Introduction
Independent inside ankle deltoid ligament injury is
a rare type of injury (1). Most of
these injuries are associated with malleolus medialis fracture and
wither joint impairment. Among patients suffering from disability
of later shin tendon, joint fusion of ankle and ankle replacement
we can also see independent impaired deltoid ligaments (2).
There are three types of common inside ligamentous
injury mechanisms: Ankle pronation-abduction, pronation-extorsion
and supination-extorsion (3).
Patients with unstable rotation need reconstruction and there are
essentially four techniques available for reconstructing the
chronically failed deltoid ligament. These are: i) Wiltberger; ii)
Deland; iii) Kitaoka; and iv) Hintermann techniques (4). Due to the difficulty of model
construction in animal ankle, clinical research usually fails to
achieve a profound understanding on biomechanics and FEA (5).
In the present study, we applied 3-dimensional
finite elements to compare the efficiency of these techniques in
reconstructing deltoid ligament injuries of the ankle joint.
Materials and methods
Establishment of finite element
model
We enrolled a healthy male volunteer (28 years of
age, 172 cm and 65 kg) without any trauma, inflammation or cancer
for the present study. His ankle joint was examined under X-ray and
using a 64-slice dual source computed tomography (CT) (Siemens
Medical Solutions, Munich, Germany) his right ankle joint was
scanned. MRI images were entered into the medical simulation
software MIMICS 10.01 (Materialise, Leuven, Belgium). Images were
divided according to the corresponding gray threshold in the MIMICS
(the CT value of bones and soft tissue was different). After the
border reading and the marrow cavity filling, the 3D model of the
bones and cartilages of the ankle was generated. Each model was
entered into software MAGICS 9.9, which was incidental to MIMICS
software and was grid partitioned. Some irregular surface
structures were repaired and smoothed. The final step was to enter
the bone and cartilage models into the ANSYS 12.0 (Swanson Inc.,
Houston, PA, USA). Ligamentous structure was generated with the aid
of ANSYS (set unit type, real constants and material property) and
the finite element model was generated (the total number of the
overall transfer units were 48,600).
The bone surface structure of the units was
partitioned by the rigid surface. The arthroidal cartilages were
partitioned by the transformable 3D-tetrahedron. Ligament structure
was simulated by bar unit which was tensioned only when the start
and endpoints were confirmed according to the anatomy and CT image.
Different ligaments were simulated by a different amount of bar
units according to its length-width ratio. Articular cartilage was
set to be the isotropic linear elastic material (E=0.7 MPa, ν=0.49)
and the simulation of the ligament around the ankle was defined by
the following formula: F=A(eB*ε-1) and parameters A and B, where F
referred to ligament stress, ε was ligament strain and the
parameter of ligament in the joint below was the same as the data
for posterior talotibial ligament. The tendon transplantation was
isotropic linear elastic material and the reconstruction needed
four types of tendons: i) Posterior tibial; ii) plantaris; iii)
peroneus longus; and iv) tendon of extensor pollicis longus. The
initial cross-sectional area in each tendon was 48, 1.4, 37 and
2.91 mm2, respectively, and the elasticity modulus was
2,076, 1,172, 2,769 and 450 MPa, respectively.
Model-verified test
The model was carried out with anterior drawer test
(ADT): We applied 50–150 N front draw force to the root bone, the
flexion angle of the ankle joint was plantar flexion 20° to dorsal
flexure 20°. We calculated the predicted moving distance of talus.
When the number of transfer units was more than 46,000, the rate of
convergence was below 0.45%.
The sensitivity test applied to the material data of
the anterior talofibular ligament was as follows: The original
parameters of the anterior talofibular ligament in the model were
A=7.18 and B=12.50. We immobilized B to 12.50 at first and then A
was changed by 0.1 A each time (6.4, 7.1, 7.9 and 8.6) while
calculation of the change in the maximum forward displacement of
talus was 0.5 mm. While forward tension was 150 N, we kept A
unchanged and changed B by 0.1 B each time (11.2, 12.5, 15 and
16.2). Forward displacement of talus was changed by 1.0 mm at the
most (forward tension was 150 N). To further confirm the effect of
the ligament pretension on the model, the ligament pretension of
anterior talofibular ligament was adjusted to 110% and forward
displacement of talus decreased by 22% under the tension of 150 N.
