Introduction
Endoscopic transforaminal nucleotomy with
foraminoplasty is an accepted procedure for the treatment of lumbar
intervertebral disc herniation, and is associated with
substantially reduced surgical trauma compared to the usual dorsal
approach (1). In addition, positive
outcomes have previously been reported. This technique has the
notable advantages of i) low invasive approach, ii) lower muscle
manipulation iii) postoperative back pain reduction and fibrosis
and iv) direct observation of decompressed root (2). A previous Swedish study also found that
endoscopic transforaminal nucleotomy with foraminoplasty had a
significant better result in visual analog scale (VAS) back and leg
pain, walking distance and patient satisfaction (3). Kim et al (4) concluded that this may be effective
surgical method in unilateral adjacent 2 levels lumbar disc
herniation through 1 skin portal incision and Choi et al
(5) also claimed that XMR-assisted
endoscopic transforaminal nucleotomy with foraminoplasty is able to
provide a precise skin entry site (5). Knight et al (6) also demonstrated that this intervention
is able to improve symptoms and function that were still sustained
10 years later in a prospective study. Based on these positive
outcomes (2–7), in January 2009, we began performing
endoscopic transforaminal nucleotomy with foraminoplasty, and the
observations indicated that lumbar disc herniations can be
categorized into three pathological types, which are different than
those described based on imaging analysis (8). While imaging analysis can identify the
location of the herniation and help guide disc removal, it is
believed that surgical treatment based on the three pathological
types identified can result in improved surgical outcomes because
surgery based on the pathological type better addresses the cause
of the symptoms. In 2011 we began performing endoscopic
transforaminal nucleotomy with foraminoplasty based on the three
pathological types identified.
Thus, the aim of the present study was to describe
the three specific pathological types among herniated discs and to
determine whether a treatment tailored specifically to the
pathological type present improves patient outcomes.
Materials and methods
Patients
The records of patients who received endoscopic
transforaminal nucleotomy with foraminoplasty for symptomatic
lumbar disc herniation between 2009 and 2013 at the Third Hospital
of Beijing Armed Police Force (Beijing, China) were retrospectively
reviewed. Patients were divided into two groups. Group A included
patients who received conventional endoscopic transforaminal
nucleotomy with foraminoplasty for removal of herniated disc
material and received surgery between 2009 and 2011. Group B
consisted of patients who received ‘targeted’ endoscopic
transforaminal nucleotomy with foraminoplasty based on the
pathological type identified at surgery. These patients received
surgery between 2011 and 2013, and patient characteristics are
presented in Table I.
 | Table I.Patient demographic data. |
Table I.
Patient demographic data.
| Characteristics | Group A (n=275) | Group B(n=316) |
|---|
| Age (years) | 46.8±7.3 | 50.2±8.6 |
| Gender
(female/male) | 147/128 | 180/136 |
| Body mass index | 22.4±3.1 | 22.7±3.3 |
| Symptom duration
(n) |
|
|
| Acute
pain within the past 2 months | 60 | 75 |
|
Recurrence within the past 2
months | 75 | 85 |
| Longer
than 2 months | 140 | 156 |
| Operated segments
(n) |
|
|
| L2/3 | 7 | 10 |
| L3/4 | 13 | 16 |
| L4/5 | 123 | 133 |
| L5/6
(lumbarization of S1) | 5 | 8 |
|
L5/S1 | 127 | 149 |
| Previous invasive
therapy (n) | 70 | 81 |
Lumbar disc herniation was diagnosed based on
symptoms and signs, laboratory examination, magnetic resonance
imaging (MRI) and/or computed tomography (CT) data. The affected
nerve root was determined according to the paraesthesia
distribution, decreased muscle power and reduced tendon reflexes.
Moreover, in order to be eligible for surgery patients should have
failed a 4–6 week course of conventional conservative therapy.
Patients with asymptomatic disc herniation were not eligible for
surgery. If symptoms and signs were typical of disc herniation,
surgery was performed even if the MRI or CT observations were
negative because the herniated nucleus pulposus may return to the
intervertebral space when a patient is placed in supine during MRI
or CT examination. In addition, patients with a multilevel disease
were excluded. The Institutional Review Board of the Third Hospital
of Beijing Armed Police Force approved the present study, and
because of its retrospective nature the requirement of patient
informed consent was waived.
Surgical techniques
Surgeries were conducted with the transforaminal
endoscopic surgical system (TESSYS) (9,10), and
conventional transforaminal endoscopic discectomy was performed as
described by Schubert and Hoogland (2). The usual access for disease at L5/S1
and L4/5 was 12–14 cm lateral to the midline, and for L3/4 and L2/3
~10 cm lateral to the midline. Both nerve root and dorsal root
ganglion are primarily located in the upper 1/3 of the foramen.
Bone was removed by drilling after reaching the superior articular
process of the lower vertebra to expand the foramen when necessary.
During drilling the end of the working cannula was placed in the
midline on anteroposterior radiograph, while it was located in the
posterosuperior margin of the lower vertebra on lateral radiograph.
Following placement of the working channel, the nerve root was
observed and nerve injury was avoided by direct manipulation.
Extreme care was taken to avoid blood vessels in the foramen. A
proper perfusion pressure was maintained, and a radiofrequency
ablation system was used to provide hemostasis at the root of
bleeding blood vessels.
