Introduction
Acute lower gastrointestinal bleeding (ALGIB) is a
common cause of hospital admission, with rectal bleeding being the
most frequent presentation (1).
Australia's most extensive cohort study of lower gastrointestinal
(LGI) bleeding demonstrated that 0.05% of patients >70 would
have clinically significant bleeding during 4 years of prospective
follow-up (2). The management of
these presentations is often resource-intensive, with treatment
ranging from blood transfusions to endoscopy, radiological
intervention and surgery. LGI endoscopy serves both diagnostic and
therapeutic roles in patients with ALGIB.
Guidelines for the treatment of ALGIB have been
published in the USA (3), Europe
(4,5) and Asia (6); however, no consensus exists on the
ideal time required to perform an endoscopy. The American College
of Gastroenterology and the American Society for Gastrointestinal
Endoscopy recommend performing a colonoscopy within 24 h of
presentation in patients with high-risk features and ongoing
bleeding, and as an inpatient for low-risk patients (3), while the British Society of
Gastroenterology (4) and the
European Society of Gastrointestinal Endoscopy (5) do not recommend urgent colonoscopy
(<24 h) for patients with ALGIB and outpatient investigations
for minor self-limiting bleeding as part of the usual clinical
practice. As per the Japan Gastroenterological Association, the
conduct of a colonoscopy within 24 h is recommended to identify the
source of bleeding and the therapeutic intervention (6).
Several randomized controlled trials have compared
early colonoscopy with elective colonoscopy and have shown that
performing an early (≤24 h) colonoscopy does not improve the
diagnostic yield or reduce re-bleeding or mortality (7,8).
However, an urgent colonoscopy increases the detection rate of
signs of recent bleeding (8).
In Australia, a lack of published local data has
been reported on the burden of LGIB on emergency department
presentations or overall hospital admissions. In addition, no
published national guidelines advocate the use of LGI endoscopy in
the setting of ALGIB, and the optimal timing of colonoscopy for
patients with ALGIB remains uncertain. It is essential to examine
whether colonoscopy needs to be performed as an emergency
procedure, for instance, during hospitalization, or whether it can
be conducted as an outpatient procedure without causing any
disadvantage to the patient.
Patients taking antiplatelet and/or anticoagulant
medications are considered high-risk, and early endoscopy is
recommended for them (2,3,9).
However, it is still unclear whether endoscopy should be performed
during hospitalization and whether it has an impact on readmission.
In the present study, it was hypothesized that the use of a patient
database could clarify the effectiveness of LGI endoscopy by
examining the readmission rates among patients receiving
antiplatelet and/or anticoagulant medications, with or without LGI
endoscopy. The primary aim of the present study was to evaluate the
role of inpatient endoscopies for patients presenting with ALGIB
and their impact on re-admissions. The secondary aim included the
comparison of re-admission rates in patients using or not using
anticoagulants and/or antiplatelets and identifying risk
factors.
Patients and methods
Patients and study design
The present single-center, retrospective cohort
study was conducted in the Colorectal Unit at Monash Health,
Melbourne, Australia. All patients aged ≥18 years with an admission
coded as ‘per-rectal bleeding’ under the Colorectal Unit >5
years from January 1, 2014 to December 31, 2018, were included in
the study. Demographic data, anticoagulant and antiplatelet use,
LGI endoscopy findings and computed tomography angiography
investigations, interventions, diagnoses and inpatient readmission
to the hospital with ‘per-rectal bleeding’ within 6 months of
discharge were extracted from patient records. Patients deemed
medically unfit to have an inpatient or outpatient LGI endoscopy
were excluded.
Outcome
The primary outcome was the number of readmissions
and a 6-month readmission rate. In the subgroup analyses, the
predictors of readmission were identified in patients presenting
with ALGIB.
Statistical analysis
All statistical analyses were conducted using R
(version 4.4.2). A descriptive summary of readmission within
6-month rates was performed using the Chi-squared test or Fisher's
exact test (for cases, where the Chi-squared test's assumptions are
not reached) for categorical variables. Subsequent baseline
characteristics of the patients who underwent inpatient LGI
endoscopy compared with those who did not, stratified by use of
antiplatelet or anticoagulants, were analyzed using the standard
Wilcoxon rank-sum test for continuous variables and either the
Chi-squared test or Fisher's exact test (as above) for categorical
variables. To identify risk factors associated with 6-month
readmission due to bleeding, both univariate and multivariate
logistic regression analyses were performed. The significance for
the multivariate model was set at P<0.05. The results of these
analyses are presented side-by-side as odds ratios (ORs), 95%
confidence intervals (CIs) and P-values.
