Introduction
Two-dimensional (2D) X-ray cephalometry for
orthodontia was first used by Broadbent in 1931 (1), and this technique has since evolved
from a manual to a computer-aided measurement (2,3).
Cephalometry is the foundation for the diagnosis, analysis and
planning for orthodontic surgery and therapy. However, the 2D
measurements based on radiation techniques are affected by a number
of issues, such as image overlapping and landmark identification,
achieved by positioning the patients body within a cone beam during
CT scanning, thus leading to low clarity of the lateral
cephalograms for precision measurement (2–4).
With the advances (2–4) in
computer software and medical technology, 3D cone-beam computed
tomography (CBCT) for craniofacial cephalometry has become
possible. This method can be applied to patient specific types of
tissues with accurate results. 3D CBCT is easy to conduct. The
technique has greatly improved and enhanced the breadth and depth
of the applications of the 3D craniofacial structure imaging in
clinical practices.
At present, there are several commonly used 3D
cephalometric methods, including X-ray skull stereo imaging, 3D CT
scanning and CBCT. CBCT is a relatively novel imaging method, with
low radiation exposure of the patient, high scanning flexibility,
image accuracy and fewer misdiagnosis, and is particularly suitable
for hard tissue imaging (5,6). These advantages have made CBCT
increasingly popular in the diagnosis and treatment planning for
various oral and craniofacial diseases (7,8).
However, due to the complexity of the 3D data, this method has not
yet been standardized. Furthermore, the third-party software used
in CBCT data analysis has not been adapted widely. Therefore, there
is no single CBCT measurement method that has been widely used in
clinical practices (9).
In the present study, CBCT-based cephalometry was
attempted on craniofacial hard tissues with the specialized
software in vivo, and the findings were compared the data
obtained from the traditional 2D lateral radiographs.
Materials and methods
Patients and inclusion criteria
A total of 40 (including 18 males and 22 females,
aged between 12 and 18 years) were randomly selected for inclusion
into the present study from the Department of Orthodontics at the
Stomatological Hospital Affiliated to Chongqing Medical University
(Chongqing, China) between January 2009 and January 2011. Inclusion
criteria were as follows: The patients had no missing teeth (with
the exception of the third molar teeth), no history of trauma, no
partial occlusion, no metal filling, no jaw or tooth tumors and no
mandibular fracture in their permanent dentition. All patients have
signed the consent statements and the study is approved by the
Ethics committee of Stomatological Hospital Affiliated to Chongqing
Medical University (Chongqing, China).
Methods
All patients in the current study were subjected to
X-ray and CBCT imaging. Traditional cephalograms were routinely
obtained with an X-ray diagnosis system (Kodak 9000; Kodak,
Rochester, NY, USA) at a voltage of 62 kV, current of 8 mA and
distance of median sagittal plane to the X-ray source of 154.5 cm.
In addition, the amplification rate of the X-ray imaging was 1.1x
more than traditional cephalograms.
CBCT scans were conducted using the Classic i-CAT
CBCT system (Imaging Science International, Hatfield, PA, USA) with
the following parameters: Visible range was set at 13×10 cm with
gray value of 14 bit; scanning was performed at a speed of 360°/sec
for 4 sec; the resolution was set to 0.4 stereo pixel at a layer
thickness of 0.4 mm; and the tube voltage and current were adjusted
to 120 kV and 5 mA, respectively. During scanning, the patient was
asked to sit in a centric occlusion position, using a chin pocket
and a head frame to fix their head. The Frankfort plane was
positioned parallel to the ground. The scanning baseline was
aligned with the occlusal plane, and scanning was performed between
the upper edges of the ears and the chin.
Marking and tracing of cephalometric landmarks using
the Tweed and Steiner standards (10). The digitized X-ray cephalograms were
uploaded into the WinCeph version 8.0 software (Rise Corporation,
Sendai, Japan). The images were adjusted for brightness and
contrast for better viewing. A total of 24 landmarks on the
craniofacial hard tissues were marked and traced by an analyzer
based on the scales marked on the X-ray films. These points were
the following: Sella center, nasion, porion, basion O-orbital,
pterygomaxillary fissure, anterior nasal spine posterior nasal
spine, alveolar seat, lower alveolar seat, upper middle incisor,
UlR-upper incisor teeth point, lower incisor, lower incisor root,
upper molar, distinct upper molar, lower molar, gonion, pogonion,
menton, gnathion center of mandibular bony joint, condyle vertex
and posterior condylar.
