Introduction
Carpal tunnel syndrome (CTS) is the most common type
of nerve compression (1-3),
with a reported incidence of ~3.8-5% (4-6).
CTS is characterized by the compression of the median nerve within
the carpal canal of the wrist, resulting in pain and numbness in
the thumb, index, and middle and radial half of the ring fingers,
as well as the weakness and subsequent atrophy of the thenar
muscles (3). Nighttime
wakefulness, pain and insomnia can severely affect the quality of
life of patients with CTS.
Since Paget first described the disease in 1854,
several studies on CTS have been conducted (7). However, controversies related to the
pathogenesis, diagnosis and treatment of CTS remain. Currently, the
diagnosis of CTS is mainly based on the clinical symptoms and
characteristic physical examination findings. While
electrophysiological studies provide an objective measurement of
the nerve conduction abnormalities in CTS, it is argued that these
studies often have varied sensitivities and specificities, as they
are affected by factors such as height, age and finger
circumference (8-12).
Tinel's and Phalen's tests are the most common methods used for the
diagnosis of CTS. Both tests are categorized as sensory evoked
tests that use various methods, such as increased carpal tunnel
pressure, to induce paresthesia in the area innervated by the
median nerve. Although these methods are widely used as they are
easy to perform, their sensitivities and specificities are still
widely under debate. As per previous literature, the sensitivities
and specificities of Tinel's and Phalen's tests are 38-100% and
42-85%, and 54-98% and 55-100%, respectively (13).
In recent years, scholars have reported few novel
diagnostic physical examination methods, which include the scratch
collapse test (SCT) and hand elevation test. The SCT is considered
positive if the patient demonstrates a loss of resistance with the
affected side after ‘scratching’, which is more objective than the
other provocative tests that rely on the patient's subjective
feeling. The hand elevation test simply requires elevation of the
patient's hands above the head. These newer tests require less of
the examiner's skill or patient's compliance than traditional
tests.
The present study evaluated different physical
examination tests, including both the new diagnostic tests, such as
the SCT and hand elevation test, as well as traditional tests, such
as Tinel's, Phalen's and reverse Phalen's tests for the diagnosis
of patients with CTS. The sensitivities and specificities of these
tests were calculated and compared, and a receiver operating
characteristic (ROC) curve was used to determine which test has the
optimal diagnostic value.
Patients and methods
Study population
The present study analyzed 243 patients with CTS who
were enrolled in the study (from Huashan Hospital, Fudan
University, Shanghai, China) from December, 2019 to January, 2021.
Patients aged 20 to 80 years who expressed willingness to
participate in the study and who were able to perform the entire
series of examinations were included in the study. Patients who
refused to take part in the examination, pregnant women, patients
with post-operative CTS, those with cerebrovascular or peripheral
vascular disease, a history of severe trauma to the upper limbs and
cervical spondylosis were excluded. In addition, 7 patients were
excluded as they had concurrent peripheral nervous system diseases.
Finally, 236 patients (465 hands) were enrolled. Furthermore,
controls with the same age range and male-to-female ratio were
selected as the patents with CTS [age range, 20-80 years;
male-to-female ratio, 1:7.94; 96 controls (170 hands)] were
enrolled. The participants were then divided into the experimental
(CTS group) and control (non-CTS group) groups. The CTS-6 scale
(14) (Table I) as the gold standard for
diagnosis. A clinical diagnosis of CTS was made if the patient had
a score of ≥12 on the CTS-6 scale. This instrument is used to
estimate the probability of CTS based on the presence or absence of
six items recorded as part of the clinical history or noted on
physical examination that were weighted for their diagnostic
importance. The point values for all positive findings were then
added together; total scores ≥12 points were defined as positive
for CTS.
 | Table ICTS-6 scoring system. |
Table I
CTS-6 scoring system.
