Introduction
Intervertebral Disc Degeneration (IDD), which is
also called degenerative disc disease, is the major cause of
degenerative spinal disease and one of the most common ailments
severely affecting quality of life in elderly populations (1). IDD is characterized by lower back pain,
intervertebral disc herniation and spinal canal stenosis (2). Degeneration of the nucleus pulposus in
spinal discs may reduce the production and secretion of
extracellular matrix components, leading to changes in disc
structure and resulting in the dysfunction of the discs (3–5). The
incidence of IDD has been shown to be influenced by gender and age,
with a prevalence in adolescents and young adults of <10%, which
increases to 30–50% in middle adulthood (6). The exact pathophysiology underlying IDD
is not well understood; however, genetic and environmental factors
are thought to be involved (7–9).
Previous studies have demonstrated that smoking, excessive
biomechanical load, obesity, gender, age, decreased nutrition and
other environmental factors are associated with a high risk of
developing IDD (10–13). Furthermore, pro-inflammatory
signaling pathways, tumor necrosis factor (TNF) and matrix
degrading enzymes may have pivotal roles in the pathogenesis of IDD
(2,14–16), and
it has been suggested that osteoprotegerin (OPG), a member
of the TNF receptor superfamily, has a crucial role in the etiology
of IDD (17,18).
OPG, which is also called osteoclastogenesis
inhibitory factor or tumor necrosis factor receptor superfamily
member 11B, is a glycoprotein and cytokine receptor containing 401
amino acid residues (19,20). OPG is primarily synthesized by
osteoblasts; however, it is also expressed in various organs and
tissues, including the heart, vessel walls, lungs, kidneys and bone
(21,22). The main role of OPG is its function
as a decoy receptor for receptor activator for nuclear factor-κB
ligand (RANKL) (23–25); by competitively binding to RANKL, OPG
prevents RANK/RANKL association and activation of RANK, thereby
modulating bone resorption, decreasing the number of osteoclasts
and acting as a regulator of osteoblast-osteoclast cross-talk in
bone homeostasis (26,27). The RANK-RANKL-OPG system regulates
the balance between osteoblasts and osteoclasts, and has a crucial
role in bone formation and absorption (28). Previous studies have suggested that a
deficiency of the OPG gene enhances osteoclastogenesis and
secondary hyperactive osteoblasts in long bones and vertebral bones
(17,29). Therefore, it has been hypothesized
that factors affecting OPG gene regulation may be major
genetic factors influencing bone mass and increasing the risk of
fractures, osteoporosis and osteoarthritis (30,31). The
human OPG gene is located on chromosome 8q23-24, has a
length of ~29 kb and consists of 5 exons and 4 introns (32). Previous studies have demonstrated
that changes in the OPG serum level are influenced by genetic
polymorphisms, including 950T/C at the rs2073617 locus, 1181 G/C at
the rs2073618 locus and 1181 G/C at the rs2073618 locus (33–35). The
association between genetic polymorphisms in the OPG gene
and bone mineral density has been the focus of previous
investigations (36,37). Previous studies have implicated
increased bone mineral density in the etiology of IDD (38,39);
however, few studies have focused on a direct association between
OPG genetic polymorphisms and the risk of IDD. Therefore,
the present study aimed to investigate the associations between
OPG genetic polymorphisms, serum OPG levels and IDD
risk.
Materials and methods
Ethical approval and patient
consent
The present study was approved by the Ethical
Committee of the First Affiliated Hospital of the University of
South China. Written informed consent was acquired from all study
participants at the time of hospitalization. In addition, the
present study was performed in accordance with the guidelines and
principles of the Declaration of Helsinki (40).
Subjects
Between January 2013 and May 2014, a total of 200
patients with IDD, including 100 females and 100 males, at the
Department of Spine Surgery of the First Affiliated Hospital of the
University of South China (Hengyang, China) were enrolled in the
present study. The average age of the patients was 52.6±6.6 years
(age range, 40–62 years). All patients were diagnosed with IDD
according to magnetic resonance imaging (MRI) results and IDD was
confirmed by postoperative pathological analyses, according to
previous studies (41,42). All patients presented with the
typical clinical and physical symptoms of IDD, including: i)
Chronic lower back pain with radiation to the lower limb; ii)
spasticity and atrophy of the paravertebral and lower limb muscles;
iii) limited activity; and iv) positive results in a nerve traction
test. In addition, the patients showed obvious disc degeneration in
the postoperative pathological analysis. Patients were excluded
from the present study if they suffered from lumbar spinal
stenosis. In addition, 200 age- and gender-matched healthy subjects
from our hospital, including 100 men and 100 women aged between 42
and 62-years (average age, 52.1±5.4 years), were recruited. The MRI
findings of the healthy controls showed normal intervertebral disc
tissue (http://www.uscspine.com/conditions/back-degenerative-disc.cfm).
No significant differences in age, gender, body mass index and
smoking history were observed between the IDD patients and
controls. The present study was approved by the Ethics Committee of
the First Affiliated Hospital of the University of South China.
Specimen collection
Blood samples (10 ml) were drawn from the patient's
elbow vein in the morning following an overnight fast, and 3 ml
blood was added to ethylenediamine tetraacetic acid (EDTA) tubes
(Sigma-Aldrich, St. Louis, MO, USA) for anticoagulation. Genomic
DNA was extracted from the 3 ml blood samples using a Whole Blood
Genomic DNA Extraction kit (cat. no. OSR-M102/M104; Tiangen
Biotech, Co., Ltd., Beijing, China). The remaining blood (without
EDTA) was allowed to clot for 1 h at room temperature, followed by
centrifugation at 1006.2 × g for 10 min at 37°C to obtain the
serum, which was stored at −80°C until further use.
High resolution melting (HRM)
analysis
The primers used for HRM genotyping were designed by
LightScanner® Primer Design software, version 1.0 (Idaho
Technology, Inc., Salt Lake City, UT USA) and are presented in
Table I. The polymerase chain
reaction (PCR)-HRM analysis was performed using a final reaction
volume of 11 µl, consisting of 1 µl genomic DNA (20 ng/l), 0.2 µl
each of the forward and reverse primers (each 10 pmol), 5 µl 2X
Taq PCR Master mix (containing Taq DNA polymerase,
Mg2+ and dNTPs; Tiangen Biotech, Co., Ltd.), 3.6 µl
sterilizing ultrapure water and 1 µl 10X LCGreen Plus dye (Idaho
Technology, Inc.). The PCR reaction was conducted using the Type-it
HRM PCR kit (cat. no. 206542; Qiagen GmbH, Hilden, Germany),
according to the manufacturer's protocol. The PCR reaction
conditions were as follows: Initial denaturation at 96°C for 5 min,
followed by 40 cycles of 96°C for 20 sec, 57°C for 20 sec and 72°C
for 20 sec. The HRM analysis was synchronized with the PCR
reaction, as follows: 95°C for 5 min, 40°C for 2 min, 60°C for 1
min and then heating from 72–95°C at 0.1°C/sec, during which time
the melting curve data was collected. Each HRM analysis detected
the standard three genotypes already known from each locus and the
genomic DNA of study subjects. LightScanner software (Idaho
Technology, Inc.) was used in the melting curve analysis to
determine the genotypes.
 | Table I.Sequences of the primers used for
polymerase chain reaction-high resolution melting genotyping of the
osteoprotegerin gene. |
Table I.
