Introduction
Thyroid nodules are commonly benign and the reported
prevalence widely varies depending on the population studied and
the methods used to detect the nodules (1). Globally, thyroid cancer is increasing
rapidly and resulted in 36,000 fatalities in 2010, an increase from
24,000 in 1990, although 5 year survival rates are high following
treatment (2–4). A previous study state that, between
1992 and 2006, a total of 43,644 thyroid cancer cases wee diagnosed
in the United States (5). In China,
thyroid cancer is the 8th most frequent cancer, and the rapid
increase in thyroid cancer incidence represents a substantial
health burden (6,7). Ultrasound (US) is an accepted standard
diagnostic method for the detection of thyroid nodules worldwide
(8). However, previous studies found
extreme variations in the assessment of thyroid nodules by US
(9–11). Conventional US has a moderate
accuracy for characterizing the nature of thyroid nodules, thus
supplementary diagnostic methods, including radionuclide scanning
and fine-needle aspiration (FNA) biopsy, are employed for improved
clinical evaluation of thyroid nodules (12–14).
With the introduction of contrast-enhanced ultrasound (CEUS) and
real-time elastography (RTE), promising results have been reported
for better accuracy in differentiating between benign and malignant
thyroid nodules (15–17).
CEUS involves the use of a contrast medium that
enhances the diagnostic imaging capabilities of traditional medical
sonography and is a milestone for diagnostics in liver tumors, with
recent studies evaluating similar application of CEUS in
characterizing thyroid gland tumors (18–23). In
addition, CEUS performed with the use of a microbubble contrast
agent may be a potentially useful adjunct in assessing thyroid
nodules, since it has a high specificity of 84.8% and high
sensitivity of 76.9% (21). CEUS is
also amenable to combination approaches, and dynamical evaluation
of microcirculation with CEUS in combination with color-coded and
power Doppler sonography was demonstrated to yield reliable
preoperative results in the characterization of thyroid adenomas
(22). Furthermore, the combination
of CEUS with acoustic radiation force impulse (ARFI) has been shown
to significantly improve the diagnostic accuracy of thyroid nodules
(23). As a noninvasive technique
for evaluating thyroid nodules, US-based elastography encompasses a
variety of approaches, including RTE, acoustic radiation force
impulse imaging and supersonic shear imaging (24). RTE is an imaging technique that can
directly reveal the physical properties of tissues through the use
of conventional US probes. Elastography was recently demonstrated
to be an invaluable diagnostic method in differentiating between
various pathologies in 283 patients with Hashimoto's thyroiditis
(16,25). A strain index ratio and cut-off value
of the thyroid tissue was higher in patients with chronic
autoimmune thyroiditis compared with the values in normal thyroid
parenchyma in RTE, suggesting that these two diagnostic parameters
may be helpful for diagnosis or follow-up of lymphoma and malign
nodules (26). Furthermore, the
diagnostic values of CEUS or RTE alone were previously assessed in
the characterization of thyroid nodules (16). RTE may be useful in the diagnosis of
thyroid nodules to exclude papillary thyroid cancer, but not
follicular carcinoma; CEUS shows no improvement in the
characterization of thyroid nodules (16). A previous study also revealed that
Q-elastography is a better tool in differentiating the underlying
nature of thyroid nodules compared with CEUS (27); however, a combination of CEUS and RTE
in the differentiation of benign and malignant thyroid nodules
requires to be further evaluated.
In the current study, the diagnostic values of CEUS
alone, RTE alone, and a combination of CEUS and RTE in
distinguishing benign from malignant thyroid nodules were
examined.
Materials and methods
Subjects
Between August 2012 and June 2014, 97 patients (50
male and 47 female patients; mean age, 48.6±12.4; age range, 27–70
years) scheduled for surgical removal of thyroid nodules were
recruited at the Department of Gland Surgery. The patient inclusion
criteria for this study were the following: i) Surgery indication
for palpable or impalpable thyroid nodules; ii) patients scheduled
for surgical removal of thyroid nodules; iii) the final diagnosis
was confirmed by histopathologic examination of resected thyroid
gland tissue; and iv) the patients did not suffer from any serious
allergies. Histopathological changes were observed by hematoxylin
and eosin (HE) staining. The study was approved by the
Institutional Review Board of the Second and Third Hospital of
Hebei Medical University. Written informed consent was obtained
from all participants. The study protocols conformed to the
Declaration of Helsinki (28).
CEUS
All patients were examined using a Philips IU22 US
system equipped with a L12-5 wide frequency linear array probe
(Philips Medical Systems, Inc., Bothell, WA, USA). Initially,
patients were assessed in a routine US examination in supine
position with the neck fully exposed. Thyroid nodules were
evaluated for location, size, margin, internal echo, evenness and
calcification. Contrast pulse sequencing was also applied, with
probe emission frequency of 9–12 MHz, mechanical index of 0.08,
imaging depth of 50 mm, 50% image gain and US pressure of 50 kPa.
SonoVue® (Bracco Imaging SpA, Milan, Italy) was used as
US contrast agent. SonoVue® was dissolved in 5 ml 0.9%
sodium chloride and was injected as an intravenous bolus of 2.4 ml
per subject via an antecubital vein, followed by additional 5 ml
0.9% sodium chloride. Subsequent to contrast agent injection,
harmonic gray-scale CEUS was applied to scan the thyroid gland and
the nodule for at least 150 sec, and the dynamic images were
recorded.
RTE
RTE was performed with an Acuson S2000 system
(Siemens Medical Solutions, Malvern, PA, USA), with a high
frequency linear array probe (6.5–13 MHz). With the patients in the
supine position, the routine US examination was performed to locate
the thyroid nodules and the ultrasonographic features of the focus
were recorded. Subsequently, RTE was performed and the
region-of-interest (ROI) was selected for the elastography
examination (2–3 times bigger than the focus) with the probe
vibrating 1–2 times/s, while the pressure indication on the screen
was controlled within 3–4 kPa. The resultant elastogram was
displayed over the B-mode image and the images were assessed by a
color scale: Green indicated ‘medium stiffness’ of the tissue in
the ROI, blue indicated ‘harder tissue’ and red indicated ‘softer
tissue’.