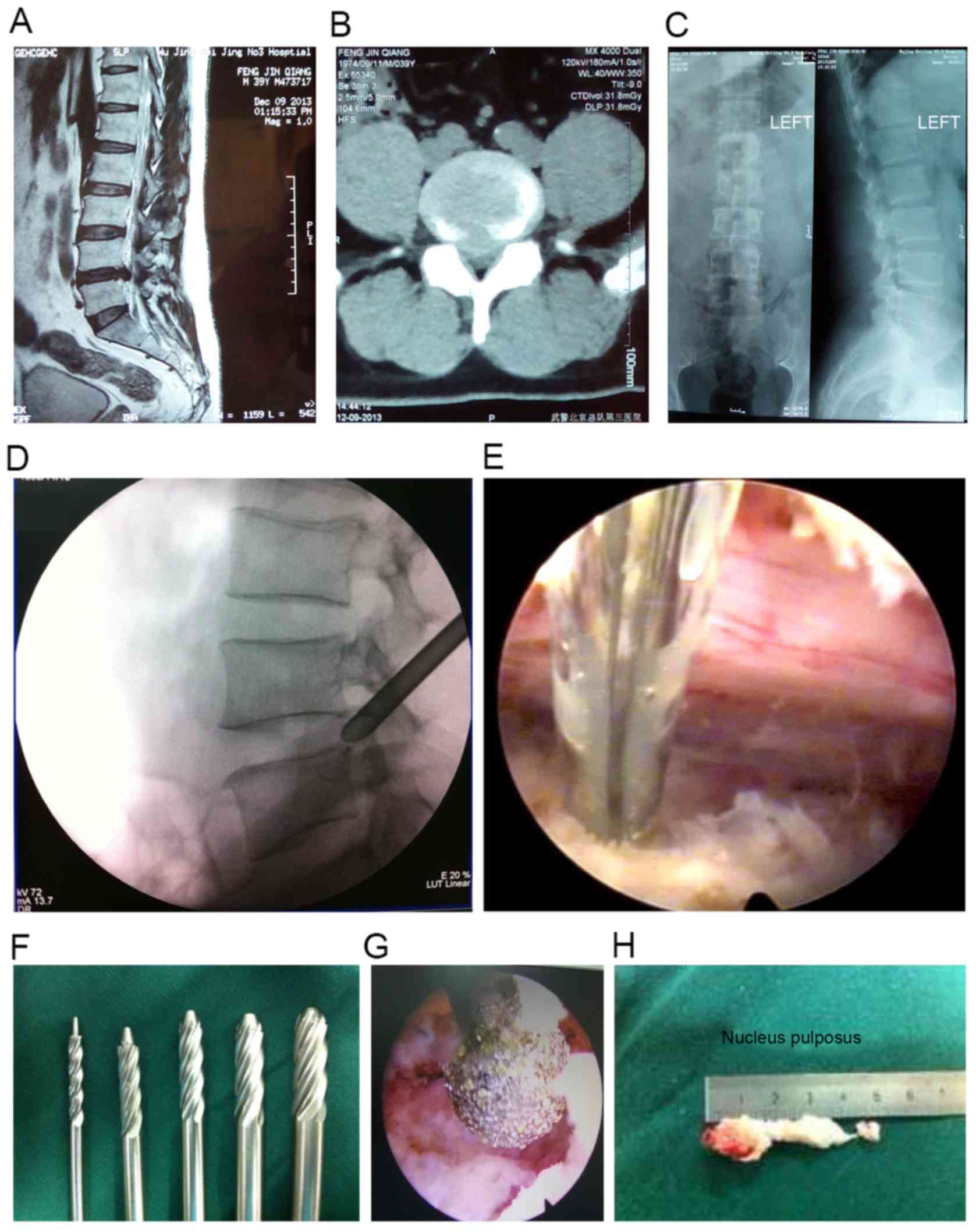
In the conventional procedure, the herniated nucleus
pulposus was removed through the working channel, and the annulus
fibrous was not cut. If no nerve root was observed, the ligamentum
flavum was identified and dissected using a radiofrequency probe to
expose the nerve root. Since application of a ring saw for removing
bone in the articular process may increase the incidence of nerve
root injury, a spiral bone drill with a nerve protection device in
front of the head was used. Representative preoperative and
intraoperative images, surgical specimen and the surgical route are
shown in Fig. 1.
In targeted therapy access to the canal was the same
as in the conventional procedure. However, the ultimate surgical
procedure was based on pathological observations identified at
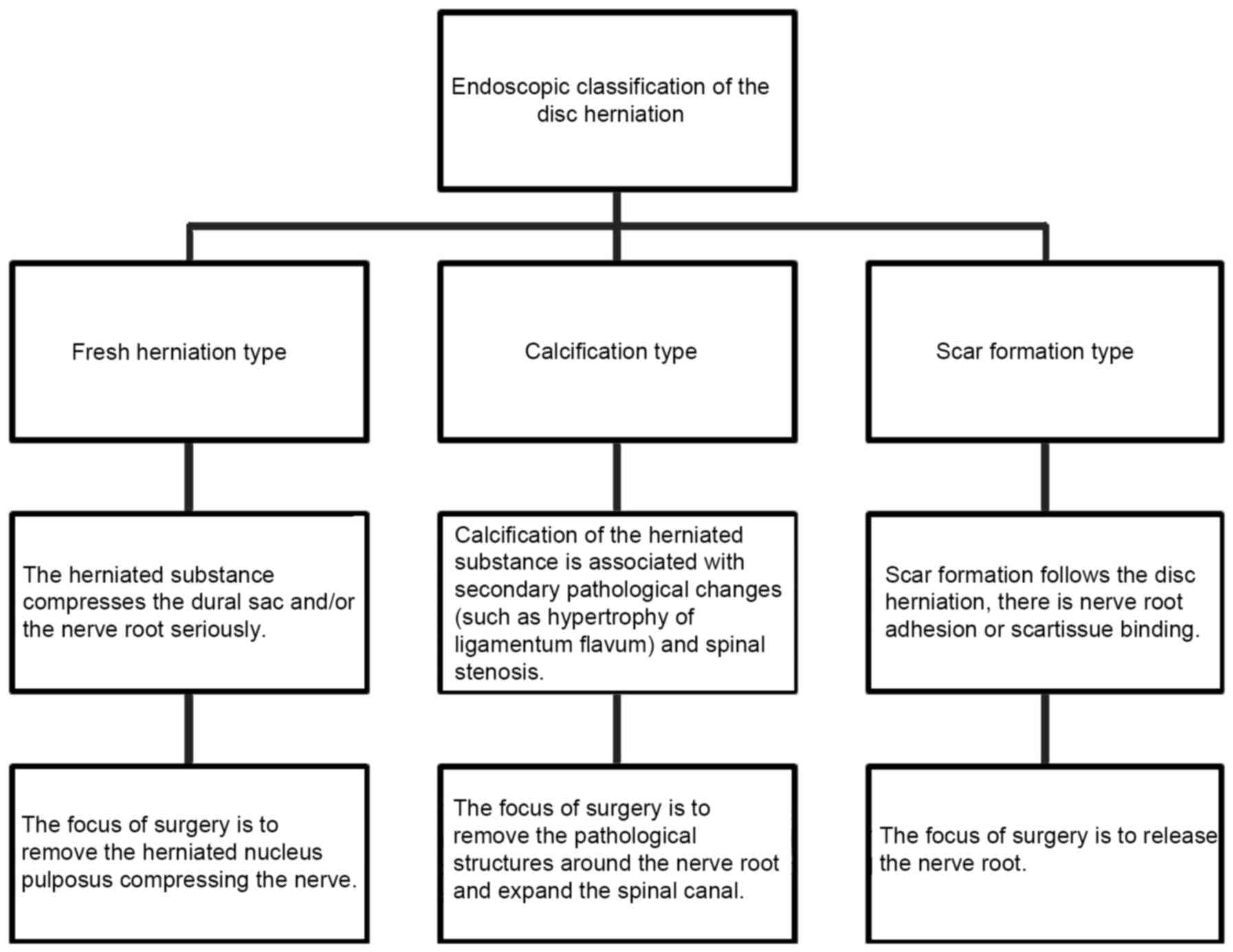
surgery. Pathological observations were categorized as fresh,
calcified and scar type disc herniation. Fresh was characterized as
annulus rupture with the nucleus pulposus protruding into the
spinal canal compressing the dural sac and/or nerve root. In this
case, the target of therapy was removing the herniated disc
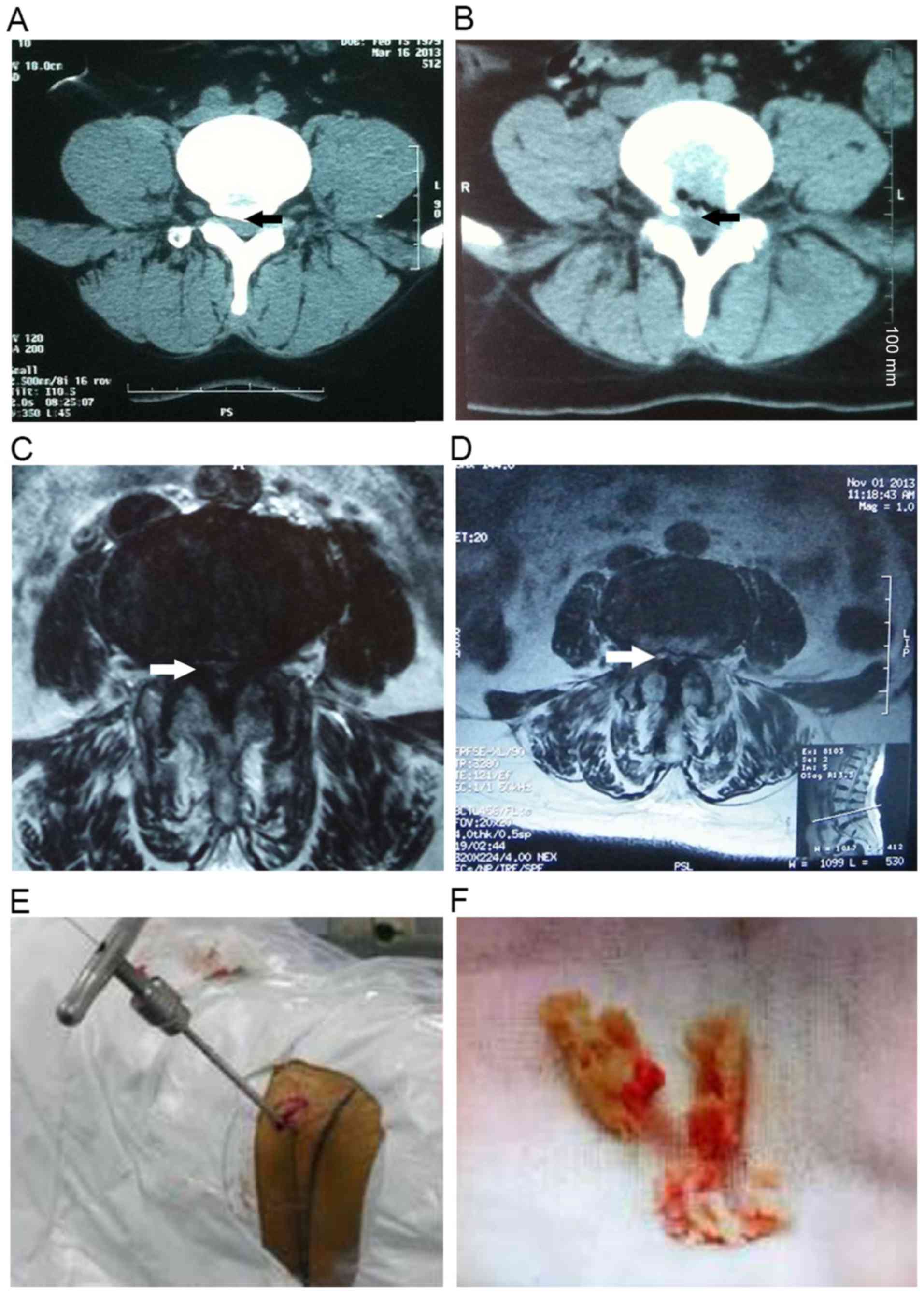
material. Calcified was characterized by calcification of herniated
material that may or may not be compressing the dural sac and/or
nerve root. Other pathological changes, including ossification of
the posterior longitudinal ligament, hypertrophy of the ligamentum
flavum, subchondral bone sclerosis and lateral recess stenosis may
also be present. The calcified disc material, calcified posterior
longitudinal ligament, thickened ligamentum flavum and subchondral
bone scleroses are the targets. The volume of the spinal canal was