Sequences of the primers used for
polymerase chain reaction-high resolution melting genotyping of the
osteoprotegerin gene.
| Locus | Primer
sequence | Product size
(bp) |
|---|
| rs2073617 | F:
5′-CTGGTAGGACAAATATTGG-3′ | 88 |
|
| R:
5′-ACTTACCATTTGCGATCACC-3′ |
|
| rs2073618 | F:
5′-CGTTGTCTTGAGAAGGTTGA-3′ | 141 |
|
| R:
5′-TCCTCAAAAACATGTCAGTGTG-3′ |
|
| rs3102735 | F: 5′-
TCCCACTATCATGATTATTTCCC-3′ | 163 |
|
| R:
5′-ATTATAGGTTTTTAAGTAATTTGT-3′ |
|
PCR-restriction fragment length
polymorphism (PCR-RFLP) assays
PCR primers were designed using Primer Premier 5.0
software (Premier Biosoft International, Palo Alto, CA, USA) and
were synthesized by Sangon Biotech Co., Ltd. (Shanghai, China). The
sequences and lengths of the primers are shown in Table II. The PCR reaction system consisted
of 100 ng genomic DNA, 125 ng each of the upstream and downstream
primers, 12.5 µl 2X Taq PCR Master mix and 9.5 µl
double-distilled H2O, in a final volume of 25 µl. The cycling
conditions were as follows: Initial denaturation at 95°C for 5 min,
followed by 30 cycles at 94°C for 30 sec, 62°C for 45 sec and 72°C
for 60 sec, and a final extension step at 72°C for 10 min.
HincII, XspI and AseI restriction enzymes (Takara
Biotechnology Co., Ltd., Dalian, China) were added to the PCR
products and then 10% agarose gel electrophoresis was used to
assess PCR fragment patterns. An automated DNA sequencer (model
370; Applied Biosystems; Thermo Fisher Scientific, Inc., Waltham,
MA, USA) was used to determine the genotypes of the rs2073617,
rs2073618 and rs3102735 loci.
| Table II.Sequences of the primers used for
polymerase chain reaction-restriction fragment length polymorphism
analysis of the three loci of the osteoprotegerin gene. |
Table II.
Sequences of the primers used for
polymerase chain reaction-restriction fragment length polymorphism
analysis of the three loci of the osteoprotegerin gene.
| Locus | Primer
sequence | Product size
(bp) | Endonucleases |
|---|
| rs2073617 | F:
5′-GAAGTGAAGGGGTCAGGCAGC-3′ | 342 | HincII |
|
| R:
5′-GTCTGTCTCTCTCTTGCTGTCTTCC-3′ |
|
|
| rs2073618 | F:
5′-GTCTGTCTCTCTCTTGCTGTCTTCC-3′ | 340 | XspI |
|
| R:
5′-GAGATGAAGACAGAAGGTTAATGAC-3′ |
|
|
| rs3102735 | F:
5′-TTCCTTCCCTTGAATCTGGTG-3′ | 300 | AseI |
|
| R:
5′-CTAAAGCCCGTGCTATTCTGC-3′ |
|
|
Measurement of OPG protein levels in
serum
Serum levels of OPG were measured using an OPG ELISA
kit (cat. no. K1011; Immundiagnostik AG, Bensheim, Germany),
according to the manufacturer's protocol. Optical density (OD)
values were measured at 450 nm using a microplate reader. The
standard curve was drawn by setting standard concentrations as the
vertical axis and OD values as the horizontal axis. All samples
were measured twice and averaged, and the detection met laboratory
quality control standards.
Construction of haplotypes
OPG rs2073617 and rs3102735 are located in
the promoter region of the OPG gene, whereas rs2073618 is located
in the exon 1 (43). Haplotype
construction of these three genotypes of polymorphic loci was
performed using the individual-driven Bayesian method implemented
in PHASE 2.1 software (http://stephenslab.uchicago.edu/phase/download.html),
as previously described (44).
Statistical analysis
SPSS software, version 18.0 (SPSS, Inc., Chicago,
IL, USA) was used to perform data analyses. Hardy-Weinberg
equilibrium was used to assess and confirm the representation of
the selected samples in the population. Measurement data are
presented as the mean ± standard deviation. One-way analysis of
variance was used for comparisons between the three groups and
Student's t-test was used to compare the measurement data
between the groups. The non-parametric Wilcoxon signed-rank test
was used to calculate the significance of comparisons when the data
did not meet the normal distribution. The χ2 test was
applied to compare the distribution frequencies of the genotypes,
alleles and haplotypes between the two groups. Logistic regression
analysis was conducted to calculate the odds ratios (OR), and 95%
confidence intervals (CI) represented the relative risk. All
statistical tests were two-sided probability tests. P<0.05 was
considered to indicate a statistically significant difference.