| Finding | | Points |
|---|
| Symptoms and
history | Numbness in median
nerve distribution: Sensory symptoms are mostly in the thumb,
index, middle and/or ring fingers | 3.5 |
| | Nocturnal symptoms:
Symptoms are prominent when patient sleeps; numbness wakes patient
from sleep | 4 |
| Physical
examination | Thenar atrophy or
weakness: The bulk of the thenar area is reduced or manual motor
testing shows strength of grade 4 or less | 5 |
| | Positive Phalen test:
Flexion of the wrist reproduces or worsens symptoms of numbness in
the median nerve territory | 5 |
| | Loss of 2-point
discrimination: A failure to discriminate two points held 5 mm or
less apart from one another, in the median nerve innervated digits,
is a positive test suggestive of CTS. | 4.5 |
| | Positive Tinel sign:
Light tapping over the median nerve at the level of the carpal
tunnel causing radiating paresthesia into the median nerve
innervated digits (not proximally) is a positive test | 4 |
The Human Research Committee of our hospital
approved the study protocol (KY2022-641). Written informed consent
was obtained from each of the participants.
Study protocol
After the assessment of clinical symptoms with a
questionnaire, physical examination and diagnostic tests were
performed by a single evaluator who underwent a 2-year hand surgery
training and was unaware of the patient histories and diagnoses.
The tests were performed in the following order: Tinel's, Phalen's,
reverse Phalen's, SCT and hand elevation test. Tinel's test was
performed by tapping the median nerve at the wrist, repeated four
to six times. The presence or absence of radiating pain or
paresthesia in the median nerve distribution was considered
positive. Phalen's test was performed by having each participant
position the wrist of the affected hand in complete palmar flexion
with the elbow flexed and the forearm pronated. The test was
considered positive if symptoms developed after 1 min (15). The reverse Phalen's test was
performed while the wrist was extended instead of flexed. The SCT
was performed by lightly scratching the patient's skin over the
area of nerve compression while the patient resisted external
rotation of the bilateral shoulders. This test was considered
positive if there was loss of resistance on the affected side after
‘scratching’ (16). The hand
elevation test was performed by elevating and maintaining both
hands of the patients above the head. The test was considered
positive if numbness and tingling in the thumb, index, and middle
and the radial half of the ring fingers developed within 2 min
(17).
Statistical and power analyses
The sensitivities and specificities of all tests
were compared using the Chi-squared test. The baseline data of the
participants are presented as the mean ± standard deviation (SD),
or as the number and percentage. The ROC curve was plotted for all
the physical examination results. P<0.05 was considered to
indicate a statistically significant difference, and the power was
set at 80%.
Results
The baseline characteristics of the study population
are presented in Table II. The
sensitivities, specificities, positive and negative predictive
values, and positive and negative likelihood ratios of the Tinel's,
Phalen's, reverse Phalen's, SCT and hand elevation tests are
presented in Table III. It was
observed that the sensitivities and specificities of the SCT and
hand elevation test were higher and lower than those of the other
tests, respectively. The positive likelihood ratio (LR+)
is the probability that an individual with the disease tested
positive divided by the probability that an individual without the
disease tested positive (i.e., LR+=true positive/false
positive). The negative likelihood ratio (LR-) is the
probability that an individual with the disease tested negative
divided by the probability that an individual without the disease
tested negative (i.e., LR-=false negative/true
negative). These tests in order of LR+ were the reverse
Phalen's test > SCT > Phalen's test > hand elevation test
> Tinel's test, thus revealing a high diagnostic accuracy. The
tests in order of LR, were the hand elevation test < SCT <
reverse Phalen's test < Phalen's test < Tinel's test, which
indicated that the hand elevation test and SCT had a high-level
ability to correctly exclude individuals without CTS.
| Table IIBaseline characteristics of the
patients with CTS and the control subjects who participated in the
present study. |
Table II
Baseline characteristics of the
patients with CTS and the control subjects who participated in the
present study.