expanded to restore the blood supply to the nerve root, and the
nerve root was mobilized so that it moves smoothly when performing
the straight leg raise test. An endoscopic drill bit, which has a
relatively thin diameter, was used to remove the calcified
material, which is different from the spiral drill bits used when
placing the working channel to expand the foramen. The scar type
was characterized as scar tissue inside the annulus fibrosus and/or
surrounding the nerve root without the presence of herniated disc
material. The goal of therapy was to remove the scar tissue such
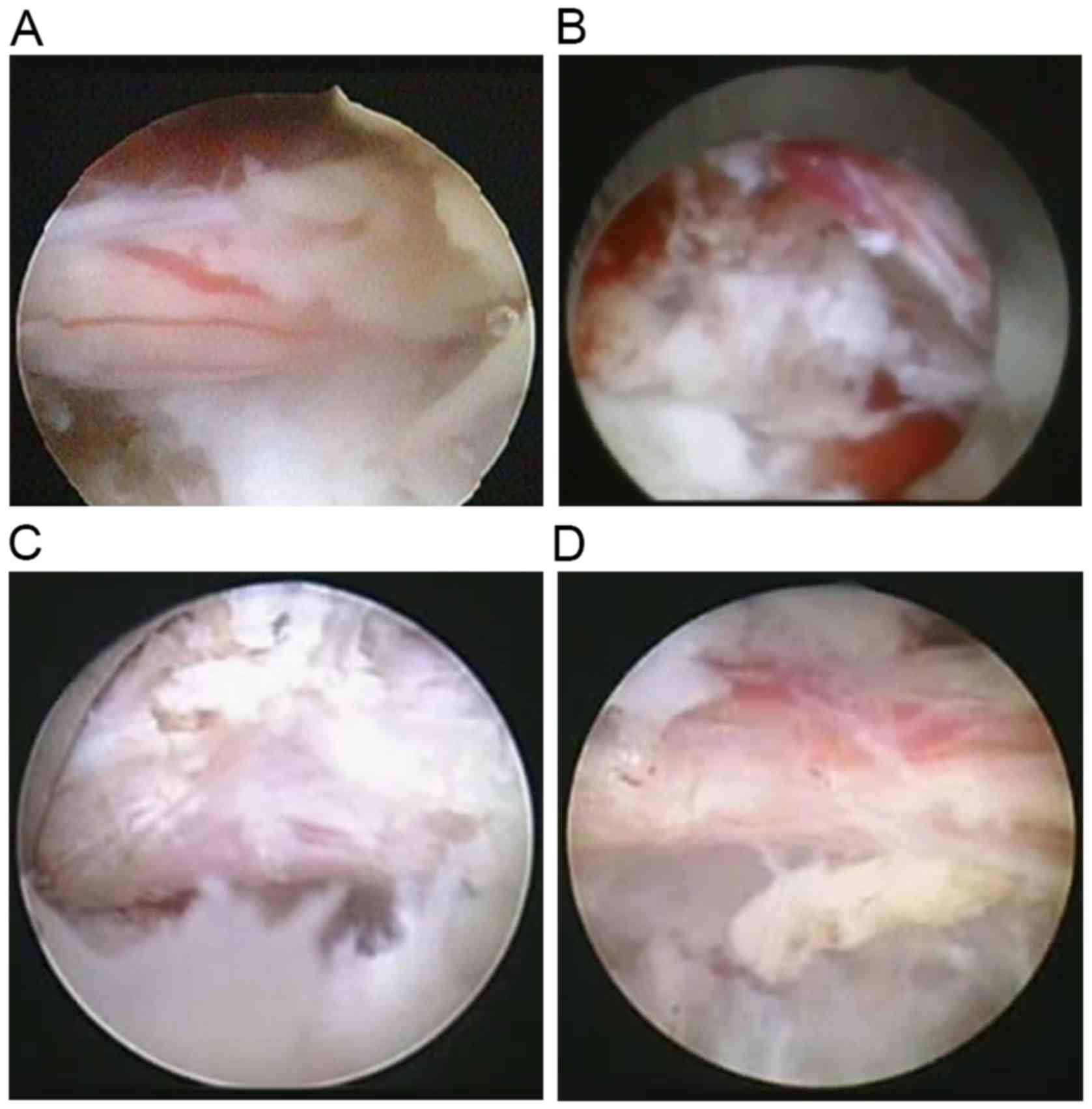
that the nerve root can move freely. A description of the three
pathological classifications is shown in Fig. 2, the surgical goals are summarized in
Fig. 3, and representative
intraoperative images targeted therapy cases are shown in Fig. 4.
Follow-up and evaluation
All patients were followed-up every three months for
a minimum of 18 months. Back and leg pain VAS (11) scores with 1 indicating minimal pain,
and 10 indicating intense pain and Oswestry Disability Index (ODI)
(12,13) scores were determined preoperatively
and at each follow-up visit. The Macnab criteria (14) were also used to classify the
outcomes.
Pathological classification and
reliability
Video recordings were made of all operations and
reviewed by a board-certified spine endoscopy surgeon for
observation of the nucleus pulposus, rupture of the annulus
fibrosus, spinal ligamentum flavum ossification, posterior
longitudinal ligament calcification, scar tissue on the nerve root
sheath surface, blood circulation of the nerve root and thecal sac,
osteophyte in the posterior body edges of lumbar vertebrae, and
lateral recess stenosis. Each case was classified into one of three
