Introduction
Gastrointestinal stromal tumor (GIST) is the most
common mesenchymal neoplasm of the digestive tract (1). In the pre-imatinib era, surgical
resection was the only effective treatment for GISTs. The 5-year
survival rate for patients with GISTs ranges from 28–80%; however,
tumor progression occurs in ~50% of patients, even following
complete resection (2). Imatinib
mesylate, a tyrosine kinase inhibitor, has been the standard
first-line pharmacological therapy for unresectable and/or
metastatic GIST since it was approved, and significantly improves
the overall survival rate (3). The
present study reports the case of a patient with GIST in the
Affiliated Hospital of Luzhou Medical College (Luzhou, China), and
presents a review of the pertinent literature. The purpose was to
assess the efficacy and safety of imatinib mesylate in the
treatment of unresectable GIST and to discuss the optimal
therapeutic plan for unresectable GIST.
Case report
A 57-year-old woman was admitted to the Department
of Gastrointestinal Surgery of the Affiliated Hospital of Luzhou
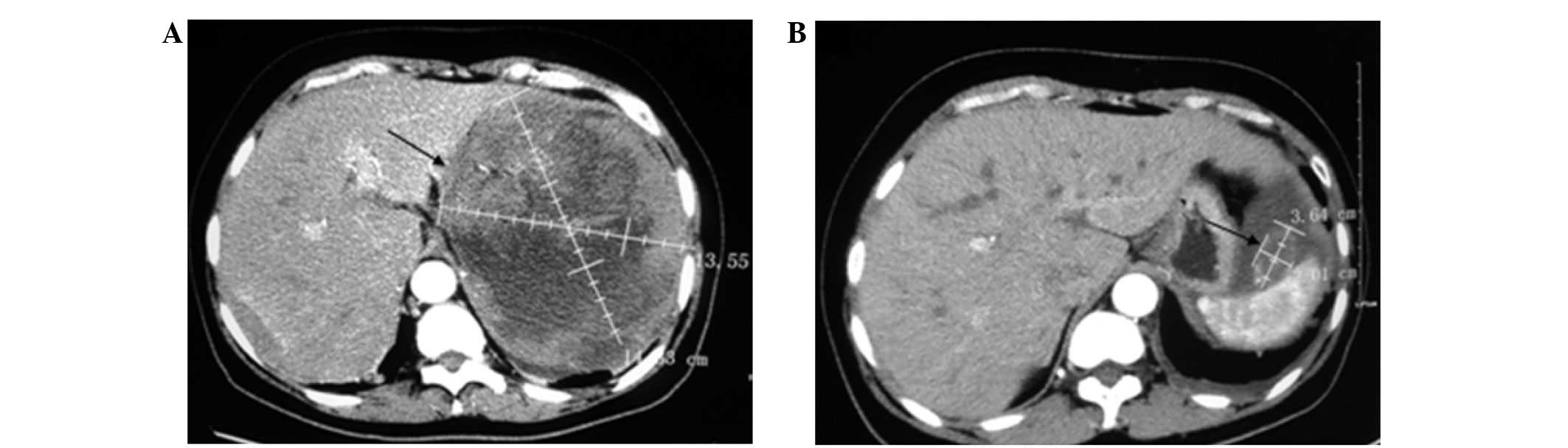
Medical College on March 25, 2013, complaining of pain in the left
upper abdomen for 10 days and aggravation for 2 days. A computed
tomography (CT)-scan showed a large mass in the left upper abdomen
(Fig. 1A), and upper
gastrointestinal tract CT enterography revealed a mass in the left
upper abdominal cavity. In addition, the lower part of the
esophagus and the fundus of the stomach were shifted, and the
stomach appeared irregular. A hard, irregular-shaped tumor outside
of the cavity, ~14×15×15 cm in size, which was closely connected
with the diaphragmatic muscle, pancreas, spleen and relevant blood
vessels, was identified during an exploratory laparotomy. A tumor
biopsy (~1.5 cm) was performed without resection of the tumor. A
pathological analysis performed by two experienced pathologists
showed GIST and a mitotic index of >5 mitoses per 50 high-power
fields. Immunohistochemical analyses were positive for CD117
(rabbit anti-CD117 polyclonal antibody; cat. no. A4502; 1:200
dilution; Dako, Glostrup, Denmark), CD34 (mouse anti-CD34
monoclonal antibody; cat. no. M7165; 1:400 dilution; Dako) and Ki67
(mouse anti-Ki67 monoclonal antibody; cat. no. M7204; 1:100
dilution; Dako), and negative for Dog1 (rabbit anti-Dog1 monoclonal
antibody; cat. no. RM-9132-R7; 1:200 dilution; Thermo Fisher
Scientific, Inc., Waltham, MA, USA), S-100 (rabbit anti-S-100
polyclonal antibody; cat. no. Z0311; 1:300 dilution; Dako), smooth
muscle actin (mouse anti-SMA monoclonal antibody; cat. no. M0851;
1:150 dilution; Dako) and P53 (mouse anti-P53 monoclonal antibody;
cat. no. M7001; 1:150 dilution; Dako). The diagnosis of a
high-grade non-metastatic GIST was thus confirmed. Treatment of the
patient was initiated with oral administration of 400 mg imatinib
(Novartis Pharma Stein AG, Stein, Switzerland) daily, without tumor
gene detection, and the patient was reviewed by abdominal CT scans
every three months. During the drug therapy period, the patient
experienced mild adverse effects, including nausea, diarrhea, edema
and leucopenia; however, these were normalized following