When adjusted to 90%, the forward displacement of talus increased
by 42% under the same tension.
Test method and observational
index
The test was carried out in two steps: i) Talus and
root bone were fixed and flexion angle of tibiofibula bucking was
set at −20°, −10°, 0°, 10° and 20°; and ii) we fixed the
tibiofibular and exerted extorsion or eversion torque to the root
bone and the extorsion and eversion torque were set to 1.7 and 3.4
nm. Initial stress of the ligament and tendon in the neutral
position was 0. The root bone was allowed to have degrees of
freedom in five directions (forward-backward translation,
medial-lateral translation, near-far translation,
intorsion-extorsion and inversion-eversion). When the model was
operational, we intercepted the horizontal view to calculate the
extorsion angle of the talus. We intercepted the anteroposterior
view to calculate the eversion angle of the talus and each angle
was tested three times by three investigators and the average
values were calculated.
Statistical analysis
SPSS 19.0 statistical software (Chicago, IL, USA)
was used for statistical analysis and data were expressed as mean ±
standard deviation. Comparison between groups was done with single
factor ANOVA analysis. The enumeration data were expressed as a
percentage. The comparison between groups was conducted using
χ2 test. P<0.05 was considered to indicate a
statistically significant difference.
Results
Test model
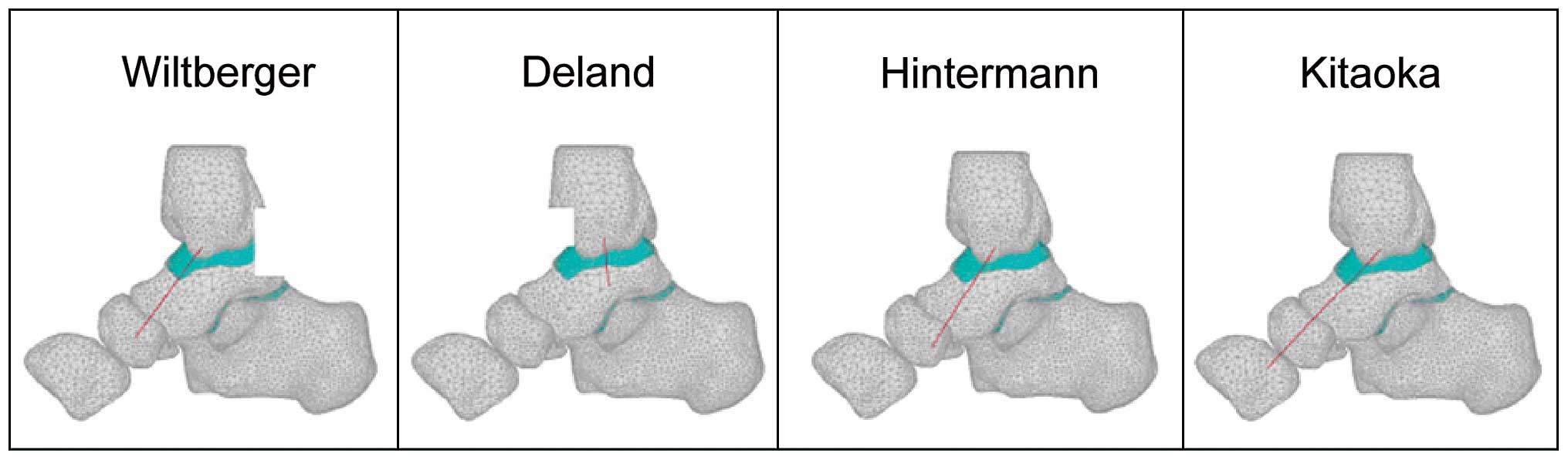
Ankle deltoid ligament 3-dimensional finite element
model (Fig. 1) and 27 link units
were used to simulate the ligament structure. Complete injury of
deltoid ligament model eradicated all deltoid ligaments from the
model. The Wiltberger reconstruction model vertically cut the
tendon. The near-end of tendon was connected to malleolus medialis
while the far-end was connected to the nut bone. The Deland
reconstruction model connected the near end of the transplanted
peroneus longus tendon to malleolus medialis while the far-end
connected to the medial cuneiform bone. Hintermann reconstruction
model connected the far-end of transplanted plantaris tendon to
tubercle of the nut bone while the near end was connected to
malleolus medialis. Kitaoka connected the near end of transplanted
hallucis longus tendon to malleolus medialis while the far end
connected to entocuneiform (Fig.
