Introduction
Erlotinib is a targeted anticancer therapy with
selective inhibitory activity for tyrosine kinase of the epidermal
growth factor receptor (EGFR) (1).
This potent drug is used for treating EGFR mutation positive lung
cancer in advanced stage as well as for other malignancies, such as
hepatic or pancreatic malignant tumors (1). Cutaneous side effects of erlotinib,
such as papulopustular rash, xerosis, pruritus, eczema craquele,
rosacea like dermatitis or paronychia, are well documented
(2); however, the number of reports
regarding cutaneous leukocytoclastic vasculitis (CLCV) are limited
(3). We have found eight published
cases of cutaneous vasculitis induced by erlotinib treatment.
Case report
In 2016, a 58-year old, 60 kg weight, non-smoking
woman was diagnosed with advanced stage of lung adenocarcinoma and
brain metastases. She was treated at the Oncology Clinic with
radiotherapy for the brain and lung lesions, and then received
multiple cycles of platinum-based chemotherapy. Due to worsening
evolution and the new brain metastases, erlotinib monotherapy was
initiated with 150 mg/day dose. After 8 months of initiating the
treatment without any complications, the patient was consulted at
the Dermatology Department for the developing of multiple palpable
round-ovular purpuric lesions, erosions and ulcerations which
appeared bilaterally on the lower legs, and dorsal on the forearm.
Moderate xerosis of skin was also found, especially on the lower
limbs area. No periungual clinical signs were found (Figs. 1 and 2). The lesions were between 3 mm and 1.5 cm
in size, gradually increased in number, became more distributed and
were associated with moderate pruritus and pain. The patient denied
having a fever, abdominal pain, arthralgia or other relevant
subjective symptoms. The presumptive clinical diagnosis of
vasculitis was made. Laboratory results showed moderately elevated
inflammatory analyses, elevated transaminase levels and discrete
anemia. The number of eosinophils was within normal range. The