symptomatic treatment. In March 7, 2014, a CT scan (Fig. 1B) showed that the mass was reduced in
size. However, the patient refused to undergo surgery and persisted
with agent therapy. At the 16-month follow-up, the mass had
decreased markedly, without tumor progression and metastasis. The
patient had achieved a partial response and had tolerated the
treatment well. This study was conducted in accordance with the
Declaration of Helsinki and with approval from the Ethics Committee
of Luzhou Medical College. Written informed consent was obtained
from the patient prior to the study.
Discussion
GISTs are the most common type of mesenchymal
neoplasm of the digestive tract (1).
GISTs most commonly arise in the stomach (60%), although they may
also occur in the small intestine (25%), rectum (5%) and other
sites along the GI tract, including the esophagus, colon, appendix
and gallbladder (4). These so-called
extra-intestinal GISTs may occupy the mesentery or omentum
(5). GISTs originate from
interstitial cells of Cajal and related stem cells, which express
c-Kit, CD117 and CD34. The majority of GISTs have oncogenic
mutations in either receptor tyrosine kinase genes (KIT) or
platelet-derived growth factor receptor-α (PDGFRα), resulting in
the activation of intracellular signaling pathways and the
deregulation of cellular proliferation and apoptosis inhibition
(6). The mutation frequencies in
exons 11 and 9 of the KIT gene are 67 and 8%, respectively. Exons
13 and 17 rarely exhibit these mutations, while exons 18 and 12
show lower mutation rates for PDGFRα of 5 and 1%, respectively
(5). The clinical manifestations of
GISTs are highly variable and depend on tumour location, size and
growth pattern (7). The most common
presenting symptoms are associated with gastrointestinal bleeding,
including melena, hematemesis or symptomatic anaemia, while other
symptoms may include abdominal fullness, early satiety and a
palpable mass or pain (7). Among
patients with GIST, 15–50% present with overt metastasis, and the
most common sites of metastases are the peritoneum and liver
(8). Metastasis of GIST to the
lungs, bones and brain is rare (9).
Diagnosis of GIST can be made using a combination of abdominal CT
scans, endoscopic ultrasonography, pathological immunohistochemical
analyses and/or genetic detection.
Imatinib mesylate is a potent and select inhibitor
of the protein tyrosine kinase Bcr-Abl, PDGFRα and KIT (10). Imatinib exerts its therapeutic effect
in chronic myeloid leukemia (CML) via competitive inhibition at the
adenosine triphosphate binding site of Bcr-Abl tyrosine of proteins
involved in Bcr-Abl signal transduction (11). In GIST, imatinib interrupts
KIT-mediated signal transduction by a mechanism of action similar
to its inhibition of Bcr-Abl tyrosine kinase in CML patients
(11). Prior to the advent of
imatinib therapy, the median survival period was 19 months in
patients with metastatic GIST and 12 months in those with
unresectable GIST (12). Imatinib
has demonstrated clinical benefit for both patient groups;
improving progression-free survival (PFS) and overall survival (OS)
rates in numerous clinical trials (13–17).
