Introduction
Epidemiological studies have consistently
demonstrated that there is a high incidence rate of stroke and
mortality (11,663/100,000 per year) in China (1). Poor outcomes after stroke have been
reported in numerous countries worldwide (2–5). The
risk factors of death after stroke include age, stroke severity,
history, previous stroke and atrial fibrillation. Previous studies
have focused on the association between death after stroke and the
decline of cognitive function or dementia caused by stroke
(6–8). The results suggested that dementia is a
potentially important factor influencing survival after stroke
(7,9–12).
With a population of 1.3 billion in China, the
prevalence of patients with ischemic stroke is extremely high
(1). Owing to racial differences and
economic lifestyle, the mortality rate and its risk factors in
Chinese patients after ischemic stroke may differ from that in
western countries (13). At present,
few studies have focused on the relationship between dementia and
survival after stroke in China.
In the present study, we studied a large cohort of
patients in Chongqing, China with acute ischemic stroke, to
investigate the association of mortality with dementia
post-stroke.
Subjects and methods
Subjects
From January 2005 to July 2008, patients with
ischemic stroke who were admitted to Daping Hospital (Chongqing,
China) were registered. Eligibility requirements included: i) acute
onset of ischemic stroke within 48 h; and ii) aged ≥55 years. The
diagnosis of ischemic stroke was confirmed when there were focal
signs of cerebral dysfunction of acute onset lasting for >24 h,
brain CT scan or MRI.
In total, 727 patients were admitted during the
study period, and 95 declined to participate. Thus, 619 patients
were enrolled into the present study.
Clinical assessment
During admission, the patients underwent structured
demographic data, medical history, neurological and head imaging
examinations. The data collected were: age, gender, educational
level (<6 or ≥6 years), cigarette smoking (current, past and
non-smoking) and alcohol intake (daily, weekly, monthly and
non-alcohol intake), heart diseases (myocardial infarction, atrial
fibrillation, and heart failure, diagnosed and treated previously
or during admission), hypertension (previously diagnosed and
treated or systolic pressure >160 mmHg and/or diastolic pressure
>90 mmHg persistently observed during admission after the acute
phase), diabetes mellitus (previously diagnosed and treated or
fasting glucose >7 mmol/l in two blood samples after the acute
phase), stroke severity (NIH stroke scale), neurological sign, and
stroke features (location, type of lesion, and stroke
mechanism).
Neuropsychological evaluation
During admission, the dementia before index stroke
was assessed by inquiring close relatives of the patients using a
Chinese version of the Informant Questionnaire on Cognitive Decline
in the Elderly (IQCODE), previously validated in the Chinese
population (14). Functional status
prior to stroke was assessed with the activity of daily living
(ADL) (15).
At three months after the index stroke, the subjects
were administered with a battery of neuropsychological tests
developed for use in epidemiologic studies of dementia (16,17).
This neuropsychological battery of tests included: the Chinese
Mini-Mental State Examination (CMMS) (18), ADL (19,20),
instrumental ADL (15), Pfeiffer's
Outpatient Disability Questionnaire (POD) (21), the Fuld Object-Memory Evaluation
(FOM) (22), rapid verbal retrieval
(RVR) (23), revised Wechsler Adult
Intelligence Scale (DS and BD subtests) (24), and the Hamilton Rating Scale for
Depression. The normative data for these tests were previously
established in a control group of healthy elderly volunteers living
in the same urban area and with the same age, gender distribution,
and cultural background (16). The
score ≤1 SD of normative value was judged as unnormative.
The diagnosis of dementia was performed by a group
of senior neurologists and psychiatrists based on criteria modified
from the Diagnostic and Statistical Manual of Mental Disorders, 4th
edition (DSM-IV) (25).
Statistical analyses
Participants who were lost or declined for follow-up
were considered as censored data. As the onset time of dementia was
not exactly observed, we defined the time to an event as the time
of a diagnosis of dementia.