2).
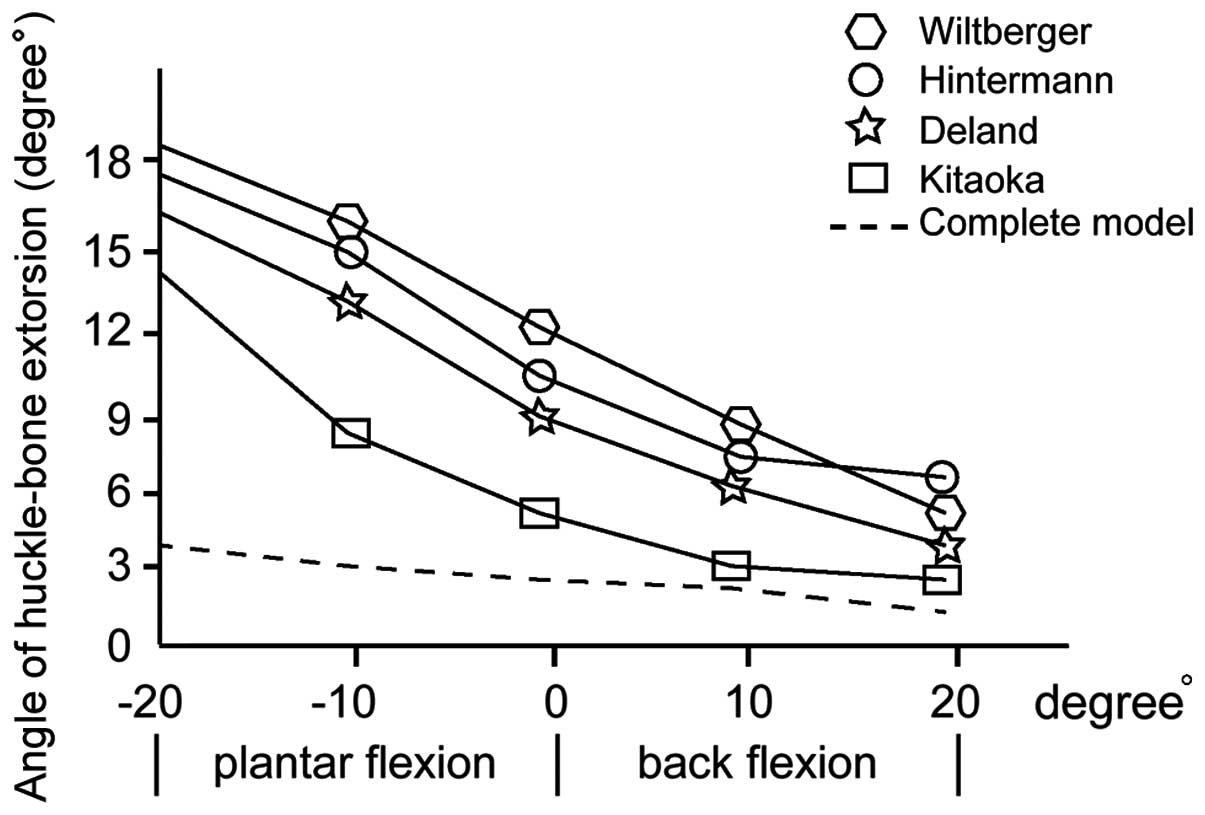
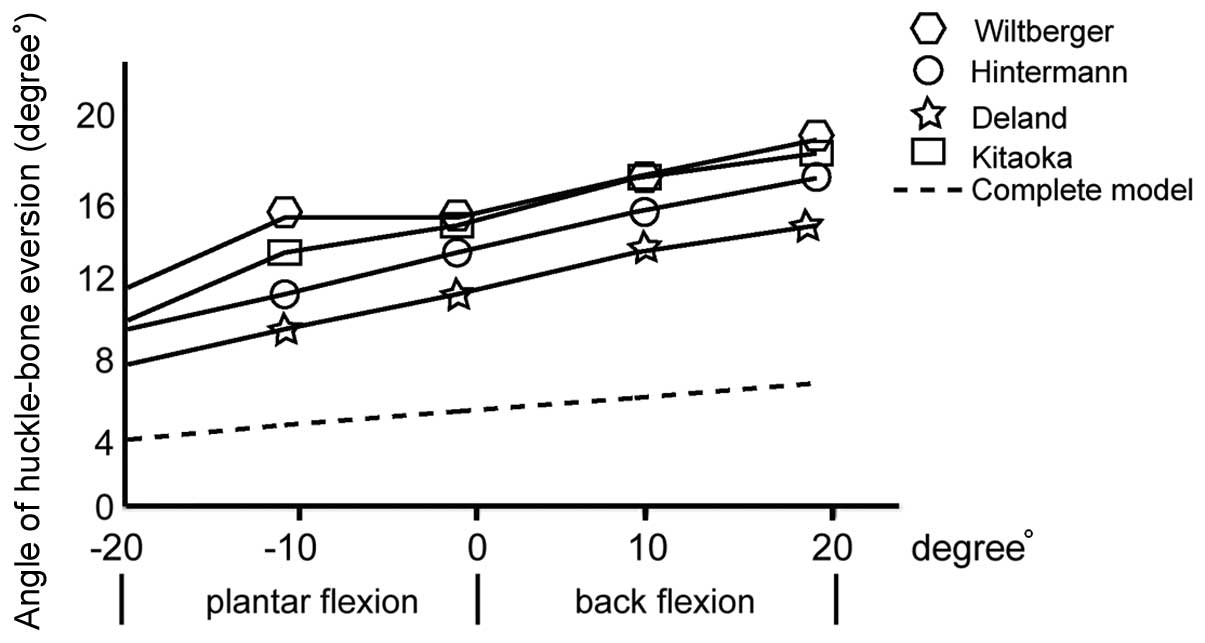
Angle of huckle-bone extorsion and
eversion
In the course of bending, from plantar flexion 20°
to back flexion 20°, the extortion of talus decreased while the
eversion increased. In the complete model of deltoid ligamentis in
neutral position the average angle of huckle-bone extorsion was
3.6±0.7° and the eversion angle was 4.2±0.5°. All four
reconstruction models failed to fix the impaired ankle completely
and there was an obvious increase in extortion and ectropion.
Kitaoka helped to decrease the extortion angle more than the other
three techniques and the difference had statistical significance
(P<0.05). No statistically significant differences were found in
the case of ectropion (Figs. 3 and
4).
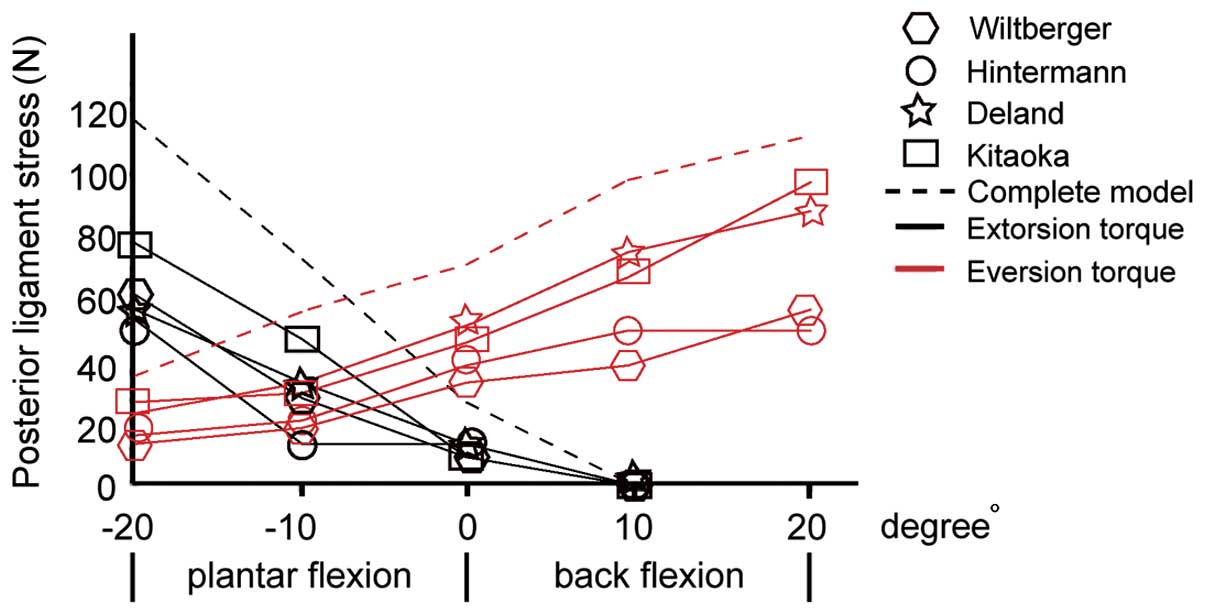
Ligament stress analysis of the
reconstruction model
The lateral ligament stress of four models was
different from the normal one. When ankle was imposed with
extortion moment of force, stress of anterior talofibular ligament
with Kitaoka reconstruction method was close to that of the
complete deltoid ligament. When ankle was imposed with eversion
moment of force, stress of anterior talofibular ligament with
Kitaoka and Deland reconstruction methods were close to that of the
complete deltoid ligament (Fig.
5).
Discussion
Wiltberger techniques mainly reconstruct the shin
ligament in the fascia colli superficialis of deltoid ligament
instead of ligament of shin heel, anterior tibial ligament and
posterior tibial ligament by means of transplanting the shin back
ligament. The entheses of ligamenta tibionavicular are medial
malleolus and tuberositas ossis navicularis, from upper back to
