DC: Induction of transitional cell
hyperplasia in the urinary bladder and aberrant crypt foci in the
colon of rats treated with individual and a mixture of drinking
water disinfection by-products. Toxicol Pathol. 31:235–242. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
169
|
Keegan TE, Simmons JE and Pegram RA: NOAEL
and LOAEL determinations of acute hepatotoxicity for chloroform and
bromodichloromethane delivered in an aqueous vehicle to F344 rats.
J Toxicol Environ Health-Part A. 55:65–75. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
170
|
Suriyo T, Tachachartvanich P,
Visitnonthachai D, Watcharasit P and Satayavivad J: Chlorpyrifos
promotes colorectal adenocarcinoma H508 cell growth through the
activation of EGFR/ERK1/2 signaling pathway but not cholinergic
pathway. Toxicology. 338:117–129. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
171
|
Chen YC, Pai MH, Chen YT and Hou YC:
Dietary exposure to chlorpyrifos affects systemic and hepatic
immune-cell phenotypes in diabetic mice. Toxicology.
452:1526982021. View Article : Google Scholar : PubMed/NCBI
|
|
172
|
Chappell GA, Wikoff DS and Thompson CM:
Assessment of Mechanistic Data for Hexavalent Chromium-Induced
Rodent Intestinal Cancer Using the Key Characteristics of
Carcinogens. Toxicol Sci. 180:38–50. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
173
|
Antonini JM and Roberts JR: Chromium in
stainless steel welding fume suppresses lung defense responses
against bacterial infection in rats. J Immunotoxicol. 4:117–127.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
174
|
Kirkeleit J, Riise T, Bjorge T, Moen BE,
Bratveit M and Christiani DC: Increased risk of oesophageal
adenocarcinoma among upstream petroleum workers. Occup Environ Med.
67:335–340. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
175
|
McLoone P, Dyussupov O, Nurtlessov Z,
Kenessariyev U and Kenessary D: The effect of expsoure to crude oil
on the immune system. Health implications for people living near
oil exploration activities. Int J Environ Health Res. 31:762–787.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
176
|
Chen HP, Pan MH, Chou YY, Sung C, Lee KH,
Leung CM and Hsu PC: Effects of di(2-ethylhexyl)phthalate exposure
on 1,2-dimethyhydrazine-induced colon tumor promotion in rats. Food
Chem Toxicol. 103:157–167. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
177
|
Adamovsky O, Buerger AN, Vespalcova H,
Sohag SR, Hanlon AT, Ginn PE, Craft SL, Smatana S, Budinska E,
Persico M, et al: Evaluation of Microbiome-Host Relationships in
the Zebrafish Gastrointestinal System Reveals Adaptive Immunity Is
a Target of Bis(2-ethylhexyl) Phthalate (DEHP) Exposure. Environ
Sci Technol. 54:5719–5728. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
178
|
Martínez Góngora V, Matthes KL, Castaño
PR, Linseisen J and Rohrmann S: Dietary Heterocyclic Amine Intake
and Colorectal Adenoma Risk: A Systematic Review and Meta-analysis.
Cancer Epidemiol Biomarkers Prev. 28:99–109. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
179
|
Yun CH, Son CG, Jung U and Han SH:
Immunosuppressive effect of 2-amino-1-methyl-6-phenylimidazo 4,5-b
pyridine (PhIP) through the inhibition of T-lymphocyte
proliferation and IL-2 production. Toxicology. 217:31–38. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
180
|
Suman S, Kumar S, Moon BH, Fornace AJ Jr
and Datta K: Low and high dose rate heavy ion radiation-induced
intestinal and colonic tumorigenesis in APC1638N/+ mice.