Results
Genotyping of the OPG gene by HRM
analysis
DNA fragments containing polymorphic loci were
amplified by PCR and analyzed by HRM. The OPG gene has some
common, functionally important genetic polymorphisms that have been
associated with various human diseases. The most important
polymorphisms of the OPG gene are rs2073617 (950T/C) and
rs3102735 (163A/G), which are located in the promoter region, and
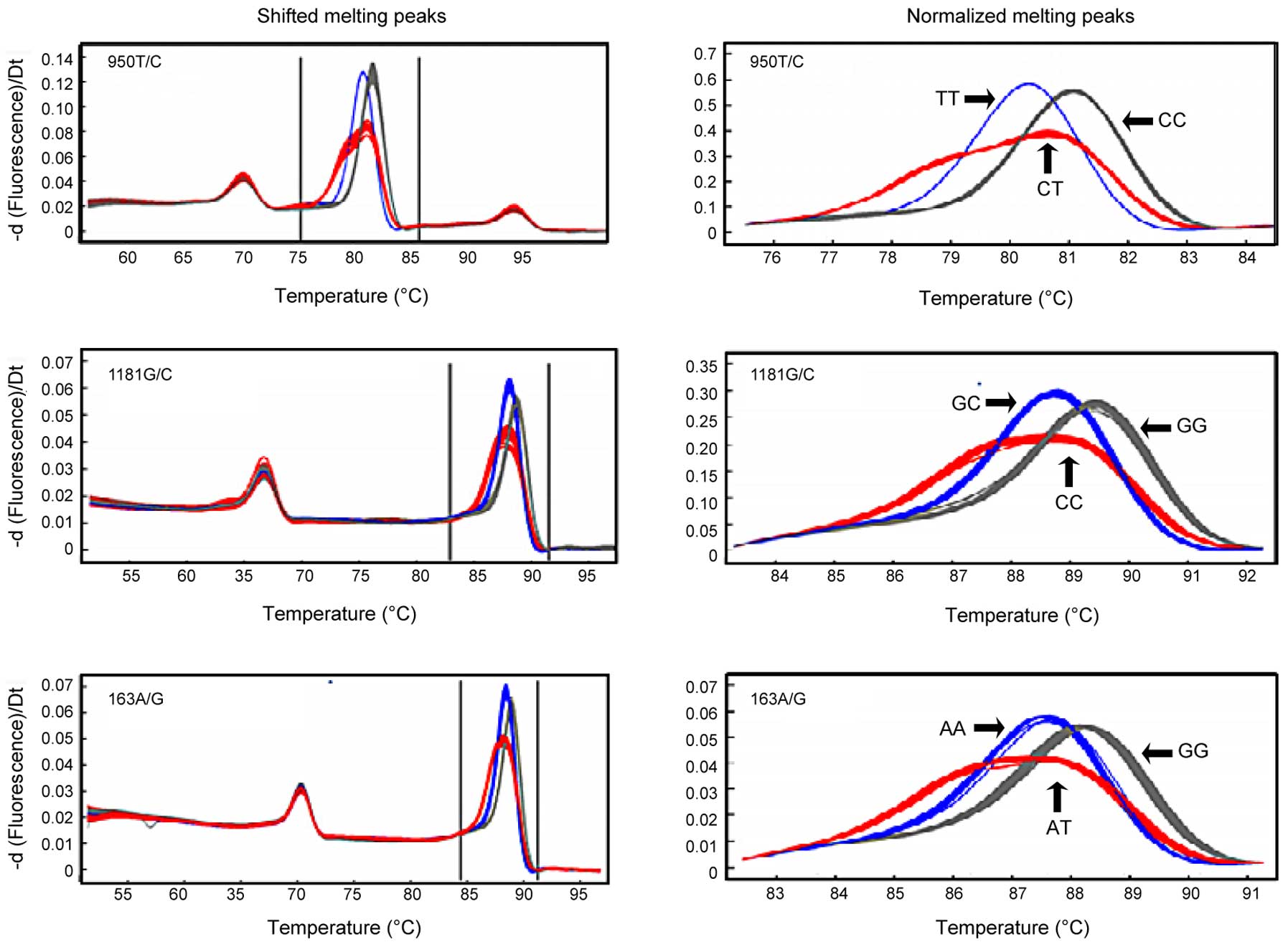
rs2073618 (1181G/C), which is located in exon 1 (44). The HRM analysis demonstrated that the
950T/C (rs2073617), 1181G/C (rs2073618) and 163A/G (rs3102735)
OPG gene polymorphisms were associated with three genotypes
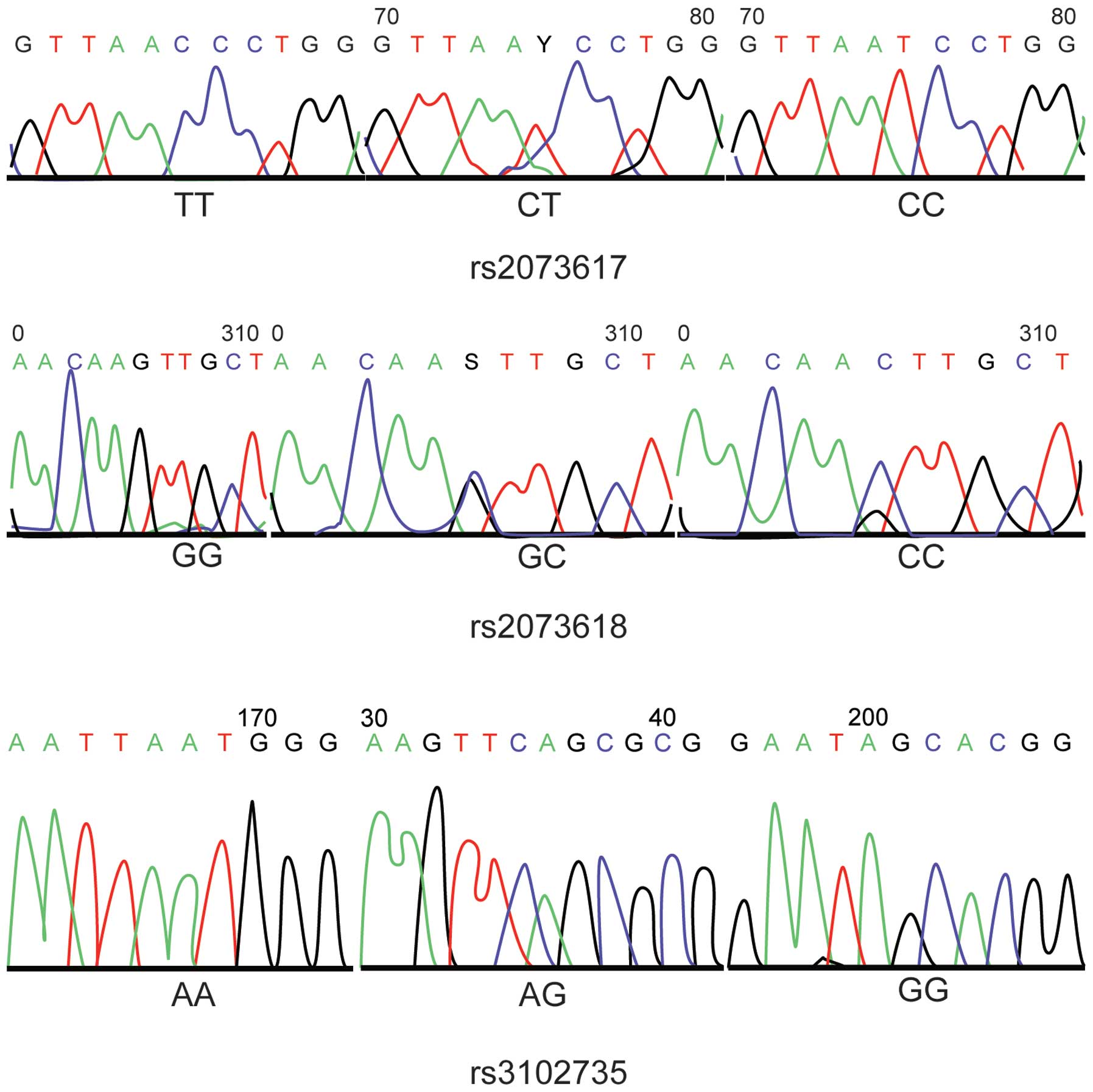
(Fig. 1). The HRM genotyping results
were consistent with the sequences of the polymorphisms, as
determined by PCR and DNA sequencing (Fig. 2).