renal function was unimpaired, and the results of urinalysis were
in normal limits. No other clinical signs or symptoms and
laboratory findings possibly related to an infection or to
inflammatory diseases were noted. For an accurate diagnosis, it is
recommended to perform the lymphoblastic transformation test to
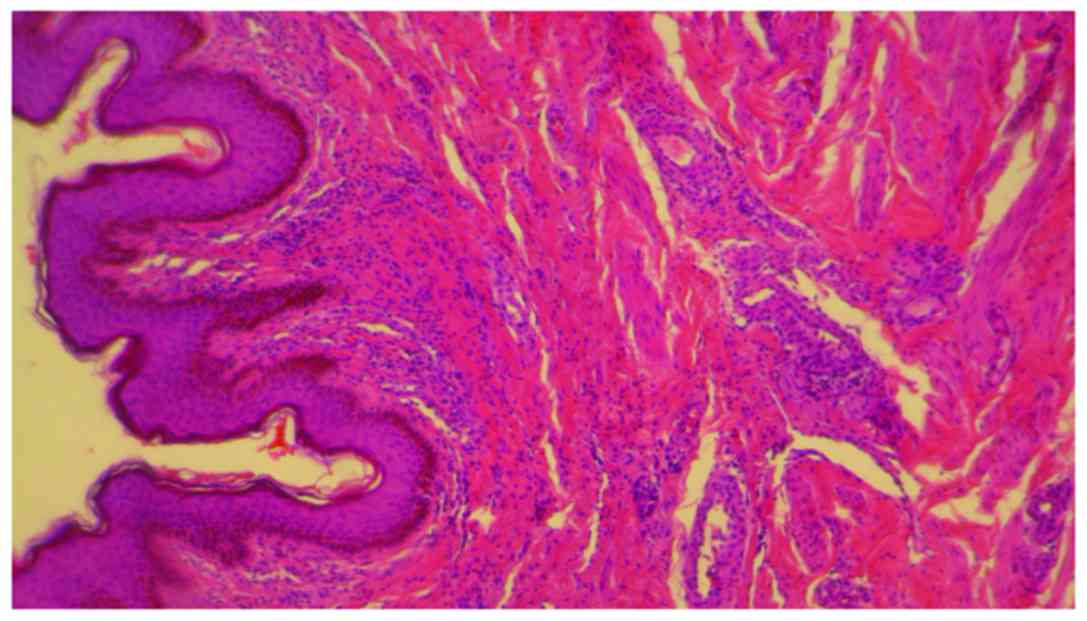
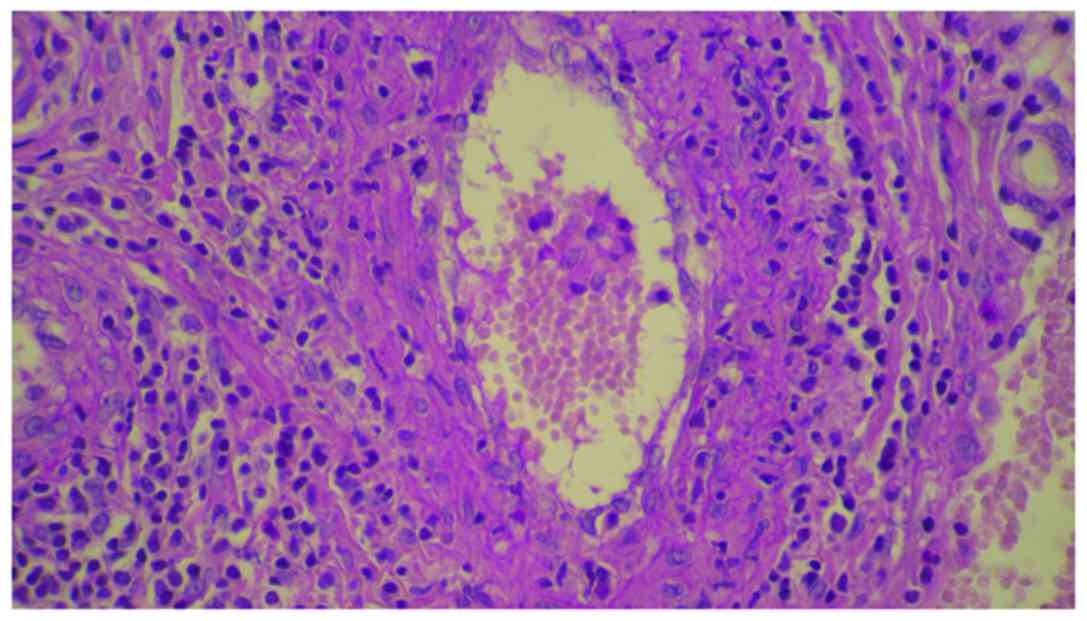
erlotinib, but unfortunately, it was not possible. Skin biopsy was
performed. The histopathology revealed a dense perivascular
neutrophilic infiltration, fibrinoid necrosis of the vessel walls,
leukocytoclastic and red blood cell extravasation, confirming the
diagnosis of cutaneous leukocytoclastic vasculitis (Figs. 3 and 4). The appearance of cutaneous vasculitis
was attributed to erlotinib toxicity. The administration of the
drug was discontinued and oral prednisolone treatment was
introduced at 1 mg/kg body weight dose for two weeks, decreasing
the dose with 5 mg, at every 3 days. The treatment was combined
with topical potent steroid and antibiotic therapy used once,
daily. The lesions cleared within 7 weeks without recurrence. The
treatment with erlotinib was restarted after 14 days with a lower
dose of 100 mg/day, based on the literature data (4). The skin lesions have not recurred.
Unfortunately, the evolution of the metastatic lung cancer was
unfavorable. At 3 months after vasculitis healing, the patient died
due to the complications of new metastases that occurred.
The Ethics approval was obtained from the Commission
of the Mures County Clinical Hospital and the Ethics Committee for
Research of the University of Medicine and Pharmacy of Tirgu Mures
(approval nos. 1537/2016 and 24/2016, respectively), and written
informed consent was obtained from the patient.
Discussion
A thorough review of the literature was performed
using international database search. Available case reports and
current review articles were investigated to provide up-to-date
information about vasculitis induced by erlotinib treatment.