The univariate analyses were taken to compare the
data of the death and survival groups, including demographic data,
smoking, drinking, comorbidities, stroke severity and
characteristics. Categorical variables were compared using the
Pearson Chi-square test, and quantitative variables were compared
using an independent samples t-test or the Mann-Whitney U test in
appreciation.
The cumulative proportion of patients surviving in
the groups with and without dementia was determined using the
Kaplan-Meier survival analyses (26). In the multivariate analysis, we
studied the association between dementia and risk of death using
the Cox proportional hazards regression analysis with a backward
procedure and with p>0.05 as the criterion for exclusion to
estimate hazard ratios (HRs), with 95% confidence intervals (CIs).
These analyses were performed using SPSS for Windows, version 10.0
(SPSS Inc., Chicago, IL, USA).
Results
Follow-up, prevalence and incidence of
dementia and mortality
Of the 619 patients, 39 (6.3%) were diagnosed with
dementia during admission and 107 (17.3%) three months after index
stroke. Thus, 146 (23.6%) patients were diagnosed with
dementia.
After a median follow-up of 10.3±5.7 months, 112
patients (16.5%) succumbed during the study. A total of 29 patients
(4.7%) were lost during follow-up. The median follow-up time was
9.1±5.3 months and four of 29 patients were diagnosed as having
dementia.
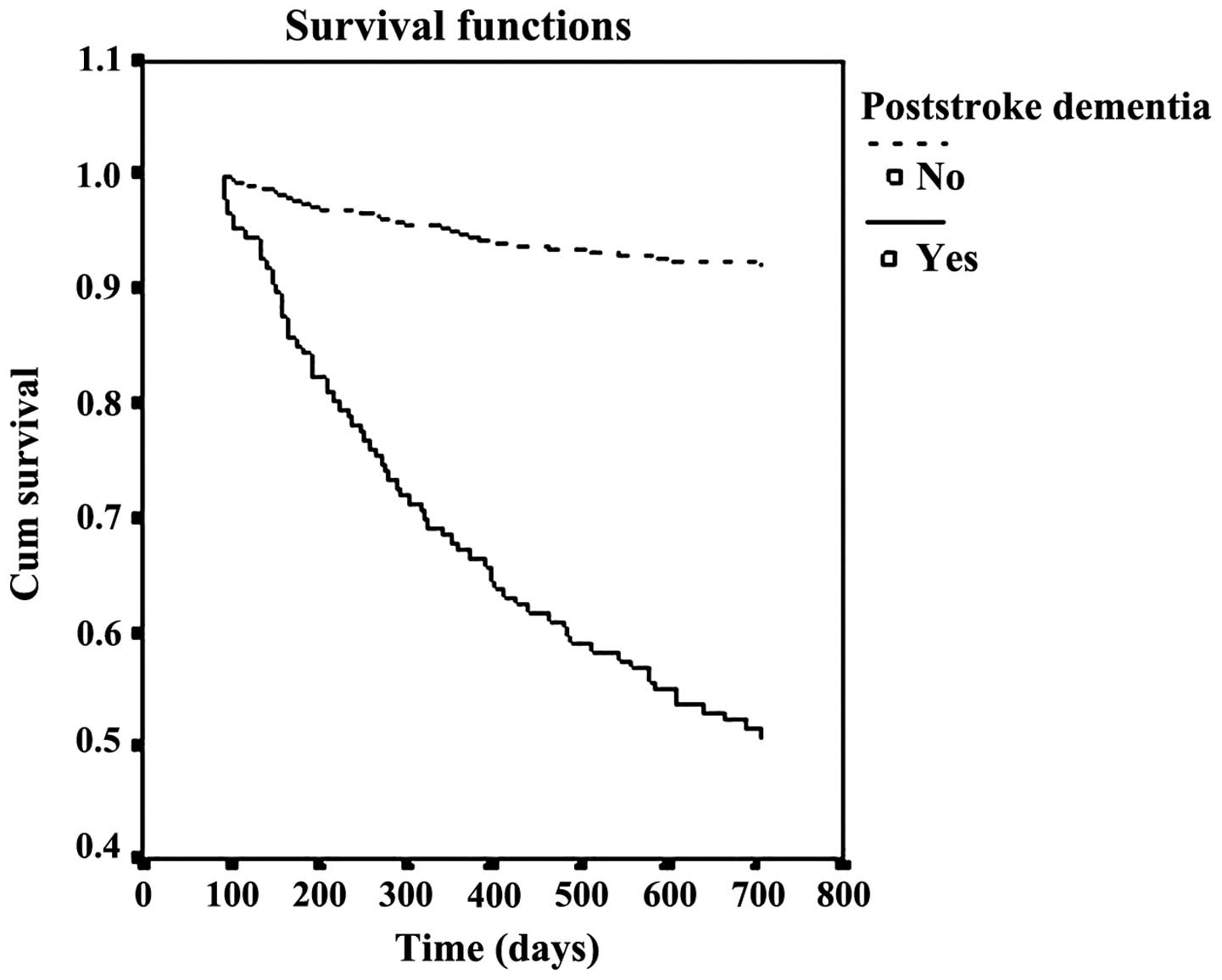
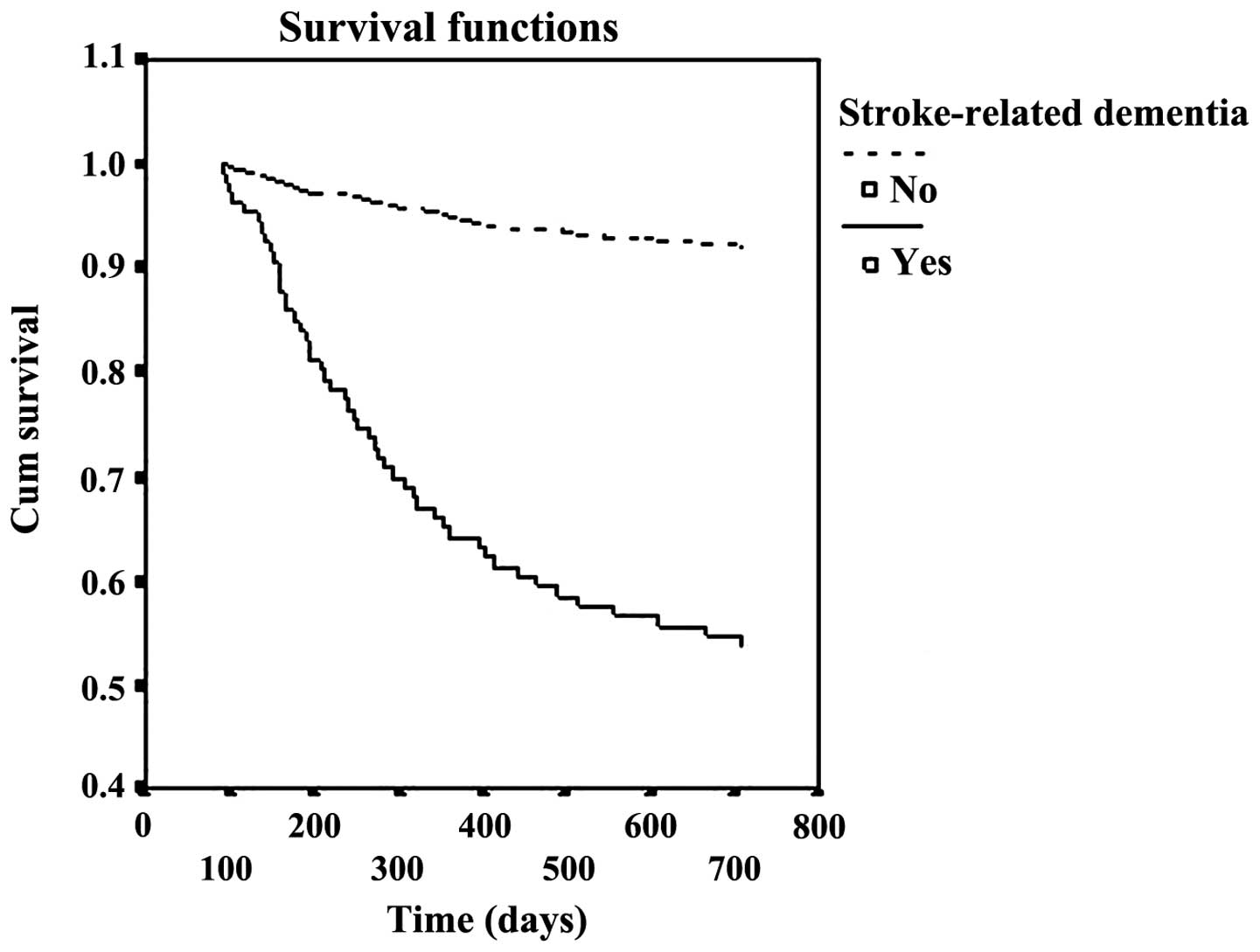
After a median follow-up of 21.2±5.6 months, the
cumulative proportion of case survival was 49.3 and 92.5% in
patients with and without dementia, respectively. The survival
curves were significantly different (p<0.001) between the two
groups (Figs. 1 and 2).
Demographic characteristics, smoking,
drinking, comorbidities, dementia and stroke features of patients
according to death
Table I indicates the
demographic characteristics, smoking and drinking status, and
comorbidities of deceased and surviving patients. Deceased patients
were older (74.6±11.2 vs. 65.2±9.3, p<0.001), less frequent with
diabetes mellitus [odds ratio (OR), 0.93; 95% CI, 0.63–1.40], and
more frequent in female (OR, 1.04; 95% CI, 0.72–1.48), hypertension
(OR, 1.13; 95% CI, 0.75–1.70), myocardial infarction (OR, 1.26; 95%
CI, 0.67–2.39), heart failure (OR, 1.22; 95% CI, 0.61–2.43), atrial
fibrillation (OR, 2.24; 95% CI, 1.41–3.53), prior stroke (OR, 2.28,
95% CI, 1.40–3.70), current smoking (OR, 1.16; 95% CI, 0.76–1.79),
daily alcohol intake (OR, 1.36; 95% CI, 0.83–2.21), and dementia
(OR, 12.01; 95% CI, 7.35–19.64). Only differences in age
(p<0.001), atrial fibrillation (p<0.001), prior stroke
(p=0.001) and dementia (p<0.001) reached statistical
significance.