To minimize selection bias, propensity score
matching (PSM) was conducted to balance the baseline
characteristics between the LGI endoscopy and the non-LGI endoscopy
groups; results are described in the text rather than shown
graphically. The propensity score was estimated using logistic
regression while adjusting for age, sex, unstable vital signs, the
requirement for blood transfusion, antiplatelet and/or
anticoagulant use and the requirement for computerized tomography
angiographic embolization. The estimated propensity scores were
subsequently used to match treated and control patients. The
logit-transformed score was used in certain analyses to ensure
linearity, where the logit(p) is the natural log of the odds of
receiving treatment. Matching was performed using a 1:1 nearest
neighbor algorithm with a caliper width of 0.2. The caliper width
of 0.2 was selected as it represents the conventional threshold
(0.2 x standard deviation of the logit of the propensity score)
recommended by Austin (2011) (10)
to optimize bias-variance trade-off. Following matching, the
treatment and control groups were well-balanced on the baseline
characteristics. The final matched dataset included 117 patients
who underwent LGI endoscopy and 117 patients who did not. In all
statistical analyses, values of P<0.05 were considered to
indicate statistically significant differences.
Results
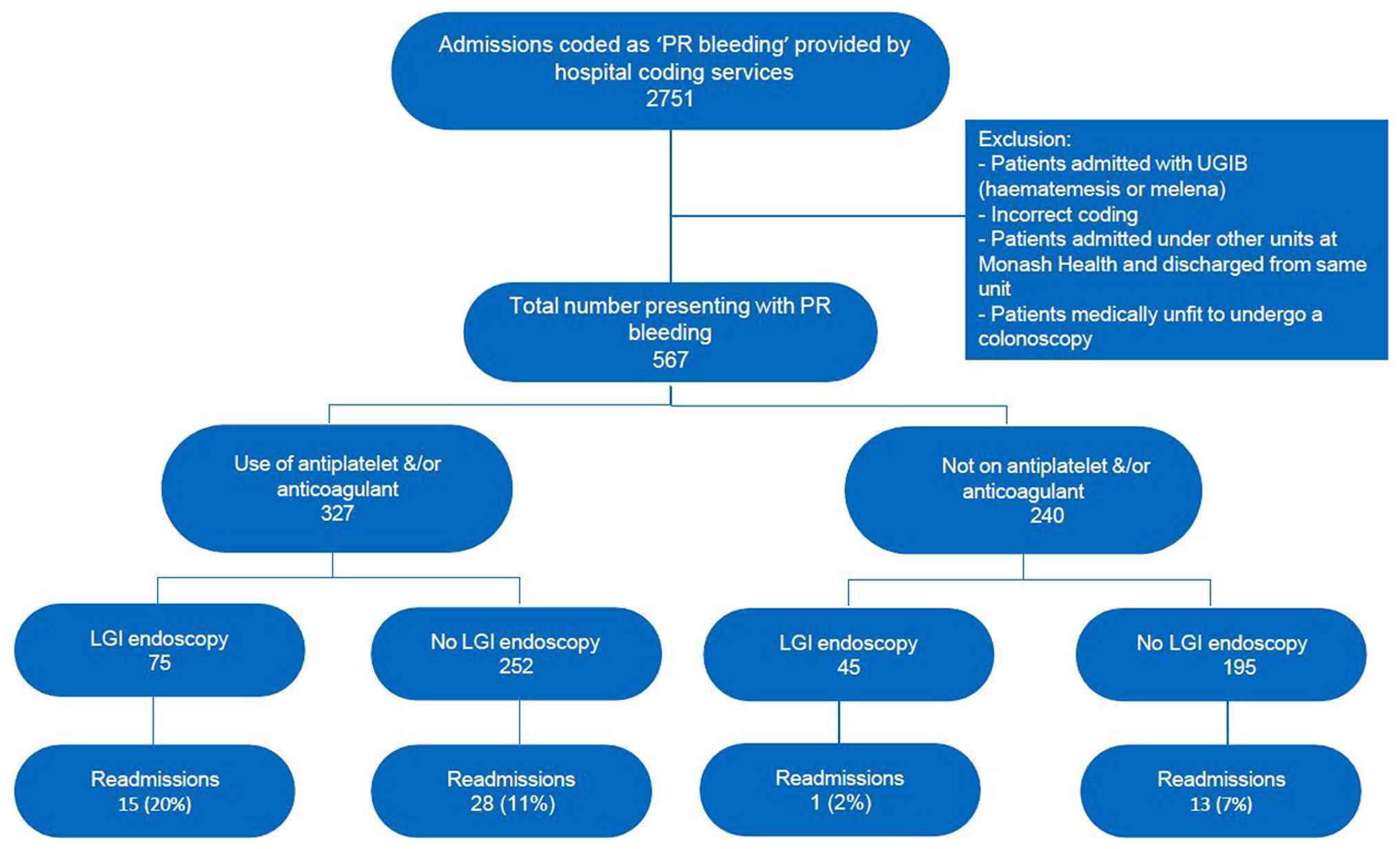
A total of 2,751 admissions were screened, and 567
patients were included in the study over the specified time frame,
categorized according to their antiplatelet/anticoagulant use and
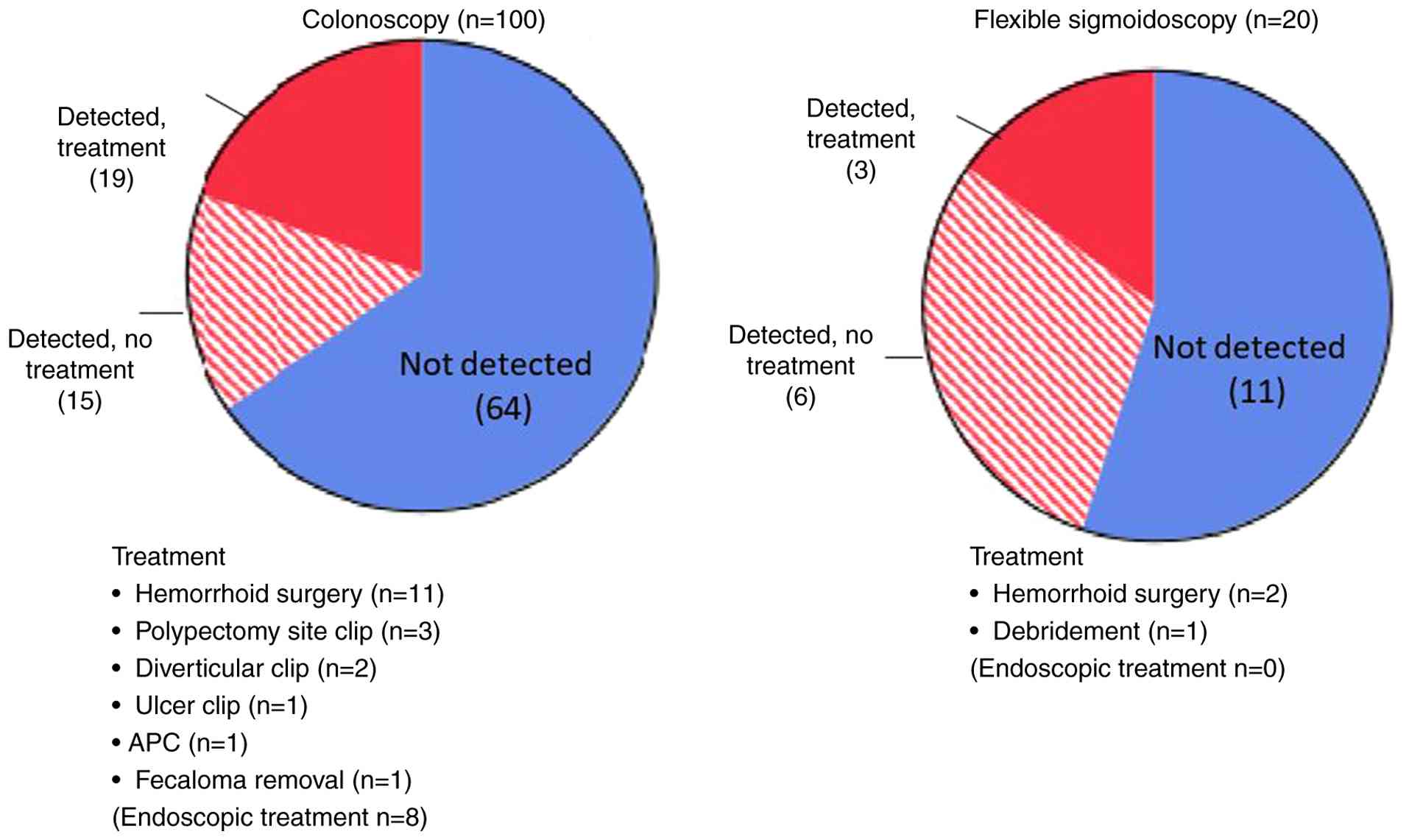
whether they received LGI endoscopy (Fig. 1). Out of the 120 patients who
underwent LGI endoscopy, 100 patients had a colonoscopy, while 20
patients had a flexible sigmoidoscopy. Among the 100 patients who
had a colonoscopy, the source of bleeding was identified in 34
cases. Of these, 8 patients required endoscopic treatment, and 11
patients underwent hemorrhoid surgery. In the group that had
flexible sigmoidoscopy, the cause of bleeding was identified in 9
patients, with 3 of those receiving treatment (Fig. 2). All patients underwent complete
6-month follow-up via linkage with the Monash Health electronic
medical record system, which captures all readmissions within the
health network. In total, 7 patients (1.2%) succumbed during
follow-up; none of the deaths were directly attributed to recurrent
LGI bleeding.
