Introduction
Non-small cell lung cancer (NSCLC) accounts for ~85%
of all lung cancers (1,2). NSCLC is often classified into three
main histological subtypes: Adenocarcinoma, squamous cell carcinoma
and large cell carcinoma (1).
Although smoking is the main risk factor for NSCLC (3), the incidence of NSCLC is also
increasing among non-smokers who are exposure to tobacco (1). The standard treatment of NSCLC
consists of surgery, chemotherapy, radiation therapy, targeted
therapy and immunotherapy (4).
Chemotherapy is the standard treatment modality for early-stage
NSCLC (4). Similarly, favorable
curative effects have been achieved through advances in
radiotherapy techniques (5).
Moreover, the most common targeted therapeutic strategy is vascular
endothelial growth factor (6–8) or
epidermal growth factor receptor inhibition (9,10).
However, issues such as drug resistance, systemic toxicity and high
costs remain major obstacles for the adoption of these
strategies.
For decades, platinum-based chemotherapeutics have
dominated the treatment of NSCLC (11–13).
Among them, cisplatin has become the most commonly used first-line
drug because of its excellent efficacy (14). Unfortunately, chemoresistance often
develops during treatment, which seriously limits the clinical
utility of cisplatin (14).
Usually, combination treatment is a powerful means to overcome this
resistance (15).
Meanwhile, fibroblast activation protein (FAP) a
type-II transmembrane serine protease, expressed almost exclusively
to pathological conditions including fibrosis, arthritis and
cancer. Across most cancer types, FAP plays critical roles in tumor
proliferation, tumor invasion, angiogenesis and drug resistance,
and elevated FAP is associated with worse clinical outcomes
(16–18). Previous research demonstrated that
treatment strategies targeting FAP in combination with other
approaches such as chemotherapy, radiotherapy and immunotherapy
could strengthen treatment efficacy (17,18).
However, the role of FAP degradation in enhancing cisplatin
sensitivity of NSCLC is unclear. Thus, the present study
investigated the effect of FAP degradation on the therapeutic
effect of cisplatin against NSCLC.
Materials and methods
Reagents
Cisplatin (cat. no. HY-17394; CAS no. 15663-27-1)
was purchased from MedChemExpress. Human anti-CD26 polyclonal
antibody (cat. no. 29403-1-AP), human anti-FAP polyclonal antibody
(cat. no. 11779-1-AP), human anti-caspase-3 polyclonal antibody
(cat. no. 19677-1-AP), HRP-conjugated goat anti-rabbit IgG (H+L)
secondary antibody (cat. no. SA00001-2) and human anti-cleaved
caspase 3 polyclonal antibody (cat. no. 25128-1-AP) were purchased
from Proteintech Group, Inc. Pomalidomide-PEG2-FAP2286: FAP-D was
obtained from Shanghai Apeptide Co., Ltd. Protein extraction kit
(cat. no. R0018M), Cell-Counting Kit-8 (CCK-8; cat. no. c0038),
radioimmunoprecipitation assay buffers (cat. no. P0013B) and
bicinchoninic acid (BCA) protein concentration assay kit (cat. no.
P0012) were purchased from Beyotime Institute of Biotechnology.
NCI-H1299 cells (cat. no. SCSP-589) were purchased from National
Collection of Authenticated Cell Cultures. All other reagents,
chemicals and cell lines were local.
Molecular docking
Molecular docking was performed using AutoDock Vina
1.2.0 (19). Concerning the docking
parameters of the receptor, the center coordinates of the docking
box (center X, center Y and center Z) were set to (38.034, 0.53 and
69.455). The number of grid points in each direction of XYZ was set
to 60×60×60, the docking accuracy exhaustiveness was 25 and the
output binding conformation was set to 100. The docking results
were visualized using PyMOL (version 2.5.0) (20) and LigPlot+(version 2.3)
(21). The structure of human FAP
alpha was obtained from Protein Data Bank (https://www.rcsb.org/structure/1Z68).
Protein degradation
NCI-H1299 cells (5×105 cells/ml) were
cultured in 96-well plates. FAP-D was added to each well (Final
concentrations: 0.01, 0.05, 0.1, 0.25, 0.5, 1, 5, 10 and 20 µM),
and cells were cultured at 37°C for 12 h. Then, proteins were
extracted from cells for western blotting. The protocols assessing
the effects of FAP-D on protein degradation in H460 cells and
effects of time on protein degradation were similar.
CCK-8 assay
H1299 cells (1×105 cells/ml) were
cultured in 96-well plates. FAP-D was added to each well (final
concentrations: 0.5, 1, 5, 10 and 20 µM), and cells were cultured
at 37°C for 24 h. Then, the culture medium was discarded, and cell
viability was determined according to the standard CCK-8 assay
protocol using the EnVision microplate reader (Revvity, Inc.). For
half-maximal inhibitory concentration (IC50) assessment,
FAP-D (0 or 5 µM) was added to each well, and cells were cultured
at 37°C for 12 h. The culture medium was discarded, and cisplatin
was added to each well (final concentrations: 0.01, 0.05, 0.1, 0.5,
1, 5, 10, 50, 100, and 500 µM), after which cells were cultured at
37°C for 12 h. After discarding the culture medium, cell viability
was determined according to the standard CCK-8 assay protocol using
the EnVision microplate reader. Volume of CCK-8 used was 20 µl and
the solutions were incubated at 37°C for 2 h. The absorbance at 450
nm of solutions cultured without drugs was defined as 100%. The
protocols of effects of FAP-D and cisplatin + FAP-D on cell
viabilities of H460 cells were similar. Unless otherwise stated,
all experiments were repeated three times.