Image analysis and diagnosis
criteria
The differential diagnosis of malignant or benign
thyroid nodules was based on the results obtained from CEUS and
RTE, and was performed by two experienced radiologists in a double
blinded manner. Enhancement features of lesion on CEUS included: i)
Margin enhancement, defined as clear or unclear based on the
clarity of the margin between the lesion and peripheral tissue; ii)
shape enhancement, classified as regular or irregular based on the
shapes observed following contrast agent injection; iii) area
enhancement, defined as <50 or ≥50% based on the area of the
enhancement part/the lesion section at the peak enhancement; iv)
enhancement degree, characterized as low, equal or high intensity
when compared with the surrounding thyroid parenchyma; and v) type
of enhancement, including homogeneous (relative homogeneous diffuse
enhancement in lesions), heterogeneous (diffuse enhancement
presenting inhomogeneous or regional microvesicle distribution) and
ring enhancement (ring structure, such as round, oval or oblate
spheroid). In CEUS, lesions that showed inhomogeneous and low
enhancement were considered as diagnostic criteria for malignant
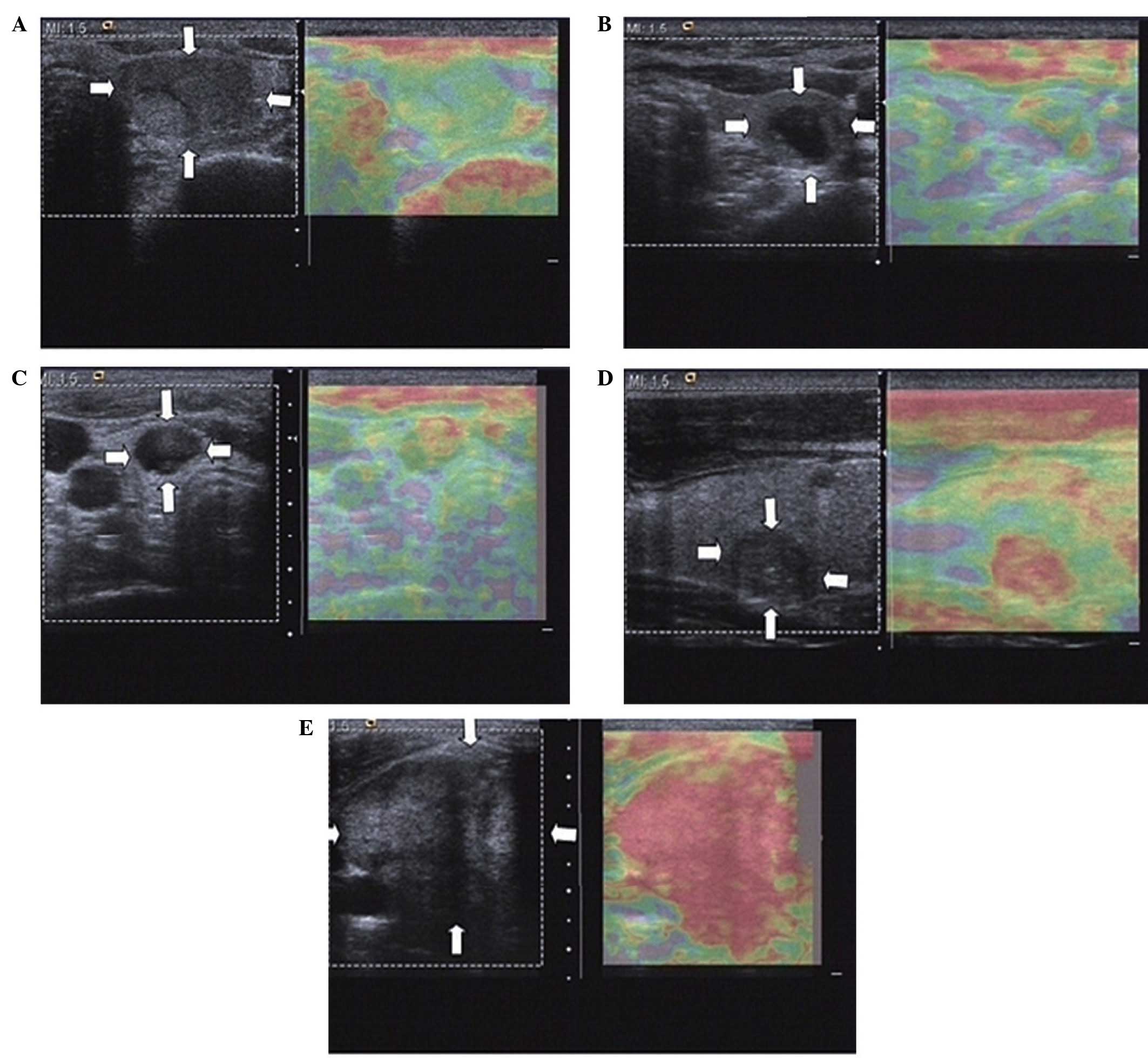
nodules (29,30). Elasticity was classified in five
different patterns on RTE scans, as described previously (31,32).
These patterns include the following: classification I, in which
the nodule is displayed homogeneously in green; classification II,
in which the nodule is displayed predominantly in green with few
red areas/spots; classification III, in which the nodule is
displayed predominantly in red with few green areas/spots;
classification IV, where the nodule is displayed homogeneously in
red; and classification V, where the nodule is displayed with
mainly red areas. The elasticity of the thyroid nodules was
observed using real-time elastography along with the corresponding
contrast enhanced ultrasound images (Fig. 1). Nodules with elasticity III–V were
suggested to be malignant thyroid nodules. The patients were
diagnosed using the following CEUS and RTE combined method: CEUS
and RTE-positive, malignancy was observed following both CEUS and
RTE image analysis; either CEUS or RTE-positive, malignancy was
observed following either CEUS or RTE image analysis; CEUS and
RTE-negative, benign in both CEUS and RTE images.
Hematoxylin and eosin staining
Thyroid nodule tissue samples were obtained by
surgery, and the the tissue samples obtained were fixed in 10%
formaldehyde solution, dehydrated and embedded in paraffin. Each
paraffin-embedded tissue sample was cut into 6 sections (3 µm)
using a microtome (1512-type Ultra-Thin Semiautomatic Microtome;
Leica Microsystems GmbH, Wetzlar, Germany). The tissue sections
were then placed on glass slides, treated with 98% sulphuric acid,
washed with distilled water, treated with 95% alcohol overnight,
and coated with 1% poly-L-lysine (Beijing Solarbio Science &
Technology Co., Ltd., Beijing, China) following high temperature
drying at 60°C. Hematoxylin and eosin staining was performed after
overnight oven treatment at 65°C. Briefly, the tissue samples were
dewaxed twice in xylene for 10 min, rehydrated with graded ethanol
(2 min/grade; 100, 95, 85 and 70% ethanol) and washed for 2–3 min
with distilled water. The tissue samples were then stained with
hematoxylin for 5 min at room temperature, rinsed in running water,
treated with 1% hydrochloric acid alcohol for 30 sec, and washed in
running water for 15 min or warm water (~50°C) for 5 min. The
tissue samples were then stained with eosin for 2 min at room
temperature, dehydrated with graded ethanol (70, 85, 95 and 100%
ethanol), twice deparaffinized with xylene for 10 min, and sealed
with neutral gum. The results were observed and images of the
tissue samples were captured using an Olympus CHK microscope
imaging system (Olympus Corporation, Tokyo, Japan).
