Introduction
Intracoronary stent implantation has been widely
used in the treatment of coronary heart disease (CHD). It has also
reduced the incidence rate of restenosis after intracoronary
intervene-tional therapy; however, the stent restenosis rate is as
high as 20% at 3–6 months after surgery (1). Albertal et al (2) and Singh et al (3) have reported that the morbidity rate of
patients with of in-stent restenosis in left anterior descending
(LAD) is higher than that in left circum-flex (LCX) and right
coronary artery (RCA), and remains the main factor to influence
long-term prognosis in the patients with CHD. Coronary angiography
(CAG) and intravascular ultrasound were typically considered as the
criterion diagnostic standard for the evaluation of in-stent
restenosis, but they are invasive and expansive (4). Therefore, in order to determine an
efficient treatment strategy, a more convenient and accurate
evaluation method for clinical screening of patients with coronary
stent restenosis is required.
Gated myocardial perfusion imaging (G-MPI) is a
convenient, non-invasive and accurate assessment method for
myocardial blood perfusion. In addition, G-MPI is a simultaneous
measurement tool for cardiac function parameters, namely left
ventricular ejection fraction (LVEF) and ventricular wall motion
(5–7). Adenosine stress G-MPI has been widely
used in the diagnosis, risk stratification, and prognosis
evaluation of CHD (8,9). However, adenosine is costly and, thus,
there is reason to identify similar pharmaceuticals to replace it.
Adenosine triphosphate (ATP) is a similar compound to adenosine
regarding its pharmacological mechanism, but also inexpensive and
thus more suitable for use in clinical practice (10).
Coronary angiography (CAG) is typically considered
as the criterion diagnostic standard for the evaluation of stent
restenosis. In the present study, the CAG diagnosis was determined
and used to investigate the clinical application efficacy of ATP
stress 99mTc-methoxyisobutylisonitrile
(99mTc-MIBI) G-MPI in the evaluation of coronary artery
stent restenosis, by comparing the results of the two methods.
Patients and methods
Ethical approval
The study protocol was approved by the Ethics Review
Board of the First Affiliated Hospital of China Medical University
(Shenyang, China). Written informed consent was obtained from all
study participants. All the procedures were conducted in accordance
with the Declaration of Helsinki and relevant policies in
China.
Patient population
A total of 71 patients with typical angina pectoris
symptoms from the hospital ward or outpatient service of the First
Affiliated Hospital of China Medical University between January
2012 and December 2014 were enrolled into the current study
(Table I). All patients had
undergone coronary stent implantations (108 coronary arteries in
total) 3 months to 10 years (2.5±2.1 years) before enrollment.
Typical angina pectoris symptoms included chest pain, stuffy chest,
left upper limb pain and left shoulder pain.
 | Table I.Clinical characteristics of the
patients in the study. |
Table I.
Clinical characteristics of the
patients in the study.
| Characteristic | Value |
|---|
| Age, years | 60.2±9.5 |
| Gender, n (%) |
|
| Men | 56 (79) |
|
Women | 15 (21) |
| Condition, n (%) |
|
|
Myocardial infarction | 36 (51) |
| Angina
pectoris | 35 (49) |
|
Single-vessel disease | 17 (24) |
|
Double-vessel disease | 23 (32) |
|
Triple-vessel disease | 31 (44) |
| Vessel, n (%) |
|
| LAD
artery | 45 (42) |
| LCX
artery | 24 (22) |
| RCA | 39 (36) |
All the patients underwent CAG and one-day ATP
stress/rest 99mTc-MIBI G-MPI on the same day within 1
month. The contraindications for the exclusion of ATP stress were
as follows: i) Acute coronary syndrome; ii) bronchial asthma or
chronic obstructive pulmonary disease; iii) sick sinus syndrome,
with second- or third-degree atrioventricular block; iv) severe
cardiac insufficiency, with cardiac function level III or IV; and
v) high systolic blood pressure (≥180 mmHg) or low systolic blood
pressure (≤90 mmHg).
Instruments and medicines
The instrument used was a VG double-probe
single-photon emission computed tomography (SPECT) scanner with a
low-energy high-resolution parallel hole collimator, which was
provided by the General Electric Healthcare (Chicago, IL, USA). ATP
was provided by Tianjin Pharmaceutical Jiaozuo Co. Ltd. (Jiaozuo,
China). 99mTc was provided by Yuanzi Gaoke Co., Ltd.
(Beijing, China), and MIBI was provided by the Jiangyuan
Pharmaceutical Factory of the Jiangsu Institute of Atomic Medicine
(Jiangsu, China).
ATP-induced stress experiment
Prior to the experiments, the patients discontinued
the administration of any β-blockers, nitrate
angiotensin-converting enzyme inhibitors and calcium ion antagonist
for at least 48 h. In addition, administration of theophylline
drugs was discontinued for at least 12 h. A double venous pathway
was established, one for the injection of ATP and the other for the
injection of 99mTc-MIBI. Using an intravenous tracer
pump, ATP was injected at 0.16 mg/kg/min at a constant speed for 6
min. After 3 min, 99mTc-MIBI 740 MBq was injected from
the other pathway. Prior to the intravenous ATP injection, a
12-lead electrocardiogram (ECG), blood pressure test, heart rate
and symptoms were recorded at various time points, as follows: At 3
min before injection, right after injection, 3 min after injection,
and we monitored them during the entire procedure (10).