Life Sci Space Res (Amst). 13:45–50. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
181
|
Baselet B, Sonveaux P, Baatout S and Aerts
A: Pathological effects of ionizing radiation: endothelial
activation and dysfunction. Cell Mol Life Sci. 76:699–728. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
182
|
Kim H, Lee J, Woo HD, Kim DW, Oh JH, Chang
HJ, Sohn DK, Shin A and Kim J: Dietary mercury intake and
colorectal cancer risk: A case-control study. Clin Nutr.
39:2106–2113. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
183
|
Silbergeld EK, Sacci JB and Azad AF:
Mercury exposure and murine response to Plasmodium yoelii
infection and immunization. Immunopharmacol Immunotoxicol.
22:685–695. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
184
|
Yan X, Zhang Y, Lu Y, He L, Qu J, Zhou C,
Hong P, Sun S, Zhao H, Liang Y, et al: The Complex Toxicity of
Tetracycline with Polystyrene Spheres on Gastric Cancer Cells. Int
J Environ Res Public Health. 17:28082020. View Article : Google Scholar : PubMed/NCBI
|
|
185
|
Hirt N and Body-Malapel M: Immunotoxicity
and intestinal effects of nano- and microplastics: A review of the
literature. Part Fibre Toxicol. 17:572020. View Article : Google Scholar : PubMed/NCBI
|
|
186
|
Zijno A, De Angelis I, De Berardis B,
Andreoli C, Russo MT, Pietraforte D, Scorza G, Degan P, Ponti J,
Rossi F and Barone F: Different mechanisms are involved in
oxidative DNA damage and genotoxicity induction by ZnO and
TiO2 nanoparticles in human colon carcinoma cells.
Toxicol In Vitro. 29:1503–1512. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
187
|
Calderón-Garcidueñas L, Torres-Jardón R,
Franco-Lira M, Kulesza R, González-Maciel A, Reynoso-Robles R,
Brito-Aguilar R, García-Arreola B, Revueltas-Ficachi P,
Barrera-Velázquez JA, et al: Environmental Nanoparticles,
SARS-CoV-2 Brain Involvement, and Potential Acceleration of
Alzheimer's and Parkinson's Diseases in Young Urbanites Exposed to
Air Pollution. J Alzheimers Dis. 78:479–503. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
188
|
Chakraborty S, Castranova V, Perez MK and
Piedimonte G: Nanoparticles increase human bronchial epithelial
cell susceptibility to respiratory syncytial virus infection via
nerve growth factor-induced autophagy. Physiol Rep. 5:e133442017.
View Article : Google Scholar : PubMed/NCBI
|
|
189
|
Lightfoot NE, Berriault CJ, Seilkop SK and
Conard BR: Nonrespiratory mortality and cancer incidence in a
cohort of Canadian nickel workers. Arch Environ Occup Health.
72:187–203. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
190
|
Guo H, Liu H, Jian Z, Cui H, Fang J, Zuo
Z, Deng J, Li Y, Wang X, Zhao L, et al: Immunotoxicity of nickel:
Pathological and toxicological effects. Ecotoxicol Environ Saf.
203:1110062020. View Article : Google Scholar : PubMed/NCBI
|
|
191
|
Schullehner J, Hansen B, Thygesen M,
Pedersen CB and Sigsgaard T: Nitrate in drinking water and
colorectal cancer risk: A nationwide population-based cohort study.
Int J Cancer. 143:73–79. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
192
|
Alamdari DH, Moghaddam AB, Amini S,
Keramati MR, Zarmehri AM, Alamdari AH, Damsaz M, Banpour H,
Yarahmadi A and Koliakos G: Application of methylene blue -vitamin
C -N-acetyl cysteine for treatment of critically ill COVID-19
patients, report of a phase-I clinical trial. Eur J Pharmacol.
885:1734942020. View Article : Google Scholar : PubMed/NCBI
|
|
193
|
Rodríguez-Estival J, Martínez-Haro M,
Martín-Hernando MA and Mateo R: Sub-chronic effects of nitrate in
drinking water on red-legged partridge (Alectoris rufa):
Oxidative stress and T-cell mediated immune function. Environ Res.
