Introduction
Acute liver failure (ALF) is a heterogeneous
syndrome, which results in rapid deterioration of liver function
with coagulopathy and encephalopathy, and induces systemic
inflammation and multiple organ failure (1,2). The
primary causes of ALF (including, hepatitis B virus infection,
acute viral hepatitis, alcohol and hepatotoxic drugs) are variable
and the mortality rate is high, ~60–80% of individuals suffer
mortality after contracting ALF (3,4). Liver
transplantation is the only effective therapy, but financial
burden, graft shortage and possible life-threatening complications
for donors present important limitations (5). Therefore, ALF continues to lack a
widely available and effective therapy.
Immune system imbalance serves a critical function
in the course of ALF (6,7). In particular, pro-inflammatory and
anti-inflammatory cytokine imbalance in the liver and circulation
triggers exaggerated immune response and induces adverse outcomes
in ALF (3). During the progression
of ALF, high levels of pro-inflammatory cytokines trigger the
synthesis and release of anti-inflammatory cytokines. These
anti-inflammatory cytokines inhibit pathogenic inflammation, but
also suppress immune function, resulting in the development of a
compensatory anti-inflammatory response (3). The relationship between
pro-inflammatory and anti-inflammatory cytokine responses is
complex (8).
Immune deregulation is now recognized as being
critical in ALF pathogenesis, and immune modulation has become a
key aspect of ALF treatment (9,10).
Thymosin α1 (Tα1), a 28-amino acid peptide, has multiple biological
activities. Tα1 was originally considered to primarily increase
T-lymphocyte function, and has been used in the treatment of
chronic cancer, immune deficiencies and hepatitis B virus infection
(11–13). However, Tα1 has also been identified
to act as an endogenous regulator of innate and adaptive immune
systems (14). Tα1 serves a unique
function in balancing pro-inflammatory and anti-inflammatory
cytokine production through the regulation of distinct Toll-like
receptors (TLRs) on different dendritic cell subsets (15). Immune system deregulation serves a
critical function in the course of sepsis. Tα1 has exhibited
beneficial effects in late-stage clinical trials for the treatment
of sepsis (16,17). However, to the best of our knowledge,
whether Tα1 is able to regulate the immune system in ALF has not
yet been investigated.
In the present study, a rat model of D-galactosamine
hydrochloride (D-GalN)/lipopolysaccharide (LPS)-induced ALF was
used in order to evaluate the efficacy of Tα1 and its mechanism of
action. More precisely, the present study aimed to quantify the
Tα1-induced pro-inflammatory and anti-inflammatory effects and the
expression of B-cell lymphoma 2 (Bcl-2) and Bcl-2-associated X
protein (Bax) associated with hepatocyte apoptosis and to evaluate
the potential therapeutic interest of Tα1 for ALF.
Materials and methods
Animals and diets
A total of 88 specific-pathogen-free 6-week-old male
Sprague-Dawley rats (weighing 180–220 g) were purchased from the
Laboratory Animal Center of Xi'an Jiaotong University Health
Science Center (Xi'an, China). Rats were housed at a temperature of
23–25°C with a 12-h light/dark cycle and 60–70% humidity. Standard
rodent food and water were supplied ad libitum and rats were housed
for 3 days prior to the experiment to enable them to acclimatize to
their environment.
Drugs and reagents
Tα1 was purchased from SciClone Pharmaceuticals,
Inc. (Foster City, CA, USA). LPS and D-GalN were both purchased
from Sigma-Aldrich (Merck KGaA, Darmstadt, Germany), and dissolved
in aseptic normal saline. Rabbit anti-mouse Bcl-2 (cat. no.
ab59348), Bax (cat. no. ab53154) and GAPDH (cat. no. ab8245) were
all purchased from Abcam (Cambridge, UK). Horseradish peroxidase
(HRP)-labeled goat anti-rabbit antibody (cat. no. TA130015) was
purchased from OriGene Technologies, Inc. (Beijing, China). ELISA
kits for interleukin-10 (IL-10; cat. no. EA100170) and tumor
necrosis factor-α (TNF-α; cat. no. EA101768) were purchased from
OriGene Technologies, Inc. The In-Situ Apoptosis Detection kit was
obtained from Promega Corporation (Madison, WI, USA). Total RNA
Extraction kits were purchased from Omega Bio-Tek, Inc. (Norcross,
GA, USA). The Sensiscript RT kit was purchased from Qiagen, Inc.
(Valencia, CA, USA). SYBR-Green Master mix was obtained from
Applied Biosystems (Thermo Fisher Scientific, Inc., Waltham, MA,
USA).
Animal grouping and drug
administration
A total of 88 rats were randomly divided into two
groups. One group of 25 rats was randomly subdivided into a control
group (CG; saline, n=5), model group (MG; D-GalN/LPS, n=10) and
treatment group (TG; Tα1/D-GalN/LPS, n=10). Survival rates were
recorded for 24 h, then all surviving rats were sacrificed. The
second group (n=63) was randomly subdivided into CG (n=3), MG
(n=30) and TG (n=30). Three rats from the MG and TG groups were
sacrificed at 3, 6, 9 and 12 h after D-GalN injection, and 3 rats
from the CG were sacrificed at 3 h following saline injection. Rats
in the CG group received an intraperitoneal injection of 2 ml
saline. Rats in the MG group received intraperitoneal injection of
D-GalN (700 mg/kg) and LPS (10 µg/kg) to induce ALF. Rats in the TG
group received an intraperitoneal injection of Tα1 (0.03 mg/kg) 1 h
before and 30 min after the establishment of the ALF model. All
animal experiments were approved by the Ethics Committee of Xi'an
Jiaotong University (Xi'an, China) in accordance with the
guidelines of the China Laboratory Animal Management Committee.
Sample collection
Blood samples (~2 ml) were obtained by cardiac
puncture in rats under 10% chloral hydrate anesthesia (300 mg/kg,
intraperitoneally), and then centrifuged at 1,200 × g for 10 min at
25°C. The supernatant was tested for the biochemical indices TNF-α
and IL-10. The rats were sacrificed by cervical dislocation
immediately after blood collection, and a portion of liver tissue
was fixed in 6% paraformaldehyde at 4°C for 24 h in PBS for
pathological examinations. Another portion of liver tissue was
frozen in liquid nitrogen for subsequent measurement of Bax and
Bcl-2 expression.