One-day stress/rest
99mTc-MIBI G-MPI
At 30 min after the ATP stress experiment, the
subjects were provided with high-fat food (sour milk) to promote
liver radioactivity removal. After 1 h from the meal, the cardiac
images were collected using a VG double-probe SPECT scanner with a
low-energy high-resolution parallel hole collimator, from the right
anterior oblique 45° to the left posterior oblique 45° planes
(6°/view, 40 sec/view, with 8 frames per cardiac cycle) using a
64×64 matrix, and observed under ×1.45 magnification. The gated
slicing image by the ECToolbox Slicing software (Emory University;
Syntermed, Inc., Atlanta, GA) was calibrated, and the slicing image
was reconstructed using Butterworth low-pass filter
back-projection, at a 6.59-mm thickness. The short axis, vertical
long axis and horizontal axial slicing images were obtained, and
the function parameters of LVEF were measured using QPS 2009 and
QGS 2009 software (Siemens Medical Systems) . After 3–4 h,
99mTc-MIBI 740 MBq injection was administered in the
state of rest. At 30 min after the intravenous injection, the
patients were fed a high-fat meal, and 1 h later an image was
obtained. The same collection method was used as that for stress
imaging (7).
Scintigraphic image
interpretation
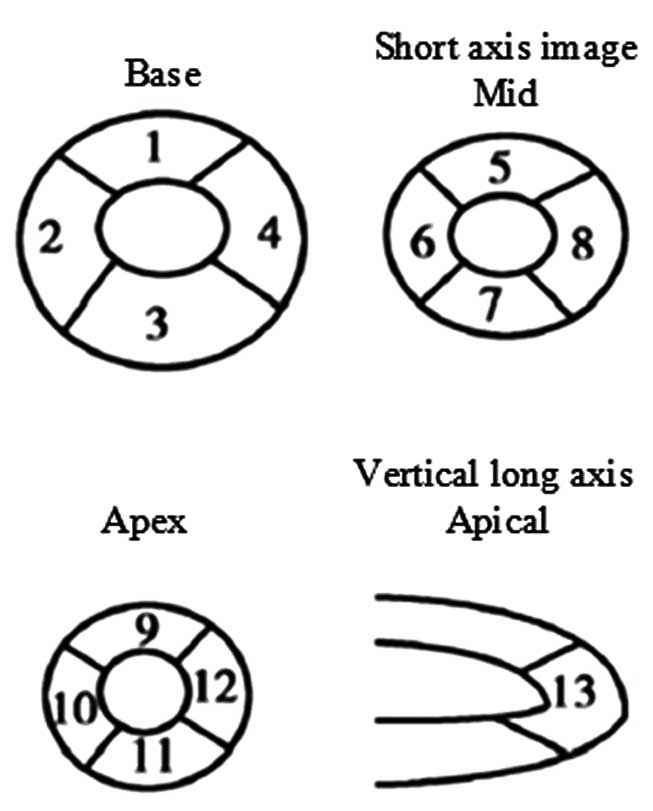
On the image obtained by 99mTc-MIBI
G-MPI, the left ventricle along the short-axis was divided into the
apex, central and basal departments. These three segments were then
respectively divided into the anterior, septum, inferior and
lateral walls, combined with the cardiac apex department of the
vertical long axis, with a total of 13 segments formed. Coronary
blood vessels dominated the areas, as shown in Fig. 1. Using the conventional visual
method, two experienced nuclear medicine physicians evaluated the
nuclide distribution of each segment of the ATP stress
99mTc-MIBI G-MPI, without reference to the clinical data
and the CAG findings of the patients. Scored visually in four
classes (0–3), normal, mildly reduced, moderately reduced and
severely reduced. Reduction of nuclide distribution were observed
on two or more consecutive slices in the same place was considered
a nuclide distribution anomaly. On a combined stress/rest G-MPI
examination, a reversible or partially reversible nuclide
distribution anomaly in the dominating region with stent blood
vessels was defined as myocardial ischemia, and in-stent resenosis,
while myocardial infarction combined with myocardial ischemia was
defined as coronary in-stent restenosis (11,12).
CAG examination
Within a month after ATP stress
99mTc-MIBI G-MPI, experienced cardiovascular
interventional physicians performed selectively left and right CAG
using Judkins method, and divided the coronary artery into the LAD
artery, LCX artery and RCA. Without reference to the ATP stress
99mTc-MIBI G-MPI, a stenosis of ≥50% of the vascular
inner diameter appearing in the coronary stent or within a 5-mm
range from the stent was defined as restenosis. In cases where
stenosis appeared at a distance of >5 mm from the stent, this
was defined as a new stenosis of other region (13).
Statistical analysis
SPSS version 17 software (SPSS, Inc., Chicago, IL,
USA) was used for statistical analysis. Enumeration data are
expressed as rate and percentages. Using CAG as the criterion
diagnostic standard, the sensitivity, specificity, accuracy,
positive predictive value and negative predictive value of ATP
stress 99mTc-MIBI G-MPI in the evaluation of stent
restenosis were calculated. The Fisher exact probability method was
used to compare the rates, and P<0.05 was considered to show
statistically significant differences.