| Characteristic | Patients with
CTS | Non-CTS controls |
|---|
| Number of hands | 465 | 170 |
| Age (years): mean ±
SD | 51.92±10.90 | 48.91±12.82 |
| Males, n (%) | 52 (11.23) | 19 (11.18) |
| Females, n (%) | 413 (89.20) | 151 (88.82) |
| Right hand, n
(%) | 233 (50.32) | 87 (51.18) |
| Left hand, n (%) | 232 (49.68) | 83 (48.82) |
| Dominant side number,
n (%) | 234 (50.54) | 81 (47.65) |
| Non-dominant side
number, n (%) | 231 (49.46) | 89 (52.35) |
| Table IIIThe sensitivity, specificity, positive
predictive value, negative predictive value, positive likelihood
rate and negative likelihood rate of the physical tests. |
Table III
The sensitivity, specificity, positive
predictive value, negative predictive value, positive likelihood
rate and negative likelihood rate of the physical tests.
| Test | Sensitivity (%) | Specificity (%) | Positive predictive
value (%) | Negative predictive
value (%) | LR+ | LR- |
|---|
| Tinel's test | 41.94 | 77.06 | 83.33 | 32.67 | 1.83 | 0.75 |
| Phalen's test | 56.13 | 73.53 | 85.29 | 37.99 | 2.12 | 0.60 |
| Reverse Phalen's
test | 55.27 | 78.82 | 87.71 | 39.18 | 2.61 | 0.57 |
| SCT | 67.74 | 71.76 | 86.78 | 44.85 | 2.40 | 0.45 |
| Hand elevation
test | 75.48 | 60.59 | 83.97 | 47.47 | 1.92 | 0.40 |
To compare the sensitivity and specificity of each
test, the Chi-squared test was used between each pair of tests
(Tables IV and V). The results revealed that all test
pairs had significantly different sensitivities [P<0.0001 for
all, apart from the reverse Phalen's vs. Phalen's tests (P=0.79);
Table IV]. Based on the results
depicted in Table III, the
sensitivities of the SCT and hand elevation test were significantly
higher than those of other traditional tests. Moreover, the
specificities between the hand elevation test and the other tests
were all significantly different (P=0.001 for the hand elevation
test vs. Tinel's test, P=0.0111 for the hand elevation test vs.
Phalen's test, P=0.0002 for the hand elevation test vs.
reverse-Phalen's test and P=0.0294 for the hand elevation test vs.
SCT); however, the specificities between the Tinel's test, Phalen's
test, reverse Phalen's test and SCT did not differ significantly
(P=0.45 for Tinel's test vs. Phalen's test, P=0.69 for Tinel's test
vs. reverse-Phalen's test, P=0.25 for Phalen's test vs.
reverse-Phalen's test, P=0.26 for SCT vs. Tinel's test, P=0.72 for
SCT vs. Phalen's test and P=0.13 for SCT vs. reverse-Phalen's test)
(Table V). Based on the results
depicted in Table III, the
specificity of the SCT was lower than that of the other traditional
tests, although no significant difference was observed.
Furthermore, the specificity of the hand elevation test was
significantly lower than that of the traditional tests.
| Table IVP-values of the Chi-squared test and
results of the sensitivity of the physical tests. |
Table IV
P-values of the Chi-squared test and
results of the sensitivity of the physical tests.
| Test | Tinel's test | Phalen's test | Reverse Phalen's
test | SCT | Hand elevation
test |
|---|
| Tinel's test | / |
<0.0001a |
<0.0001a |
<0.0001a |
<0.0001a |
| Phalen's test | / | / | 0.79 | 0.0003a |
<0.0001a |
| Reverse Phalen's
test | / | / | / |
<0.0001a |
<0.0001a |
| SCT | / | / | / | / | 0.0088a |
| Hand elevation
test | / | / | / | / | / |
| Table VP-values of the Chi-squared test and
results of the specificity of the physical tests. |
Table V
P-values of the Chi-squared test and
results of the specificity of the physical tests.
