Introduction
Papillary thyroid carcinoma (PTC) is the most
commonly occurring type of thyroid cancer, accounting for >80%
of all thyroid malignancies. Typically, PTC is associated with a
favorable prognosis and a slow progression. Although uncommon, PTC
can exhibit an aggressive behavior, such as invading the vascular
system and extending into the major vessels (1). PTC occurs two- to four-fold more
frequently in women than in men. It can exhibit a wide range of
gross morphologic appearances, and the tumors may arise in any
region of the thyroid gland (2).
In a normal thyroid gland, the squamous epithelium is absent;
therefore, the presence of squamous epithelial cells is considered
unusual. Squamous differentiation in a thyroid tumor denotes a
well-differentiated carcinoma, such as PTC, that exhibits areas of
squamous differentiation without any anaplastic or poorly
differentiated features (3). This
may occur, for instance, when well-differentiated thyroid
carcinomas such as PTC, particularly the tall cell variant, undergo
further differentiation (4). While
PTC is frequently associated with focal or extensive squamous
metaplasia in ~20-40% of cases, the occurrence of true squamous
differentiation within PTC is exceedingly rare (3). These rare variants of thyroid
malignancy tend to exhibit an aggressive clinical behavior, and
their prognostic outcomes remain poorly understood (5). The present study reports two cases of
PTC with squamous differentiation (PTC-SD). In accordance with the
CaReL guidelines, a brief literature review was also included in
the present study, and all references have been checked to ensure
no content was cited from blacklisted journals (6,7). The
literature search was conducted on Google Scholar using the keyword
‘allintitle: squamous AND thyroid AND carcinoma AND papillary’.
Case report
Case one. Patient information
On December 1, 2024, a 28-year-old female patient
presented to Smart Health Tower (Sulaymaniyah, Iraq) with a neck
mass and hoarseness. An analysis of her medical history did not
reveal any notable findings, apart from a prior cesarean section.
She had no family history of thyroid disease or malignancy.
Clinical findings. A physical examination
revealed a firm, non-tender grade I goiter without any other
abnormalities.
Diagnostic approach. An ultrasonography of
the thyroid revealed scattered microcalcifications in the lower
third of the right lobe. Additionally, a solid hypoechoic nodule
with an irregular surface, measuring 16x14x12 mm, was observed in
the middle to lower third of the left lobe (data not shown). It
contained both micro- and macrocalcifications, increased
perinodular and intranodular vascularity, and was classified as
TR5. Multiple small lymph nodes (LNs) were observed around the
gland, predominantly on the left side. The largest, measuring 10x7
mm, was located below the lower pole of the left lobe and appeared
highly suspicious. Furthermore, a few left-sided cervical LNs were
noted, with the largest measuring 6x3 mm in the left group III. A
suspicious LN, measuring 5.6x3.7 mm, was identified in the left
group IV, located behind the distal left jugular vein. The patient
subsequently underwent fine needle aspiration cytology, which
yielded a Bethesda II result (data not shown).
