Introduction
Heart failure (HF) remains one of the leading causes
of morbidity, mortality and hospitalization worldwide, representing
a substantial and persistent burden on healthcare systems (1). The prevalence of HF continues to rise
due to the aging of the population and improved survival following
cardiovascular events, leading to a growing population of patients
requiring chronic management (2).
This increasing prevalence underscores the urgent need for
effective strategies to mitigate the associated clinical, societal
and economic consequences of HF (1).
In Asia, including Indonesia, the epidemiological
landscape of HF poses distinct challenges, with prevalence rates
remaining high across diverse populations (3). Regional studies have reported
estimates approaching 900 cases per 100,000 population,
highlighting the considerable disease burden within these
communities (4). This impact is
further compounded by region-specific etiological factors,
inequities in healthcare access, and socioeconomic disparities that
influence both disease progression and treatment outcomes.
Consequently, the identification of modifiable determinants of
adverse outcomes, particularly those contributing to prolonged
hospitalization, has become an essential public health and clinical
priority (3).
Among these determinants, the cardiorenal axis has
emerged as a critical pathway influencing the prognosis of patients
with HF. Cardiorenal syndrome, defined by bidirectional dysfunction
between the heart and kidneys, represents a common and deleterious
comorbidity in patients with HF (5). Contemporary registry data confirm
that renal dysfunction is highly prevalent in this population and
serves as an independent predictor of poor outcomes (6). Worsening renal function during
hospitalization has been consistently associated with an extended
length of stay (LOS) in the hospital, increased in-hospital
mortality rates and higher rates of re-hospitalization (7). In addition to renal dysfunction,
right ventricular impairment has been identified as a key
determinant of LOS, reflecting the multifactorial nature of
congestion and organ dysfunction in patients with HF (8).
Echocardiography remains the cornerstone of HF
diagnosis and classification; however, reliance on left ventricular
ejection fraction (LVEF) alone as a prognostic marker has been
increasingly challenged (9). While
LVEF provides essential information on systolic function, its
capacity to predict short-term outcomes, such as LOS or
re-hospitalization is limited. Additionally, there is limited
comparative evidence available evaluating the relative prognostic
value of renal biomarkers versus echocardiographic parameters in
predicting hospital LOS among patients with HF, particularly in low
to middle income settings. This limitation highlights the need to
integrate additional physiological markers, particularly renal
biomarkers, into risk prediction frameworks.
To address this gap, the present study aimed to
directly compare the prognostic performance of routinely measured
renal biomarkers with standard echocardiographic parameters in
predicting hospital LOS among patients admitted with HF.
Furthermore, the present study integrated conventional statistical
modelling with machine learning approaches, thereby enhancing
predictive accuracy and early risk stratification. Such an approach
could inform individualized management, optimize resource
allocation, and support data-driven strategies to improve outcomes
for patients with HF (8,10).
Patients and methods
Study population
The present retrospective study cohort comprised
