Introduction
Central pontine myelinolysis (CPM), also known as
osmotic demyelination syndrome (ODS), is a rare demyelinating
disorder characterized by the loss of myelin in the center of the
basis pontis (1). CPM was originally
considered to be the result of excessively rapid correction of
slowly progressive hyponatremia in patients with chronic medical
conditions, such as chronic alcoholism, malnutrition and malignancy
(2,3). The proposed mechanism of CPM is that
neuronal demyelination begins when osmotically active substances
such as sodium are depleted from the serum and free water shifts
into the brain (4). However, there
have been occasional reports of CPM not accompanied by hyponatremia
or drastic changes in serum sodium level (2,3). The
exact incidence of CPM is unknown. In a study of 3,000 brains
examined postmortem, 15 cases of asymptomatic CPM were evident
(5). Kleinschmidt-Demasters et
al (6,7) reported that 39.4% of patients of CPM
were diagnosed with alcohol poisoning, 21.5% had a history of
correcting hyponatremia, and 17.4% received a liver
transplantation. Although earlier reports on CPM described very
poor outcome with mortality rates as high as 50% in the first 2
weeks after presentation and 90% at 6 months, recent results
suggest the decreased mortality mainly due to early diagnosis and
improved intensive care treatment (7). Chronic alcoholism is frequently
associated with CPM, which can have a variable clinical outcome. In
the present case report, a chronic alcoholic patient who suffered
from CPM without hyponatremia is described. The patient eventually
completely recovered.
Case report
A 70-year-old female with a history of alcohol abuse
for two months presented with intermittent psychosis and
involuntary tremors at the First Hospital of Jilin University
(Jilin, China), in November 2014. The patient's psychiatric
symptoms were characterized by auditory and visual hallucinations
intermittently. The onset of the symptoms began after two months of
alcohol abuse, when she began to drink a half bottle of white
spirits per day. The patient denied other substance use, and her
vital signs were stable. At the initial neurological examination,
the patient was cooperative and her language was intact with no
word-finding disorder. The patient was well oriented, her pupils
were equal size (3.0 mm) and light reflexes were normal on both
sides. The patient did not have extraocular movement limitations or
nystagmus, and her motor strength, sensory exam and deep tendon
reflexes were normal.