Therapeutic intervention. A total
thyroidectomy with left lateral and central neck dissection was
performed through a collar incision. Both recurrent laryngeal
nerves and parathyroid glands were carefully preserved. Hemostasis
was achieved, and the wound was closed in layers with a left-sided
drain. A histopathological examination of the surgical specimen was
performed by the hospital laboratory. This was performed on
5-µm-thick paraffin-embedded sections. The sections were fixed in
10% neutral buffered formalin at room temperature for 24 h and
stained with hematoxylin and eosin (Bio Optica Co.) for 1-2 min at
room temperature. The sections were then observed under a light
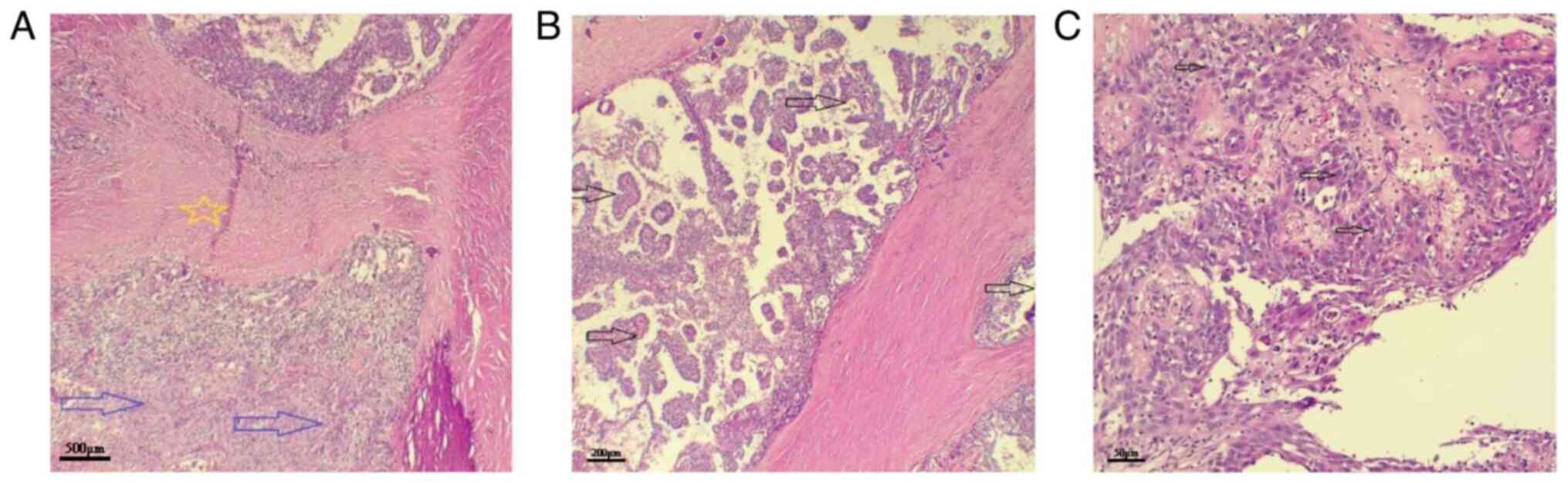
microscope (Leica Microsystems GmbH). The histopathological
examination revealed papillary formations lined by thyroid
follicular cells that had elongated, crowded, and cleared nuclei
with crowding, grooves and pseudoinclusions. Separated by areas of
fibrosis, parts of the tumor were composed of larger cells with an
abundant eosinophilic cytoplasm and squamous differentiation. These
features were indicative of PTC-SD (Fig. 1). Out of the 34 LNs examined, six
were involved by the papillary component of the tumor, four of
which were from the central compartment, and two from the lateral
compartment. Immunohistochemistry (IHC) was performed as follows:
The paraffin blocks were cut into 4-6-µm-thick sections and
transferred onto charged glass slides. Subsequently, they were
placed in an oven at 60˚C overnight. Antigen retrieval was
performed using the Dako PT Link (Agilent Technologies, Inc.) by
boiling the sections at 100˚C for 5 to 10 min. A solution of pH 6.0
or pH 9.0 was used for the target antibody. The slides were then
subjected to a 15-min wash with a 20 ml buffer solution (0.05 mol/l
Tris/HCl, 0.15 mol/l NaCl, 0.05% Tween-20, pH 7.6) at room
temperature. To facilitate the process, the slides were welled
using the Dako Pen (Agilent Technologies, Inc.). Furthermore,
endogenous peroxidase was blocked using 3% hydrogen peroxide.
