Introduction
Resveratrol
(3,4′,5-trihydroxy-trans-stilbene) is a polyphenolic
phytoalexin that is naturally produced in plants as a response to
injuries or stresses, such as a pathogenic attack or irradiation
with ultraviolet light. This compound is found in grapes, peanuts,
berries, groundnut, spruce, mulberries and dried roots of
Polygonum cuspidatum (also known as kojo-kon in Japanese),
which have long been used in traditional oriental medicine
(1,2). In plants, resveratrol inhibits the
development of an infection (3). In
humans, it has several beneficial effects due to its antioxidant,
anti-inflammatory, anticarcinogenic, antidiabetic,
cardioprotective, estrogenic and anti-aging properties (4–6).
Resveratrol is widely available in the human diet, although
exposure to this substance is enhanced upon ingestion of grapes,
red wine and peanuts (4–13). It has been intensively studied in
clinical and nonclinical trials, and was found to act on a number
of different targets using various mechanisms of action that can
explain its diverse biological activities, including: Free-radical
scavenging activity (14),
anti-inflammatory activity (5,9,11,12,14,15),
prevention of tumour growth and anticancer activity (6–9,16), estrogenic activity (11), inhibition of lipid peroxidation,
modulation of lipid metabolism (9),
chelation of copper and inhibition of platelet aggregation
(9,13).
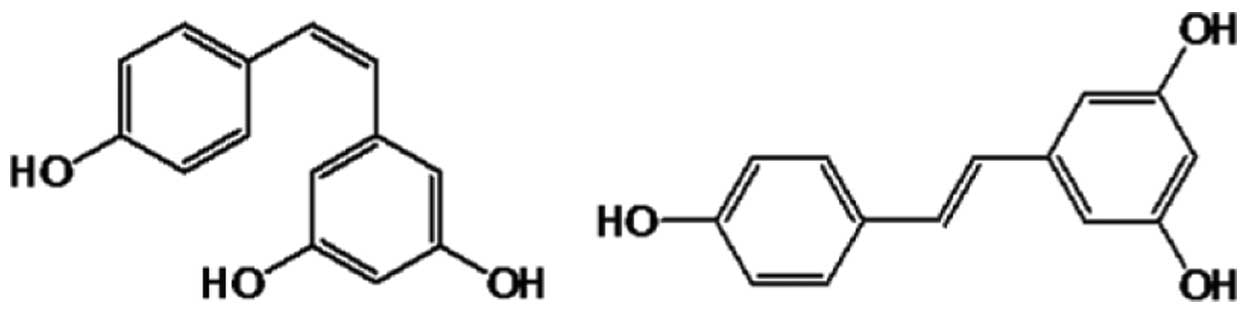
Resveratrol exists as two geometric isomers:
Cis and trans (Fig. 1)
(8,9). The trans form is able to undergo
isomerization into the cis form upon exposure to ultraviolet
irradiation (9). Although the two
isomers often exist in combination, the trans form is more
biologically active and more frequently investigated (8,9,17,18). Red
wine is known to contain a high concentration of
trans-resveratrol. The levels of trans- and
cis-resveratrol in 26 wines were evaluated by Gu et
al in 1999 (17), and
trans-resveratrol levels ranged between 0.987 and 25.4
µmol/l, while cis-resveratrol levels were considerably
lower.
Previous in vitro data have shown that 5
µmol/l resveratrol is the minimum concentration required for the
chemopreventive effects of the compound to be elicited (15). Following oral administration in
humans, 75% of resveratrol is absorbed, possibly by transepithelial
diffusion. However, oral bioavailability is low (<1%) due to
rapid and extensive metabolism in the intestine and liver (18,19).
These levels are maintained even after repeated or increased dosage
administration. The major metabolites identified in the plasma and
urine by metabolic studies are resveratrol glucuronides and
sulphates (20–22). Other metabolites of resveratrol have
been reported in the literature, including reduced
dihydro-resveratrol conjugates and other unknown highly polar
products (21,23). As already mentioned, the major sites
of metabolism are the intestine and liver; however, colonic
bacterial metabolism may be an important metabolic pathway
(24). The efficacy of resveratrol
at the target site may be enhanced by deconjugating enzymes, such
as β-glucuronidase and sulphatase, as well as by specific tissue
accumulation of resveratrol (24).
Lu et al (25) showed that
resveratrol is delivered as a stable sulphate conjugated form to
the target tissues, where the parent compound is gradually
regenerated and provides the beneficial in vivo effects. The
activities of the metabolites have also been investigated. The
metabolites were found to be pharmacologically active and thus are
considered to contribute to the in vivo biological effects
of the parent compound (6,25).
Considering all the beneficial effects of
resveratrol on human health, drug supplements containing
resveratrol have been developed. The aim of the present study was
to assess the pharmacokinetic properties and safety of resveratrol
following a 500 mg single oral dose (one Evelor 500 mg tablet;
Agetis Supplements Ltd., Limassol, Cyprus) administered to fasting
healthy male and female subjects. In order to evaluate the
bioavailability of resveratrol, plasma concentration-time curves of
the parent compound and its metabolites (glucuronides, sulphates
and mixed conjugates) were used to assess the rate and extent of
absorption.