down front. When the ankle extorts, the displacement of the nut
bone is obviously larger than the huckle-bone. Ligamenta
tibionaviculare is passively extended then generates obvious force
against extortion which maintains the stability of the ankle
extortion. Both front and back ligaments play a crucial role in
maintaining the stability of the ankle extortion. Therefore,
Wiltberger can just partly recover the stability of ankle extortion
(6). Hintermann mainly reconstructed
shin ligament by transplanting plantaris muscle tendon instead of
ligament of shin heel, anterior tibial ligament and posterior
tibial ligament. The main difference between these techniques is
not in the treatment results, but in the material used and the
error occurs during the process (7).
As for the Deland techniques, its entheses are the inside ankle and
calcaneus. Line feed is roughly the same as long axis of the body.
When the ankle extorts outward, the displacement of calcaneus is
obviously larger than that of the huckle-bone. Ligament of shin
heel is passively extended then generates obvious force against
eversion which maintains the stability of the ankle eversion.
However, the extortion circumference ratio of calcaneus is smaller
than that of huckle-bone and its displacement is also smaller than
that of the huckle-bone. Moreover, shin and ligament are in
vertical position against each other which implies that Deland
technique performs poorly against the ankle extortion (8). Kitaoka mainly reconstructed the shin
ligament of deltoid ligament instead of ligament of shin heel,
front and back by means of transplanting the hallux longus tendon.
Compared with the Wiltberger and Hintermann techniques, the main
difference is in its starting point and terminal point,