Subsequently, the primary antibodies [CK5/6 (1:100, mouse
monoclonal, clone D5/16 B4, cat. no. M7237), p40 (1:100, mouse
monoclonal, clone BC28, cat. no. M7317) and TTF-1 (1:100, mouse
monoclonal, clone 8G7G3/1, cat. no. M3575) all form Dako; Agilent
Technologies, Inc.] were applied at room temperature and left for
80 min. The secondary antibody, which was horseradish
peroxidase-conjugated (1:200, cat. no. P0447, Dako; Agilent
Technologies, Inc.) was then applied, along with the chromogen
(diaminobenzidine) (MilliporeSigma), both at room temperature for
15 min. To achieve counterstaining, hematoxylin Gill II (Thermo
Fisher Scientific, Inc.) was applied at room temperature for a
duration of 30 sec. The slides were dried and coverslips were
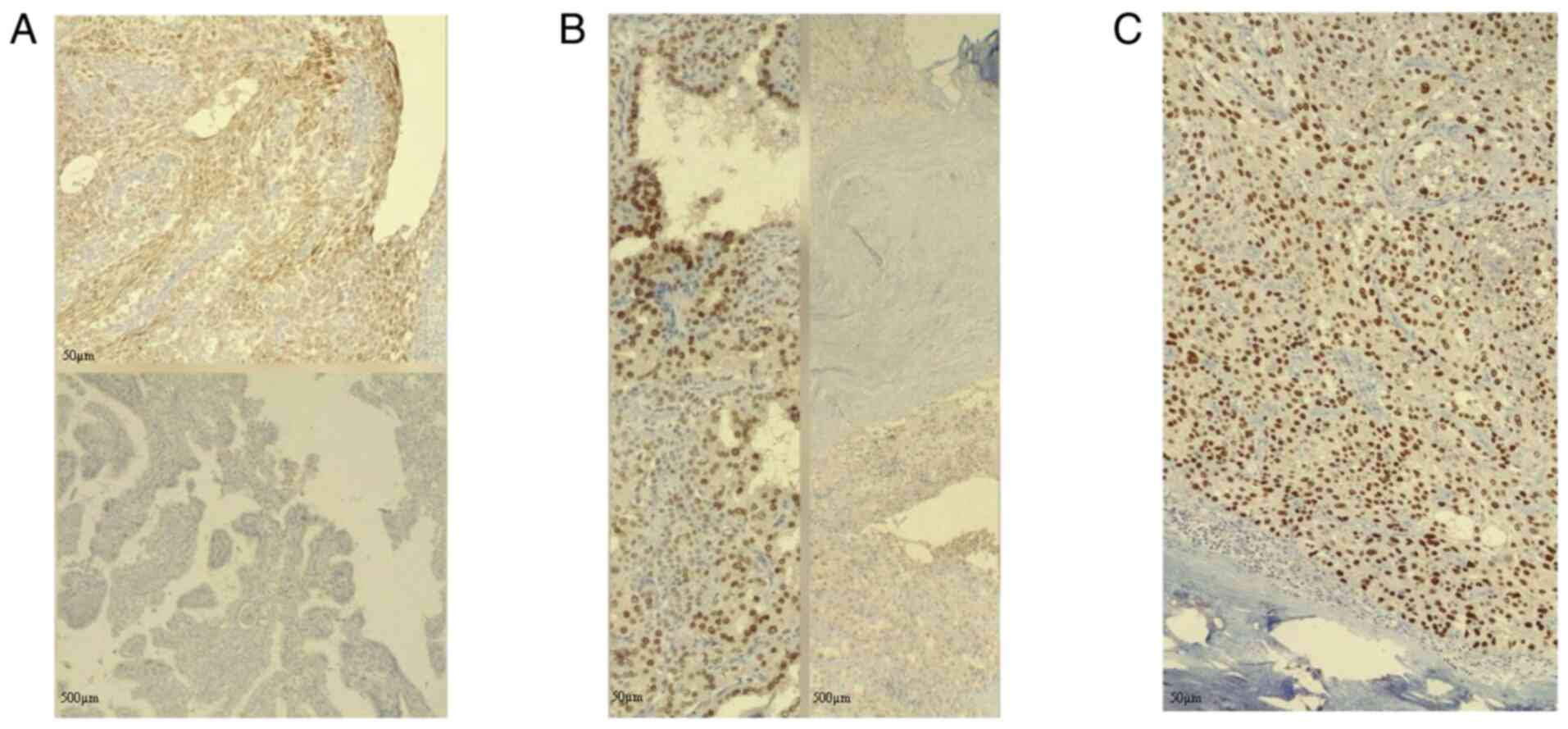
applied. IHC revealed the positive staining of the squamous areas
for CK5/6 and p40, with negative staining for TTF-1, whereas the
conventional papillary areas showed the opposite staining patterns
(Fig. 2).