Liver function tests
Plasma alanine aminotransferase (ALT), aspartate
aminotransferase (AST) and total bilirubin (TBIL) levels were
determined using an LST008 Biochemistry Analyzer (Hitachi, Ltd.,
Tokyo, Japan).
Histopathology
Liver tissue, fixed in 6% paraformaldehyde in PBS,
was dehydrated using ethyl alcohol. Ethyl alcohol in the tissues
was then eliminated with xylene, and the liver sections embedded in
paraffin for sectioning. The 5-µm-thick sections were stained with
hematoxylin for 20 min and eosin for 3 min at 25°C and a light
microscope was used to examine the sections.
TUNEL assay
Fixed liver tissues were permeabilized with 1%
Triton X-100 for 10 min. TUNEL staining was conducted with an
In-Situ Apoptosis Detection kit, according to the manufacturer's
instructions and the results were examined under a light
microscope. The percentage of TUNEL-positive liver cells was
calculated manually following observation. Five higher
magnification images were selected to obtain a quantitative
analysis of the positive cells, and the apoptotic index (AI) was
calculated as follows: AI (%) = apoptotic cell number/total cell
number × 100.
ELISA assay
Plasma levels of TNF-α and IL-10 were measured with
ELISA kits, according to the manufacturer's instructions.
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR)
RT-qPCR for the analysis of Bax and Bcl-2 was
performed as previously described (18). Briefly, total RNA was extracted from
liver tissue using RNA Extraction kits. mRNA was converted to cDNA
using a Sensiscript RT kit according to the manufacturer's
instructions and qPCR was performed using SYBR-Green Master mix,
according to the manufacturer's instructions. The sequences of the
primers used are presented in Table
I. β-actin was used as an internal control and the
2−∆∆Cq method was used to quantify the results (19).
 | Table I.Primer sequences for polymerase chain
reaction. |
Table I.
Primer sequences for polymerase chain
reaction.
| Genes | Primer |
|---|
| β-actin | F:
5′-TCTGTGTGGATTGGTGGCTCTA-3′ |
|
| R:
5′-CTGCTTGCTGATCCACATCTG-3′ |
| Bcl-2 | F:
5′-GGGATGCCTTTGTGGAACTATATG-3′ |
|
| R:
5′-TGAGCAGCGTCTTCAGAGACA-3′ |
| Bax | F:
5′-GACACCTGAGCTGACCTTGGA-3′ |
|
| R:
5′-GACACTCGCTCAGCTTCTTGGT-3′ |
Western blot analysis
Liver tissue was homogenized in lysis buffer (cat.
no. 78510) with protease inhibitor (cat. no. 78443) (both from
Thermo Fisher Scientific, Inc.) by sonication. Protein
concentration was determined using Pierce™ BCA assay
(cat. no. 23225; Thermo Fisher Scientific, Inc.) Total lysate (50
µg/lane) was separated by 12% SDS-PAGE and transferred to
polyvinylidene fluoride membranes. The membranes were then blocked
with 5% milk for 1 h at 25°C and incubated with primary antibodies
against Bcl-2 (dilution 1:500), Bax (dilution 1:500) and GAPDH
(dilution 1:1,000). for 24 h at 4°C. After washing, the membranes
were incubated with appropriate HRP-conjugated secondary antibodies
(dilution 1:5,000) at room temperature for 2 h. Protein bands
obtained were visualized using an enhanced chemiluminescence system
(cat. no. 35055; Thermo Fisher Scientific, Inc.). The protein bands
were detected using the Bio-Rad ChemiDoc™ MP imaging
system (Bio-Rad Laboratories, Inc., Hercules, CA, USA).
Statistical analysis
Statistical analyses were performed using SPSS
version 16.0 (SPSS, Inc., Chicago, IL, USA) and GraphPad Prism 5
(GraphPad Software, Inc., La Jolla, CA, USA). Survival was
evaluated using life tables constructed from survival data with
Kaplan-Meier plots. The comparisons with the model group were
assessed using analysis of variance followed by post hoc multiple
comparison tests (Tukey's) at each time-point. P<0.05 was
considered to indicate a statistically significant difference.
Results
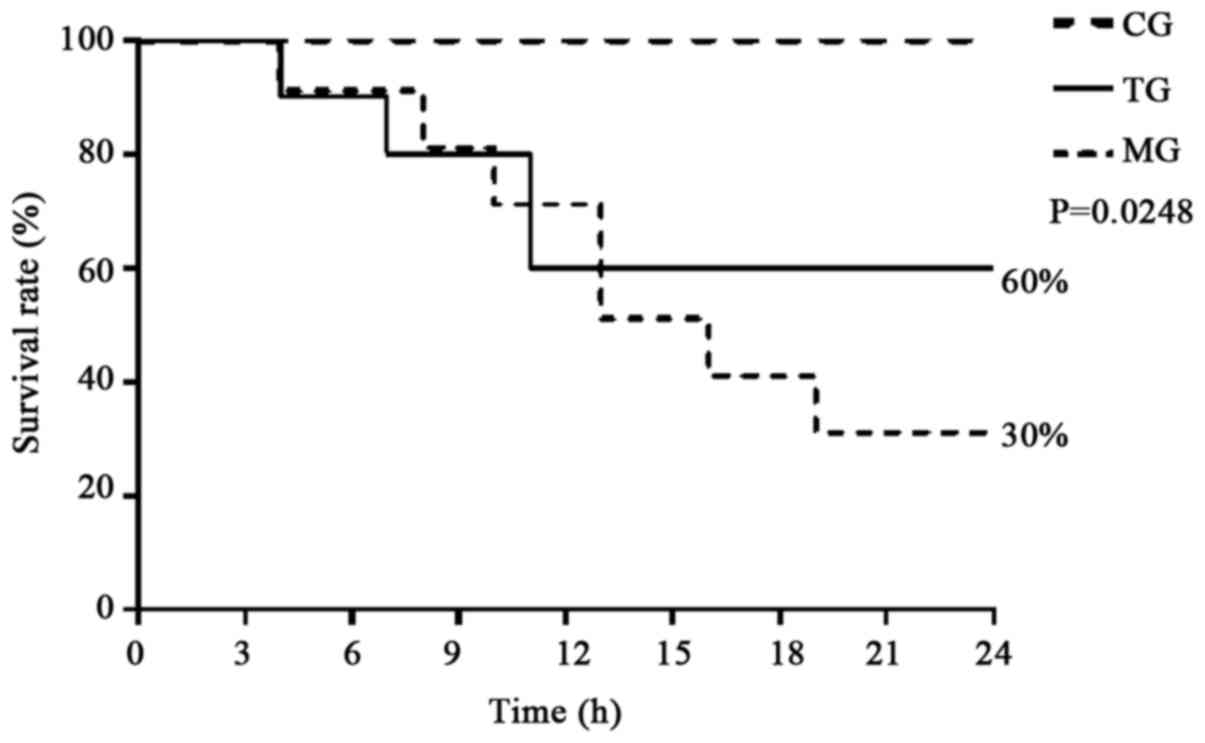
Tα1 treatment improves survival in
ALF
As shown in Fig. 1,
all rats in the CG survived for 24 h, whereas the number of animals
that died increased over time (from 3 to 24 h) in the MG and TG.
