Introduction
Primary cutaneous lymphomas (PCLs) are a diverse
group of lymphoproliferative malignancies restricted to the skin at
diagnosis without involving the lymph nodes, bone marrow, or other
organs. While non-Hodgkin lymphoma (NHL) is relatively common, PCLs
account for only 4% of all NHL cases annually. These lymphomas
primarily originate from T-lymphocytes (65%), B-lymphocytes (25%),
or natural killer cells (10%) (1).
The incidence of primary cutaneous B-cell lymphomas
(PCBCLs) is estimated to be <1 per 100,000 individuals per year,
with a rise in frequency as with the increase in age (2). The World Health Organization-European
Organization for Research and Treatment of Cancer classifies PCBCLs
into three main subtypes: Primary cutaneous marginal zone lymphoma
(PCMZL), primary cutaneous follicle center lymphoma (PCFCL) and
primary cutaneous diffuse large B-cell lymphoma, leg type
(PCDLBCL-LT) (3).
PCDLBCL-LT is rare and aggressive, marked by the
abnormal growth of B-cells in the skin (4). This condition typically involves the
dermis and subcutaneous layers, resulting in rapidly growing, red
to blueish nodular tumors, usually on the lower limbs. However, it
can also occur in other parts of the body. PCDLBCL-LT accounts for
4% of all newly diagnosed PCLs annually. It primarily affects older
women and is associated with a worse prognosis (4).
Cases of PCDLBCL that were not categorized as
PCDLBCL-LT have long been termed primary cutaneous diffuse large
B-cell lymphomas, other (PCLBCL/other). In the WHO classification
for skin tumors, these were renamed as primary cutaneous diffuse
large B-cell lymphomas, not otherwise specified (PCDLBCL-NOS)
(3).
The present study describes the case of a
45-year-old female patient with PCDLBCL on the scalp. PCDLBCL on
the scalp is extremely rare, with only a few cases documented in
the literature to date (4-8).
Case report
Patient information
A 45-year-old female patient presented to Smart
Health Tower (Sulaymaniyah, Iraq) in January, 2025 with localized
hair loss on the scalp lasting for 4 months, accompanied by mild
redness and itching. No notable systemic symptoms were
reported.
Clinical findings
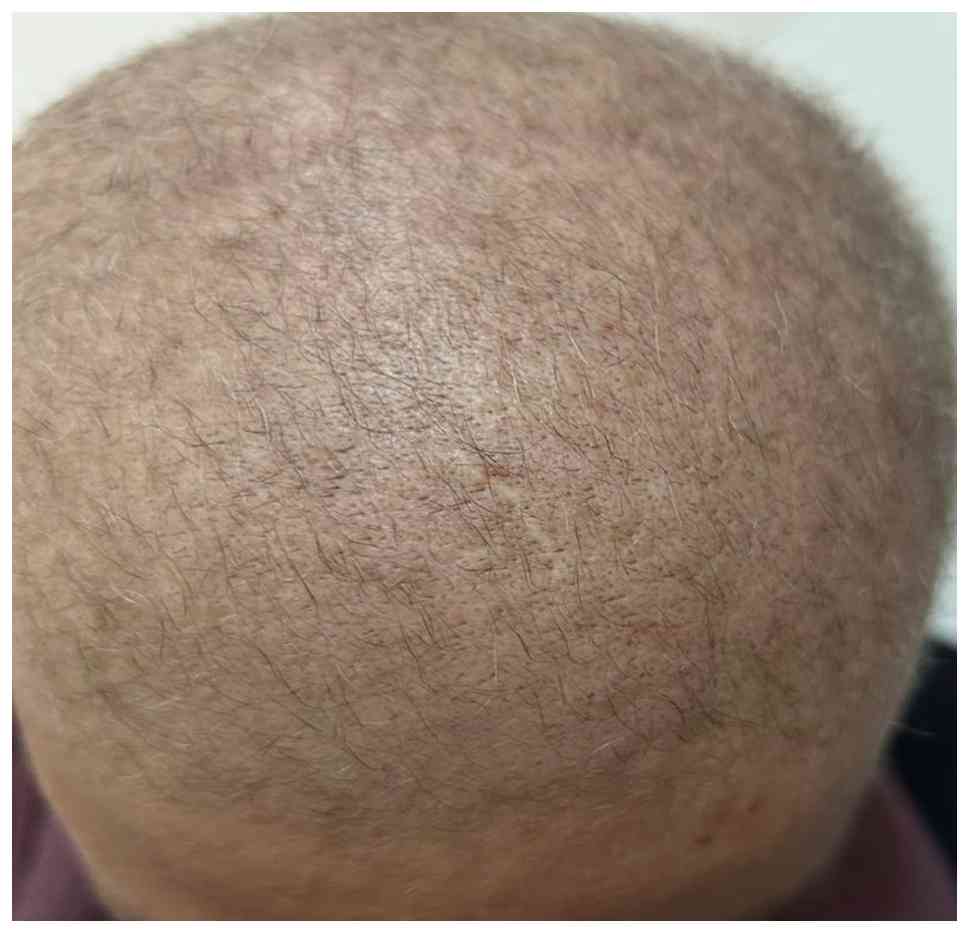
Upon a clinical examination, irregular patches of
hair thinning, each a few centimeters in size, were observed on an
erythematous base, accompanied by slight swelling but no palpable
mass (Fig. 1). There was no
lymphadenopathy or similar lesions elsewhere on the body.