The factors linked to readmission for bleeding
within 6 months are outlined in Table
I. These factors are derived from demographic data, hemodynamic
status, the requirement for blood transfusions, the use of
anticoagulants and/or antiplatelet agents, the requirement for CT
angiography and subsequent CT angiographic interventions and
inpatient GI endoscopy and interventions for bleeding based on
endoscopic findings. This analysis compared two groups regarding
their readmission rates within 6 months. No significant difference
was noted in the re-admission rates between patients who had
inpatient endoscopy and those who did not (P=0.775) Similarly,
antiplatelet use alone was not associated with a significant
difference in readmission rates (P=0.836). Blood transfusion
requirements, CT angiography and angiographic embolization were
also not independently associated with readmission in the
univariate analysis (all P>0.05). There was a numerical increase
in readmission rates among patients receiving anticoagulant therapy
and among those receiving combined antiplatelet and/or
anticoagulant therapy; however, these differences did not reach
statistical significance in the univariate analysis (P=0.053 and
P=0.121, respectively) (Table
I).
 | Table IDemographic data, anticoagulant and
antiplatelet use, and blood transfusion and inpatient LGI endoscopy
stratified by readmission within 6 months. |
Table I
Demographic data, anticoagulant and
antiplatelet use, and blood transfusion and inpatient LGI endoscopy
stratified by readmission within 6 months.
| | Readmission within 6
months | |
|---|
| Parameters | No | Yes | P-value |
|---|
| Age, median
(IQR)b | 74 (59-82) | 77 (68-84) | 0.287 |
| Sex, n
(%)c | | | 0.913 |
|
Female | 174 (42.0) | 16 (41.0) | |
|
Male | 241 (58.0) | 23 (59.0) | |
| Inpatient LGI
endoscopy, n (%)c | | | 0.621 |
|
No | 333 (80.0) | 30 (77.0) | |
|
Yes | 82 (20.0) | 9 (23.0) | |
| Antiplatelet use, n
(%)c | | | 0.706 |
|
No | 247 (60.0) | 22 (56.0) | |
|
Yes | 168 (40.0) | 17 (44.0) | |
| Anticoagulant use, n
(%)c | | | 0.033a |
|
No | 319 (77.0) | 24 (62.0) | |
|
Yes | 96 (23.0) | 17 (44.0) | |
| Antiplatelet and/or
anticoagulant use, n (%)c | | | 0.085 |
|
No | 187 (45.0) | 12 (31.0) | |
|
Yes | 228 (55.0) | 27 (69.0) | |
| Blood transfusion, n
(%)d | | | 0.756 |
|
No | 383 (92.0) | 37 (95.0) | |
|
Yes | 32 (7.7) | 2 (5.1) | |
| Angioembolization, n
(%)d | | | 0.172 |
|
No | 401 (97.0) | 36 (92.0) | |
|
Yes | 14 (3.4) | 3 (7.7) | |
| CT angiography, n
(%)c | | | 0.518 |
|
No | 297 (72.0) | 26 (67.0) | |
|
Yes | 118 (28.0) | 13 (33.3) | |
Subgroup analysis was performed using antiplatelet
and/or anticoagulant therapy (Table
II). Among the patients receiving antiplatelet or anticoagulant
therapy, inpatient LGI endoscopy was not associated with a
statistically significant difference in readmission rates
(P=0.309). Within the subgroup not receiving antiplatelet or
anticoagulant therapy, patients undergoing inpatient LGI endoscopy
were more likely to undergo CT angiography (P=0.007), reflecting
greater diagnostic investigation in this cohort; however, this did
not translate into higher readmission rates.
| Table IIDemographic data, anticoagulant and
antiplatelet use, blood transfusion and re-admission rates within 6
months for all patients stratified by inpatient LGI endoscopy and
layered by risk grade. |
Table II
Demographic data, anticoagulant and
antiplatelet use, blood transfusion and re-admission rates within 6
months for all patients stratified by inpatient LGI endoscopy and
layered by risk grade.