| Test | Tinel's test | Phalen's test | Reverse Phalen's
test | SCT | Hand elevation
test |
|---|
| Tinel's test | / | 0.45 | 0.69 | 0.26 | 0.001a |
| Phalen's test | / | / | 0.25 | 0.72 | 0.0111a |
| Reverse-Phalen's
test | / | / | / | 0.13 | 0.0002a |
| SCT | / | / | / | / | 0.0294a |
| Hand elevation
test | / | / | / | / | / |
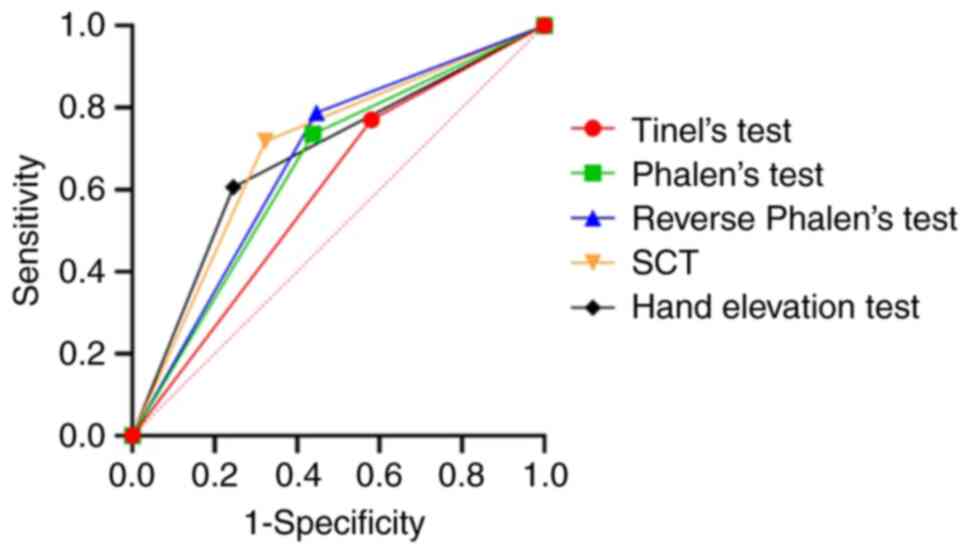
The area under the curve (AUC) of the ROC and 95%
confidence interval (CI) of the dichotomous physical tests are
presented in Fig. 1 and Table VI, respectively. The order of the
AUC was SCT > hand elevation test > reverse Phalen's test
> Phalen's test > Tinel's test.
| Table VIThe AUC of the ROC curve of the
physical tests. |
Table VI
The AUC of the ROC curve of the
physical tests.
| Test | AUC | 95% CI |
|---|
| Tinel's test | 0.5950 | 0.5468 | 0.6432 |
| Phalen's test | 0.6483 | 0.6011 | 0.6955 |
| Reverse Phalen's
test | 0.6705 | 0.6248 | 0.7161 |
| SCT | 0.6975 | 0.6513 | 0.7437 |
| Hand elevation
test | 0.6804 | 0.6317 | 0.7290 |
Discussion
In the present study, 236 patients with CTS (465
hands) and 96 controls (170 hands) were analyzed. Between these
groups, the number of right and left hands, as well as the dominant
and non-dominant sides were comparable. Therefore, the dominant
side was not a confounder in the present study and did not need to
be adjusted or set as a subgroup for analysis.
An ideal clinical diagnostic test should be easily
performed, reliable, reproducible and have high sensitivity and
specificity. Herein, five dichotomous tests used to diagnose CTS
were conducted, and their sensitivities and specificities were
compared. It was observed that the sensitivities of the SCT and
hand elevation test were significantly higher than those of the
traditional tests, and the specificity of the hand elevation test
was significantly lower than that of the traditional tests. From
the LR+ result, the SCT exhibited the highest diagnostic
accuracy, and from the LR- result, the hand elevation
test and SCT had high level ability to correctly exclude
individuals without CTS. The ROC AUC of the SCT and hand elevation
test were larger than those of the other tests, which shows that
these tests are valuable for the diagnosis of CTS.