Diagnostic approach
Laboratory investigations at initial presentation
revealed anemia with a hemoglobin level of 7.7 g/dl (reference
range, 12-16 g/dl) and leukopenia with a white blood cell count of
2.1x109/l (reference range, 4.0-11.0x109/l),
while the platelet count was within normal limits at
167x109/l (reference range, 150-400x109/l).
The erythrocyte sedimentation rate was elevated at 38 mm/h
(reference range, 0-20 mm/h). A peripheral blood smear examination
demonstrated normochromic anemia with neutropenia, with no
circulating atypical lymphoid cells or blast forms. Liver and renal
function test results were within normal ranges: Alanine
aminotransferase, 22 U/l (reference range, 7-56 U/l); aspartate
aminotransferase, 25 U/l (reference range, 10-40 U/l); alkaline
phosphatase, 86 U/l (reference range, 44-147 U/l); total bilirubin,
0.8 mg/dl (reference range, 0.2-1.2 mg/dl); serum creatinine, 0.9
mg/dl (reference range, 0.6-1.3 mg/l); blood urea nitrogen, 14
mg/dl (reference range, 7-20 mg/dl). Serological testing for human
immunodeficiency virus, hepatitis B surface antigen and hepatitis C
virus yielded negative results. A 4-mm punch biopsy was obtained
from an active erythematous alopecic lesion on the parietal region
of the scalp. The specimen was fixed in 10% neutral buffered
formalin at room temperature for 24 h, embedded in paraffin, and
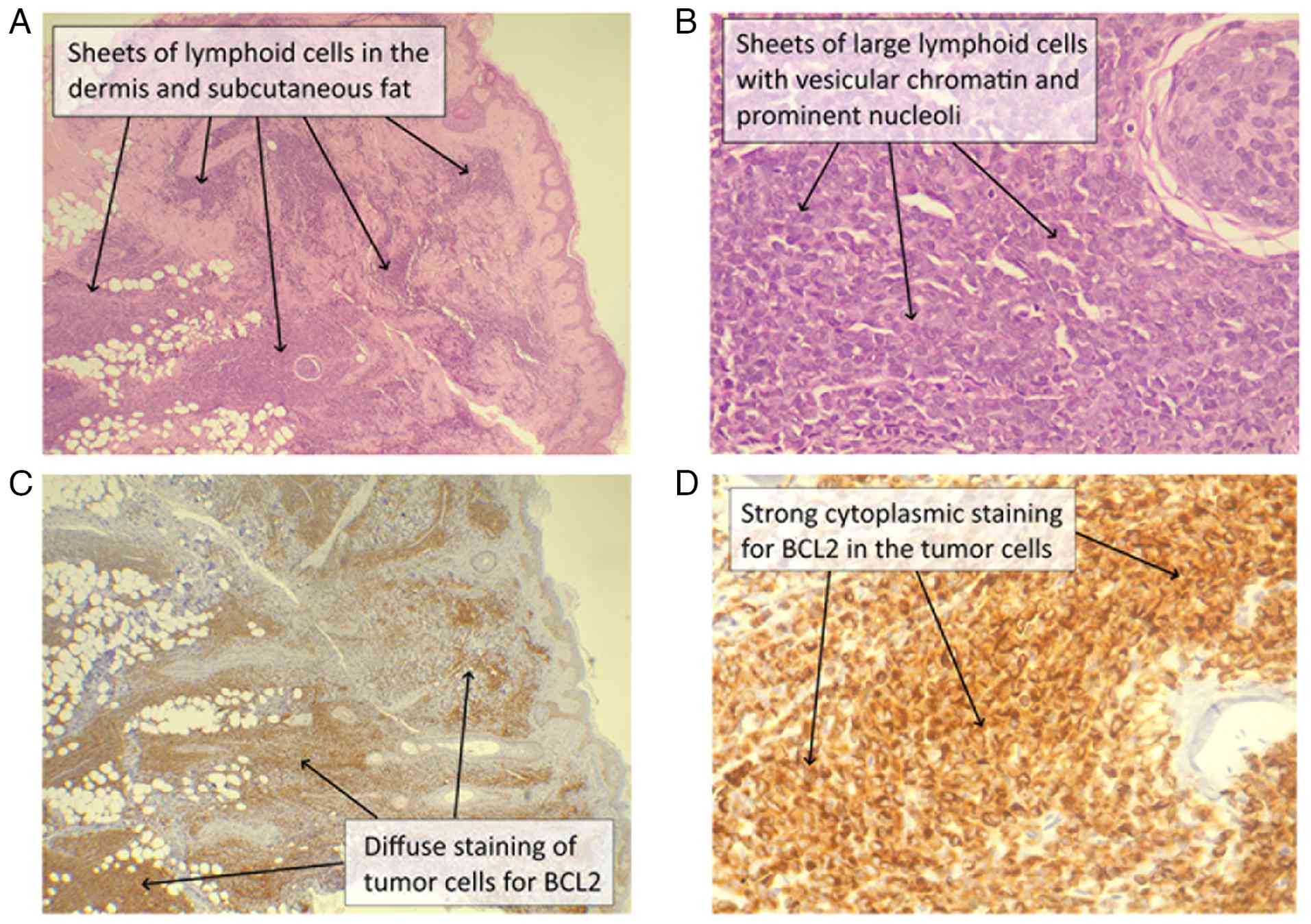
sectioned at a thickness of 5 µm. A histological examination was
performed using hematoxylin and eosin (H&E) staining (Bio
Optica Co.), applied for 1-2 min at room temperature, and evaluated
under a light microscope (Leica Microsystems GmbH). Microscopic
analysis revealed multiple sheets of atypical cells with scant
cytoplasm and large vesicular nuclei with prominent nucleoli,
infiltrating the reticular dermis and subcutaneous fat and
surrounding the hair follicles, while the overlying epidermis
remained uninvolved. In our institution, immunohistochemical
analysis for BCL2 was performed on formalin-fixed,
paraffin-embedded tissue sections cut at a thickness of 4-5 µm and