Statistical analysis
Continuous variables are presented as the mean ±
standard deviation, while categorical variables are presented as
percentages of the total value. Comparisons between groups were
performed using χ2 test and Student's t-test, as
appropriate. Considering the postoperative pathological results as
the golden standard, the sensitivity, specificity, positive
predictive value (PPV), negative predictive value (NPV) and
accuracy of CEUS alone, RTE alone and combination of CEUS and RTE
were calculated. To characterize the diagnostic performance of RTE
and CEUS, receiver operating characteristic (ROC) curve analyses
were implemented and estimated by Hanley-McNeil non-parametric
analysis. Statistical analysis was conducted using the SPSS version
20.0 software (IBM Corp., Armonk, NY, USA). P<0.05 was
considered to indicate a statistically significant difference.
Results
Pathological examination and US
characteristics of thyroid nodules
Pathological examination of 109 nodules in the 97
patients (some patients had more than one nodule) showed 66
papillary carcinomas and 43 benign lesions (including 21 adenoma
and 22 nodular goiters). In addition, among the 109 nodules,
solitary nodules were observed in 14 cases and multiple nodules
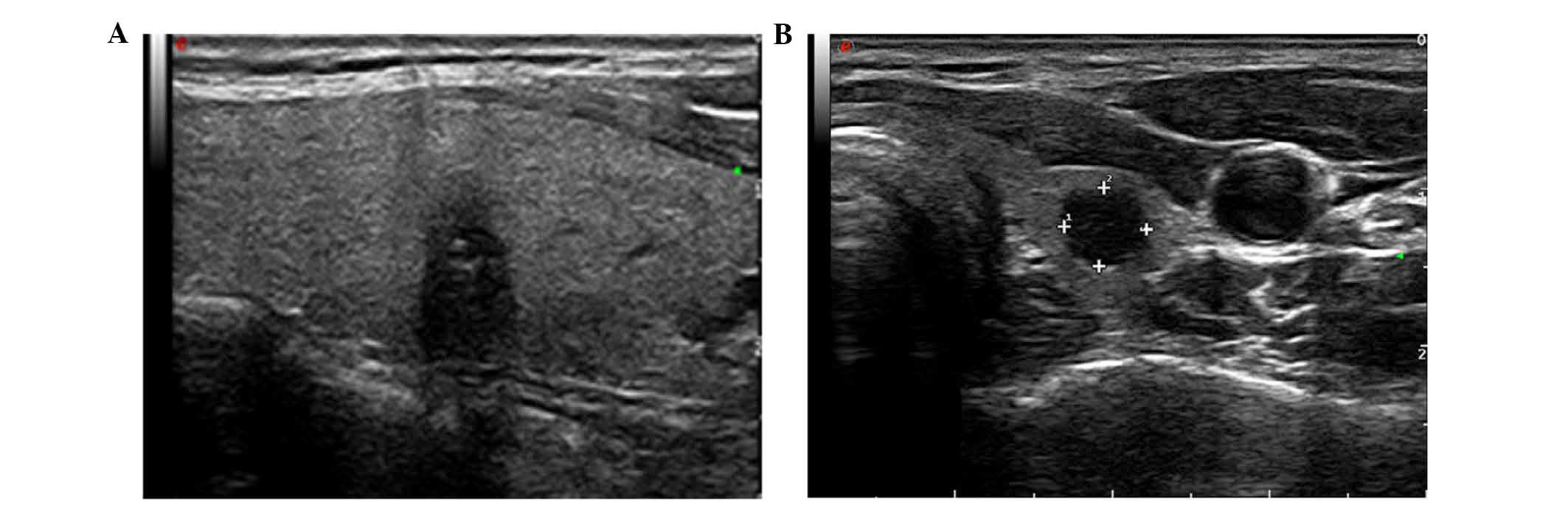
were observed in 83 cases. Conventional US of the 66 papillary
carcinomas revealed 37 nodules with irregular shape, 34 nodules
with a longitudinal/transverse diameter aspect ratio of >1, 39
nodules with heterogeneous internal echoes and 49 nodules with
microcalcifications (Fig. 2A). All
papillary carcinoma nodules presented with a poorly-defined margin
and marked hypoechogenicity, while the mean diameter of the nodules
was 2.41±1.14 cm.
Among the 43 benign lesions, conventional US showed
20 nodules with irregular shape, 9 nodules with an aspect ratio of
>1, 30 nodules with marked hyperechogenicity, 20 nodules with
heterogeneous internal echoes, and 13 nodules with
microcalcifications (Fig. 2B). In
addition, all nodules presented with a poorly-defined margin and
the mean size of the examined nodules was 2.32±1.04 cm.