respectively, the inside ankle and the inside entocuneifor. When
the ankle extorts, the circumference of entocuneiform is obviously
larger than that of the huckle-bone and nut bone. Hence, Kitaoka
techniques can generate significant moment against extortion and
maintain the stability of the ankle extortion, but cannot recover
the impaired ankle completely (9).
By constructing a 3-dimensional finite element model
of normal ankle and analyzing the impairment reconstruction, we
realized that all four techniques failed to fully recover the
impaired ankle. These techniques could only reconstruct a part of
the ligaments which could be useful to maintain the stability of
extortion and eversion. Kitaoka technique obviously decreased the
extortion angle which was related to Kitaoka's enthesis (10). As for eversion angle, there was no
distinct difference among the four techniques. Our results revealed
that Deland technique performed much better in terms of stability
of eversion and this was because of the structure of the model
(11). A few strategies were
adopted: i) The material of ligament, bone structure and
cartilaginous were mostly referred to pertinent literature
therefore there may be a rather large bias (12); ii) the ligament material
characteristic was defined as nonlinearity superelasticity
(13); and iii) ankle joint was
being fixed, but during the process of eversion, the movement of
ankle joint was crucial (14). The
stress of lateral ligament in the four techniques was different
from the normal one. When the ankle was forced by extortion, the
stress of anterior talofibular ligament was close to that of a
complete one, and when the ankle was forced by eversion, the stress
of posterior talofibular ligament was close to that of a complete
one.