| | Use of antiplatelet
or anticoagulant | No antiplatelet or
anticoagulant |
|---|
| | Inpatient LGI
endoscopy | | Inpatient LGI
endoscopy | |
|---|
| Layer
Parameters | No | Yes | P-value No | No | Yes | P-value |
|---|
| Age, median
(IQR)b | 79.0
(71.0-85.0) | 78.0
(68.0-83.6) | 0.209 | 61.0
(48.3-76.8) | 57.0
(45.0-78.0) | 0.350 |
| Sexc | | | 0.279 | | | 0.255 |
|
Female | 73 (36.7) | 25 (44.6) | | 79 (48.2) | 13 (37.1) | |
|
Male | 126 (63.3) | 31 (55.4) | | 85 (51.8) | 22 (62.9) | |
| Blood
transfusiond | | | 0.081 | | | 0.166 |
|
No | 188 (94.5) | 49 (87.5) | | 153 (93.3) | 30 (85.7) | |
|
Yes | 11 (5.5) | 7 (12.5) | | 11 (6.7) | 5 (14.3) | |
| CT
angiographyc | | | 0.819 | | | 0.007a |
|
No | 179 (70.8) | 49 (66.2) | | 150 (76.5) | 25 (56.8) | |
|
Yes | 74 (29.2) | 25 (33.8) | | 46 (23.5) | 19 (43.2) | |
|
Angioembolizationd | | | 0.535 | | | 0.176 |
|
No | 185 (93.0) | 54 (96.4) | | 164 (100.0) | 34 (97.1) | |
|
Yes | 14 (7.0) | 2 (3.6) | | - | 1 (2.9) | |
|
NA | | | | | | |
| Re-admission within
6 monthsd | | | 0.309 | | | NS |
|
No | 180 (90.5) | 48 (85.7) | | 153 (93.3) | 24 (97.1) | |
|
Yes | 19 (9.5) | 8 (14.3) | | 11 (6.7) | 1 (2.9) | |
Univariable logistic regression (Table III) identified
antiplatelet/anticoagulant therapy as showing a trend toward
increased odds of readmission (OR, 1.85; 95% CI, 0.93-3.87;
P=0.089). Other factors, including age, sex, transfusion, CTA and
angioembolization were not significantly associated with
readmission. In the reduced multivariable model (Table IV), antiplatelet/anticoagulant
therapy remained the only variable approaching significance (OR,
1.85; 95% CI, 0.93-3.87; P=0.089).
| Table IIIUnivariable logistic regression model
for risk of readmission at 6 months between patient
characteristics. |
Table III
Univariable logistic regression model
for risk of readmission at 6 months between patient
characteristics.
| Characteristic | OR | 95% CI | P-value |
|---|
| Colonoscopy | | | |
|
No
colonoscopy | - | - | |
|
Had
colonoscopy | 1.22 | 0.53-2.57 | 0.621 |
| Antiplatelet or
anticoagulants | | | |
|
No | - | - | |
|
Yes | 1.85 | 0.93-3.87 | 0.089a |
|
Age | 1.01 | 0.99-1.04 | 0.258 |
| Sex | | | |
|
Female | - | - | |
|
Male | 1.04 | 0.54-2.06 | 0.913 |
| Transfusion | | | |
|
No
transfusion | - | - | |
|
Yes
transfusion | 0.65 | 0.10-2.25 | 0.561 |
|
Angioembolization | | | |
|
No | - | - | |
|
Yes | 1.14 | 0.58-2.20 | 0.706 |
| CT angiography | | | |
|
No | - | - | |
|
Yes | 1.26 | 0.61-2.49 | 0.519 |
| Table IVFull to reduced multivariable
logistic regression model for risk of readmission at 6 months
between patient characteristics. |
Table IV
Full to reduced multivariable
logistic regression model for risk of readmission at 6 months
between patient characteristics.
| | Full model | Reduced model |
|---|
| Characteristic | OR | 95% CI | P-value | OR | 95% CI | P-value |
|---|
| Antiplatelet or
anticoagulants | | | | | | |
|
No | - | - | | | | |
|
Yes | 1.65 | 0.76-3.80 | 0.221 | 1.85 | 0.93-3.87 | 0.089 |
|
Age | 1.00 | 0.98-1.03 | 0.734 | | | |
| Sex | | | | | | |
|
Female | - | - | | | | |
|
Male | 0.97 | 0.49-1.94 | 0.928 | | | |
| Transfusion | | | | | | |
|
No
transfusion | - | - | | | | |
|
Yes
transfusion | 0.63 | 0.10-2.25 | 0.543 | | | |
|
Angioembolization | | | | | | |
|
No | - | - | | | | |
|
Yes | 1.93 | 0.39-7.54 | 0.371 | | | |
| CTA | | | | | | |
|
No | - | - | | | | |
|
Yes | 1.10 | 0.49-2.32 | 0.801 | | | |
Propensity score matching was used to balance the
endoscopic and non-endoscopic groups concerning key demographic and
clinical variables. Prior to PSM, significant differences were
noted between the treatment and control groups with regard to their
transfusion requirements (P=0.002) and CT angiography (P=0.02),
with higher rates in those who underwent LGI endoscopy. Following
matching, the group baseline characteristics were more balanced,
and the differences in transfusion requirements and CT angiography
were no longer significant (all P>0.05), indicating successful
balancing by PSM. Following matching, standardized mean differences
for all covariates were <0.1, confirming adequate balance
between the LGI endoscopy and non-endoscopy groups (Fig. S1).