SCT was considered positive if the patient
demonstrated a loss of resistance on the affected side after
‘scratching’, which is a more objective measure than the results of
the other four provocative tests (Tinel's, Phalen's, reverse
Phalen's and hand elevation tests) that rely on the patient's
subjective feeling. Scratching to stimulate the skin around the
area of nerve damage results in a short period of inhibition of
voluntary muscle activity, termed the ‘silent period’. This ‘silent
period’ can be tested by resisting the external rotation of the
shoulder (usually a weak movement), and if the movement is
suppressed, the examiner can break the external rotation (‘arm
collapse’) (16,18). This is probably mediated mainly by
the small-diameter slow-conducting A-δ fibers and could be an
inhibitory spinal reflex, possibly playing a protective role
(19,20). Therefore, the SCT is applied not
only to diagnose CTS, but also other nerve compression syndromes;
it can be used to indicate the location of nerve entrapment.
In previous studies on the application of SCT for
the diagnosis pf CTS, Cheng et al (16) reported a sensitivity and
specificity of 0.69 and 0.99 in 228 cases, Gillenwater et al
(21) reported 0.77 and 0.99 in 24
cases, Huynh et al (22)
performed a meta-analysis of Blok et al (23), Makanji et al (24) and Simon (25) et al who reported a
sensitivity and specificity of 0.32 and 1.00 in 37 cases, 0.34 and
0.61 in 88 cases, and 0.28 and 0.38 in 40 cases, respectively . The
sensitivity and specificity reported by Montgomery et al
(26) were 0.07-0.15 and 0.78-0.87
in 92 cases, respectively. Simon et al (25) reported a sensitivity and
specificity of 0.24 and 0.6 in a study comprising 40 cases. The
sensitivities and specificities of the aforementioned studies were
not consistent with those of the present study, which revealed
higher values. While the SCT provides an objective assessment,
performing it is more complex than the other tests, and the result
can be influenced by different operators (27). In the present study, all the tests
were conducted by the same evaluator who underwent a 2-year
training for hand surgery and was blinded to the patient histories
and diagnoses. On the other hand, the specificity observed in
previous studies may be overestimated.
Performing the hand elevation test is simple
compared to the SCT. Therefore, it is less dependent on the skills
of the examiners or compliance of the patients. Ischemia of the
median nerve has been recognized as one of the primary causes of
spontaneous compression neuropathy. Thickening of the flexor
synovialis leads to ischemia, which worsens median nerve edema. The
hand elevation test further reduces the blood supply to the already
compromised median nerve by transient ischemia, and thus,
reproduces the symptoms of CTS. From the comparison of the
sensitivity and specificity (0.7548 and 0.6059) of the hand
elevation test with that was observed in previous studies [Ahn
(17), 0.755 and 0.985 in 400
cases; Ma and Kim (28), 0.867 and
0.889 in 90 cases; and Amirfeyz et al (29), 0.88 and 0.98 in 60 cases,
respectively], it was found that the sensitivity was highly
consistent with that of the present study, although the specificity
was not. This indicates that the hand elevation test is
reproducible as a primary screening test. However, the small sample
size may affect the specificity.
Considering that the sensitivities of the SCT and
hand elevation test were significantly higher than those of the
other three tests, whereas the specificities were not, these two
examinations could be used as a primary screening test. Tinel's
test, reverse Phalen's test could be conducted subsequently for
exclusion.
The present study has some limitations which should
be mentioned: As there is no universally acknowledged diagnostic
reference standard for CTS, the present study used CTS-6 as gold
standard, which used the symptoms, history and physical
examinations to comprehensively evaluate CTS. As the CTS-6 contains
the Phalen's and Tinel's tests, the sensitivities and specificities
of these two tests would become higher due to the inner confounder.
Regardless, the sensitivity and specificity of SCT and the
sensitivity of the hand elevation test were still high, whereas the
specificity of hand elevation test was still acceptable.
In conclusion, SCT is an objective assessment of CTS
that is reliable and has a high sensitivity. Furthermore, the hand
elevation test is easy to perform, is reproducible, and has a high
sensitivity. Both tests may be valuable for the diagnosis of
CTS.