Accordingly, imatinib is currently approved as the first-line
option for the treatment of unresectable GISTs.
The clinical studies B2222 and S0033 were reviewed
in the present study, with particular emphasis on the recently
reported results of the long-term clinical outcome of imatinib for
unresectable GIST. The results from the two studies (Tables I and II) (13–17)
indicate that imatinib achieves long-term tumor control and remains
well tolerated over long-term administration.
 | Table I.Efficacy reported by imatinib trials
for unresectable gastrointestinal stromal tumor. |
Table I.
Efficacy reported by imatinib trials
for unresectable gastrointestinal stromal tumor.
| Study parameter | Phase II US-Finland
study B2222 (13–15) | Phase III North
American intergroup study S0033 (16,17) |
|---|
| Patients |
|
|
|
Number | 147 | 694 |
|
Grouping | Randomized, 400 or
600 mg/day | Randomized, 400
mg/day (arm A) or 800 mg/day (arm B) |
| Overall response
rate |
|
|
| Follow-up
period | 63 months | 4.5 years |
| Median
response rate (%) | 68.1 | 45 |
|
Arms/treatment | Similar between
arms | Similar between
arms |
| Median PFS |
|
|
| Follow-up
period | 63-month median
follow-up: | Median follow-up of
4.5 years: |
|
| 24 months | 18 months for arm
A |
|
| 9.4-year median
follow-up: | 20 months for arm
B |
|
| Estimated time to
progression rate for all patients was 14% |
|
| Median OS |
|
|
|
| 63-month median
follow-up: | Median follow-up of
4.5 years: |
|
| 57 months | 55 months for arm
A |
|
| 9.4-year median
follow-up: Estimated | 51 months for arm
B |
|
| OS rate for all
patients was 35% | Median follow-up of
8.8 years: |
|
| 38% for patients with
CR/PR | 136 patients
alive |
|
| 49% for patients with
SD | Estimated OS: |
|
| 0% for patients with
PD | 8 years: 31% |
|
|
| 9 years: 26% |
|
|
| 10 years: 21% |
| Table II.Safety results of imatinib trials for
unresectable gastrointestinal stromal tumor. |
Table II.
Safety results of imatinib trials for
unresectable gastrointestinal stromal tumor.
| Study parameter | Phase II US-Finland
study B2222 (13–15) | Phase III North
Americanintergroup study S0033 (16,17) |
|---|
| Common adverse
events | Edema, nausea,
fatigue, diarrhea, myalgia, dermatitis, headache, | Edema, nausea,
fatigue, rash, pain abdominal pain |
| Mild or moderate
adverse events (grade 1 or 2)* | The majority of the
common adverse events were mild or moderate | The majority of the
common adverse events were mild or moderate, particularly for arm A
patients |
| Serious adverse
events (grades 3–5)* | Grade 3 or 4 events
occurred in 21.1% of patients. | Grade 3–5 events
occurred in 43% of arm A patients and 63% of arm B. |
|
|
| Two lose-dose
patients (1%) and nine high-dose patients (3%) underwent possible
treatment-associated mortality. |
The studies are open-label, multicenter trial,
double-blinded and random trials, with a maximum follow-up time of
10 years for patients with unresectable GIST. The results of the
S0033 are consistent with the long-term efficacy and safety of
imatinib that was observed in B2222. During the median follow-up of
5 years, the results of both studies showed a similar median PFS of
~20 months and median OS of ~56 months. Long-term data from the two
clinical trials also reveal that certain patients remain alive
after long-term imatinib treatment, including 35% at 9 years in the
B2222 study and 31% at 8 years in the S0033 study (Table I). Imatinib has been suggested to be
suitable for long-term administration due to its favorable safety
profile. Indeed, no major toxicities were noted in patients who
were treated with imatinib for ~10 years in the B2222 and S0033
studies (14,17), and the majority of
imatinib-associated adverse events are minor (Table II). Collectively, the results from
the phase II B2222 and phase III S0033 trials suggest that imatinib
achieves long-term tumor control in a significant proportion of
patients with unresectable GIST for periods approaching 10
years.