Follow-up and outcome. The post-operative
period was uneventful, and levothyroxine (100 mg daily) was
prescribed. Subsequently, the patient was referred for radioactive
iodine ablation. Following the ablation, thyroglobulin levels
decreased to <0.04, indicating a favorable response. The patient
condition was in a good at 3-months of follow up.
Case two. Patient information
A 49-year-old male patient was being treated for a
dental issue when, during an unrelated neck ultrasound, a
suspicious thyroid lesion was incidentally discovered. The patient
was referred to Smart Health Tower on October 22, 2024. The
analysis of the past medical and family history of the patient
yielded negative results for any thyroid disease.
Clinical findings. Upon a physical
examination of the cervical region, there was no palpable mass.
Diagnostic approach
The patient was euthyroid, with the following
laboratory results: Thyroid-stimulating hormone level of 1.58 mIU/l
(normal range, 0.4-4.0 mIU/l) and free FT4 level of 18.0 pmol/l
(normal range, 12.0-22.0 pmol/l). An ultrasonography of the neck
revealed a well-defined hypoechoic nodule in the mid-upper third of
the right thyroid lobe (14x10x8 mm) classified as TR3, and a
smaller nodule in the lower third of the left lobe (6x5x5 mm),
classified as TR1 (image was not archived). Both thyroid lobes were
normal in size, with a homogeneous echotexture and normal
vascularity. No marked cervical pathological lymphadenopathy was
detected, and the submandibular and parotid glands appeared normal
with no focal lesions. Due to the right mid-upper lobe nodule,
further evaluation included serum calcitonin, which was normal
(8.99 pg/ml), and ultrasound-guided fine-needle aspiration of the
TR3 nodule, which yielded a Bethesda VI result, highly suspicious
for malignancy.
Therapeutic intervention. Pre-operatively,
the patient underwent an evaluation, which revealed normal
bilateral vocal cord function and normal serum calcium levels (9.16
mg/dl). Thyroglobulin was measured at 33.2 ng/ml for baseline
assessment. The patient underwent a total thyroidectomy. A