adult patients admitted to Karsa Husada Hospital, Batu in Indonesia
between January 1, 2024 and May 31, 2025 with a primary diagnosis
of HF. Data were collected from June to July 2025 after ethics
approval for the study had been obtained. Karsa Husada Hospital
serves as a teaching hospital affiliated with the Faculty of
Medicine and Health Sciences, Maulana Malik Ibrahim Islamic State
University Malang.
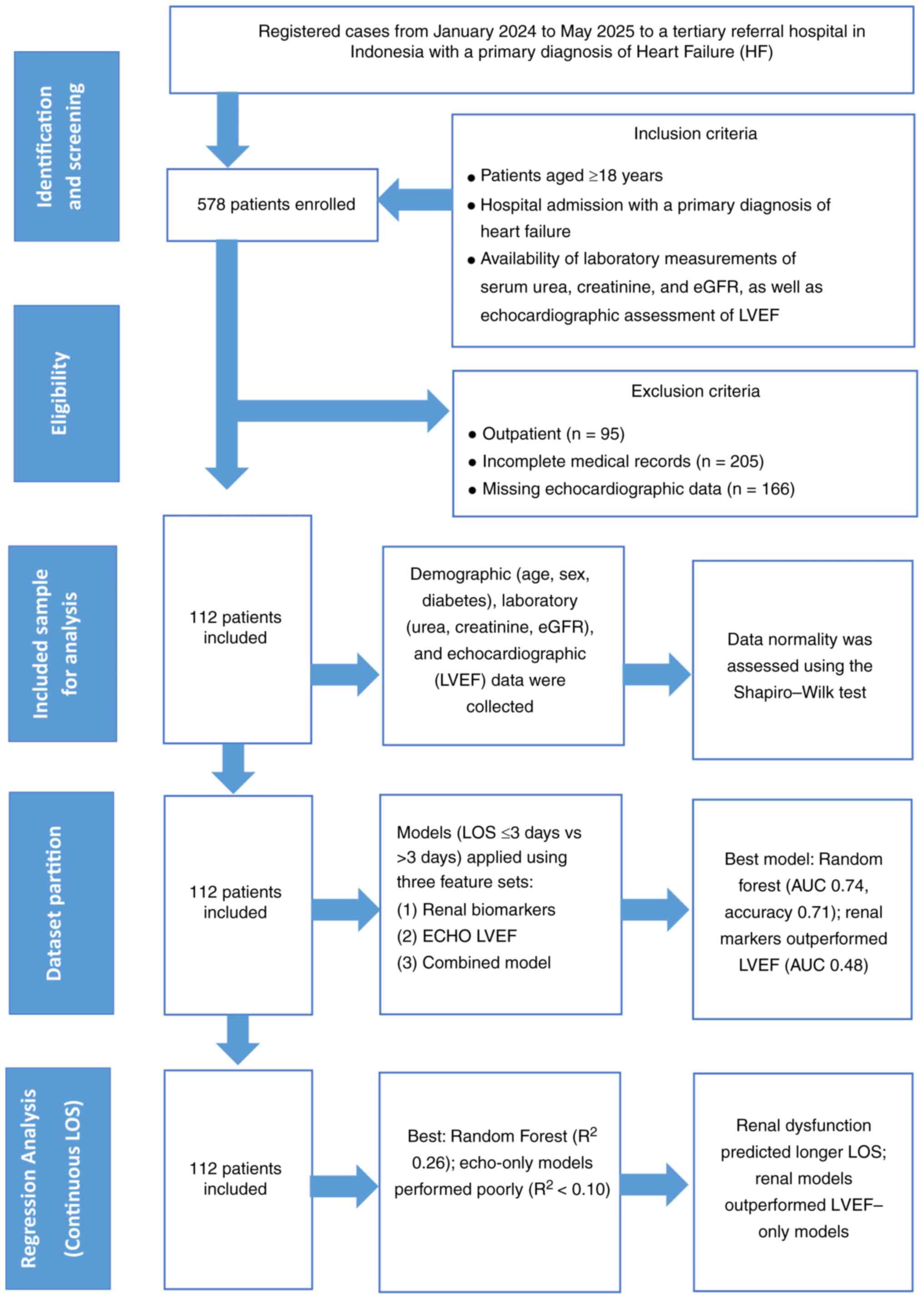
A total of 112 patients met the eligibility criteria
and were included in the final analysis. Patients were included
using a consecutive sampling approach, whereby all eligible
patients meeting the inclusion criteria during the study period
were enrolled sequentially to minimize bias. As the present study
was a retrospective study utilizing all available data within the
study period, no formal sample size calculation was performed. The
inclusion criteria were: i) An age ≥18 years; ii) admission with HF
as the primary diagnosis; and iii) the availability of laboratory
measurements for serum urea, serum creatinine and estimated
glomerular filtration rate (eGFR), along with the echocardiographic
assessment of LVEF. Patients were excluded if essential clinical or
laboratory data were not available, if they were discharged or
transferred within 24 h of admission, or if HF was not the primary
reason for hospitalization. The workflow of patient selection is
depicted in (Fig. 1).
The present study was approved by the Health
Research Ethics Committee of Faculty of Medicine, Maulana Malik
Ibrahim Islamic State University Malang, Indonesia (Approval no.
60/01/EC/KEPK-FKIK/10/2024). Only de-identified medical records
were analyzed, with a waiver of written informed consent granted
due to the retrospective, anonymized data use, and
non-interventional design (Letter no.
009/KEPK.FKIK/KP/XI/2025).
Variables and outcome definition
Demographic variables included age, sex and diabetes
mellitus status (coded as 1 for presence, 0 for absence).
Laboratory parameters consisted of serum urea (mg/dl), serum
creatinine (mg/dl) and eGFR (ml/min/1.73 m2), calculated
using the Modification of Diet in Renal Disease (MDRD) equation.
Echocardiographic assessment included LVEF (%), measured using the
biplane Simpson method in accordance with American Society of
Echocardiography guidelines (11).
LVEF was selected as the primary echocardiographic parameter as it
is the most routinely available and standardized measure across all
patients in clinical practice. Other echocardiographic parameters,
such as right ventricular function or diastolic indices, were not
included due to their inconsistent availability in the dataset. The
primary outcome was hospital LOS, defined as the number of days
from admission to discharge. LOS was analyzed both as a continuous
variable and as a categorical variable dichotomized at the median
value: ≤3 days vs. >3 days. Patients with a hospital LOS >3
days were classified as having a prolonged period of
hospitalization for subsequent descriptive and inferential
analyses.
Statistical analysis
Continuous variables are reported as the mean ±
standard deviation (SD) or median with interquartile range (IQR),
depending on the underlying distribution, while categorical
variables are presented as frequencies and percentages. Normality
was assessed using the Shapiro-Wilk test. Comparisons between
patients with a short (≤3 days) and prolonged (>3 days) LOS were
performed using the Mann-Whitney U test for continuous variables
and the Chi-squared test for categorical variables. A two-tailed
P-value <0.05 was considered to indicate a statistically
significant difference.