The survival rate of the rats was significantly higher in the TG as
compared with the MG (60 vs. 30%, P=0.0248).
Tα1 reduces liver injury in ALF
As shown in Tables
II–IV, the plasma levels of
ALT, AST and TBIL were significantly higher in the TG and MG
compared with the CG at all time-points (P<0.05). Furthermore,
the levels in the TG were significantly lower compared with the MG
at all time-points (P<0.05), with the exception of TBIL at 3
h.
| Table II.Measurements of ALT values at each
time-point. |
Table II.
Measurements of ALT values at each
time-point.
|
| ALT (U/l) |
|---|
|
|
|
|---|
| Group | 3 h | 6 h | 9 h | 12 h |
|---|
| CG | 33.33±4.84 |
|
|
|
| MG |
1,379.33±4.33a |
2,894.50±5.21a |
4,991.97±553.30a |
9,297.43±81.54a |
| TG |
985.50±3.80a,b |
1,863.34±36.89a,b |
2,583.35±174.73a,b |
6,187.67±182.89a,b |
| Table IV.Measurements of TBIL values at each
time-point. |
Table IV.
Measurements of TBIL values at each
time-point.
|
| TBIL (µmol/l) |
|---|
|
|
|
|---|
| Group | 3 h | 6 h | 9 h | 12 h |
|---|
| CG | 3.76±0.45 |
|
|
|
| MG |
7.07±0.61a |
11.60±1.08a |
16.30±0.87a |
22.50±2.11a |
| TG |
6.97±0.60a |
9.23±0.49a,b |
11.37±0.50a,b |
14.67±0.45a,b |
Typical hepatic histopathological features are
presented in Fig. 2. Liver samples
from the control rats exhibited an intact hepatic structure with
normal hepatic lobule, and an absence of hepatocellular necrosis,
hemorrhage or inflammatory cell infiltration (Fig. 2C). By contrast, notable damage was
observed in the MG (Fig. 2A) and TG
(Fig. 2B) samples. Evident
destruction of architecture was observed, with a large number of
apoptotic and necrotic cells in the two groups. In addition,
infiltrating cells and congested red blood cells in the sinusoids
were observed. Furthermore, the features of ALF were aggravated