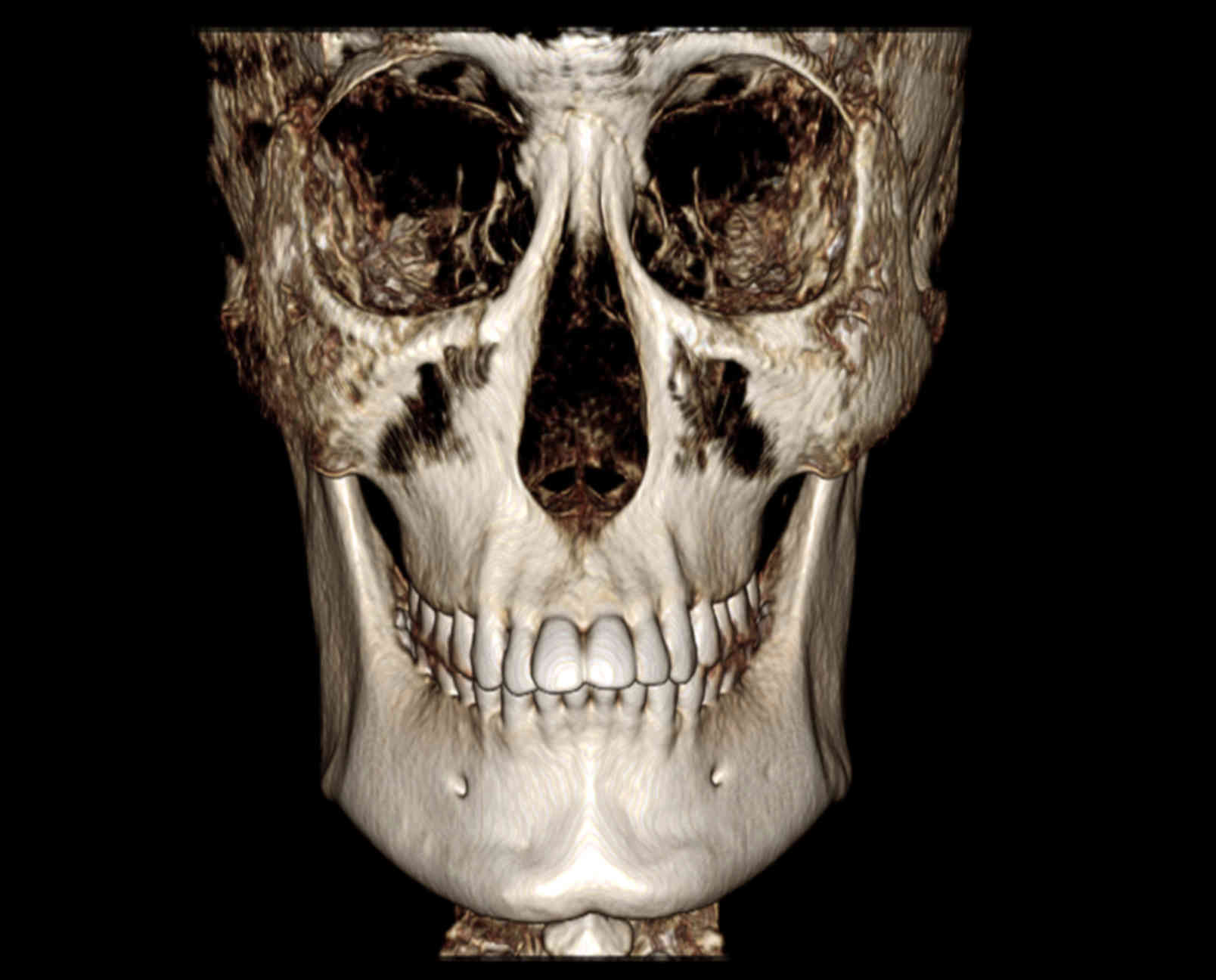
CBCT scan data were fed to the DICOM 3.0 in
vivo version 5.1 software (Anatomage, San Jose, CA, USA). The
data were marked and traced by the same analyzer for the following
20 craniofacial hard tissue landmarks and profiles. Figs. 1 and 2
are representative three-dimensional images reconstructed from a
cone-beam computed tomography scan using in vivo dental
software and representative marked and traced image of
three-dimensional cone-beam computed tomography scanning, obtained
using in vivo dental software: Right orbital point, left
orbital point, N, right ear point, left ear point, right orbital
profile, left orbital profile, right mandible profile, left
mandible profile, symphyseal profile, S, Sella profile, nasion
profile, Ba, upper right incisor profile, upper left incisor
profile, lower right incisor profile, lower left incisor profile,
maxillary profile and D.