For predictive modeling, three feature sets were
evaluated: i) Renal biomarkers alone (serum urea, creatinine and
eGFR); ii) echocardiographic variable alone (LVEF); and iii) a
combined feature set incorporating renal biomarkers, LVEF, age, sex
and diabetes status. Missing values were imputed using the median
of each variable. Prior to modeling, the class distribution of the
outcome variable (LOS ≤3 days vs. >3 days) was assessed. As the
proportion of the two groups was relatively balanced, no resampling
techniques, such as oversampling or undersampling were applied.
Additionally, synthetic data generation methods were not used to
avoid potential overfitting given the relatively small sample size.
The dataset was randomly split into training (70%) and testing
(30%) subsets. To enhance model robustness and reduce variability
associated with a single data split, k-fold cross-validation (k=5)
was performed on the training set. Logistic and linear regression
models were used as baseline approaches due to their
interpretability, while ensemble methods, including random forest
and gradient boosting, were selected to capture non-linear
associations and interactions among variables. Hyperparameter
optimization for random forest and gradient boosting models was
conducted using grid search within the cross-validation framework
to identify optimal parameter combinations. For binary
classification of prolonged LOS, logistic regression (with feature
standardization) and random forest classifiers were applied. Model
performance was quantified using accuracy, area under the receiver
operating characteristic curve (AUC), precision, recall, and
F1-score.
Continuous LOS prediction was performed using linear
regression and random forest regression, with performance metrics
including mean absolute error (MAE), mean squared error (MSE) and
the coefficient of determination (R2). Receiver
operating characteristic (ROC) curves were generated to visualize
classifier performance, and feature importance values were derived
from random forest models. For regression analyses, scatter plots
comparing predicted vs. observed LOS were constructed to evaluate
model fit. All statistical analyses and machine learning workflows
were implemented in Python (pandas, scikit-learn, scipy,
matplotlib). To improve reproducibility, all machine learning
models were implemented with a fixed random_state. Random forest
models were constructed using 100 trees (n_estimators=100) with
default depth settings. Continuous variables were standardized
using z-score normalization prior to logistic regression modelling.
Model performance was evaluated on a held-out test set (30% of the
data), while the remaining 70% was used for training. Overfitting
was assessed by comparing model performance between training and
testing datasets. Given the relatively small sample size, a
parsimonious modelling approach was adopted to balance predictive
performance and generalizability.
Results
Group comparisons
Baseline demographic and laboratory characteristics
stratified by hospital LOS are summarized in (Table I). Patients were evenly distributed
between those discharged within 3 days and those hospitalized for
longer durations. Age (61.1±10.9 vs. 63.4±10.9 years; P=0.28), sex
distribution (65.5 vs. 68.5% male; P=0.74) and the prevalence of
diabetes (22.4 vs. 20.4%; P=0.80) were comparable between the
groups. By contrast, significant differences were observed in renal
function parameters. Patients with prolonged periods of
hospitalization exhibited markedly higher blood urea concentrations
(53.9±39.3 vs. 30.6±18.9 mg/dl; P=0.003) and serum creatinine
levels (1.39±1.16 vs. 0.88±0.52 mg/dl; P=0.001), indicating greater
renal dysfunction. LVEF did not differ significantly between the
groups (44.3±17.0 vs. 46.1±15.3%; P=0.49), suggesting that renal
dysfunction, rather than systolic cardiac performance, was more
strongly associated with prolonged hospitalization.
 | Table IBaseline characteristics of patients
with heart failure stratified by hospital LOS. |
Table I
Baseline characteristics of patients
with heart failure stratified by hospital LOS.