Wound-healing assay
H1299 or H460 cells were cultured in serum-free
medium without/with cisplatin (5 µM, 24 h) or cisplatin (5 µM) +
FAP-D (5 µM; cells were cultured with FAP-D for 12 h and then with
cisplatin for 12 h). Cells were then cultured to confluence and
scratched with a cell scraper. The debris was removed via washes
with the culture medium. The cells were subsequently cultured in an
incubator for 24 h. The images were acquired by microscopy and
analyzed using ImageJ software (version 1.52a; National Institutes
of Health).
Western blotting
The samples were prepared according as follows:
cells were lysed using the radioimmunoprecipitation assay buffers
and the solutions were centrifuged (14,000 × g 10 min). The protein
concentrations were obtained using BCA assay. The samples were
separated through 10% sodium dodecyl sulfate polyacrylamide gel
electrophoresis and then transferred onto polyvinylidene difluoride
membranes (transfer current set to 250 mA). The membranes were
blocked in 5% milk at room temperature for 1 h, and then were
incubated with primary antibodies (FAP antibody: Dilution, 1:1,000;
CD26 antibody: Dilution, 1:1,500; caspase-3 antibody: Dilution,
1:1,000; and cleaved caspase 3 antibody: Dilution, 1:1,000) at 4°C.
Membranes were then washed with Tris-buffered saline with Tween-20
(0.05%) buffer and incubated with horseradish peroxidase-modified
secondary antibodies (1:10,000) at room temperature for 1 h.
Lastly, the membranes were imaged through Amersham™ ImageQuant™ 800
western blot imaging systems. The densitometric analysis were
performed from ImageJ software (1.52a; National Institutes of
Health)
Animal experiments
The animal experiments were approved by the
institutional animal ethics committee of Kunming Medical University
(approval no. kmmu20241355; Kunming, China). BALB/c mice were
purchased from the Department of Experimental Zoology, Kunming
Medical University (Kunming, China). All clinical procedures were
conducted in accordance with the relevant provisions of the
Declaration of Helsinki. The studies were additionally conducted in
accordance with local legislation and institutional requirements.
Body weights of mice were ~18–19 g (healthy, 5–6 weeks old). Mice
were fed at 25°C in the standard animal experiment lab and the
humidity were maintained at 53%. The feeds and water were replaced
every 3 days. The light/dark cycle was set as 12 h light/12 h dark.
For biosafety experiments, BALB/c mice were randomly divided into
two groups (n=5/group): PBS (control) group and FAP-D group. Mice
in the FAP-D group were first anesthetized with 3% isoflurane via
inhalation and then intraperitoneally injected with FAP-D (3 mg/kg,
once daily for 7 days). Mice in the control group were first
anesthetized with 3% isoflurane via inhalation and then
intraperitoneally injected with phosphate-buffered saline (PBS).
After treatment, mice were sacrificed via spinal dislocation, and
the major organs were collected for analysis. For intervention
experiments, nude BALB/c mice were randomly divided into three
groups (n=6/group): PBS (control) group, cisplatin group, and
cisplatin + FAP-D group. The mice were first subcutaneously
injected with H1299 cells (5×106 cells, 100 µl, in the
right sides of the mice back) and monitored for 10 days to permit
tumor growth. After tumor formation, mice in the cisplatin group
were first anesthetized with 3% isoflurane via inhalation and then
intratumorally injected with cisplatin (20 mg/kg, once every 3
days, 3 times). Then, the body weight and volume were recorded
every 3 days. After treatment, mice were sacrificed via spinal
dislocation, and the tumors were weighed and then sliced or mashed
for further experiments. Mice in the cisplatin + FAP-D group were
first anesthetized with 3% isoflurane via inhalation and then
intratumorally injected with FAP-D (1.5 mg/kg, once every 3 days,
three times), followed by an intraperitoneal injection of cisplatin
(20 mg/kg, once every 3 days, three times) after 12 h. Mice were
euthanized after 21 days or upon reaching tumor volume ≥2.000
mm3 or >20% body weight loss, with tumors processed
for analysis. The other protocols were similar.
Statistical analysis
Statistical analysis was performed using GraphPad
Prism 9.0 (Dotmatics) and Origin 9 software (OriginLab
Corporation). All data are determined from at least three
independent experiments and presented as the mean ± standard
deviation (SD). Statistical significance was assessed by ANOVA
followed by Dunnett post-hoc test. P<0.05 was considered to
indicate a statistically significant difference.
Results
FAP degradation
FAP-D consisted of three components: Pomalidomide,
the FAP-binding peptide FAP 2286, and a linker (Diethylene glycol,
Fig. 1A). The results of
high-performance liquid chromatography and mass spectrometry are
presented in Figs. S1 and S2. Molecular docking exhibited that
several hydrophobic interactions and hydrogen bonds were formed
between FAP-D and FAP (Figs. 1A and
S3). Specifically, Arg123, Tyr124
and Gln547 in FAP formed hydrogen bonds with oxygen atoms in FAP-D.