Materials and methods
Study design
The study was an open label, one period, one
sequence, noncontrolled, bioavailability study of 500 mg
resveratrol, which was performed on healthy male and female
volunteers under fasting conditions. The study was approved by an
independent Ethics Committee (County Ethics Committee for Drug
Clinical Studies, Suceava, Romania) and was performed respecting
the Good Clinical Practice requirements. A written informed consent
was obtained from each subject prior to participation in the
study.
Study population
A total of 15 healthy male and female subjects, with
an age of 18–55 years and body mass index (BMI) of 20–30
kg/m2, were enrolled in the study. Demographic
characteristics are presented in Table
I. The subjects were selected based on the following
eligibility criteria: Normal physical examination, vital signs and
laboratory screening results within normal ranges, willingness to
abstain from specific aliments and drink beverages, ability to
understand the full nature and purpose of the study, and
nonpregnant and nonlactating women. The exclusion criteria included
the following: History of hypersensitivity to the test substance
and to the inactive ingredients, hospitalization for any reason or
donation of blood (≥450 ml) within 8 weeks prior to the initiation
of the study, intake of any drugs within 2 weeks prior to or during
the study, history or presence of any relevant medical condition,
history of drug or alcohol abuse, and subjects that were vegetarian
or followed a particular diet.
 | Table I.Demographic characteristics of the
study population. |
Table I.
Demographic characteristics of the
study population.
| Subject no. | Gender | Age (years) | Weight (kg) | Height (cm) | BMI |
|---|
| 1 | M | 31 | 98 | 185 | 28.6 |
| 2 | M | 22 | 79 | 182 | 23.8 |
| 3 | M | 46 | 73 | 178 | 23.0 |
| 4 | M | 36 | 75 | 176 | 24.2 |
| 5 | F | 35 | 52 | 160 | 20.3 |
| 6 | F | 49 | 49 | 150 | 21.8 |
| 7 | F | 33 | 65 | 170 | 22.5 |
| 8 | F | 27 | 62 | 162 | 23.6 |
| 9 | F | 50 | 90 | 174 | 29.7 |
| 10 | F | 29 | 55 | 165 | 20.2 |
| 11 | M | 36 | 68 | 170 | 23.5 |
| 12 | M | 19 | 72 | 185 | 21.0 |
| 13 | M | 20 | 69 | 173 | 23.1 |
| 14 | M | 19 | 67 | 180 | 20.7 |
| 15 | M | 19 | 62 | 172 | 21.0 |
Three days prior to the study and until the end of
the study period (24 h post-dose), the volunteers kept a strict
diet. The subjects did not consume aliments or beverages with a
high content of resveratrol, including red/black fruit, kiwi,
red/black grapes, peanuts, nuts and red wine. In addition, the diet
was strictly controlled during the entire confinement period. The
subjects received standard light meals that avoided aliments
containing high quantities of resveratrol.
Resveratrol dose
The test product used in the present study was
Evelor 500 mg tablets (containing trans-resveratrol), which were
obtained from Agetis Supplements Ltd. These tablets were
manufactured under the Good Manufacturing Practice guidelines and
according to a patented procedure (26).
Each subject received one 500-mg tablet of Evelor
subsequent to overnight fasting. Evelor was administered orally
with 200 ml water under the direct observation of the clinical
investigator.
Sample preparation
During the treatment day, about 5 ml venous blood
samples were drawn in labelled tubes containing lithium heparin as
an anticoagulant (Monovettes®; Sarstedt, Nümbrecht, Germany), at
the following time points: Prior to resveratrol administration, and
at 0.083, 0.167, 0.33, 0.5, 0.75, 1.0, 2.0, 3.0, 4.0, 5.0, 6.0,
7.0, 8.0, 10.0, 12.0, 16.0 and 24.0 h after resveratrol
administration.
Each blood sample containing heparin was immediately
centrifuged at 1,500 × g for 5 min at 4°C. The plasma was separated
and placed in duplicate labelled test tubes (two aliquots per
sample). Subsequently, the test tubes were securely closed, and the
plasma samples were racked, frozen and stored at −20°C or cooler
until tested.
Bioanalytical method
The identification and quantification of resveratrol
and its metabolites in plasma was performed by high performance
liquid chromatography (HPLC) (27)
with detection by tandem mass spectrometry (MS/MS), using a triple
quadrupole AB-Sciex model API 4000 mass spectrometer (AB Sciex,
Ontario, Canada), equipped with an atmospheric pressure
electrospray ionization interface. Analyses were performed on a
multiplexing HPLC system controlled by Cohesive Aria software
(Thermo Fisher Scientific, San Jose, CA, USA) and composed by two
binary chromatographic pumps (Agilent 1100 Series, Agilent
Technologies, Santa Clara, CA, USA) and an HTS PAL autosampler (CTC
Analytics, Zwingen, Switzerland). Data were acquired in negative
ions mode using a multiple reaction monitoring method (27).