pathological classifications: Fresh herniation, calcified and
scar.
To determine the reliability of the pathological
classifications, videos of 100 operations were selected randomly.
Two examiners assessed each video, and assigned each video to one
classification. For all video assessments, the examiner was masked
regarding patient data. This process was repeated two weeks later
by the same two examiners. Intra-rater and inter-rater reliability
of video group assignment was determined by calculating a Kappa
coefficient (κ).
Histopathological staining
Surgical specimens were fixed in 10% formalin,
embedded in paraffin, cut into 6-µm slices, stained with
hematoxylin-eosin and viewed under a light microscope (N-800M;
Medical Instruments Co., Ltd., Jinan, China).
Statistical analysis
Data were presented by the mean ± standard deviation
for continuous variables, while the number and percentage were
reported for categorical variables. To identify potential
predictors of each type of disc herniation, three logistic
regression models were performed using the forward stepwise method.
The initial model included age, gender, body mass index (BMI),
symptom duration, operated segment, previous invasive therapy and
endoscopic pathological type. A value of P<0.10 was applied to
enter variables into the final model. Odds ratios (ORs) and 95%
confidence intervals (CIs) were also calculated. To examine the
differences in change of surgical outcomes between two groups,
Student's t-test was used for VAS pain and ODI scores, and
χ2 test or Fisher's exact test was used for the Macnab
criteria. All statistical analyses were conducted using SPSS
software version 19.0 (IBM SPSS, Armonk, NY, USA). P<0.05 was
used to indicate a statistically significant difference.