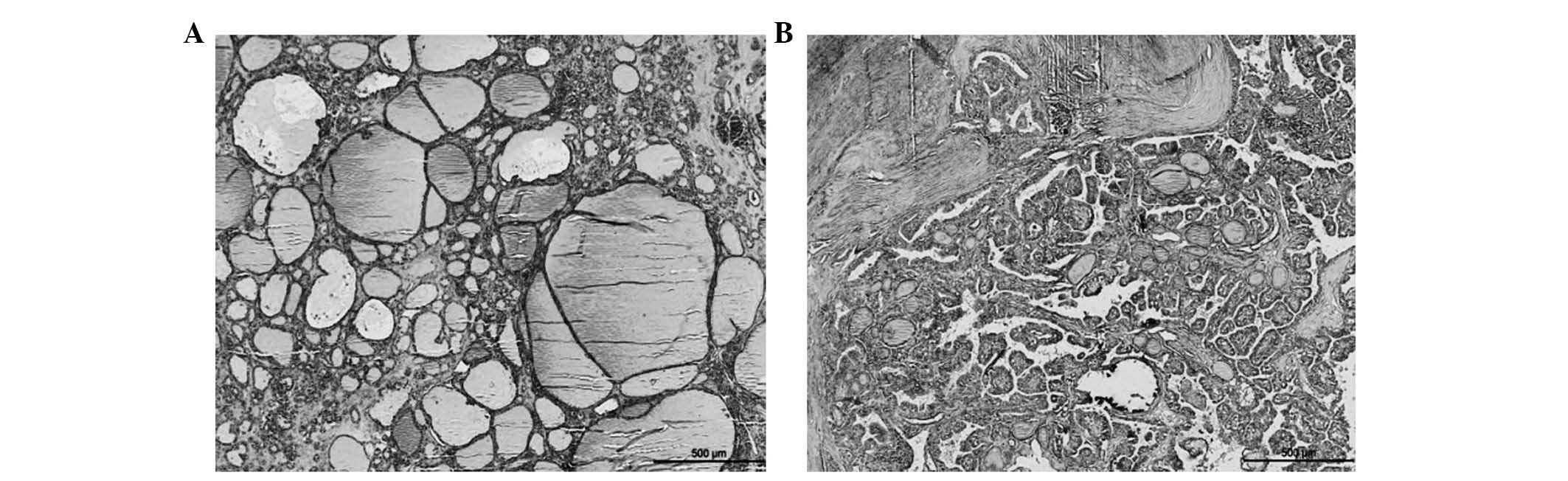
Significant differences were detected in the aspect
ratio, margin, echogenicity and presence of calcifications (all
P<0.05) between the malignant and benign tumors. However, no
significant differences were identified in the lesion shape or
echotexture (both P>0.05; Table
I). The results demonstrate that thyroid nodules with poorly
defined tumors, aspect ratios >1 and microcalcifications are
likely to be malignant (as shown in Table I). The histopathological images of
the benign and malignant tumors are shown in Fig. 3.
 | Table I.Characteristics of conventional
ultrasound of benign and malignant thyroid nodules. |
Table I.
Characteristics of conventional
ultrasound of benign and malignant thyroid nodules.
| Characteristic | Malignant (n=66) | Benign (n=43) | χ2 | P-value |
|---|
| Shape |
|
|
0.952 |
0.329 |
|
Regular | 29 | 23 |
|
|
|
Irregular | 37 | 20 |
|
|
| Aspect ratio |
|
| 10.200 |
0.001 |
|
<1 | 32 | 34 |
|
|
| ≥1 | 34 | 9 |
|
|
| Margin |
|
| 77.840 | <0.001 |
|
Well-defined, smooth | 9 | 43 |
|
|
|
Poorly-defined | 57 | 0 |
|
|
| Echogenicity |
|
| 21.010 | <0.001 |
|
Hyperechogenicity | 17 | 30 |
|
|
|
Isoechogenicity | 24 | 8 |
|
|
|
Hypoechogenicity | 25 | 5 |
|
|
| Echotexture |
|
|
0.333 |
0.564 |
|
Homogeneous | 27 | 20 |
|
|
|
Heterogeneous | 39 | 23 |
|
|
| Calcification |
|
| 20.560 | <0.001 |
|
Microcalcification | 49 | 13 |
|
|
|
Macrocalcification | 17 | 30 |
|
|
CEUS characteristics of thyroid
nodules
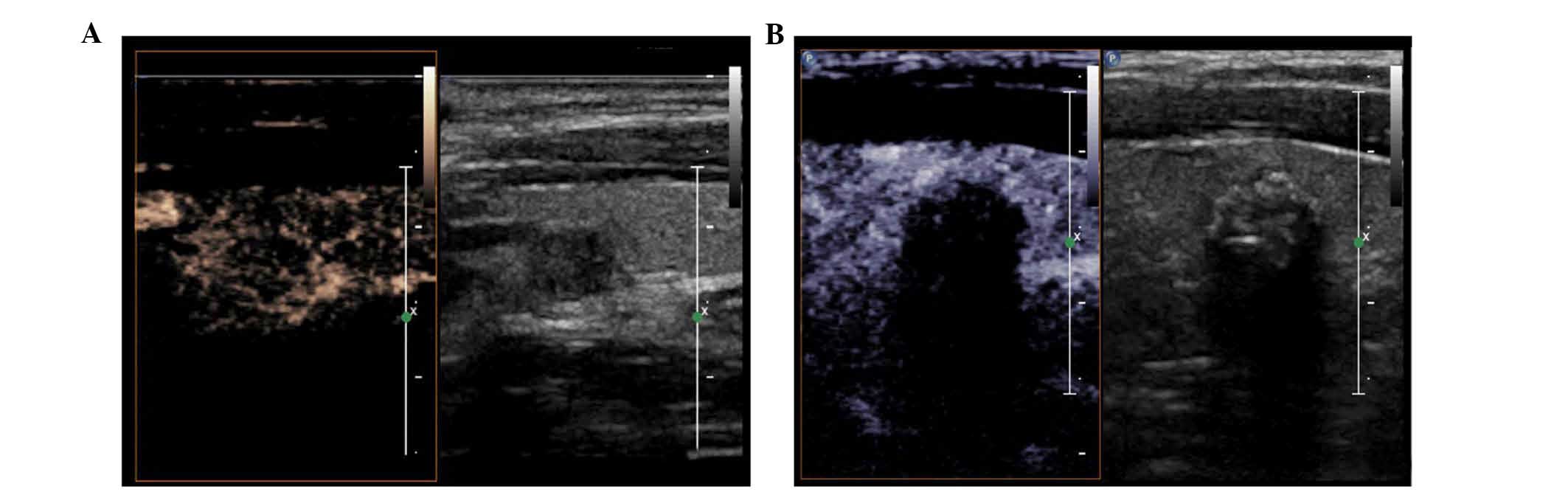
On CEUS scans, 40 out of the 43 benign nodules
appeared to have well-defined margins, 38 nodules had a regular
shape, 22 nodules showed an area of enhancement of >50% and
equal or high intensity, 4 nodules had lesions with heterogeneous
enhancement, 26 nodules showed homogeneous enhancement, and 13
nodules presented with ring enhancement. The characteristics of
representative examples of benign nodules on CEUS are presented in
Fig. 4A. By contrast, out of the 66
malignant nodules, 15 nodules had lesions with well-defined margin,
15 nodules exhibited a regular shape, 50 nodules had area of
enhancement of >50% with equal or high intensity, 7 nodules had
lesions with homogeneous enhancement, 53 heterogeneous enhancement
and 6 ring enhancement. The characteristics of representative
examples of malignant nodules on CEUS are presented in Fig. 4B. The findings showed statistically
significant differences in the enhancement margin, shape,
enhancement area, intensity and type of enhancement between benign
and malignant thyroid nodules (all P<0.05; Table II).
| Table II.Characteristics of contrast-enhanced
ultrasound of benign and malignant thyroid nodules. |
Table II.