Trp623, Leu571, Ala554, Val552, Ile367, Phe350, Phe579, Gly349,
Phe351, Val352, Ala207 and Ile398 in FAP formed hydrophobic
interactions with FAP-D. The binding energy between FAP-D and FAP
was −10.484 kcal/mol. These results suggested the binding force
between FAP-D and FAP was strong. Western blotting demonstrated
that FAP degradation increased as the FAP-D concentration increased
(Figs. 1B and S4). Conversely, CD26 was not degraded by
FAP-D, supporting the selectivity of FAP-D. In addition, FAP was
degraded by FAP-D within 12 h (Figs.
1C and S5). These findings
indicate that FAP-D is an ideal FAP degrader.
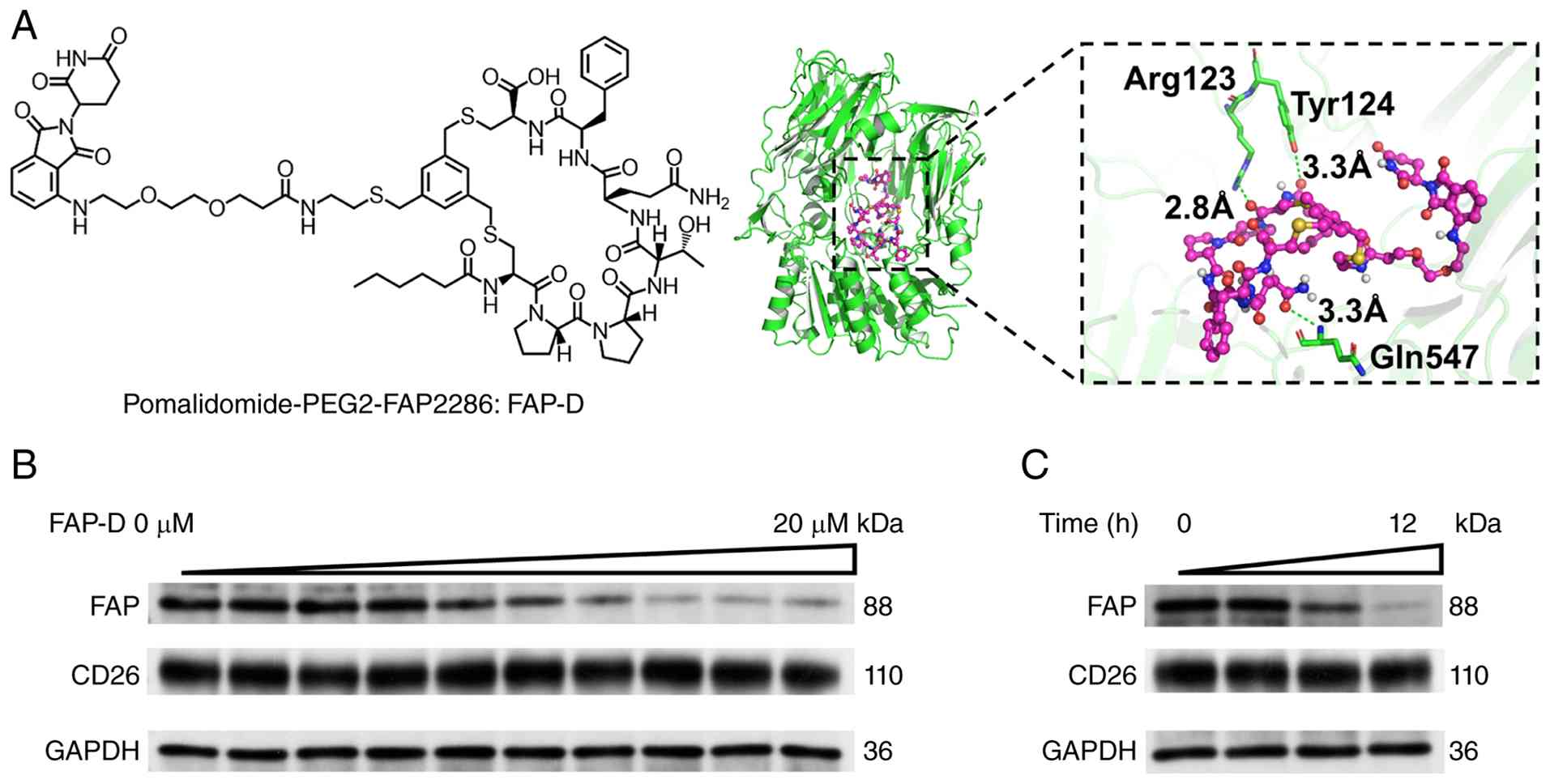 | Figure 1.(A) Chemical formula of FAP-D and the
binding model between FAP-D and FAP (PDB: 1z68). (B) Western
blotting of FAP (n=3) and CD26 expression in H1299 cells treated
with different concentrations of FAP-D (0, 0.01, 0.05, 0.1, 0.25,
0.5, 1, 5, 10 and 20 µM) for 12 h. (C) Western blotting of FAP
(n=3) and CD26 expression in H1299 cells treated with 5 µM FAP-D
for 0, 3, 6, or 12 h. FAP, fibroblast activation protein; FAP-D,
FAP degrader. |
Enhancement of the cisplatin
sensitivity of H1299 cells by FAP-D
Considering the degradation performance of FAP-D,
its effect on the cisplatin sensitivity of H1299 cells was
explored. First, the effects of FAP-D on H1299 cell viability were
studied. As presented in Fig. 2A,
the viability of H1299 cells was reduced from 100 to 80% in
response to increasing FAP-D concentration, suggesting that FAP
degradation has little effect on cell viability. Second, FAP
degradation was found to reduce the IC50 of cisplatin in
H1299 cells (1.36 µM vs. 5.71 µM, Fig.