There are numerous factors that affect the response
of GIST to imatinib therapy, including kinase genotype mutation,
hemoglobin, albumin level, primary tumor site and metastasis
location; however, KIT mutation is one of the most important
factors (18). Corless and Heinrich
(18) reported correlations between
tumor genotype and objective response (complete and partial) in a
review of four trials. The objective response rates for patients
with mutations in exons 11 or 9 of KIT, or with wild-type GISTs,
are 72, 38 and 28%, respectively. Likewise, the probabilities of
primary resistance to imatinib for patients with mutations in exons
11 or 9 of KIT, or with wild-type GISTs, are 5, 16 and 23%,
respectively. Secondary resistance to imatinib increases with the
duration of drug treatment; however, the mechanism underlying this
resistance is unclear. It is widely speculated that this phenomenon
is associated with secondary KIT mutations (18). Tumors with an underlying primary KIT
mutation in exon 11 exhibit improved response rates compared with
other mutational subtypes, but are at higher risk of developing
secondary mutations than those with an KIT exon 9 mutation or
wild-type GISTs (19).
A previous review (20) concluded that neoadjuvant imatinib
should be administered to reduce tumor bulk and thus facilitate the
complete surgical resection or increase the likelihood of organ
preservation of initially unresectable or borderline resectable
GISTs. As the first-line treatment for unresectable GISTs, certain
reports (21) have suggested
imatinib interruption is associated with a major risk of rapid
progression. Thus, imatinib administration should be continued
until disease progression or intolerance to toxicity in patients in
whom disease control has been achieved. The initial dose is usually
400 mg/day; however, it may be increased to 600 mg/day in patients
with KIT exon 9 mutations. Surgical removal of the lesion
may be performed and postoperative imatinib dose should increase
when local progression emerged after excluding patient compliance
(22,23). In cases of widespread progression,
imatinib dose may be increased to 600 mg/day, which may be more
appropriate for Chinese patients (24), or the second-line sunitinib may
alternatively be administered. If patients show no response to
imatinib or sunitinib, regorafenib is recommended as the third-line
therapy (25). A prospective,
randomized, double-blind trial (26)
revealed that certain patients with GIST may retain sensitivity to
certain tyrosin-kinase inhibitors following the failure of all
approved inhibitors. Thus, the reintroduction of tyrosine-kinase
inhibitors may delay disease progression.
During surgery in the present case, the tumor was
found to be closely connected with the diaphragmatic muscle,
pancreas, spleen and relevant blood vessels, and was therefore
identified as a case of unresectable GIST. Without tumor gene
detection, the patient initially received the standard 400 mg/day
dose of imatinib. At the 16-month follow-up, the patient achieved a
partial response, with an abdominal CT scan showing a significant
reduction of the tumor size (~70%). During the treatment period,
the patient experienced mild side effects, including nausea,
diarrhea, edema and leucopenia; however, these symptoms became
normal following symptomatic treatment. Thus, the present case
conforms with the good efficacy and safety of imatinib in GIST
reported in the aforementioned literature. According to the
proposal in a previous review (20),
surgery may be considered a viable option for patients with stable
disease following imatinib therapy. However, the patient refused to
undergo resection of the lesion after the tumor volume was reduced
and ultimately received imatinib therapy alone. Two clinical
studies, B2222 and S0033, demonstrated that long-term imatinib use
increased the 9-year OS rate in patients with unresectable GIST by
35 and 26%, respectively, and that side effects were relatively
rare. Prior studies (2,27) have suggested that patients with
advanced GIST exhibiting stable disease or limited progression
while receiving kinase inhibitor therapy exhibit prolonged PFS and
OS following debulking surgery. However, these were small-scale and
short-term clinical trials with no prominent clinical value.