mounted on positively charged glass slides. The sections were
incubated in an oven at 60˚C overnight, followed by
deparaffinization in xylene and rehydration through graded alcohol
solutions to distilled water. Heat-induced antigen retrieval was
carried out using the Dako PT Link system (Agilent Technologies,
Inc.) at 100˚C for 20 min using alkaline buffer (pH 9.0).
Endogenous peroxidase activity was quenched using 3% hydrogen
peroxide at room temperature. The slides were then rinsed in
Tris-buffered saline containing 0.05% Tween-20 (pH 7.6), and a
hydrophobic barrier was created using a Dako Pen (Agilent
Technologies, Inc.). The primary antibody used was a mouse
monoclonal anti-BCL2 antibody (clone 124; cat. no. M0887;
Dako/Agilent Technologies, Inc.), applied at a dilution of 1:100
and incubated at room temperature for 60-80 min. Immunoreactivity
was detected using a horseradish peroxidase-labeled polymer-based
secondary detection system (EnVision™+ System-HRP, anti-mouse)
obtained from Dako/Agilent Technologies, Inc. (cat. no. K5007),
with 3,3'-diaminobenzidine (DAB) used as the chromogen. Finally,
the sections were counterstained with Gill II hematoxylin for 30
sec, dehydrated, cleared, and mounted for light microscopic
examination. All slides were evaluated using a standard light
microscope (Leica Microsystems GmbH). Immunohistochemistry
subsequently demonstrated diffuse BCL2 positivity (Fig. 2). These findings were consistent
with a diagnosis of non-Hodgkin's lymphoma involving the hair
follicles and subcutaneous fat, for which a comprehensive
immunohistochemical panel was required for definitive confirmation
and subtyping. Another punch biopsy was performed at an external
hospital (Shorsh General Hospital, Sulaymaniyah). A
histopathological examination demonstrated a diffuse dermal and
perifollicular infiltrate of atypical intermediate- to large-sized
lymphoid cells with vesicular to hyperchromatic nuclei, prominent
nucleoli, and a moderate amount of pale cytoplasm. Extension of the
infiltrate into the subcutaneous tissue was also observed.