OPG genotyping
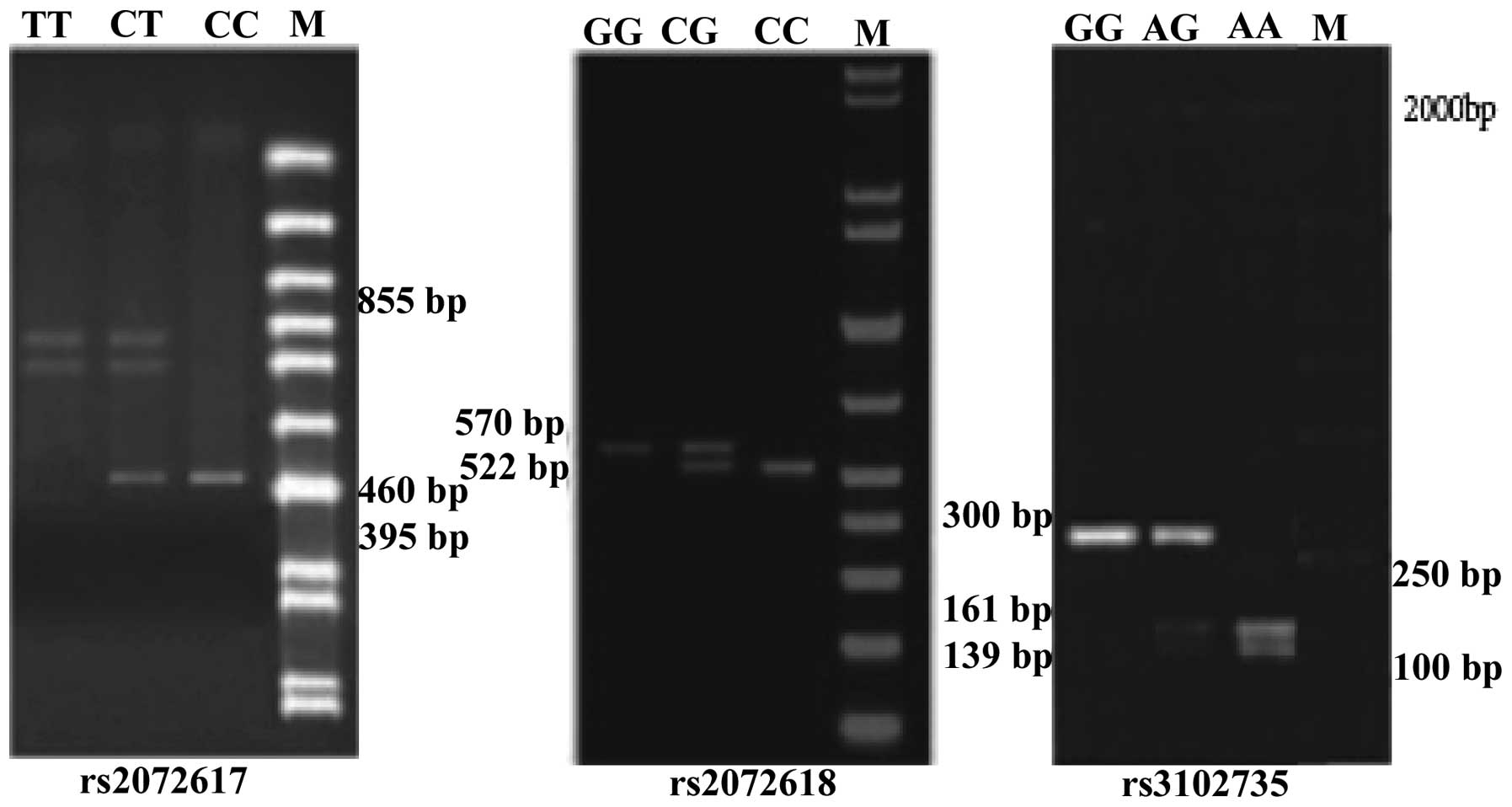
PCR-RFLP analysis of the OPG rs2073617 locus
detected a single band of 855 bp corresponding to the homozygous
wild-type genotype (TT), three fragments of 855 bp, 460 bp and 395
bp corresponding to the heterozygous mutated genotype (TC), and two
fragments of 395 bp and 460 bp corresponding to the homozygous
mutated genotype (CC). Similarly, for rs2073618, an undigested and
single band of 570 bp corresponded to the homozygous wild-type GG
genotype, three fragments of 570 bp, 522 bp and 48 bp corresponded
to the heterozygous mutated GC genotype, and two bands of 522 bp
and 48 bp corresponded to the homozygous mutant CC genotype,
although the 48 bp fragment was too small to be visible.
Furthermore, the OPG rs3102735 locus showed three genotypes:
Homozygous wild-type (A/A) with 161 bp and 139 bp fragments;
heterozygous mutated genotype (G/A) with 300 bp, 161 bp and 139 bp
fragments, and homozygous mutated genotype (G/G) with a 300 bp
fragment. The results of DNA sequencing confirmed the existence of
these genotypes for the rs2073617, rs2073618 and rs3102735 loci
(Figs. 2 and 3).
Allele and genotype frequency
distributions of OPG polymorphisms
The genotype and allele frequencies of OPG
rs2073617, rs2073618 and rs3102735 polymorphisms were in accordance
with the Hardy-Weinberg equilibrium, thus suggesting that each
polymorphism had reached equilibrium and that the selected sample
was representative of the population (P>0.05). There were
significant differences in the allele and genotype frequencies of
the OPG rs2073617 polymorphisms between the case and control
groups (P<0.05). In addition, patients carrying the C allele
exhibited an increased risk of IDD, as compared with carriers of
the other alleles (OR=1.79; 95% CI=1.33–2.41; P<0.001). However,
no significant differences were observed in the allele and genotype
frequencies of the rs2073618 and rs3102735 polymorphisms between
the case and control groups (P>0.05; Table III).
| Table III.Genotype and allele frequency
distributions of osteoprotegerin genetic polymorphisms and their
associations with intervertebral disc degeneration risk. |
Table III.
Genotype and allele frequency
distributions of osteoprotegerin genetic polymorphisms and their
associations with intervertebral disc degeneration risk.