| Characteristic | ≤3 days (mean ±
SD) | >3 days (mean ±
SD) | P-value |
|---|
| Age (years) | 61.14±10.91 | 63.43±10.94 | 0.28 |
| Sex, n (%) | | | |
|
Male | 38 (65.5%) | 37 (68.5%) | 0.74 |
|
Female | 20 (34.5%) | 17 (31.5%) | |
| Diabetes, n (%) | | | |
|
Yes | 13 (22.4%) | 11 (20.4%) | 0.80 |
|
No | 45 (77.6%) | 43 (79.6%) | |
| Urea (mg/dl) | 30.59±18.93 | 53.91±39.27 | 0.003 |
| Creatinine
(mg/dl) | 0.88±0.52 | 1.39±1.16 | 0.001 |
| eGFR (ml/min/1.73
m2) | 100.89±44.80 | 69.89±33.63 | 0.001 |
| LVEF (%) | 46.09±15.26 | 44.26±17.04 | 0.49 |
Classification performance
The data for predictive model performance on the
held-out test sets are presented in Table II. Using only renal biomarkers,
the logistic regression demonstrated modest discrimination
(accuracy, 0.56; AUC, 0.68; 95% CI, 0.58-0.78) with limited recall
(0.38) and F1 score (0.44). By contrast, tree-based ensemble
approaches demonstrated superior discrimination: The random forest
classifier improved accuracy to 0.71 with recall (0.63) and F1
score (0.67) alongside good discrimination (AUC, 0.74; 95% CI,
0.65-0.83) outperforming both logistic regression and gradient
boosting. Gradient boosting achieved a slightly higher AUC of 0.76
(95% CI, 0.67-0.85), although with lower recall (0.56) and F1 score
(0.62). Models trained exclusively on LVEF features exhibited a
poor predictive ability (AUC, 0.48; 95% CI, 0.38-0.58) and low
classification metrics (accuracy, 0.50; F1 score, 0.32). Although
random forest improved recall substantially (0.81), overall
discrimination remained limited, indicating LVEF alone provides
insufficient prognostic information for LOS. Incorporating
additional clinical covariates, including LVEF, age, sex and
diabetes, did not substantially enhance model performance. Logistic
regression exhibited minimal improvement (accuracy, 0.56; AUC,
0.64; 95% CI, 0.54-0.74) while random forest delivered the most
robust and consistent performance (accuracy, 0.71; AUC, 0.68; 95%
CI, 0.58-0.78; F1 score, 0.67), underscoring its superior ability
to leverage multimodal clinical information. From a clinical
perspective, an AUC of 0.74 indicates acceptable discriminative
ability, indicating that the model can correctly distinguish
between patients with prolonged and non-prolonged LOS ~74% of the
time. This level of performance suggests potential utility for
early risk stratification in hospital settings, although it may
still be insufficient as a standalone decision-making tool and
should be interpreted in conjunction with clinical judgment and
other patient-specific factors.
| Table IIPerformance of predictive models for
prolonged hospital LOS in patients with heart failure using
different feature sets. |
Table II
Performance of predictive models for
prolonged hospital LOS in patients with heart failure using
different feature sets.
| Feature set | Model | Accuracy | AUC (95% CI) | Precision | Recall | F1 |
|---|
| Renal | Logistic
regression | 0.56 | 0.68 (0.58-0.78) | 0.55 | 0.38 | 0.44 |
| | Random forest | 0.71 | 0.74 (0.65-0.83) | 0.71 | 0.63 | 0.67 |
| | Gradient
boosting | 0.68 | 0.76
(0.67-0.85) | 0.69 | 0.56 | 0.62 |
| Echocardiography
(LVEF) | Logistic
regression | 0.50 | 0.48
(0.38-0.58) | 0.44 | 0.25 | 0.32 |
| | Random forest | 0.53 | 0.52
(0.42-0.62) | 0.50 | 0.81 | 0.62 |
| Combined (renal +
LVEF + age + sex + diabetes) | Logistic
regression | 0.56 | 0.64
(0.54-0.74) | 0.54 | 0.44 | 0.48 |
| | Random forest | 0.71 | 0.68
(0.58-0.78) | 0.71 | 0.63 | 0.67 |
Regression performance
The results of regression analysis are summarized in
Table III. Using the renal
feature set, the linear regression model predicted LOS with an MAE
of 1.16 days and explained ~10% of the variance
(R2=0.10). The random forest model did not yield
substantial improvement, demonstrating a slightly higher MAE of
1.30 days and a lower R2 of 0.04. Models based solely on
echocardiographic (LVEF) features performed poorly, with both
linear and random forest regressions explaining minimal variance
(R2=0.04 and 0.09, respectively) and achieving
comparable MAE values (1.26-1.27 days). By contrast, incorporating
additional clinical variables in the combined feature set (renal +
LVEF + age + sex + diabetes) modestly enhanced predictive
performance. Linear regression achieved an MAE of 1.24 days
(R2=0.09; 95% CI, 0.00-0.20), whereas the random forest
model improved to an MAE of 1.18 days and R2 of 0.26
(95% CI, 0.11-0.41). Although the overall variance explained
remained modest, the random forest model using combined features
demonstrated the best balance of predictive accuracy and
generalizability across all tested configurations.
| Table IIIRegression model performance for
predicting hospital LOS in patients with heart failure. |
Table III
Regression model performance for
predicting hospital LOS in patients with heart failure.
| Feature set | Model | MAE (days) | MSE (days²) | R² (95% CI) |
|---|
| Renal | Linear
regression | 1.16 | 3.28 | 0.10
(0.00-0.21) |
| | Random forest
regressor | 1.30 | 3.50 | 0.04
(0.00-0.14) |
| Echocardiography
(LVEF) | Linear
regression | 1.26 | 3.51 | 0.04
(0.00-0.14) |
| | Random forest
regressor | 1.27 | 3.34 | 0.09
(0.00-0.20) |
| Combined (renal +
LVEF + age + sex + diabetes) | Linear
regression | 1.24 | 3.32 | 0.09
(0.00-0.20) |
| | Random forest
regressor | 1.18 | 2.70 | 0.26
(0.11-0.41) |
The comparative performance of predictive models and
their graphical summaries are presented in (Fig. 2). The ROC curve for the logistic
regression model trained on the combined clinical, renal, and
echocardiographic feature set (Fig.