Results
Participants
A total of 591 patients (327 females and 264 males)
with a mean age of 48.45 years were included. Of the 591 patients,
135 (22.8%) had acute pain (i.e., first episode of back/leg pain
within the past two months), 160 (27.1%) had a recurrence of
previous symptoms within the past two months, and 296 (50.1%)
reported symptoms of longer than two months. There were 275
patients in group A and 316 in group B. Moreover, there were no
significant differences in age, gender, BMI, symptom duration,
operated segments or previous invasive therapy between the two
groups. The patient demographic data are summarized in Table I.
Surgery was only performed for patients who were
definitely diagnosed with lumbar disc herniation by symptoms or
imaging findings and did not respond to the regular conservative
treatment. This population accounted for only a small portion
(~10%) of those diagnosed with lumbar disc herniation during the
study period, and an operation was performed on only one segment
for every patient. In the majority, but not all patients, the
annulus was ruptured. A total of 17 patients were operated at
segment L2/3, 29 at L3/4, 256 at L4/5, 13 at L5/6 (lumbarization of
S1) and 276 at L5/S1. Among the 591 patients, 151 (25.5%) had
undergone previous invasive therapies, including open surgery and
percutaneous ablative techniques on the same segment.
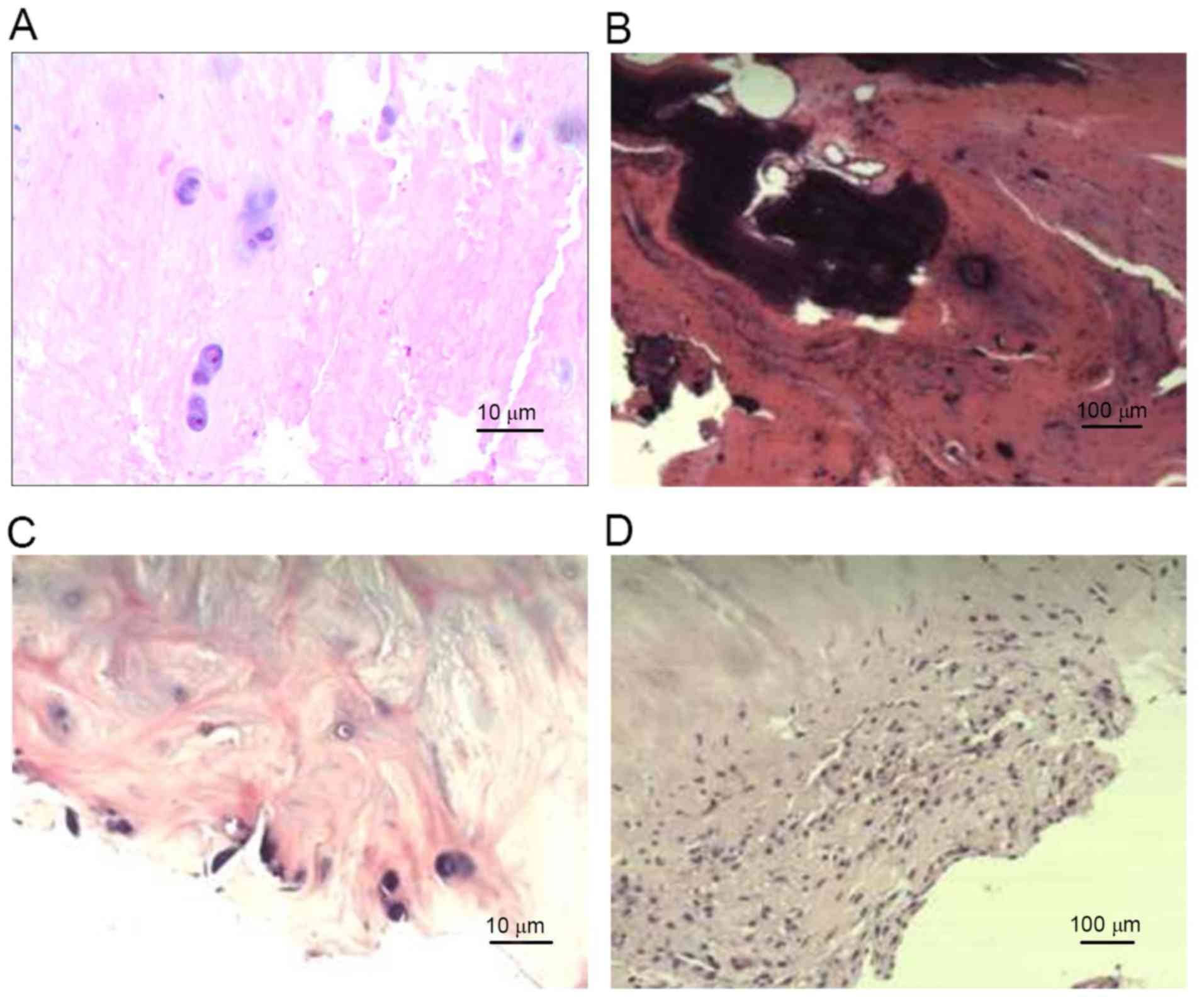
Pathological classifications
Review of the operative videos revealed that there
were 186 cases of fresh type, 313 of calcified type and 92 of scar
type. Representative histopathological images of the three types
are shown in Fig. 5. In the fresh
type, the nucleus pulposus had shrunk, the stroma had decreased and
increased numbers of disordered collagen fibers and cell necrosis
were noted. In the calcified type, red staining calcifications in
the ruptured annulus fibrosus were noted, and chondrocytes could
seldomly be observed. In the scar type, proliferation of
capillaries and inflammatory cell infiltration in tissue removed
from the surface of the nerve sheath was noted. The agreement
between histological and surgical observations for fresh, calcified
and scar type specimens were 92.3, 96.8 and 72.4%,
respectively.
Reliability of pathological
classifications and associations with patient characteristics
The intra-rater reliability Kappa coefficient for
classifying patients into one of the three types was 0.82 for
examiner 1 and 0.78 for examiner 2. The inter-rater reliability
Kappa coefficient for the classification was 0.76 for the first
comparison and 0.77 for the second comparison (Table II). In addition, the results of the
multiple logistic regression analysis are summarized in Table III. The most predictive observation
of the calcified type was an age >40 years (OR=2.32; 95% CI:
1.31–4.02, P=0.002), followed by a longer symptom duration
(OR=2.17; 95% CI: 1.05–3.54, P=0.015). Moreover, previous invasive
therapy was most predictive of the scar type (OR=2.98; 95% CI:
1.43–4.68, P=0.008).
| Table II.Reliability of the transforaminal
endoscopic pathological classification. |
Table II.