 | Table I.Demographic characteristics, smoking,
drinking and comorbidities according to death after stroke. |
Table I.
Demographic characteristics, smoking,
drinking and comorbidities according to death after stroke.
| Variable | Death (n=112) | Survival (n=507) | P-value or OR (95%
CI)a |
|---|
| Age (years), mean ±
SD | 74.6±11.2 | 65.2±9.3 | p<0.001 |
| Lower education (≤6
y), n (%) | 38 (33.9) | 187 (36.9) | 0.881
(0.543–1.429) |
| Female, n (%) | 57 (50.9) | 249 (49.1) | 1.04 (0.72–1.48) |
| Hypertension, n
(%) | 63 (56.3) | 271 (53.5) | 1.13 (0.75–1.70) |
| Diabetes mellitus, n
(%) | 34 (30.3) | 158 (31.1) | 0.93 (0.63–1.40) |
| Myocardial
infarction | 12 (10.7) | 43 (8.5) | 1.26
(0.67–2.39) |
| Heart failure, n
(%) | 15 (13.4) | 59 (11.6) | 1.22
(0.61–2.43) |
| Atrial
fibrillation, n (%) | 39 (34.8) | 97 (19.1) | 2.24
(1.41–3.53) |
| Prior stroke, n
(%) | 28 (25.0) | 65 (12.8) | 2.28
(1.40–3.70) |
| Current smoking, n
(%) | 47 (41.9) | 192 (37.1) | 1.16
(0.76–1.79) |
| Daily alcohol
intake, n (%) | 39 (34.8) | 149 (28.8) | 1.36
(0.83–2.21) |
| Post-stroke
dementia, n (%) | 74 (66.1) | 72 (14.2) | 12.01
(7.35–19.64) |
Table II shows the
stroke features according to death. Stroke features associated with
death included multiple stroke lesions (OR, 2.15; 95% CI,
1.49–3.11), and embolism (OR, 4.21; 95% CI, 2.36–7.53), and NIH
stroke scale score (p<0.001).