| Locus |
Genotype/Allele | Control Group [n
(%)] | Case group [n
(%)] | P1 | OR (95% CI) | P2 |
|---|
| rs2073617 | TT | 112 (56.0) | 84 (41.8) | 0.018 | Ref. |
|
|
| TC | 55 (32.8) | 70 (35.2) |
| 1.69
(1.07–2.67) | 0.021 |
|
| CC | 33 (11.2) | 46 (23.0) |
| 1.19
(1.10–3.16) | 0.020 |
|
| TC+CC | 88 (46.0) | 116 (58.2) |
| 1.76
(1.18–2.61) | 0.005 |
|
| T | 290 (72.4) | 238 (59.4) | <0.001 | Ref. |
|
|
| C | 110 (27.6) | 162 (40.6) |
| 1.79
(1.33–2.41) | <0.001 |
| rs2073618 | GG | 107 (53.5) | 111 (55.2) | 0.890 | Ref. |
|
|
| CG | 77 (38.5) | 75 (37.8) |
| 0.94
(0.62–1.42) | 0.765 |
|
| CC | 16 (8.0) | 14 (7.0) |
| 0.84
(0.39–1.81) | 0.662 |
|
| CC+CG | 93 (46.5) | 89 (44.8) |
| 1.04
(0.70–1.53) | 0.845 |
|
| G | 291 (72.8) | 304 (74.1) | 0.292 | Ref. |
|
|
| C | 109 (27.3) | 96 (25.9) |
| 1.07
(0.78–1.47) | 0.682 |
| rs3102735 | AA | 116 (58.4) | 113 (56.6) | 0.945 | Ref. |
|
|
| AG | 54 (26.4) | 55 (27.0) |
| 1.05
(0.87–1.17) | 0.848 |
|
| GG | 30 (15.2) | 32 (16.4) |
| 1.10
(0.62–1.92) | 0.781 |
|
| AG+GG | 84 (41.6) | 87 (43.4) |
| 1.06
(0.71–1.58) | 0.761 |
|
| A | 287 (71.6) | 280 (70.1) | 0.586 | Ref. |
|
| G | 113 (28.4) | 120 (29.9) |
| 1.09
(0.80–1.47) | 0.586 |
Association between serum OPG levels
and OPG genotype frequency distributions
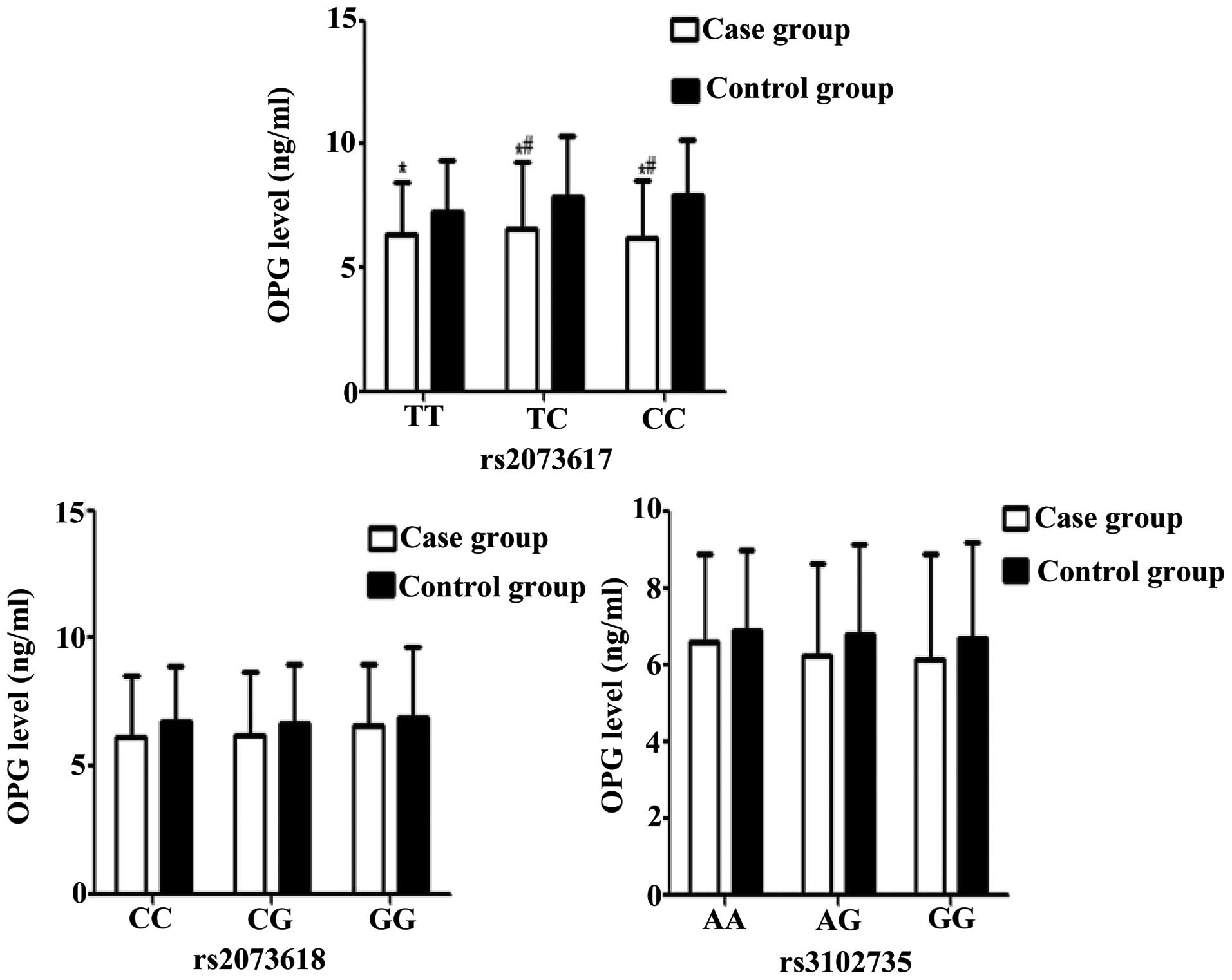
Serum levels of OPG were significantly higher in IDD
patients with TT, TC or CC genotypes at the OPG rs2073617
locus, as compared with the control group (all P<0.05). In
addition, OPG serum levels were significantly higher in IDD
patients harboring the TC or CC mutated genotypes, as compared with
those carrying the wild-type homozygous (TT) genotype (P<0.05).
No significant differences were observed between the patient and
control groups in the OPG serum levels associated with the various
genotypes of the rs3102735 and rs2073618 loci (P>0.05; Table IV and Fig. 4). These results suggest that TT, TC
and CC genotypes may contribute to the elevation of serum OPG
levels in IDD patients.
| Table IV.OPG serum levels in individuals with
certain genetic polymorphisms of the OPG gene. |
Table IV.
OPG serum levels in individuals with
certain genetic polymorphisms of the OPG gene.
| SNP | Genotype | Control group
(ng/ml) | Case group
(ng/ml) |
|---|
| rs2073617 | TT |
6.36±2.10 |
7.25±2.12a |
|
| TC |
6.56±2.45 |
7.86±2.70a,b |
|
| CC |
6.20±2.23 |
7.95±2.30a,b |
| rs2073618 | CC |
6.16±2.13 |
6.75±2.34 |
|
| CG |
6.21±2.35 |
6.69±2.45 |
|
| GG |
6.54±2.82 |
6.84±2.41 |
| rs3102735 | AA |
6.56±2.13 |
6.86±2.30 |
|
| AG |
6.21±2.16 |
6.76±2.42 |
|
| GG |
6.14±2.52 |
6.69±2.74 |
Statistical analysis of haplotype
frequencies of three polymorphic loci
The T-G-A haplotype was shown to be a potential
protective factor for IDD (OR=0.62; 95% CI=0.41–0.94; P=0.02),
whereas the C-G-G haplotype was a potential risk factor for IDD
(OR=2.24; 95% CI=1.09–4.60; P=0.02; Table V).
| Table V.Frequency distributions of the
haplotypes of osteoprotegerin genetic polymorphisms in the case and
control groups. |
Table V.