Chromatographic separations were performed on
Discovery HSC18 chromatographic columns (100 × 2.1 mm, 5 µm;
Supelco, Sigma-Aldrich, Bellefonte, PA, USA). For data acquisition
and processing, the Analyst software (version 1.6; AB Sciex) was
used.
The analytical standard of resveratrol used to
prepare the calibration curves and quality control samples was
purchased from Sigma-Aldrich. The internal standard added during
extraction (resveratrol-13C6) was obtained from TLC Pharmaceutical
Standards, Ltd. (Vaughan, Ontario, Canada)
Pharmacokinetic parameters
The parameters calculated for resveratrol and the
metabolites using a noncompartmental approach were as follows:
AUC0-t, which is the area under the curve that was
integrated (by the trapezoidal rule) from the plasma concentrations
between time 0 h and the last quantifiable sample; Cmax,
which is the maximum plasma concentration, obtained directly from
the data without interpolation; Tmax, which is the time
to reach the Cmax, obtained directly from the data
without interpolation; AUC0-inf, which is the area under
the curve that was integrated from the blood concentrations by
extrapolation of the terminal elimination period; % extrapolated
AUC, which is the ratio of (AUC0-inf -
AUC0-t)/AUC0-inf × 100;
T1/2, which is the plasma half life,
calculated as 0.693/elimination rate constant; MRT, which is the
mean residence time, calculated as
AUMCinf/AUC0-inf, where AUMCinf is
the area under the moment curve.
Safety assessment
Safety assessments were then performed. In
particular, adverse events were monitored from the screening visit
for the entire duration of the study. Screening and follow-up
safety tests included physical examinations, electrocardiograms and
investigation of clinical laboratory parameters, including
hematology (red cells, hemoglobin, hematocrit, white cells,
differential count and platelet count), clinical chemistry (uric
acid, total nitrogen, glucose, creatinine, total bilirubine,
aspartate transaminase, alanine transaminase, total cholesterol and
triglyceride levels) and urinalysis examinations. Vital signs were
also evaluated, including the sitting systolic arterial pressure,
diastolic arterial pressure and heart rate. Pre-dose safety
evaluation included analysis of the blood glucose levels, vital
signs (in laying position), oxygen saturation and body
temperature.
Statistical analysis
Bioavailability and statistical calculations were
performed using the SAS software (version 9.1; SAS Analytical
Solutions S.R.L., Bucharest, Romania). Descriptive statistics was
performed for all parameters [arithmetic mean, harmonic mean,
geometric mean, standard error of mean, standard deviation (SD),
median and range]. Mean comparisons for the safety data were
conducted using analysis of variance testing, with P<0.05
considered to indicate a statistically significant difference.
Results
Patient characteristics
All volunteers that were enrolled completed the
study. The demographic characteristics of the subjects included in
the present study are presented in Table
I. The mean age of the patients was 31.40±10.80 years (age
range, 19–50 years), the mean weight was 69.07±13.22 kg (weight
range, 49–98 kg), the mean height was 172.13±9.80 cm (height range,
150–185 cm), and the mean BMI value was 23.13±2.79 (BMI range,
20.2–29.7). Mean values are presented as the mean ± SD.
Pharmacokinetic parameters
The pharmacokinetic parameters for resveratrol and
its metabolites (glucuronides, sulphates and mixed conjugates)
following oral administration of a single dose of 500 mg
resveratrol were determined based on the plasma levels from 15
healthy volunteers.
The results indicated that the pharmacokinetic
parameters for free resveratrol were as follows: Cmax,
71.18 ng/ml; Tmax, 1.3 h; and AUC0-inf, 179.1
ng/ml. The mean pharmacokinetic characteristics for resveratrol are
presented in the Table II
| Table II.Mean pharmacokinetic characteristics
of free resveratrol. |
Table II.
Mean pharmacokinetic characteristics
of free resveratrol.
| Value | Cmax
(ng/ml) | Tmax
(h) | AUC0-t
(ng/ml/h) | AUC0-inf
(ng/ml/h) | AUC extra% | T1/2
(h) | MRT (h) |
|---|
| Mean | 71.181 |
1.339 | 154.545 | 179.074 | 13.303 |
5.114 |
7.064 |
| SD | 42.431 |
1.297 |
67.250 |
79.151 |
7.572 |
4.185 |
4.279 |
| CV | 59.609 | 96.867 |
43.515 |
44.200 | 56.922 | 81.827 | 60.571 |
In the case of sulphated resveratrol, the
Cmax of 1,516.01 ng/ml was reached within 2.8 h
(Tmax) and the AUC0-inf was found to be
14,441.7 ng/ml. The mean pharmacokinetic characteristics of
sulphated resveratrol are listed in the Table III.
| Table III.Mean pharmacokinetic characteristics
of sulphated resveratrol. |
Table III.