2IA) yielded an AUC of 0.64, reflecting modest discriminative
ability. The curve, which plots the true positive rate against the
false positive rate across varying thresholds, lies only slightly
above the diagonal reference line denoting chance-level
classification. This indicates that the model captured limited but
discernible signal within the data, consistent with partial
discrimination between patients with prolonged versus shorter
hospital stays. This implies traditional linear models using
routinely collected variables may have limited utility as
standalone tools for early risk stratification at admission.
 | Figure 2Model performance and feature
importance across clinical, renal, and echocardiographic
predictors. Comparative performance of predictive models using
different feature sets. (A) ROC curve for the logistic regression
model combining clinical, renal, and echocardiographic variables,
showing modest discrimination (AUC, 0.64). This suggests limited
ability of conventional linear models to reliably distinguish
patients at risk of prolonged hospitalization. (B) Feature
importance from the random forest model, identifying age and serum
urea as dominant predictors of prolonged hospitalization. This
highlights the greater prognostic relevance of renal biomarkers
compared with echocardiographic parameters. (C) Association between
predicted and observed LOS derived from the linear regression model
using renal biomarkers, demonstrating weak overall correlation,
indicates that renal function alone cannot fully explain
variability in LOS. (D) ROC curve for the gradient boosting model
trained on renal biomarkers, showing the strongest discrimination
(AUC, 0.76), suggests that advanced models capturing nonlinear
relationships may improve early identification of high-risk
patients. ROC, receiver operating characteristic; LOS, length of
stay. |
Feature importance derived from the random forest
classifier trained on the same combined feature set is shown in
Fig. 2B. Age emerged as the most
influential predictor (Gini importance >0.2), followed by serum
urea concentration and LVEF. Other renal markers, including eGFR
and creatinine, also contributed meaningfully, albeit with lower
relative weights. These results indicate that renal biomarkers and
age primarily drive model predictions, while echocardiographic
indices provide comparatively limited incremental value, reinforces
the clinical relevance of renal function assessment at
admission
The association between the predicted and observed
LOS for the linear regression model based on renal biomarkers is
displayed in Fig. 2C. The red
dashed line represents the line of identity, whereas the blue line
denotes the model's best-fit regression line. The dispersion of
points around the identity line indicates that the model captured
the general direction of the association but with weak correlation,
underscoring that renal parameters alone explain only a fraction of
the variability in LOS among patients with HF, hence is
insufficient to fully explain variability in LOS, highlighting the
multifactorial nature of HF outcomes.
By contrast, the gradient boosting classifier
trained exclusively on renal biomarkers demonstrated markedly
enhanced discrimination (AUC, 0.76) (Fig. 2D). The ROC curve rises
substantially above the diagonal reference line, indicating
improved sensitivity and specificity in identifying patients at
risk of prolonged hospitalization. This suggests that more advanced
models capable of capturing nonlinear relationships may provide
clinically meaningful improvements in identifying high-risk
patients early during hospitalization. Compared with logistic
regression and random forest models, Gradient boosting more
effectively captured nonlinear interactions among renal variables,
resulting in superior predictive accuracy. Collectively, these
findings highlight the prognostic relevance of renal dysfunction
and support the utility of ensemble-based learning approaches for
clinical risk stratification in HF.
Discussion
The present study demonstrated that renal
dysfunction is a key determinant of prolonged periods of
hospitalization in patients with HF, with renal biomarkers
consistently outperforming echocardiographic parameters in
predicting LOS. These findings are consistent with previous
evidence indicating that worsening renal function (WRF) is common
in acute HF and correlates with longer LOS. Emmens et al
(12) reported that LOS increased
from 2.2 to 4.2 days in patients with WRF. Similarly, a
cross-sectional study found that 33.7% of patients with HF with
reduced ejection fraction (HFrEF) developed WRF, which was
associated with longer hospitalization and higher mortality
(13). Collectively, these data
highlight renal function as a critical determinant of hospital stay
duration.
The association between renal dysfunction and
prolonged hospital LOS involves the complex pathophysiology of the
cardiorenal interaction. In HF, reduced cardiac output and elevated
venous congestion lead to decreased renal perfusion and increased
renal interstitial pressure, impairing glomerular filtration. The
activation of the neurohormonal system, including the
renin-angiotensin-aldosterone system and sympathetic nervous
system, further exacerbates sodium and water retention, promoting
volume overload and diuretic resistance. Additionally, systemic
inflammation and endothelial dysfunction contribute to
microvascular impairment within the kidneys. These mechanisms
create a self-perpetuating cycle in which cardiac dysfunction
worsens renal function and vice versa, ultimately prolonging
decongestion time and LOS (5,14).