Statistical analysis
Paired t-tests were conducted to determine
differences between 17 measurements obtained from the 2D and 3D
techniques using SPSS software (version 17.0; SPSS, Inc., Chicago,
IL, USA). Differences were considered as statistically significant
when P<0.05. The data were also analyzed for the discrete degree
indicators standard deviation (SD), standard error (SE) and
coefficient of variation.
Results
Cephalometric data from 2D X-ray
images and 3D CBCT cephalograms
Significant differences (P<0.05) were detected in
all 12 angle and 5 linear measurements between the two methods
(Table I). The discrete degree was
higher in the 2D images than the 3D data (Fig. 1).
 | Table I.Cephalometric data from 2D X-ray
images and 3D CBCT cephalograms. |
Table I.
Cephalometric data from 2D X-ray
images and 3D CBCT cephalograms.
|
|
|
|
| 95% CI |
|
|
|---|
|
|
|
|
|
|
|
|
|---|
| Measurement | Mean | SD | SE | Minimum | Maximum | t-value | P-value |
|---|
| SNA | 3.055 | 2.249 | 0.356 | 2.335 | 3.774 | 8.590 | <0.001 |
| SNB | 1.578 | 1.870 | 0.296 | 0.979 | 2.176 | 5.336 | <0.001 |
| ANB | 1.644 | 1.929 | 0.305 | 1.027 | 2.261 | 5.389 | <0.001 |
| MP-FH | 4.758 | 4.471 | 0.707 | 3.328 | 6.188 | 6.730 | <0.001 |
| SL | −3.013 | 7.843 | 1.240 | −5.521 | −0.504 | −2.429 | 0.002 |
| SE | −1.114 | 1.713 | 0.271 | −1.662 | −0.566 | −4.114 | <0.001 |
| SND | 3.300 | 2.149 | 0.340 | 2.613 | 3.988 | 9.711 | <0.001 |
| U1-NA (mm) | 0.607 | 0.488 | 0.077 | 0.451 | 0.763 | 7.860 | <0.001 |
| U1-NA (°) | −2.073 | 6.173 | 0.976 | −4.047 | −0.09865 | −2.124 | 0.040 |
| U1-L1 | 4.489 | 9.074 | 1.435 | 1.587 | 7.391 | 3.129 | 0.003 |
| L1-NB (mm) | −0.236 | 0.679 | 0.107 | −0.454 | −0.019 | −2.199 | 0.034 |
| L1-NB (°) | 1.697 | 1.484 | 0.235 | 1.222 | 2.171 | 7.234 | <0.001 |
| L1-MP | −3.437 | 5.205 | 0.823 | −5.102 | −1.772 | −4.176 | <0.001 |
| L1-FH | −3.231 | 2.284 | 0.362 | −3.961 | −2.500 | −8.947 | <0.001 |
| OP to SN | −1.801 | 1.479 | 0.234 | −2.274 | −1.327 | −7.699 | <0.001 |
| Pog to NB (mm) | 0.298 | 0.844 | 0.134 | 0.028 | 0.568 | 2.232 | 0.031 |
| GoGn to SN | 1.470 | 2.743 | 0.434 | 0.592 | 2.347 | 3.389 | 0.002 |
Comparison of the mean, SD, SE and
coefficient of variation values between the two methods
Positioning of in vivo specimens is different
from traditional multiplaner reconstruction and is based on four
reference points at the N, Or-R, and left and right ears (Fig. 2). 3D measurements were less scattered
and therefore, provided a higher degree of accuracy, compared with
the 2D measurements, as determined by the standard deviation and
coefficient of variation values. Therefore, 3D CBCT may be able to
provide more accurate data for orthodontic physicians for better
therapeutic planning and have great potential clinical application
(Table II).
| Table II.Comparison of the mean, SD, SE and
coefficient of variation values between the two methods. |
Table II.