Immunohistochemistry revealed positive CD20, CD10 and CD79a. At the
same time, CD3 and MUM1 were negative. Representative
immunohistochemistry images were not available, as this component
of the diagnostic evaluation was performed at an external
institution and the original histopathology and
immunohistochemistry image files could not be retrieved. These
findings were diagnostic of non-Hodgkin lymphoma, specifically
diffuse large B-cell lymphoma of germinal center type. Computed
tomography (CT) scans of the neck, chest, abdomen and pelvis
revealed no evidence of lymphadenopathy, hepatosplenomegaly, or
visceral organ involvement. The corresponding CT images were not
available for review, as the imaging was performed at an external
radiology facility. Based on the localized cutaneous disease,
negative systemic imaging, histopathological findings and
immunophenotypic profile, the diagnosis of PCDLBCL-NOS, stage
IA(E), was established. Viral screening was negative, and bone
marrow aspiration and biopsy demonstrated lymphoma involvement.
Therapeutic intervention
The patient received six cycles of standard-dose
R-CHOP chemotherapy administered every 21 days, consisting of
rituximab 375 mg/m2 intravenously on day 1,
cyclophosphamide 750 mg/m2 intravenously on day 1,
doxorubicin (hydroxydaunorubicin) 50 mg/m2 intravenously
on day 1, vincristine (Oncovin) 1.4 mg/m2 intravenously
on day 1 (maximum dose 2 mg), and prednisone 100 mg orally on days
1-5. Prophylactic antibiotics and granulocyte colony-stimulating
factor (G-CSF) were administered according to the institutional
protocol. During treatment, the patient developed
chemotherapy-induced neutropenia, which was managed with supportive
care, including the administration of G-CSF, the close monitoring
of complete blood counts and prophylactic broad-spectrum
antibiotics. Antibacterial prophylaxis consisted of oral
levofloxacin 500 mg once daily. No treatment interruptions were
required, and subsequent chemotherapy cycles were continued with
G-CSF support.
Follow-up and outcome
The patient was followed-up for a total duration of
6 months following the completion of chemotherapy. Follow-up
assessments included regular clinical examinations, laboratory
investigations and contrast-enhanced CT scans of the chest and
abdomen, as well as positron emission tomography imaging. At the
6-month follow-up, all scalp lesions were completely resolved, with
no evidence of residual or recurrent disease on imaging and no
signs of lymph node or internal organ involvement (Fig. 3). The patient continued to undergo
clinical and radiological surveillance.
Subsequently, the patient developed pancytopenia.
Repeat bone marrow aspiration and biopsy, along with flow
cytometry, led to the diagnosis of B-cell acute lymphoblastic
leukemia.
Molecular analysis for the BCR-ABL fusion gene was
conducted at an external medical facility (Hiwa Cancer Hospital,
Sulaymaniyah, Iraq) using reverse transcription polymerase chain
reaction (RT-PCR) on RNA extracted from bone marrow aspirate
specimens. Primers specific for the major (b2a2, b3a2) and minor
(e1a2) BCR-ABL fusion transcripts were used. No amplification of
BCR-ABL transcripts was detected, confirming the absence of the
Philadelphia chromosome. Detailed technical information regarding
the RNA extraction buffer and manufacturer, the reverse
transcription reagents, as well as the exact temperature and
cycling protocols, was not available to the authors. In addition,
cytogenetic evaluation was also performed at the same external
facility using standard G-banding techniques on short-term cultured
bone marrow aspirate cells, with a minimum of 20 metaphase spreads
analyzed. The karyotype revealed a normal chromosomal complement
without evidence of recurrent or complex cytogenetic abnormalities.