Acknowledgements
The corresponding author would like to thank Dr
Joideep Phadnis at Brighton and Sussex University Hospitals NHS
Trust who evoked her interest in conducting the study.
Funding
Funding: The present study was sponsored by the Natural Science
Foundation of China (grant nos. 81971150 and 81972122), the
Shanghai Municipal Key Clinical Specialty (grant no.
shslczdzk05601), the Research Projects of Shanghai Municipal
Commission of Health and Family Planning (grant no. 20184Y0368) and
Shanghai ‘Rising Stars of Medical Talent’ Youth Development Program
(Youth Medical Talents-Medical Imaging Practitioner Program).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JC collected and analyzed the patient data. TJ
performed the physical tests. JL and JR designed the study and JR
was a major contributor to the writing of the manuscript. AL
assisted in the analysis of the results. JC and JR confirm the
authenticity of all the raw data. All authors have read and
approved the final manuscript.
Ethics approval and consent to
participate
All procedures performed involving human
participants were in accordance with the ethical standards of The
Human Research Committee of Huashan hospital Fudan University
(KY2022-641) and with the 1964 Helsinki declaration and its later
amendments or comparable ethical standards. Written informed
consent was obtained from all individual participants included in
the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ibrahim I, Khan WS, Goddard N and Smitham
P: Carpal tunnel syndrome: A review of the recent literature. Open
Orthop J. 6:69–76. 2012.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Hanewinckel R, Ikram MA and Van Doorn PA:
Peripheral neuropathies. Handb Clin Neurol. 138:263–282.
2016.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Graham B, Peljovich AE, Afra R, Cho MS,
Gray R, Stephenson J, Gurman A, MacDermid J, Mlady G, Patel AT, et
al: The American Academy of Orthopaedic Surgeons Evidence-Based
Clinical Practice Guideline on: Management of carpal tunnel
syndrome. J Bone Joint Surg Am. 98:1750–1754. 2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Mondelli M, Giannini F and Giacchi M:
Carpal tunnel syndrome incidence in a general population.
Neurology. 58:289–294. 2002.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Atroshi I, Gummesson C, Johnsson R,
Ornstein E, Ranstam J and Rosen I: Prevalence of carpal tunnel
syndrome in a general population. JAMA. 282:153–158.
1999.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Hulkkonen S, Shiri R, Auvinen J, Miettunen
J, Karppinen J and Ryhanen J: Risk factors of hospitalization for
carpal tunnel syndrome among the general working population. Scand
J Work Environ Health. 46:43–49. 2020.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Paroski MW and Fine EJ: Sir James Paget
and the carpal tunnel syndrome. Neurology. 35(448)1985.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Jablecki CK, Andary MT, So YT, Wilkins DE
and Williams FH: Literature review of the usefulness of nerve
conduction studies and electromyography for the evaluation of
patients with carpal tunnel syndrome. AAEM Quality Assurance
Committee. Muscle Nerve. 16:1392–1414. 1993.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Campion D: Electrodiagnostic testing in
hand surgery. J Hand Surg Am. 21:947–956. 1996.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Stetson DS, Albers JW, Silverstein BA and
Wolfe RA: Effects of age, sex, and anthropometric factors on nerve
conduction measures. Muscle Nerve. 15:1095–1104. 1992.PubMed/NCBI View Article : Google Scholar
|
|
11
|
LaJoie AS, McCabe SJ, Thomas B and Edgell
SE: Determining the sensitivity and specificity of common
diagnostic tests for carpal tunnel syndrome using latent class
analysis. Plast Reconstr Surg. 116:502–507. 2005.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Ghasemi-Rad M, Nosair E, Vegh A, Mohammadi
A, Akkad A, Lesha E, Mohammadi MH, Sayed D, Davarian A,
Maleki-Miyandoab T and Hasan A: A handy review of carpal tunnel
syndrome: From anatomy to diagnosis and treatment. World J Radiol.