Reliability of the transforaminal
endoscopic pathological classification.
| Variable | Kappa (SE) | 95% CI |
|---|
| Intra-rater
reliability |
|
|
| Examiner
1 | 0.82 (0.04) | 0.72–0.72 |
| Examiner
2 | 0.78 (0.05) | 0.69–0.69 |
| Inter-rater
reliability |
|
|
|
Comparison 1 | 0.76 (0.06) | 0.67–0.67 |
|
Comparison 2 | 0.77 (0.05) | 0.69–0.69 |
| Table III.Multiple logistic regression
analysis. |
Table III.
Multiple logistic regression
analysis.
| Disc herniation
classification | Predictors | Odds ratio | 95% CI | P-value |
|---|
| Fresh | Age <40 years | 1.52 | 1.03–2.03 | 0.056 |
|
| Symptoms <2
months | 1.65 | 1.06–2.06 | 0.043 |
| Calcified | Age >40 years | 2.32 | 1.31–4.31 | 0.002 |
|
| Symptoms >2
months | 2.17 | 1.05–3.05 | 0.015 |
| Scar | Symptoms >2
months | 1.95 | 1.01–3.01 | 0.011 |
|
| Previous invasive
therapy | 2.98 | 1.43–4.43 | 0.008 |
Clinical outcomes
Evaluation of VAS pain and ODI scores revealed that
patients in group B had a greater improvement in symptoms than
those in group A (all, P<0.05) (Tables IV and V). The outcomes of the two groups evaluated
by the Macnab criteria were not significantly different (P=0.563;
Table V). In both groups, some cases
of transitory dysaesthesia or hyperalgesia were reported (<10%),
which were resolved within 2–4 weeks of treatment with oral
corticoids in all cases. Furthermore, no dural tears, neurological
damage or wound infections occurred in either group.
| Table IV.Comparisons of changes in the visual
analogue scale for pain and Oswestry disability index between
groups. |
Table IV.
Comparisons of changes in the visual
analogue scale for pain and Oswestry disability index between
groups.
|
| Group A | Group B |
|---|
|
|
|
|
|---|
| Variable | Pre | Post | Difference | Pre | Post | Difference |
|---|
| Visual analogue
scale for pain |
|
|
|
|
|
|
| Back
pain |
8.5 |
3.1 |
5.4 |
8.7 | 1.3 |
7.4a |
| Leg
pain |
8.8 |
2.8 |
6.0 |
8.6 | 1.2 |
7.4a |
| Oswestry disability
index | 28.5 | 13.1 | 15.4 | 30.1 | 8.3 | 21.8a |
| Table V.MacNab classification. |
Table V.
MacNab classification.
| Grade | Group A | Group
Ba | Total |
|---|
| Excellent | 137 (49.8) | 166 (52.5) | 303 (51.3) |
| Good | 122 (44.4) | 138 (43.7) | 260 (44.0) |
| Fair | 13 (4.7) | 11 (3.5) | 24 (4.1) |
| Poor | 3 (1.0) | 1 (0.3) | 4 (0.7) |
The recurrence rate was 1.0% (3/275) in group A and
0.3% (1/316) in group B. In group A, the three patients with
recurrence received a second surgery, of which two were identified
as the calcified type and one as the scar type. Patients in group A
received conventional endoscopic transforaminal nucleotomy with
foraminoplasty, and surgery aimed to remove the nucleus pulposus,
however, the true lesions causing symptoms were not removed. In
group B, the scar type was found in the one patient with a
recurrence. This patient had scar type, and the nerve root
adhesions were difficult to release resulting in a poor
outcome.
Discussion
The present study has presented a new pathological
classification of lumbar disc herniation based on endoscopic
observations. In total, three pathological types were identified
and referred to as fresh, calcified and scar, and definitive
treatment based on the type was associated with improved outcomes
when compared to conventional removal of the protruding nucleus
pulposus only. The reliability of identification of the three
pathological types was good, and the types were consistent with
histopathological examination of specimens removed at surgery.
Since its introduction, endoscopic transforaminal
nucleotomy with foraminoplasty has become a widely accepted method
of treating lumbar disc disease that is associated with good
surgical outcomes and minimal surgical trauma (4–6). Novel
approaches to the procedure include magnetic resonance assisted
surgery (5), irrigation discectomy
(15), and an ‘inside out’ technique
that identifies pain generators with the patient in an awake and
aware state using local anesthesia (16). Although the procedure is generally
considered safe, reported complications include post-discectomy
pseudocyst formation (17), dural
tears (18) and exiting root injury
(19). While some studies have
indicated that the rate of recurrence is higher with endoscopic
procedures, surgical indications and surgeon experience are crucial
factors that affect outcomes (7). In
fact, a study by Genevay et al (20) identified wide variability in the
number and type of eligibility criteria of back pain syndromes and
surgical indications.
The natural history of lumbar disc herniation is
complex and variable, and degeneration of the disc continues two
years after onset. It is generally recommended that six to eight
weeks of conservative treatment should be performed, and surgical
treatment should be carried out if conservative treatment fails
(21). Masui et al (22) followed 21 patients with lumbar disc
herniation treated non-surgically with serial MRI for a minimum of
seven years. The mean space occupying the ratio of herniation
demonstrated a significant reduction both on the two-year and final
scans, and progression of degeneration of the intervertebral disc
was observed in all patients on the final scan. Furthermore, no MRI
factors were detected which could distinguish patients who were and
were not eventually to develop lumbago and/or sciatica, and
morphological changes of lumbar disc herniation continued to occur
even after two years. Parisini et al (23) examined the results of 129 patients
who received surgery for lumbar disc herniation and reported
excellent or good short-term results in 95% of cases, which
decreased to 87% at a follow-up of 12.4 years. Atlas et al
(24) performed a 10-year long-term
follow-up study for 400 patients with sciatica caused by lumbar
disc herniation, of which 217 received surgery and 183 conservative
treatments. At the last follow-up, 69% of patients who received
surgery considered that surgery improved their symptoms and 71% of
patients were satisfied with the status quo; the rates were 61 and
56%, respectively, in patients who received conservative
treatment.
