Introduction
Gout is a metabolic disease that is characterized by
hyperuricemia. It can attack the first metatarsal joint (1), hand and wrist (2,3). The
incidence of gout in the western population is 1–2% (4). The most common symptom of gout is an
acute recurrent attack of inflammatory arthritis. The
metatarsal-phalangeal joint is the most affected joint in almost
half of patients. The heels, wrists, knees and fingers can also be
affected (5). Gout in the wrist can
cause crystal deposits in the hyaline cartilage and synovial
membrane, which lead to a reduced vascular supply of the lunate and
bone destruction. Hyperuricemia is a feature of gout, but some
patients with high uric acid levels never develop gout, and ~50% of
gout patients do not have this symptom (6). Medications to reduce serum uric acid
levels can be used.
Kienböck's disease is a disorder of the lunate bone
in the wrist, which is characterized by avascular necrosis
(7). It is a rare disease, and the
incidence of has not been reported. The exact etiology of
Kienbock's disease is not known. Median wrist pain is one of the
key symptoms. The primary method of treatment is surgery, with the
aim of restoring blood supply to the lunate (8). Cases of Kienböck's disease combined
with gout are rarely observed (9).
To the best of our knowledge, this is the third report in the
literature (9,10).
Case report
In May 2014, a 49-year-old male patient presented to
the Department of Hand Surgery at The First Affiliated Hospital of
Zhejiang University (Hangzhou, China) with swelling and pain in his
right wrist for one month (Fig. 1).
The pain had been bearable at first and the patient did not take
any medication. At 1 week prior to admission, when the pain became
severe, the patient had visited a local hospital. The patient was
advised to take non-steroidal anti-inflammatory drugs (Celebrex;
Pfizer, Inc., New York, NY, USA; 200 mg twice a day) and given a
splint fixation, but there was no notable improvement in pain
relief. Upon examination at the present hospital, redness, pain and
swelling were noted on the dorsal aspect of his right wrist. Palmar
flexion was reduced by 60% and dorsiflexion was reduced by 80%
compared with the unaffected wrist. The grip strength was 25% of
the unaffected side. The painful pressure spot was located over the
central proximal row of the carpal bones. The patient reported no
history of trauma. Laboratory test results were performed,
including a leukocyte count (11,000 cells/µl; normal range,
4,000–10,000 cells/µl), uric acid measurement (427 µmol/l; normal
range, 208–428 µmol/l), C-reactive protein concentration assay
(64.30 mg/dl; normal range, 0–8 mg/dl) and a rheumatological blood
screen (rheumatoid factor, <20 U/ml, normal range, 0–20 U/ml;
anti-streptolysin 37 IU/ml, normal range, 0–100 IU/ml) (normal
result). Radiographs indicated a blurred joint surface in the
distal radius, the proximal pole of the lunate and the scaphoid,
narrowing of the joint space, sclerosis and collapse of the lunate
bone (Fig. 2). Computed tomography
(CT) imaging indicated lunate bone sclerosis with subchondral small
cysts, a decrease of lunate height and a narrowing in the joint
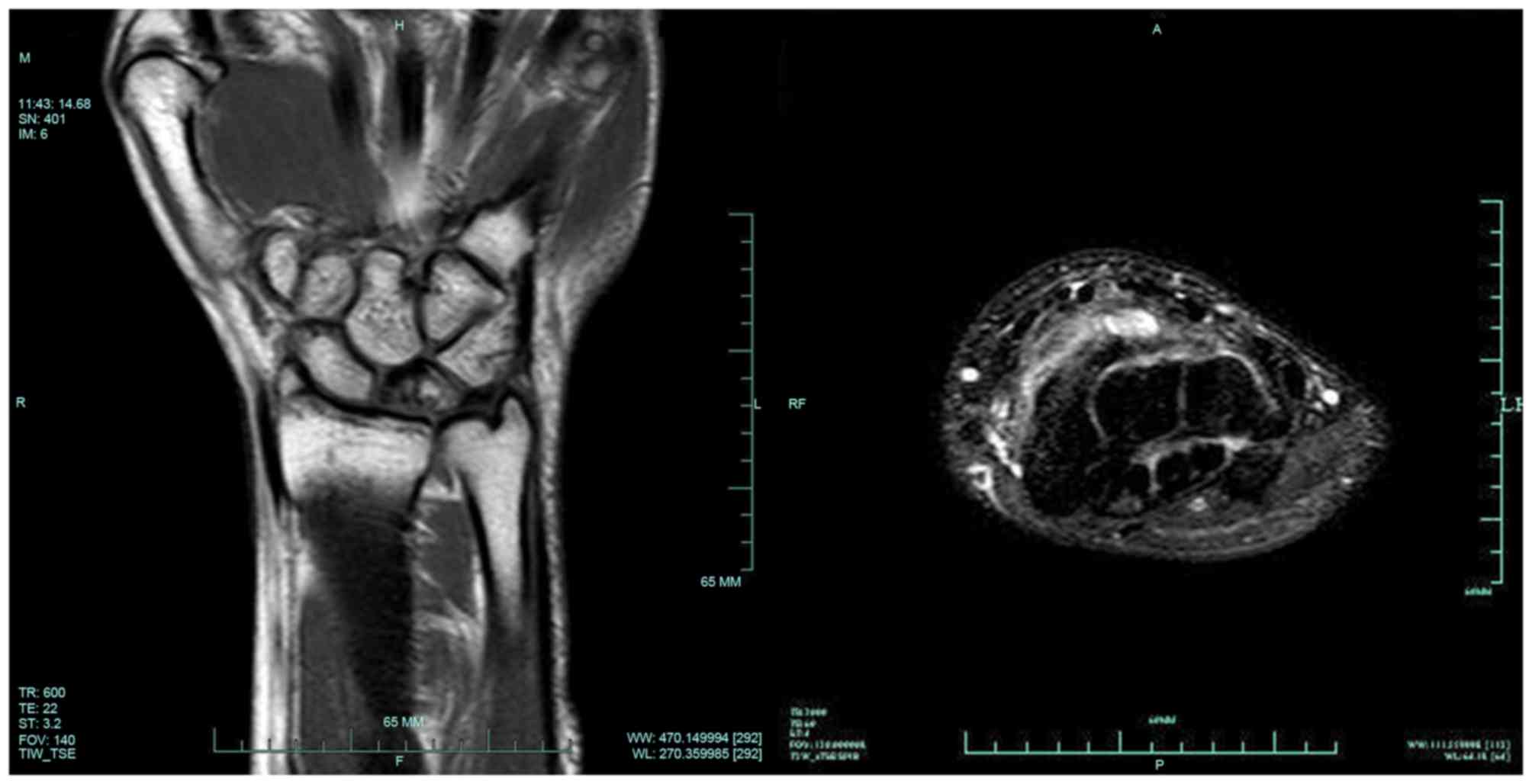
space of the distal radiocarpal joint (Fig. 3). Magnetic resonance imaging (MRI)