Comparison of the mean, SD, SE and
coefficient of variation values between the two methods.
|
| Mean | SD | Coefficient of
variation (%) |
|---|
|
|
|
|
|
|---|
| Measurement | CBCT | Winceph8 | CBCT | Winceph8 | CBCT | Winceph 8 |
|---|
| SNA | 84.88 | 87.32 | 1.576 | 1.941 | 1.86 | 2.22 |
| SNB | 82.09 | 82.82 | 1.700 | 1.996 | 2.07 | 2.41 |
| ANB | 2.93 | 2.90 | 1.115 | 1.124 | 38.08 | 38.76 |
| MP-FH | 18.73 | 18.93 | 0.923 | 1.002 | 4.93 | 5.29 |
| SL | 44.77 | 44.23 | 2.329 | 2.312 | 5.20 | 5.22 |
| SE | 22.81 | 22.35 | 0.996 | 1.003 | 4.37 | 4.48 |
| SND | 79.05 | 80.35 | 1.254 | 1.223 | 1.59 | 1.52 |
| U1-NA (mm) | 6.49 | 6.32 | 0.362 | 0.367 | 5.58 | 5.80 |
| U1-NA (°) | 40.73 | 39.02 | 1.129 | 1.171 | 2.77 | 3.00 |
| U1-L1 | 102.89 | 101.39 | 1.072 | 1.078 | 1.04 | 1.06 |
| L1-NB (mm) | 4.12 | 4.04 | 0.493 | 0.487 | 11.97 | 12.05 |
| L1-NB (°) | 33.47 | 32.69 | 0.589 | 0.590 | 1.76 | 1.80 |
| L1-MP | 108.31 | 107.02 | 1.760 | 1.775 | 1.63 | 1.66 |
| L1-FH | 54.31 | 54.28 | 0.496 | 0.516 | 0.91 | 0.95 |
| OP to SN | 20.90 | 20.20 | 0.762 | 0.792 | 3.65 | 3.92 |
| Pog to NB (mm) | 1.83 | 1.77 | 0.476 | 0.484 | 2.60 | 2.73 |
| GoGn to SN | 26.74 | 26.79 | 2.324 | 2.397 | 8.69 | 8.95 |
Discussion
Successful orthodontic treatment planning depends on
accurate measurements on the cranio-maxillofacial skeleton,
relative position of teeth, soft tissue lateral profile and
craniofacial growth trends. The accuracy of such measurements is
mainly affected by the quality of the lateral cephalograms
(6).
Traditional 2D lateral cephalograms have certain
inherent limitations. Firstly, it is difficult to precisely locate
anatomical landmarks using 2D cephalograms due to image
overlapping. Secondly, the images may present certain distortions
as a result of different magnification due to differences in the
distances between the film and craniofacial anatomy structures.
Finally, 2D cephalogram measurements are easily affected by the
head posture during imaging (9).
Therefore, other techniques, such as 3D X-ray cephalography, 3D CT
and 3D CBCT, have been developed to overcome these shortcomings.
However, 3D X-ray cephalography is unable to present accurate
cephalometric morphology for diagnosis and treatment (11–13). In
addition, 3D CT imaging requires a long scanning time and higher
radiation exposure for the patients. It also produces artifacts if
there are metal fillings in the mouth and is therefore not
recommended as a routine diagnosis method (14). CBCT is a computerized image
reconstruction method developed from CT with an improved
computational algorithm. Radiation exposure during this method is
similar to that of X-ray cephalography (15,16).
Furthermore, cone-beam scanning improves the 3D spatial resolution,
shortens the data acquisition time and reduces artifacts. CBCT has
high quality imaging capacity and is easy to operate, thus may
allow wide adaption by dentists in their clinical practices, and
may contribute to accurate diagnosis and treatment of orthodontic
diseases (17,18).