over time (3–12 h) in the MG and TG. Notably, in the Tα1-treated
rats, the hepatocytes appeared healthier, with fewer apoptotic
cells, as compared with those from the MG at the same
time-points.
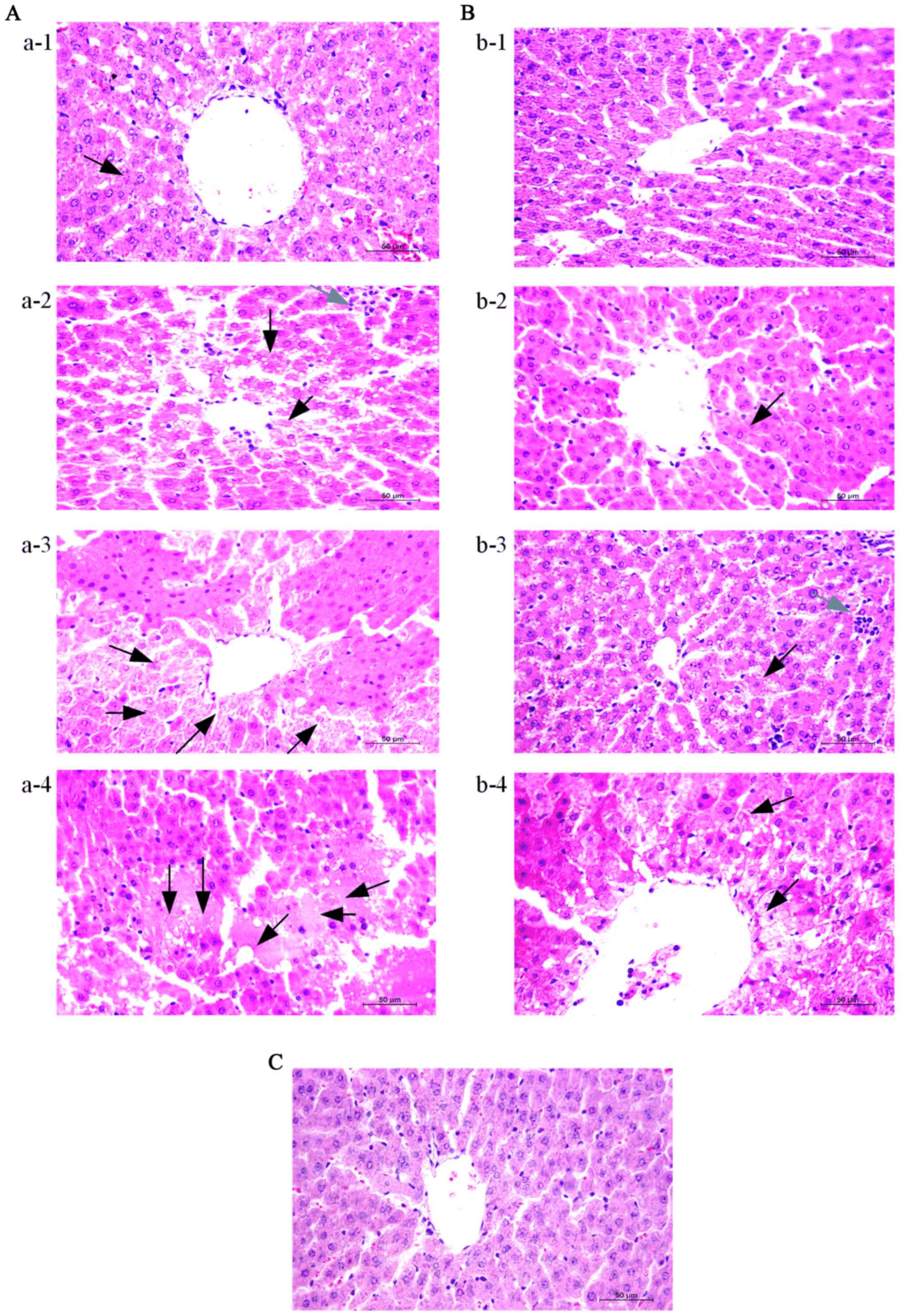 | Figure 2.Thymosin α1 treatment attenuates
hepatic tissue injury in D-galactosamine
hydrochloride/lipopolysaccharide-induced ALF. Liver tissues were
harvested at 3, 6, 9 and 12 h after the establishment of ALF for
histopathological examination (magnification, ×400). Representative
images from 3 rats/group were selected. (A) MG at A-1, 3 h; A-2, 6
h; A-3, 9 h; and A-4, 12 h. (B) TG at B-1, 3 h; B-2, 6 h; B-3, 9 h;
and B-4, 12 h. (C) CG 3 h. Black arrows indicate apoptosis and
necrosis, grey arrows indicate inflammatory cell infiltration. ALF,
acute liver failure; CG, control group; MG, model group; TG,
treatment group. |
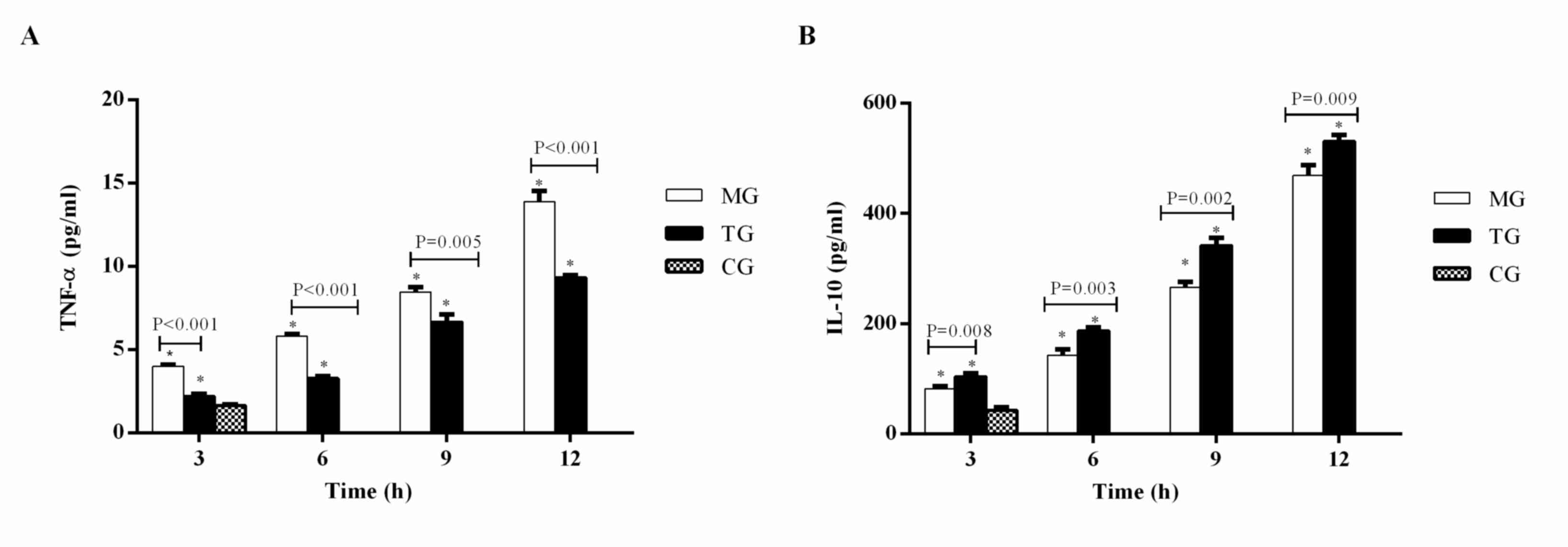
Tα1 inhibits pro-inflammatory TNF-α
and promotes anti-inflammatory IL-10
Plasma TNF-α (Fig.
3A) and IL-10 (Fig. 3B) levels
were significantly higher in the MG and TG compared with the CG at
3 h (P<0.05). Furthermore, the levels of TNF-α and IL-10
increased in the MG and TG at each time-point from 3 to 12 h. The
level of TNF-α was significantly lower in the TG compared with the
MG at each time-point (3 h, P<0.001; 6 h, P<0.001; 9 h,
P=0.005; 12 h, P<0.001), whereas IL-10 was significantly higher
in the TG compared with the MG (3 h, P=0.008; 6 h, P=0.003; 9 h,
P=0.002; 12 h, P=0.009).
Tα1 inhibits hepatocyte apoptosis in
ALF
As shown in Fig. 4,
apoptotic liver cells were observed in the MG (Fig. 4A) and TG (Fig. 4B). The liver cell AI was
significantly higher in the MG and TG compared with the CG at each
time-point. The liver cell AI in the MG and TG increased at each
time-point from 3 to 12 h (Fig. 4C).