Cutaneous side effects of protein kinase inhibitors, such as
maculopapular rash, hand-foot syndrome, pruritus, bullous
dermatitis, target like purpura, xerosis and vasculitis, are well
documented (3,5,6). Faye
et al in 2013 analyzing ninety-four cases of patients
treated with protein kinase inhibitors, showed that sorafenib was
responsible in 40% of the cases for serious cutaneous adverse
reactions, followed by erlotinib in 25.2% of the cases (2). Regarding the appearance of vasculitis
induced by these drugs, only in one case erlotinib treatment was
found responsible. Zhu et al in 2018 reported on different
adverse cutaneous reactions associated with erlotinib treatment at
20 Chinese patients with cancer. None of them suffered of cutaneous
vasculitis (7). Cutaneous vasculitis
is a well-recognized side effect of many common drugs including
penicillin, sulfonamides, thiazides and oral contraceptives (10–15%
of vasculitis). Other new anticancer targeted therapies have been
found to induce vasculitis, as gefitinib, sorafenib, sunitinib,
bortezomib and everolimus (1,8,9). We searched PubMed/MEDLINE, Google
Scholar, and Web of Science databases and found eight published
cases of cutaneous vasculitis induced by erlotinib treatment
(1,3,4,10–14), one
of the authors presented two clinical cases (4). Erlotinib treatment was indicated in six
cases of lung carcinoma, in two cases of hepatic and in one case of
pancreatic malignancy. In all cases the clinical aspect was of
vasculitis, excepting a case that appeared as Henoch-Schőnlein
purpura (13). In seven cases the
onset of vasculitis occured at the age over 70 years, in two cases
the patients were under 55 years old. Two cases were males, and
seven females. The onset of the vasculitis occurred between 14 days
and 80 days after initiating erlotinib therapy, in our case the
onset was after 240 days. In all the cases the treatment with
erlotinib was stopped and restarted with a lower dose of 100
mg/day, on average after 14 days, or after the disappearance of the
cutaneous lesions. In one case systemic treatment with prednisolone
was introduced similarly to our case. The cutaneous vasculitis
healed between 21 and 80 days. In all cases, systemic
complications, such as renal failure, abdominal discomfort, and
arthralgia, were not mentioned. Boeck et al was the first to
report two cases of cutaneous vasculitis; in both, erlotinib
treatment was stopped, and skin lesions improved with oral steroid
therapy, similarly to our case (4).
In all cases, after a short period of erlotinib withdrawal, the
vasculitis did not appear and we continued with the administration
of a reduced dose of erlotinib.
The mechanism of erlotinib-induced vasculitis
remains unknown, and it is probably a dose-dependent phenomenon, as
the reduced-dose of erlotinib re-administration did not produce
vasculitis. Concerning the evolution of the basic disease and the
efficacity of the lower dose of erlotinib, only Brandi mentioned
that his patient died after 65 months after the occurrence of the
vasculitis (1). In none of the cases
has a new flare of vasculitis appeared. Several studies have
reported so far a connection between the antitumor efficacy of EGFR
inhibitors and cutaneous adverse effects (15–17). Jin
et al reports that multiple cutaneous toxicities could
indicate a good tumor response (14). In our case the fatal evolution, at 3
months after the cutaneous vasculitis healed, possibly indicating
the inefficiency of erlotinib. The late onset of 240 days of the
vasculitis in our case, and the presumed inefficiency of the drug
lead to the speculation that the appearance of cutaneous vasculitis
could be a worsening clinical marker of the tumor response.
Erlotinib induced cutaneous vasculitis are very
rare. The mechanism of erlotinib-induced vasculitis remains
unknown. Some consider that cutaneous vasculitis might reflect
better anticancer efficacy. Our case suggests that cutaneous
vasculitis could be a worsening clinical marker of the tumor
response. This limited number of cases precludes any meaningful
interpretation of data on erlotinib induced cutaneous vasculitis.
Further investigations are needed to assess cutaneous vasculitis
(1). We consider that a complete
clinical examination of the skin at regular intervals is mandatory
for all patients, no matter the type of cancer.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
GLF was responsible for the clinical management of
patient, the evaluation and analysis of data, and contibuted to
writing the manuscript. LF was responsible for the preparation of
biopsy, the analysis of data, and the revision of manuscript for
important intellectual content. The final version of the manuscript
was approved by all authors.
Ethics approval and consent to
participate
The Ethics approval was obtained from the Commission
of the Mures County Clinic Hospital and the Ethics Committee for
Research of the University of Medicine and Pharmacy Tirgu Mures
(approval nos. 1537/2016 and 24/2016, respectively), and written
informed consent was obtained from all the patients.
Patient consent for publication
Written informed consent of the patient were
obtained.
Competing interests
The authors declare that they have no competing
interests.
Authors' information
GLF is the Associate Professor of Dermatology,
Department of Dermatology, Dermatology Clinic, University of
Medicine and Pharmacy, Târgu Mureş, Romania.