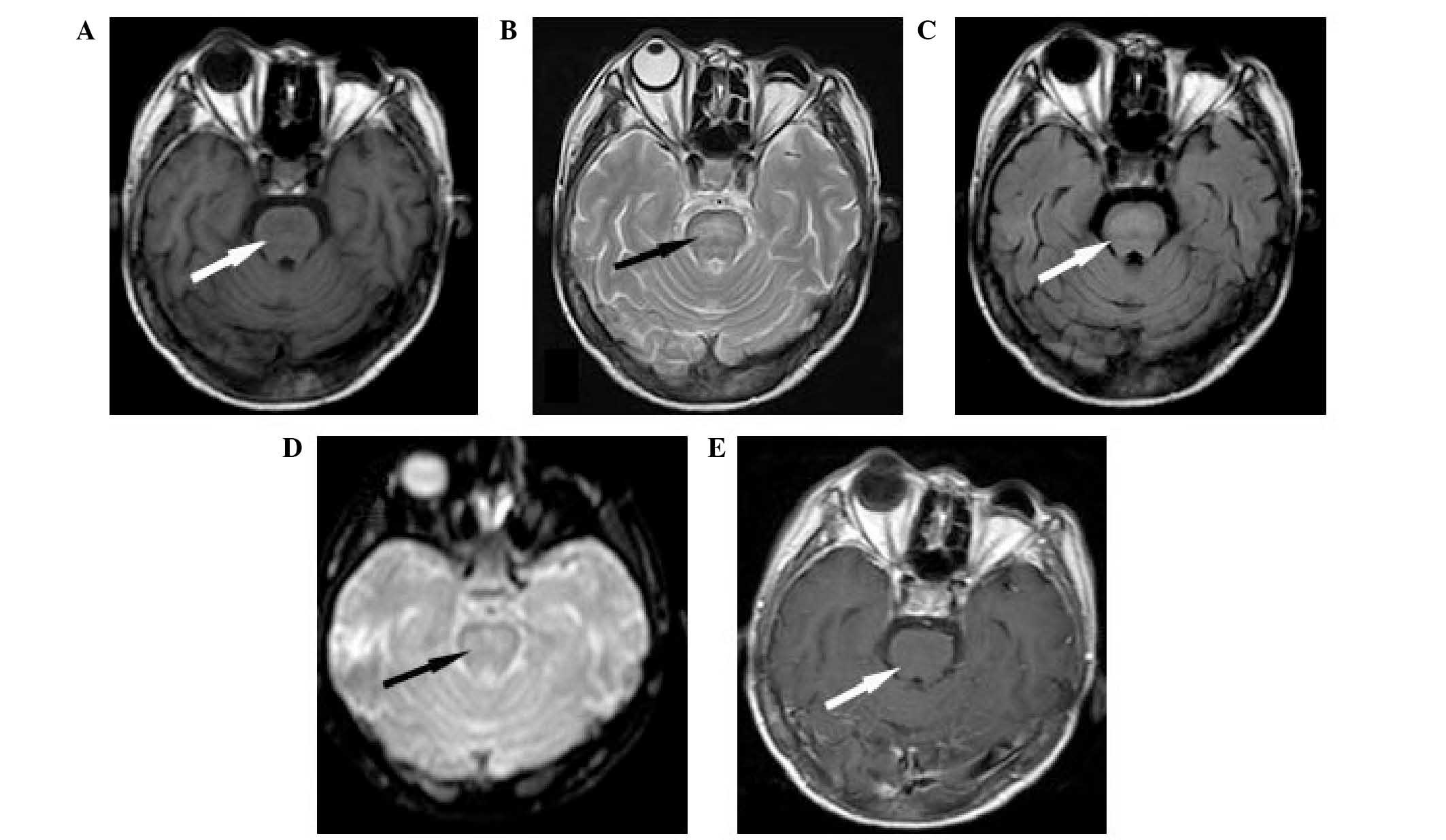
Routine laboratory data showed that the electrolytes
and renal and liver function tests were within normal ranges.
However, brain magnetic resonance imaging (MRI) identified a
central pontine lesion, hyperintense on T2-weighted and
fluid-attenuated inversion-recovery (FLAIR) imaging (Fig. 1). An increased signal on
diffusion-weighted imaging (DWI) indicated abnormal restricted
diffusion. The lesion was hypointense on T1-weighted and
non-contrast enhanced imaging. No remarkable changes were detected
in the thalamus or mammillary bodies.
The patient's symptoms gradually improved after one
week of supplementation with vitamin B1 (300 mg/day) and
vitamin B12 (1,000 µg/day), and the intermittent mental
symptoms and tremor of the limbs soon disappeared. The patient
fully recovered to a normal mental and physical state, and was
discharged after two weeks. The MRI at the one month follow-up
visit showed a reduction in the hyperintensity and extent of the
pontine lesion evident on the FLAIR and T2 weighted images. Written
informed consent was obtained from the patient prior to their
inclusion in the present study.
Discussion
Underlying chronic diseases may be central to the
development of CPM, such as chronic alcoholism, malnutrition and
liver transplantation. CPM can develop in the absence of serum
sodium fluctuations, with more than one predisposing factor.
Chronic alcoholism is the most common reason for developing CPM
(6). However, only a small number of
cases of CPM following alcohol withdrawal have been reported
(8,9); the majority of the cases are associated
with normonatremia (10). In the
present report, the patient with chronic alcoholism developed CPM
following alcohol abuse for two months. Laboratory examination
revealed normal blood sodium levels.
The clinical presentation of CPM includes a range of
neurological severity, between asymptomatic presentation and
quadriparesis and coma, depending on the distribution of
demyelination in the pontine (1,11).
Symptoms typically begin with weakness, confusion and dysarthria,
and may progress to pseudobulbar palsy and locked-in-syndrome.
Psychotic symptoms have rarely been described in association with
CPM. However, one previously reported case described an alcoholic
patient who developed psychotic symptoms during alcohol withdrawal
(9). This patient presented with
limb tremors and intermittent mental abnormalities following heavy
drinking, and was in accordance with the clinical presentation of
CPM.