In conclusion, Kitaoka and Deland techniques
performed better in impaired ankle deltoid ligament and could
largely recover its biomechanical characteristics. However, further
verification with larger clinical samples and control are
needed.
References
|
1
|
Warner SJ, Garner MR, Hinds RM, Helfet DL
and Lorich DG: Correlation between the Lauge-Hansen classification
and ligament injuries in ankle fractures. J Orthop Trauma.
29:574–578. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jung HG, Park JT, Eom JS, Jung MG and Lee
DO: Reconstruction of superficial deltoid ligaments with allograft
tendons in medial ankle instability: a technical report. Injury.
47:780–783. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wang H, Gu Z, Liu Y, Xu J, Jan J, Zhang J
and Peng C: Effectiveness of surgery in treatment of ankle
fractrures associated with deltoid ligament injury. Zhongguo Xiu Fu
Chong Jian Wai Ke Za Zhi. 29:416–419. 2015.(In Chinese). PubMed/NCBI
|
|
4
|
Deland JT, de Asla RJ and Segal A:
Reconstruction of the chronically failed deltoid ligament: a new
technique. Foot Ankle Int. 25:795–799. 2004.PubMed/NCBI
|
|
5
|
Xu C, Zhang MY, Lei GH, Zhang C, Gao SG,
Ting W and Li KH: Biomechanical evaluation of tenodesis
reconstruction in ankle with deltoid ligament deficiency: a finite
element analysis. Knee Surg Sports Traumatol Arthrosc.
20:1854–1862. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Clanton TO, Williams BT, James EW,
Campbell KJ, Rasmussen MT, Haytmanek CT, Wijdicks CA and LaPrade
RF: Radiographic identification of the deltoid ligament complex of
the medial ankle. Am J Sports Med. 43:2753–2762. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hintermann B, Valderrabano V and Kundert
HP: Lengthening of the lateral column and reconstruction of the
medial soft tissue for treatment of acquired flatfoot deformity
associated with insufficiency of the posterior tibial tendon. Foot
Ankle Int. 20:622–629. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Chun KY, Choi YS, Lee SH, Kim JS, Young
KW, Jeong MS and Kim DJ: Deltoid ligament and tibiofibular
syndesmosis injury in chronic lateral ankle instability: magnetic
resonance imaging evaluation at 3T and comparison with arthroscopy.
Korean J Radiol. 16:1096–1103. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kitaoka HB, Luo ZP and An KN:
Reconstruction operations for acquired flatfoot: biomechanical
evaluation. Foot Ankle Int. 19:203–207. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Schottel PC, Baxter J, Gilbert S, Garner
MR and Lorich DG: Anatomic ligament repair restores ankle and
syndesmotic rotational stability as much as syndesmotic screw
fixation. J Orthop Trauma. 30:e36–e40. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hogan MV, Dare DM and Deland JT: Is
deltoid and lateral ligament reconstruction necessary in varus and
valgus ankle osteoarthritis, and how should these procedures be
performed? Foot Ankle Clin. 18:517–527. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Perrier A, Bucki M, Luboz V, Vuillerme N
and Payan Y: 3D musculoskeletal finite element analysis of the foot
kinematics under muscle activation with and without ankle
arthrodesis. Comput Methods Biomech Biomed Engin. 14:1–2. 2015.
View Article : Google Scholar
|
|
13
|
Liu Q, Zhao G, Yu B, Ma J, Li Z and Zhang
K: Effects of inferior tibiofibular syndesmosis injury and screw
stabilization on motion of the ankle: a finite element study. Knee
Surg Sports Traumatol Arthrosc. 24:1228–1235. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jay Elliot B, Gundapaneni D and Goswami T:
Finite element analysis of stress and wear characterization in
total ankle replacements. J Mech Behav Biomed Mater. 34:134–145.
2014. View Article : Google Scholar : PubMed/NCBI
|