6:284–300. 2014.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Padua L, Coraci D, Erra C, Pazzaglia C,
Paolasso I, Loreti C, Caliandro P and Hobson-Webb LD: Carpal tunnel
syndrome: Clinical features, diagnosis, and management. Lancet
Neurol. 15:1273–1284. 2016.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Graham B, Regehr G, Naglie G and Wright
JG: Development and validation of diagnostic criteria for carpal
tunnel syndrome. J Hand Surg Am. 31:919–924. 2006.PubMed/NCBI
|
|
15
|
Phalen GS and Kendrick JI: Compression
neuropathy of the median nerve in the carpal tunnel. J Am Med
Assoc. 164:524–530. 1957.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Cheng CJ, Mackinnon-Patterson B, Beck JL
and Mackinnon SE: Scratch collapse test for evaluation of carpal
and cubital tunnel syndrome. J Hand Surg Am. 33:1518–1524.
2008.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Ahn DS: Hand elevation: A new test for
carpal tunnel syndrome. Ann Plast Surg. 46:120–124. 2001.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Uncini A, Kujirai T, Gluck B and Pullman
S: Silent period induced by cutaneous stimulation.
Electroencephalogr Clin Neurophysiol. 81:344–352. 1991.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Serrao M, Parisi L, Pierelli F and Rossi
P: Cutaneous afferents mediating the cutaneous silent period in the
upper limbs: Evidences for a role of low-threshold sensory fibres.
Clin Neurophysiol. 112:2007–2014. 2001.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Kofler M: Functional organization of
exteroceptive inhibition following nociceptive electrical fingertip
stimulation in humans. Clin Neurophysiol. 114:973–980.
2003.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Gillenwater J, Cheng J and Mackinnon SE:
Evaluation of the scratch collapse test in peroneal nerve
compression. Plast Reconstr Surg. 128:933–939. 2011.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Huynh MNQ, Karir A and Bennett A: Scratch
collapse test for carpal tunnel syndrome: A systematic review and
meta-analysis. Plast Reconstr Surg Glob Open.
6(e1933)2018.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Blok RD, Becker SJ and Ring DC: Diagnosis
of carpal tunnel syndrome: Interobserver reliability of the blinded
scratch-collapse test. J Hand Microsurg. 6:5–7. 2014.PubMed/NCBI View Article : Google Scholar
|
|
24
|
Makanji HS, Becker SJ, Mudgal CS, Jupiter
JB and Ring D: Evaluation of the scratch collapse test for the
diagnosis of carpal tunnel syndrome. J Hand Surg Eur Vol.
39:181–186. 2014.PubMed/NCBI View Article : Google Scholar
|
|
25
|
Simon J, Lutsky K, Maltenfort M and
Beredjiklian PK: The Accuracy of the scratch collapse test
performed by blinded examiners on patients with suspected carpal
tunnel syndrome assessed by electrodiagnostic studies. J Hand Surg
Am. 42:386.e1–e386.e5. 2017.PubMed/NCBI View Article : Google Scholar
|
|
26
|
Montgomery K, Wolff G and Boyd KU:
Evaluation of the scratch collapse test for carpal and cubital
tunnel syndrome-a prospective, blinded study. J Hand Surg Am.
45:512–517. 2020.PubMed/NCBI View Article : Google Scholar
|
|
27
|
Cebron U and Curtin CM: The scratch
collapse test: A systematic review. J Plast Reconstr Aesthet Surg.
71:1693–1703. 2018.PubMed/NCBI View Article : Google Scholar
|
|
28
|
Ma H and Kim I: The diagnostic assessment
of hand elevation test in carpal tunnel syndrome. J Korean
Neurosurg Soc. 52:472–475. 2012.PubMed/NCBI View Article : Google Scholar
|
|
29
|
Amirfeyz R, Gozzard C and Leslie IJ: Hand
elevation test for assessment of carpal tunnel syndrome. J Hand
Surg Br. 30:361–364. 2005.PubMed/NCBI View Article : Google Scholar
|