References
|
1
|
Brandi G, Venturi M, Dika E, Maibach H,
Patrizi A and Biasco G: Cutaneous leukocytoclastic vasculitis due
to erlotinib: Just an adverse event or also a putative marker of
drug efficacy? Cutan Ocul Toxicol. 32:336–338. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Faye E, Bondon-Guitton E, Olivier-Abbal P
and Montastruc JL: French Network of Regional Pharmacovigilance
Centers: Spontaneous reporting of serious cutaneous reactions with
protein kinase inhibitors. Eur J Clin Pharmacol. 69:1819–1826.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sawada T, Suehiro M and Hiranuma O:
Cutaneous leukocytoclastic vasculitis associated with erlotinib.
Indian J Dermatol. 61:2382016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Boeck S, Wollenberg A and Heinemann V:
Leukocytoclastic vasculitis during treatment with the oral EGFR
tyrosine kinase inhibitor erlotinib. Ann Oncol. 18:1582–1583. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Rezaković S, Paštar Z, Bukvić Mokos Z,
Pavliša G and Kovačević S: Erlotinib-induced rosacea-like
dermatitis. Acta Dermatovenerol Croat. 24:65–69. 2016.PubMed/NCBI
|
|
6
|
Rungtrakulchai R and Rerknimitr P:
Erlotinib induced target-like purpura. Dermatol Online J.
20:62014.
|
|
7
|
Zhu H, Zhu Z, Huang W, Cheng X, He J,
Xiong C and Han J: Common and uncommon adverse cutaneous reactions
to erlotinib: A study of 20 Chinese patients with cancer. Cutan
Ocul Toxicol. 37:96–99. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Panebianco M, Ragazzi M, Asensio NM,
Pagano M, Gnoni R and Boni C: A case of necrotizing vasculitis with
panniculitis, during sorafenib treatment for hepatocellular
carcinoma, appeared in disease progression. J Gastrointest Oncol.
5:E121–E124. 2014.PubMed/NCBI
|
|
9
|
Karadimou A, Migou M, Economidi A,
Stratigos A, Kittas C, Dimopoulos MA and Bamias A: Leukocytoclastic
vasculitis after long-term treatment with sunitinib: A case report.
Case Rep Oncol. 4:385–391. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Takahashi Y, Ebi N, Yamaguchi O, Fukusho
R, Sugimoto Y and Tsuruno K: A case of cutaneous vasculitis caused
by erlotinib treatment and a review of literature. Nihon Kokyuki
Gakkai Zasshi. 49:663–666. 2011.(In Japanese). PubMed/NCBI
|
|
11
|
Hakeem AH, Aziz SA, lone AR, Bhat GM, Wani
B and Hussain I: Erlotinib induced vasculitis. JMSCR. 3:3890–3895.
2015.
|
|
12
|
Su BA, Shen WL, Chang ST, Feng LY, Wu CJ
and Feng YH: Successful rechallenge with reduced dose of erlotinib
in a patient with lung adenocarcinoma who developed
erlotinib-associated leukocytoclastic vasculitis: A case report.
Oncol Lett. 3:1280–1282. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yuba T, Nagata K, Shiotsu S, Okano A,
Hatsuse M, Murakami S, Morihara K and Shimazaki C: Henoch-Schönlein
purpura induced by erlotinib (Tarceva): A case report. Nihon
Kokyuki Gakkai Zasshi. 48:81–85. 2010.(In Japanese). PubMed/NCBI
|
|
14
|
Jin F, Zhu H, Kong L and Yu J: A spectrum
of cutaneous toxicities from erlotinib may be a robust clinical
marker for non-small-cell lung therapy: A case report and
literature review. Onco Targets Ther. 8:943–946. 2015.PubMed/NCBI
|
|
15
|
Liu HB, Wu Y, Lv TF, Yao YW, Xiao YY, Yuan
DM and Song Y: Skin rash could predict the response to EGFR
tyrosine kinase inhibitor and the prognosis for patients with
non-small cell lung cancer: A systematic review and meta-analysis.
PLoS One. 8:e551282013. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Brănișteanu DE, Ianoşi SL, Dimitriu A,
Stoleriu G, Oanţǎ A and Brănișteanu DC: Drug-induced Rowell
syndrome, a rare and difficult to manage disease: A case report.
Exp Ther Med. 15:785–788. 2018.PubMed/NCBI
|
|
17
|
Gheorghe I, Tatu AL, Lupu I, Thamer O,
Cotar AI, Pircalabioru GG, Popa M, Cristea VC, Lazar V and
Chifiriuc MC: Molecular characterization of virulence and
resistance features in Staphylococcus aureus clinical
strains isolated from cutaneous lesions in patients with drug
adverse reactions. Rom Biotechnol Lett. 22:12321–12327. 2017.
|