Results
CAG results
Of the 71 patients originally included in the
present study, data for 5 patients were excluded from the final
analysis due to the occurrence of new stenosis. Therefore, the
study included a total of 66 patients with stent implantation
performed in 99 coronary arteries. Among these, 39 patients (59%)
presented in-stent restenosis, 19 presented myocardial infarction
and 20 presented non-myocardial infarction. In-stent restenosis was
observed in 45 coronary arteries out of the 99 arteries subjected
to stent implantation (~45%), including 24 LAD arteries, 6 LCX
arteries and 15 RCAs.
ATP stress 99mTc-MIBI G-MPI
efficacy in diagnosing stent restenosis
The ability of ATP stress 99mTc-MIBI
G-MPI to diagnose stent restenosis was analyzed against the
diagnostic ability of CAG. In those 39 positive patients diagnosed
by CAG, 33 were diagnosed positve by ATP stress
99mTc-MIBI G-MPI. In those 27 negative patients
diagnosed by CAG, three were diagnosed positive by ATP stress
99mTc-MIBI G-MPI. The diagnostic sensitivity,
specificity, accuracy, positive predictive value and negative
predictive value of ATP stress 99mTc-MIBI G-MPI for all
the patients were found to be 85, 89, 86, 92 and 80%, respectively
(Table II). This result indicated
that ATP stress 99mTc-MIBI G-MPI has higher clinical
value in diagnosing in-stent restenosis.
| Table II.Values of adenosine triphosphate
stress 99mTc-MIBI G-MPI for evaluating stent
restenosis. |
Table II.
Values of adenosine triphosphate
stress 99mTc-MIBI G-MPI for evaluating stent
restenosis.
|
| CAG |
|
|---|
|
|
|
|
|---|
| 99mTc-MIBI
G-MPI | Positive | Negative | Total |
|---|
| Positive | 33 | 3 | 36 |
| Negative | 6 | 24 | 30 |
| Total | 39 | 27 | 66 |
ATP stress 99mTc-MIBI G-MPI
efficacy in diagnosing stent restenosis in different types of
CHD
The diagnostic sensitivity, specificity, accuracy,
positive predictive value and negative predictive value of ATP
stress 99mTc-MIBI G-MPI were 79, 88, 83, 88 and 78%,
respectively, when evaluating stent restenosis in patients with
myocardial infarction. Similarly, these values were 90, 91, 90, 95
and 83%, respectively, when evaluating patients with non-myocardial
infarction (Table III). Therefore,
the diagnostic values were higher in patients with non-myocardial
infarction compared with those in patients with myocardial
infarction; however, no statistically significant difference was
observed between the two patient groups (P>0.05).
| Table III.ATP stress 99mTc-MIBI
G-MPI efficacy in diagnosing stent restenosis in different types of
CHD. |
Table III.
ATP stress 99mTc-MIBI
G-MPI efficacy in diagnosing stent restenosis in different types of
CHD.
|
| CAG in myocardial
infarction patients | CAG in
non-myocardial infarction patients |
|---|
|
|
|
|
|---|
|
99mTc-MIBI G-MPI | Positive | Negative | Total | Positive | Negative | Total |
|---|
| Positive | 15 | 2 | 17 | 18 | 1 | 19 |
| Negative | 4 | 14 | 18 | 2 | 10 | 12 |
| Total | 19 | 16 | 35 | 20 | 11 | 31 |
ATP stress 99mTc-MIBI G-MPI
efficacy in diagnosing stent restenosis in different coronary
arteries
The diagnostic sensitivity, specificity, accuracy,
positive predictive value and negative predictive value of ATP
stress 99mTc-MIBI G-MPI in the evaluation of stent
restenosis in different artery types were as follows: 83, 89, 86,
91 and 80%, respectively, in LAD arteries; 83, 81, 82, 63 and 93%,
respectively, in LCX arteries; 80, 75, 77, 71 and 83%,
respectively, in RCAs (Table IV).
These results indicate that the sensitivity, specificity and
accuracy of diagnosis with ATP stress 99mTc-MIBI G-MPI
were higher for the LAD artery stent restenosis compared with the
LCX artery and RCA stent restenosis diagnoses; however, no
statistically significant differences were observed among the three
different artery categories (P>0.05).
| Table IV.ATP stress 99mTc-MIBI
G-MPI efficacy in diagnosing stent restenosis in different coronary
arteries. |
Table IV.
ATP stress 99mTc-MIBI
G-MPI efficacy in diagnosing stent restenosis in different coronary
arteries.
|
| CAG in LAD
artery | CAG in LCX
artery | CAG in RCA |
|---|
|
|
|
|
|
|---|
|
99mTc-MIBI G-MPI | Positive | Negative | Total | Positive | Negative | Total | Positive | Negative | Total |
|---|
| Positive | 20 | 2 | 22 | 5 | 3 | 8 | 12 | 5 | 17 |
| Negative | 4 | 16 | 20 | 1 | 13 | 14 | 3 | 15 | 18 |
| Total | 24 | 18 | 42 | 6 | 16 | 22 | 15 | 20 | 35 |
ATP stress 99mTc-MIBI G-MPI
efficacy in diagnosing stent restenosis in the patients with
different number of diseased vessels
The diagnostic sensitivity, specificity, accuracy,
positive predictive value and negative predictive value of ATP
stress 99mTc-MIBI G-MPI according to the number of
diseased vessels in the patients were as follows: Patients with
single-vessel disease, 80, 100, 87, 100 and 71%, respectively;
patients with double-vessel disease, 91, 82, 86, 83 and 90%,
respectively; and patients with triple-vessel disease, 83, 91, 86,
94 and 77%, respectively. The results showed no significant
difference in diagnosing in-stent restenosis by ATP stress
99mTc-MIBI G-MPI between these different number of
diseased vessels (P>0.05) (Table
V).
| Table V.ATP stress 99mTc-MIBI
G-MPI efficacy in diagnosing stent restenosis in patients with a
different number of diseased vessels. |
Table V.