Frequency distributions of the
haplotypes of osteoprotegerin genetic polymorphisms in the case and
control groups.
| Haplotypes | Case group | Control group | χ2 | P-value | OR (95% CI) |
|---|
| T-C-A | 21 (10.5) | 28 (14.0) | 0.82 | 0.36 | 0.70
(0.40–1.32) |
| T-C-G | 9 (4.5) | 12 (6.0) | 0.19 | 0.66 | 0.73
(0.30–1.79) |
| C-C-A | 14 (7.0) | 10 (5.0) | 0.71 | 0.39 | 1.43
(0.61–3.30) |
| C-C-G | 6 (3.0) | 4 (2.0) | 0.41 | 0.52 | 1.51
(0.42–5.45) |
| T-G-A | 55 (27.5) | 76 (38.0) | 5.01 | 0.02 | 0.62
(0.41–0.94) |
| T-G-G | 26 (13.0) | 30 (15.0) | 0.33 | 0.56 | 0.84
(0.48–1.50) |
| C-G-A | 44 (22.0) | 28 (14.0) | 2.61 | 0.06 | 1.73
(1.03–2.91) |
| C-G-G | 25 (12.5) | 12 (6.0) | 5.03 | 0.02 | 2.24
(1.091–4.60) |
Logistic regression analysis
A multivariate stepwise logistic regression was
performed to calculate the adjusted OR. The IDD was the dependent
variable and the genotypes and haplotypes of OPG rs2073617,
rs3102735 and rs2073618 loci, body mass index, smoking, OPG levels
(>6.69 ng/ml as high levels and ≤6.69 ng/ml as low levels), age
and gender, were the independent variables. The multivariate
stepwise logistic regression results showed that upregulated OPG
serum levels were positively correlated with IDD risk, whereas the
T-C-A, T-G-A and T-G-G haplotypes were negatively correlated with
IDD risk (P<0.05; Table VI).
| Table VI.Multivariate stepwise logistic
regression analysis for the associated risk factors of patients
with intervertebral disc degeneration. |
Table VI.
Multivariate stepwise logistic
regression analysis for the associated risk factors of patients
with intervertebral disc degeneration.
| Variable | B | S.E. | Wald | df | P-value | Exp (B) | 95% CI |
|---|
| T-C-A | −1.022 | 0.455 | 5.051 | 1 | 0.025 | 0.360 | 0.148–0.878 |
| T-G-A | −1.057 | 0.393 | 7.228 | 1 | 0.007 | 0.347 | 0.161–0.751 |
| T-G-G | −0.877 | 0.442 | 3.942 | 1 | 0.047 | 0.416 | 0.175–0.989 |
| High serum level of
OPG | 0.567 | 0. 141 | 7.791 | 1 | 0.005 | 1.758 | 1.183–2.611 |
Discussion
The pathogenesis of IDD is considered
multifactorial, involving various genetic and environmental factors
(7,9); however, the exact mechanism underlying
IDD remains incompletely understood. The present study evaluated
the associations between polymorphisms of the OPG gene and
the risk of IDD, and demonstrated that the 950T/C variant at the
rs2073617 locus was associated with an increased risk of IDD, as
compared with the 950T/T wild-type genotype. Conversely, the
1181G/C (rs2073618) and 163A/G (rs3102735) SNPs were not associated
with an increased susceptibility to IDD. These results suggested
that the OPG gene, in particular the 950T/C (rs2073617) SNP,
may serve as a potential indicator of IDD risk. Previous studies
based on pathophysiological analyses have reported the involvement
of various cytokines in IDD (45,46). In
addition, the RANK/RANKL/OPG signaling pathway has been proposed to
have a role in bone metabolism (26,47,48).
Previous studies have demonstrated that disruption of the RANKL/OPG
balance led to cartilage degradation due to mechanical loading and
resulted in the progression of IDD or osteoarthritis (49,50). In
addition, it has been reported that OPG genetic
polymorphisms negatively influence bone resorption, and thereby
regulate bone mineral density, resulting in the deterioration of
patients with IDD (51,52). OPG gene expression has a
crucial role in maintaining the integrity of endplate cartilage by
preventing its resorption by osteoclasts (17).
In the present study, a haplotype analysis suggested
that the G-T-G, T-C-A, T-G-A and T-G-G haplotypes were associated
with protection against IDD, whereas the G-C-G haplotype was
associated with an increased susceptibility to IDD. Furthermore,
the serum levels of OPG were significantly higher in IDD patients
with TT, TC and CC genotypes at the OPG rs2073617 locus, as
compared with the control group (P<0.05), which suggested that
TT, TC and CC genotypes may be significant risk factors for IDD
development and that upregulated serum levels of OPG are correlated
with IDD risk.
Insufficient nutrition has been shown to be involved
in the degeneration of intervertebral discs (50,53,54).
Metabolism and nutrient exchange at intervertebral discs is
dependent on the interaction of endplate cartilage with
intervertebral discs (55), and
endplate cartilage has an important role in the biomechanical
structure of intervertebral discs (55). OPG polymorphisms have been
closely associated with the degeneration of endplate cartilage and
intervertebral discs by upregulating OPG serum levels; thus OPG has
already been associated with an increased risk of IDD (53,56).
Furthermore, a previous study demonstrated that the TT, TC and CC
genotypes of the rs2073617 locus affected the protein expression
levels of OPG and were associated with elevated OPG serum levels;
thus suggesting that upregulated OPG expression is a high risk
factor for IDD (57). In addition,
it was reported that the CC genotype of the rs2073617 locus was
associated with increased serum levels of OPG and increased
production of OPG by osteoblasts in order to restore disrupted bone
metabolism (58). Consistent with
this, the present study demonstrated that IDD patients with the TT,
TC or CC genotypes of the OPG rs2073617 polymorphism had
significantly higher serum levels of OPG, as compared with the
healthy controls. These results suggested that IDD patients with
high OPG serum levels and the 950T/C SNP at the rs2073617 locus may
be at a high risk of developing impaired bone metabolism and
endplate cartilage degeneration, resulting in IDD.
In conclusion, the present study demonstrated that
the OPG genetic polymorphism, 950T/C (rs2073617), was
associated with an increased risk of IDD, and that the C allele may
be a high risk factor for elevated IDD risk by promoting increased
serum levels of OPG. In addition, the G-T-G haplotype was
associated with protection against IDD, whereas the G-C-G haplotype
was associated with an elevated risk of IDD. Furthermore, an
elevated OPG serum level was positively correlated with IDD risk,
whereas the T-C-A, T-G-A and T-G-G haplotypes were negatively
correlated with IDD risk. These results suggested that genetic
polymorphisms of the OPG gene may influence susceptibility
to IDD by altering the protein serum levels of OPG. With continued
efforts, the OPG rs2073617 polymorphism may emerge as a biomarker
for the diagnosis of IDD, and targeting OPG may represent a novel
and promising therapeutic strategy for biologically-induced disc
repair in early stage disc degeneration.
References
|
1
|
Sakai D: Future perspectives of cell-based
therapy for intervertebral disc disease. Eur Spine J. 17(Suppl 4):
452–458. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sudo H, Yamada K, Iwasaki K, Higashi H,
Ito M, Minami A and Iwasaki N: Global identification of genes
related to nutrient deficiency in intervertebral disc cells in an
experimental nutrient deprivation model. PLoS One. 8:e588062013.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Richardson SM, Walker RV, Parker S, Rhodes
NP, Hunt JA, Freemont AJ and Hoyland JA: Intervertebral disc
cell-mediated mesenchymal stem cell differentiation. Stem Cells.