histopathological examination specimen was performed by the
hospital laboratory. This was performed on 5-µm-thick
paraffin-embedded sections. The sections were fixed in 10% neutral
buffered formalin at room temperature for 24 h and stained with
hematoxylin and eosin (Bio Optica Co.) for 1-2 min at room
temperature. The sections were then observed under a light
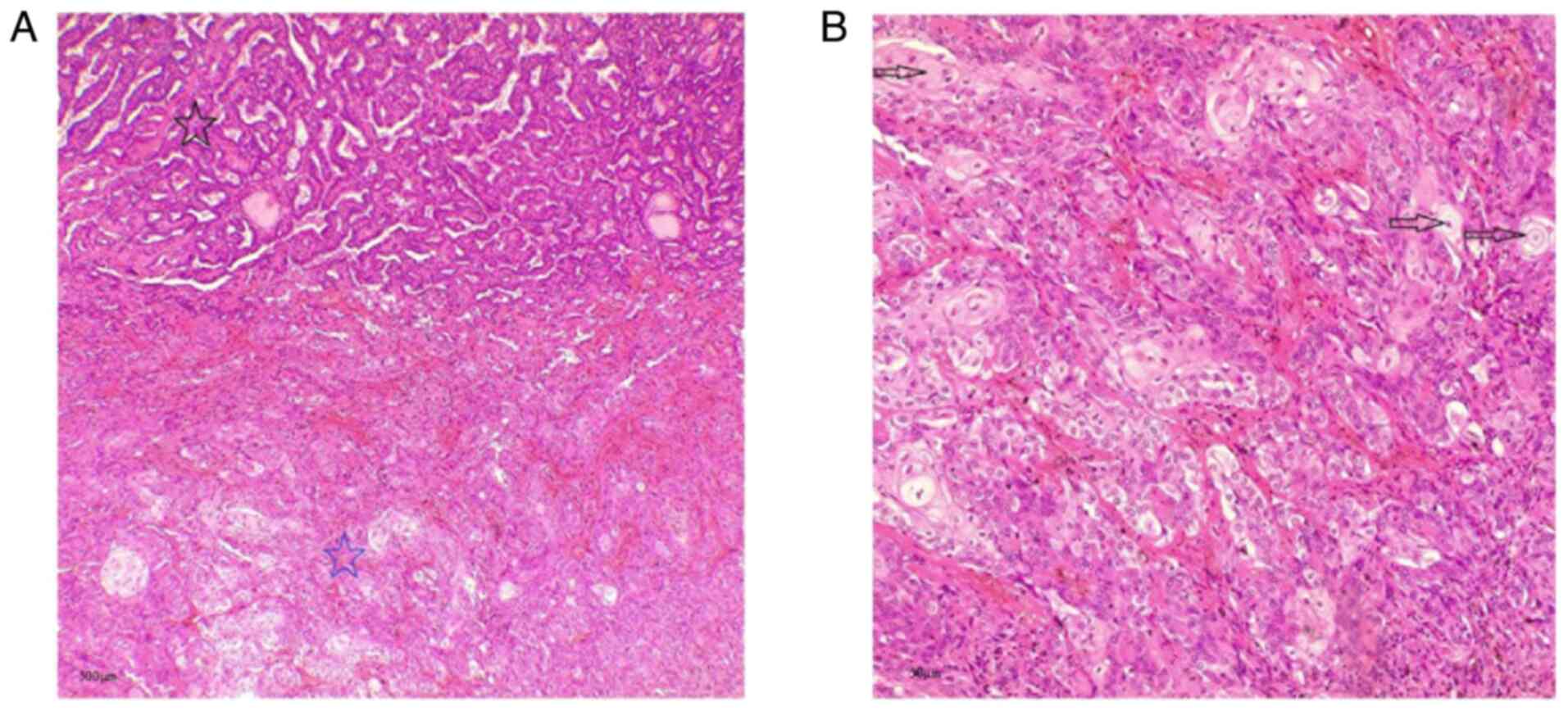
microscope (Leica Microsystems GmbH). The histopathological
examination revealed a unifocal, unencapsulated PTC-SD (Fig. 3) in the right lobe, measuring 1.2
cm, comprising areas of conventional PTC, as well as areas of
squamous differentiation without anaplastic dedifferentiation or
high-grade features (increased mitotic activity or necrosis). There
was no evidence of lympho-vascular invasion, perineural invasion,
or extrathyroidal extension. The background parenchyma showed
thyroid follicular nodule disease. A total of five LNs were
isolated, and all were tumor-free.
Follow-up and outcome. Post-operatively, the
patient remained stable with no complications and began receiving
levothyroxine. Serum calcium levels remained within the normal
range (9.45 mg/dl), and thyroglobulin decreased to 0.338 ng/ml. The
patient was scheduled for further follow-up. At 3-months of follow
up, the condition of the patient was stable.
Discussion
The presence of squamous epithelium in the thyroid
can result from various causes, including primary thyroidal
squamous cell carcinoma (SCC), benign squamous metaplasia in
conditions such as nodular goiter or lymphocytic thyroiditis, SCC
arising through dedifferentiation in recurrent thyroid cancers
often with anaplastic features, thymus-like differentiation in a
cancer, metastasis from a squamous carcinoma elsewhere, or a
typical PTC undergoing squamous differentiation at initial
diagnosis (3). Anaplastic
carcinomas may sometimes exhibit focal squamous differentiation on
histological examination. However, they are typically
non-keratinizing and poorly differentiated, displaying marked
pleomorphism along with classic anaplastic features, such as
spindle cell and giant cell components, unlike PTC-SD (8,9).