Mean pharmacokinetic characteristics
of sulphated resveratrol.
| Value | Cmax
(ng/ml) | Tmax
(h) | AUC0-t
(ng/ml/h) | AUC0-inf
(ng/ml/h) | AUC extra% | T1/2
(h) | MRT (h) |
|---|
| Mean | 1,516.014 |
2.783 | 12,020.275 | 14,441.755 | 12.288 |
8.397 | 11.971 |
| SD |
639.020 |
1.544 |
4,835.531 |
7,593.180 | 11.332 |
5.107 |
5.649 |
| CV |
42.151 | 55.459 |
40.228 |
52.578 | 92.213 | 60.822 | 47.186 |
With regards to glucuronated resveratrol, the
Cmax was 4,083.90 ng/ml and this was reached within 3.0
h (Tmax), while the AUC0-inf value was
39,732.4 ng/ml. The mean pharmacokinetic characteristics of
glucuronated resveratrol are presented in the Table IV.
| Table IV.Mean pharmacokinetic characteristic
of glucuronated resveratrol. |
Table IV.
Mean pharmacokinetic characteristic
of glucuronated resveratrol.
| Value | Cmax
(ng/ml) | Tmax
(h) | AUC0-t
(ng/ml/h) | AUC0-inf
(ng/ml/h) | AUC extra% | T1/2
(h) | MRT (h) |
|---|
| Mean | 4,083.900 |
3.050 | 33,535.028 | 39,732.442 | 12.226 |
7.815 | 12.081 |
| SD | 1,704.447 |
2.172 |
9,781.198 | 16,145.561 | 10.775 |
4.142 |
4.895 |
| CV |
41.736 | 71.202 |
29.167 |
40.636 | 88.129 | 53.004 | 40.522 |
Furthermore, the pharmacokinetic parameters of mixed
conjugates (glucuronide and sulphate metabolites) were also
considered, and their values were reported as follows:
Cmax, 5,440.4 ng/ml; Tmax, 3.2 h; and
AUC0-inf, 63,536.6 ng/ml. The mean pharmacokinetic
characteristics for mixed metabolites are presented in the Table V.
| Table V.The mean pharmacokinetic
characteristic of sulphated and glucuronated resveratrol (mixed
conjugates). |
Table V.
The mean pharmacokinetic
characteristic of sulphated and glucuronated resveratrol (mixed
conjugates).
| Value | Cmax
(ng/ml) | Tmax
(h) | AUC0-t
(ng/ml/h) | AUC0-inf
(ng/ml/h) | AUC extra% | T1/2
(h) | MRT (h) |
|---|
| Mean | 5,440.383 |
3.200 | 50,668.459 | 63,536.643 | 15.691 |
9.244 | 14.035 |