Discussion
The present retrospective study aimed to determine
the optimal timing for LGI endoscopy in patients with ALGIB and its
impact on the rate of readmissions. Studies evaluating the role of
inpatient endoscopies for ALGIB on readmission rates in the public
hospital setting in Australia have not been published
previously.
Endoscopic treatment was performed in only 8
patients (8% of colonoscopy cases and 1.4% of all patients). The
exclusion of bleeding from polypectomy (3 out of 8) significantly
impacts the overall evaluation of the clinical utility of
colonoscopy in the context of ALGIB. When bleeding from polypectomy
is excluded, the incidence of bleeding decreases to just 5 out of
564 cases (0.8%). The diagnostic yield (36%) and therapeutic
intervention rate (19%) align with international studies on
inpatient ALGIB management, which report diagnostic yields of
30-45% and therapeutic yields of 15-25% (7). These values reflect real-world
practice rather than sampling bias. Post-matching covariates were
well balanced, confirming model stability. Sonnenberg (11) performed a decision analysis and
demonstrated that pursuing colonoscopy for delayed PPB was
effective in detecting and addressing a bleeding lesion in 22% of
cases, requiring treatment for 4.5 patients. The author concluded
that attempting a repeat colonoscopy would be advantageous, while
also acknowledging that it is prudent to manage certain patients
conservatively. This finding indicates that by recognizing patients
at risk for polypectomy-related bleeding through their history, it
is possible to pinpoint those for whom colonoscopy may offer
limited clinical benefit. Consequently, it appears that colonoscopy
may not be essential for treating ALGIB in patients without a
history of polypectomy-associated bleeding.
The data further indicates a lack of therapeutic
benefit of LGI endoscopy in reducing readmission rates. However,
not surprisingly, the use of antiplatelets and/or anticoagulants
increased the risk of readmission in 6 months. Although previous
research, such as the ASPREE trial, reported an increased GI
bleeding risk with aspirin, single antiplatelet therapy was not
associated with increased readmission in the cohort examined in the
present study (2).
A similar retrospective cohort study conducted in
the USA with the primary outcome of 30-day all-cause readmission
and a secondary outcome of the impact of early colonoscopy on
30-day readmission indicated similar results to those observed in
the present study. The 30-day readmission rate was 16.4% compared
with that noted in the 6-month readmission rate (10%). However, it
was also suggested that early colonoscopy did not affect the 30-day
readmission rate (12).
Rebleeding is a significant complication following
initial control of ALGIB. ALGIB exhibits a rebleeding rate that is
>2-fold of that noted in upper GI bleeding (13). Previous studies have demonstrated
that early colonoscopy (≤24 h) employed for acute lower GI bleeding
does not reduce rebleeding (14)
or mortality rates compared with elective colonoscopy (15-17).
Based on these findings, previous studies have suggested that
patients generally do not require an early colonoscopy examination
(7,8).
A multicenter retrospective cohort study suggested
that early colonoscopy correlated with increased risk of rebleeding
and reduced length of hospitalization (15). By contrast, the present study did
not demonstrate a significant difference in readmission rates
between patients who underwent inpatient endoscopy and those who
did not (P=0.775, Table I).
Subgroup analyses likewise showed no significant impact of
endoscopic interventions on readmission (Table II). While patients receiving
antiplatelet and/or anticoagulant therapy exhibited a trend toward
higher readmission rates, this appeared independent of endoscopy
itself. These findings suggest that, although colonoscopy may
facilitate identification of recent bleeding, its role in reducing
rebleeding or readmission remains uncertain. A recent large
retrospective study from Japan indicated similar results. The
present study indicated that early colonoscopy was limited to
higher detection of recent signs of bleeding, and the 30-day
rebleeding rate was not reduced in patients who underwent early
colonoscopy compared with those who underwent elective or late
colonoscopy (7).
Active bleeding requiring angiographic embolization
has been identified as a significant risk factor for both
rebleeding and readmission. Gobinet-Suguro et al (18) reported that the incidence of early
and late rebleeding was notably higher in patients experiencing
active bleeding associated with diverticular LGI bleeding compared
with those with non-active bleeding, which supports the
aforementioned observation.