In the present study, predictive modeling further
demonstrated that renal biomarkers provided stronger discriminatory
power than echocardiographic parameters such as LVEF. By contrast,
LVEF demonstrated a limited predictive value for LOS. These
findings are in agreement with those of previous research
demonstrating that WRF combined with persistent congestion
contributes to longer hospitalizations and poorer outcomes
(15). While LVEF reflects left
ventricular systolic function, it does not adequately capture the
hemodynamic complexity of HF, particularly congestion status, right
ventricular dysfunction, or filling pressures, which are more
directly related to hospitalization duration (16,17).
AlShammari et al (18) also
reported that 27% of patients with HF experienced WRF, which was
associated with prolonged periods of hospitalization and increased
complications. Taken together, these results suggest that renal
function on admission reflects acute pathophysiological changes
more accurately than LVEF alone.
Herein, the addition of demographic or clinical
variables such as age, sex and diabetes did not meaningfully
improve model performance. LVEF, despite its traditional role in HF
stratification, exhibited limited predictive value. Schmitt et
al (16) similarly observed
that LVEF categories, reduced ejection fraction, mildly reduced
ejection fraction, or preserved ejection fraction, did not
consistently predict LOS or short-term mortality. Tarekegn et
al (19) also found that
demographic factors had minimal influence, whereas clinical
features including edema, hepatomegaly and pleural effusion were
stronger predictors. These findings reinforce that structural
parameters alone may not adequately capture hospitalization
risk.
The application of machine learning models in the
present study further highlights the prognostic value of renal
biomarkers. Tree-based ensemble methods, particularly random forest
and gradient boosting, demonstrated superior performance compared
to logistic regression, likely due to their ability to capture
non-linear association and complex feature interaction. These
findings are in line with those of recent studies which have
demonstrated improved predictive performance when incorporating
multidimensional clinical data, particularly laboratory parameters,
in machine learning (20,21). To the best of our knowledge, the
present study is among the first to directly compare the predictive
performance of renal biomarkers and echocardiographic parameters
using both conventional statistical methods and machine learning
approaches in the Indonesian population. This is particularly
important given regional differences in patient characteristics,
healthcare access and disease prevention, which may limit the
generalizability of findings from high-income settings.
Feature importance analysis confirmed that renal
biomarkers, particularly urea, creatinine and eGFR, along with age,
were dominant predictors of LOS, while LVEF contributed minimally.
This underscores the importance of assessing renal function at
admission for early risk stratification. This finding was
consistent with the findings of the study by Ignatavičiūtė et
al (22), in which an eGFR ≤50
ml/min/1.73 m2 independently predicted LOS >9 days in
acute HF. Elmaghawry et al (23) also demonstrated that the WATCH-DM
score, which includes renal function and age, accurately predicted
longer hospitalization among patients with HF and diabetes (AUC
0.93). Integrating renal parameters into risk assessment therefore
provides prognostic value beyond conventional measures.
Although renal biomarker-based models exhibited
optimal performance, their predictive power remained modest
(R2<0.30), suggesting that other factors contribute
to LOS. These may include hemodynamic instability, congestion
severity, right ventricular dysfunction and comorbidities.
Ignatavičiūtė et al (22)
identified elevated N-terminal pro-B-type natriuretic peptide
(NT-proBNP), low systolic pressure and significant tricuspid
regurgitation as independent predictors for a prolonged LOS.
Similarly, Tarekegn et al (19) found that edema, hepatomegaly and
pleural effusion were stronger determinants than demographic
characteristics. Thus, while renal dysfunction plays a key role, it
forms part of a multifactorial pathway influencing hospitalization
duration.
Clinically, these findings emphasize the importance
of early renal function assessment as part of a comprehensive risk
stratification of patients with HF. Routine measurements of urea,
creatinine and eGFR may help identify patients who are at a higher
risk for prolonged hospitalization and guide timely interventions.
Future multicenter prospective studies are required to evaluate
whether interventions targeting renal dysfunction, such as
optimized diuretic therapy, NT-proBNP-guided management, or
multiparametric risk scores such as WATCH-DM, can shorten LOS and
improve outcomes (23). Including
socioeconomic factors, treatment adherence and advanced
echocardiographic parameters, such as right ventricular function
and filling pressures may further enhance predictive accuracy.
Integrating renal biomarkers with clinical and social determinants
could support a more holistic approach to modern HF management
(18).
The present study has limitations which should be
mentioned. The sample size was modest, derived from a single
center, and no formal sample size calculation was performed which
may limit generalizability and may introduce potential selection
bias, as the study population may not fully represent the broader
spectrum of patients with HF in different healthcare settings.