2B), indicating enhanced cisplatin sensitivity. In addition,
the mobility of H1299 cells treated with cisplatin + FAP-D was
reduced (Fig. 2C and D). This
result suggested that the extracellular matrix, which is
responsible for proliferation and migration, was destroyed by
FAP-D, leading to reduced cell viability. Lastly, the expression of
cleaved caspase 3 (a major index of apoptosis) was increased by
treatment with cisplatin + FAP-D (Figs.
2E and S6). These results
reveal that the cisplatin sensitivity of H1299 cells was enhanced
by FAP-D, resulting in strengthened apoptosis. Similarly, these
results were confirmed through H460 cells (Figs. S7A-E and S8).
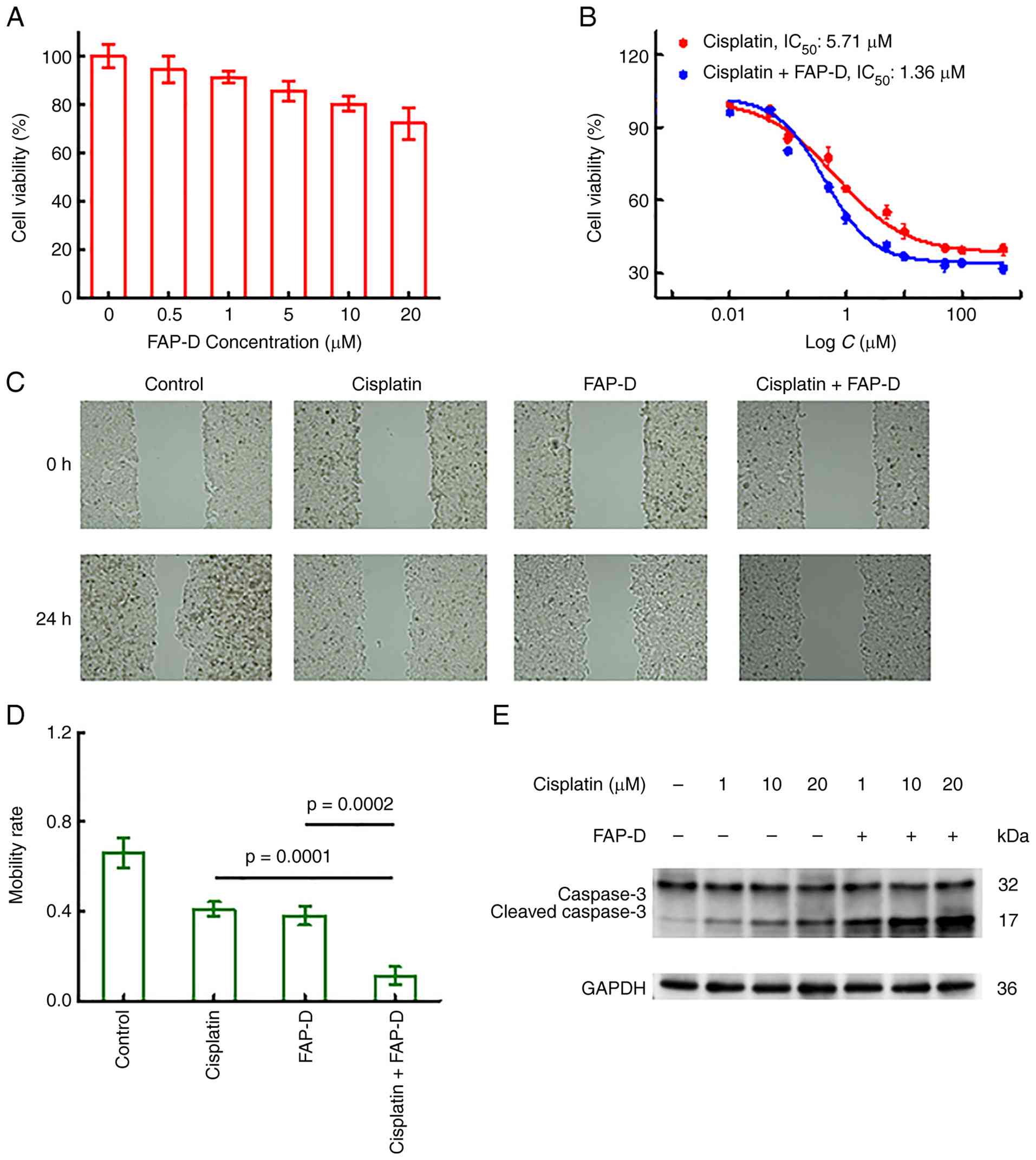 | Figure 2.(A) Effect of different
concentrations of FAP-D (24 h of treatment) on H1299 cell
viability. (B) Effects of cisplatin or cisplatin + FAP-D
concentrations (treatment for 24 h) on H1299 cell viabilities. (C)