The patient was commenced on the HYPER-CVAD chemotherapy protocol,
consisting of alternating courses of hyperfractionated
cyclophosphamide, vincristine, doxorubicin (Adriamycin), and
dexamethasone (course A), and high-dose methotrexate with
cytarabine (course B). Course A included cyclophosphamide at 300
mg/m2 intravenously every 12 h on days 1-3, vincristine
at 2 mg intravenously on days 4 and 11, doxorubicin 50
mg/m2 intravenously on day 4, and dexamethasone at 40 mg
orally or intravenously on days 1-4 and 11-14. Course B consisted
of methotrexate 1 g/m2 intravenously over a period of 24
h on day 1, followed by cytarabine at 3 g/m2
intravenously every 12 h on days 2 and 3. Cycles were planned to
alternate every 21-28 days according to hematologic recovery.
During treatment, she developed severe pancytopenia complicated by
neutropenic sepsis. Despite appropriate supportive and
antimicrobial management, the patient unfortunately succumbed to
sepsis.
Discussion
Systemic lymphomas can affect the skin as secondary
cutaneous lymphomas exhibit distinct clinical behaviors and
prognoses compared to PCL, necessitating different treatment
approaches (6). PCBCLs often
manifest as smooth, well-defined, erythematous to non-ulcerated
violaceous nodules, primarily appearing on the trunk, head and neck
regions. Among cutaneous sites, the scalp is a rare location for
these lymphomas (6). Čolović et
al (8) described a case of
scalp PCDLBCL characterized by regional hair loss, a scalp rash and
itching that had been present for 16 years. By contrast, Khatib
et al (5) reported a case
involving a solitary scalp swelling that progressively enlarged
over a period of 5 months. In the case presented herein, the
patient exhibited localized scalp hair loss, mild redness and
itching for 4 months. Viral screening was negative, and bone marrow
aspiration and biopsy demonstrated lymphoma involvement.
PCDLBCL-LT is most frequently diagnosed in elderly
women, with a median age of 70 years at diagnosis. Typically,
PCDLBCL-LT presents as solitary or multiple asymptomatic, rapidly
growing red or purple dermal nodules, primarily affecting one or
both legs. However, in 15-20% of cases, the initial tumor arises at
sites other than the legs (1,4). A
literature search was performed using PubMed and Google Scholar to
identify previously reported cases of PCDLBCL involving the scalp.
Combinations of the terms ‘primary cutaneous diffuse large B-cell
lymphoma’, ‘scalp’, ‘cutaneous lymphoma’, ‘non-Hodgkin lymphoma’
and ‘case report’ were used, with no time restrictions applied. All
available articles up to the time of submission were screened based
on the relevance of the title and abstract, followed by full-text
review of potentially relevant reports. Through this process, five
previously reported cases of scalp PCDLBCL were identified, all
occurring in male patients aged 46-92 years (4-8)
(Table I). By contrast, the
patient in the present case report was a 45-year-old female.
 | Table IReview of 5 cases of PCBCLs affecting
the scalp identified in the literature. |
Table I
Review of 5 cases of PCBCLs affecting
the scalp identified in the literature.
| | IHC | |
|---|
| First author | Year of
publication | Age, years | Sex | Presentation | Examination | Imaging | Positive | Negative | Treatment | Outcome | (Refs.) |
|---|
| Behera | 2022 | 62 | Male | 7-month history of a
gradually enlarging, asymptomatic swelling on the right
temple. | An erythematous
lobulated plaque (5x2 cm) with telangiectasia a satellite papule on
the right temporal area, and two arcuate plaques on the occipital
scalp. | A CT of the scalp
showed bone erosion up to the dura beneath the temporal
lesion. | CD20 Bcl-2 Bcl-6 | CD10 CD5 CD30 CD138
CD21 CyclinD1 ALK1 MUM1 | The patient underwent
six cycles of R-CHOP and intrathecal methotrexate | At 1 year
post-therapy, the patient remains well, with no recurrence or
recurrence or | (4) |
| Khatib | 2017 | 57 | Male | A solitary scalp
swelling gradually increased over 5 months. | A nontender scalp
swelling (2x2 cm) with a bosselated surface, irregular margins, and
firm consistency. | An axial CT of the
brain showed an ill-defined hyperdense lesion in the right parietal
scalp with irregular margins extending into the deeper layers, with
no bony erosion. | CD20
Bcl-6a | CD3 Bcl-2 CD10 CD30
MUM-1 CD23 CD4 | The patient received
three cycles of R-CHOP chemotherapy | The skin lesion fully
regressed after treatment. | (5) |
| Liao | 2017 | 92 | Male | Multiple large
nodular scalp masses on the right parieto-occipital region for 7
months. | A firm, painless,