Furthermore, the relatively small sample size may have limited the
robustness and generalizability of the machine learning models. Its
retrospective design precludes causal inference, and unmeasured
confounders could have influenced the results. Echocardiographic
variables beyond LVEF, such as right ventricular function or
filling pressures, were unavailable and may have restricted the
ability to fully assess the contribution of cardiac structure and
hemodynamics to LOS. In addition, the absence of external
validation limits the ability to confirm the generalizability of
the predictive models across different populations. Despite
imputation, missing data could have introduced bias. In addition,
although machine learning models were applied, the relatively small
sample size limited the use of more complex optimization
strategies, and model performance should be interpreted with
caution. External validation in larger multicenter cohorts is
warranted.
In conclusion, in the present study, renal
dysfunction was found to be significantly associated with prolonged
periods of hospitalization among patients with HF. Predictive
modeling demonstrated that renal biomarkers outperformed
echocardiographic indices such as LVEF in predicting LOS. Among the
evaluated models, Random forest using renal features achieved the
strongest overall performance (AUC, 0.74; R2=0.26).
Collectively, these findings highlight the importance of renal
function markers in refining risk stratification for LOS and should
be prioritized during hospital admission for patients with HF to
enable early risk stratification and guide targeted clinical
management. While these findings highlight the clinical utility of
renal biomarkers, further multicenter validation is required before
widespread implementation.
Acknowledgements
The authors wish to express their sincere gratitude
to the healthcare workers at Karsa Husada General Hospital and the
faculty members of the Faculty of Medicine and Health Sciences,
Maulana Malik Ibrahim Islamic State University Malang, for their
valuable assistance and support throughout the research.
Funding
Funding: No funding was received.
Availability of data and materials
The data that support the findings of this study are
not publicly available due to confidentiality concerns, as they
contain patient identities and hospital medical records. Access to
the data is restricted to the corresponding author and the
institutional medical data committee. Data may be made available to
other parties only upon formal request and with written approval
from the hospital ethics or data committee. Requests should be
directed to the corresponding author via email.
Authors' contributions
NFA led the conceptualization, data curation, formal
analysis, investigation, methodology development, software
implementation, validation, visualization and drafting of the
manuscript. AZA contributed to formal analysis, methodology,
project administration and resources. IRA participated in the
conceptualization of the study, methodology development, project
administration, data interpretation, resource provision and in the
revision of the manuscript. AH contributed to data interpretation,
methodology development and critical revision of the manuscript. DS
contributed to the conceptualization of the study, data
investigation, validation and in the critical revision of the
manuscript. MNDA, FA and AP assisted with data curation,
visualization and the drafting of the initial manuscript. SPW
contributed to data investigation and study supervision. MH oversaw
the formal analysis, methodology, funding acquisition, supervision,
validation, and the critical reviewing and editing of the
manuscript. NFA and MH confirm the authenticity of all the raw
data. All authors have read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
The present study was approved by the Health
Research Ethics Committee of Faculty of Medicine, Maulana Malik
Ibrahim Islamic State University Malang, Indonesia (Approval no.
60/01/EC/KEPK-FKIK/10/2024). Only de-identified medical records
were analyzed, with a waiver of written informed consent granted
due to the retrospective, anonymized data use, and
non-interventional design (Letter No.
009/KEPK.FKIK/KP/XI/2025).
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Savarese G, Becher PM, Lund LH, Seferovic
P, Rosano GMC and Coats AJS: Global burden of heart failure: A
comprehensive and updated review of epidemiology. Cardiovasc Res.
118:3272–3287. 2022.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Vaduganathan M, Claggett BL, Inciardi RM,
Fonarow GC, McMurray JJV and Solomon SD: Estimating the benefits of
combination medical therapy in heart failure with mildly reduced
and preserved ejection fraction. Circulation. 145:1741–1743.
2022.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Feng J, Zhang Y and Zhang J: Epidemiology
and burden of heart failure in asia. JACC Asia. 4:249–264.
2024.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Tromp J and Teng THK: Regional differences
in the epidemiology of heart failure. Korean Circ J.
54(591)2024.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Rangaswami J, Bhalla V, Blair JEA, Chang
TI, Costa S, Lentine KL, Lerma EV, Mezue K, Molitch M, Mullens W,
et al: Cardiorenal syndrome: Classification, pathophysiology,
diagnosis, and treatment strategies: A scientific statement from
the american heart association. Circulation. 139:E840–E878.
2019.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Tang WHW, Bakitas MA, Cheng XS, Fang JS,
Fedson SE, Fiedler AG, Martens P, McCallum WI, Ogunniyi MO,
Rangaswami J, et al: Evaluation and management of kidney
dysfunction in advanced heart failure: A scientific statement from
the American heart association. Circulation. 150:e280–e295.
2024.PubMed/NCBI View Article : Google Scholar
|
|
7
|
Janse RJ, Milders J, Rotmans JI, Caskey
FJ, Evans M, Torino C, Szymczak M, Drechsler C, Wanner C, Pippias
M, et al: Predicting hospitalization and related outcomes in
advanced chronic kidney disease: A systematic review, external
validation, and development study. Kidney Med.