Characteristics of contrast-enhanced
ultrasound of benign and malignant thyroid nodules.
| Enhancement
characteristics | Malignant
(n=66) | Benign (n=43) | χ2 | P-value |
|---|
| Margin |
|
| 51.47 | <0.001 |
|
Well-defined | 15 | 40 |
|
|
|
Poorly-defined | 51 | 3 |
|
|
| Shape |
|
| 44.91 | <0.001 |
|
Regular | 15 | 38 |
|
|
|
Irregular | 51 | 5 |
|
|
| Area |
|
| 7.024 | <0.008 |
|
<50% | 16 | 21 |
|
|
|
≥50% | 50 | 22 |
|
|
| Intensity |
|
| 52.63 | <0.001 |
|
High | 7 | 20 |
|
|
|
Equal | 6 | 19 |
|
|
|
Low | 53 | 4 |
|
|
| Type |
|
| 10.23 |
0.006 |
|
Heterogeneous | 53 | 4 |
|
|
|
Homogeneous | 7 | 26 |
|
|
|
Ring | 6 | 13 |
|
|
RTE characteristics of thyroid
nodules
As shown in Table
III, in the 43 benign thyroid nodules, elasticity I was seen in
25 nodules, elasticity II in 13 nodules, elasticity III in 4
nodules, elasticity IV in 1 nodule, and no nodule exhibited an
elasticity classification V. By contrast, in the 66 malignant
thyroid nodules, there were 6 nodules in elasticity I, 5 nodules in
elasticity II, 17 nodules in elasticity III, 25 nodules in
elasticity IV, 13 nodules in elasticity V. The results indicated
that significant differences existed in the elasticity
classifications I, II, IV and V between malignant and benign
nodules (all P<0.001), whereas no difference was identified in
elasticity classification III (P>0.05). These results suggest
that benign tumors commonly exhibit lower elasticity grades,
whereas elasticity grades III–V are predominantly observed in
malignant nodules.
| Table III.Elasticity imaging classification of
benign and malignant thyroid nodules. |
Table III.
Elasticity imaging classification of
benign and malignant thyroid nodules.
| Elasticity imaging
classification | Malignant
(n=66) | Benign (n=43) | χ2 | P-value |
|---|
| I | 6 | 25 | 16.400 | <0.001 |
| II | 5 | 13 |
6.731 |
0.010 |
| III | 17 | 4 |
2.931 |
0.075 |
| IV | 25 | 1 | 12.110 | <0.001 |
| V | 13 | 0 |
7.920 |
0.005 |
Diagnostic accuracy of CEUS alone, RTE
alone and CEUS+RTE in thyroid nodules
The sensitivity and specificity of CEUS in
differentiating benign and malignant thyroid nodules were 81.82 and
90.70%, respectively. In addition, the PPV was 93.10, the NPV was
90.70%, and the accuracy was found to be 85.32%. With respect to
RTE, the sensitivity was 80.30%, and the specificity was 88.37%,
while the PPV and NPV were 91.38 and 88.37%, respectively, and the
accuracy of RTE was 83.49%. Combined diagnosis using CEUS and RTE
had a sensitivity of 95.45%, a specificity of 95.35%, a PPV of
96.92, an NPV of 95.35%, and an accuracy of 96.00%. Compared with
the CEUS and RTE alone, the combined RTE and CEUS approach was
associated with higher sensitivity and specificity for predicting
benign and malignant thyroid nodules (P<0.05). Notably, there
was no significant difference in the sensitivity, specificity, PPV,
NPV and accuracy between CEUS and RTE (P>0.05; Table IV).
| Table IV.Comparison of the sensitivity,
specificity, PPV, NPV and accuracy of CEUS alone, RTE alone and
combination of CEUS + RTE in the differential diagnosis of
malignant and benign thyroid nodules. |
Table IV.
Comparison of the sensitivity,
specificity, PPV, NPV and accuracy of CEUS alone, RTE alone and
combination of CEUS + RTE in the differential diagnosis of
malignant and benign thyroid nodules.
|
| Pathological
results |
|
|
|
|
|
|---|
|
|
|
|
|
|
|
|
|---|
| Detection | Malignant
(n=66) | Benign (n=43) | Sensitivity | Specificity | PPV | NPV | Accuracy |
|---|
| CEUS |
|
| 81.82% | 90.70% | 93.10% | 90.70% | 85.32% |
|
Malignant | 54 | 4 |
|
|
|
|
|
|
Benign | 12 | 39 |
|
|
|
|
|
| RTE |
|
| 80.30% | 88.37% | 91.38% | 88.37% | 83.49% |
|
Malignant | 53 | 5 |
|
|
|
|
|
|
Benign | 13 | 38 |
|
|
|
|
|
| CEUS + RTE |
|
| 95.45%a,b | 95.35%a,b | 96.92% | 95.35% | 95.41%
a,b |
|
Positive (all/any) | 63 | 2 |
|
|
|
|
|
|
Negative (all) | 3 | 41 |
|
|
|
|
|
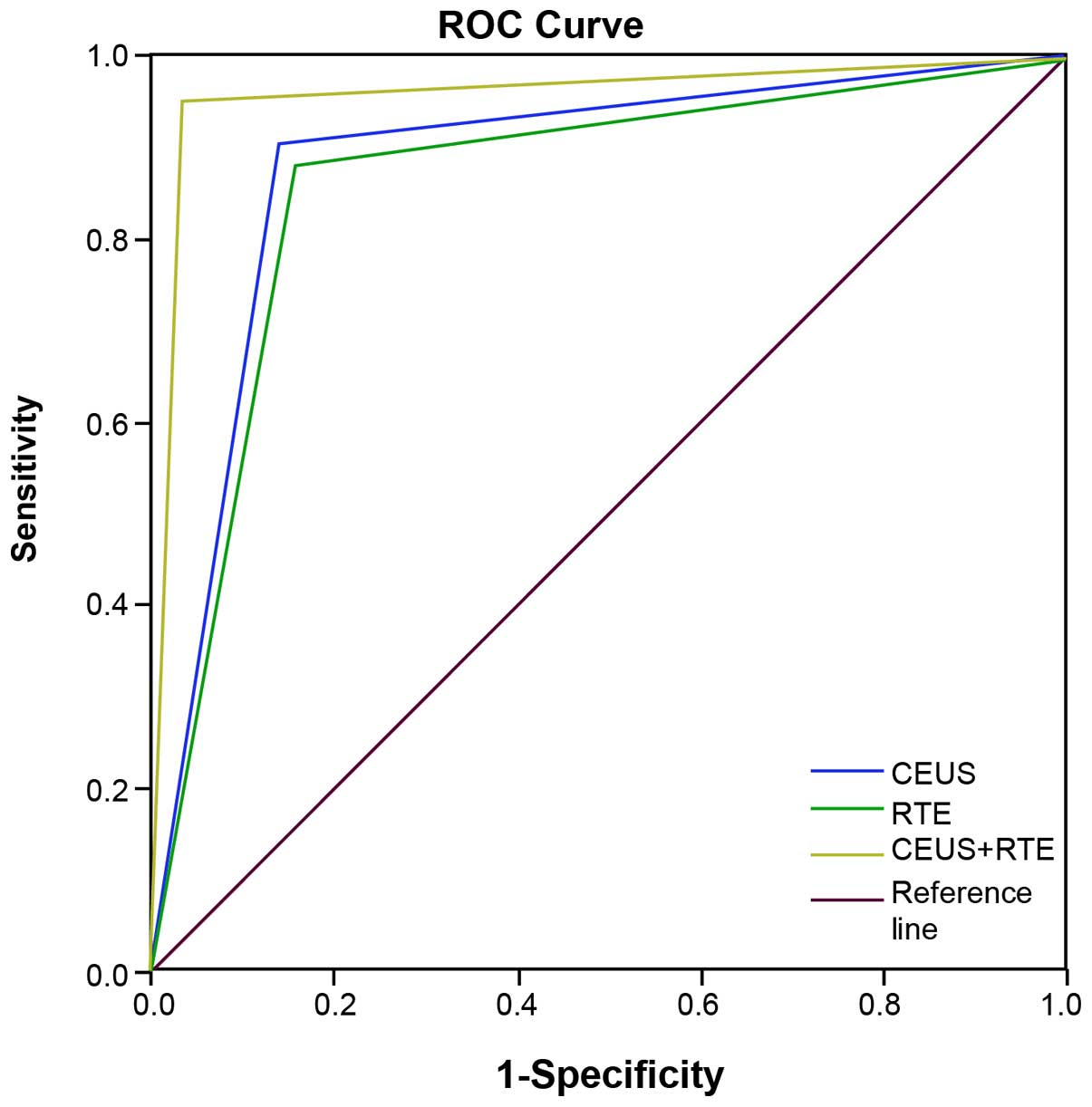
Based on the results of ROC analysis, the area under