Therefore, when patients with unresectable GISTs have obtained
stable disease or limited progression after receiving imatinib
therapy, it remains unclear whether a combination of imatinib with
surgical resection is more beneficial than receiving imatinib
alone. Thus, further long-term, large-scale, multicenter,
controlled trials are required to elucidate this unknown.
References
|
1
|
Søreide K, Sandvik OM, Søreide JA, Giljaca
V, Jureckova A and Bulusu VR: Global epidemiology of
gastrointestinal stromal tumours (GIST): A systematic review of
population-based cohort studies. Cancer Epidemiol. 40:39–46. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Du CY, Zhou Y, Song C, Wang YP, Jie ZG, He
YL, Liang XB, Cao H, Yan ZS and Shi YQ: Is there a role of surgery
in patients with recurrent or metastatic gastrointestinal stromal
tumours responding to imatinib: A prospective randomised trial in
China. Eur J Cancer. 50:1772–1778. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
ESMO/European Sarcoma Network Working
Group, . Gastrointestinal stromal tumours: ESMO Clinical Practice
Guidelines for diagnosis, treatment and follow-up. Ann Oncol.
25:(Suppl 3). iii21–iii26. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Corless CL, Fletcher JA and Heinrich MC:
Biology of gastrointestinal stromal tumors. J Clin Oncol.
22:3813–3825. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Barnett CM, Corless CL and Heinrich MC:
Gastrointestinal stromal tumors: Molecular markers and genetic
subtypes. Hematol Oncol Clin North Am. 27:871–888. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Corless CL, Barnett CM and Heinrich MC:
Gastrointestinal stromal tumours: Origin and molecular oncology.
Nat Rev Cancer. 11:865–878. 2011.PubMed/NCBI
|
|
7
|
Iorio N, Sawaya RA and Friedenberg FK:
Review article: The biology, diagnosis and management of
gastrointestinal stromal tumours. Aliment Pharmacol Ther.
39:1376–1386. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Joensuu H, Fletcher C, Dimitrijevic S,
Silberman S, Roberts P and Demetri G: Management of malignant
gastrointestinal stromal tumors. Lancet Oncol. 3:655–664. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Miettinen M, Furlong M, Sarlomo-Rikala M,
Burke A, Sobin LH and Lasota J: Gastrointestinal stromal tumors,
intramural leiomyomas, and leiomyosarcomas in the rectum and anus:
A clinicopathologic, immunohistochemical, and molecular genetic
study of 144 cases. Am J Surg Pathol. 25:1121–1133. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Day E, Waters B, Spiegel K, Alnadaf T,
Manley PW, Buchdunger E, Walker C and Jarai G: Inhibition of
collagen-induced discoidin domain receptor 1 and 2 activation by
imatinib, nilotinib and dasatinib. Eur J Pharmacol. 599:44–53.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Peng B, Lloyd P and Schran H: Clinical
pharmacokinetics of imatinib. Clin Pharmacokinet. 44:879–894. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
DeMatteo RP, Lewis JJ, Leung D, Mudan SS,
Woodruff JM and Brennan MF: Two hundred gastrointestinal stromal
tumors: Recurrence patterns and prognostic factors for survival.
Ann Surg. 231:51–58. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Blanke CD, Demetri GD, von Mehren M,
Heinrich MC, Eisenberg B, Fletcher JA, Corless CL, Fletcher CD,
Roberts PJ, Heinz D, et al: Long-term results from a randomized
phase II trial of standard-versus higher-dose imatinib mesylate for
patients with unresectable or metastatic gastrointestinal stromal
tumors expressing KIT. J Clin Oncol. 26:620–625. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
von Mehren M, Heinrich MC, Joensuu H,
Blanke CD, Wehrle E and Demetri GD: Follow-up results after 9 years
(yrs) of the ongoing, phase II B2222 trial of imatinib mesylate
(IM) in patients (pts) with metastatic or unresectable KIT+
gastrointestinal stromal tumors (GIST). J Clin Oncol. 29:(Suppl):
Abstract 10016. 2011.PubMed/NCBI
|
|
15
|
Demetri GD, von Mehren M, Blanke CD, Van
den Abbeele AD, Eisenberg B, Roberts PJ, Heinrich MC, Tuveson DA,
Singer S, Janicek M, et al: Efficacy and safety of imatinib
mesylate in advanced gastrointestinal stromal tumors. N Engl J Med.