The AI in the TG was significantly lower compared with that in the
MG at 6, 9 and 12 h (6 h, P<0.001; 9 h, P=0.002; 12 h,
P<0.001).
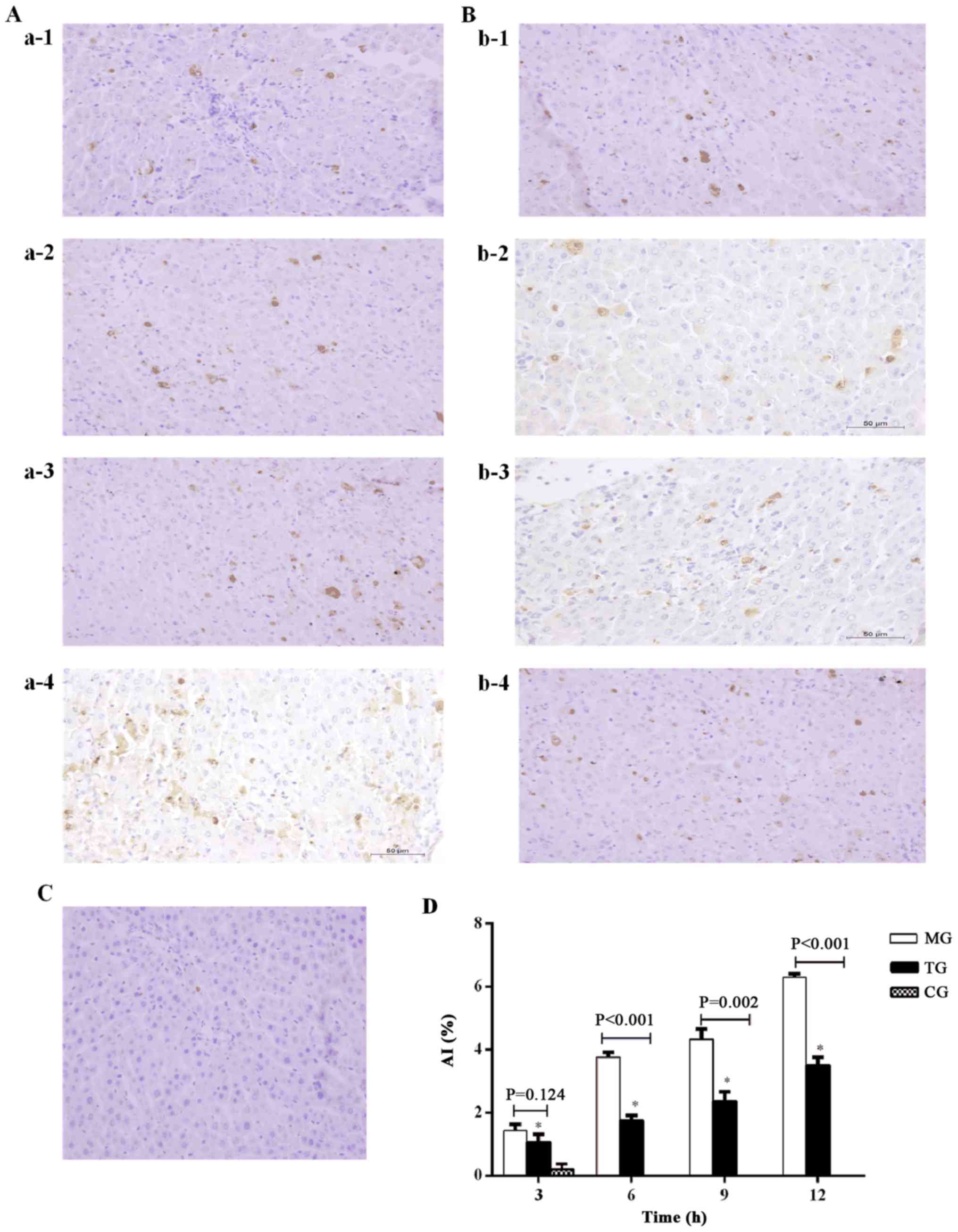 | Figure 4.Thymosin α1 treatment inhibits
hepatocyte apoptosis in D-galactosamine
hydrochloride/lipopolysaccharide-induced ALF. Liver tissues were
harvested at 3, 6, 9 and 12 h after the establishment of a rat
model of ALF and a TUNEL assay was performed (magnification, ×400).