the curve (AUC) was 0.883 [95% confidence interval (CI),
0.810–0.956], 0.863 (95% CI, 0.785–0.841) and 0.959 (95% CI,
0.904–1.000) for CEUS, RTE and CEUS + RTE, respectively (Table V). Statistically significant
differences in AUC were detected between CEUS, RTE and CEUS + RTE,
and the reference (AUC=0.5; all P<0.001). Additionally, a
significant difference in AUC was found between RTE and CEUS + RTE
(P<0.05), while a similar association was not observed between
CEUS and RTE, CEUS and CEUS+RT (all P>0.05; Table V). The ROC curve for CEUS, RTE and
CEUS + RTE (Hanley-McNeil non-parametric analysis) for
differentiation of thyroid nodules is shown in Fig. 5.
| Table V.Results of receiver operating
characteristic (ROC) curve analysis for CEUS alone, RTE alone and
combination of CEUS + RTE in the differential diagnosis of
malignant and benign thyroid nodules. |
Table V.
Results of receiver operating
characteristic (ROC) curve analysis for CEUS alone, RTE alone and
combination of CEUS + RTE in the differential diagnosis of
malignant and benign thyroid nodules.
|
|
|
|
| 95% CI |
|---|
|
|
|
|
|
|
|---|
| Diagnostic
approach | AUC | Standard error |
P-valueb | Upper limit | Lower limit |
|---|
| CEUS | 0.883 | 0.037 | <0.001 | 0.810 | 0.956 |
| RTE | 0.863 | 0.040 | <0.001 | 0.785 | 0.841 |
| CEUS + RTE |
0.959a | 0.023 | <0.001 | 0.904 | 1.000 |
Discussion
The present study evaluated the clinical value of
CEUS and RTE, alone and in combination, in differentiating between
benign and malignant thyroid nodules. To the best of our knowledge,
this is the first such analysis to conclude that a combination of
RTE and CEUS has a better diagnostic value for thyroid nodules.
Significant findings in the present study demonstrated that CEUS +
RTE displayed a higher sensitivity and specificity when compared
with CEUS or RTE alone, indicating the high diagnostic performance
of CEUS + RTE in distinguishing benign from malignant thyroid
nodules.
The diagnostic performance of CEUS and RTE has been
individually assessed by numerous studies (33–35). On
CEUS scans, papillary thyroid carcinoma shows a heterogeneous low
enhancement pattern, whereas nodular goiters show an equal
enhancement pattern (28). The
detection of papillary thyroid carcinomas with low enhancement has
a sensitivity of 96.8%, specificity of 95.0% and accuracy of 95.9%
(36). CEUS has been demonstrated to
have a high diagnostic value in the differential diagnosis of
benign and malignant calcified thyroid nodules, with sensitivity,
specificity, PPV, NPV and accuracy of 92.75, 90.91, 86.49, 95.24
and 91.62%, respectively (30). A
previous meta-analysis assessed the accuracy of CEUS in diagnosing
thyroid nodules and the pooled sensitivity, specificity, and
positive and negative likelihood ratios were found to be 0.853,
0.876, 5.822 and 0.195, respectively (19). In addition, the diagnostic odds ratio
and AUC were 34.730 and 0.9162, respectively (19). It has been suggested that RTE has a
high sensitivity and specificity for the diagnosis of malignant
thyroid nodules, with an overall mean sensitivity and specificity
of 92% (95% CI, 88–96) and 90% (95%CI, 85–95), respectively
(37). This demonstrated that RTE
may be useful in conjunction or even instead of fine-needle
aspiration biopsy for the selection of patients with thyroid
nodules requiring surgery (37).
Furthermore, according to semiquantitative elastosonography, the
sensitivity, specificity, PPV and NPV were 95, 88, 97 and 91%
respectively, whereas in CEUS, the sensitivity, specificity, PPV
and NPV were 79, 91, 83 and 89% respectively (22). CEUS and quantitative-elastosonography
are both more specific when compared with US, while
semiquantitative elastosonography seems to be more sensitive than
CEUS (27). RTE is a promising
diagnostic method that may be applied with a high NPV in the
investigation of thyroid nodules in order to exclude papillary
thyroid carcinoma, while CEUS with SonoVue® have not
been found to improve the characterization of thyroid nodules
(16).