non-pulsating subcutaneous scalp mass measuring approximately 8x12
cm, with multiple nodules | An MRI showed a
large, multiple-nodular scalp mass with heterogeneous signals, low
on T1-weighted imaging and variable on T2-weighted imaging. | CD20 Bcl-2 | N/A | underwent surgery for
partial removal of the scalp mass. | The tumor recurred
in situ after 6 months, and the patient died from dyscrasia
2 years later. | (6) |
| Ochiai | 2010 | 72 | Male | The patient presented
with a slow-growing mass in the left temporoparietal area of the
scalp. | A 7 cm, firm,
slow-growing mass was noted in the left temporoparietal
region. | A CT scan revealed a
subcutaneous mass in the left temporoparietal region and an
extra-axial mass beneath it, without skull bone invasion. | CD 20 CD79α | CD3 CD45R0 | The patient had a
craniotomy, revealing a gray, hard, hypovascular tumor then he
received whole-brain radiation and CHOP chemotherapy | The patient was
discharged without any neurological deficits. | (7) |
| Čolović | 2008 | 46 | Male | Regional baldness,
scalp rash, and itching occurred 16 years prior. | N/A | The head tomo-graphic
scan was normal, except for a tumorous mass in the scalp's soft
tissue. | CD 20 CD79α | Bcl-2 CD30 CD3 CD5
Bcl-10 | The patient was
treated with the R-CHOP regimen, completing 8 cycles, which
resulted in a notable local response. | Follow-up skin biopsy
revealed normal skin histology with no evidence of lymphomatous
infiltration. | (8) |
The defining features of PCDLBCL-NOS are not yet
well-established. Recent research indicates that this condition is
more common in younger individuals and typically manifests as a
gradually enlarging plaque exceeding 5 cm at diagnosis, often due
to delayed medical attention. The PCDLBCL-NOS subtype usually
involves multiple lesions confined to one or two adjacent body
areas. A notable difference in tumor location on the lower leg has
been identified between the PCDLBCL-LT and PCDLBCL-NOS subtypes,
although no significant difference in ulceration rates has been
observed. Nevertheless, tumor location alone cannot provide a
definitive diagnosis (4). In a
review of 2,831 cases of B-cell lymphomas conducted by Kim et
al (9), only 21 patients were
identified with PCLBCL, of which only two cases belonged to the
PCLBCL-NOS subtype.
The exact pathogenesis of PCBCL is not yet fully
understood. It is hypothesized that PCBCL may arise as a
lymphoproliferative response to antigenic stimuli in the skin,
similar to the process observed in mucosa-associated lymphoid
tissue in the gastrointestinal tract (5). Molecular analyses on PCBCL support
this theory, revealing a characteristic pattern of somatic
hypermutation and intraclonal diversity in B-cell immunoglobulin
genes, suggesting an antigen-driven germinal center origin
(5).
Both variants of DCLBCL are aggressive, with a
5-year survival rate ranging from 20 to 60% (4). It is crucial to differentiate DCLBCL
from PCFCL, particularly those with a diffuse growth pattern, as
PCFCL requires a different therapeutic approach and has a highly
favorable prognosis, with a 90% 5-year survival rate (4).
Histopathological features of PCDLBCL include a
non-epidermotropic, diffuse infiltration of the dermis by large
cells, predominantly composed of centroblasts and immunoblasts,
which may extend into the subcutis. The infiltration is
characterized by its monotonous nature and prominent mitotic
activity, with few inflammatory or reactive T-cells present
(4). Tumor cells exhibit
B-cell-related antigens, including CD19, CD20, CD22, CD79a and
Pax-5. The majority of PCBCLs express germinal center-associated
antigen BCL6 and post-germinal center antigen mum-1/IRF-4, while
CD5 and CD10 are generally negative, and the t(14;18) (q32;q21)
translocation is absent. The apoptosis-regulating protein BCL2 is
strongly expressed in 100% of PCDLBCL-LT cases, but only in 50% of
PCDLBCL-LT cases (10). CD10 is
expressed in 28-40% of patients with DLBCL and is a follicular
center cell origin marker. Research indicates that CD10-positive
patients generally have improved survival outcomes. Furthermore,
~25% of patients with DLBCL exhibit the expression of CD43, which
has been identified as an independent poor prognostic factor for
the disease (11). In the case in
the present study, immunohistochemistry revealed positive staining
for CD20, CD10 and CD79a, along with diffuse BCL2 staining, while
CD3 and MUM1 were negative. Considering the clinical presentation,
imaging findings, histopathology and immunohistochemistry results,
the diagnosis was confirmed as PCDLBCL-NOS.