347:472–480. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Blanke CD, Rankin C, Demetri GD, Ryan CW,
von Mehren M, Benjamin RS, Raymond AK, Bramwell VH, Baker LH, Maki
RG, et al: Phase III randomized, intergroup trial assessing
imatinib mesylate at two dose levels in patients with unresectable
or metastatic gastrointestinal stromal tumors expressing the kit
receptor tyrosine kinase: S0033. J Clin Oncol. 26:626–632. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Blanke CD, Rankin C, Benjamin R, Raymond
AK, Heinrich MC, Fletcher CDM, Crowley J, Borden EC, Demetri GD and
Baker LH: Long-term survival on S0033-a phase III randomized,
intergroup trial assessing imatinib mesylate at two dose levels in
patients with unresectable or metastatic gastrointestinal stromal
tumors (GISTs). Eur J Cancer. 47:(Suppl 1): Abstract 9404. 2011.
View Article : Google Scholar
|
|
18
|
Corless CL and Heinrich MC: Molecular
pathobiology of gastrointestinal stromal sarcomas. Annu Rev Pathol.
3:557–586. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wardelmann E, Merkelbach-Bruse S, Pauls K,
Thomas N, Schildhaus HU, Heinicke T, Speidel N, Pietsch T, Buettner
R, Pink D, et al: Polyclonal evolution of multiple secondary KIT
mutations in gastrointestinal stromal tumors under treatment with
imatinib mesylate. Clin Cancer Res. 12:1743–1749. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Serrano C and George S: Recent advances in
the treatment of gastrointestinal stromal tumors. Ther Adv Med
Oncol. 6:115–127. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Patrikidou A, Chabaud S, Ray-Coquard I,
Bui BN, Adenis A, Rios M, Bertucci F, Duffaud F, Chevreau C,
Cupissol D, et al: French Sarcoma Group: Influence of imatinib
interruption and rechallenge on the residual disease in patients
with advanced GIST: Results of the BFR14 prospective French Sarcoma
Group randomised, phase III trial. Ann Oncol. 24:1087–1093. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Blay JY and Rutkowski P: Adherence to
imatinib therapy in patients with gastrointestinal stromal tumors.
Cancer Treat Rev. 40:242–247. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Patel S: Managing progressive disease in
patients with GIST: Factors to consider besides acquired secondary
tyrosine kinase inhibitor resistance. Cancer Treat Rev. 38:467–472.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Li J, Gong JF, Li J, Gao J, Sun NP and
Shen L: Efficacy of imatinib dose escalation in Chinese
gastrointestinal stromal tumor patients. World J Gastroenterol.
18:698–703. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Demetri GD, Reichardt P, Kang YK, Blay JY,
Rutkowski P, Gelderblom H, Hohenberger P, Leahy M, von Mehren M,
Joensuu H, et al: Efficacy and safety of regorafenib for advanced
gastrointestinal stromal tumors after failure of imatinib and
sunitinib (GRID): An international, multicentre, randomised,
placebo-controlled, phase 3 trial. Lancet. 381:295–302. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kang YK, Ryu MH, Yoo C, Ryoo BY, Kim HJ,
Lee JJ, Nam BH, Ramaiya N, Jagannathan J and Demetri GD: Resumption
of imatinib to control metastatic or unresectable gastrointestinal
stromal tumours after failure of imatinib and sunitinib (RIGHT): A
randomised, placebo-controlled, phase 3 trial. Lancet Oncol.
14:1175–1182. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Park SJ, Ryu MH, Ryoo BY, Park YS, Sohn
BS, Kim HJ, Kim CW, Kim KH, Yu CS, Yook JH, et al: The role of
surgical resection following imatinib treatment in patients with
recurrent or metastatic gastrointestinal stromal tumors: Results of
propensity score analyses. Ann Surg Oncol. 21:4211–4217. 2014.
View Article : Google Scholar : PubMed/NCBI
|