In the current study, the margin, shape, area,
intensity and type of enhancement presented with evident
differences between benign and malignant thyroid nodules on CEUS
scans. The sensitivity and specificity of CEUS in the
differentiation between benign and malignant thyroid nodules were
81.82 and 90.70%, respectively, with PPV and NPV of 93.10 and
90.70%, respectively, while the accuracy was found to be 85.32%. As
for RTE, the elasticity classifications I, II, IV and V observed in
the scans differed between benign and malignant thyroid nodules.
The sensitivity was 80.30%, the specificity was 88.37%, PPV was
91.38 and NPV was 88.37%, while the accuracy of RTE was 83.49%. No
significant difference was found in the diagnostic performance of
CEUS or RTE alone for distinguishing benign from malignant thyroid
nodules. CEUS + RTE presented with higher sensitivity and
specificity when compared with CEUS or RTE alone in differentiating
between the nodules. This may be due to CEUS + RTE providing
noninvasive imaging of the mechanical characteristics of tissues,
along with the use of a contrast medium providing an indirect
description of intra-nodular vascularisation (38,39). RTE
conducted during endoscopic ultrasound allows the evaluation of
tissue stiffness for better characterization of the lesions
(39). In a previous study, liver
metastases were not visible on conventional US, while multiple
metastases were observed with the application of contrast agents,
which indicates the usefulness of CEUS in the prediction of liver
metastases (40). In addition, RTE
has been suggested to be a useful tool for detecting lymph node
metastases, which have been proven to be useful prognostic factors
for papillary thyroid carcinoma (41–43).
Therefore, the potential role of CEUS + RTE in predicting the tumor
aggressiveness of thyroid nodules should be further assessed.
In conclusion, based on the results reported in the
present study, the combination of CEUS + RTE may be the most
efficient and effective diagnostic method for differential
diagnosis of malignant and benign thyroid nodules. Thus, we present
a potential improvement in the noninvasive diagnostic approach
currently used, which may lead to successful implementation in
accurate diagnosis and treatment of thyroid nodules. Further
studies are required in order to further investigate the role of
CEUS and RTE combined in the differential diagnosis of malignant
and benign thyroid nodules.
References
|
1
|
Dean DS and Gharib H: Epidemiology of
thyroid nodules. Best Pract Res Clin Endocrinol Metab. 22:901–911.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
La Vecchia C, Malvezzi M, Bosetti C,
Garavello W, Bertuccio P, Levi F and Negri E: Thyroid cancer
mortality and incidence: A global overview. Int J Cancer.
136:2187–2195. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Vigneri R, Malandrino P and Vigneri P: The
changing epidemiology of thyroid cancer: Why is incidence
increasing? Curr Opin Oncol. 27:1–7. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lozano R, Naghavi M, Foreman K, Lim S,
Shibuya K, Aboyans V, Abraham J, Adair T, Aggarwal R, Ahn SY, et
al: Global and regional mortality from 235 causes of death for 20
age groups in 1990 and 2010: A systematic analysis for the Global
Burden of Disease Study 2010. Lancet. 380:2095–2128. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Aschebrook-Kilfoy B, Ward MH, Sabra MM and
Devesa SS: Thyroid cancer incidence patterns in the United States
by histologic type, 1992–2006. Thyroid. 21:125–134. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Chen W, Zheng R, Zeng H, Zhang S and He J:
Annual report on status of cancer in China, 2011. Chin J Cancer
Res. 27:2–12. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wang Y and Wang W: Increasing incidence of
thyroid cancer in Shanghai, China, 1983–2007. Asia Pac J Public
Health. 27:NP223–NP229. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Morris LF, Ragavendra N and Yeh MW:
Evidence-based assessment of the role of ultrasonography in the
management of benign thyroid nodules. World J Surg. 32:1253–1263.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tamsel S, Demirpolat G, Erdogan M, Nart D,
Karadeniz M, Uluer H and Ozgen AG: Power Doppler US patterns of
vascularity and spectral Doppler US parameters in predicting
malignancy in thyroid nodules. Clin Radiol. 62:245–251. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kim JY, Lee CH, Kim SY, Jeon WK, Kang JH,
An SK and Jun WS: Radiologic and pathologic findings of nonpalpable
thyroid carcinomas detected by ultrasonography in a medical
screening center. J Ultrasound Med. 27:215–223. 2008.PubMed/NCBI
|
|
11
|
Algin O, Algin E, Gokalp G, Ocakoğlu G,
Erdoğan C, Saraydaroglu O and Tuncel E: Role of duplex power
Doppler ultrasound in differentiation between malignant and benign
thyroid nodules. Korean J Radiol. 11:594–602. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Iannuccilli JD, Cronan JJ and Monchik JM:
Risk for malignancy of thyroid nodules as assessed by sonographic
criteria: The need for biopsy. J Ultrasound Med. 23:1455–1464.
2004.PubMed/NCBI
|
|
13
|
Paschke R, Schmid KW, Gartner R, Mann K,
Dralle H and Reiners C: Epidemiology, pathophysiology,
guideline-adjusted diagnostics and treatment of thyroid nodules.
Med Klin (Munich). 105:80–87. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Russ G, Leboulleux S, Leenhardt L and
Hegedüs L: Thyroid incidentalomas: Epidemiology, risk
stratification with ultrasound and workup. Eur Thyroid J.
3:154–163. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Moon WJ, Jung SL, Lee JH, Na DG, Baek JH,
Lee YH, Kim J, Kim HS, Byun JS, Lee DH, et al: Benign and malignant
thyroid nodules: US differentiation-multicenter retrospective
study. Radiology. 247:762–770. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Friedrich-Rust M, Sperber A, Holzer K,
Diener J, Grünwald F, Badenhoop K, Weber S, Kriener S, Herrmann E,
Bechstein WO, et al: Real-time elastography and contrast-enhanced
ultrasound for the assessment of thyroid nodules. Exp Clin
Endocrinol Diabetes. 118:602–609. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wang Y, Dan HJ, Dan HY, Li T and Hu B:
Differential diagnosis of small single solid thyroid nodules using
real-time ultrasound elastography. J Int Med Res. 38:466–472. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Minami Y and Kudo M: Ultrasound fusion
imaging of hepatocellular carcinoma: A review of current evidence.