Representative images from 3 rats/group were selected. (A) MG at
a-1, 3 h; a-2, 6 h; a-3, 9 h; and a-4, 12 h. (B) TG at b-1, 3 h;
b-2, 6 h; b-3, 9 h; and b-4, 12 h. (C) CG 3 h. (D) Quantification
of liver cell apoptosis. Data are expressed as the mean ± standard
error of the mean (n=3). *P<0.05 vs. the CG group. ALF, acute
liver failure; CG, control group; MG, model group; TG, treatment
group; AI, apoptotic index. |
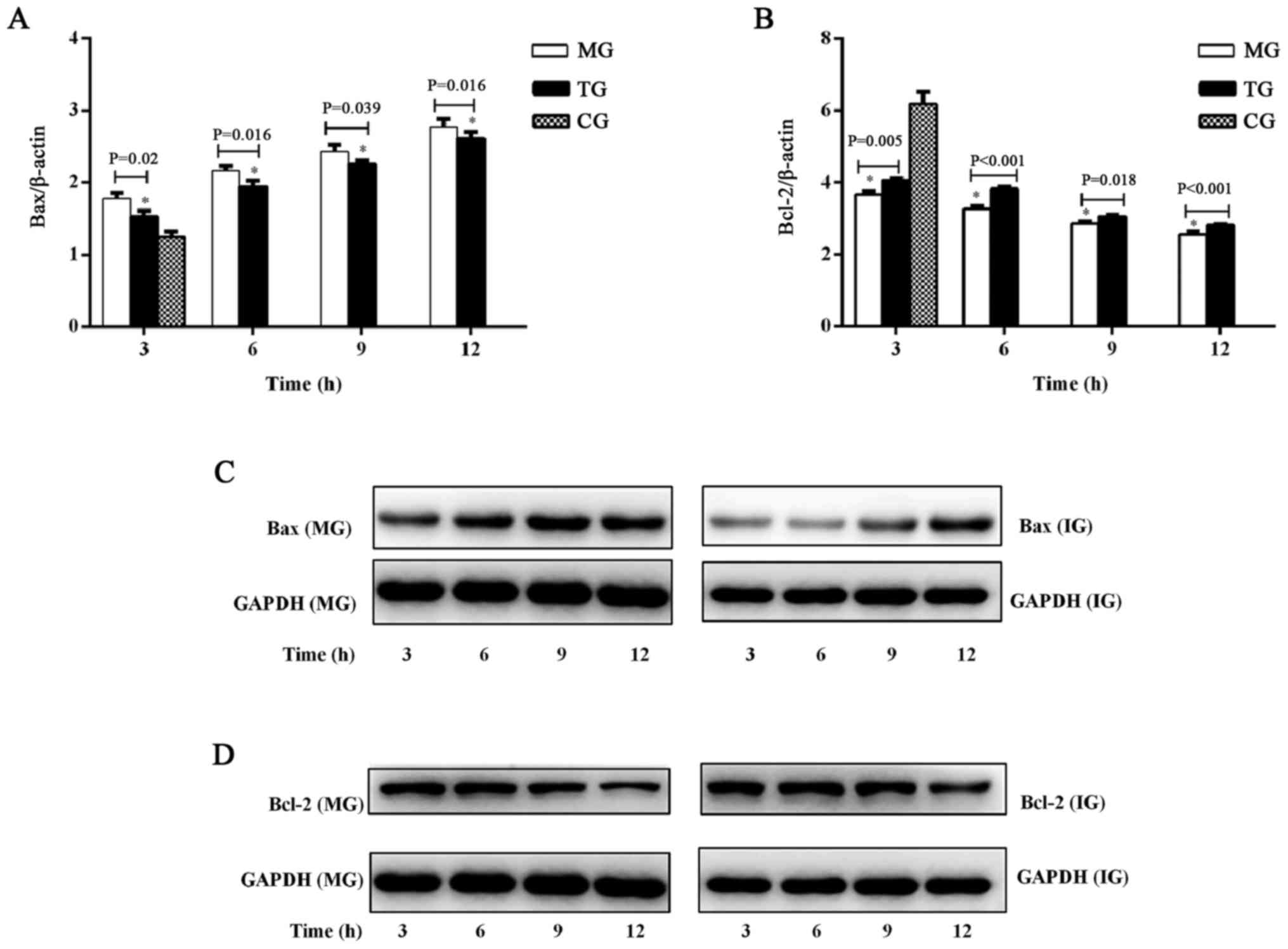
To confirm the apoptotic changes in the liver, Bax
and Bcl-2 were investigated in ALF with or without Tα1 treatment,
using RT-qPCR (Fig. 5A and B) and
western blot analysis (Fig. 5C and
D). Bax mRNA expression was significantly increased in the TG
and MG compared with the CG at 3 h (Fig.
5A). The expression of Bax mRNA (Fig. 5A) and Bax protein (Fig. 5C) increased over time, from 3 to 12
h. The mRNA expression of Bax was significantly higher in the MG
compared with the TG at each time-point (3 h, P=0.02; 6 h, P=0.016;
9 h, P=0.039; 12 h, P=0.016). However, compared with the CG, Bcl-2
mRNA expression was significantly decreased in the TG and MG at all
time-points (Fig. 5B). Bcl-2 mRNA
(Fig. 5B) and protein (Fig. 5D) expression decreased over time,
from 3 to 12 h. Bcl-2 mRNA expression was significantly lower in
the MG compared with the TG at each time-point (3 h, P=0.005; 6 h,
P<0.001; 9 h, P=0.018; 12 h, P=0.01).
Discussion
The present study aimed to investigate the effects
of Tα1 in a rat model of ALF, and to establish an experimental
basis for the administration of Tα1 in the treatment of ALF. The
results demonstrated that administration of Tα1, following the
development of ALF, decreased plasma levels of ALT, AST, TBIL and
TNF-α. Tα1 administration resulted in significantly higher plasma
IL-10, together with reduced hepatic histological damage. Tα1
administration also improved the survival rates in this ALF rat
model, suggesting that Tα exerted an overall beneficial effect by
reducing the inflammatory reaction, decreasing cell damage and
enhancing immune function in ALF rats.
Tα1 has been clinically demonstrated to exert an
immune modulatory activity by promoting the maturation of T cells
and natural killer cells, activating dendritic cells (20–22),
increasing cytokine production, and modulating major
histocompatibility complex class I surface molecules and tumor
antigens (23,24). Therefore, Tα1 has been used to treat
hepatitis B, resistance to infection and breast cancer (13,25,26). Tα1
is a peptide that affects multiple immune subsets associated with
immune suppression (27).
Furthermore, previous studies have reported that Tα1 serves a
critical function in balancing pro- and anti-inflammatory cytokine
production through the involvement of distinct TLRs acting on
different dendritic cell subsets and the MyD88-dependent signaling
pathway (28). Tα1 may attenuate
tissue injury and reduce the mortality rate through reducing the
release of inflammatory factors and cytokines, and increasing IL-10
to control inflammation (21,29,30).
Increased necrosis and apoptosis of hepatocytes is
believed to release various inflammatory cytokines in ALF (31). TNF-α serves a key function in liver
injury and hepatic apoptosis (32,33).
Pro-inflammatory TNF-α expression is markedly upregulated in ALF,
which is critical to reducing the survival rate of mouse models of
ALF induced by D-GalN/LPS (34). The
present study identified that TNF-α and AI in the TG were lower
compared with those in the MG following Tα1 treatment, suggesting
that Tα1 reduced TNF-α levels through the inhibition of apoptosis
to counteract liver failure. Furthermore, the rat mortality rate
decreased with Tα1 treatment, in line with the changes in
TNF-α.