| Table II.Stroke features according to death
after stroke. |
Table II.
Stroke features according to death
after stroke.
| Variable | Death) (n=112 | Survival
(n=507) | P-value or OR (95%
CI) |
|---|
| Location, n
(%) |
|
|
|
| Left
hemisphere | 47 (41.9) | 206 (40.1) | 1.48
(0.95–2.28)a |
| Right
hemisphere | 49 (43.8) | 145 (28.6) |
|
|
Vertebrobasilar | 16 (14.3) | 156 (30.8) |
|
| Type of lesion, n
(%) |
|
| 2.15
(1.49–3.11)b |
|
Single | 66 (58.9) | 386 (76.9) |
|
|
Multiple | 46 (41.1) | 116 (23.1) |
|
| Stroke mechanism, n
(%) |
|
| 4.21
(2.36–7.53)c |
|
Thrombotic | 86 (76.8) | 461 (90.9) |
|
|
Embolic | 23 (20.5) | 30 (5.9) |
|
|
Others | 3 (2.7) | 16 (3.2) |
|
| NIH stroke scale
(SD) | 9.34 (6.7) | 6.81 (4.7) | p<0.001 |
Multivariate analysis of death after
ischemic stroke in patients with dementia
Independent predictors for death in patients with
ischemic stroke were age (HR, 1.06; 95% CI, 1.02–1.10), atrial
fibrillation (HR, 1.78; 95% CI, 1.32–2.40), previous stroke (HR,
2.14; 95% CI, 1.49–3.08), NIH stroke scale score (HR, 1.95; 95% CI,
1.04–1.27), and dementia (HR, 7.21; 95% CI, 3.85–13.49) in the
Cox's regression model (Table
III).
| Table III.Cox proportional hazards regression
analysis according to dementia. |
Table III.
Cox proportional hazards regression
analysis according to dementia.
| Variable | SE OR (95% CI) |
|---|
| Age (years) | 1.06
(1.02–1.10) |
| Atrial
fibrillation | 1.78
(1.32–2.40) |
| Previous
stroke | 2.14
(1.49–3.08) |
| NIH stroke
scale | 1.15
(1.04–1.27) |
| Dementia | 7.21
(3.85–13.49) |
Discussion
Chongqing, the largest city in southwest China, has
an urban population of five million individuals, of whom 93.6% are
Han, and have similar lifestyles (27). Furthermore, the social and economic
characteristics of the city is a miniature version of China today,
and can be a good sample to study disease features. In the present
study, the Kaplan-Meier analysis revealed that the cumulative
proportion of survival cases was 49.3 and 92.5% in patients with
and without dementia, after median follow-up of 21.2±5.6 months.
The mortality rate of patients with dementia was >4-fold that of
patients without dementia.