Images of wounded H1299 cells in the different groups. Conditions:
cisplatin (5 µM, 24 h), FAP-D (5 µM, 24 h), and cisplatin + FAP-D
(5 µM FAP-D for 12 h followed by 5 µM cisplatin for 12 h). (D) The
statistical results from 2C. ANOVA test (n=3). (E) Western blotting
of caspase 3 and cleaved caspase 3 (Cle. Cas 3, n=3) expression in
different groups of H1299 cells. Cells were treated with cisplatin
(1, 10, or 20 µM, 24 h) or cisplatin + FAP-D (5 µM FAP-D for 12 h
followed by 1, 10, or 20 µM cisplatin for 12 h). FAP, fibroblast
activation protein; FAP-D, FAP degrader. |
Therapeutic effects of cisplatin +
FAP-D in vivo
The in vivo therapeutic effects of cisplatin
+ FAP-D were then studied. First, the potential in vivo
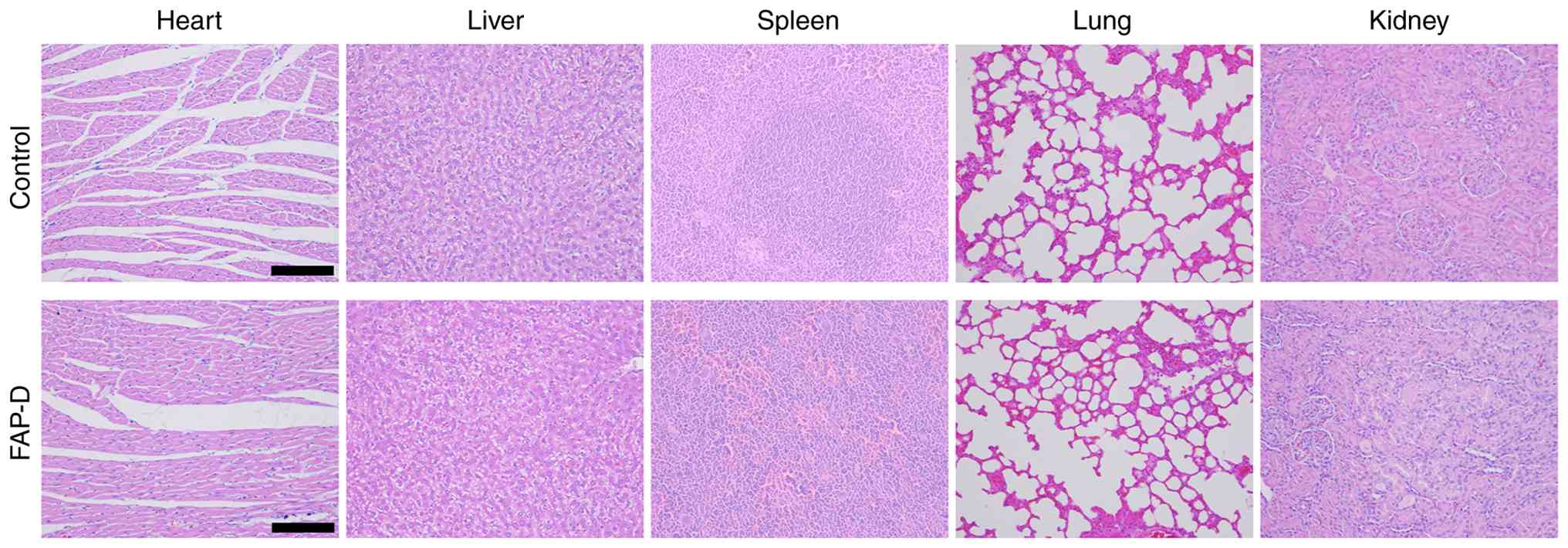
toxicity of FAP-D was investigated. As presented in Fig. 3, no damage was observed in the major
organs (heart, liver, spleen, lungs and kidneys) of mice treated
with FAP-D, indicating its favorable biocompatibility.