The differential diagnosis of patchy alopecia with a
dermal lymphoid infiltrate includes alopecia areata, PCFCL,
metastatic carcinoma or secondary systemic lymphoma involving the
skin, and inflammatory/scarring alopecias with lymphoid infiltrate.
Alopecia areata is a non-scarring autoimmune hair loss
characterized histologically by a peribulbar lymphocytic infiltrate
of mainly T-cells around anagen hair bulbs and features, such as
increased catagen/telogen hairs and follicular miniaturization; it
lacks sheets of atypical B-cells and a clonal B-cell
immunophenotype, making it distinct from a neoplastic infiltrate
observed in lymphoma (12).
Primary cutaneous follicle center lymphoma is an indolent B-cell
lymphoma presenting as plaques or nodules often on the scalp or
trunk with a follicular and/or diffuse architecture composed mainly
of centrocytes and centroblasts; unlike diffuse large B-cell
lymphoma, PCFCL exhibits fewer confluent sheets of large cells and
a different immunophenotype, and distinguishing features were
absent in the present study (13).
The standard front-line treatment for PCDLBCL is the
R-CHOP regimen, with or without involved-site radiation therapy.
Despite this approach, relapses are common, occurring in ~70% of
patients (1). Liao et al
(6) reported the case of a
92-year-old patient with scalp PCDLBCL. The mass was partially
resected surgically, but no additional treatment was provided due
to the patient's advanced age and poor physical condition. The
tumor recurred at the same site after 6 months, and the patient
passed away 2 years thereafter (6). By contrast, the other four reported
cases by Behera et al (4),
Khatib et al (5), Ochiai
et al (7) and Čolović et
al (8) were successfully
treated with the R-CHOP regimen, with no recurrences. Similarly,
the patient in the present report was treated with the R-CHOP
regimen and exhibited no recurrence after 6 months.
The present case report provides several key
teaching points that add to the limited existing literature on
scalp PCDLBCL. First, unlike the majority of previously reported
cases that presented as solitary or multiple nodular masses
(5-7),
the patient in the present case report exhibited patchy alopecia
with mild erythema and pruritus, a presentation that may mimic
inflammatory or autoimmune scalp disorders and delay diagnosis.
Second, the immunohistochemical profile in the present case, CD10
positivity with MUM1 negativity, is relatively uncommon in reported
scalp PCDLBCL cases and may suggest biological heterogeneity within
the PCDLBCL-NOS category. Third, despite the aggressive nature
traditionally associated with diffuse large B-cell lymphomas,
early-stage disease confined to the skin responded well to R-CHOP
chemotherapy, resulting in complete clinical remission at six-month
follow-up. Collectively, these findings highlight the need for
heightened clinical suspicion, timely biopsy of atypical alopecic
scalp lesions, and the potential effectiveness of standard systemic
chemotherapy in selected cases.
The present case report has several limitations.
First, although molecular analysis for the BCR-ABL1 fusion gene and
conventional cytogenetic evaluation were performed, both
investigations were conducted at an external medical facility.
Detailed methodological parameters for the RT-PCR assay, including
reagent specifications, primer sequences, and cycling conditions,
were not available, and representative cytogenetic (G-banding)
images could not be retrieved from the external laboratory's
archival system; therefore, these data could not be illustrated or
described in greater technical detail. Second, although
histopathological and immunohistochemical confirmation was
achieved, complete immunohistochemistry image documentation was not
available, as part of the diagnostic evaluation was performed at an
external institution and the original histopathology and
immunohistochemistry image files could not be retrieved. Third,
representative CT scan images could not be included, as the imaging
studies were performed at an external radiology facility and the
original Digital Imaging and Communications in Medicine (DICOM)
files were not accessible. Fourth, some potentially informative
prognostic markers, such as serum lactate dehydrogenase levels and
the Ki-67 proliferation index, were not reported, which may have
provided further insight into disease activity and prognosis.
Finally, comprehensive molecular and cytogenetic profiling relevant
to lymphoma biology, such as fluorescence in situ
hybridization (FISH) for MYC, BCL2 and BCL6 rearrangements,
next-generation sequencing, and formal cell-of-origin
classification using the Hans algorithm, were not performed due to
the limited availability of advanced molecular diagnostic
facilities. Only basic targeted molecular testing (RT-PCR for
BCR-ABL) and conventional karyotyping were available as part of
routine clinical diagnostics.