The results of the present study with regard to the
cumulative proportion of survival of dementia after stroke str
consistent with other studies in western countries. Previous
findings on vascular dementia suggested that patients with vascular
dementia had a higher risk for mortality compared to the control
subjects (28,29). A study in Finland showed dementia is
a significant predictor of poor long-term survival and death from
brain-associated causes in patients with acute stroke (30). Barba et al (31) also found that dementia increased the
risk for mortality in stroke patients. A study demonstrated that
the mortality rate was 15.90 deaths/100 person-years in dementia
patients with ischemic stroke and 5.37 deaths/100 person-years in
non-dementia patients with ischemic stroke during a period of up to
10 years of follow-up (32). Another
study suggested that the cumulative proportion surviving after a
median follow-up of 58.6 months was 38.9±0.08% for those with
dementia and 74.5±0.04% for those without dementia (12). There are discrepancies between our
findings and those of the abovementioned studies. The reason may be
because the duration gap and outpatient treatment is different.
Consistent with other studies (9,23–38),
age, atrial fibrillation, NIH stroke scale, and prior stroke were
found to be associated with death after stroke in the present
study. We also found that dementia was associated with long-term
survival of stroke patients. This association was independent of
other predictors of post-stroke death such as older age, higher
stroke severity, presence of atrial fibrillation and previous
stroke. In a prospective study on the association between mortality
and dementia after stroke, dementia was demonstrated to adversely
influence long-term survival after stroke, even after adjusting for
other commonly accepted predictors of stroke mortality (12). In studies of cognitive decline and
death after first-ever stroke, dementia was also proven to be an
important predictor (9,39). Dementia was considered to have
prognostic implications in stroke patients, i.e., stroke prior to
the index stroke and dementia developed after stroke may determine
a significant reduction in survival and were among the most
important risk factors of mortality in these patients (31). Dementia was identified to be a
significant independent risk factor for reduced survival after
ischemic stroke, after adjusting for other recognized predictors of
mortality in a 10-year follow-up study (32).
Four explanations may be proposed for the mechanism
of the elevated risk of death among patients with dementia after
ischemic stroke (6,10,12,32,40,41).
First, patients with dementia after stroke have an increased burden
of cerebrovascular disease, which later may in return increase
their risk of death. Second, patients with dementia tend to be
treated less aggressively for stroke prophylaxis as well as other
medical conditions for their weakened social abilities. Third,
patients with dementia may be less compliant with prescribed
treatment regiments. Fourth, dementia, either degenerative or
vascular, tends to appear in an already weak individual and
constitutes by itself a general deleterious condition.
In conclusion, mortality is increased in Chinese
stroke patients with dementia. Dementia is a risk factor for death
after stroke, independent of other factors including age, stroke
severity, atrial fibrillation and previous stroke. Prevention and
management of the dementia after stroke is critical to reduce the
mortality after stroke.
Acknowledgements
The present study was funded by contract no.
2001-54-23 from the Science and Technology Committee of Chongqing,
China.
References
|
1
|
Liu M, Wu B, Wang WZ, Lee LM, Zhang SH and
Kong LZ: Stroke in China: Epidemiology, prevention, and management
strategies. Lancet Neurol. 6:456–464. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bonita R, Ford MA and Stewart AW:
Predicting survival after stroke: a three-year follow-up. Stroke.
19:669–673. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hollander M, Koudstaal PJ, Bots ML,
Grobbee DE, Hofman A and Breteler MM: Incidence, risk, and case
fatality of first ever stroke in the elderly population. The
Rotterdam Study. J Neurol Neurosurg Psychiatry. 74:317–321. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Barker-Collo SL, Feigin VL, Lawes CM,
Parag V, Senior H and Rodgers A: Reducing attention deficits after
stroke using attention process training: a randomized controlled
trial. Stroke. 40:3293–3298. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Arac A, Blanchard V, Lee M and Steinberg
GK: Assessment of outcome following decompressive craniectomy for
malignant middle cerebral artery infarction in patients older than
60 years of age. Neurosurg Focus. 26:E32009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Barba R, Martínez-Espinosa S,
Rodríguez-García E, Pondal M, Vivancos J and Del Ser T: Poststroke
dementia : clinical features and risk factors. Stroke.