Squamous differentiation in PTC is considered to
develop either through the metaplastic reprogramming of thyroid
follicular cells or via a multistep dedifferentiation of the
original tumor clone. Chronic inflammation may promote metaplasia,
as observed in thyroid cancers and Hashimoto's thyroiditis, which
often co-express the squamous transcription factor p63(10). Similarly, Ding et al
(11) reported cases in which
Hashimoto's foci adjacent to PTC exhibited squamous metaplastic
changes. Other studies support a clonal progression toward a
squamous phenotype. Thewjitcharoen et al (12) described a metastatic case
exhibiting intermixed classical PTC and poorly differentiated
squamous cells sharing thyroid markers (PAX8 and CK19), while only
the squamous component was CK5/6-positive, indicating a common
origin. Handra-Luca (13) likewise
observed PTC metastases, in which p63-positive papillary epithelium
gave rise to CK5/6-positive squamous cells, suggesting the
activation of a latent squamous differentiation program. On a
molecular level, the progression from PTC to squamous morphology
parallels anaplastic transformation, with tumors typically
harboring early MAPK pathway mutations (BRAF or RAS) alongside
additional alterations, such as TP53 and TERT promoter mutations
and CDKN2A loss (11). Advanced
primary cancers from nearby components, such as the larynx, base of
the tongue, upper esophagus, or pharynx, can directly extend into
the thyroid gland. Although the thyroid has an extensive blood
supply, metastases to the thyroid are uncommon, representing only
2-3% of all cancerous thyroid tumors, with SCC comprising only a
small portion of these cases (8).
Due to their varied clinical and biological characteristics, it is
crucial to distinguish PTC-SD from other conditions that involve
squamous epithelium in a thyroid specimen (3). Even though PTC generally has a
favorable prognosis, with an >90% survival rate at 20 years,
several variables can negatively impact the outlook. These include
being >45 years of age at diagnosis, incomplete surgical
removal, large tumors, an advanced stage, the presence of
metastasis, specific histological variants such as columnar, tall
cell and diffuse sclerosing types, as well as evidence of local
tissue invasion (3). Squamous
cells of the thyroid are documented in connection with the tall
cell variant of PTC. This variant is generally larger than the
classic form, tends to arise in older individuals, and is
associated with a more aggressive clinical behavior. The observed
link between the tall cell variant and squamous differentiation
implies a potential histopathological relationship in the
progression of thyroid cancer (9).
However, the tall cell variant PTC was not present in the cases
described herein.
In the present study, four cases of PTC-SD were
reviewed in the literature (3,9,13,14).
Although the sample size in these studies was small, the findings
suggested a poorer outcome than conventional PTC, with 1 patient
succumbing to the disease and another developing a recurrent lesion
in the left clavicle (Table I).
IHC examinations were performed in all the cases to determine
origin of the tumor, which assisted in the differential diagnosis.
Beninato et al (5) reviewed
patients with PTC-SD identified either during lymph node dissection
for recurrent disease or at initial total thyroidectomy from a
single-center cancer registry (1995-2015) and identified only 10
cases. A total of 4 patients had PTC-SD metastases detected during
surgery for recurrence, while 6 patients exhibited PTC-SD in
primary tumor specimens at an initial thyroidectomy. Despite the
small sample size, their findings suggested that this variant
represents an aggressive form of thyroid carcinoma (5). Similarly, Ito et al (4) identified only 10 patients with PTC
containing squamous components among 5,749 cases evaluated between
2006 and 2010, accounting for 0.2% and confirming its rarity. The
atypical behavior of PTC is frequently observed in elderly patients
who demonstrate rapid disease progression. Accordingly, cases of
PTC with squamous differentiation are also commonly reported in
older individuals (3). In the
study by Beninato et al (5), at least half of the PTC-SD cases
demonstrated multifocal tumors, extrathyroidal extension and lymph
node metastases with extranodal spread. Moreover, all patients
exhibited tumor involvement at the inked surgical margins (5).
 | Table IReview of four cases of papillary
thyroid carcinoma with squamous differentiation identified in the
literature. |
Table I
Review of four cases of papillary
thyroid carcinoma with squamous differentiation identified in the
literature.