| SD | 2,101.507 |
2.007 | 14,130.030 |
27,641.662 | 13.093 |
5.448 |
6.611 |
| CV |
38.628 | 62.723 |
27.887 |
43.505 | 83.443 | 58.937 | 47.108 |
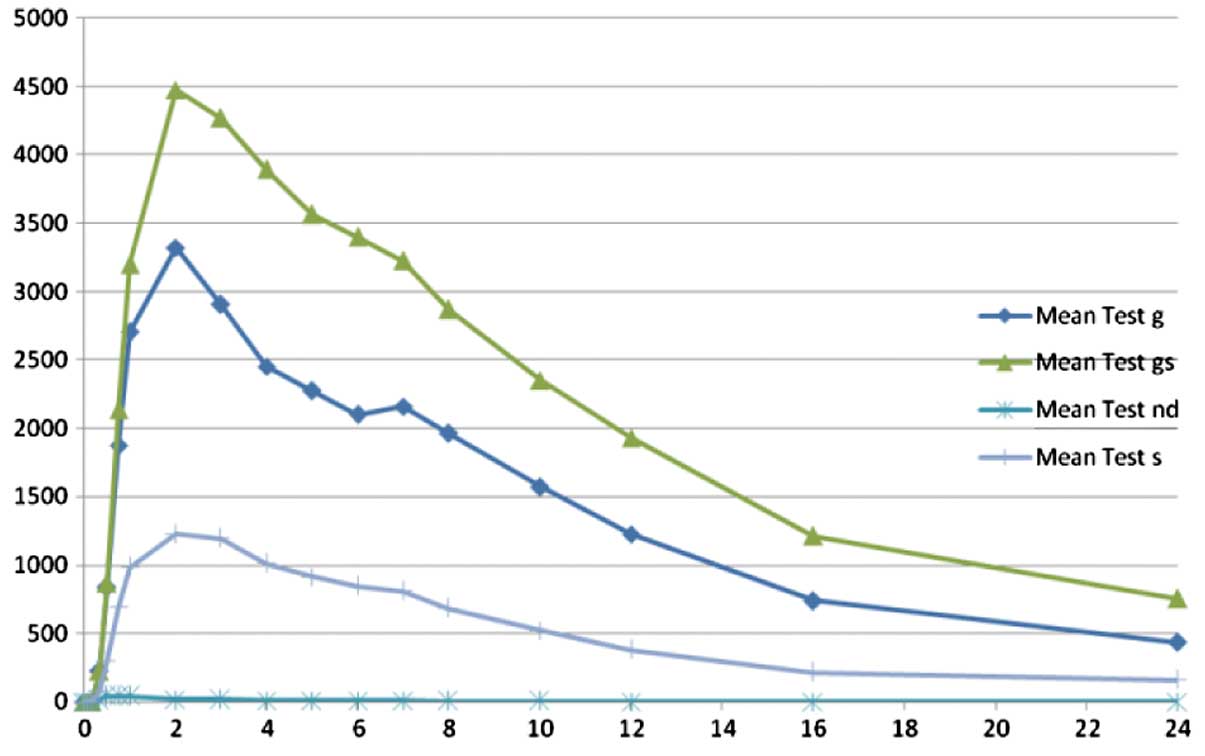
As already mentioned, low levels of resveratrol
(parent compound) were identified when compared with the metabolite
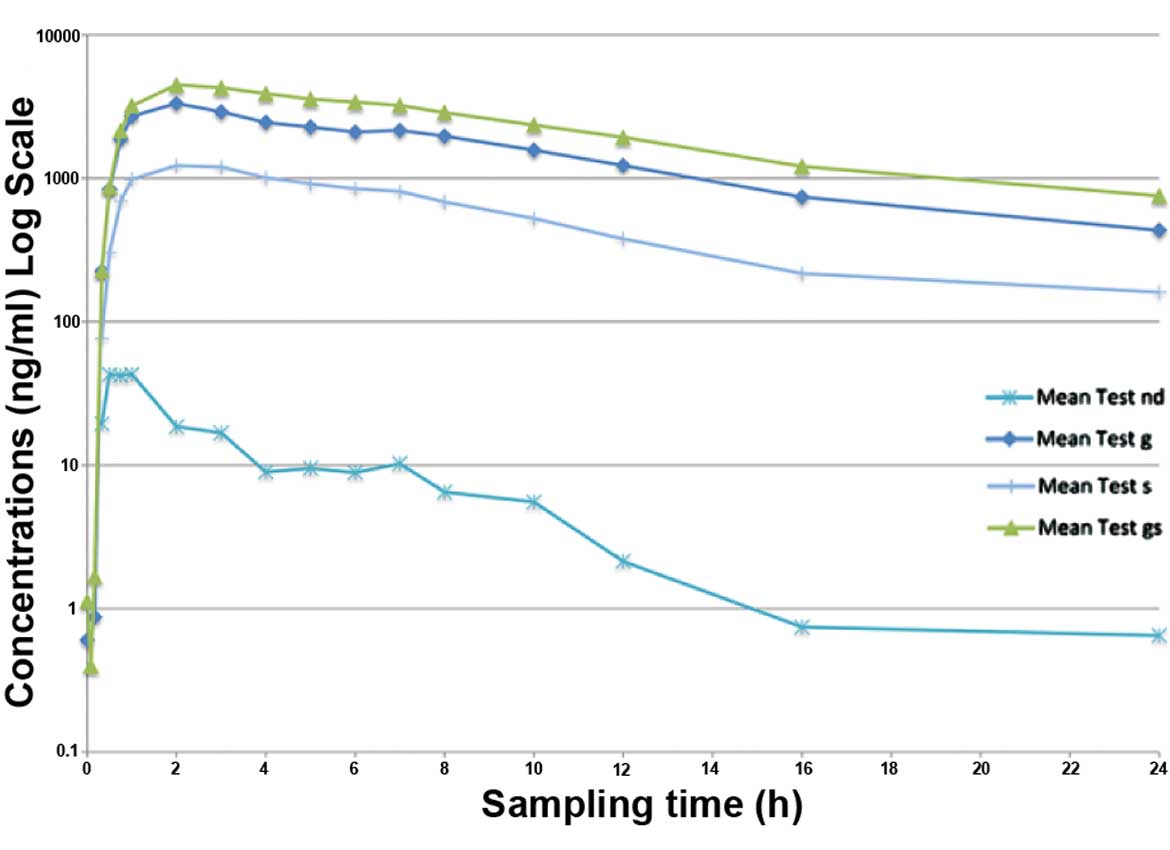
levels. The plasma concentration versus time curves for resveratrol
and its metabolites are depicted in Figs. 2 and 3. In Fig. 2,
as the plasma levels of resveratrol were low, the curve for
resveratrol is superposing the 0 point. Fig. 3 is a magnified version of Fig. 2 that demonstrates the resveratrol
levels, while the plasma levels of metabolites are presented only
as a guide to show their high levels.
Safety results
The resveratrol 500 mg tablet was well-tolerated by
all study participants. Only one adverse event (traumatic cutaneous
wound) of moderate intensity occurred in 1 subject in the present
study; however, this was not associated with the medication used in
the study. No statistically significant differences in any of the
safety parameters considered were observed at follow-up compared
with the parameters at screening, with the exception of lower
values of red blood cells and hematocrit at follow-up compared with
their values at screening; however, these statistical differences
are devoid of clinical significance.
Discussion
Previous studies have demonstrated that resveratrol
is well-absorbed following oral administration, with ~75% of the
dose absorbed. Following absorption, resveratrol undergoes rapid
and extensive metabolism leading to low bioavailability (18,19).
Resveratrol pharmacokinetics have shown circadian variation, with
higher bioavailability after morning administration (18). Resveratrol is mainly metabolized in
the intestines and liver, and its major metabolites are resveratrol
glucuronides and sulphates (20–22).