ATP stress 99mTc-MIBI
G-MPI efficacy in diagnosing stent restenosis in patients with a
different number of diseased vessels.
|
| CAG in
single-vessel patients | CAG in
double-vessel patients | CAG in
triple-vessel patients |
|---|
|
|
|
|
|
|---|
|
99mTc-MIBI G-MPI | Positive | Negative | Total | Positive | Negative | Total | Positive | Negative | Total |
|---|
| Positive | 8 | 0 | 8 | 10 | 2 | 12 | 15 | 1 | 16 |
| Negative | 2 | 5 | 7 | 1 | 9 | 10 | 3 | 10 | 13 |
| Total | 10 | 5 | 15 | 11 | 11 | 22 | 18 | 11 | 29 |
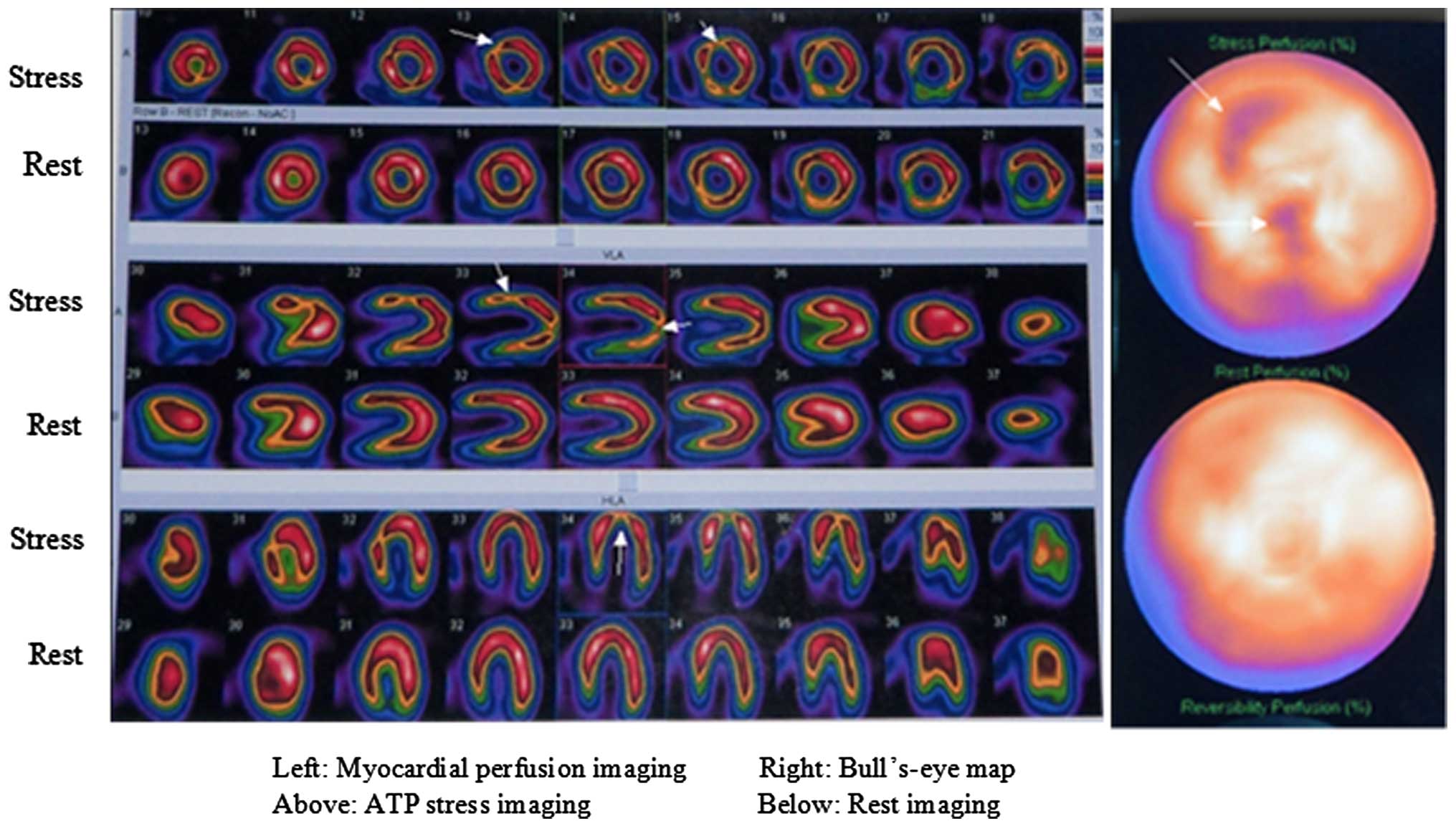
Typical case
A 56-year-old male patient with angina pectoris, who
underwent coronary stent implantation in the LAD artery 10 years
previously, experienced intermittent episodes of chest pain that
were persistent for 1 month. ATP stress/rest 99mTc-MIBI
G-MPI was performed as shown in Fig.