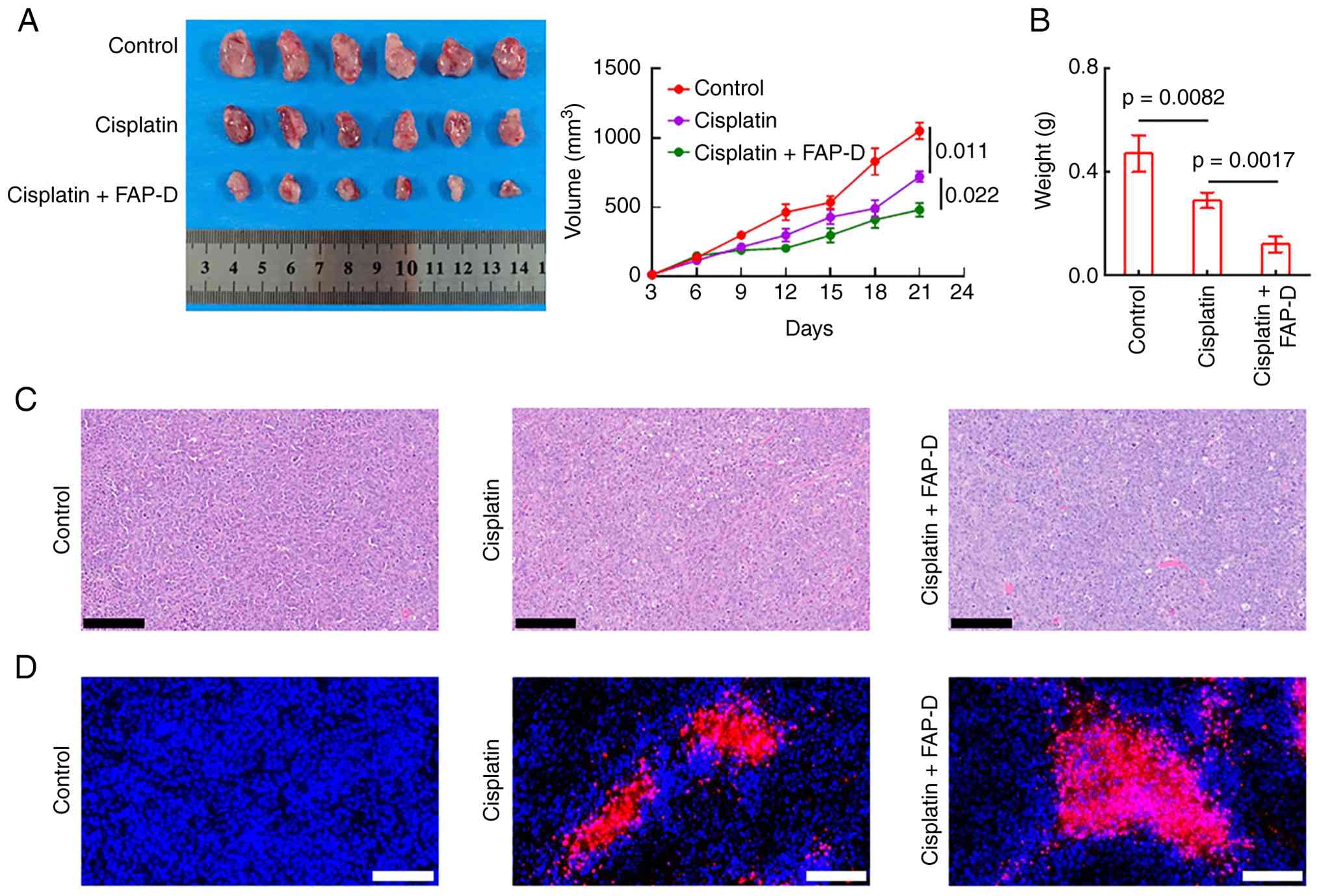
After confirming the biocompatibility of FAP-D, the
in vivo therapeutic effects of cisplatin + FAP-D were
systematically examined. As illustrated in Fig. 4A, the tumor volumes of mice treated
with cisplatin alone were smaller than those in control mice.
Interestingly, tumor growth was inhibited in mice pre-treated with
FAP-D, as confirmed by tumor weight (Fig. 4B). Moreover, H&E and TUNEL
staining revealed that apoptosis was enhanced in the tumors of mice
co-treated with FAP-D (Fig. 4C and
D). In addition, no significant changes in body weights were
observed (Fig. S9). These results
reveal that apoptosis was enhanced by FAP-D in tumors.
Discussion
Cisplatin resistance has become a serious issue in
NSCLC (22–24), which can be overcome by combination
treatment strategies (15). In the
past, a high response rate with modest side effects could be
achieved in stage IIIB and IV NSCLC by the combination of
gemcitabine and cisplatin (25).
Additionally, cisplatin-etoposide combination chemotherapy achieved
success (26). Meanwhile,
combinations of traditional Chinese medicine and cisplatin have
emerged as effective strategies (27,28).
Moreover, the treatment efficacy of chemotherapy can be
strengthened by targeting FAP (17,18).
In light of the development of nanotechnology in recent years,
novel nanoparticles co-loaded with cisplatin and oridonin were
developed for NSCLC treatment (29). Unfortunately, treatment efficacy can
be restricted by resistance or side effects from other drugs. Thus,
an auxiliary medicine with low drug resistance is urgently needed
for cisplatin-based combination regimens.
Protein degraders with the advantages of high
selectivity, catalytic dosages and extremely low drug resistance
(30,31) are ideal candidates for this purpose.
In the present study, a FAP-D was pioneered instead of a FAP
inhibitor to eliminate side effects. FAP was degraded by FAP-D with
excellent selectivity (Fig. 1). As
expected, the IC50 of cisplatin in H1299 cells was
lowered by combined treatment with FAP-D (Fig. 2), suggesting enhanced cisplatin
sensitivity. In addition, H1299/H460 cell apoptosis was strengthen
by this combination strategy (Figs.
2 and S7) and FAP-D exhibited
favorable biocompatibility (Fig.