24:707–716. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sobajima S, Vadala G, Shimer A, Kim JS,
Gilbertson LG and Kang JD: Feasibility of a stem cell therapy for
intervertebral disc degeneration. Spine J. 8:888–896. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Song YQ, Karasugi T, Cheung KM, Chiba K,
Ho DW, Miyake A, Kao PY, Sze KL, Yee A, Takahashi A, et al: Lumbar
disc degeneration is linked to a carbohydrate sulfotransferase 3
variant. J Clin Invest. 123:4909–4917. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wang YX, Griffith JF, Zeng XJ, Deng M,
Kwok AW, Leung JC, Ahuja AT, Kwok T and Leung PC: Prevalence and
sex difference of lumbar disc space narrowing in elderly chinese
men and women: Osteoporotic fractures in men (Hong Kong) and
osteoporotic fractures in women (Hong Kong) studies. Arthritis
Rheum. 65:1004–1010. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hangai M, Kaneoka K, Kuno S, Hinotsu S,
Sakane M, Mamizuka N, Sakai S and Ochiai N: Factors associated with
lumbar intervertebral disc degeneration in the elderly. Spine J.
8:732–740. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Liu G, Cao P, Chen H, Yuan W, Wang J and
Tang X: MiR-27a regulates apoptosis in nucleus pulposus cells by
targeting PI3K. PLoS One. 8:e752512013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kalichman L and Hunter DJ: The genetics of
intervertebral disc degeneration. Familial predisposition and
heritability estimation. Joint Bone Spine. 75:383–387. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Guehring T, Wilde G, Sumner M, Grünhagen
T, Karney GB, Tirlapur UK and Urban JP: Notochordal intervertebral
disc cells: Sensitivity to nutrient deprivation. Arthritis Rheum.
60:1026–1034. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Smith LJ, Nerurkar NL, Choi KS, Harfe BD
and Elliott DM: Degeneration and regeneration of the intervertebral
disc: Lessons from development. Dis Model Mech. 4:31–41. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Takatalo J, Karppinen J, Taimela S,
Niinimäki J, Laitinen J, Blanco Sequeiros R, Paananen M, Remes J,
Näyhä S, Tammelin T, et al: Body mass index is associated with
lumbar disc degeneration in young Finnish males: Subsample of
Northern Finland birth cohort study 1986. BMC Musculoskelet Disord.
14:872013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wang YX and Griffith JF: Menopause causes
vertebral endplate degeneration and decrease in nutrient diffusion
to the intervertebral discs. Med Hypotheses. 77:18–20. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Omair A, Holden M, Lie BA, Reikeras O and
Brox JI: Treatment outcome of chronic low back pain and
radiographic lumbar disc degeneration are associated with
inflammatory and matrix degrading gene variants: A prospective
genetic association study. BMC Musculoskelet Disord. 14:1052013.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kalb S, Martirosyan NL, Kalani MY, Broc GG
and Theodore N: Genetics of the degenerated intervertebral disc.
World Neurosurg. 77:491–501. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Purmessur D, Walter BA, Roughley PJ,
Laudier DM, Hecht AC and Iatridis J: A role for TNF-α in
intervertebral disc degeneration: A non-recoverable catabolic
shift. Biochem Biophys Res Commun. 433:151–156. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Liang QQ, Li XF, Zhou Q, Xing L, Cheng SD,
Ding DF, Xu LQ, Tang DZ, Bian Q, Xi ZJ, et al: The expression of
osteoprotegerin is required for maintaining the intervertebral disc
endplate of aged mice. Bone. 48:1362–1369. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ciacli C and Puşchiţă M: RANKL/RANK/OPG
molecular complex-control factors in bone remodeling in psoriatic
arthritis. Rev Med Chir Soc Med Nat Iasi. 115:354–360.
2011.PubMed/NCBI
|
|
19
|
Chollet ME, Brouland JP, Bal Dit Sollier
C, Bauduer F, Drouet L and Bellucci S: Evidence of a colocalisation
of osteoprotegerin (OPG) with von Willebrand factor (VWF) in
platelets and megakaryocytes alpha granules. Studies from normal
and grey platelets. Br J Haematol. 148:805–807. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Pobeha P, Petrasova D, Tkacova R and Joppa
P: Circulatory osteoprotegerin is related to osteoporosis of the
hip in patients with COPD. Respir Med. 108:621–627. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Jayakumar P and Di Silvio L: Osteoblasts
in bone tissue engineering. Proc Inst Mech Eng H. 224:1415–1440.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Tousoulis D, Siasos G, Maniatis K,
Oikonomou E, Kioufis S, Zaromitidou M, Paraskevopoulos T, Michalea
S, Kollia C, Miliou A, et al: Serum osteoprotegerin and osteopontin
levels are associated with arterial stiffness and the presence and
severity of coronary artery disease. Int J Cardiol. 167:1924–1928.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Trouvin AP and Goeb V: Receptor activator
of nuclear factor-κB ligand and osteoprotegerin: Maintaining the
balance to prevent bone loss. Clin Interv Aging. 5:345–354.
2010.PubMed/NCBI
|
|
24
|
Ohmori R, Momiyama Y, Taniguchi H, Tanaka
N, Kato R, Nakamura H, Ohsuzu F, Nagano M and Egashira T:
Association between osteoprotegerin gene polymorphism and coronary
artery disease in Japanese men. Atherosclerosis. 187:215–217. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Granchi D, Pellacani A, Spina M, Cenni E,
Savarino LM, Baldini N and Giunti A: Serum levels of
osteoprotegerin and receptor activator of nuclear factor-kappaB
ligand as markers of periprosthetic osteolysis. J Bone Joint Surg
Am. 88:1501–1509. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Vega D, Maalouf NM and Sakhaee K: CLINICAL
Review #: The role of receptor activator of nuclear factor-kappaB
(RANK)/RANK ligand/osteoprotegerin: Clinical implications. J Clin
Endocrinol Metab. 92:4514–4521. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Grimaud E, Soubigou L, Couillaud S,
Coipeau P, Moreau A, Passuti N, Gouin F, Redini F and Heymann D:
Receptor activator of nuclear factor kappaB ligand
(RANKL)/osteoprotegerin (OPG) ratio is increased in severe
osteolysis. Am J Pathol. 163:2021–2031. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Silva I and Branco JC: Rank/Rankl/opg:
Literature review. Acta Reumatol Port. 36:209–218. 2011.PubMed/NCBI
|
|
29
|
Nakamura M, Udagawa N, Matsuura S, Mogi M,
Nakamura H, Horiuchi H, Saito N, Hiraoka BY, Kobayashi Y, Takaoka
K, et al: Osteoprotegerin regulates bone formation through a
coupling mechanism with bone resorption. Endocrinology.
144:5441–5449. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Jurado S, Nogués X, Agueda L,
Garcia-Giralt N, Urreizti R, Yoskovitz G, Pérez-Edo L, Saló G,
Carreras R, Mellibovsky L, et al: Polymorphisms and haplotypes
across the osteoprotegerin gene associated with bone mineral
density and osteoporotic fractures. Osteoporos Int. 21:287–296.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Sun T, Chen M, Lin X, Yu R, Zhao Y and
Wang J: The influence of osteoprotegerin genetic polymorphisms on
bone mineral density and osteoporosis in Chinese postmenopausal
women. Int Immunopharmacol. 22:200–203. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Morinaga T, Nakagawa N, Yasuda H, Tsuda E
and Higashio K: Cloning and characterization of the gene encoding
human osteoprotegerin/osteoclastogenesis-inhibitory factor. Eur J
Biochem. 254:685–691. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
García-Unzueta MT, Riancho JA, Zarrabeitia
MT, Sañudo C, Berja A, Valero C, Pesquera C, Paule B,
González-Macías J and Amado JA: Association of the 163A/G and
1181G/C osteoprotegerin polymorphism with bone mineral density.