Diagnosis of CPM is based on a clinical neurologic
examination and is confirmed by imaging studies. MRI is the primary
method for diagnosis, and is superior to computed tomography
(12,13). Besides hypointense T1- and
hyperintense T2-weighted lesions on MRI (14), DWI can be useful in diagnosing and
predicting the prognosis of ODS. The lesions identified in patients
with CPM may appear between days and weeks after the onset of
symptoms and may resolve completely over a period of months, and
the majority of patients have a good prognosis with supportive
treatment (14). In the present case
report, a brain MRI of the patient confirmed the characteristic of
CPM.
The prognosis of CPM is typically poor, and may
result in permanent neurological sequelae or mortality (11). Currently, no effective treatment is
available for CPM; however, with supportive care, spontaneous
recovery is possible. In the current case report, the patient
developed CPM following heavy drinking, rather than from
withdrawal. Laboratory examination did not indicate the presence of
hyponatremia, and the patient's symptoms were uncommon; however,
MRI confirmed CPM. In conclusion, it is apparent that physicians
should pay attention to the development of CPM in alcoholic
patients.
References
|
1
|
Adams RD, Victor M and Mancall EL: Central
pontine myelinolysis: A hitherto undescribed disease occurring in
alcoholic and malnourished patients. AMA Arch Neurol Psychiatry.
81:154–172. 1959. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lampl C and Yazdi K: Central pontine
myelinolysis. Eur Neurol. 47:3–10. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lupato A, Fazio P, Fainardi E, Cesnik E,
Casetta I and Granieri E: A case of asymptomatic pontine
myelinolysis. Neurol Sci. 31:361–364. 2001. View Article : Google Scholar
|
|
4
|
Laureno R and Karp BI: Myelinolysis after
correction of hyponatremia. Ann Intern Med. 126:57–62. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Newell KL and Kleinschmidt-DeMasters BK:
Central pontine myelinolysis at autopsy; a twelve year
retrospective analysis. J Neurol Sci. 142:134–139. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Huang WY, Weng WC, Peng TI, Ro LS, Yang CW
and Chen KH: Central pontine and extrapontine myelinolysis after
rapid correction of hyponatremia by hemodialysis in a uremic
patient. Ren Fail. 29:635–638. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kleinschmidt-Demasters BK, Rojiani AM and
Filley CM: Central and extrapontine myelinolysis: Then. and now. J
Neuropathol Exp Neurol. 65:1–11. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Korn-Lubetzki I, Virozub Y and Orbach H:
Central pontine myelinolysis after alcohol withdrawal. Isr Med
Assoc J. 4:6562002.PubMed/NCBI
|
|
9
|
Yoon B, Shim YS and Chung SW: Central
pontine and extrapontine myelinolysis after alcohol withdrawal.
Alcohol Alcohol. 43:647–649. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Martin RJ: Central pontine and
extrapontine myelinolysis: The osmotic demyelination syndromes. J
Neurol Neurosurg Psychiatry. 75(Suppl 3): iii22–iii28.
2004.PubMed/NCBI
|
|
11
|
Mochizuki H, Masaki T, Miyakawa T, Nakane
J, Yokoyama A, Nakamura Y, Okuyama K, Kamakura K, Motoyoshi K,
Matsushita S and Higuchi S: Benign type of central pontine
myelinolysis in alcoholism-clinical, neuroradiological and
electrophysiological findings. J Neurol. 250:1077–1083. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kwon HG and Jang SH: Motor recovery
mechanism in a quadriplegic patient with locked-in syndrome.
NeuroRehabilitation. 30:113–117. 2012.PubMed/NCBI
|
|
13
|
Rippe DJ, Edwards MK, D'Amour PG, Holden
RW and Roos KL: MR imaging of central pontine myelinolysis. J
Comput Assist Tomogr. 11:724–726. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Menger H and Jörg J: Outcome of central
pontine and extrapontine myelinolysis (n=44). J Neurol.
246:700–705. 1999. View Article : Google Scholar : PubMed/NCBI
|