110:469–475. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
194
|
Jakszyn P and Gonzalez CA: Nitrosamine and
related food intake and gastric and oesophageal cancer risk: A
systematic review of the epidemiological evidence. World J
Gastroenterol. 12:4296–4303. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
195
|
Gao XQ, Fei F, Huo HH, Huang B, Meng XS,
Zhang T and Liu BL: Impact of nitrite exposure on plasma
biochemical parameters and immune-related responses in
Takifugu rubripes. Aquat Toxicol. 218:1053622020. View Article : Google Scholar : PubMed/NCBI
|
|
196
|
Ethan CJ, Mokoena KK, Yu Y, Shale K, Fan
Y, Rong J and Liu F: Association between PM2.5 and
mortality of stomach and colorectal cancer in Xi'an: A time-series
study. Environ Sci Pollut Res Int. 27:22353–22363. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
197
|
Ogen Y: Assessing nitrogen dioxide
(NO2) levels as a contributing factor to coronavirus
(COVID-19) fatality. Sci Total Environ. 726:1386052020. View Article : Google Scholar : PubMed/NCBI
|
|
198
|
Pathmanathan S, Krishna MT, Blomberg A,
Helleday R, Kelly FJ, Sandström T, Holgate ST, Wilson SJ and Frew
AJ: Repeated daily exposure to 2 ppm nitrogen dioxide upregulates
the expression of IL-5, IL-10, IL-13, and ICAM-1 in the bronchial
epithelium of healthy human airways. Occup Environ Med. 60:892–896.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
199
|
Howsam M, Grimalt JO, Guinó E, Navarro M,
Martí-Ragué J, Peinado MA, Capellá G and Moreno V; Bellvitge
Colorectal Cancer Group, : Organochlorine exposure and colorectal
cancer risk. Environ Health Perspect. 112:1460–1466. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
200
|
Lie E, Larsen HJ, Larsen S, Johansen GM,
Derocher AE, Lunn NJ, Norstrom RJ, Wiig Ø and Skaare JU: Does high
organochlorine (OC) exposure impair the resistance to infection in
polar bears (Ursus maritimus)? Part 1: Effect of OCs on the
humoral immunity. J Toxicol Environ Health A. 67:555–582. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
201
|
Li Y, Fu Y, Hu K, Zhang Y, Chen J, Zhang
S, Zhang B and Liu Y: Positive correlation between human exposure
to organophosphate esters and gastrointestinal cancer in patients
from Wuhan, China. Ecotoxicol Environ Saf. 196:1105482020.
View Article : Google Scholar : PubMed/NCBI
|
|
202
|
Rajak P, Ganguly A, Sarkar S, Mandi M,
Dutta M, Podder S, Khatun S and Roy S: Immunotoxic role of
organophosphates: An unseen risk escalating SARS-CoV-2
pathogenicity. Food Chem Toxicol. 149:1120072021. View Article : Google Scholar : PubMed/NCBI
|
|
203
|
Medina-Buelvas DM, Estrada-Muñiz E,
Rodríguez-Sosa M, Shibayama M and Vega L: Increased heart fibrosis
and acute infection in a murine Chagas disease model associated
with organophosphorus pesticide metabolite exposure. Sci Rep.
9:175392019. View Article : Google Scholar : PubMed/NCBI
|
|
204
|
Cheng J, Su H and Xu Z: Intraday effects
of outdoor air pollution on acute upper and lower respiratory
infections in Australian children. Environ Pollut. 268:1156982021.
View Article : Google Scholar : PubMed/NCBI
|
|
205
|
Lin YC, Wei PL, Tsai YT, Wong JH, Chang
CM, Wang JY, Hou MF, Lee YC, Chuang HY and Chang WC:
Pb2+ induced IL-8 gene expression by extracellular
signal-regulated kinases and the transcription factor, activator
protein 1, in human gastric carcinoma cells. Environ Toxicol.