Colonic bacterial metabolism is also considered to be an important
metabolic pathway (24). The plasma
levels of the conjugated metabolites were reported to be higher
compared with those of the parent compound in animal and in human
studies (15,28).
Numerous beneficial effects of resveratrol have been
reported, although low levels of this compound are detected in the
plasma. According to Biasutto et al (29), up to 76% of resveratrol is not
accounted for when only plasma is evaluated; the cellular fraction
of resveratrol is missed if analysis of the whole blood is not
performed and therefore its bioavailability is not accurately
determined (29). According to data
in the literature, the conjugate metabolites have relevant
biological activities, and the efficacy of resveratrol is also
mediated by its metabolites and through accumulation in specific
tissues (24,30).
Studies in humans revealed that resveratrol was
well-tolerated and the adverse events, if any, were mild in
severity (18,19,22).
Only high doses of resveratrol (2.5 and 5 g) were associated with
mild to moderate gastrointestinal symptoms (22).
The purpose of the present study was to evaluate the
rate and extent of absorption, and the safety of resveratrol 500 mg
tablets. Plasma levels of resveratrol and its metabolites were
determined in 15 healthy volunteers using a validated HPLC-MS/MS
method. The plasma levels of resveratrol were lower when compared
with those of its conjugated metabolites. The predominant
conjugates were the glucuronated resveratrol (62.53% of total
resveratrol) and sulphated resveratrol (22.73% of total
resveratrol). Free (unconjugated) resveratrol was 0.28% of the
total resveratrol. Cmax values for resveratrol,
glucuronated resveratrol and sulphated resveratrol were found to be
71.2±42.4, 4,083.9±1,704.4 and 1,516.0±639.0 ng/ml, respectively,
while the AUC0-inf values were found to be 179.1±79.1,
39,732.4±16,145.6 and 14,441.7±7,593.2 ng/ml, respectively. In
addition, Tmax was 1.3 h for resveratrol, 3.0 h for
glucuronated resveratrol and 2.8 h for sulphated resveratrol.
Similar results were reported in studies by Brown
et al (22) and Almeida et
al (18), in which repeated
administration of resveratrol (doses between 0.15 and 5 g) led to
lower concentrations of the parent compound and higher levels of
glucuronide and sulphate conjugates in the plasma.
The results of the present study were compared with
the results reported by Boocock et al (15), and the pharmacokinetics of 500 mg
resveratrol treatment in these two studies are presented in
Table VI. In the study by Boocock
et al (15), 42 volunteers
(age, 19–61 years) received a single dose of 0.5, 1.0, 2.5 or 5.0 g
resveratrol, but only the data obtained from the 500 mg dose were
used for comparison with the present study. The Cmax and
AUC0-inf values for resveratrol that were observed in
the two studies were similar. In the case of the sulphate
conjugate, similar results were observed for Cmax, while
for AUC0-inf, the levels registered in the present study
were 3.5 times higher than the data obtained by Boocock et
al (15). This difference can be
justified by the fact that in the study of Boocock et al
only a specific sulphate form was measured, while it is possible
that other types of sulphates were not detected; however, these
were measured in the present study after enzymatic digestion. A
similar situation was observed for glucuronated resveratrol, for
which the differences between the two studies were even greater,
with higher levels observed following the enzymatic degradation.
Resveratrol was well-tolerated and no severe adverse reactions were
reported in the two studies.
| Table VI.Pharmacokinetics parameters reported
in the current study and in the study of Boocock et al
(15). |
Table VI.
Pharmacokinetics parameters reported
in the current study and in the study of Boocock et al
(15).
| Parameter | Present study
(Evelor 500 mg tablets)a | Study by Boocock
et al (15) (500 mg
resveratrol) |
|---|
| Free resveratrol
(ng/ml) |
|
|
|
Cmax | 71.2±42.4 | 72.6
(48.9%)a |
|
AUC0-inf | 179.1±79.1 | 223.7b |
| Glucuronated
resveratrolc
(ng/ml) |
|
|
|
Cmax |
4,083.9±1,704.4 | 774.1
(38%)d |
|
AUC0-inf |
39,730.3±16,145.9 | 3,206
(30%)d |
| Sulfated
resveratrol (ng/ml) |
|
|
|
Cmax | 1,516.0±639.0 | 1,135
(25.7)d |
|
AUC0-inf |
14,441.0±7,593.3 | 4,049
(26.6%)d |
In addition, the present study investigated the
doses of resveratrol used in various in vivo and in
vitro studies, as well as the concentration required to elicit
noteworthy pharmacological activities (8–18,22,23).
In vitro data showed that a minimum of 5 µmol/l resveratrol
is required for the chemopreventive effects to be elicited
(15). In humans, the plasma level
of resveratrol following oral administration is very low; however,
the metabolite levels are much higher. Considering that back
conversion from metabolite to parent compound in the target tissues
has been described in the case of resveratrol (30), and also that the metabolites are
pharmaceutically active (6,25), the plasma levels of resveratrol along
with the plasma levels of the metabolites have to be considered
when investigating the concentrations expected to achieve in
vivo biological effects. The levels of total plasma resveratrol
(free resveratrol and metabolites) reported in the current study
are well above the minimum 5 µmol/l level required to promote in
vitro biological effects, as described in the literature
(15).