Endoscopic transforaminal nucleotomy with
foraminoplasty for lumbar disk herniation not only has evident
therapeutic advantages (1,10), but the enhanced visualization can
provide new insights into the disease process. Understanding and
treatment of lumbar disc herniation has focused on removal of
herniated disc material. However, secondary changes such as
ligamentum flavum ossification, posterior longitudinal ligament
calcification, poor blood circulation of the nerve root and thecal
sac and stenosis of the lateral recess are often identified.
Usually, excision of the ligamentum flavum or enlargement of the
neural canal is performed, but in a large percentage of cases
symptoms are not relieved.
In the present study, lumbar disc herniation
observed under endoscopy was classified into three types: Fresh
herniation, calcified and scar. In the fresh herniation, after
annulus rupture the nucleus pulposus protruding into the spinal
canal may compress the dural sac and/or nerve root resulting in low
and leg pain. In the calcified type the extruded nucleus is
absorbed spontaneously, and the symptom may diminish or completely
resolve. However, in certain cases the extruded material may become
calcified, particularly in elderly patients with a prolonged
disease course (10). Other
pathological changes, including ossification of the posterior
longitudinal ligament, hypertrophy of the ligamentum flavum,
subchondral bone sclerosis and lateral recess stenosis may also be
present (10,25). Altogether, these factors can result
in a reduced spinal canal volume and the calcified tissue may
compress or stimulate the dural sac and/or the nerve root. Scar
type is associated with scar tissue around the nerve, and may be
the result of an immune reaction. Under normal circumstances, the
nucleus pulposus is contained within the annulus fibrosus and
isolated from the immune system. Following herniation, it becomes a
foreign body and may induce an immune response (26). This may be the reason for spontaneous
absorption or calcification of the herniated nucleus pulposus
observed in some cases (27).
However, the immune response is also an inflammatory process, and
can result in scar tissue formation. If the scar tissue is limited
to the inside the annulus fibrosus, pink fibrous tissue may be
observed at endoscopy and symptoms may be completely relieved after
removing it. Moreover, if the scar tissue is adhered to the surface
of the nerve root, radicular pain may not be completely relieved
even if the nerve root is carefully dissected. In these cases no
obvious herniated material can be observed at endoscopy, and the
dural sac and/or nerve root may not be compressed (28). In addition, the present study has
identified that these three types are not necessarily associated
with each other. For example, in some elderly patients with a
prolonged disease course a protruding nucleus pulposus compressing
the dural sac and/or nerve root is identified but no calcifications
are observed. This would be considered a fresh herniation type.
It is hypothesized by the present authors that the
three pathological types may represent stages in the progression of
the disease. Fresh type represents the early stage of the disease
when herniation first occurs, and calcified and scar type are later
phases but have different outcomes. Moreover, disc herniation as a
result of degeneration and/or trauma can result in rupture of the
annulus fibrosus and extrusion of the nucleus pulposus, which
compresses the nerve root and thecal sac (25). However, the tissue is also exposed to
the immune system. An immune response may be a partial cause of
radicular symptoms (26), and may
eventually lead to calcification of the extruded tissue or the
formation of scar tissue. This postulation is somewhat supported by
the observation that the calcified type was associated with a more
advanced age and longer symptom duration, and scar type was
associated with previous invasive therapy. Most importantly,
targeted treatment based on the endoscopic observations resulted in
better outcomes as measured by VAS pain and ODI scores compared to
conventional management of simply removing the herniated disc
material. In addition, it should be noted that there was no
difference in MacNab score between the two groups. A VAS pain score
is a measure of subjective feelings of pain, and the ODI is also a
measure of pain and primarily the ability to perform activities of
daily life. MacNab criteria are primarily based on whether pain
affects the ability to work.
Although symptoms such as pain were not
significantly improved following surgery, the changes in the VAS
score and ODI were not evident in several patients of group A.
However, those patients in group A were able to return to work and
were graded as ‘good’. Based on the aforementioned explanations,
some patients in group A did not have a ‘fair or poor’ MacNab
grade, although the therapeutic efficacy of surgery for those
patients was poor. That is the possible reason that the MacNab
grade was comparable between groups A and B. However, the changes
between post- and pre-operative in VAS and ODI scores in group B
were more significantly observed than in group A.
In the present study, there was relatively lower
agreement between histological observations and clinical
intraoperative assessment in scar type herniation compared to the
other types. Moreover, sample collection was relatively difficult
in scar type herniation. In the collected samples, there were
scattered adhesions on the surface of the nerve roots, which did
not meet the requirement for pathological staining. In the
collected annulus fibrosus, contamination of scar tissues on the
surface with cells from the annulus fibrosus could not be avoided,
and these cells were hard to differentiate. However, only a
pathological examination could differentiate these cells from scar
tissues. This may be the reason for the agreement between
histological observations and clinical intraoperative assessment
with the scar type herniation.
There are a number of limitations to the present
study. Firstly, there was lack of a systematic procedure for the
diagnosis of the pain generator. Secondly, patients were not
classified by imaging data (e.g., the McCulloch classification) for
comparison with the three pathological types. Classification of
lumbar disc herniation according to preoperative imaging data can
only indicate the location of the herniation, and in many cases is
not predictive of a surgical outcome. Thus, we do not believe it
would be useful to strictly compare imaging data with the three
pathological types.
In conclusion, the present study suggests three
distinct pathological types of lumber disc herniation, and targeted
surgical therapy based on the endoscopic pathological type. This
resulted in better outcomes than simple removal of herniated disc
material. These results suggest that the removal of the herniated
material should not be the sole goal of surgery, and that factors
other than disc herniation alone can be responsible for pain
associated with lumbar disc herniation.
References
|
1
|
Gibson JN, Cowie JG and Iprenburg M:
Transforaminal endoscopic spinal surgery: The future ‘gold
standard’ for discectomy?-A review. Surgeon. 10:290–296. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Schubert M and Hoogland T: Endoscopic
transforaminal nucleotomy with foraminoplasty for lumbar disk
herniation. Oper Orthop Traumatol. 17:641–661. 2005.(In English,
German). View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Iprenburg M and Godschalx A:
Transforaminal endoscopic surgery in lumbar disc herniation in an
economic crisis-the TESSYS method. US Musculoskeletal Review.