IL-10 is a key cytokine derived from T cells,
macrophages and monocytes, which is able to inhibit the production
of multiple immune active cytokines and to alleviate tissue damage
(35,36). A shift to IL-10 production occurs
following the pro-inflammatory phase and this shift is initiated by
high TNF-α levels (37). In a
previous study, although serum concentrations of TNF-α and IL-10
were increased in ALF, treatment with IL-10 resulted in
normalization of aminotransferase levels, improved liver histology
and reduced fibrosis (38). In
addition, administration of recombinant IL-10 prior to the
establishment of ALF has been demonstrated to reduce the production
of these pro-inflammatory cytokines and improve liver injury
(39). The present study identified
that the plasma levels of IL-10 were higher in the TG compared with
the MG after Tα1 treatment, indicating that Tα1 promoted the
anti-inflammatory cytokine IL-10 to suppress excessive immune
response (particularly inflammatory TNF-α) and prevent further
liver cell apoptosis. Tα1 can also affect the relative ability of
dendritic cells to balance T helper cells and regulatory T cells to
stimulate IL-10 in vitro and in vivo (28). IL-10 in turn negatively regulates the
immune response and prevents a large excess of cytokines, known as
a ‘cytokine storm’ (40).
However, the present study should be regarded as a
pilot study, as it only investigated plasma TNF-α and IL-10, and
the results of immunomodulation in animal models do not directly
translate to clinical settings. Further investigations are required
at the biochemical level (including additional liver function and
cytokine testing) and molecular level (such as gene expression
studies) in order to fully understand the immunological mechanisms
underlying ALF and the effects of Tα1.
In conclusion, the use of immunomodulatory agent Tα1
may have beneficial effects in ALF by alleviating inflammatory
responses and reducing cell, tissue and organ damage. Therefore,
the clinical application of immunomodulation therapy in ALF
treatment deserves further investigation.
Acknowledgements
The present study was supported by The National
Science and Technology Major Project (grant no.
2012ZX10002004-007).
References
|
1
|
Karkhanis J, Verna EC, Chang MS, Stravitz
RT, Schilsky M, Lee WM and Brown RS Jr; Acute Liver Failure Study
Group, : Steroid use in acute liver failure. Hepatology.
59:612–621. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sarin SK and Choudhury A: Acute-on-chronic
liver failure: Terminology, mechanisms and management. Nat Rev
Gastroenterol Hepatol. 13:131–149. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wu Z, Han M, Chen T, Yan W and Ning Q:
Acute liver failure: Mechanisms of immune-mediated liver injury.
Liver Int. 30:782–794. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
European Association for The Study of the
Liver, . Electronic address. simpleeasloffice@easloffice.euClinical
practice guidelines panel. Wendon J Panel members, Cordoba J,
Dhawan A, Larsen FS, Manns M, Samuel D, et al: EASL clinical
practical guidelines on the management of acute (fulminant) liver
failure. J Hepatol. 66:1047–1081. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Xu X, Liu X, Ling Q, Wei Q, Liu Z, Xu X,
Zhou L, Zhang M, Wu J, Huang J, et al: Artificial liver support
system combined with liver transplantation in the treatment of
patients with acute-on-chronic liver failure. PLoS One.
8:e587382013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Krenkel O, Mossanen JC and Tacke F: Immune
mechanisms in acetaminophen-induced acute liver failure.
Hepatobiliary Surg Nutr. 3:331–343. 2014.PubMed/NCBI
|
|
7
|
Jalan R, Gines P, Olson JC, Mookerjee RP,
Moreau R, Garcia-Tsao G, Arroyo V and Kamath PS: Acute-on chronic
liver failure. J Hepatol. 57:1336–1348. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Donnelly MC, Hayes PC and Simpson KJ: Role
of inflammation and infection in the pathogenesis of human acute
liver failure: Clinical implications for monitoring and therapy.
World J Gastroenterol. 22:5958–5970. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Antoniades CG, Berry PA, Wendon JA and
Vergani D: The importance of immune dysfunction in determining
outcome in acute liver failure. J Hepatol. 49:845–861. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Possamai LA, Thursz MR, Wendon JA and
Antoniades CG: Modulation of monocyte/macrophage function: A
therapeutic strategy in the treatment of acute liver failure. J
Hepatol. 61:439–445. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chadwick D, Pido-Lopez J, Pires A, Imami
N, Gotch F, Villacian JS, Ravindran S and Paton NI: A pilot study
of the safety and efficacy of thymosin alpha 1 in augmenting immune
reconstitution in HIV-infected patients with low CD4 counts taking
highly active antiretroviral therapy. Clin Exp Immunol.
134:477–481. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Qiu SJ, Zhou ZG, Shen F, Li AJ, Chen MS,
Ying MG, Chen Z, Zhang YX, Sun HC and Fan J: A multicenter,
randomized, observation-controlled clinical trial to evaluate the
efficacy and safety of thymalfasin adjuvant therapy in patients
with HBV-related HCC after curative resection-first announcement of
the protocol. Expert Opin Biol Ther. 15 Suppl 1:S133–S137. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lao X, Li B, Liu M, Shen C, Yu T, Gao X
and Zheng H: A modified thymosin alpha 1 inhibits the growth of
breast cancer both in vitro and in vivo: Suppressment of cell
proliferation, inducible cell apoptosis and enhancement of targeted
anticancer effects. Apoptosis. 20:1307–1320. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Romani L, Bistoni F, Montagnoli C, Gaziano
R, Bozza S, Bonifazi P, Zelante T, Moretti S, Rasi G, Garaci E and
Puccetti P: Thymosin alpha1: An endogenous regulator of
inflammation, immunity, and tolerance. Ann N Y Acad Sci.
1112:326–338. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Liu F, Wang HM, Wang T, Zhang YM and Zhu
X: The efficacy of thymosin alpha1 as immunomodulatory treatment
for sepsis: A systematic review of randomized controlled trials.