2. It was observed that nuclide distribution was mildly
decreased and completely reversible in the anterior, anteroseptum
and apex areas, while it was incompletely reversible in the
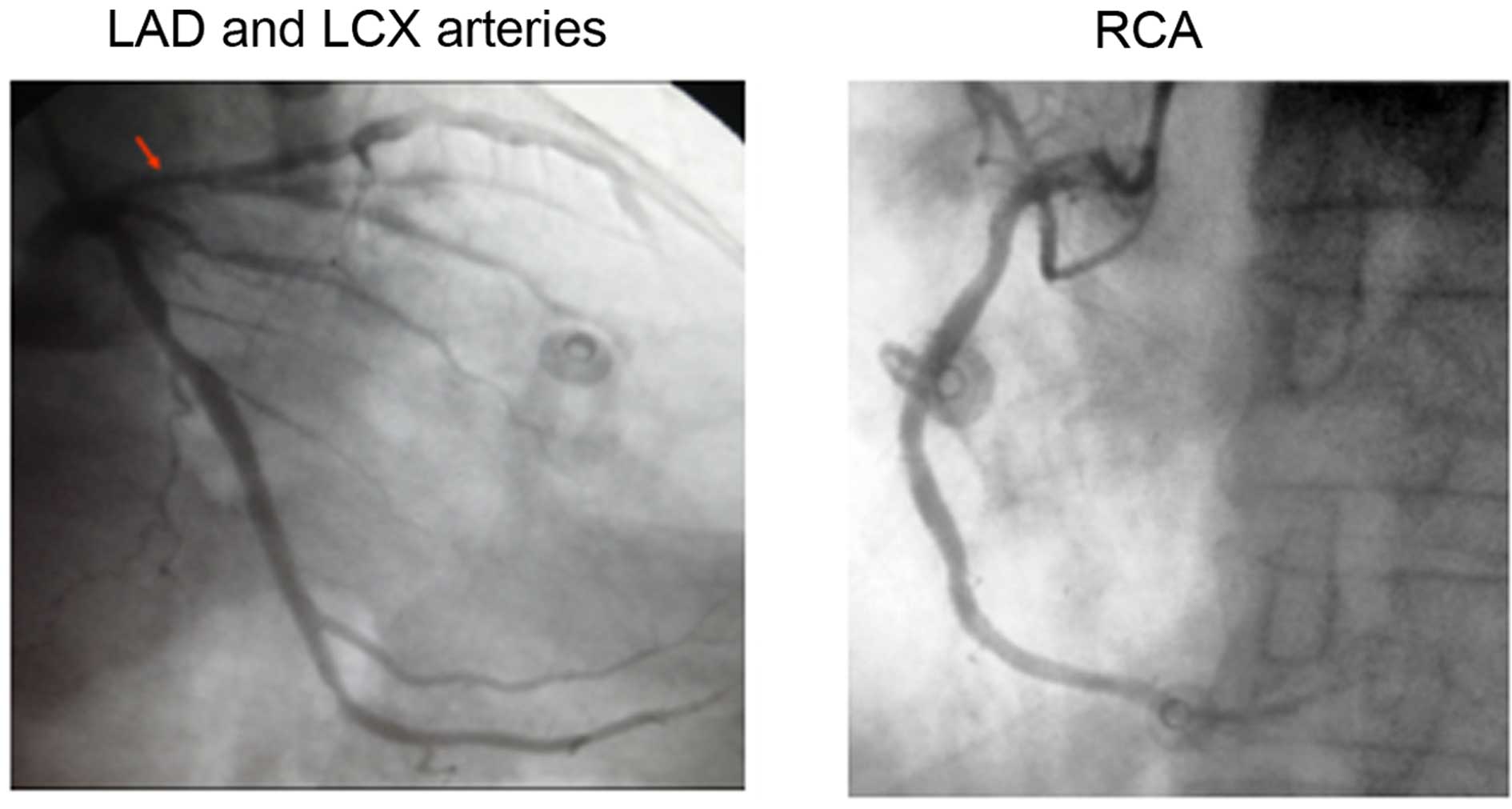
anteroposterior and posterolateral areas. Subsequently, CAG was
performed 2 days after ATP stress/rest 99mTc-MIBI G-MPI.
As shown in Fig. 3, 80% stent
stenosis was observed in the LAD artery, as well as 40% stenosis in
the RCA and LCX artery, confirming that the LAD artery had stent
restenosis. Thus in this case, ATP stress/rest
99mTc-MIBI G-MPI agree with CAG.
Discussion
The methods currently used for diagnosing coronary
stent restenosis mainly include CAG, exercise ECG, coronary
computed tomography angiography (CTA) and stress MPI. Although CAG
is known as the criterion standard for the diagnosis of coronary
artery stenosis and stent restenosis, it is an invasive
examination, with high cost and low patient compliance. In
addition, although exercise ECG is a more affordable technique, it
has low sensitivity. Buchler et al (14) reported that the sensitivity rates of
exercise ECG for detecting coronary artery stent restenosis were
57.3, 54.5 and 38.5% at 6 weeks, 6 months and 1 year, respectively,
after coronary stent implantation. So, the result indicated the
presence of myocardial ischemia and LAD in-stent resenosis in this
patient. Furthermore, coronary CTA image quality is easily
affected, not only by arteriosteogenesis, but also by the patients'
heart rate, heart rate fluctuations and partial stent volume.