3:47–49. 2008.
|
|
4
|
Kim HS, Ju CI, Kim SW, Kim JG, Lee SM and
Kim BW: Minimally invasive percutaneous endoscopic 2 levels
adjacent lumbar discectomy through 1 portal skin incision:
Preliminary study. Asian J Neurosurg. 10:95–101. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Choi G, Modi HN, Prada N, Ahn TJ, Myung
SH, Gang MS and Lee SH: Clinical results of XMR-assisted
percutaneous transforaminal endoscopic lumbar discectomy. J Orthop
Surg Res. 8:142013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Knight MT, Jago I, Norris C, Midwinter L
and Boynes C: Transforaminal endoscopic lumbar decompression &
foraminoplasty: A 10 year prospective survivability outcome study
of the treatment of foraminal stenosis and failed back surgery. Int
J Spine Surg. 8:212014. View
Article : Google Scholar
|
|
7
|
Anichini G, Landi A, Caporlingua F,
Beer-Furlan A, Brogna C, Delfini R and Passacantilli E: Lumbar
endoscopic microdiscectomy: Where are we now? An updated literature
review focused on clinical outcome, complications and rate of
recurrence. Biomed Res Int. 2015:4178012015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Milette PC: Classification, diagnostic
imaging, and imaging characterization of a lumbar herniated disk.
Radiol Clin North Am. 38:1267–1292. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
TESSYS technique (transforaminal
endoscopic surgical system). http://www.joimax.com/us/products/endoscopy/tessys/TESSYS_concept.phpAccessed.
Jan 2–2015.
|
|
10
|
Nellensteijn J, Ostelo R, Bartels R, Peul
W, van Royen B and van Tulder M: Transforaminal endoscopic surgery
for symptomatic lumbar disc herniations: A systematic review of the
literature. Eur Spine J. 19:181–204. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Aitken RC: Measurement of feelings using
visual analogue scales. Proc R Soc Med. 62:989–993. 1969.PubMed/NCBI
|
|
12
|
Fairbank JC, Couper J, Davies JB and
O'Brien JP: The Oswestry low back pain disability questionnaire.
Physiotherapy. 66:271–273. 1980.PubMed/NCBI
|
|
13
|
Monticone M, Baiardi P, Ferrari S, Foti C,
Mugnai R, Pillastrini P, Vanti C and Zanoli G: Development of the
Italian version of the Oswestry Disability Index (ODI-I): A
cross-cultural adaptation, reliability, and validity study. Spine
(Phila Pa 1976). 34:2090–2095. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Macnab I: Negative disc exploration. An
analysis of the causes of nerve-root involvement in sixty-eight
patients. J Bone Joint Surg Am. 53:891–903. 1971. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Soliman HM: Irrigation endoscopic
discectomy: A novel percutaneous approach for lumbar disc prolapse.
Eur Spine J. 22:1037–1044. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Gore S and Yeung A: The ‘inside out’
transforaminal technique to treat lumbar spinal pain in an awake
and aware patient under local anesthesia: Results and a review of
the literature. Int J Spine Surg. 8:2014. View Article : Google Scholar
|
|
17
|
Kang SH and Park SW: Symptomatic
post-discectomy pseudocyst after endoscopic lumbar discectomy. J
Korean Neurosurg Soc. 49:31–36. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ahn Y, Lee HY, Lee SH and Lee JH: Dural
tears in percutaneous endoscopic lumbar discectomy. Eur Spine J.
20:58–64. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Choi I, Ahn JO, So WS, Lee SJ, Choi IJ and
Kim H: Exiting root injury in transforaminal endoscopic discectomy:
Preoperative image considerations for safety. Eur Spine J.
22:2481–2487. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Genevay S, Atlas SJ and Katz JN: Variation
in eligibility criteria from studies of radiculopathy due to a
herniated disc and of neurogenic claudication due to lumbar spinal
stenosis: A structured literature review. Spine (Phila Pa 1976).
35:803–811. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Awad JN and Moskovich R: Lumbar disc
herniations: Surgical versus nonsurgical treatment. Clin Orthop
Relat Res. 443:183–197. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Masui T, Yukawa Y, Nakamura S, Kajino G,
Matsubara Y, Kato F and Ishiguro N: Natural history of patients
with lumbar disc herniation observed by magnetic resonance imaging
for minimum 7 years. J Spinal Disord Tech. 18:121–126. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Parisini P, Di Silvestre M, Greggi T,
Miglietta A and Paderni S: Lumbar disc excision in children and
adolescents. Spine (Phila Pa 1976). 26:1997–2000. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Atlas SJ, Keller RB, Wu YA, Deyo RA and
Singer DE: Long-term outcomes of surgical and nonsurgical
management of sciatica secondary to a lumbar disc herniation: 10
year results from the Maine lumbar spine study. Spine (Phila Pa
1976). 30:927–935. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Yoshiiwa T, Miyazaki M, Kawano M, Ikeda S
and Tsumura H: Analysis of the relationship between hypertrophy of
the ligamentum flavum and lumbar segmental motion with aging
process. Asian Spine J. 10:528–535. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Hasegawa T, An HS, Inufusa A, Mikawa Y and
Watanabe R: The effect of age on inflammatory responses and nerve
root injuries after lumbar disc herniation: An experimental study
in a canine model. Spine (Phila Pa 1976). 25:937–940. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Shamji MF, Allen KD, So S, Jing L, Adams
SB Jr, Schuh R, Huebner J, Kraus VB, Friedman AH, Setton LA and
Richardson WJ: Gait abnormalities and inflammatory cytokines in an
autologous nucleus pulposus model of radiculopathy. Spine (Phila Pa
1976). 34:648–654. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wassenaar M, van Rijn RM, van Tulder MW,
Verhagen AP, van der Windt DA, Koes BW, de Boer MR, Ginai AZ and
Ostelo RW: Magnetic resonance imaging for diagnosing lumbar spinal
pathology in adult patients with low back pain or sciatica: A
diagnostic systematic review. Eur Spine J. 21:220–227. 2012.
View Article : Google Scholar : PubMed/NCBI
|