BMC Infect Dis. 16:4882016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wu J, Zhou L, Liu J, Ma G, Kou Q, He Z,
Chen J, Ou-Yang B, Chen M, Li Y, et al: The efficacy of thymosin
alpha 1 for severe sepsis (ETASS): A multicenter, single-blind,
randomized and controlled trial. Crit Care. 17:R82013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Li C, Bo L, Liu Q and Jin F: Thymosin
alpha1 based immunomodulatory therapy for sepsis: A systematic
review and meta-analysis. Int J Infect Dis. 33:90–96. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Xu Y, Wang H, Bao S, Tabassam F, Cai W,
Xiang X, Zhao G, Wu H, Gao T, Li H and Xie Q: Amelioration of liver
injury by continuously targeted intervention against TNFRp55 in
rats with acute-on-chronic liver failure. PLoS One. 8:e687572013.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Peng Y, Chen Z, Yu W, Zhou Q, Xu L, Mao
FF, Huang G, Zhang X, Li S, Lahn BT and Xiang AP: Effects of thymic
polypeptides on the thymopoiesis of mouse embryonic stem cells.
Cell Biol Int. 32:1265–1271. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Romani L, Bistoni F, Gaziano R, Bozza S,
Montagnoli C, Perruccio K, Pitzurra L, Bellocchio S, Velardi A,
Rasi G, et al: Thymosin alpha 1 activates dendritic cells for
antifungal Th1 resistance through toll-like receptor signaling.
Blood. 103:4232–4239. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Yao PL, Lin YC, Sawhney P and Richburg JH:
Transcriptional regulation of FasL expression and participation of
sTNF-alpha in response to sertoli cell injury. J Biol Chem.
282:5420–5431. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Xu YG, Guan XT, Liu ZM, Tian CY and Cui
LC: Immunogenicity in swine of orally administered recombinant
Lactobacillus plantarum expressing classical swine fever virus E2
protein in conjunction with thymosin α-1 as an adjuvant. Appl
Environ Microbiol. 81:3745–3752. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Garaci E, Pica F, Serafino A, Balestrieri
E, Matteucci C, Moroni G, Sorrentino R, Zonfrillo M, Pierimarchi P
and Sinibaldi-Vallebona P: Thymosin α1 and cancer: Action on immune
effector and tumor target cells. Ann N Y Acad Sci. 1269:26–33.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Naylor PH and Mutchnick MG: Immunotherapy
for hepatitis B in the direct acting antiviral era: Reevaluating
the thymosin α1 efficacy trials in the light of a combination
therapy approach. J Viral Hepat. Oct 20–2017.(Epub ahead of print).
PubMed/NCBI
|
|
26
|
Camerini R and Garaci E: Historical review
of thymosin α 1 in infectious diseases. Expert Opin Biol Ther. 15
Suppl 1:S117–S127. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
King R and Tuthill C: Immune modulation
with thymosin alpha 1 treatment. Vitam Horm. 102:151–178. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Romani L, Bistoni F, Perruccio K,
Montagnoli C, Gaziano R, Bozza S, Bonifazi P, Bistoni G, Rasi G,
Velardi A, et al: Thymosin alpha1 activates dendritic cell
tryptophan catabolism and establishes a regulatory environment for
balance of inflammation and tolerance. Blood. 108:2265–2274. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Bozza S, Gaziano R, Bonifazi P, Zelante T,
Pitzurra L, Montagnoli C, Moretti S, Castronari R, Sinibaldi P,
Rasi G, et al: Thymosin alpha1 activates the
TLR9/MyD88/IRF7-dependent murine cytomegalovirus sensing for
induction of anti-viral responses in vivo. Int Immunol.
19:1261–1270. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Yang X, Qian F, He HY, Liu KJ, Lan YZ, Ni
B, Tian Y, Fu XL, Zhang J, Shen ZG, et al: Effect of thymosin
alpha-1 on subpopulations of Th1, Th2, Th17, and regulatory T cells
(Tregs) in vitro. Braz J Med Biol Res. 45:25–32. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Nakama T, Hirono S, Moriuchi A, Hasuike S,
Nagata K, Hori T, Ido A, Hayashi K and Tsubouchi H: Etoposide
prevents apoptosis in mouse liver with
D-galactosamine/lipopolysaccharide-induced fulminant hepatic
failure resulting in reduction of lethality. Hepatology.
33:1441–1450. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Chastre A, Belanger M, Beauchesne E,
Nguyen BN, Desjardins P and Butterworth RF: Inflammatory cascades
driven by tumor necrosis factor-alpha play a major role in the
progression of acute liver failure and its neurological
complications. PLoS One. 7:e496702012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wang K: Molecular mechanisms of hepatic
apoptosis. Cell Death Dis. 5:e9962014. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Zhang P, Shen H, Huang J, Wang H, Zhang B,
Zhou R, Zhong B and Fan X: Intraperitoneal administration of
fetuin-A attenuates D-galactosamine/lipopolysaccharide-induced
liver failure in mouse. Dig Dis Sci. 59:1789–1797. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Boomer JS, To K, Chang KC, Takasu O,
Osborne DF, Walton AH, Bricker TL, Jarman SD II, Kreisel D,
Krupnick AS, et al: Immunosuppression in patients who die of sepsis
and multiple organ failure. JAMA. 306:2594–2605. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Chen X, Wang Y, Luo H, Luo Z, Liu L, Xu W,
Zhang T, Yang N, Long X, Zhu N, et al: Ulinastatin reduces urinary
sepsisrelated inflammation by upregulating IL10 and downregulating
TNF-α levels. Mol Med Rep. 8:29–34. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Volk HD, Reinke P and Döcke WD: Clinical
aspects: From systemic inflammation to ‘immunoparalysis’. Chem
Immunol. 74:162–177. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Nagaki M, Iwai H, Naiki T, Ohnishi H, Muto
Y and Moriwaki H: High levels of serum interleukin-10 and tumor
necrosis factor-alpha are associated with fatality in fulminant
hepatitis. J Infect Dis. 182:1103–1108. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Leifeld L, Cheng S, Ramakers J, Dumoulin
FL, Trautwein C, Sauerbruch T and Spengler U: Imbalanced
intrahepatic expression of interleukin 12, interferon gamma, and
interleukin 10 in fulminant hepatitis B. Hepatology. 36:1001–1008.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Orabona C, Puccetti P, Vacca C, Bicciato
S, Luchini A, Fallarino F, Bianchi R, Velardi E, Perruccio K,
Velardi A, et al: Toward the identification of a tolerogenic
signature in IDO-competent dendritic cells. Blood. 107:2846–2854.
2006. View Article : Google Scholar : PubMed/NCBI
|