3). In vivo, apoptosis in tumors was more strongly
induced in mice co-treated with FAP-D (Fig. 4). Compared with previous results
(32), the dosage of FAP-D used in
the present study was lower, and the biocompatibility was
excellent, highlighting the advantages of FAP-D.
In the present study, the therapeutic effects of
cisplatin + FAP-D on H1299 cells and heterogeneous tumors were
investigated systematically. The results demonstrated that the
cisplatin sensitivity of H1299 cells and tumors was enhanced by
co-treatment with FAP-D. The present findings revealed the great
clinical utility of cisplatin + FAP-D for NSCLC treatment.
The present study establishes a link between FAP-D
co-treatment and enhanced cisplatin sensitivity in NSCLC. However,
several limitations exist: The therapeutic effects of such method
on the organoids models are lack. Moreover, patient-derived tumor
xenograft models are also worth exploring. Finally, the deep
molecular mechanism of the role of the cisplatin + FAP-D needs to
be investigated. All the aforementioned approaches represent
important directions for our future investigations.
Supplementary Material
Supporting Data
Acknowledgements
The authors would like to thank Dr Joe Barber Jr.
from Liwen Bianji (Edanz) (www.liwenbianji.cn) for editing the English text of a
draft of this manuscript.
Funding
The present study was supported by the Doctoral Research Fund
Project of the First Affiliated Hospital of Kunming Medical
University (grant nos. 2022BS031 and 2023BS013), the Yunnan
Provincial Department of Education Science Research Fund Projects
(grant nos. 2025J0175 and 2025J0177), the Yunnan Fundamental
Research Kunming Medical University Projects (grant nos.
202501AY070001-063 and 202301AY070001-205), the Key Clinical
Specialty of Thoracic Surgery in Yunnan (grant no. 300067-3) and
the Science and Technology Department of Yunnan (grant no.
202401AT070066).
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
YZ, RL, XC and CZ conducted all experiments and
analyzed the data. YZ, RL, XC, CZ, YB, YC, XT and TX assisted in
data acquisition, data analysis and drafted the manuscript. XY and
JY performed the MD assays and assisted in data analysis. YZ and XY
designed the project and acquired funding. YZ, RL and XY confirm
the authenticity of all the raw data. All authors read and approved
the final version of the manuscript.
Ethics approval and consent to
participate
The animal experiments were permitted by the
institutional animal ethics committee of Kunming Medical University
(approval no. kmmu20241355; Kunming, China). All clinical
procedures were conducted in accordance with the relevant
provisions of the Declaration of Helsinki. The studies were
conducted in accordance with the local legislation and
institutional requirements.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Hendriks LEL, Remon J, Faivre-Finn C,
Garassino MC, Heymach JV, Kerr KM, Tan DSW, Veronesi G and Reck M:
Non-small-cell lung cancer. Nat Rev Dis Primers. 10:712024.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Travis WD, Brambilla E and Riely GJ: New
pathologic classification of lung cancer: Relevance for clinical
practice and clinical trials. J Clin Oncol. 31:992–1001. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Barta JA, Powell CA and Wisnivesky JP:
Global epidemiology of lung cancer. Ann Glob Health. 85:82019.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Araghi M, Mannani R, Heidarnejad Maleki A,
Hamidi A, Rostami S, Safa H, Faramarzi F, Khorasani S, Alimohammadi
M, Tahmasebi S and Akhavan-Sigari R: Recent advances in non-small
cell lung cancer targeted therapy; an update review. Cancer Cell
Int. 23:1622023. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Howington JA, Blum MG, Chang AC, Balekian
AA and Murthy SC: Treatment of stage I and II non-small cell lung
cancer: Diagnosis and management of lung cancer, 3rd ed: American
College of Chest Physicians evidence-based clinical practice
guidelines. Chest. 143 (Suppl 5):e278S–e313S. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhao YS, Guo SP, Deng J, Shen J, Du FK, Wu
X, Chen Y, Li MX, Chen MJ, Li XB, et al: VEGF/VEGFR-targeted
therapy and immunotherapy in non-small cell lung cancer: Targeting
the tumor microenvironment. Int J Biol Sci. 18:3845–3858. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lind JSW and Smit EF: Angiogenesis
inhibitors in the treatment of non-small cell lung cancer. Ther Adv
Med Oncol. 1:95–107. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Le XN, Nilsson M, Goldman J, Reck M,
Nakagawa K, Kato T, Ares LP, Frimodt-Moller B, Wolff K,
Visseren-Grul C, et al: Dual EGFR-VEGF pathway inhibition: A
promising strategy for patients with EGFR-mutant NSCLC. J Thorac
Oncol. 16:205–215. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fu K, Xie FC, Wang F and Fu LW:
Therapeutic strategies for EGFR-mutated non-small cell lung cancer
patients with osimertinib resistance. J Hematol Oncol. 15:1732022.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Passaro A, Mok T, Peters S, Popat S, Ahn
MJ and Marinis FD: Recent advances on the role of EGFR tyrosine
kinase inhibitors in the management of NSCLC with uncommon, non
exon 20 insertions, EGFR mutations. J Thorac Oncol. 16:764–773.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ellis PA, Smith IE, Hardy JR, Nicolson MC,
Talbot DC, Ashley SE and Priest K: Symptom relief with MVP
(mitomycin C, vinblastine and cisplatin) chemotherapy in advanced
non-small-cell lung cancer. Br J Cancer. 71:366–370. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Cosaert J and Quoix E: Platinum drugs in
the treatment of non-small-cell lung cancer. Br J Cancer.