| First author, year of
publication | Age, years | Sex | Clinical finding | Imaging | Histopathological and
Immunohistochemical examinations | Fine needle
aspiration | Molecular
examinations | Treatment | Postoperative
treatment | Outcome | (Refs.) |
|---|
| Sheta, 2023 | 30 | M | Left-sided neck
swelling | US: Thyroidal
homogeneous echo-texture, solitary thyroid nodule | HPE: PTC and
malignant squamous epithelial cells, psammoma bodies. IHC: +ve
CK5/6 and Tg | Suspicious for PTC
and staged as Bethesda V | Not mentioned | Total thyroidectomy,
axillo-bilateral breast approach | Not mentioned | Stable condition | (3) |
| Dennis, 2018 | 65 | F | Fluctuant left-sided
neck mass | None | IHC: +ve p63, CK5/6
and BRAF V600E, -ve TTF-1 and Tg. HPE: Admixed PTC and squamous
cells | Brightly eosinophilic
cells with squamoid features | Not mentioned | Surgical
resection | Chemoradiation
(carboplatin and taxol), and radioactive iodine ablation | Left clavicular
lesion 2 months later | (9) |
| Grove, 2018 | 68 | M | Neck mass, history of
PTC | Unknown | IHC: +ve CK5/6, P63,
and PAX8 | Keratinizing squamous
cells, papillary follicular cells, amongst malignant squamous
cells | Not mentioned | Total
laryngectomy | Not mentioned | Deceased | (14) |
| Handra-Luca,
2018 | 21 | F | Neck mass | None | HPE: multifocal
thyroiditis and a neck thymus parathyroid unit. IHC: +ve P63, TTF1
Tg, and B-Raf in thyroid PTC, the same plus Ck5/6 in LN squamous
differentiation | Not mentioned | Not mentioned | Total thyroidectomy
with neck lymph node dissection | Radioactive iodide
& substitutive thyroid hormones | Stable condition | (13) |
IHC analysis with markers specific for thyroidal and
squamous differentiation aids diagnosis by demonstrating the
characteristic biphasic pattern (3). Handra-Luca (13) reported a case of a 21-year-old
patient with a neck mass who underwent total thyroidectomy with LN
dissection. The thyroid tumor was identified as bilateral PTC. IHC
analysis revealed focal p63 expression, diffuse TTF-1 positivity,
and the presence of thyroglobulin and B-Raf. Notably, squamous
differentiation was detected in 15 of the 19 metastatic lymph
nodes, with positive staining for CK5/6, p63, TTF-1, thyroglobulin
and B-Raf, indicating squamous differentiation arising from PTC
metastases (13). In the present
study, in the first reported case, IHC revealed positive staining
of the squamous areas for CK5/6 and p40, with negative staining for
TTF-1.
The morphological features of PTC-SD and its
potential occurrence at metastatic sites can make distinguishing
between squamous metaplasia and true squamous differentiation
difficult when based solely on histology. The detection of BRAF
mutations can serve as a valuable tool in excluding metastatic SCC
(13). Negative molecular
prognostic indicators include TERT promoter mutations and the
coexistence of multiple concurrent mutations, while the prognostic
significance of the BRAFV600E mutation remains controversial
(3). Although the incidence of
well-differentiated thyroid cancer is increasing and overall
survival remains high, supporting more conservative surgical and
adjuvant approaches, certain subtypes are associated with a poorer
prognosis and require timely identification and aggressive
management. Patients with PTC-SD should undergo careful, lifelong
monitoring and, in the absence of a specific treatment protocol,
should be managed according to established evidence-based
guidelines for high-risk thyroid cancers (5). The majority of reported cases in the
literature underwent surgical resection, often followed by
post-operative radioactive iodine ablation (5,9). The
main limitations of the present case report include the lack of
molecular testing due to the high cost for patients and the
inability to retrieve preoperative ultrasound image data, cell
counts, and nuclear characteristics. A minor limitation is the lack
of an IHC control sample.
In conclusion, clinicians should consider the
possibility of squamous differentiation in PTC, despite its rarity.
Hence, recognizing this variant is crucial for accurate diagnosis
and appropriate treatment planning.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
FHK and AMS were major contributors to the
conception of the study, as well as to the literature search for
related studies. HAA, AAQ and RMA contributed to the clinical
management of the patients, assisted in data acquisition and
interpretation, and participated in the literature review and
manuscript preparation. HAY and TOS contributed to the conception
and design of the study, in the literature review, in the critical
revision of the manuscript, and in the processing of the table. IJH
and SHH assisted in the diagnosis and management of the patients
and participated in manuscript review. AMA was the pathologist who
performed the diagnoses. FHK and AMS confirm the authenticity of
all the raw data. All authors have read and approved the final
manuscript.