30:315–322. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
206
|
Fernandez-Cabezudo MJ, Ali SA, Ullah A,
Hasan MY, Kosanovic M, Fahim MA, Adem A and al-Ramadi BK:
Pronounced susceptibility to infection by Salmonella
enterica serovar Typhimurium in mice chronically exposed to
lead correlates with a shift to Th2-type immune responses. Toxicol
Appl Pharmacol. 218:215–226. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
207
|
Miao C, Ma J, Zhang Y, Chu Y, Li J, Kuai
R, Wang S and Peng H: Perfluorooctanoic acid enhances colorectal
cancer DLD-1 cells invasiveness through activating NF-κB mediated
matrix metalloproteinase-2/-9 expression. Int J Clin Exp Pathol.
8:10512–10522. 2015.PubMed/NCBI
|
|
208
|
Ait Bamai Y, Goudarzi H, Araki A, Okada E,
Kashino I, Miyashita C and Kishi R: Effect of prenatal exposure to
per- and polyfluoroalkyl substances on childhood allergies and
common infectious diseases in children up to age 7 years: The
Hokkaido study on environment and children's health. Environ Int.
143:1059792020. View Article : Google Scholar : PubMed/NCBI
|
|
209
|
Huang X, Guan S, Wang J, Zhao L, Jia Y, Lu
Z, Yin C, Yang S, Song Q, Han L, et al: The effects of air
pollution on mortality and clinicopathological features of
esophageal cancer. Oncotarget. 8:58563–58576. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
210
|
Hutter HP, Poteser M, Moshammer H,
Lemmerer K, Mayer M, Weitensfelder L, Wallner P and Kundi M: Air
Pollution Is Associated with COVID-19 Incidence and Mortality in
Vienna, Austria. Int J Environ Res Public Health. 17:92752020.
View Article : Google Scholar : PubMed/NCBI
|
|
211
|
Farina F, Sancini G, Battaglia C, Tinaglia
V, Mantecca P, Camatini M and Palestini P: Milano Summer
Particulate Matter (PM10) Triggers Lung Inflammation and Extra
Pulmonary Adverse Events in Mice. PLoS One. 8:e566362013.
View Article : Google Scholar : PubMed/NCBI
|
|
212
|
Meo SA, Abukhalaf AA, Alomar AA, Alessa
OM, Sami W and Klonoff DC: Effect of environmental pollutants
PM-2.5, carbon monoxide, and ozone on the incidence and mortality
of SARS-COV-2 infection in ten wildfire affected counties in
California. Sci Total Environ. 757:1439482021. View Article : Google Scholar : PubMed/NCBI
|
|
213
|
Zhu H, Wu Y, Kuang X, Liu H, Guo Z, Qian
J, Wang D, Wang M, Chu H, Gong W, et al: Effect of PM2.5 exposure
on circulating fibrinogen and IL-6 levels: A systematic review and
meta-analysis. Chemosphere. 271:129565. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
214
|
Stølevik SB, Nygaard UC, Namork E, Haugen
M, Meltzer HM, Alexander J, Knutsen HK, Aaberge I, Vainio K, van
Loveren H, et al: Prenatal exposure to polychlorinated biphenyls
and dioxins from the maternal diet may be associated with
immunosuppressive effects that persist into early childhood. Food
Chem Toxicol. 51:165–172. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
215
|
Roshandel G, Semnani S, Malekzadeh R and
Dawsey SM: Polycyclic aromatic hydrocarbons and esophageal squamous
cell carcinoma. Arch Iran Med. 15:713–722. 2012.PubMed/NCBI
|
|
216
|
Domingo JL and Rovira J: Effects of air
pollutants on the transmission and severity of respiratory viral
infections. Environ Res. 187:1096502020. View Article : Google Scholar : PubMed/NCBI
|
|
217
|
Låg M, Øvrevik J, Refsnes M and Holme JA:
Potential role of polycyclic aromatic hydrocarbons in air
pollution-induced non-malignant respiratory diseases. Respir Res.