87:825–833. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Goffin J, Lacchetti C, Ellis PM, Ung YC
and Evans WK; Lung Cancer Disease Site Group of Cancer Care
Ontario's Program in Evidence-Based Care, : First-line systemic
chemotherapy in the treatment of advanced non-small cell lung
cancer: A systematic review. J Thorac Oncol. 5:260–274. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Fennell DA, Summers Y, Cadranel J, Benepal
T, Christoph DC, Lal R, Das M, Maxwell F, Visseren-Grul C and Ferry
D: Cisplatin in the modern era: The backbone of first-line
chemotherapy for non-small cell lung cancer. Cancer Treat. Rev.
44:42–50. 2016.
|
|
15
|
Yao YF, Fareed R, Zafar A, Saleem K, Huang
T, Duan YT and Rehman MU: State-of-the-art combination treatment
strategies for advanced stage non-small cell lung cancer. Front
Oncol. 12:9585052022. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Fitzgerald AA and Weiner LM: The role of
fibroblast activation protein in health and malignancy. Cancer
Metast Rev. 39:783–803. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lee HH and Al-Ogaili Z: Fibroblast
activation protein and the tumour microenvironment: Challenges and
therapeutic opportunities. Oncol Rev. 19:16174872025. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wang Q, Song C, Zhao CY, Wei XY, Li DL, Wu
QT, Li J and Yang XM: Decoding tumors from fibroblast activation
protein: A review of the latest diagnostic and therapeutic
prospects. Int J Biol Macromol. 318:1450062025. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Eberhardt J, Santos-Martins D, Tillack AF
and Forli S: AutoDock Vina 1.2.0: New docking methods, expanded
force field, and python bindings. J Chem Inf Model. 61:3891–3898.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
DeLano WL: PyMOL: An open-source molecular
graphics tool. CCP4 Newsletter on Protein Crystallography.
40:82–92. 2002.https://www.scirp.org/reference/ReferencesPapers?ReferenceID=2323923
|
|
21
|
Laskowski RA and Swindells MB:
LigPlot+: Multiple ligand-protein interaction diagrams
for drug discovery. J Chem Inf Model. 51:2778–2786. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kurokawa M, Ise N, Omi K, Goishi K and
Higashiyama S: Cisplatin influences acquisition of resistance to
molecular-targeted agents through epithelial-mesenchymal
transition-like changes. Cancer Sci. 104:904–911. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Skowron MA, Oing C, Bremmer F, Ströbel P,
Murray MJ, Coleman N, Amatruda JF, Honecker F, Bokemeyer C, Albers
P and Nettersheim D: The developmental origin of cancers defines
basic principles of cisplatin resistance. Cancer Lett. 519:199–210.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Liu SX, Yang PS, Wang L, Zou XF, Zhang DD,
Chen WY, Hu C, Xiao DQ, Ren HZ, Zhang H and Cai SW: Targeting PAK4
reverses cisplatin resistance in NSCLC by modulating ER stress.
Cell Death Discov. 10:362024. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Crinò L, Scagliotti G, Marangolo M, Figoli
F, Clerici M, Marinis FD, Salvati F, Cruciani G, Dogliotti L, Pucci
F, et al: Cisplatin-gemcitabine combination in advanced
non-small-cell lung cancer: A phase II study. J Clin Oncol.
15:297–303. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ardizzoni A, Antonelli G, Grossi F, Tixi
L, Cafferata M and Rosso R: The combination of etoposide and
cisplatin in non-small-cell lung cancer (NSCLC). Ann Oncol. 10
(Suppl 5):S13–S17. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Zhao CC, Yan HF, Pang WT, Wu T, Kong XB,
Li XJ, Liu HG, Zhao LL, Liang F and Jia YJ: Lentinan combined with
cisplatin for the treatment of non-small cell lung cancer. Medicine
(Baltimore). 100:e252202021. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Xi ZC, Dai RC, Ze YF, Jiang X, Liu MF and
Xu HX: Traditional Chinese medicine in lung cancer treatment. Mol
Cancer. 24:572025. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Fan XL, Wang T, Ji ZY, Li QP, Shen HY and
Wang J: Synergistic combination therapy of lung cancer using
lipid-layered cisplatin and oridonin co-encapsulated nanoparticles.
Biomed Pharmacother. 141:1118302021. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Zhong GC, Chang XY, Xie WL and Zhou XX:
Targeted protein degradation: Advances in drug discovery and
clinical practice. Signal Transduct Target Ther. 9:3082024.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Martín-Acosta P and Xiao XS: PROTACs to
address the challenges facing small molecule inhibitors. Eur J Med
Chem. 210:1129932021. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Cho JM, Yang EH, Quan WY, Nam EH and Cheon
HG: Discovery of a novel fibroblast activation protein (FAP)
inhibitor, BR103354, with anti-diabetic and anti-steatotic effects.
Sci Rep. 10:212802020. View Article : Google Scholar : PubMed/NCBI
|