However, stress MPI is a non-invasive method that can accurately
evaluate coronary in-stent restenosis.
The stress testing method mainly includes exercise-,
adenosine-, dipyridamole-, dobutamine- and ATP-induced stresses.
Exercise-induced stress is often not inducible in elderly people,
while dobutamine-induced stress is time-consuming and not suitable
for patients with high blood pressure. In addition, dipyridamole
has a long half-life period and adenosine is expensive, thus
limiting their application in stress testing. By contrast, ATP has
a short half-life period (<20 sec) and is eliminated quickly
from the body. In addition, ATP has relatively few adverse side
effects, it is easily converted to adenosine in the body, and its
cost is much lower than that of adenosine. Therefore, ATP has a
more extensive application value compared with the other compounds
(15).
ATP decomposes rapidly in vivo, producing
adenosine diphosphate, adenosine phosphate and adenosine. The
resulting adenosine then combines with vascular smooth muscle cells
and binds with the A2 receptor, activating adenylate cyclase, which
increases cycle adenosine monophosphate levels, activates potassium
channels, reduces intracellular calcium uptake and expands coronary
arteries. In addition, adenosine can significantly expand normal
coronary arteries, although it does not significantly influence the
increase in arterial blood flow in stenosis. The blood flow
resistance is lower in the non-ischemic zone compared with that in
the ischemic areas into the non ischemia areas are through the
collateral circulation reflux to the non-ischemia area, which is
namely the transverse vascular steal phenomenon (16). Furthermore, adenosine increases the
coronary blood flow, which not only increases the pressure
difference cross the stenosed coronary arteries, but also decrease
the distal blood flows of stenosed vessels, and cause the blood
flows of epicardium increasing and blood flows of endocardium
decreasing, this is known as the longitudinal vascular steal
phenomenon. This type of uneven blood flow distribution causes
uneven myocardial nuclide uptake. In cases where G-MPI reveals
radionuclide reduction or defects in stress state, the radionuclide
defects may improve partly or fully in rest state (17).
In the present study, 59% of 66 patients presented
in-stent restenosis, with 45% of 99 coronary arteries with in-stent
restenosis, which is higher than the 20% incidence of patients
previously reported in the literature (1). This may be explained by the fact that
the present study selected patients with typical angina pectoris
symptoms subsequent to stenting rather than randomly selecting
patients who had undergone stenting.
Galassi et al (18) detected stent restenosis using sports
stress 99mTc-tetrofosmin MPI in 97 patients subsequent
to coronary stenting. This previous study observed sensitivity,
specificity, accuracy, positive predictive value and negative
predictive values of 82, 84, 83, 69 and 91%, respectively. By
contrast, these values in the present study were 85, 89, 86, 92 and
86%, respectively, which are slightly higher compared with those
reported by Galassi et al (18). In total, 6 patients in our study
showed positive results on CAG and negative results on ATP stress
99mTc-MIBI G-MPI, mainly due to the presence of
collateral circulation. In addition, the regulating function of the
coronary artery itself was not affected in 50% of the critical
coronary in-stent stenosis, the blood flow reserve capacity was
close to normal, and the stress myocardial perfusion had no
reversible defects in the state of stress. Furthermore, 3 patients
demonstrated negative results on CAG and positive results on ATP
stress 99mTc-MIBI G-MPI, as microangiopathy mainly led
to the appearance of decreased perfusion in the non-stenosis
coronary area by reducing the mild nuclide distribution.
Kósa et al (19) reported the sensitivity and
specificity of stress MPI for detecting stent restenosis in 82
patients. The study identified that the sensitivity and specificity
of MPI in the myocardial infarction area were 64 and 72%,
respectively, while these values in the non-myocardial infarction
area were 100 and 82%, respectively. In the present study, the
sensitivity, specificity and accuracy of the G-MPI technique used
were 79, 88 and 83%, respectively, in the myocardial infarction
group, whereas these values in the non-myocardial infarction group
were 90, 91 and 90%, respectively. It is evident that the
sensitivity was lower for the myocardial infarction group compared
with that for the non-myocardial infarction group, as scar tissue
formed in the infarction area and the number of viable myocardial
cells was reduced, leading to a significant reduction in myocardial
cell nuclide uptake; thus, the stress/rest nuclide MPI reversible
distribution was not clear. In addition, 5 patients in the current
study developed complete myocardial infarction due to the stent
implantation vessel governing area having no viable myocardium,
namely the myocardial scar, and fixed defects were detected on
stress/rest MPI. Although 2 patients presented stent restenosis on
CAG, stress/rest MPI have not shown that radionucleotide distribute
reberseibly or partly reversibly in rest state, and showed false
negative results. Therefore, the sensitivity of ATP stress
99mTc-MIBI G-MPI for detecting in-stent restonosis was
reduced in the patients with myocardial dysfunction.
In the present study, the sensitivity, specificity
and accuracy of ATP stress 99mTc-MIBI G-MPI for
evaluating stent restenosis in various arteries were as follows: In
LAD arteries, 83, 89 and 86%, respectively; in LCX arteries, 83, 81
and 82%, respectively; and in RCAs, 80, 75 and 77%, respectively.