Kumar et al (19) and van Vlijmen et al (20) observed that there was no significant
measurement difference between different types of cephalograms.
However, these studies used 2D, not 3D, cephalograms for
measurements. Following the comparison of 2D and 3D measurements,
Gribel et al identified that there was no difference in
linear measurements between 3D CBCT and direct dry skull
measurements; however, a difference was detected between the 2D
lateral X-ray imaging and direct dry skull measurement (21). Furthermore, Periago et al
(22) and Baumgaertel et al
(23) also demonstrated that 3D
cephalometry was similar to direct skull measurement.
The results of the present study revealed that there
were significant differences in all 12 angle and 5 linear
measurements between the two methods (Tables I and II), and that 3D measurements were less
scattered and therefore, a higher degree of accuracy, compared with
the 2D measurements, as determined by the standard deviation and
coefficient of variation values. These findings suggested that 3D
CBCT has better measurement repeatability and accuracy when
compared with the traditional 2D cephalometric measurements.
Therefore, 3D CBCT may be able to provide more accurate data for
orthodontic physicians for better therapeutic planning and have
great potential clinical application.
In vivo 5.1 software (24) was used in the present study, which
was developed by Anatomage specifically for CBCT image analysis. It
can reconstruct 3D anatomical images from DICOM files generated by
medical CT and magnetic resonance imaging instruments. The software
can integrate the image, anatomical impression and CBCT data into a
single file, which can then be opened by an application. Through
the 3D analysis module, physicians create 3D cephalometric files
that are compatible with the existing 2D analysis files. In
addition, they are able to customize the modules by setting linear
and point parameters, and to add new measurements (for example,
other auxiliary points and lines, such as bisector of angle,
perpendicular bisector and parallel line for better positioning and
tracing). Additional programs can be coded to meet the requirements
of different analyses and projects. All operations are easy, no
additional device is required for the measurement, and all results
are generated automatically and compared with the average from the
patient specific group. The nasion is used as an origin to measure
the linear distance at each angle.
In conclusion, the orthodontic in vivo
application of aided CBCT technology remains at an early stage. The
use of the 3D cephalometric method for orthodontic diagnosis is
currently investigated further. The results of these investigations
will provide theoretical support of the technology in orthodontic
clinical practice and research. The current study demonstrated that
the volumetric data obtained from a single CBCT scan can be
processed by the image reconstruction techniques and used for
cephalometric measurements to meet the clinical requirements prior
to orthodontic surgery and examination for maxillofacial
supernumerary teeth, embedded teeth and temporomandibular joint.
This method can therefore be used to partially replace
orthopantomogram and traditional cephalogram as the routine
orthodontic examination option.
Acknowledgements
The present study was supported by the Research
Projects, Department of Sichuan Education (Chengdu, China; grant
no. 13ZB0251) and Nanchong Municipal Science and Technology Bureau
(Sichuan, China; grant no. 13A0044).
References
|
1
|
Broadbent BH: A new x-ray technique and
its application to orthodontia. Angle Orthod. 1:45–66. 1931.
|
|
2
|
Baumrind S and Frantz RC: The reliability
of head film measurements. 1. Landmark identification. Am J Orthod.
60:111–127. 1971. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Li XZ, Wen XT, Zhou J and Wang P: X-ray
film quality on hand-point repeatability influence. Zhongguo Xibu
Kou Qiang Yi Xue Za Zhi. 22:342–343. 2004.(In Chinese).
|
|
4
|
Liu Y, Zhao J, Ding Y, et al: Precision of
cephalometric landmark identification from cone-beam computed
tomography. Zhonghua Kou Qiang Yi Xue Za Zhi. 17:61–65. 2010.(In
Chinese).
|
|
5
|
Feng Q and Qian Y: 3-Dimensional image
measurements for craniofacial hard tissue. Kou Qiang Cai Liao Qi
Xie Za Zhi. 15:140–142. 2006.(In Chinese).