Ethics approval and consent to
participate
Written informed consent was obtained from the
patients for participation in the present study.
Patient consent for publication
Written informed consent was obtained from the
patients for the publication of the present case report and any
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Adnan Z, Sabo E and Kassem S: Metastatic
papillary thyroid carcinoma with internal jugular vein tumor
thrombus-A case report and review of the literature. Front
Endocrinol (Lausanne). 16(1505800)2025.PubMed/NCBI View Article : Google Scholar
|
|
2
|
LiVolsi VA: Papillary thyroid carcinoma:
An update. Mod Pathol. 24 (Suppl 2):S1–S9. 2011.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Sheta H, Abd El Hafez A, Harb D, Zuhdy M
and Elzahaby IA: A Rare Entity: Papillary thyroid carcinoma with
squamous differentiation diagnosed in a middle-aged man following
endoscopic total thyroidectomy via axillo-bilateral breast
approach. Middle East J Cancer. 14:170–175. 2023.
|
|
4
|
Ito Y, Hirokawa M, Higashiyama T, Kihara
M, Tomoda C, Takamura Y, Kobayashi K, Miya A and Miyauchi A:
Biological behavior of papillary carcinoma of the thyroid including
squamous cell carcinoma components and prognosis of patients who
underwent locally curative surgery. J Thyroid Res.
2012(230283)2012.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Beninato T, Kluijfhout WP, Drake FT,
Khanafshar E, Gosnell JE, Shen WT, Duh QY and Suh I: Squamous
differentiation in papillary thyroid carcinoma: A rare feature of
aggressive disease. J Surg Res. 223:39–45. 2018.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Abdullah HO, Abdalla BA, Kakamad FH, Ahmed
JO, Baba HO, Hassan MN, Bapir R, Rahim HM, Omar DA, Kakamad SH, et
al: Predatory publishing lists: A review on the ongoing battle
against fraudulent actions. Barw Med J. 2:26–30. 2024.
|
|
7
|
Prasad S, Nassar M, Azzam AY, José FG,
Jamee M, Sliman RKA, Evola G, Mustafa AM, Abdullah HO, Abdalla BA,
et al: CaReL guidelines: A consensus-based guideline on case
reports and literature review (CaReL). Barw Med J. 2:13–19.
2024.
|
|
8
|
Syed MI, Stewart M, Syed S, Dahill S,
Adams C, McLellan DR and Clark LJ: Squamous cell carcinoma of the
thyroid gland: Primary or secondary disease? J Laryngol Otol.
125:3–9. 2011.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Dennis K, O'Neil M and Harrington A: Not
all neck mass fine-needle aspirations with squamous cells are
squamous cell carcinoma; Report of a case of recurrent thyroid
carcinoma with papillary and squamous components. Cytojournal.
15(23)2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Unger P, Ewart M, Wang BY, Gan LI, Kohtz
DS and Burstein DE: Expression of p63 in papillary thyroid
carcinoma and in Hashimoto's thyroiditis: A pathobiologic link? Hum
Pathol. 34:764–769. 2003.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Ding W, Gao X and Ran X: Progress in
diagnosing and treating thyroid squamous cell carcinoma under the
5th edition of WHO classification. Front Endocrinol (Lausanne).
14(1273472)2024.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Thewjitcharoen Y, Krittiyawong S, Butadej
S, Nakasatien S, Polchart S, Junyangdikul P, Kanchanapituk A and
Himathongkam T: De-differentiation of papillary thyroid carcinoma
into squamous cell carcinoma in an elderly patient: A case report.
Medicine (Baltimore). 99(e19892)2020.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Handra-Luca A: Squamous cell
differentiation in metastatic papillary thyroid carcinoma:
metaplastic reversion or progression? Iran J Pathol.
13(276)2018.PubMed/NCBI
|
|
14
|
Grove N, Hartenstine J and Gallegos N: 81
potential pitfall: Papillary thyroid carcinoma mimicking squamous
cell carcinoma. Am J Clin Pathol. 149 (Suppl 1)(S35)2018.
|