These values were similar to those reported in the study of Elhendy
et al (20). In general, the
sensitivity, specificity, and accuracy of ATP stress
99mTc-MIBI G-MPI for evaluating coronary artery branch
restenosis were high, particularly for the LAD artery, indicating
that this technique is useful in determining the ‘culprit vessel’.
Furthermore, 99mTc-MIBI G-MPI in the present study was
less sensitive and specific in detecting RCA restenosis compared
with its detection ability in the other two coronary arteries. As
there are numerous patients with inferior wall myocardial
infarction in the current study, the inferior wall myocardial
nuclide uptake was evidently reduced, which affected the refilling
of the inferior wall myocardial nuclide distribution, leading to
reduced sensitivity for the diagnosis of RCA restenosis. In
addition, myocardial nuclide uptake was susceptible to the
attenuation effect of the surrounding tissues, such as those of the
liver and gall, due to the inferior wall. Although the present
study corrected for attenuation, the inferior wall myocardial
nuclide distribution unavoidably showed false positive results,
particularly in certain obese patients; therefore, the specificity
of 99mTc-MIBI G-MPI to detect right coronary artery
restenosis was reduced.
The current research results also demonstrated the
diagnostic sensitivity, specificity, accuracy, positive predictive
value and negative predictive value of ATP stress
99mTc-MIBI in patients with different number of diseased
arteries. In single-vessel disease patients, these values for G-MPI
were 80, 100 and 87%, respectively; similarly, these values were
91, 82 and 86%, respectively, in patients with double-vessel
disease, and 83, 91 and 86%, respectively, in patients with
triple-vessel disease. These values are higher compared with those
reported by Wei and Shi (21). Among
these values, the sensitivity for diagnosis in patients with
double- and triple-vessel disease was higher compared with that for
single-vessel disease patients; this is due to the larger number of
diseased vessels, and the greater scope and degree of myocardial
ischemia. Thus, it was not easy to form collateral circulation, and
only few false-negative results in the patients with double and
triple vessel disease were detected.
In the ATP stress test performed in the present
study, a total of 60 cases (85%) with adverse reactions were
encountered, mainly in the form of chest pain (22 cases; 31%),
stuffy chest (29 cases; 41%), dyspnea (7 cases; 10%) and
ventricular premature beats (2 cases; 3%). However, these symptoms
were mild, and therefore, ATP stress experiments were not stopped
in these patients. In addition, the patients were relieved several
minutes after the drug was discontinued, and none of them required
administration of nitroglycerin or other drugs orally, similar to
patients in previous studies (22,23). It
is, thus, clear that ATP stress 99mTc-MIBI G-MPI is safe
to use in such patients.
However, the present study presented certain
limitations. Firstly, the number of cases in the study was small,
and a higher number of cases will be analyzed in our future
research. Furthermore, the patients did not undergo stress MPI
prior to percutaneous coronary intervention; therefore, the results
before and after this procedure cannot be compared. We will focus
on this area in our future research study.
In conclusion, the present study observed that the
ATP stress 99mTc-MIBI G-MPI technique showed
characteristics of high sensitivity, specificity and accuracy, as
well as non-invasiveness and relative affordability, for the
diagnosis of stent restenosis. This method has high clinical
application value for evaluating coronary restenosis following
stent implantation.
Acknowledgements
The present study was supported by the Science and
Technology Project Plan of Liaoning, China (grant no.
2007225004-2).
References
|
1
|
Mercado N, Boersma E, Wijns W, Gersh BJ,
Morillo CA, de Valk V, van Es GA, Grobbee DE and Serruys PW:
Clinical and quantitative coronary angiographic predictors of
coronary restenosis: A comparative analysis from the
balloon-to-stent era. J Am Coll Cardiol. 38:645–652. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Albertal M, Abizaid A, Munoz JS, Mintz GS,
Abizaid AS and Feres F: A novel mechanism explaining early lumen
loss following balloon angioplasly for the treatment of in-stent
restenosis. Am J Cardiol. 95:751–755. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Singh M, Gersh BJ, MeClelland RL, Ho KK,
Willerson JT and Penny WF: Clinical and angiographic predictors of
restenosis after percutaneous coronary intervention. Circulation.
109:2727–2731. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Veselka J, Cadova P, Tomasov P, Theodor A
and Zemanek D: Dual-source CT angiography for detection and
quantification of in-stent restenosis in the left main coronary
artery: comparison with intracoronary ultrasound and coronary
angiography. J Invasive Cardiol. 23:460–464. 2011.PubMed/NCBI
|
|
5
|
Dowsley T, Al-Mallah M, Ananthasubramaniam
K, Dwivedi G, McArdle B and Chow BJ: The role of noninvasive
imaging in coronary artery disease detection, prognosis, and
clinical decision making. Can J Cardiol. 29:285–296. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Uebleis C, Hellweger S, Laubender RP,
Becker A, Sohn HY, Lehner S, Haug A, Bartenstein P, Cumming P, Van
Kriekinge SD, et al: Left ventricular dyssynchrony assessed by
gated SPECT phase analysis is an independent predictor of death in
patients with advanced coronary artery disease and reduced left
ventricular function not undergoing cardiac resynchronization
therapy. Eur J Nucl Med Mol Imaging. 39:1561–1569. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Akalin EN, Yaylali O, Kıraç FS, Yüksel D
and Kılıç M: The role of myocardial perfusion gated SPECT study in
women with coronary artery disease: A correlative study. Mol
Imaging Radionucl Ther. 21:69–74. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Shaw LJ, Hendel R, Borges-Neto S, Lauer
MS, Alazraki N, Burnette J, Krawczynska E, Cerqueira M and Maddahi
J: Myoview Multicenter Registry: Prognostic value of normal
exercise and adenosine triphosphate (99m) Tc-tetrofosmin-SPECT
imaging: Results from the multicenter registry of 4,728 patients. J
Nucl Med. 44:134–139. 2003.PubMed/NCBI
|
|
9
|
Wang LJ, Li XJ, Sun YX, Li N and Li YM:
The clinical value of adenosine stress 99mTc-MIBI gated
myocardial perfusion imaging in diagnosis of coronary artery
disease. Zhong Guo Xun Huan Za Zhi. 26:170–173. 2011.(In
Chinese).