7(101016)2025.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Palazzuoli A, Dini FL, Pugliese NR, Ruocco
G, Severino P, Vizza D, Carbonara R, Passantino A and Carluccio E:
Right ventricular–pulmonary artery uncoupling and strain in acute
heart failure. J Am Heart Association. 14(e039858)2025.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Adamczak DM, Oduah MT, Kiebalo T,
Nartowicz S, Bęben M, Pochylski M, Ciepłucha A, Gwizdała A, Lesiak
M and Straburzyńska-Migaj E: Heart failure with preserved ejection
fraction-a concise review. Curr Cardiol Rep. 22(82)2020.PubMed/NCBI View Article : Google Scholar
|
|
10
|
van der Stam JA, Bouwmeester S, van Loon
SLM, vanRiel NAW, Dekker LR, Boer AK, Houthuizen P and Scharnhorst
V: Prognostic value of combined biomarkers in patients with heart
failure: The heartmarker score. Ann Lab Med. 43:253–262.
2023.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Lang RM, Badano LP, Mor-Avi V, Afilalo J,
Armstrong A, Ernande L, Flachskampf FA, Foster E, Goldstein SA,
Kuznetsova T, et al: Recommendations for cardiac chamber
quantification by echocardiography in adults: An update from the
American society of echocardiography and the european association
of cardiovascular imaging. J Am Soc Echocardiogr. 28:1–39.e14.
2015.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Emmens JE, ter Maaten JM, Matsue Y,
Figarska SM, Sama IE, Cotter G, Cleland JGF, Davison BA, Felker GM,
Givertz MM, et al: Worsening renal function in acute heart failure
in the context of diuretic response. Eur J Heart Fail. 24:365–374.
2022.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Asbagh AG, Sadeghi MT, Ramazanilar P and
Nateghian H: Worsening renal function in hospitalized patients with
systolic heart failure: Prevalence and risk factors. ESC Heart
Fail. 10:2837–2842. 2023.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Damman K and Testani J: Cardiorenal
interactions in heart failure: Insights from recent therapeutic
advances. Cardiovasc Res. 120:1372–1384. 2024.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Cooper L, DeVore A, Cowger J, Pinney S,
Baran D, DeWald TA, Burt T, Pietzsch TB, Walton A, Aaronson K and
Shah P: Patients hospitalized with acute heart failure, worsening
renal function, and persistent congestion are at high risk for
adverse outcomes despite current medical therapy. Clin Cardiol.
46:1163–1172. 2023.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Schmitt A, Behnes M, Weidner K,
Abumayyaleh M, Reinhardt M, Abel N, Lau F, Forner J, Ayoub M,
Mashayekhi K, et al: Prognostic impact of prior LVEF in patients
with heart failure with mildly reduced ejection fraction. Clin Res
Cardiol. 114:570–588. 2025.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Epelde F: Heterogeneity in heart failure
with preserved ejection fraction: A systematic review of phenotypic
classifications and clinical implications. J Clin Med.
14(4820)2025.PubMed/NCBI View Article : Google Scholar
|
|
18
|
AlShammari A, Magdits M, Majdalani R,
Devarajan S, Hughes A, McCann L, Ionescu N and Raiszadeh F: Heart
failure and worsening renal function: Prevalence, risk factors, and
impact on hospital readmissions in an urban minority population. J
Clin Med. 14:2025.PubMed/NCBI View Article : Google Scholar
|
|
19
|
Tarekegn GY, Wondm SA, Tamene FB, Anberbr
SS, Moges TA, Dagnew SB, Zeleke TK and Dagnew FN: Determinant
factors of prolonged hospitalization in acute heart failure
patients at jimma medical center, southwest ethiopia. Sci Rep.
15(11670)2025.PubMed/NCBI View Article : Google Scholar
|
|
20
|
Xie Y and Zhang L, Sun W, Zhu Y, Zhang Z,
Chen L, Xie M and Zhang L: Artificial intelligence in diagnosis of
heart failure. J Am Heart Association. 14(e039511)2025.PubMed/NCBI View Article : Google Scholar
|
|
21
|
Gautam N, Mueller J, Alqaisi O, Gandhi T,
Malkawi A, Tarun T, Alturkmani HJ, Zulqarnain MA, Pontone G and
Al'Aref SJ: Machine learning in cardiovascular risk prediction and
precision preventive approaches. Curr Atheroscler Rep.
25:1069–1081. 2023.PubMed/NCBI View Article : Google Scholar
|
|
22
|
Ignatavičiūtė E, Žaliaduonytė D and
Zabiela V: Prognostic factors for prolonged in-hospital stay in
patients with heart failure. Medicina (Kaunas).
59(930)2023.PubMed/NCBI View Article : Google Scholar
|
|
23
|
Elmaghawry ML, Mabrouk RRA, Shereef SA and
El-Shetry SM: Length of hospital stay in acute heart failure with
type 2 diabetes mellitus: Forecasting Using WATCH-DM Score. Heart
Failure Journal of India. 2:90–96. 2024.
|