31:1494–1501. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Melkas S, Oksala NK, Jokinen H,
Pohjasvaara T, Vataja R, Oksala A, Kaste M, Karhunen PJ and
Erkinjuntti T: Poststroke dementia predicts poor survival in
long-term follow-up: influence of prestroke cognitive decline and
previous stroke. J Neurol Neurosurg Psychiatry. 80:865–870. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Shipley BA, Der G, Taylor MD and Deary IJ:
Association between mortality and cognitive change over 7 years in
a large representative sample of UK residents. Psychosom Med.
69:640–650. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Appelros P, Nydevik I and Viitanen M: Poor
outcome after first-ever stroke: predictors for death, dependency,
and recurrent stroke within the first year. Stroke. 34:122–126.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Moroney JT, Bagiella E, Tatemichi TK, Paik
MC, Stern Y and Desmond DW: Dementia after stroke increases the
risk of long-term stroke recurrence. Neurology. 48:1317–1325. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Rockwood K, Wentzel C, Hachinski V, Hogan
DB, MacKnight C and McDowell I: Vascular Cognitive Impairment
Investigators of the Canadian Study of Health and Aging: Prevalence
and outcomes of vascular cognitive impairment. Neurology.
54:447–451. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tatemichi TK, Paik M, Bagiella E, Desmond
DW, Pirro M and Hanzawa LK: Dementia after stroke is a predictor of
long-term survival. Stroke. 25:1915–1919. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Chen X, Zhou L, Zhang Y and Yi D, Liu L,
Rao W, Wu Y, Ma D, Liu X, Zhou XH, Lin H, Cheng D and Yi D: Risk
factors of stroke in Western and Asian countries: A systematic
review and meta-analysis of prospective cohort studies. BMC Public
Health. 14:7762014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Fuh JL, Teng EL, Lin KN, Larson EB, Wang
SJ, Liu CY, Chou P, Kuo BI and Liu HC: The Informant Questionnaire
on Cognitive Decline in the Elderly (IQCODE) as a screening tool
for dementia for a predominantly illiterate Chinese population.
Neurology. 45:92–96. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chen P, Yu ES, Zhang M, Liu WT, Hill R and
Katzman R: ADL dependence and medical conditions in Chinese older
persons: a population-based survey in Shanghai, China. J Am Geriatr
Soc. 43:378–383. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zhou H, Deng J, Li J, Wang Y, Zhang M and
He H: Study of the relationship between cigarette smoking, alcohol
drinking and cognitive impairment among elderly people in China.
Age Ageing. 32:205–210. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zhou DH, Wang JY, Li J, Deng J, Gao C and
Chen M: Study on frequency and predictors of dementia after
ischemic stroke: the Chongqing stroke study. J Neurol. 251:421–427.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Katzman R, Zhang MY, Ouang-Ya-Qu Wang ZY,
Liu WT, Yu E, Wong SC, Salmon DP and Grant I: A Chinese version of
the Mini-Mental State Examination; impact of illiteracy in a
Shanghai dementia survey. J Clin Epidemiol. 41:971–978. 1988.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Katz S, Downs TD, Cash HR and Grotz RC:
Progress in development of the index of ADL. Gerontologist.
10:20–30. 1970. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lawton MP and Brody EM: Assessment of
older people: self-maintaining and instrumental activities of daily
living. Gerontologist. 9:179–186. 1969. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Pfeiffer E: A short portable mental status
questionnaire for the assessment of organic brain deficit in
elderly patients. J Am Geriatr Soc. 23:433–441. 1975. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Fuld PA: The Fuld Object-Memory
Evaluation. Stoelting Instrument Co. Chicago, IL: 1981.
|
|
23
|
Zhang M: Prevalence study on dementia and
Alzheimer disease. Zhonghua Yi Xue Za Zhi. 70424–428. (30)1990.(In
Chinese). PubMed/NCBI
|
|
24
|
Zhou B, Hong Z and Huang M: Prevalence of
dementia in Shanghai urban and rural area. Zhonghua Liu Xing Bing
Xue Za Zhi. 22:368–371. 2001.(In Chinese). PubMed/NCBI
|
|
25
|
American Psychiatric Association:
Diagnostic and Statistical Manual of Mental Disorders (4th).