In clinical studies, numerous biological effects of
resveratrol have been studied and the dose employed varied widely
between 10 mg and 5 g (31). Brasnyó
et al (32) found that 10 mg
oral resveratrol was sufficient to decrease insulin resistance.
According to Bhatt et al (33), 250 mg resveratrol improved glycemic
control and was proposed as a potential adjuvant in the treatment
of diabetes. The study of Patel et al (30) showed that oral doses of 500 mg and 1
g resveratrol administered daily to patients with histologically
confirmed colorectal cancer provided plasma levels of resveratrol
under the limit of quantification. However, Patel et al
(30) were investigating the tissue
levels of resveratrol and metabolites in the gastrointestinal tract
associated with anticarcinogenic effects. A recent study performed
in Germany by Witte et al (34) showed that 200 mg resveratrol
administered daily to elderly individuals improved memory
performance in correlation with improved glucose metabolism and
also increased the hippocampal functional connectivity. Therefore,
the proposed 500 mg dose of resveratrol used in the present study
is considered to provide adequate plasma and target tissue
concentrations to promote various beneficial biological
effects.
With regard to the safety profile, 500 mg
resveratrol was well-tolerated by all the subjects, with no adverse
reactions associated with resveratrol reported during the study.
Similarly, good tolerability of 500 mg resveratrol was reported by
Brown et al (22), who also
found that only 2.5 and 5 g doses caused mild to moderate
gastrointestinal symptoms.
In conclusion, the results of the present human
pharmacokinetic study proved that resveratrol is well-absorbed
following oral administration of Evelor 500 mg tablets. The plasma
levels of resveratrol were comparable with those reported in the
literature for other formulations of resveratrol. In addition,
plasma concentrations of resveratrol and its metabolites were found
to be within the range reported to promote noteworthy
pharmacological activities in vitro. Finally, resveratrol
was well-tolerated by all the participant subjects.
References
|
1
|
Arichi H, Kimura Y, Okuda H, Baba K,
Kozawa M and Arichi S: Effects of stilbene components of the roots
of Polygonum cuspidatum Sieb. et Zucc. on lipid metabolism. Chem
Pharm Bull (Tokyo). 30:1766–1770. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Baur JA and Sinclair DA: Therapeutic
potential of resveratrol: The in vivo evidence. Nat Rev Drug
Discov. 5:493–506. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
3
|
Gambini J, López-Grueso R, Olaso-González
G, Inglés M, Abdelazid K, El Alam IM, Bonet-Costa V, Borrás C and
Viña J: Resveratrol: Distribution, properties and perspectives. Rev
Esp Geriatr Gerontol. 48:79–88. 2013.(In Spanish). View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bertell AA and Das DK: Grapes, wines,
resveratrol, and heart health. J Cardiovasc Pharmacol. 54:468–476.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bishayee A, Darvesh AS, Politis T and
McGory R: Resveratrol and liver disease: From bench to bedside and
community. Liver Int. 30:1103–1114. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Aires V, Limagne E, Cotte AK, Latruffe N,
Ghiringhelli F and Delmas D: Resveratrol metabolites inhibit human
metastatic colon cancer cells progression and synergize with
chemotherapeutic drugs to induce cell death. Mol Nutr Food Res.
57:1170–1181. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Aziz MH, Kumar R and Ahmad N: Cancer
chemoprevention by resveratrol: In vitro and in vivo studies and
the underlying mechanisms (review). Int J Oncol. 23:17–28.
2003.PubMed/NCBI
|
|
8
|
Asensi M, Medina I, Ortega A, Carretero J,
Baño MC, Obrador E and Estrela JM: Inhibition of cancer growth by
resveratrol is related to its low bioavailability. Free Radic Biol
Med. 33:387–398. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Frémont L: Biological effects of
resveratrol. Life Sci. 66:663–673. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hung LM, Chen JK, Huang SS, Lee RS and Su
MJ: Cardioprotective effect of resveratrol, a natural antioxidant
derived from grapes. Cardiovasc Res. 47:549–555. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Bhat KPL, Kosmeder JW II and Pezzuto JM:
Biological effects of resveratrol. Antioxid Redox Signal.
3:1041–1064. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
de la Lastra CA and Villegas I:
Resveratrol as an anti-inflammatory and anti-aging agent:
Mechanisms and clinical implications. Mol Nutr Food Res.
49:405–430. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ulrich S, Wolter F and Stein JM: Molecular
mechanisms of the chemopreventive effects of resveratrol and its
analogs in carcinogenesis. Mol Nutr Food Res. 49:452–461. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jan-Kan C and Li-man H: Therapeutic use of
resveratrol for hyperglycemia. US patent 2006/0034763 A1. Filed.