In conclusion, PCDLBCL should be considered in the
differential diagnosis of scalp lesions, and the R-CHOP regimen
could be an effective treatment option for managing PCDLBCL
cases.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
FHK and SSO were major contributors to the
conception of the study, as well as to the literature search for
related studies. RSA, DOK, HAN and KAN contributed to the clinical
management of the patient, assisted in data acquisition and
interpretation, and participated in the literature review and
manuscript preparation. SQH, SOS and SSA contributed to the
conception and design of the study, the literature review, the
critical revision of the manuscript, and the processing of the
table. RMA was the pathologist who performed the diagnosis of the
case. FHK and RSA confirm the authenticity of all the raw data. All
authors have read and approved the final manuscript.
Ethics approval and consent to
participate
Ethical approval was not required by the
institutional review board for this single case report. Written
informed consent was obtained from the patient for participation in
the study.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of the present case report and any
accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kraft RM, Ansell SM, Villasboas JC,
Bennani NN, Wang Y, Habermann TM, Thanarajasingam G, Lester SC,
Macon W, Inwards DJ, et al: Outcomes in primary cutaneous diffuse
large B-cell lymphoma, leg type. Hematol Oncol. 39:658–663.
2021.PubMed/NCBI View
Article : Google Scholar
|
|
2
|
Krenitsky A, Klager S, Hatch L,
Sarriera-Lazaro C, Chen PL and Seminario-Vidal L: Update in
diagnosis and management of primary cutaneous B-cell lymphomas. Am
J Clin Dermatol. 23:689–706. 2022.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Willemze R, Cerroni L, Kempf W, Berti E,
Facchetti F, Swerdlow SH and Jaffe ES: The 2018 update of the
WHO-EORTC classification for primary cutaneous lymphomas. Blood.
133:1703–1714. 2019.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Behera B, Palit A, Nayak AK, Panigrahi A,
Mishra P and Sethy M: Clinico-dermoscopic-pathological features of
a rare case of locally invasive multifocal primary cutaneous
diffuse large B-cell lymphoma-leg type over the face and scalp.
Indian J Dermatol. 67:283–286. 2022.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Khatib Y, Dande M, Patel RD and Makhija M:
Primary cutaneous large B-cell lymphoma of scalp: Case report of a
rare variant. Indian J Pathol Microbiol. 60:268–271.
2017.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Liao C, Yang M, Liu P and Zhang W: A
92-year-old man with primary cutaneous diffuse large B-cell
non-Hodgkin's lymphoma manifesting as a giant scalp mass: A case
report. Medicine (Baltimore). 96(e6270)2017.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Ochiai H, Kawano H, Miyaoka R, Kawano N,
Shimao Y and Kawasaki K: Primary diffuse large B-cell lymphomas of
the temporoparietal dura mater and scalp without intervening skull
bone invasion: Case report. Neurol Med Chir. 50:595–598.
2010.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Čolović N, Jurišić V and Čolović M:
Rituximab for primary cutaneous large B-cell non-Hodgkin's lymphoma
of the scalp. Arch Oncol. 16:14–15. 2008.
|
|
9
|
Kim MJ, Hong ME, Maeng CH, Jung HA, Hong
JY, Choi MK, Kim SJ, Ko YH and Kim WS: Clinical features and
treatment outcomes of primary cutaneous B-cell lymphoma: A
single-center analysis in South Korea. Int J Hematol. 101:273–278.
2015.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Jia J, Li W and Zheng Y: Primary cutaneous
diffuse large B-cell lymphoma-other successfully treated by the
combination of R-CHOP chemotherapy and surgery: A case report and
review of literature. Medicine. 96(e6161)2017.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Ma XB, Zheng Y, Yuan HP, Jiang J and Wang
YP: CD43 expression in diffuse large B-cell lymphoma, not otherwise
specified: CD43 is a marker of adverse prognosis. Hum Pathol.
46:593–599. 2015.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Whiting DA: Histopathologic features of
alopecia areata: A new look. Arch Dermatol. 139:1555–1559.
2003.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Skala SL, Hristov B and Hristov AC:
Primary cutaneous follicle center lymphoma. Arch Pathol Lab Med.
142:1313–1321. 2018.PubMed/NCBI View Article : Google Scholar
|