The present study provides further insight to
previous studies that have demonstrated that the lack of readily
apparent benefit in performing LGI endoscopy can be used to reduce
the readmission rate for ALGIB. The conduct of inpatient
colonoscopies increases the burden caused on already overburdened
hospital resources for emergency and endoscopy equipment access
without clear evidence of benefit to patients or the healthcare
system. An Australian guideline on the indication for early
colonoscopies in ALGIB would be useful to streamline subsets of
patients who may benefit from them. Further research into the
financial implications of LGI endoscopy on the public health system
in Australia is required.
The present retrospective study exhibits certain
limitations, such as coding errors, which were addressed via
meticulous record reviews. The 6-month follow-up period may be
inadequate, and only in-hospital readmissions within Monash Health
were captured, excluding other health services. This study has
limitations, including the lack of specific data on the use of
non-steroidal anti-inflammatory drugs and granular classification
of antithrombotic regimens. Additionally, clinical and laboratory
parameters such as comorbidities, body mass index and biochemical
data were inconsistently recorded and thus excluded. These
constraints limit the scope of multivariate analysis to
consistently available variables. The lack of quantitative data on
bleeding volume and inconsistent recording of comorbidities limited
certain types of analyses; however, key predictors such as age,
hemodynamics, transfusions, antithrombotic use and angiography were
included. Future studies are thus required to incorporate
standardized comorbidity scoring and account for changes in
antithrombotic therapy over time. The reliance on medication use at
admission may potentially cause a misclassification of exposure;
however, its results align with previous findings on anticoagulants
and rebleeding. Clinicians selected patients for LGI endoscopy
individually, with PSM used to control confounding parameters.
Residual bias likely exists due to the more frequent selection for
inpatient procedures in patients who were in a more serious disease
state. This resulted in inpatient endoscopy being a marker of
severity rather than a cause of readmission. Future prospective
studies are required to clarify procedural effects and unmeasured
confounders. The present study excluded patients with multiple
Emergency Department visits and lacked detailed bleeding source
classification, requiring future multicenter, prospective research
with comprehensive data and longer follow-up to enable an improved
understanding of rebleeding risks.
In conclusion, the present study suggests that the
rationale for LGI endoscopy in an algorithm used to manage ALGIB
should not focus on the presumed benefit of early detection of
pathology to minimize readmission. The results demonstrate a lack
of evidence of a reduction in the 6-month readmission rate for
patients with LGIB following LGI endoscopy. To the best of our
knowledge, this is the first study to analyze the impact of
inpatient LGI endoscopy on readmission risk in an Australian public
hospital setting. These findings provide critical local data that
can be used in the establishment of Australian-specific clinical
pathways and guidelines for managing acute LGI, an area currently
guided largely by international evidence. The development of
Australian guidelines on the indications for LGI endoscopy is
required to guide healthcare resource expenditure. However, there
is an urge to at least add pro-rata costing against the impact to
justify the intervention.
Supplementary Material
Distribution of propensity scores and
logit-transformed scores for the LGI endoscopy and non-endoscopy
groups. LGI, lower gastrointestinal.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
SC, RT, HC, ZD, TCN and WT conceptualized the study.
SF, WI, YKT, JL and KN were involved in data curation. SF, WI, JL,
CS and EA were involved in formal analysis. SF, TCN, AA, CS and VN
were involved in data analysis. SF, TCN, HC and TSS were involved
in the study methodology. YKT and JL were involved in project
administration. WI and RT were involved in the writing of the
original draft of the manuscript. WI, SF, HC and CS were involved
in the writing, reviewing and editing of the manuscript. All
authors have read and approved the final manuscript. WI, SF and RT
confirm the authenticity of all the raw data.
Ethics approval and consent to
participate
All research was performed per relevant guidelines
and regulations, including the Declaration of Helsinki. Monash
Health Research Support Services approved and exempted the project
from Human Research Ethics Review, categorizing it as Quality
Assurance/Minimal Risk Research. Informed consent was waived due to
the retrospective nature of the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Fok KY, Murugesan JR, Maher R and Engel A:
Management of per rectal bleeding is resource intensive. ANZ J
Surg. 89:E113–E116. 2019.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Mahady SE, Margolis KL, Chan A, Polekhina
G, Woods RL, Wolfe R, Nelson MR, Lockery JE, Wood EM, Reid C, et
al: Major GI bleeding in older persons using aspirin: Incidence and
risk factors in the ASPREE randomised controlled trial. Gut.