Horm Metab Res. 40:219–224. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Vidal C, Formosa R and Xuereb-Anastasi A:
Functional polymorphisms within the TNFRSF11B (osteoprotegerin)
gene increase the risk for low bone mineral density. J Mol
Endocrinol. 47:327–333. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Kim JG, Kim JH, Kim JY, Ku SY, Jee BC, Suh
CS, Kim SH and Choi YM: Association between osteoprotegerin (OPG),
receptor activator of nuclear factor-kappaB (RANK) and RANK ligand
(RANKL) gene polymorphisms and circulating OPG, soluble RANKL
levels and bone mineral density in Korean postmenopausal women.
Menopause. 14:913–918. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Liu S, Yi Z, Ling M and Shi J: Association
between g.19163A>G and g.23298T>C genetic variants of the
osteoprotegerin gene and bone mineral density in Chinese women.
Hormones (Athens). 12:578–583. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Wang Q, Chen Z, Huang Y, Li Q, Zhu L, Cai
X, He G, Xie Y and Liu Q: The relationship between osteoprotegerin
gene polymorphisms and bone mineral density in Chinese
postmenopausal women. Int Immunopharmacol. 17:404–407. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Wang Y, Battié MC, Boyd SK and Videman T:
The osseous endplates in lumbar vertebrae: Thickness, bone mineral
density and their associations with age and disk degeneration.
Bone. 48:804–809. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Salo S, Leinonen V, Rikkonen T, Vainio P,
Marttila J, Honkanen R, Tuppurainen M, Kröger H and Sirola J:
Association between bone mineral density and lumbar disc
degeneration. Maturitas. 79:449–455. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
World Medical Association: World Medical
Association Declaration of Helsinki: Ethical principles for medical
research involving human subjects. JAMA. 310:2191–2194. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Kim NK, Shin DA, Han IB, Yoo EH, Kim SH
and Chung SS: The association of aggrecan gene polymorphism with
the risk of intervertebral disc degeneration. Acta Neurochir
(Wien). 153:129–133. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Mwale F, Iatridis JC and Antoniou J:
Quantitative MRI as a diagnostic tool of intervertebral disc matrix
composition and integrity. Eur Spine J. 17(Suppl 4): 432–440. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Hashemi M, Ebrahimi M, Amininia S, Naderi
M, Eskandari-Nasab E and Taheri M: Evaluation of rs3102735 and
rs2073617 Osteoprotegerin Gene Polymorphisms and the Risk of
Childhood Acute lymphoblastic Leukemia in Zahedan Southeast Iran.
Int J Hematol Oncol Stem Cell Res. 8:39–44. 2014.PubMed/NCBI
|
|
44
|
Stephens M and Scheet P: Accounting for
decay of linkage disequilibrium in haplotype inference and
missing-data imputation. Am J Hum Genet. 76:449–462. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Risbud MV and Shapiro IM: Role of
cytokines in intervertebral disc degeneration: Pain and disc
content. Nat Rev Rheumatol. 10:44–56. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Shamji MF, Setton LA, Jarvis W, So S, Chen
J, Jing L, Bullock R, Isaacs RE, Brown C and Richardson WJ:
Proinflammatory cytokine expression profile in degenerated and
herniated human intervertebral disc tissues. Arthritis Rheum.
62:1974–1982. 2010.PubMed/NCBI
|
|
47
|
Li WF, Hou SX, Yu B, Li MM, Férec C and
Chen JM: Genetics of osteoporosis: Accelerating pace in gene
identification and validation. Hum Genet. 127:249–285. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Zupan J, Mencej-Bedrac S, Jurković-Mlakar
S, Prezelj J and Marc J: Gene-gene interactions in RANK/RANKL/OPG
system influence bone mineral density in postmenopausal women. J
Steroid Biochem Mol Biol. 118:102–106. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Shimizu S, Asou Y, Itoh S, Chung UI,
Kawaguchi H, Shinomiya K and Muneta T: Prevention of cartilage
destruction with intraarticular osteoclastogenesis inhibitory
factor/osteoprotegerin in a murine model of osteoarthritis.
Arthritis Rheum. 56:3358–3365. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Kadri A, Ea HK, Bazille C, Hannouche D,
Lioté F and Cohen-Solal ME: Osteoprotegerin inhibits cartilage
degradation through an effect on trabecular bone in murine
experimental osteoarthritis. Arthritis Rheum. 58:2379–2386. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Styrkarsdottir U, Halldorsson BV,
Gretarsdottir S, Gudbjartsson DF, Walters GB, Ingvarsson T,
Jonsdottir T, Saemundsdottir J, Center JR, Nguyen TV, et al:
Multiple genetic loci for bone mineral density and fractures. N
Engl J Med. 358:2355–2365. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Lee YH, Woo JH, Choi SJ, Ji JD and Song
GG: Associations between osteoprotegerin polymorphisms and bone
mineral density: A meta-analysis. Mol Biol Rep. 37:227–234. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Stolina M, Schett G, Dwyer D, Vonderfecht
S, Middleton S, Duryea D, Pacheco E, Van G, Bolon B, Feige U, et
al: RANKL inhibition by osteoprotegerin prevents bone loss without
affecting local or systemic inflammation parameters in two rat
arthritis models: Comparison with anti-TNFalpha or anti-IL-1
therapies. Arthritis Res Ther. 11:R1872009. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Kepler CK, Ponnappan RK, Tannoury CA,
Risbud MV and Anderson DG: The molecular basis of intervertebral
disc degeneration. Spine J. 13:318–330. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Raj PP: Intervertebral disc:
Anatomy-physiology-pathophysiology-treatment. Pain Pract. 8:18–44.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Matzko ME, Bowen TR and Smith WR:
Orthogenomics: An update. J Am Acad Orthop Surg. 20:536–546. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Biscetti F, Porreca CF, Bertucci F,
Straface G, Santoliquido A, Tondi P, Angelini F, Pitocco D, Santoro
L, Gasbarrini A, et al: TNFRSF11B gene polymorphisms increased risk
of peripheral arterial occlusive disease and critical limb ischemia
in patients with type 2 diabetes. Acta Diabetol. 51:1025–1032.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Straface G, Biscetti F, Pitocco D,
Bertoletti G, Misuraca M, Vincenzoni C, Snider F, Arena V,
Stigliano E, Angelini F, et al: Assessment of the genetic effects
of polymorphisms in the osteoprotegerin gene, TNFRSF11B, on serum
osteoprotegerin levels and carotid plaque vulnerability. Stroke.
42:3022–3028. 2011. View Article : Google Scholar : PubMed/NCBI
|