American Psychiatric Association. Washington, DC: 1994.
|
|
26
|
Dinse GE and Lagakos SW: Nonparametric
estimation of lifetime and disease onset distributions from
incomplete observations. Biometrics. 38:921–932. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Gao BW, Wang W and Zou DC: Effects of
change in urban-rural statistical definition in two censuses on
urbanization process of Chongqing. Popul Res. 26:10–14. 2002.(In
Chinese).
|
|
28
|
Koedam EL, Pijnenburg YA, Deeg DJ, Baak
MM, van der Vlies AE, Scheltens P and van der Flier WM: Early-onset
dementia is associated with higher mortality. Dement Geriatr Cogn
Disord. 26:147–152. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Knopman DS, Rocca WA, Cha RH, Edland SD
and Kokmen E: Survival study of vascular dementia in Rochester, MN.
Arch Neurol. 60:85–90. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Melkas S, Laurila JV, Vataja R, Oksala N,
Jokinen H, Pohjasvaara T, Leppavuori A, Kaste M, Karhunen PJ and
Erkinjuntti T: Post-stroke delirium in relation to dementia and
long-term mortality. Int J Geriatr Psychiatry. 27:401–408.
2012.PubMed/NCBI
|
|
31
|
Barba R, Morin MD, Cemillán C, Delgado C,
Domingo J and Del Ser T: Previous and incident dementia as risk
factors for mortality in stroke patients. Stroke. 33:1993–1998.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Desmond DW, Moroney JT, Sano M and Stern
Y: Mortality in patients with dementia after ischemic stroke.
Neurology. 59:537–543. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kimura K, Minematsu K and Yamaguchi T:
Japan Multicenter Stroke Investigators' Collaboration (J-MUSIC):
Atrial fibrillation as a predictive factor for severe stroke and
early death in 15,831 patients with acute ischaemic stroke. J
Neurol Neurosurg Psychiatry. 76:679–683. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Vemmos KN, Bots ML, Tsibouris PK, Zis VP,
Takis CE, Grobbee DE and Stamatelopoulos S: Prognosis of stroke in
the south of Greece: 1 year mortality, functional outcome and its
determinants: the Arcadia Stroke Registry. J Neurol Neurosurg
Psychiatry. 69:595–600. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Vohra EA, Ahmed WU and Ali M: Aetiology
and prognostic factors of patients admitted for stroke. J Pak Med
Assoc. 50:234–236. 2000.PubMed/NCBI
|
|
36
|
Rabkin SW, Mathewson FA and Tate RB: The
relation of blood pressure to stroke prognosis. Ann Intern Med.
89:15–20. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Woo J, Kay R, Yuen YK and Nicholls MG:
Factors influencing long-term survival and disability among
three-month stroke survivors. Neuroepidemiology. 11:143–150. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Baptista MV, van Melle G and Bogousslavsky
J: Prediction of in-hospital mortality after first-ever stroke: the
Lausanne Stroke Registry. J Neurol Sci. 166:107–114. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Srikanth VK, Quinn SJ, Donnan GA, Saling
MM and Thrift AG: Long-term cognitive transitions, rates of
cognitive change, and predictors of incident dementia in a
population-based first-ever stroke cohort. Stroke. 37:2479–2483.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Hoffmann M, Schmitt F and Bromley E:
Comprehensive cognitive neurological assessment in stroke. Acta
Neurol Scand. 119:162–171. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Ukraintseva S, Sloan F, Arbeev K and
Yashin A: Increasing rates of dementia at time of declining
mortality from stroke. Stroke. 37:1155–1159. 2006. View Article : Google Scholar : PubMed/NCBI
|