70:717–724. 2021.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Strate LL and Gralnek IM: ACG clinical
guideline: Management of patients with acute lower gastrointestinal
bleeding. Am J Gastroenterol. 111:459–474. 2016.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Oakland K, Chadwick G, East JE, Guy R,
Humphries A, Jairath V, McPherson S, Metzner M, Morris AJ, Murphy
MF, et al: Diagnosis and management of acute lower gastrointestinal
bleeding: Guidelines from the British society of gastroenterology.
Gut. 68:776–789. 2019.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Triantafyllou K, Gkolfakis P, Gralnek IM,
Oakland K, Manes G, Radaelli F, Awadie H, Camus Duboc M,
Christodoulou D, Fedorov E, et al: Correction: Diagnosis and
management of acute lower gastrointestinal bleeding: European
society of gastrointestinal endoscopy (ESGE) guideline. Endoscopy.
53(C10)2021.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Nagata N, Ishii N, Manabe N, Tomizawa K,
Urita Y, Funabiki T, Fujimori S and Kaise M: Guidelines for colonic
diverticular bleeding and colonic diverticulitis: Japan
gastroenterological association. Digestion. 99 (Suppl 1):S1–S26.
2019.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Tsay C, Shung D, Stemmer Frumento K and
Laine L: Early colonoscopy does not improve outcomes of patients
with lower gastrointestinal bleeding: Systematic review of
randomized trials. Clin Gastroenterol Hepatol. 18:1696–1703.e2.
2020.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Seth A, Khan MA, Nollan R, Gupta D, Kamal
S, Singh U, Kamal F and Howden CW: Does urgent colonoscopy improve
outcomes in the management of lower gastrointestinal bleeding? Am J
Med Sci. 353:298–306. 2017.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Aoki T, Yamada A, Nagata N, Niikura R,
Hirata Y and Koike K: External validation of the NOBLADS score, a
risk scoring system for severe acute lower gastrointestinal
bleeding. PLoS One. 13(e0196514)2018.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Austin PC: Optimal caliper widths for
propensity-score matching when estimating differences in means and
differences in proportions in observational studies. Pharm Stat.
10:150–161. 2011.PubMed/NCBI View
Article : Google Scholar
|
|
11
|
Sonnenberg A: Management of delayed
postpolypectomy bleeding: A decision analysis. Am J Gastroenterol.
107:339–342. 2012.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Sharma S, Sallout D, Acharya A and Adler
DG: early colonoscopy does not affect 30-day readmission after
lower GI bleeding: Insights from a nationwide analysis. Dig Dis
Sci. 67:3948–3954. 2022.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Kwak MS, Cha JM, Han YJ, Yoon JY, Jeon JW,
Shin HP, Joo KR and Lee JI: The clinical outcomes of lower
gastrointestinal bleeding are not better than those of upper
gastrointestinal bleeding. J Korean Med Sci. 31:1611–1616.
2016.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Kherad O, Restellini S, Almadi M, Strate
LL, Ménard C, Martel M, Roshan Afshar I, Sadr MS and Barkun AN:
Systematic review with meta-analysis: Limited benefits from early
colonoscopy in acute lower gastrointestinal bleeding. Aliment
Pharmacol Ther. 52:774–788. 2020.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Niikura R, Nagata N, Yamada A, Honda T,
Hasatani K, Ishii N, Shiratori Y, Doyama H, Nishida T, Sumiyoshi T,
et al: Efficacy and safety of early vs elective colonoscopy for
acute lower gastrointestinal bleeding. Gastroenterology.
158:168–175.e6. 2020.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Shiratori Y, Ishii N, Aoki T, Kobayashi K,
Yamauchi A, Yamada A, Omori J, Aoyama T, Tominaga N, Sato Y, et al:
Timing of colonoscopy in acute lower GI bleeding: A multicenter
retrospective cohort study. Gastrointest Endosc. 97:89–99.e10.
2023.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Anvari S, Lee Y, Yu J, Doumouras AG, Khan
KJ and Hong D: Urgent versus standard colonoscopy for management of
acute lower gastrointestinal bleeding: A systematic review and
meta-analysis of randomized controlled trials. J Clin
Gastroenterol. 54:493–502. 2020.PubMed/NCBI View Article : Google Scholar
|
|
18
|
Gobinet-Suguro M, Nagata N, Kobayashi K,
Yamauchi A, Yamada A, Omori J, Ikeya T, Aoyama T, Tominaga N, Sato
Y, et al: Treatment strategies for reducing early and late
recurrence of colonic diverticular bleeding based on stigmata of
recent hemorrhage: A large multicenter study. Gastrointest Endosc.
95:1210–1222.e12. 2022.PubMed/NCBI View Article : Google Scholar
|