revealed low signal intensity in the lunate bone on T1-weighted
images and small pieces of high signal intensity on T2-weighted
images (Fig. 4). In addition, the
synovial tissue exhibited obvious thickening on the dorsal
radiocarpal joint (Fig. 4).
The patient was initially diagnosed with stage
IIIB-IV Kienböck's disease [according to the classification of
Lichtman and Degnan (11)] and
synovitis (due to hyperplasia of synovium). An open extra-articular
synovectomy was performed, and multiple monosodium urate crystal
deposits were observed during the surgery (Fig. 5). A synovectomy with arthroscopy was
then performed. The articular surface of the lunate, the lunate
facet of the distal radius and the articular surface of the
capitate were floating. Synovitis and gouty deposits, and localized
articular bone loss were also observed in the arthroscopy. The
patient was Grade 3 according to the arthoscopic assessment and
classification of Kienböck's disease (12). The final diagnosis was Kienböck's
disease (stage IIIB-IV) combined with gout. The patient's wrist
swelling had decreased markedly 1 week after the synovectomy with
arthroscopy. Bearing heavy loads on the wrist was not recommended.
The patient received colchicine (KPC Pharmaceuticals, Inc.,
Kunming, China; 0.5 mg twice a day) for 1 month after the surgery
and was then prescribed allopurinol (Zhejiang Hisun Pharmaceutical
Co., Ltd., Taizhou, China; 200 mg, three times a day) when the pain
had completely ceased. A total of 2 years after the surgery, the
patient had no recurrence of wrist pain or limitation of motion,
and radiographs revealed no degeneration of the wrist (Fig. 6).
Written informed consent was obtained from the
patient for publication of the present case report and accompanying
images. Ethical approval was provided by the Medical Ethics
Committee of The First Affiliated Hospital of Zhejiang
University.
Discussion
Gout in the wrist can lead to scapholunate
dissociation (13), carpal tunnel
syndrome and tendon entrapment or rupture (14). To the best of our knowledge, only two
cases of Kienböck's disease combined with gout have previously been
reported. Castagnoli et al (9) reported the case of 42-year-old male
laborer with Kienböck's disease and gout; however, the report did
not describe the treatment procedures and only provided the imaging
findings. Shin et al (10)
reported the case of a 54-year-old patient who presented with stage
II Kienböck's disease combined with gout. Arthroscopic synovectomy,
intra-articular injection of corticosteroid and partial wrist
denervation were performed. The wrist was subsequently pain-free
with range of motion and there was no further development of the
Kienböck's disease. The two patients described in the
aforementioned case reports exhibited hyperuricemia, but the
patient in the present study had a normal uric acid level and no
history of gout; thus, gout as the initial diagnosis was easily
ignored. Monosodium urate crystal deposits observed during the
synovectomy made the diagnosis of gout definitive.
The aetiology of Kienböck's disease is unknown,
although negative ulnar variance, corticosteroid use, low arterial
inflow and trauma are all risk factors for its development
(4,15–17).