21:2992020. View Article : Google Scholar : PubMed/NCBI
|
|
218
|
Lee W, Ahn YS, Lee S, Song BM, Hong S and
Yoon JH: Occupational exposure to crystalline silica and gastric
cancer: a systematic review and meta-analysis. Occup Environ Med.
73:794–801. 2016.PubMed/NCBI
|
|
219
|
Naidoo RN and Jeebhay MF: COVID-19: a new
burden of respiratory disease among South African miners? Curr Opin
Pulm Med. 27:79–87. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
220
|
Benmerzoug S, Bounab B, Rose S, Gosset D,
Biet F, Cochard T, Xavier A, Rouxel N, Fauconnier L, Horsnell WGC,
et al: Sterile Lung Inflammation Induced by Silica Exacerbates
Mycobacterium tuberculosis Infection via STING-Dependent Type 2
Immunity. Cell Rep. 27:2649–2664.e5. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
221
|
Chang CJ, Tu YK, Chen PC and Yang HY: Talc
exposure and risk of stomach cancer: Systematic review and
meta-analysis of occupational cohort studies. J Formos Med Assoc.
119:781–792. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
222
|
Radić I, Vucak I, Milosević J, Marusić A,
Vukicević S and Marusić M: Immunosuppression induced by talc
granulomatosis in the rat. Clin Exp Immunol. 73:316–321.
1988.PubMed/NCBI
|
|
223
|
Xie G, Peng Z and Raufman JP: Src-mediated
aryl hydrocarbon and epidermal growth factor receptor cross talk
stimulates colon cancer cell proliferation. J Physiol Gastrointest
Liver Physiol. 302:G1006–G1015. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
224
|
Fiorito F, Santamaria R, Irace C, De
Martino L and Iovane G: 2,3,7,8-tetrachlorodibenzo-p-dioxin and the
viral infection. Environ Res. 153:27–34. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
225
|
Fredriksson M, Bengtsson NO, Hardell L and
Axelson O: Colon cancer, physical activity, and occupational
exposures. A case-control study. Cancer. 63:1838–1842. 1989.
View Article : Google Scholar : PubMed/NCBI
|
|
226
|
Selgrade MK and Gilmour MI: Suppression of
pulmonary host defenses and enhanced susceptibility to respiratory
bacterial infection in mice following inhalation exposure to
trichloroethylene and chloroform. J Immunotoxicol. 7:350–356. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
227
|
Hou N, Zhang X, Zhao L, Zhao X, Li Z, Song
T and Huang C: A novel chronic stress-induced shift in the Th1 to
Th2 response promotes colon cancer growth. Biochem Biophys Res
Commun. 439:471–476. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
228
|
Lamontagne SJ, Pizzagalli DA and Olmstead
MC: Does inflammation link stress to poor COVID-19 outcome? Stress
Health. 37:401–414. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
229
|
Schmidt SAJ, Sørensen HT, Langan SM and
Vestergaard M: Perceived psychological stress and risk of herpes
zoster: A nationwide population-based cohort study. Br J Dermatol.
185:130–138. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
230
|
Lin Q, Wang F, Yang R, Zheng X, Gao H and
Zhang P: Effect of Chronic Restraint Stress on Human Colorectal
Carcinoma Growth in Mice. Plos One. 8:e614352013. View Article : Google Scholar : PubMed/NCBI
|
|
231
|
Cai Y, Li YF, Tang LP, Tsoi B, Chen M,
Chen H, Chen XM, Tan RR, Kurihara H and He RR: A new mechanism of
vitamin C effects on A/FM/1/47(H1N1) virus-induced pneumonia in
restraint-stressed mice. Biomed Res Int. 2015:6751492015.
View Article : Google Scholar : PubMed/NCBI
|