|
|
6
|
Mah J and Hatcher D: Diagno´stico por
imagen craneofacial enortodoncia. Capı´tulo 2Grabber TM, Vanarsdall
RL and Vig KWL: Orthodontics: Current Principles and Techniques. St
Louis, MO: Elsevier; pp. 71–100. 2005
|
|
7
|
De Vos W, Casselman J and Swennen GR:
Cone-beam computed tomography (CBCT) imaging of the oral and
maxillofacial region: A systemic review of the literature. Int J
Oral Maxillofac Surg. 38:609–625. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Arnheiter C, Scarfe WC and Farman AG:
Trends in maxillofacial cone-beam computed tomography usage. Oral
Radiology. 22:80–85. 2006. View Article : Google Scholar
|
|
9
|
Major PW, Johnson DE, Hesse KL and Glover
KE: Effect of head orientation on posterior anterior cephalometric
landmark identification. Angle Orthod. 66:51–60. 1996.PubMed/NCBI
|
|
10
|
Xü T, Ahn J and Baumrind S: Sensitivity of
four representative angular cephalometric measures. Zhonghua Kou
Qiang Yi Xue Za Zhi. 35:221–223. 2000.(In Chinese). PubMed/NCBI
|
|
11
|
Baumrind S, Moffitt FH and Curry S: The
geometry of three-dimensional measurement from paired coplanar
x-ray images. Am J Orthod. 84:313–322. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wang B, Li S and Zhou L: Development of a
video system for three-dimensional cephalometry and dental cast
analysis. Zhonghua Kou Qiang Yi Xue Za Zhi. 35:230–232. 2000.(In
Chinese). PubMed/NCBI
|
|
13
|
Yao S: Studies of three-dimensional
measurement and analysis of cranio-mandibular-facial hard-soft
tissue morphology and clinical applicationPhD dissertation, The
Fourth Military Medical School. Xi'an: 1993
|
|
14
|
AYi-jiang MiCong-bo: Application of 3D
measurement techniques in orthodontics. Journal of Clinical
Rehabilitative Tissue Engineering Research,. 26:(15). 48692011.
|
|
15
|
Swennen GR and Schutyser F:
Three-dimensional cephalometry: Spiral multi-slice vs cone-beam
computed tomography. Am J Orthod Dentofacial Orthop. 130:410–416.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zhang JH, Chen WJ, Chen H and Fang Y:
Clinical application of multi-slice spiral CT tooth surface imaging
in the diagnosis of impacted tooth. Wen Zhou Yi Xue Yuan Xue Bao
Bian Ji Bu. 34:221–222. 2004.(In Chinese).
|
|
17
|
Scarfe WC, Farman AG and Sukovic P:
Clinical applications of cone-beam computed tomography in dental
practice. J Can Dent Assoc. 72:75–80. 2006.PubMed/NCBI
|
|
18
|
Zhang J and Zhu S: Advances in cone beam
computed tomography technology for the quantitative measurements in
orthodontics. Zhonghua Kou Qiang Yi Xue Za Zhi (electronic
version). 4:400–403. 2010.(In Chinese).
|
|
19
|
Kumar V, Ludlow J, Cevidanes Soares LH and
Mol A: In vivo comparison of conventional and cone beam CT
synthesized cephalograms. Angle Orthod. 78:873–879. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
van Vlijmen OJ, Bergé SJ, Swennen GR,
Bronkhorst EM, Katsaros C and Kuijpers-Jagtman AM: Comparison of
cephalometric radiographs obtained from cone-beam computed
tomography scans and conventional radiographs. Int J Oral
Maxillofac Surg. 67:92–97. 2009. View Article : Google Scholar
|
|
21
|
Gribel BF, Gribel MN, Frazäo DC, McNamara
JA Jr and Manzi FR: Accuracy and reliability of craniometric
measurements on lateral cephalometry and 3D measurements on CBCT
scans. Angle Orthod. 81:26–35. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Periago DR, Scarfe WC, Moshiri M, Scheetz
JP, Silveira AM and Farman AG: Linear accuracy and reliability of
cone beam CT derived 3-dimensional images constructed using an
orthodontic volumetric rendering program. Angle Orthod. 78:387–395.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Baumgaertel S, Palomo JM, Palomo L and
Hans MG: Reliability and accuracy of cone-beam computed tomography
dental measurements. Am J Orthod Dentofacial Orthop. 136:19–28.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ma X: Clinical Application of
Maxillofacial Cone Beam CT. People's Health Publishing House;
Beijing: pp. 94–995. 2011
|