Gout in the wrist can cause crystal deposits in the hyaline
cartilage and synovial membrane, which leads to reduced vascular
supply of the lunate and bone destruction (10). The concomitant phenomenon of
Kienböck's disease and gout may not be a coincidence, and requires
further research. Gout may affect blood supply to the lunate,
resulting in Kienböck's disease. Resnick et al (18) reported that calcium pyrophosphate
dihydrate deposition disease of the lunate bone can appear
increasingly opaque compared with normal carpal bone, mimicking the
appearance of Kienböck's disease. The diagnosis is characterized
histologically in gout by deposits of monosodium urate crystals.
MRI serves a critical role in the diagnosis of Kienböck's disease,
and could provide early identification of avascular necrosis of the
lunate Marked thickening of the area with synovitis on T2-weighted
images in cases of Kienböck's disease combined with gout make it
distinct from typical Kienböck's disease.
The primary treatment for Kienböck's disease in
patients with gout is to control the symptoms of gout effectively.
In the present study, a revascularization procedure or wrist fusion
was not performed. Synovectomy for stage II Kienböck's disease
(10) and IIIB-IV Kienböck's
disease, as in the present case, has been demonstrated to achieve
good results. The wrist of the patient in the present study was
observed to be more stable compared with ordinary patients with
joint degeneration.
In conclusion, the rarity of Kienböck's disease
combined with gout makes it difficult to examine the potential
association between gout and Kienböck's disease. Kienböck's disease
combined with gout tends to be ignored and easily misdiagnosed.
Gout may be a potential cause of Kienböck's disease. The surgical
procedure chosen for Kienböck's disease combined with gout is
markedly different from the conventional surgeries; for instance,
more revascularization procedures or wrist fusion are performed for
Kienböck's disease alone. The current study outlines a successful
treatment strategy for gout combined with Kienbock's disease.
Acknowledgements
The current study was supported by the Zhejiang
Traditional Chinese Medicine Research Program (grant no.
2016ZA124), the Zhejiang Medicine and Hygiene Research Program
(grant no. 2016KYB101), the National Natural Science Foundation of
China (grant no. 81702135) and the Zhejiang Natural Science
Foundation (grant no. LY16H180002).
Glossary
Abbreviations
Abbreviations:
|
MRI
|
magnetic resonance imaging
|
|
CT
|
computed tomography
|
References
|
1
|
Hepburn AL and Feher MD: Gout. N Engl J
Med. 350:519–520. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Fitzgerald BT, Setty A and Mudgal CS: Gout
affecting the hand and wrist. J Am Acad Orthop Surg. 15:625–635.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kamimura T, Hatakeyama M, Okazaki H and
Minota S: Acute gout attack in the wrist joint. Intern Med.
43:641–642. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Beredjiklian PK: Kienbock's disease. J
Hand Surg Am. 34:167–175. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Schlesinger N: Diagnosing and treating
gout: A review to aid primary care physicians. Postgrad Med.
122:157–161. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Sturrock RD: Gout. Easy to misdiagnose.
BMJ. 320:132–133. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Dubey PP, Chauhan NK, Siddiqui MS and
Verma AK: Study of vascular supply of lunate and consideration
applied to Kienböck disease. Hand Surg. 16:9–13. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tamai S, Yajima H and Ono H:
Revascularization procedures in the treatment of Kienböck's
disease. Hand Clin. 9:455–466. 1993.PubMed/NCBI
|
|
9
|
Castagnoli M, Giacomello A, Argentina RS
and Zoppini A: Kienböck's disease in gout. Arthritis Rheum.
24:974–975. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Shin AY, Weinstein LP and Bishop AT:
Kienböck's disease and gout. J Hand Surg Br. 24:363–365. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Lichtman DM and Degnan GG: Staging and its
use in the determination of treatment modalities for Kienböck's
disease. Hand Clin. 9:409–416. 1993.PubMed/NCBI
|
|
12
|
Bain GI and Begg M: Arthroscopic
assessment and classification of Kienböck's disease. Tech Hand Up
Extrem Surg. 10:8–13. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ohishi T, Koide Y, Takahashi M, Miyata R
and Kushida K: Scapholunate dissociation caused by gouty arthritis
of the wrist. Case report. Scand J Plast Reconstr Surg Hand Surg.
34:189–191. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Schuind FA, Van Geertruyden J, Stallenberg
B, Remmelink M and Pasteels JL: A rare manifestation of gout at the
wrist-a case report. Acta Orthop Scand. 73:594–596. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Paksima N and Canedo A: Kienböck's
Disease. J Hand Surg Am. 34:1886–1889. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Irisarri C: Aetiology of Kienböck's
disease. J Hand Surg Br. 29:281–287. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Watson HK and Guidera PM: Aetiology of
Kienböck's disease. J Hand Surg Br. 22:5–7. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Resnick D, Niwayama G, Goergen TG,
Utsinger PD, Shapiro RF, Haselwood DH and Wiesner KB: Clinical,
radiographic and pathologic abnormalities in calcium pyrophosphate
dihydrate deposition disease (CPPD): Pseudogout. Radiology.
122:1–15. 1977. View
Article : Google Scholar : PubMed/NCBI
|