|
|
10
|
Karpova IE, Samoĭlenko LE, Soboleva GN,
Sergienko VB, Karpov IuA, Chernysheva IE and Ioseliani DG:
Adenosine triphosphate stress (99m)Tc-MIBI single-photon emission
computed tomography in the diagnosis Miocardial Iscemia in patients
with Microvascular Angina. Kardiologiia. 54:4–8. 2014.(In Russian).
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Milavetz JJ, Miller TD, Hodge DO, Holmes
DR and Gibbons RJ: Accuracy of single-photon emission computed
tomography myocardial perfusion imaging in patients with stents in
native coronary arteries. Am J Cardiol. 82:857–861. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Xu ZN, Li DF, Li JH, Feng JL and Cheng X:
The value of gated myocardial perfusion imaging for evaluating
stent restenosis after percutaneous coronary interventions. Lin
Chuang Xin Xue Guan Bing Za Zhi. 25:302–305. 2009.(In Chinese).
|
|
13
|
Coroleu SF, De Vita M, Burzotta F, Trani
C, Porto I, Niccoli G, Leone AM, Tommasino A, Talarico GP,
Schiavoni G and Crea F: Angiographic and clinical outcome of
percutaneous coronary intervention for in-stent restenosis of
bifurcated lesions. EuroIntervention. 8:701–707. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Buchler RD, Ribeiro EE, Ade P Mansur,
Smanio P, Meneghelo RS, Chalela WA, Buchpiguel CA, Buchler JR,
Bates ER and Martinez EE: Noninvasive assessment of patients
undergoing percutaneous intervention in myocardial infarction. Arq
Bras Cardiol. 95:555–562. 2010.(In English, Portuguese). View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Ohtaki Y, Chikamori T, Hida S, Tanaka H,
Igarashi Y, Hatano T, Usui Y, Miyagi M and Yamashina A: Clinical
characteristics in patients showing ischemic electrocardiographic
changes during adenosine triphosphate loading single-photon
emission computed tomography. J Cardiol. 55:370–376. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Conti A, Mariannini Y, Canuti E, Petrova
T, Innocenti F, Zanobetti M, Gallini C and Costanzo E: Nuclear scan
strategy and outcomes in chest pain patients value of stress
testing with dipyridamole or adenosine. World J Nucl Med.
13:94–101. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Chen GB, Wu H, He XJ, Huang JX, Yu D, Xu
WY and Yu H: Adenosine stress thallium-201 myocardial perfusion
imaging for detecting coronary artery disease at an early stage. J
Xray Sci Technol. 21:317–322. 2013.PubMed/NCBI
|
|
18
|
Galassi AR, Foti R, Azzarelli S, Coco G,
Condorelli G, Russo G, Musumeci S, Tamburino C and Giuffrida G:
Usefulness of exercise tomographic myocardial perfusion imaging for
detection of restenosis after coronary stent implantation. Am J
Cardiol. 85:1362–1364. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kósa I, Blasini R, Schneider-Eicke J,
Neumann FJ, Matsunari I, Neverve J, Schömig A and Schwaiger M:
Myocardial perfusion scintigraphy to evaluate patients after
coronary stent implantation. J Nucl Med. 39:1307–1311.
1998.PubMed/NCBI
|
|
20
|
Elhendy A, Schinkel AF, van Domberg RT,
Bax JJ, Valkema R and Poldermans D: Non-invasive diagnosis of in
stent stenosis by stress 99m technetium tetrofosmin myocardial
perfusion imaging. Int J Cardiovasc Imaging. 22:657–662. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Wei HY and Shi RF: The clinical value of
SPECT 99mTc-MIBI ST/RE myocardial imagings in restenosis
after percutaneous coronary angioplasty. Zhong Guo Xin Xue Guan Za
Zhi. 9:199–201. 2004.(In Chinese).
|
|
22
|
AlJaroudi WA, Alraies MC, Cerquiera MD and
Jaber WA: Safety and tolerability of regadenoson in 514 SPECT MPI
patients with and without coronary artery disease and submaximal
exercise heart rate response. Eur J Nucl Med Mol Imaging.
40:341–348. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Karamitsos TD, Arnold JR, Pegg TJ, Cheng
AS, van Gaal WJ, Francis JM, Banning AP, Neubauer S and
Selvanayagam JB: Tolerance and safety of adenosine stress perfusion
cardiovascular magnetic resonance imaging in patients with severe
coronary artery disease. Int J Cardiovasc Imaging. 25:277–283.
2009. View Article : Google Scholar : PubMed/NCBI
|