August 11–2004.issued February 16, 2006.
|
|
15
|
Boocock DJ, Faust GE, Patel KR, Schinas
AM, Brown VA, Ducharme MP, Booth TD, Crowell JA, Perloff M, Gescher
AJ, et al: Phase I dose escalation pharmacokinetic study in healthy
volunteers of resveratrol, a potential cancer chemopreventive
agent. Cancer Epidemiol Biomarkers Prev. 16:1246–1252. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Agarwal B, Campen MJ, Channell MM, Wherry
SJ, Varamini B, Davis JG, Baur JA and Smoliga JM: Resveratrol for
primary prevention of atherosclerosis: Clinical trial evidence for
improved gene in vascular endothelium. Int J Cardiol. 166:246–248.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Gu X, Creasy L, Kester A and Zeece M:
Capillary electrophoretic determination of resveratrol in wines. J
Agric Food Chem. 47:3223–3227. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Almeida L, Vaz-da-Silva M, Falcão A,
Soares E, Costa R, Loureiro AL, Fernandes-Lopes C, Rocha JF, Nunes
T, Wright L and Soares-da-Silva P: Pharmacokinetic and safety
profile of trans-resveratrol in a rising multiple-dose study
in healthy volunteers. Mol Nutr Food Res. 53(Suppl 1): S7–S15.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Cottart CH, Nivet-Antoine V,
Laguillier-Morizot C and Beaudeux JL: Resveratrol bioavailability
and toxicity in humans. Mol Nutr Food Res. 54:7–16. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kuhnle G, Spencer JP, Chowrimootoo G,
Schroeter H, Debnam ES, Srai SK, Rice-Evans C and Hahn U:
Resveratrol is absorbed in the small intestine as resveratrol
glucuronide. Biochem Biophys Res Commun. 272:212–217. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Rotches-Ribalta M, Andres-Lacueva C,
Estruch R, Escribano E and Urpi-Sarda M: Pharmacokinetics of
resveratrol metabolic profile in healthy humans after moderate
consumption of red wine and grape extract tablets. Pharmacol Res.
66:375–382. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Brown A, Patel KR, Viskaduraki M, Crowell
JA, Perloff M, Booth TD, Vasilinin G, Sen A, Schinas AM, Piccirilli
G, et al: Repeat dose study of the cancer chemopreventive agent
resveratrol in healthy volunteers: Safety, pharmacokinetics, and
effect on the insulin-like growth factor axis. Cancer Res.
70:9003–9011. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wang D, Hang T, Wu C and Liu W:
Identification of the major metabolites of resveratrol in rat urine
by HPLC-MS/MS. J Chromatogr B Analyt Technol Biomed Life Sci.
829:97–106. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Walle T: Bioavailability of resveratrol.
Ann N Y Acad Sci. 1215:9–15. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lu DL, Ding DJ, Yan WJ, Li RR, Dai F, Wang
Q, Yu SS, Li Y, Jin XL and Zhou B: Influence of glucuronidation and
reduction modifications of resveratrol on its biological
activities. Chembiochem. 14:1094–1104. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Sergides C and Pittas A: Resveratrol
compositions for use as dietary supplements. Patent EP2403479 A1.
Filed. March 3–2010.issued January 11, 2012.
|
|
27
|
Liu X, Teng Z, Zhang Y, Huan M and Zhou S:
High performance liquid chromatographytandem mass spectrometric
determination of resveratrol and its metabolites in rat tissues.
Anal Lett. 43:557–569. 2010. View Article : Google Scholar
|
|
28
|
Muzzio M, Huang Z, Hu SC, Johnson WD,
McCormick DL and Kapetanovic IM: Determination of resveratrol and
its sulfate and glucuronide metabolites in plasma by LC-MS/MS and
their pharmacokinetics in dogs. J Pharm Biomed Anal. 59:201–208.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Biasutto L, Marotta E, Garbisa S, Zoratti
M and Paradisi C: Determination of quercetin and resveratrol in
whole blood-implications for bioavailability studies. Molecules.
15:6570–6579. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Patel KR, Brown VA, Jones DJ, Britton RG,
Hemingway D, Miller AS, West KP, Booth TD, Perloff M, Crowel JA, et
al: Clinical pharmacology of resveratrol and its metabolites in
colorectal cancer patients. Cancer Res. 70:7392–7399. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Tomé-Carneiro J, Larrosa M,
González-Sarrías A, Tomás-Barberán FA, García-Conesa MT and Espín
JC: Resveratrol and clinical trials: The crossroad from in vitro
studies to human evidence. Curr Pharm Des. 19:6064–6093. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Brasnyó P, Molnár GA, Mohás M, Markó L,
Laczy B, Cseh J, Mikolás E, Szijártó IA, Mérei A, Halmai R, et al:
Resveratrol improves insulin sensitivity, reduces oxidative stress
and activates the Akt pathway in type 2 diabetic patients. Br J
Nutr. 106:383–389. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Bhatt JK, Thomas S and Nanjan MJ:
Resveratrol supplementation improves glycemic control in type 2
diabetes mellitus. Nutr Res. 32:537–541. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Witte AV, Kerti L, Margulies DS and Flöel
A: Effects of resveratrol on memory performance, hippocampal
functional connectivity, and glucose metabolism in healthy older
adults. J Neurosci. 34:7862–7870. 2014. View Article : Google Scholar : PubMed/NCBI
|