Dig Dis. 32:690–695. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yu D, Han Y and Chen T: Contrast-enhanced
ultrasound for differentiation of benign and malignant thyroid
lesions: Meta-analysis. Otolaryngol Head Neck Surg. 151:909–915.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Jiang J, Huang L, Zhang H, Ma W, Shang X,
Zhou Q, Gao Y, Yu S and Qi Y: Contrast-enhanced sonography of
thyroid nodules. J Clin Ultrasound. 43:153–156. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Nemec U, Nemec SF, Novotny C, Weber M,
Czerny C and Krestan CR: Quantitative evaluation of
contrast-enhanced ultrasound after intravenous administration of a
microbubble contrast agent for differentiation of benign and
malignant thyroid nodules: Assessment of diagnostic accuracy. Eur
Radiol. 22:1357–1365. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Agha A, Jung EM, Janke M, Hornung M,
Georgieva M, Schlitt HJ, Schreyer AG, Strosczcynski C and Schleder
S: Preoperative diagnosis of thyroid adenomas using high resolution
contrast-enhanced ultrasound (CEUS). Clin Hemorheol Microcirc.
55:403–409. 2013.PubMed/NCBI
|
|
23
|
Deng J, Zhou P, Tian SM, Zhang L, Li JL
and Qian Y: Comparison of diagnostic efficacy of contrast-enhanced
ultrasound, acoustic radiation force impulse imaging and their
combined use in differentiating focal solid thyroid nodules. PLoS
One. 9:e906742014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kwak JY and Kim EK: Ultrasound
elastography for thyroid nodules: Recent advances. Ultrasonography.
33:75–82. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Şahin M, Çakal E, Özbek M, Güngünes A,
Arslan MS, Akkaymak ET, Uçan B, Ünsal IÖ, Bozkurt NÇ and Delibaşi
T: Elastography in the differential diagnosis of thyroid nodules in
Hashimoto thyroiditis. Med Oncol. 31:972014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Menzilcioglu MS, Duymus M, Gungor G, Citil
S, Sahin T, Boysan SN and Sarica A: The value of real-time
ultrasound elastography in chronic autoimmune thyroiditis. Br J
Radiol. 87:201406042014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Cantisani V, Consorti F, Guerrisi A,
Guerrisi I, Ricci P, Di Segni M, Mancuso E, Scardella L, Milazzo F,
D'Ambrosio F and Antonaci A: Prospective comparative evaluation of
quantitative-elastosonography (Q-elastography) and
contrast-enhanced ultrasound for the evaluation of thyroid nodules:
Preliminary experience. Eur J Radiol. 82:1892–1898. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
M PN: World Medical Association publishes
the Revised Declaration of Helsinki. Natl Med J India.
27:562014.PubMed/NCBI
|
|
29
|
Zhang B, Jiang YX, Liu JB, Yang M, Dai Q,
Zhu QL and Gao P: Utility of contrast-enhanced ultrasound for
evaluation of thyroid nodules. Thyroid. 20:51–57. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Zhou Q, Xu YB, Jiang J, Ma WQ, Wang H, Li
M and Lei XY: Differential diagnostic value of contrast-enhanced
ultrasound in calcified thyroid nodules. Zhonghua Er Bi Yan Hou Tou
Jing Wai Ke Za Zhi. 48:726–729. 2013.(In Chinese). PubMed/NCBI
|
|
31
|
Yuan WH, Chiou HJ, Chou YH, Hsu HC, Tiu
CM, Cheng CY and Lee CH: Gray-scale and color Doppler
ultrasonographic manifestations of papillary thyroid carcinoma:
Analysis of 51 cases. Clin Imaging. 30:394–401. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Stacul F, Bertolotto M, De Gobbis F,
Calderan L, Cioffi V, Romano A, Zanconati F and Cova MA: US,
colour-Doppler US and fine-needle aspiration biopsy in the
diagnosis of thyroid nodules. Radiol Med. 112:751–762. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Patel KV1, Huang DY1 and Sidhu PS1:
Metachronous bilateral segmental testicular infarction:
multi-parametric ultrasound imaging with grey-scale ultrasound,
Doppler ultrasound, contrast-enhanced ultrasound (CEUS) and
real-time tissue elastography (RTE). J Ultrasound. 2014 May
31;17(3): 233–8. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Zheng XJ, Zhang YK, Zhao CY, Shi XL, Li
CS, Jiang JF, Wang H and Ye B: Diagnosis of thyroid space-occupying
lesions using real-time contrast-enhanced ultrasonography with
sulphur hexafluoride microbubbles. Chinese Journal of
Otorhinolaryngology Head and Neck Surgery. 44:277–281. 2009.(In
Chinese). PubMed/NCBI
|
|
35
|
Frey H: Realtime elastography. A new
ultrasound procedure for the reconstruction of tissue elasticity.
Radiologe. 43:850–855. 2003.(In German). View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Jiang J, Shang X, Zhang H, Ma W, Xu Y,
Zhou Q, Gao Y, Yu S and Qi Y: Correlation between maximum intensity
and microvessel density for differentiation of malignant from
benign thyroid nodules on contrast-enhanced sonography. J
Ultrasound Med. 33:1257–1263. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Bojunga J, Herrmann E, Meyer G, Weber S,
Zeuzem S and Friedrich-Rust M: Real-time elastography for the
differentiation of benign and malignant thyroid nodules: A
meta-analysis. Thyroid. 20:1145–1150. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Argalia G, De Bernardis S, Mariani D,
Abbattista T, Taccaliti A, Ricciardelli L, Faragona S, Gusella PM
and Giuseppetti GM: Ultrasonographic contrast agent: Evaluation of
time-intensity curves in the characterisation of solitary thyroid
nodules. Radiol Med. 103:407–413. 2002.(In English, Italian).
PubMed/NCBI
|
|
39
|
Dietrich CF, Saftoiu A and Jenssen C: Real
time elastography endoscopic ultrasound (RTE-EUS), a comprehensive
review. Eur J Radiol. 83:405–414. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Lorentzen T and Skjoldbye B: Diagnosis and
biopsy of liver metastases using ultrasound contrast agent. Ugeskr
Laeger. 171:9072009.(In Danish). PubMed/NCBI
|
|
41
|
Aoyagi S, Izumi K, Hata H, Kawasaki H and
Shimizu H: Usefulness of real-time tissue elastography for
detecting lymph-node metastases in squamous cell carcinoma. Clin
Exp Dermatol. 34:e744–e747. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Sugitani I, Kasai N, Fujimoto Y and
Yanagisawa A: A novel classification system for patients with PTC:
Addition of the new variables of large (3 cm or greater) nodal
metastases and reclassification during the follow-up period.
Surgery. 135:139–148. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Sugitani I, Fujimoto Y, Yamada K and
Yamamoto N: Prospective outcomes of selective lymph node dissection
for papillary thyroid carcinoma based on preoperative
ultrasonography. World J Surg. 32:2494–2502. 2008. View Article : Google Scholar : PubMed/NCBI
|